Albenza
| Contato
Página Inicial

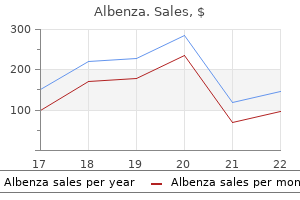
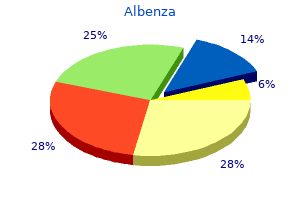
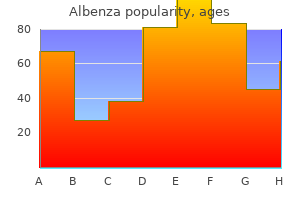
"Albenza 400 mg buy with mastercard, 5 medications related to the lymphatic system".
W. Murat, MD
Co-Director, University of Maryland School of Medicine
Persistent hyperparathyroidism in renal allograft recipients: vitamin D receptor symptoms lactose intolerance discount 400 mg albenza free shipping, calcium-sensing receptor treatment 4s syndrome generic albenza 400 mg mastercard, and apoptosis medicine dosage chart 400 mg albenza buy overnight delivery. An financial comparability of surgical and medical remedy in sufferers with secondary hyperparathyroidism-the German perspective medications vertigo albenza 400 mg discount mastercard. Association of serum phosphorus and calcium � phosphorus product, and parathyroid hormone with cardiac mortality risk in continual hemodialysis patients. The National Kidney Foundation recommends the following postoperative remedy of hypocalcemia: the blood stage of ionized calcium ought to be measured every 12 hours for the first forty eight to 72 hours after surgical procedure after which twice day by day till the patient is stable. The calcium infusion ought to be steadily reduced when the extent of ionized calcium attains the traditional vary and stays steady. When oral consumption is possible, the affected person ought to obtain calcium carbonate 1 to 2 g 3 instances a day in addition to calcitriol of up to 2 g/day, and these therapies ought to be adjusted as essential to maintain the extent of ionized calcium in the regular vary. Parathyroid operate as a determinant of the response to calcitriol therapy in the hemodialysis affected person. Which is the predominant parathyroid pathology seen in sufferers with secondary hyperparathyroidism Embryonic parathyroid rests happen commonly and have implications in the administration of secondary hyperparathyroidism. Allelic loss on chromosome 11 is unusual in parathyroid glands of sufferers with hypercalcaemic secondary hyperparathyroidism. Role of parathyroid intervention within the management of secondary hyperparathyroidism. Secondary and tertiary hyperparathyroidism: causes of recurrent disease after 446 parathyroidectomies. Parathyroidectomy promotes wound healing and prolongs survival in sufferers with calciphylaxis from secondary hyperparathyroidism. Postoperative hungry bone syndrome in sufferers with secondary hyperparathyroidism of renal origin. The uremic gangrene syndrome: improved healing in spontaneously forming wounds following subtotal parathyroidectomy. Subtotal parathyroidectomy versus total parathyroidectomy and autotransplantation in secondary hyperparathyroidism: a randomized trial. Usefulness of the combination of ultrasonography and 99mTc-sestamibi scintigraphy in the preoperative analysis of uremic secondary hyperparathyroidism. However, management of persistent hyperparathyroidism following surgery may be difficult. Careful preoperative evaluation of factors that result in the failure of the initial surgery should be performed prior to reoperative parathyroidectomy. After affirmation of the diagnosis of persistent hyperparathyroidism, all prior operative reviews, pathology stories, and imaging research should be reviewed intimately. Planning for reoperation ought to embrace acquiring new imaging, when indicated, and formulating a methodical operative plan. Surgery may be difficult by tissue fibrosis, edema, irritation, and loss of surgical landmarks. Careful affirmation of the analysis of main hyperparathyroidism is crucial before planning the operation. A detailed discussion with the affected person concerning the risks of reoperative surgical procedure is critical. Personal historical past 1) Endocrinopathies, including thyroid disorders or carcinoma, pheochromocytoma 2) Renal illness (increased probability that subtotal parathyroidectomy is critical for cure) 3) Hypothalamus-pituitary axis illness d. Family history of endocrinopathies (multiple endocrine neoplasia syndromes, familial hyperparathyroidism). Medications 1) Exogenous calcium/vitamin D supplementation 2) Anticoagulants 3) Diuretics (especially thiazides) 4) Use of lithium 5) Allergies Physical Examination 1. Palpation of any midline or lateral neck lots (unlikely, but when present raise the concern of coexistent thyroid pathology or parathyroid carcinoma) b. Signs or symptoms of hypercalcemia 1) Nephrolithiasis 2) Severe osteoporosis 3) Pancreatitis 4) Abdominal pain 5) Extremity (bone and muscle) ache 6) Depression, anxiousness, fatigue b. Specimens removed (assessment of measurement, weight and variety of glands eliminated or biopsied, thyroid removal). This helps to avoid pointless exploration in regions devoid of parathyroid tissue. Complications encountered: the presence of preexisting vocal fold paralysis would significantly influence the random exploration of the paratracheal area on the ipsilateral aspect of the functioning vocal fold to stop tracheostomy. Ultrasound of the neck: identifies concomitant thyroid illness and doubtlessly irregular parathyroid glands 2. Dexa bone density scan: Patients with extreme osteoporosis, particularly with pathologic fractures, must strongly be thought-about for reoperation, even if persistently nonlocalizing. Persistent symptomatic hypercalcemia within 6 months following prior parathyroidectomy 2. Recurrent main hyperparathyroidism larger than 6 months following parathyroidectomy three. Bone mineral density higher than 2 normal deviations under gender- and age-matched group (z rating <-2. Recurrent laryngeal nerve damage contralateral to parathyroid adenomas (relative) 3. Inferior parathyroid glands: the inferior parathyroids, just like the thymus, are derived from the third branchial pouch. They are more variable in place because of their longer descent however are sometimes discovered along the posterolateral aspect of the inferior thyroid pole, superficial (anterior) to the airplane of the recurrent laryngeal nerve. Paralysis or paresis of recurrent laryngeal nerve Postoperative hypocalcemia Intraoperative hemorrhage from innominate artery Esophageal perforation Surgical Technique 1. Lateral strategy (especially in localizable illness by imaging during which the affected person has had prior midline strategy. The senior author prefers the lateral method for unilaterally localizable disease. Use of gamma probe to establish parathyroid adenoma (useful adjunct in re-exploration if the offending gland is localizable on Tc99m Sestamibi imaging)5 c. Bipolar cautery: essential for careful dissection in beforehand dissected tissues 3. Recurrent laryngeal nerve: the nerve ascends in the tracheoesophageal groove bilaterally, coming into the larynx at the inferior border of the inferior pharyngeal constrictor. External branch of superior laryngeal nerve: this department provides the cricothyroid muscle. It descends alongside the inferior constrictor muscle within 1 cm of the superior pole of thyroid. In roughly 20% of instances, the nerve could additionally be closely adherent to the superior pole. Inadequate preoperative localization Failure to identify recurrent laryngeal nerve Insufficient four gland exploration Incorrect diagnosis of major hyperparathyroidism. In cases of hypercalcemia Reoperative Parathyroidectomy 581 scenario, which might represent secondary hyperparathyroidism, metabolic bone disease with or without vitamin D deficiency, or persistent main hyperparathyroidism. Parathyroid positioned in paratracheal groove after sufficient mobilization and medial retraction of thyroid gland. Right lateral approach for reoperative parathyroidectomy using methylene blue as an intraoperative adjunct and demonstrating a right superior parathyroid adenoma and a standard inferior gland. Answer It is clear that reoperative surgery represents a challenge because of the elevated risk of ectopic gland location, likelihood of multiple gland disease, and the presence of postsurgical scarring from the initial surgical exploration. Nuclear drugs examination with Sestamibi scanning is paramount in identifying metabolically lively parathyroid tissue. This allows for the identification of ectopic parathyroid tissue in additional than 80% of cases. Failure to protect adequate volume of practical parathyroid tissue or think about reimplantation of a portion of a gland into a well-vascularized recipient bed Editorial Comment Parathyroid surgery for primary hyperparathyroidism has a high success rate on preliminary surgical procedure, but reoperative surgical procedure faces particular challenges that will include irregular affected person anatomy, scarring from earlier surgery, and concomitant thyroid pathology. Detailed evaluation of earlier reviews and operative attempts, as properly as repeat attempts at localization, is essential in maximizing success. When possible, reoperative surgical procedure ought to be carried out by skilled parathyroid surgeons in the presence of intraoperative parathyroid hormone monitoring. Excision effectivity of radioguided occult lesion localization in reoperative thyroid and parathyroid surgery. Reoperative parathyroidectomy: an algorithm for imaging and monitoring of intraoperative parathyroid hormone levels that results in a successful centered method.
Together medicine 02 generic 400 mg albenza with amex, these distinct oncologic features mix to make most cancers of the floor of the mouth one of the extra aggressive and potentially lethal neoplasms of the oral cavity medicine ball chair 400 mg albenza discount amex. Patient selection and careful preoperative planning are essential for optimizing oncologic and practical outcomes medicine numbers generic albenza 400 mg without prescription. Reconstructive efforts ought to purpose to provide cheap cosmesis whereas restoring competent physiologic function to each speech and swallowing symptoms 32 weeks pregnant 400 mg albenza cheap with visa. Airway planning, both at the time of surgery and through the postoperative recovery, is important for limiting morbidity and mortality. The role of the elective neck dissection stays controversial however seems to supply a survival benefit. Thus assessment of surgical candidacy sometimes requires a multidisciplinary method, which includes evaluations by internal medical specialists, medical and radiation oncologists, speech and swallow therapists, nutritionists, and anesthesiologists. For those deemed match enough to bear surgical resection, the surgeon must next assess the resectability of the most cancers. Particular consideration is paid to the presence of local invasion into surrounding constructions of the oral cavity. An correct evaluation of the relationship of the most cancers to the lingual floor of the mandible helps to define surgical planning and method. In the immediate preoperative setting, clear and concise communication between surgeon and anesthesiologist is paramount for safe airway administration. A retrospective review of 320 patients with cancer of the floor of the mouth by Shaha et al. Approaching patient selection as a perfunctory preoperative train is a grave disservice to the patient. However, a diligent history and bodily examination, along with a multidisciplinary approach towards surgical optimization, can place the affected person for a profitable surgical end result. Thus a systematic method to affected person selection is crucial not only for figuring out surgical candidacy but additionally for maximizing oncologic and functional surgical outcomes. The foundation of the preoperative analysis is the historical past and bodily examination. Squamous cell carcinoma of the ground of the mouth is extremely related to the consumption of tobacco and alcohol. Review of occupational calls for, significantly of those in the culinary industry, and of speech requirements. Mandible 1) Bimanual palpation of the cancer and mandible has been demonstrated to be superior to imaging in predicting cortical invasion. Neck 1) Palpation of each necks in the analysis of nodal metastasis 2) Postradiation skin changes, which can point out the presence of neck fibrosis 3) Previous neck incisions, which may indicate prior surgeries. Malnutrition, cachexia 1) Present in 50% of head and neck most cancers patients3 2) Independent predictor of survival4 2. Oral cavity 1) Observation a) Exophytic b) Deep infiltration c) Ulcerations d) Papillary Imaging 1. Routine examination of the oral cavity revealed an early cancer of the floor of the mouth. This was managed by excision of the most cancers and reconstruction with a split-thickness pores and skin graft on the time of the laryngectomy. Edentulous affected person with hypoplastic mandible with cancer that might otherwise meet standards for marginal mandibulectomy d. Cancer abutting diseased dentition with involvement of the periodontal ligament four. Wide native three-dimensional excision of soppy tissue only; most cancers not approaching or involving the mandible 2. Cancer in shut proximity to the mandibular periosteum with no evidence of bone invasion c. Cancer abutting wholesome dentition with out involvement of the periodontal ligament 3. Cancer invasion to the occlusal surface of the mandible in an edentulous patient Excision of Cancer of the Floor of the Mouth 213 1) Nutrition a) Gross abnormalities may delay surgical procedure or restructure postoperative nutrition planning. Nasotracheal intubation-better publicity with out the endotracheal tube in the oral cavity b. Marking pen used to draw a minimal of a 1-cm margin of normal mucosa surrounding the most cancers f. If the papilla is within the space marked for surgical resections, the duct may be canalized with a lacrimal probe to help in successful rerouting of the ductal structure. After sufficient time for the native vasoconstriction to take place, the mucosa is incised with either monothermy or needle-tip cautery. A 2-0 silk suture is positioned in the anterior edge of the specimen to mark the anterior margin. The deep margin of resection is established on the stage of the sublingual glands. A nondepolarizing neuromuscular agent is normally required so as to acquire acceptable access to the floor of mouth. If the submandibular gland is preserved and the proximal ductal architecture is contained throughout the resection, ductal rerouting ought to be performed. This is most easily achieved by following the lacrimal probe placed within the duct initially of the case. The finish of the transected duct is then sutured to the remnant flooring of the mouth mucosa. A Dobhoff feeding tube is then handed and secured with a 3-0 silk secured to the nasal septum. The mucosal margins of resection are outlined initially of the case with a surgical marker. Although the first cancer could be resected separately from the mandible, every effort ought to be made to resect both the mandible and gentle tissue en bloc to help in the orientation for the pathologist. If the patient is dentulous, the tooth adjoining to the deliberate margin is extracted in preparation for vertical osteotomies, which are carried out in the tooth socket, preserving as much bone as potential to help the residual tooth without compromising the surgical margins. A needle-tip bovie is used to make the index incisions through the mucosa and carried down by way of periosteum onto the mandibular cortex. A Freer or periosteal elevator is used to gently elevate the mucoperiosteum to expose the mandibular cortex. A horizontal reciprocating saw is positioned at the anterior aspect of the canine extraction web site in preparation for the vertical osteotomy. In planning the inferior extent of the vertical osteotomy, care is taken to remove only the alveolar process whereas preserving no less than 1. It is important that the buccal and lingual plates of bone be minimize throughout in order to stop splintering or fracturing the bone. Once the lingual cortex is minimize via and the mandibular fragment is freed, the bone is retracted superiorly and posteriorly together with the delicate tissue and the the rest of the resection is then carried out. The bony margins of the mandible are smoothed with a cutting bur to remove any spicules of bone or sharp corners. A split-thickness skin graft can be used to resurface each the delicate tissue and the residual mandibular bone. A Dobhoff feeding tube is then handed and secured to the nasal septum with a 3-0 silk. Two main surgical approaches are available: intraoral/ cervical "pull by way of" or mandibulotomy. Intraoral/transcervical "pull through" 1) the lateral margins surrounding the cancer are established with a monothermy needle tip and prolonged with sharp dissection. A first primary cancer had been excised elsewhere from the left floor of the mouth 25 years earlier than this second main appeared. Some patients could have destruction of the anterior phase of the mandible with infiltration of the skin of the chin, which is taken with the specimen. Dental extractions are carried out in the dentulous patient at the website of osteotomy. A periosteal or Freer elevator is used to free the periosteum from the underlying mandibular cortex. Osteotomies are made with a reciprocating saw positioned at the anterior facet of the tooth extraction web site. Excision of the recurrent cancer and a marginal mandibulectomy of the anterior segment of the mandible were carried out en bloc. Overly aggressive marginal mandibulectomy, leaving an inferior alveolar ridge of lower than 1 cm of remaining bone 3.
Neural monitoring of motor perform provides guidance in neural mapping of the placement of the motor nerve fibers on the surface of the tumor symptoms 5 days post embryo transfer purchase albenza 400 mg amex. This supplies additional accuracy in preventing harm to the first nerve during enucleation treatment croup buy albenza 400 mg visa. One should consider function-sparing intracapsular enucleation because the therapy of selection for cervical schwannomas by which the first nerve of origin nonetheless has vital neural operate medications memory loss albenza 400 mg cheap amex. Additional concerns for determination making in schwannoma treatment have been summarized by other authors treatment molluscum contagiosum albenza 400 mg buy online. Infratemporal fossa approach to lesions within the temporal bone and base of the skull. Endoscopic endonasal dissection of the pterygopalatine fossa, infratemporal fossa, and post-styloid compartment. Anatomical relationships and significance of the eustachian tube in endoscopic skull base surgery. What space is now exposed and which important vascular construction should be identified subsequent Subtemporal-preauricular infratemporal fossa strategy to giant lateral and posterior cranial base neoplasms. Intracranial extension happens via the skull base foramina and by the erosion of bone. Early signs embody unilateral nasal obstruction and recurrent unilateral epistaxis. Large tumors can displace regular constructions, leading to facial swelling, proptosis, diplopia, visible loss, and facial hypesthesia. The major therapy is surgical excision, with endoscopic surgical procedure changing open approaches for most tumors. It can even differentiate the tumor from obstruction of a sinus with retained secretions. The blood provide is often derived from branches of the external carotid artery (internal maxillary and ascending pharyngeal arteries) and is often bilateral in larger tumors. If a biopsy is necessary, it must be performed beneath general anesthesia with management of the airway. For small tumors, an various selection to embolization is surgical ligation of the interior maxillary artery lateral to the tumor margin firstly of the operation. In older sufferers, surgical procedure can be delayed for a quantity of weeks to enable banking of autologous blood for transfusion. The inside carotid arteries (arrows) and tumor vasculature seem as circulate voids. Positioning � Supine � Mayfield headholder If intraoperative navigation is used for skull base involvement, the top can be mounted in a Mayfield head holder to preserve accuracy of navigation, to stabilize the pinnacle for the drilling of bone, and to enhance positioning. Angiography demonstrates a large amount of residual vascularity from the interior carotid artery following embolization of the inner maxillary artery (see coils in proximal trunk). The normal relationship of the pterygoid canal and foramen rotundum are visible on the contralateral side. Prerequisite Skills � Endoscopic sinus surgery � Caldwell Luc approach � Medial maxillectomy. The pterygoid canal containing the vidian nerve and artery is positioned inferomedial to the lateral recess of the sphenoid sinus and is instantly behind the sphenopalatine foramen. The nerve is often stretched over the surface of the tumor and the contents of the pterygopalatine space have to be dissected from the surface of the tumor in a medial to lateral path to protect this nerve. Injury to the larger palatine nerve leads to ipsilateral numbness of the palate. This sensory nerve is a terminal branch of the maxillary nerve and have to be preserved to forestall numbness of the cheek. Surgical Technique the choice of surgical approach is decided by the stage of the tumor (extent and vascularity). Larger tumors with residual vascularity would require augmentation with a transmaxillary approach. Tumors with lateral extension to the middle cranial fossa or infratemporal space could benefit from a mixed anterior and lateral (infratemporal) strategy. Palatal incision, LeFort I osteotomy, lateral rhinotomy, and facial translocation are approaches that have been largely supplanted by endoscopic methods. The choice of strategy also depends on the traits of the patient (age, size) and the expertise of the surgeon with different approaches. Endoscopic Endonasal Approach � the nasal cavity is decongested with cottonoid pledgets soaked in 0. Juvenile Angiofibroma 823 � Nasal endoscopy is carried out to assess the extent of the tumor. Overlying bone is removed with Kerrison rongeurs (1 to 2 mm) to expose the pterygopalatine space. The removing of bone extends lateral to the margin of the tumor and superiorly towards foramen rotundum. The inferior portion of the middle turbinate is resected with sinus scissors or thru-cutting ethmoid forceps. Removal of ethmoid air cells continues posteriorly with exposure of the roof of the ethmoid and the medial wall of the orbit. If possible, the anterior wall of the sphenoid sinus is opened superior to the tumor. Care is taken to keep away from any instrumentation of the tumor, though its floor could be bluntly dissected from the anterior cranial base and gently displaced inferiorly. A sphenoidotomy is carried out with elimination of the podium to provide binarial access. The overlying tissues are dissected from medial to lateral to find a way to protect the larger palatine nerve, which is usually displaced anteriorly by the tumor. Dissection proceeds on the surface of the tumor with supply of nodules of tumor from the masticator space and posterior to the maxilla. The tumor is bluntly dissected from the bone and the vidian artery (and nerve) is cauterized using bipolar electrocautery. Large tumors could be divided into vascular segments using ultrasonic (Harmonic scalpel, Ethicon) and radiofrequency (Coblation, Smith & Nephew) ablation. The delicate tissues at the pyriform aperture are incised with electrocautery and the periosteum is elevated with a Cottle elevator from the edge of the bone and the anterior wall of the maxilla. The masseter muscle is separated from the inferior margin of the zygomatic arch with electrocautery. The periorbita is elevated from the lateral wall of the orbit and the inferior orbital fissure is identified. The ultimate osteotomy throughout the malar eminence, connecting to the inferior orbital fissure, releases the orbitozygomatic bone phase for removal as one unit. Common Errors in Technique � Inadequate exposure Exposure is enhanced with a medial maxillectomy and bilateral sphenoidotomies. A Caldwell Luc method supplies added room for instrumentation, particularly the introduction of bipolar electrocautery forceps. It is sometimes helpful to manually palpate the gentle tissues intraorally to help to deliver the tumor into the surgical area. Transmaxillary Approach � A medial maxillectomy is carried out endoscopically (see Chapter 106). If a Caldwell Luc strategy was used, oral hygiene with a chlorhexidine rinse is prescribed. Most widespread sites for residual tumor include the cavernous sinus, middle cranial fossa, and masticator space. Small remnants of tumor could not develop and could be monitored until vital progress is observed. It could also be considered for a poor surgical candidate because of medical co-morbidities or refusal of surgery. Vascular segments of the tumor ought to be addressed sequentially to control blood loss.
Supernumerary (more than four) parathyroid glands could occur in up to treatment xerophthalmia purchase albenza 400 mg line 15% of the inhabitants treatment 1st metatarsal fracture albenza 400 mg discount mastercard, and 1% to 3% of parathyroid glands are ectopic treatment 4 letter word albenza 400 mg on-line. A palpable mass in the neck in the affected person with hypercalcemia may indicate parathyroid carcinoma treatment yeast infection male 400 mg albenza order with amex. Symptoms of hypercalcemia 1) Urinary system: Polydipsia, polyuria, nephrolithiasis 2) Skeletal system: Osteopenia, osteoporosis, or osteitis fibrosa cystic, which presents with bone pain, pathologic fractures, and/or "brown tumors" Imaging 1. Invasive localization strategies could additionally be employed if earlier imaging is nonlocalizing or conflicting. Selective venous sampling and arteriography effectively localize pathologic parathyroid glands. Associated with risks corresponding to hematoma of the groin, potential embolic occasions, and contrast-induced anaphylaxis or acute kidney injury three. Ultrasound 1) Parathyroid adenomas have a homogeneous hypoechoic appearance on ultrasound. Video-assisted (endoscopic) parathyroidectomy is a minimally invasive technique that has wonderful security and outcomes. Monitoring � Routine anesthesia monitoring � Generally no neural intraoperative monitoring is important, but could additionally be used depending on surgeon choice. Instruments and Equipment to Have Available � � � � � � � � Basic head and neck set Ultrasonic scalpel for thyroidectomy Monopolar and bipolar cautery Kittner/peanut sponges for blunt dissection, retraction, and safety of nerves from thermal vitality Babcock forceps are helpful in greedy and retracting thyroid tissue. McCabe dissector � Its curved, precise, nonlocking ideas are glorious for identification and dissection of nerves. Ectopic places of the superior (B, partially descended; D, tracheoesophageal groove; G, mediastinal) and inferior (A, undescended; C, intrathyroid; E, mediastinal outlet; F, intrathymic; H, anterior mediastinal) parathyroid glands. Once an enlarged parathyroid gland is identified, dissect it circumferentially from surrounding buildings before sealing the vessels (Video 84. Excise the parathyroid gland and send for frozen section evaluation in order to verify that it was indeed parathyroid tissue that was eliminated. Over 95% of adenomatous parathyroid glands are eliminated transcervically, however a median sternotomy could also be needed if a mediastinal enlarged gland is inaccessible via the neck. Conclude the process by reapproximating the strap muscle tissue and platysma with interrupted absorbable sutures, and shut the skin with a running subcuticular absorbable suture or adhesive Steri-Strips. The objective of parathyroid surgical procedure is to induce eucalcemia that lasts a minimal of 6 months after the operation. Persistent or recurrent hyperparathyroidism is the most common complication, occurring in as much as 5%. Given the elevated problem and complication rates related to re-exploration of the neck, extensive preoperative analysis is acceptable. Reoperative surgical procedure 1) Even in reoperation, the most common explanation for hyperparathyroidism is a single adenoma, so a centered method could additionally be acceptable with optimistic localization. Reoperation leads to related success rates as initial procedures when carried out by experienced surgeons. Evacuation of a cervical hematoma is required in lower than 1% of all parathyroidectomy sufferers. Common Errors in Technique � Poor hemostasis resulting in staining of the surgical area � the airplane between the strap muscular tissues and thyroid capsule is particularly vascular. Presents with paresthesias and numbness however can progress to life-threatening tetany, seizures, and arrhythmias. Treatment involves oral calcium and calcitriol; intravenous calcium may be administered if the patient remains symptomatic regardless of oral supplementation. Presents with hyperthyroidism within the quick postoperative part, but hypothyroidism might result long run financial savings in comparison with scintigraphy. However, sonography is proscribed by operator dependence, and patient elements corresponding to gland dimension, body mass index, and serum calcium can additional influence its accuracy. A combination of these two comparatively cheap, minimally invasive strategies likely leads to the best outcomes, since concurrence between ultrasound and planar sestamibi results indicates wonderful accuracy. Abnormal parathyroid glands normally appear hypointense on T1 and hyperintense on T2. A robust information of thyroid and parathyroid embryology and anatomy will assist the surgeon. Fortunately, advances in imaging and intraoperative serology have aided the surgeon in enhancing success and lowering operative time. Accuracy of early-phase versus dual-phase single-photon emission computed tomography/ computed tomography within the localization of parathyroid disease. Guidelines for the management of asymptomatic major hyperparathyroidism: abstract assertion from the Fourth International Workshop. Is minimally invasive parathyroidectomy associated with higher recurrence in comparability with bilateral exploration Factors contributing to negative parathyroid localization: an analysis of 1000 sufferers. [newline]Sensitivity for proper lateralization of the hyperfunctioning gland with this modality varies widely, but most report rates above 70%. Unfortunately, this leaves a significant cohort with nonlocalizing scans, even when the etiology is a single adenoma. When carried out by skilled surgeons, ultrasound may be more delicate than planar sestamibi,5 even in the presence of multiglandular disease. In which of the next situations is preoperative localization of the abnormal parathyroid gland(s) most useful Elderly asymptomatic affected person with normal bone mineral density however elevated serum calcium c. Patient who has undergone previous parathyroidectomy however has persistent hyperparathyroidism. Which of the following is false with regard to intraoperative identification of parathyroid glands Superior parathyroid glands are mostly discovered on the posterolateral surface of the higher two-thirds of the thyroid lobes d. However, he presents 2 months later with persistently elevated serum calcium and worsening bone ache, fatigue, and memory issues. Attempt to localize the irregular parathyroid gland(s) with both sonography and sestamibi scintigraphy d. Combining the methods results in slightly improved sensitivity than ultrasound alone). The surgical strategy should give consideration to an accurate steadiness between the extent of parathyroid resection with prevention of recurrence while also minimizing everlasting hypoparathyroidism. Therefore built-in, multidisciplinary care is vital to detect one of the best surgical timing as well as cautious postoperative care to management for metabolic alterations. Increased parathyroid function is stimulated by calcium deficiency (presenting with normocalcemia or hypocalcemia); thus the parathyroid gland has no functional autonomy. The hypertrophic gland transformation occurs over years of progressive kidney illness. Subsequently, some cells contained in the parathyroid gland can proliferate in a monoclonal growth pattern, which ends up in an advanced sort of nodular hyperplasia. Whether a regression of parathyroid hyperplasia can occur after medical remedy with calcitriol or vitamin D3 remains uncertain. Also, regression of parathyroid hyperplasia has been reported in uncommon cases of spontaneous infarction of the glands. However, the required medications may be expensive, and the price of 9 months of calcimimetic remedy could exceed that of surgical therapy. However, abnormalities could also be already detectable by laboratory or radiographic studies. Current therapeutic methods include the modification of calcium and phosphorus balance by restricting the intake of dietary calcium and phosphorus and their removal during hemodialysis in addition to the administration of phosphate binders, vitamin D receptor activators (calcitriol and newer vitamin D analogues), and a calcimimetic. The glandular growth/hyperplasia is hyperactive, irregular, asymmetrical, and asynchronous; this course of is expounded to the time on dialysis till the parathyroid gland finally turns into autonomous. This condition, referred to as tertiary hyperparathyroidism, can jeopardize the transplant surgery and long-term viability of the transplanted kidney. Surgical intervention ought to be thought of in symptomatic patients who current with bone or muscle ache, muscle weak point, irritability, pruritus, bone loss, the exacerbation of anemia because of resistance to erythropoietin, or worsening cardiomyopathy. There are patients who develop resistance or intolerance to medical therapy; they too should be considered candidates for surgical intervention.
Albenza 400 mg generic with visa. Marijuana withdrawal symptoms - You must see it !!.