
Cipro
| Contato
Página Inicial

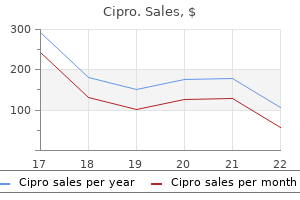
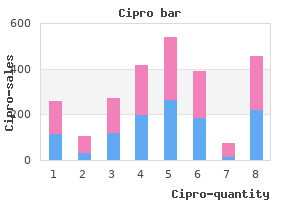
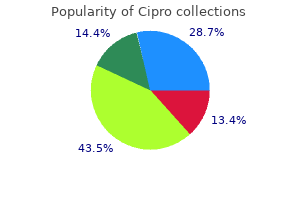
"Buy generic cipro 1000 mg on line, antibiotic nebulizer".
S. Curtis, M.A.S., M.D.
Associate Professor, Dartmouth College Geisel School of Medicine
This could be distinguished from vascular claudication antimicrobial spray cipro 500 mg order visa, as a outcome of the ache of neurogenic claudication begins even whereas the patient stands still antibiotics for sinus infection how long does it take to work 250 mg cipro purchase amex. The pain is worsened by extension of the backbone antibiotics for uti names buy discount cipro 750 mg, which happens with standing or strolling antibiotic resistance livestock cipro 500 mg order online, and improves with flexion, similar to sitting or leaning forward. In reality, many radiographic anomalies, such as spina bifida occulta, single-disk narrowing, spondylosis, aspect joint abnormalities, and several congenital anomalies, are equally common in symptomatic and asymptomatic people. Although adults are extra apt to have disk abnormalities, muscle strain, and degenerative changes associated with low back ache, athletically lively adolescents are more doubtless to have posterior factor derangements, such as stress fractures of the pars interarticularis. Early recognition of this spondylolysis and treatment by bracing and limitation of activity could prevent nonunion, persistent ache, and incapacity. Radiation of pain down one or both legs may occur, however often not under the knee or accompanied by optimistic straight-leg elevating or neurologic deficit. They may complain of generalized superficial tenderness if you flippantly pinch the pores and skin over the affected lumbar area. When straightleg raising is equivocally constructive after testing the patient in a supine place, use distraction and reexamine the patient in the sitting position to see if the preliminary findings are reproduced. The rotation take a look at can additionally be carried out, by which the patient stands together with his arms at his sides. Hold his wrists next to his hips and switch his body from facet to side, passively rotating his shoulders, trunk, and pelvis as a unit. This maneuver creates the phantasm that the spinal rotation is being examined, however, actually, the spinal axis has not been altered, and any complaint of back ache ought to be suspect. Malmivaara A, Hakkinen U, Aro T, et al: the therapy of acute low back pain: mattress relaxation, exercise, or odd exercise Miller P, Kendrick D, Bentley E, et al: Cost-effectiveness of lumbar spine radiography in main care patients with low again pain, Spine 27:2291�2297, 2002. A systematic evaluate of randomized controlled trials of the most common interventions, Spine 22:2128�2156, 1997. Rapid onset with fever and native warmth suggests the potential of septic arthritis. A prominent monarticular synovitis with comparatively little pain, however where the joint is warm with a large effusion, especially of the knee, is typical of Lyme illness. A historical past of similar assaults, especially of the primary metatarsophalangeal joint, suggests the risk of gouty arthritis. A history of recurrent knee swelling with minimal erythema and gradual onset after overuse or minor trauma is extra likely related to osteoarthritis and pseudogout. A youngster between the ages of three and 10 years who presents with a limp or lack of ability to stroll may have a transient synovitis of the hip or a extra critical septic arthritis. Remember that although a high-grade fever is very concerning, the elderly or immunocompromised affected person could fail to mount a fever in the face of infection. Examine the affected joint and doc the extent of effusion, involvement of adjacent structures, and degree of erythema, tenderness, heat, and limitation of range of movement. True intra-articular issues cause restriction of lively and passive range of motion, whereas periarticular problems. Intra-articular fluid accumulation can often be detected by urgent on one side of the affected joint and, at the similar time, palpating a wavelike fluctuance on the alternative facet of the joint. In the knee, when the medial or lateral compartment is stroked, the fluid strikes in to the other compartment, leading to a visible bulge. Blood cultures are constructive in about 50% of nongonococcal infections but are hardly ever constructive (about 10%) in gonococcal infection. Lyme antibodies may be applicable as Lyme illness is changing into increasingly more prevalent, even in the absence of recognized tick bites. Consider obtaining radiographs of the affected joint to detect possible unsuspected fractures or evidence of continual disease, corresponding to rheumatoid arthritis. The discovering of crystalinduced chondrocalcinosis might support but not verify the prognosis of pseudogout arthritis or osteoarthritis. Perform arthrocentesis to take away joint fluid for analysis, to relieve ache, and, within the case of septic or crystal-induced arthritis, to reduce the bacterial and crystal load throughout the joint. Identify the joint line to be entered, make a pressure mark on the overlying skin with the closed finish of a retractable pen to function a target. Then utilizing sterile method all through, cleanse the skin over probably the most superficial space of the joint effusion with alcohol and povidone-iodine (Betadine), anesthetize the pores and skin with 1% plain buffered lidocaine, and aspirate as much joint fluid as possible through a 16- to 18-gauge needle (smaller in small joints). Hold the needle parallel to the mattress surface, and direct it just posterior to the patella in to the subpatellar house. The finest site for needle entry of the wrist is on the dorsal radial side on the proximal finish of the anatomic snuff field and the distal articulation of the radius. For small joints, enter the midline on the dorsolateral side and advance a small needle in to the joint space. Joints of the digits could need to be distracted by pulling on the end to enlarge the joint house. Fluoroscopy may be useful in guiding needle placement for hip or shoulder joint aspiration. Clear, light-yellow fluid is attribute of osteoarthritis or delicate inflammatory or traumatic effusions. Grossly cloudy fluid is attribute of extra extreme inflammation or bacterial an infection. Blood within the joint is characteristic of trauma (a fracture or tear contained in the synovial capsule) or bleeding from hemophilia or anticoagulants. Wet the ideas of two gloved fingers with joint fluid, repeatedly touch them collectively, and slowly draw them apart. As this maneuver is repeated 10 or 20 occasions, and the joint fluid dries, regular synovial fluid will form longer and longer strings, normally to 5 to 10 cm in size. If microscopic examinations are delayed, a tube with ethylenediaminetetraacetic acid must be used for anticoagulation, as a result of anticoagulants. The most essential laboratory checks on joint fluid include a Gram stain and culture for potential septic arthritis. Gram-positive bacteria may be seen in 80% of culture-positive synovial fluid, but gram-negative bacteria are seen less often; gram-negative diplococci are seen rarely. A joint fluid total and differential leukocyte depend is the next most useful take a look at to order. Clinical judgment predominates in this range, with an emphasis on presumptive antibiotic therapy until a prognosis is established. Identification of crystals can set up a diagnosis of gout or pseudogout and keep away from unnecessary hospitalization for suspected infectious arthritis. If Gram stain shows gram-positive cocci in clusters, add vancomycin (Vancocin), 1. For kids older than 5 years of age, prescribe nafcillin (Unipen) or oxacillin (Prostaphlin), one hundred fifty to 200 mg/kg/day divided in to four to 6 doses, plus ceftriaxone (Rocephin), 50 mg/kg/day (maximum 2 g) divided bid. If an infection can be confidently excluded from the diagnosis, intra-articular injections of corticosteroids is normally a useful adjunctive or various therapy. Using the strategies described above, with a 3- to 5-ml syringe and a 11/4-inch 27-gauge needle, inject 1 to 2 mL of forty mg/mL methylprednisolone (Depo-Medrol) with 2 to eight mL of bupivacaine (Marcaine), zero. Alternatively, triamcinolone hexacetonide (Aristospan Intra-articular), 20 to forty mg/injection may be used. Warn patients of the 10% to 15% threat for postinjection flare or recurrent pain for twenty-four to 48 hours after the local anesthetic wears off. Children complaining of acute hip ache have to be evaluated for the potential for a septic arthritis versus a transient synovitis. Similar signs are present in these two diseases on the early levels, and differential diagnosis is difficult. Five reportedly independent predictors of septic arthritis are a temperature larger than 37� C (98. In a small examine, this was proven to shorten the length of signs of transient synovitis by 2 days. What Not To Do: Do not faucet a joint through an area of apparent contamination, corresponding to subcutaneous cellulitis. Do not send synovial fluid for chemistries, proteins, rheumatoid issue, or uric acid, as a end result of the results could also be deceptive. Do not be misled by bursitis, tenosynovitis, or myositis with out joint involvement. An infected or infected joint could have a reactive effusion, which can be evident as fullness, fluctuance, reduced vary of movement, or joint fluid that may be drawn off with a needle. Do not treat hyperuricemia with drugs that lower uric acid levels, such as allopurinol or probenecid, during an acute attack of gout (see Chapter 114). Relative contraindications embody renal insufficiency, quantity depletion, gastritis, inflammatory bowel illness, asthma, hypertension, and congestive heart disease.
The neck is angled medially on the shaft antibiotics for uti emedicine buy cipro 250 mg without a prescription, the open neck-shaft angle being about 130� virus envelope 750 mg cipro generic free shipping. It can also be normally angled forward (anteverted) from the coronal airplane by about 15� within the adult bacteria pseudomonas 250 mg cipro generic free shipping. These angles are important in the consideration of proximal femoral fractures and in the insertion of proximal femoral prostheses treatment for uti while breastfeeding buy cipro 250 mg amex. Their presence also determines the road of motion of muscle tissue acting about the hip. The head is more than half a sphere, and is completely coated with articular cartilage besides in the base of the central pit or fovea for the attachment of the ligament of the head of the femur (ligamentum teres). The neck is narrower proximally than distally, and is demarcated from the shaft by the intertrochanteric crest posteriorly and line anteriorly. Subcapital femoral fractures occur by way of the slim more proximal neck, and (per)trochanteric fractures move by way of the intertrochanteric area. The line of capsular attachment from the hip joint passes distal to the line of subcapital fractures however proximal to that of trochanteric fractures. A the top of the femur has been separated from the acetabulum to show the labrum and ligament of the pinnacle of the femur. The greater trochanter is especially an attachment for the abductors and brief rotators of the hip, however vastus lateralis encroaches upon it anteriorly. Gluteus medius attaches superiorly, gluteus minimus more anteriorly, and the brief rotator (obturators and piriformis) attachments are grouped across the trochanteric fossa medially. The progress plate for the pinnacle is entirely within the line of attachment of the hip capsule. Apart from a tiny medial portion of the greater, the trochanteric development plates are extracapsular. The arterial anastomosis from the circumflex femoral arteries, from which the blood supply to the head of the femur derives, lies near bone on the stage of the mid- and distal femoral neck. The posterior floor of the neck is separated only by the quick rotators from the sciatic nerve. The shaft of the femur is a very strong, anteriorly bowed tube of compact bone, expanding distally in to the metaphyseal supracondylar area. Its major feature is the posteriorly placed linea aspera, a raised and roughened muscle attachment. This line splits superiorly, persevering with laterally in to the raised space for the femoral attachment of gluteus maximus. It also splits inferiorly because the shaft expands, giving the two supracondylar strains and ridges which border the popliteal floor of the bone. The three named adductors of the femur attach to the linea aspera, along with the quick head of biceps femoris, the vasti and the intermuscular septa. Vastus intermedius also attaches to the proximal two-thirds of the anterior facet of the shaft. The shaft of the femur is attached to the stockinglike fascia lata by the medial and lateral intermuscular septa, dividing the thigh in to anterior extensor and posterior flexor osteofascial compartments. The septa connect along the entire of the linea aspera and its distal prolongations. The perforating arteries, branches of the profunda femoris, pass very near the shaft as they run from the extensor in to the flexor compartment. The distal expanded finish of the femur consists of the metaphysis and popliteal floor and the 2 condyles. The adductor tubercle, the distal attachment of adductor magnus, lies simply proximal to the medial epicondyle. The femoral vessels turn into the popliteal as they move through a hiatus in the lower part of this attachment, and are thereafter intently associated to the popliteal surface of the femur, the artery mendacity on the bone and consequently being very liable to injury in supracondylar fractures of the femur. The horseshoe-shaped articular floor for the tibia is prolonged anteriorly in to that for the patella, which extends additional forward laterally than medially. Between the condyles is the intercondylar notch, whose floor is intracapsular but extrasynovial. The lateral wall of the notch is a part of the lateral condyle and provides attachment to the anterior cruciate ligament, whereas its medial wall, from the medial condyle, bears the attachment of the posterior cruciate. The development plate of the distal femur runs almost horizontally at the degree of the adductor tubercle, and is extracapsular except for a small central phase anteriorly. Muscular markings Quadriceps Femoris Facet for lateral femoral condyle Facet for medial femoral condyle Apex A B. From its decrease pole the patellar tendon (ligamentum patellae) runs to the tibial tubercle, and the bulk of the quadriceps tendon inserts in to its upper (proximal) floor. The quadriceps expansions, aponeurotic attachments from the vasti, be part of its medial and lateral borders. Its anterior, nonarticular floor is subcutaneous, with the prepatellar bursa intervening. Its posterior floor articulates with the femur, and is divided by a longitudinal ridge in to a smaller medial and a larger lateral side for the respective femoral condyles. Viewed from behind, the patella lies in a circumferential cushion or pad of fat, which articulates in extension with a similar pad on the anterior floor of the femoral metaphysis. Its superior surface or plateau articulates with the femur and menisci: the fibula articulates with the inferior floor of the lateral condyle. The medial condyle has a posterior transverse groove for the attachment of semimembranosus, and the smaller, more round, lateral condyle has a flattened space anterolaterally for the attachment of the iliotibial tract of fascia lata. Anteriorly within the midline is the outstanding tibial tubercle, to which attaches the patellar tendon (ligament). In the intercondylar region the central eminence divides the anterior from the posterior non-articular areas. The anterior cruciate ligament attaches to the centre of the anterior area, with the anterior meniscal attachments anteromedially and posterolaterally. The posterior cruciate attaches to the posterior lip of the posterior non-articular space, with both the meniscal attachments anterior to it. The capsule of the knee joint attaches at the margins of the articular surface besides anteriorly, where it extends almost all the method down to the tibial tubercle. The proximal growth plate of the tibia lies totally outdoors the capsule, and has an anterodistal projection to include the tibial tubercle. On the medial aspect of the proximal metaphysis lie the attachments for the superficial part of the medial collateral ligament and for the pes anserinus, the flattened frequent tendon of sartorius, gracilis and semitendinosus. Popliteus attaches to the posterior metaphyseal surface above the oblique linear attachment of soleus, lying between the popliteal artery and the bone. The anterior border and medial surface are subcutaneous all through their length, making the tibia notably liable to open fracture. The lateral surface, lateral to the anterior border, is covered proximally by the attachment of tibialis anterior. Posteriorly, distal to the linear soleal attachment, tibialis posterior attaches laterally and flexor digitorum longus medially. The distal third of the shaft is devoid of muscle attachments, the ensuing reduced vascularity adversely affecting fracture healing on this space. The distal expanded finish continues distally and medially in to the medial malleolus, grooved posteriorly by the tendon of tibialis posterior. On the lateral floor at the similar stage lies the notch for articulation with the fibula. The inferior surface bears the articular floor for the talus, and is wider anteriorly than posteriorly. The capsule of the ankle joint attaches around the margins of the articular surface: the distal growth plate of the tibia, like the proximal, is totally extracapsular. Biceps femoris attaches to the top around the base of the styloid process, and the frequent peroneal nerve is vulnerable the place it crosses the neck of the bone just below the top. The attachments of the muscles to the upper shaft extend proximally on to the top anteriorly and posteriorly. The progress plate for the pinnacle lies totally exterior the capsules of the knee and superior tibiofibular joints. The distal expanded finish varieties the lateral malleolus, the talar articular surface lying medially. Proximal to this surface lies the realm of attachment for the interosseous ligament.
Cipro 500 mg buy low price. Reversing the Crisis of Antibiotic Resistance.
Human infection rash 750 mg cipro effective, cat virus children discount cipro 1000 mg amex, pig virus 52 cipro 250 mg purchase with amex, wild carnivore antibiotic resistance lab high school cipro 500 mg discount fast delivery, and monkey bites which are apart from abrasions and superficial split-thickness lacerations additionally require prophylactic antibiotics. When a prophylactic antibiotic is indicated, prescribe amoxicillin/clavulanic acid (Augmentin), 875/125 mg � 5 days for adults. For youngsters, 45 mg amoxicillin/kg/day, divided bid (80 to ninety mg/kg/day if drug-resistant S. Before antibiotics are began, get hold of cardio and anaerobic cultures from deep inside the wound and then irrigate and d�bride as described. Other indications for admission or specialty consultation after a bite harm embody harm or probable injury to deep structures (bones, joints, tendons, arteries, or nerves). This would include persons who have been in the identical room because the bat and who could be unaware that a bite or direct contact had occurred. If a biting animal with regular conduct has been captured, it ought to be quarantined with a veterinarian or reliable proprietor for 10 days. For hand accidents or crushing injuries and contusions, apply an immobilizing splint with a light compressive dressing and have the patient hold the extremity elevated above the extent of the heart. After 24 hours, the affected person ought to begin cleansing the wound once daily with mild cleaning soap and water, adopted by reapplication of a model new dressing. Hand injuries should remain immobilized for two to 3 days until edema and pain have largely resolved. Explain the potential for a serious complication, such as septic arthritis, osteomyelitis, and tenosynovitis, which will require specialty session. Preparing sufferers for the worst whereas initiating aggressive treatment is the best defense against any potential future litigation. Do not use buried absorbable sutures, which act as a international body and a nidus for infection. Do not attempt to treat chunk wounds using monotherapy with penicillin, clarithromycin, amoxicillin, or a first-generation cephalosporin. Do not present rabies prophylaxis for incidental contact, corresponding to petting a rabid animal or contact with blood, urine, or feces. Discussion Animal bites are sometimes introduced promptly to the eye of medical personnel, if solely due to a legal requirement to report the bite or because of fear of rabies. Bite wounds account for 1% of all emergency department visits in the United States, most brought on by canine and cats. Although these wounds may look innocuous initially, they regularly lead to severe infection with a possible for severe issues. A single chew may comprise varied kinds of harm, including abrasions, contusions, avulsions, lacerations, crush accidents, or puncture wounds. Less readily apparent are injuries to deeper tissues (including vascular buildings, tendons, nerves, and bone), in addition to potential overseas our bodies. Both dog and cat bites show high rates of an infection with Staphylococcus and Streptococcus species, in addition to Pasteurella multocida and many various gramnegative and anaerobic micro organism. In addition to these organisms, 10% to 30% of all human bites are infected with Eikenella corrodens, which typically reveals resistance to the semisynthetic penicillins but sensitivity to penicillin. A variety of threat components that determine the probability of wound infection and outline the affected person likely to develop this complication have been recognized. Facial wounds show an an infection fee of solely 4%, no matter remedy, whereas hand wounds have an an infection fee of 28%. Human bites typically are more extreme than animal bites, notably in clenched-fist accidents. The enamel might trigger a deep laceration that implants oral organisms in to the joint capsules or dorsal tendons, causing devastating problems that include cellulitis, septic arthritis, tenosynovitis, and osteomyelitis. Approximately 2% to 5% of all typical dog bite wounds seen in emergency departments turn into contaminated. Wounds that have absolutely penetrated the pores and skin have an infection fee of 6% to 13%, depending on location. In comparison, the infection price of unpolluted lacerations of every kind repaired in the emergency division is approximately 3% to 5%. The incubation interval for people is dependent upon the distance from the chunk to the brain, with a median of 1 to three months. Given this relatively long incubation interval, postexposure prophylaxis for rabies is considered a medical urgency, not a medical emergency. For questions on local rabies threat, local public health companies may be out there and supply valuable support. Since 1980, a complete of 21 (50%) of the 36 human circumstances of rabies recognized in the United States have been associated with bat variants. In the continental United States, rabies amongst dogs is reported mostly along the United States�Mexico border and sporadically in areas with enzootic wildlife rabies. During many of the Nineties, extra cats than canines have been reported to be rabid in the United States. Most of these cases have been associated with the epizootic of rabies amongst raccoons in the japanese United States. During work hours, cellphone (404) 639-1050; after hours and on weekends and holidays, call (770) 488-7100. In most different countries-including most of Asia, Africa, and Latin America-dogs remain the major species with rabies and the most common source of rabies among humans. In addition to being extremely prone to severe an infection, they might trigger an inoculum of the herpes B virus and require antiviral remedy with acyclovir, valacyclovir, or famciclovir. Brook I: Microbiology and management of human and animal bite wound infections, Prim Care 30:25�39, 2003. Freer L: North American wild mammalian accidents, Emerg Med Clin N Am 22:445�473, 2004. Marine animal envenomations may be divided in to two main classes: puncture wounds and focal rashes. Severe envenomations can be accompanied by systemic symptoms, corresponding to vomiting, paralysis, seizures, respiratory distress, and hypotension. There is instant local intense ache, edema of sentimental tissue, and a variable quantity of bleeding. The ache is excruciating and appears out of proportion to what might be anticipated based on the wound look alone. The pain often peaks after 60 to 90 minutes, may radiate centrally, typically resolves over a number of hours, and may final so lengthy as forty eight hours. Untreated, the pain peaks 60 to 90 minutes after the sting, persists for a minimal of 6 to 12 hours, and generally lasts for days. The severity of envenomations appears to be mild for lionfish, more extreme for scorpion fish, and most extreme and even life-threatening for stonefish, which is one other member of the Scorpaenidae. The dorsal or pectoral fin spines of the catfish can usually inflict an envenomation when puncturing the pores and skin. Symptoms include intense ache, paresthesias, and numbness which will last 30 minutes to 48 hours. Erythema, hemorrhage, edema, cyanosis, and lymphangitis also are common localized findings. Multiple small punctures in an erratic sample, with or without purple discoloration, or retained fragments are typical of sea urchin envenomations. Some spines include a blue-black dye that stains the wound or causes temporary tattooing. Contact with feather hydroids and sea anemones induces a light reaction, consisting of instantaneous burning, itching, and urticaria. Envenomation may end in a lesion with a pale center and an erythematous or petechial ring; this is adopted by rising edema and ecchymosis. Although most lesions resolve in forty eight hours, more extreme envenomations might result in vesicle formation, which may result in an abscess, eschar, or hyperpigmentation. The sting of the fire coral induces intense burning pain, redness, itching, and painful pruritus with large wheals, with central radiation and reactive regional lymphadenopathy. Fire coral (not a real coral) has a razor-sharp lime carbonate exoskeleton that may trigger skin lacerations containing exoskeleton debris. Envenomation from a jellyfish causes quick ache that may be described as delicate to average stinging or burning. What To Do: Puncture Wounds To most successfully relieve pain and attenuate some of the thermolabile protein parts of the venom, soak the wound in sizzling (not scalding) water (approximately 45� C [113� F]) for 30 to ninety minutes or longer for pain management. Have the affected person use an unaffected limb as a management to take a look at the water temperature and thereby avoid scalding. During scorching water remedy or while waiting for it to be out there, infiltrate in or around the wound with zero.
The lateral wall is also skinny and separates the sinus form the cavernous sinus and the interior carotid artery virus your computer has been blocked department of justice generic cipro 500 mg on-line. It capabilities to stop the lung and pleura rising additional in to the neck throughout respiration antibiotic neurotoxicity order cipro 250 mg free shipping. The subclavian artery and vein and the brachial plexus lie on the suprapleural membrane antibiotic for uti proteus order 500 mg cipro amex. Subclavian artery the proper subclavian artery is a department of the brachiocephalic trunk and the left arises directly from the arch of the aorta beyond the origin of the left inside Left recurrent laryngeal nerve Phrenic nerve Scalenus medius Stellate ganglion of sympathetic trunk Oesophagus Thoracic duct Trachea Carotid sheath Common carotid artery Scalenus anterior Brachial plexus Upper trunk Middle trunk Lower trunk Subclavian artery Vagus nerve Subclavian vein Internal jugular vein virus neutralization assay buy cheap cipro 500 mg on-line. The carotid sheath and contents are reduce and reflected to present the deep constructions within the neck. The subclavian vein runs parallel to the artery but in entrance of the scalenus anterior at a slightly decrease stage. The roots and the trunks of the brachial plexus lie behind the subclavian artery on the first rib between the scalenus anterior and the scalenus medius muscle tissue. The branches of the subclavian artery are as follows: Subclavian venepuncture can be carried out using an infraclavicular or supraclavicular strategy. In the former the needle is inserted beneath the clavicle at the junction of its center and medial thirds and superior upwards and medially behind the clavicle in direction of the sternoclavicular joint. In the supraclavicular strategy the needle is inserted about 2 cms above the clavicle on the junction between its center and medial thirds on the lateral border of the sternocleidomastoid. The needle is superior downwards and medially towards the sternoclavicular joint and aspirated for the free move of blood from the vein. There is the risk of pneumothorax and an inadvertent puncture of the subclavian artery in both of these approaches. A variety of approaches are described to block the brachial plexus within the supraclavicular area. In the supraclavicular perivascular technique the needle is inserted on the middle of the clavicle just lateral to the subclavian artery pulsation and directed backwards downwards and inwards. In the interscalene method the needle is inserted at the next degree on the stage of the cricoid cartilage and advanced in path of the transverse means of the sixth cervical vertebra and the native anaesthetic is injected deep to the prevertebral fascia (the aircraft containing the nerves). Phrenic nerve paralysis and/or inadvertent injection in to the vertebral artery are issues. It enters the foramen transversarium on the sixth cervical vertebra and ascends by way of the foramina transversaria of the sixth to the primary cervical vertebrae and enters the cranial cavity and branches to supply the brain and spinal twine. The inside thoracic (mammary) artery passes vertically downwards a fingers breadth lateral to the sternum. In the sixth intercostal space it divides in to the musculophrenic artery and the superior epigastric artery. The thyrocervical trunk is a branch of the subclavian artery medial to the scalenus anterior. It divides in to the inferior thyroid artery, the transverse cervical and the suprascapular arteries. The inferior thyroid artery lies behind the carotid sheath and ascends in front of the scalenus anterior. At the extent of the transverse strategy of the sixth cervical vertebra the artery arches medially and enters the postero-medial facet of the capsule of the thyroid gland at its decrease third. The recurrent laryngeal nerve is closely related to the artery and its branches close to the decrease pole of the thyroid gland. Thoracic duct this duct carries lymph from the whole body besides that from right facet of thorax, proper upper limb, and right facet of head and neck. It arises in the abdomen, passes via the thorax and enters the neck mendacity on the left facet of the oesophagus. At the basis of the neck it arches laterally lying between the carotid sheath and the vertebral artery. Inadvertent puncture or laceration of the thoracic duct will cause escape of lymph in to the surrounding tissue and occasionally chylothorax. Subclavian vein the subclavian vein follows the course of the subclavian artery in the neck, but lies in entrance of the scalenus anterior on the primary rib. Veins accompanying the branches of the subclavian artery drain in to the external jugular, the subclavian vein or its continuation, the brachiocephalic vein (formed by the union of the subclavian and the inner jugular veins). The superior ganglion lies on the degree of C2 & C3, the center on the level of C6, and the inferior ganglion on the neck of the first rib behind the vertebral artery. Often the inferior ganglion is fused with the first thoracic ganglion to kind the stellate ganglion. Grey rami from this attain the upper limb through the roots of the brachial plexus largely via C7 and C8. The preganglionic input to the cervical ganglia (including the stellate) are from the higher thoracic white rami. The thoracic a part of the sympathetic chain can be seen lying on the heads of the upper ribs through a thoracoscope after deflating the lung. Resection of T2�T4 section is carried out to produce a dry hand in patients suffering from hyperhidrosis. Afferents to these nodes are from the superficial tissues of the areas corresponding to those drained by the veins alongside which they lie. Deep lymph nodes of the top and neck Most of the deep lymph nodes are organized roughly in a vertical chain alongside the inner jugular vein and a round chain. Vertical chain crucial of this group is the deep cervical nodes which is the terminal group for all lymphatics in the head and neck. All tissues in the head and neck drain in to middleman groups after which in to the deep cervical nodes. The deep cervical nodes lie covered by the fascia of the carotid sheath, closely related to the interior jugular vein. They are subdivided into: Cervical rib it is a situation during which an additional rib or a part of a rib may develop as a prolongation of its transverse process. It could be bony, fibrous, or partly fibrous and partly bony; and if full will lengthen as much as the tubercle of the primary rib. The parts of the brachial plexus which normally lie on the first rib get displaced upwards by the extra rib leading to compression of the lower trunk (C8 T1). The superior group lies in the region where the posterior belly of the digastric crosses the internal jugular vein and therefore, nodes listed beneath are also recognized as the jugulodigastric nodes. They drain the tonsil and the tongue and the efferents go to the lower deep cervical nodes and/or to the jugular trunk. The decrease group lies where the omohyoid crosses the interior jugular vein and therefore are referred to as the juguloomohyoid group. A few nodes in the deep cervical group prolong in to the posterior triangle and lie along the course of the accessory nerve. There are additionally few nodes within the root of the neck � the supraclavicular nodes which enlarge in late levels of malignancies of thorax and stomach. Submental nodes the afferents to this group come from the tip of the tongue, the ground of the mouth and the central part of the lower lip. Submandibular nodes these nodes lie contained in the capsule of the submandibular salivary gland. Afferents are obtained from the facet of the nose, higher lip, lateral part of the lower lip, cheek, gums, and the anterior two-thirds of the margin of the tongue. Buccal or facial nodes these lie on the buccinator alongside the facial vein and drain the eyelid, conjunctiva, nose and cheek. Parotid nodes There are few nodes in this group, some mendacity superficial and others deep to the parotid capsule. The superficial nodes drain the eyelids, entrance of the scalp, external ear, and the middle ear. The preauricular node is superficial and drains the pinna of the ear and the side of the scalp. Posterior auricular nodes or the mastoid nodes A few nodes mendacity on the mastoid course of drain the again of the scalp, back of the auricle and the exterior auditory meatus. Occipital nodes Situated on the upper attachment of the trapezius, they drain the again of the scalp. Besides these mentioned above, there are lymph nodes closely associated to the pharynx, trachea, and the larynx.