Clomipramine
| Contato
Página Inicial

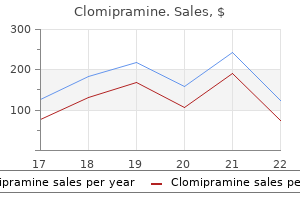
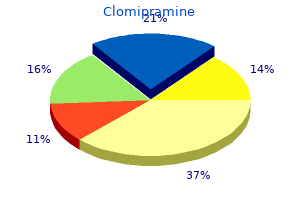
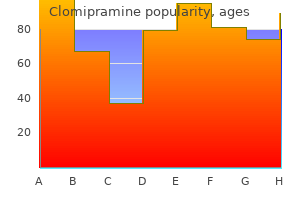
"Generic 25 mg clomipramine with mastercard, bipolar depression or major depression".
A. Hatlod, M.A., M.D., M.P.H.
Co-Director, Minnesota College of Osteopathic Medicine
K-wires across the distal radius could be removed in the clinic setting 4�6 weeks after insertion depression gastric symptoms clomipramine 10 mg trusted. Complications of K-wires embrace pin site infection mood disorder nos 2969 clomipramine 75 mg for sale, wire breakage mood disorder vs anxiety disorder clomipramine 10 mg discount on line, loss of fixation and wire migration prenatal depression symptoms uk cheap clomipramine 10 mg line. Hybrid variations are infinite, with combinations of anchor fixation modalities and frame constructs. The main drawback of exterior fixation is that they are often cumbersome to the patient and pin website infection could be a drawback (Table 28. In basic, plates and screws are used the place attainable in articular and periarticular fractures where an anatomical reduction is required, often by way of open means, adopted by the appliance of the plate and screws to obtain a inflexible assemble. In extra-articular fractures, the place mechanical alignment is required along with relative stability, one possibility is the utilization of locking plate know-how. This permits a closed reduction and percutaneous placement of the plate with locking screws to create an inside construct, which behaves like an external fixator. Injury-specific plating techniques have revolutionised the flexibility to treat sure accidents, with plates pre-bent and pre-shaped for particular anatomical regions and specific damage patterns. Advantages No interference with fracture site Adjustable after utility: alignment; biomechanics Soft tissues accessible for cosmetic surgery Rapid stabilisation of fracture Hardware simple to take away Disadvantages Pin web site infection Interferes with plastic surgical procedures Soft-tissue tethering Cumbersome for the affected person Intramedullary nails Diaphyseal fractures are finest suited to intramedullary nailing. Where mechanical alignment is required along with relative stability, they permit for oblique bone healing. After nail insertion, mechanical alignment is checked significantly for length, alignment and rotation. Locking screws are then positioned proximally and distally to preserve length and alignment. However, with improved implant Martin Kirschner, 1879�1942, Professor of Surgery, Heidelberg, Germany, introduced the utilization of skeletal traction wires in 1909. Gavriil Abramovich Ilizarov, 1921�1993, orthopaedic surgeon, Kurgan, Western Siberia, Russia. More design and the flexibility to lock the nails very distally and in a quantity of directions, the indications for intramedullary nailing is expanding. Reaming is the process whereby the intramedullary canal is widened barely to permit passage of a larger diameter nail, regarding the final reamer dimension used. Implant longevity and degree of activities following implant insertion need to be matched. Traditionally, arthroplasty for trauma was restricted to hip and shoulder hemiarthroplasty. Total hip replacement, acute distal femoral replacement, radial head alternative, total and hemi-elbow arthroplasty, and reverse polarity shoulder arthroplasty are current remedy choices for older patients with osteoporotic periarticular fractures. The choice of a selected approach will depend on clinical evidence and our beforehand acknowledged goal to return sufferers to optimal perform as soon as potential. It ought to be considered within the context that it can be costly and require considerable other resources to make the process protected and long lasting. The major indication is that operation will produce a better outcome; the rules are given beneath. Well known factors that slow down bone therapeutic embody diabetes mellitus (doubles time to union), diminished blood supply (peripheral vascular disease, vascular injury at time of injury), smoking, non-steroidal anti-inflammatory drugs and an infection on the fracture site. Several chemical and mechanical methods have been tried to improve fracture therapeutic, including bone marrow injections into the fracture website and other orthobiologics similar to bone morphogenic proteins. Mechanical methods embody managed axial micromotion (using an external fixator), electromagnetic stimulation and low intensity pulsed ultrasound. Angular malunion of a diaphyseal fracture of the weight-bearing long bones will lead to irregular joint forces on the joint above and below, leading to ache and secondary degenerative joint disease. Diaphyseal fractures are typically properly suited to intramedullary fixation techniques, as beforehand discussed. It is commonly not essential to wait until bone union before beginning rehabilitation. It is important to transfer the affected joints and the joints in close proximity to the fracture. Fixation of metaphyseal fractures is less predictable with intramedullary nailing, subsequently plate and screw fixation, external fixation or, in the smaller joints, K-wire fixation is used. Metaphyseal fractures are close to the joint and so consideration is given to secure fixation to permit early joint movement and rehabilitation. Each was a high-energy harm; (b) and (e) present a temporary spanning exterior fixator utilized in each case; (c) and (f) show definitive relative stability was achieved with different strategies of bridging fixation. Despite irregularities on the fracture websites the overall position was passable and performance was good. However, these ideas should be balanced with the elevated wound problems of open surgical procedure and devitalising bone fragments with excessive exposure of the bone. Although anatomical discount may be achieved, inflexible fixation units could cut out of soft bone. As such, a displaced waist of scaphoid fracture interrupts the blood provide to the proximal pole, leading to avascular necrosis. The normal protocol of a suspected scaphoid fracture is to immobilise the wrist and examine once more 10�14 days later. In displaced or unstable fractures (>1 mm) consideration should be given to open reduction and rigid fixation with a headless compression screw. Complications of scaphoid fractures include: non-union, avascular necrosis, malunion and carpal instability. A lunate dislocation is where the lunate bone dislocates out of the radiocarpal joint. In a perilunate dislocation the lunate remains in the radiocarpal joint and the relaxation of the carpus dislocates across the lunate. Anatomical carpal alignment is troublesome to maintain and therefore surgical reconstruction of damaged intrinsic ligaments, along with K-wire fixation of the carpal bones, is often undertaken. K-wires are saved in place for eight weeks and the wrist casted or splinted for 3 months. Due to the distinctive anatomical association of adductor policis, if the ligament undergoes full rupture the aponeurosis may become interposed, inhibiting ligament to bone healing. Complete ruptures with a Stener lesion (interposed aponeurosis) require open reduction of the ligament to restore bone contact, with a suture anchor restore of the associated ulnar collateral ligament. However, some will slip or collapse with forged treatment, and so shut evaluate for the first few weeks is advocated. Fractures with significant initial displacement and dorsal comminution are vulnerable to early and late collapse. After thorough counselling the patient could select to have the fracture reduced and then held surgically with K-wires, plate and screw fixation (volar or dorsal) or exterior fixation. The K-wires could also be placed throughout the fracture fragments or intrafocally, going by way of the fracture web site. Intra-articular fractures (types B and C) of the distal radius require anatomical discount of the joint floor; a gap or step of less than 2 mm could be accepted within the radius. If a closed reduction could be achieved with manipulation, the fracture fragments can subsequently be held with K-wires, plate and screw fixation or external fixation. The most common form of therapy is closed discount and percutaneous K-wire fixation, supplemented with a plaster forged for 4�6 weeks. Forearm fractures (radius and ulna) Fractures of the diaphyseal shaft of the radius and ulna are technically, in the anatomic sense of the word, extraarticular. However, the forearm bones work collectively, being coupled at the proximal and distal radioulnar joints to enable Robert William Smith, 1807�1873, Professor of Surgery, Trinity College, Dublin, Ireland, described the reverse Colles fracture in 1847. Abraham Colles, 1773�1843, President of the Royal College of Surgeons of Ireland (1802), Professor of Anatomy Physiology and Surgery (1804) and described distal radial fracture in 1814. Non-operative treatment with useful bracing will obtain union in an appropriate position inside 12 weeks in over 80% of circumstances. Gravity can provide traction on the arm and at the facet of a humeral brace help to maintain alignment and permit early vary of movement of the elbow. Active shoulder abduction is avoided till fracture union, to forestall varus deformity. Shoulder movement should not be absent throughout remedy and so gravity assisted pendulum workouts are instituted early on to forestall shoulder stiffness. As the fracture approaches the metaphyseal area of the humerus it turns into tougher to management with humeral bracing.
The carbohydrate load in the small bowel causes a rise within the plasma glucose unipolar depression definition 50 mg clomipramine discount visa, which mood disorder quest cheap clomipramine 50 mg visa, in flip depression help groups order clomipramine 75 mg without a prescription, causes insulin ranges to rise mood disorder 29690 symptoms clomipramine 50 mg generic with visa, inflicting a secondary hypoglycaemia. This can be simply demonstrated by serial measurements of blood glucose in a patient following a take a look at meal. Post-vagotomy diarrhoea this can be essentially the most devastating symptom to afflict patients having peptic ulcer surgical procedure. Most patients will suffer some looseness of bowel motion to a point (with the exception of extremely selective vagotomy) however, in about 5%, it might be intractable. Following truncal vagotomy, the biliary tree, as well as the stomach, is denervated, resulting in stasis and hence stone formation. However, this will induce or worsen different postpeptic ulcer surgical procedure syndromes similar to bilious vomiting and postvagotomy diarrhoea. The problems of peptic ulceration the widespread issues of peptic ulcer are perforation, bleeding and stenosis. However, there was a considerable change within the epidemiology of perforated peptic ulcer in resource-rich countries during the last 20 years. With time there was a gentle increase in the age of the patients suffering this complication and an increase in the numbers of females, such that perforations now happen most commonly in elderly female patients. The patient, who may have a historical past of peptic ulceration, develops sudden-onset extreme generalised abdominal pain due to the irritant effect of gastric acid on the peritoneum. The abdomen displays a board-like rigidity and the affected person is disinclined to transfer due to the ache. Patients with this type of presentation want an operation, without which the patient will deteriorate with a septic peritonitis. This classical presentation of the perforated peptic ulcer is observed less generally than up to now. The board-like rigidity seen within the stomach of younger sufferers may also not be observed and a better index of suspicion is important to make the right analysis. They could current only with ache in the epigastrium and proper iliac fossa because the fluid may track down the best paracolic gutter. Sometimes perforations will seal owing to the inflammatory response and adhesion within the stomach cavity, and so the perforation may be selflimiting. All of those elements could mix to make the diagnosis of perforated peptic ulcer tough. By far the commonest website of perforation is the anterior facet of the duodenum. However, the anterior or incisural gastric ulcer could perforate and, as properly as, gastric ulcers could perforate into the lesser sac, which can be notably tough to diagnose. All sufferers ought to have serum amylase carried out, as distinguishing between peptic ulcer, perforation and pancreatitis can be difficult. In the case of a classically presenting perforated ulcer, the abdominal motion is restricted or absent. Laparotomy is performed, often via an upper midline incision if the diagnosis of perforated peptic ulcer can be made with confidence. The most essential component of the operation is a thorough peritoneal rest room to take away all the fluid and meals particles. If the perforation is in the duodenum it may possibly normally be closed by a number of well-placed sutures, closing the ulcer in a transverse path as with a pyloroplasty. It is widespread to place an omental patch over the perforation within the hope of enhancing the possibilities of the leak sealing. Gastric ulcers ought to, if possible, be excised and closed, in order that malignancy may be excluded. Occasionally a affected person is seen who has a massive duodenal or gastric perforation such that simple closure is impossible; in these patients a distal gastrectomy with Roux-en-Y reconstruction is the process of selection. All sufferers should be handled with systemic antibiotics along with a radical peritoneal lavage. In the past, many surgeons performed definitive procedures similar to both truncal vagotomy and pyloroplasty or, more lately and possibly more successfully, extremely selective vagotomy in the course of the course of an operation for a perforation. Studies present that in well-selected sufferers and in expert palms this is a very protected strategy. However, these days, surgical procedure is confined to first-aid measures mostly, and the peptic ulcer is treated medically as described earlier on this chapter. Perforated peptic ulcers can usually be managed by minimally invasive techniques if the experience is available. A nice deal has been written in regards to the conservative management of perforated ulcer. A number of factors have been associated with poor outcome after perforated peptic ulcer, together with: delay in prognosis (>24 hours); medical comorbidities; shock; increasing age (>75). There is little evidence to advocate the conservative management of sufferers who exhibit any of these traits. Despite improvements in analysis and the proliferation in therapy modalities over the previous few decades, an in-hospital mortality of 5�10% can be anticipated. In sufferers in whom the trigger of bleeding could be found, the most typical causes are peptic ulcer, erosions, Mallory�Weiss tear and bleeding oesophageal varices (Table 63. First, the affected person ought to be adequately resuscitated and, following this, the patient ought to be investigated urgently to determine the trigger of the bleeding. For any important gastrointestinal bleed, intravenous entry should be established and, for those with extreme bleeding, central venous pressure monitoring should be arrange and bladder catheterisation carried out. Blood should be cross-matched and the patient transfused as clinically indicated, usually when >30% of blood quantity has been misplaced. In these circumstances, resuscitation, prognosis and treatment ought to be carried out simultaneously. Condition Ulcers Oesophageal Gastric Duodenal Erosions Oesophageal Gastric Duodenal Mallory�Weiss tear Oesophageal varices Tumour Vascular lesions. All sufferers are generally started on either an H2-antagonist or a proton pump antagonist, and up to date evidence confirms the benefit of proton pump inhibitor administration to forestall rebleeding after endoscopy. Furthermore, meta-analysis of studies means that tranexamic acid, an inhibitor of fibrinolysis, may reduce general mortality. Therapeutic endoscopy can achieve haemostasis in roughly 70% of instances, with one of the best evidence supporting a mix of adrenaline injection with heater probe and/or clips. The threat of significant ischaemia following embolisation is low because of the wealthy collateral blood provide of the abdomen and duodenum. The surgeon ought to be mindful that rescue surgery after failed embolisation is related to poor outcome and it may be advantageous to proceed directly to surgery. For occasion, in patients with known oesophageal varices and uncontrollable bleeding, a Sengstaken�Blakemore tube may be inserted before an endoscopy has been carried out. The most important current causes of this are liver disease and inadequately managed warfarin remedy. In these circumstances the coagulopathy ought to be corrected, if possible, with fresh-frozen plasma or concentrated clotting elements. Upper gastrointestinal endoscopy ought to be carried out by an experienced operator as soon as practicable after the affected person has been stabilised. In patients in whom the bleeding is relatively delicate, endoscopy could also be carried out on the morning after admission; this is normally guided by native coverage. A number of scoring methods have been advocated for the assessment of rebleeding and death after upper gastrointestinal haemorrhage. This can be utilized in a pre-endoscopy format to stratify sufferers to secure early discharge and postendoscopy it could possibly comparatively accurately predict rebleeding and dying. The solely exception applies in expert centres with 24-hour interventional radiology and experience of angiographic embolisation the place makes an attempt may be made to arrest bleeding and keep away from surgical procedure. Patients with a visual vessel in the ulcer base, a spurting vessel or an ulcer with a clot within the base are statistically likely to require surgical remedy to stop the bleeding. Elderly and unfit patients usually have a tendency to die because of bleeding than youthful sufferers. A patient who has required greater than six units of blood generally wants surgical remedy. The introduction of endoscopy has greatly helped within the management of upper gastrointestinal bleeding as a surgeon can usually be confident about the site of bleeding prior to operation.
Early elective intubation is safest Delay could make intubation very difficult because of swelling Be able to anxiety over health clomipramine 10 mg line perform an emergency cricothyroidotomy depression definition in urdu clomipramine 10 mg cheap free shipping, if intubation is delayed the potential of damage further to the burn have to be sought each clinically and from the history bipolar mood disorder icd 9 clomipramine 25 mg otc, and handled appropriately depression hormone test 75 mg clomipramine purchase with mastercard. Not all burned patients will need to be admitted to a burns unit, but the principle standards are given in Table 41. The key within the management of airway burn is the historical past and early indicators, somewhat than the symptoms. Clues on examination embrace blisters on the hard palate, burned nasal mucosa and loss of all of the hair within the nostril (the anterior hairs are sometimes burned), but maybe the most valuable indicators are the presence of deep burns across the mouth and in the neck. It also takes into consideration completely different proportional body floor space in youngsters in accordance with age. A historical past of being trapped within the presence of smoke or hot gases Burns on the palate or nasal mucosa, or loss of all of the hairs in the nose Deep burns around the mouth and neck Breathing Inhalational damage Time is also an element; anyone trapped in a hearth for greater than a couple of minutes must be observed for signs of smoke inhalation. Other signs that raise suspicion are the presence of soot within the nose and the oropharynx and a chest radiograph displaying patchy consolidation. The clinical features are a progressive enhance in respiratory effort and price, rising pulse, anxiousness and confusion and lowering oxygen saturation. These symptoms will not be obvious instantly and might take 24 hours to 5 days to develop. If the situation deteriorates, steady or intermittent optimistic pressure may be used with a masks or T-piece. In the severest circumstances, intubation and administration in an intensive care unit might be wanted. The key, due to this fact, within the administration of inhalational injury is to suspect it from the historical past, institute early administration and observe carefully for deterioration. Carboxyhaemoglobin levels raised above 10% must be handled with high impressed oxygen for twenty-four hours to velocity its displacement from haemoglobin. There may also be carbon dioxide retention and high inspiratory pressures if the affected person is ventilated. The remedy is to make some scoring cuts through the burned pores and skin to permit the chest to increase (escharotomy). Taking an instance of sizzling water at 65�C: publicity for forty five s will produce a full-thickness burn, for 15 s a deep partial-thickness burn and for 7 s a superficial partial-thickness burn. Cause of burn Scald Probable depth of burn Superficial, however with deep dermal patches within the absence of excellent first aid. Will be deep in a younger toddler Deep dermal Mixed deep dermal and full thickness Often deep dermal or full thickness Weak concentrations superficial; sturdy concentrations deep dermal Full thickness (c) Fat burns Flame burns Alkali burns, including cement Acid burns Electrical contact burn Summary field 41. Superficial partial-thickness burns the harm in these burns goes no deeper than the papillary dermis. These burns are completely anaesthetised: a needle could be stuck deep into the dermis without any pain or bleeding. There is commonly abundant fixed capillary staining, particularly if examined after 48 hours. Sensation is decreased, and the affected person is unable to distinguish sharp from blunt strain when examined with a needle. The burn is pale because it was dressed with silver sulphadiazine cream, however no blanching was seen underneath this layer. The affected person was unable to differentiate between stress from the sharp and blunt ends of a needle. It is due to this fact applicable to give oral rehydration with a solution corresponding to Dioralyte. The resuscitation quantity is comparatively fixed in proportion to the area of the body burned and, subsequently, there are formulae that calculate the approximate volume of fluid wanted for the resuscitation of a affected person of a given physique weight with a given proportion of the body burned. These regimes observe the fluid loss, which is at its most within the first 8 hours and slows, such that, by 24�36 hours, the affected person can be maintained on his or her normal every day necessities. This calculates the fluid to get replaced in the first 24 hours by the next formulation: complete share physique floor area � weight (kg) � 4 = quantity (mL). Half this quantity is given in the first eight hours and the second half is given in the subsequent sixteen hours. Plasma proteins are responsible for the inward oncotic strain that counteracts the outward capillary hydrostatic stress. Proteins should be given after the first 12 hours of burn as a outcome of, earlier than this time, the large fluid shifts trigger proteins to leak out of the cells. Monitoring of resuscitation the necessary thing to monitoring of resuscitation is urine output. If the urine output is inadequate and the affected person is displaying signs of hypoperfusion (restlessness with tachycardia, cool peripheries and a excessive haematocrit), then a bolus of 10 mL/kg body weight must be given. Other measures of tissue perfusion similar to acid�base balance are appropriate in bigger, more complex burns, and a haematocrit measurement is a helpful tool in confirming suspected under- or over-hydration. Those with cardiac dysfunction, acute or chronic, may nicely want extra actual measurement of filling strain, preferably by transoesophageal ultrasound or with the more invasive central line. Crystalloids are mentioned to be as efficient as colloids for sustaining intravascular volume. Another cause for using crystalloids is that even giant protein molecules leak out of capillaries following burn injury; nonetheless, non-burnt capillaries continue to sieve proteins virtually usually. The tourniquet impact of this harm is well handled by incising the whole size of full-thickness burns. One should do not forget that an escharotomy may cause a appreciable quantity of blood loss; due to this fact, enough blood ought to be out there for transfusion if required. Thereafter, the management of the burn wound remains the identical, regardless of the scale of the damage. Fullthickness burns and deep partial-thickness burns that will require operative remedy might need to be dressed with an antibacterial dressing to delay the onset of colonisation of the wound. Hypertonic saline Hypertonic saline has been effective in treating burns shock for a quantity of years. Advantages embody less tissue oedema and a resultant decrease in escharotomies and intubations. It is often used as a 5% topical solution, but has been associated with metabolic acidosis. It induces a sterile eschar on the burned skin and has been shown in sure situations, especially in elderly sufferers, to cut back a number of the cell-mediated immunosuppression that happens in burns. Cerium nitrate forms a sterile eschar and is especially useful in treating burns when a conservative remedy choice has been chosen. Cerium nitrate has additionally been proven to boost cell-mediated immunity in these patients. Upper limb Hand Mid-axial, anterior to the elbow medially to keep away from the ulnar nerve Midline in the digits. Posterior to the ankle medially to keep away from the saphenous vein Down the chest lateral to the nipples, across the chest beneath the clavicle and across the chest at the level of the xiphisternum Extend the wound beyond the deep burn Diathermy any vital bleeding vessels Apply haemostatic dressing and elevate the limb postoperatively Superficial partial-thickness wounds and mixed-depth wounds Around the world, a extensive variety of gear are used to treat these wounds, from honey or boiled potato peel to artificial biological dressings with stay cultured fibroblasts within the matrix. This is testomony to the reality that superficial partialthickness burns will heal virtually no matter the dressing. Thus, the necessary thing lies with dressings which might be simple to apply, nonpainful, reduce ache, simple to handle and domestically available. Here, the selection of dressing could make the distinction between scar and no scar and/or operation and no operation. The preliminary exudate needs to be managed by frequent adjustments of fresh linen around the patient however, after a number of days, a dry eschar types, which then separates as the wound epithelialises. However, this technique is painful and requires an intensive quantity of nursing help. A variation on this theme is to cowl the wound with a permeable wound dressing, similar to Mefix or Fixamol. A comparable method of managing most of these burn is to place a Vaseline-impregnated gauze (with or without an antiseptic, similar to chlorhexidine) over the wound. The Vaseline gauze or silicone layer is used to forestall the swabs adhering to the wound and reduces the stiffness of the dry eschar, stopping it from cracking so easily. Hydrocolloid dressings have to be changed Lower limb Chest General guidelines Full-thickness burns and apparent deep dermal wounds the four commonest dressings for full-thickness and contaminated wounds are listed in Table 41. This gives broad spectrum prophylaxis in opposition to bacterial colonisation and is especially effective against Pseudomonas aeruginosa and likewise methicillin-resistant Staphylococcus aureus. The other disadvantage of this solution is that it needs to be changed or the injuries resoaked every 2�4 hours. Small burns, particularly superficial burns, respond well to simple oral analgesia, paracetamol and non-steroidal anti-inflammatory drugs. Subacute In patients with large burns, steady analgesia is required, starting with infusions and persevering with with oral tablets, corresponding to slow-release morphine.
Established arterial occlusions are handled as for atheromatous illness depression testosterone levels generic clomipramine 75 mg free shipping, but amputations may ultimately be required anxiety lightheadedness discount 50 mg clomipramine amex. Treatment is directed primarily at the underlying situation clinical depression symptoms quiz buy discount clomipramine 25 mg line, although the conservative measures outlined above are often useful depression coping skills clomipramine 75 mg low cost. The syndrome when secondary to collagen disease leads frequently to necrosis of digits and a quantity of amputations. Nifedipine, steroids and vasospastic antagonists might all have a task in remedy. Other forms of arteritis Arteritis happens in affiliation with many connective tissue disorders. This is usually the province of the specialist doctor, but the surgeon could also be called on to carry out minor amputations. Temporal arteritis is a illness by which localised infiltration with inflammatory and giant cells results in arterial occlusion, ischaemic headache and tender, palpable, pulseless (thrombosed) arteries in the scalp. The surgeon may be required to perform a temporal artery biopsy, but this could not delay instant steroid therapy to arrest and reverse the process before the ophthalmic artery is involved. It tends to affect young ladies Mikito Takayasu, 1860�1938, Japanese ophthalmologist, described this disease in 1908. Cervical sympathectomy Open cervical sympathectomy was previously performed for vasospastic conditions affecting the arms and to treat palmar (sometimes axillary) hyperhidrosis. The operation is now out of date, having been changed by endoscopic transthoracic sympathectomy. Chemical sympathectomy requires the injection of small quantities of a sclerosant into the lumbar sympathetic chain beneath radiographic control. Lumbar sympathectomy Lumbar sympathectomy has been used to treat chronic decrease limb ischaemia in the past. This extraordinary prevalence together with the associated impairment in healthrelated quality of life make it a vital area of surgical apply. Surgical intervention has been revolutionised by the event of endovenous techniques, and level 1 proof has demonstrated that remedy could be associated with very high clinical- and cost-effectiveness. Despite the considerable significance positioned on decrease limb operate through the administration of orthopaedic and arterial ailments, venous illnesses are sometimes forgotten or dismissed as beauty apply. The superficial veins drain into the deep system, both at junctions or through fascial perforating veins, and the deep veins then return blood to the best atrium of the heart. These six veins intercommunicate and are available together in the popliteal fossa to kind the popliteal vein, which additionally receives the soleal and gastrocnemius veins. The popliteal vein passes up by way of the adductor hiatus to enter the subsartorial canal because the femoral vein, which receives the deep (profunda) femoral vein (or veins) within the femoral triangle before passing behind the inguinal ligament to turn out to be the exterior iliac vein. The inner iliac vein combines with the external iliac vein within the pelvis to form the widespread iliac vein. The left widespread iliac vein passes behind the best frequent iliac artery to be part of the proper common iliac vein on the right aspect of the belly aorta to kind the inferior vena cava, which fits on to the right atrium. As the solely real of the foot is usually placed under significant strain, the vast majority of the venous drainage of the foot is into the dorsal venous arch, running in the subcutaneous tissues over the metatarsal heads. This is the longest vein in the physique and essentially the most frequently affected by superficial incompetence. In the groin, it unites with tributaries comparable to the arterial branches of the widespread femoral artery, before piercing the cribriform fascia overlaying the saphenous opening (approximately 2. In this occasion, its origin is usually a confluence of small tributaries across the knee. However, this junction is highly variable and the vein may terminate as low as the mid-calf. In the calf and thigh there are a number of valved perforating (communicating) veins that be a part of the superficial to the deep veins at inconstant websites and which permit blood Cranial extension of small saphenous (Giacomini) vein Saphenopopliteal junction Small saphenous vein (c) to flow from the superficial to the deep venous system. The most essential of these are the direct perforating veins of the medial and lateral calf and the speaking veins across the knee and within the mid-thigh. The venous system accommodates approximately 60% of the total blood volume, with a median pressure of round 5�10 mmHg. Mechanical elements, alongside the autonomic nervous and endocrine techniques, management the rate Carlo Giacomini, 1840�1898, anatomist, Turin, Italy, on his death left his skeleton to the Anatomical Museum in Turin. As the calf muscle tissue contract, the veins are compressed and the valves only enable blood to move in the path of the center. The stress throughout the calf compartment rises to 200�300 mmHg during muscle contraction. Rapid blood flow in the deep veins at junctions and perforators attracts blood from the superficial veins, driving this up the deep veins additionally. During muscle relaxation, the strain falls and further blood from the superficial veins enters the deep vein. Each time this occurs the strain falls in the superficial venous compartment till a threshold is reached, when the venous inflow keeps pace with ejection from the deep veins. This is normally round 30 mmHg, a fall of roughly two-thirds of the resting venous pressure. The web reduction in the stress of the superficial system depends on the presence of a pressure gradient between the leg and the thorax and a patent and compliant venous system containing competent valves. An absence of a quantity of of these results in venous hypertension, which finally ends up in additional vein wall damage together with loss of compliance, thickening, dilatation and valvular dysfunction. This venous injury goes on to scale back the function of the affected veins, worsening the venous hypertension in a vicious cycle. When exposed to high venous and capillary pressures chronically, the delicate tissues of the leg might be broken, inflicting a spectrum of harm that turn out to be irreversible. Through its results upon myocardial contractility by way of the Starling mechanism, venous return is likely considered one of the factors responsible for figuring out cardiac output. Blood enters the lower limb by way of the femoral arteries before passing by way of arterioles into the capillaries, which have a strain of about 32 mmHg at their arterial ends. This stress is lowered alongside the course of the capillaries and is approximately 12 mmHg on the venular finish of the capillary. The pressure continues to fall in the main veins, and is as little as 5 mmHg at the upper end of the vena cava the place it enters the best atrium. The venous stress in a foot vein on standing is equivalent to the peak of a column of blood extending from the center to the foot. To allow blood to be returned in opposition to gravity within the standing place a stress gradient must exist between the veins within the leg and the chest. Firstly, the increase in thoracic quantity during inspiration decreases intrathoracic strain. The deep veins of the calf are capacious and are joined by blind-ending sacks known as the soleal sinusoids, which drive blood into the popliteal and crural veins during calf muscle pump contraction. Rudolf Virchow, 1821�1902, pathologist Charite Hospital, Berlin, Germany, was the first to be credited with describing iliac vein compression. It was not until 1957 that May and Thurner (Innsbruck, Austria) clearly described compression of the left widespread iliac vein by the right widespread iliac artery. The majority of patients with venous illness have an issue primarily with the vein wall construction and in most this is confined to the superficial veins. Little is thought about the mechanism of initiation of the adjustments within the vein wall. These adjustments are advanced, but are typified by valvular failure allowing retrograde circulate within the vein with gravity (venous incompetence). It is not thought that venous incompetence is brought on by a primary mechanical valvular failure. The vein wall adjustments include inflammatory cell infiltration and activation, dysfunctional clean muscle cell proliferation, collagen deposition, decreased elastin content and increased matrix metalloproteinases. These results sometimes lead to lack of compliance, dilatation, elongation (causing tortuosity) and secondary valvular dysfunction. Secondary varicose veins may develop in patients with post-thrombotic limbs and in sufferers with congenital abnormalities such because the Klippel� Trenaunay syndrome or a quantity of arteriovenous fistulae. The extent and variety of incompetent veins governs the extent of the venous hypertension and correlates to the severity of the delicate tissue problems seen. Importantly nevertheless, neither the reflux burden nor the presence of pores and skin modifications, wanting ulceration, correlate with the presence or degree of symptoms. Corona phlebectatica (malleolar flare): a fan-shaped sample of telangiectasia on the ankle or foot. Commonly starts distally and moves extra proximally with increasing venous dysfunction.
10 mg clomipramine order. Bipolar disorder (depression & mania) - causes symptoms treatment & pathology.