
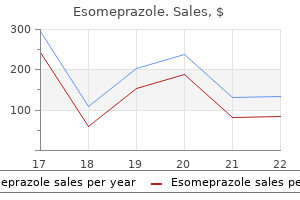
Esomeprazole
| Contato
Página Inicial

"Esomeprazole 40 mg order, gastritis or appendicitis".
N. Rathgar, M.B. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Medical University of South Carolina College of Medicine
The dialysate and ultrafiltrate are then drained from the peritoneal cavity and recent dialysate is instilled gastritis diet ����������� 40 mg esomeprazole purchase. The affected person is liable for performing the exchanges gastritis like symptoms generic 20 mg esomeprazole mastercard, taking very important indicators gastritis diet chart cheap 20 mg esomeprazole with mastercard, weighing themselves gastritis diet sweet potato esomeprazole 40 mg discount visa, and using their judgment to determine the correct dextrose concentrations for their dwells (thereby affecting their fluid removal). Exit website infections current with ache on the exit website, erythema, and purulent drainage. The commonest organisms associated with exit web site infections are coagulasenegative Staphylococcus, S. Unless the patient has a history of Pseudomonas exit web site infection, initial treatment could be directed towards gram-positive organisms and tailor-made depending on tradition knowledge. Empiric antibiotic therapy of peritonitis requires coverage for both gram-positive and gram-negative micro organism. Finally, catheter problems, similar to kinking or malposition, can result in issues with dialysis and should require surgical correction. If patients proceed to have uremic signs on dialysis, the dose must be elevated. On hemodialysis, the dose could be elevated by increasing the dialysis time, blood circulate price, or the surface space of the dialysis filter. In the absence of uremic symptoms, measuring urea clearance with dialysis presents a method to monitor dialysis dose. The standard dose group received, on average, 190 minute dialysis therapies 3 times every week, while the high-dose group received 219 minutes per remedy. After a follow-up of over 2 years, there was no distinction in mortality between the two teams; each groups had a median yearly Table 12-2. Based on the observational data and the interventional research, it is suggested for hemodialysis patients to have a minimal single-pool Kt/V of 1. In the United States, the overwhelming majority of the patients on dialysis die from cardiovascular causes, corresponding to acute myocardial infarction, sudden cardiac death, and congestive heart failure. Unfortunately, reducing cardiovascular mortality has been hampered by the shortage of evidence-based therapies. Achieving euvolemia requires each fluid elimination with dialysis and affected person adherence to a low-salt food plan. Data from observational studies in dialysis sufferers may be useful but, sadly, observational research have shown conflicting results regarding blood strain ranges and cardiovascular mortality. This is partly as a end result of excessive variability of blood strain readings in hemodialysis patients depending on the timing of the measurement. In reality, ambulatory blood stress displays predict mortality higher in dialysis patients than blood stress measurements throughout dialysis. To achieve blood strain control, sustaining euvolemia is crucial; however, regardless of attaining euvolemia, many sufferers would require antihypertensive drugs. Dialysis sufferers also can have a type of bone illness often recognized as osteomalacia, a disease of faulty bone mineralization sometimes related to aluminum toxicity. Although blood markers might help distinguish forms of bone disease, a bone biopsy is the only definitive way to diagnose the precise Chapter 12 the Patient Receiving Chronic Renal Replacement with Dialysis 261 abnormality in bone metabolism. Preventing malnutrition improves the quality of life for dialysis patients and sure improves mortality. Dialysis patients are at risk for malnutrition due to enhanced muscle breakdown, inadequate caloric consumption, and protein losses due to dialysis itself. A complete assessment of dietary standing contains serial weight measurements, serum markers (albumin, prealbumin, or creatinine), questionnaires (Subjective Global Assessment), dietary interviews, anthropomorphic measurements, and presumably urine collections to measure nitrogen excretion (an estimate of every day protein intake). The suggestions additionally state that hemodialysis patients eat protein greater than 1. There is a major body of data demonstrating that therapy of metabolic acidosis improves nutritional status. In observational studies, anemia was related to a decrease in quality of life, impairment in cardiac perform, and mortality. In the previous, anemia was handled with pink blood cell transfusions, a treatment that would trigger iron overload or sensitization to future transplants and which conferred risks of infections similar to hepatitis B and C. Since there have been no direct comparisons of the 2 remedy courses, treatment of anemia varies significantly relying on affected person characteristics and provider preferences. Clinical practice guidelines for anemia in continual kidney disease: problems and options. Advantages embody longer affected person survival, much less morbidity, value financial savings, and improved quality of life compared with dialysis. Living kidney donation remains the best therapy, with common graft survival of approximately 12 to 15 years, with longer survival for well-matched sibling transplants. This excellent news is tempered by the truth that demand for transplant kidneys far exceeds the provision of obtainable organs. Recipient Evaluation the targets of evaluating a possible recipient must be to determine potential barriers to transplantation, identify treatable circumstances that may attenuate the danger of the surgery or immunosuppression, and clarify the benefits and risks. Comorbid situations and the consequences of immunosuppression on these situations are considered. Patient age older than 50 years, 263 264 Chapter 13 the Patient with a Kidney Transplant diabetes, abnormal electrocardiogram, angina, or congestive heart failure have been demonstrated as predictors of cardiac dying and nonfatal cardiac events with kidney transplantation. Noninvasive methods such as thallium perfusion imaging and dobutamine stress echo have demonstrated the power to predict cardiac occasions and should prevent high-risk sufferers from requiring angiography. In sufferers with malignancies, a 2- to 5-year remission could additionally be required earlier than transplantation relying on tumor kind, invasiveness, and prior remedy. Although obesity is a risk for wound-related problems, long-term outcomes are just like nonobese patients except heart problems exists. Imaging or functional analysis of the kidneys and decrease urinary tract may be necessary in sure patients. After a affected person has been accepted as a candidate, she or he is added to the transplant waiting listing, at which period initial medical screening of potential residing kidney donors can take place. A affected person on the ready list for more than 1 12 months must be seen periodically to replace his or her situation. Although the dangers of kidney donation are small, these risks must be carefully defined to a possible residing donor. Infection, bleeding, and other postoperative complications happen in as much as 15% of sufferers. Mild blood stress elevation and proteinuria after donation has been reported in some studies however not all, and the long-term penalties are at present unclear. Donors are rigorously screened for kidney disease to forestall the risk of loss of perform within the remaining kidney. Hypertension, proteinuria, weight problems, kidney stones, and structural Chapter thirteen the Patient with a Kidney Transplant 265 or useful kidney illness are all relative contraindications to donation relying on severity. When recipients are affected by hereditary issues similar to polycystic kidney illness or hereditary nephritis, the situation should be dominated out in related donors either clinically or with genetic testing. Donors with hepatitis C are sometimes accepted for hepatitis C�positive recipients. A mixture of factors similar to hypertension, advanced age, elevated serum creatinine, oliguria, or dependence on pressor help could exclude a donor. They are generally utilized in recipients with characteristics associated with poor dialysis survival similar to advanced age or diabetes. Predictors of Outcome Recipient elements, donor elements, and donor/recipient compatibility all affect long-term graft survival. Race and ethnicity could have an effect on graft survival for both donors and recipients, with nonblack donor kidneys and nonblack, non-Hispanic recipients of grafts having the longest graft survival. Kidneys from residing associated or unrelated donors survive longer on average than deceased donor kidneys, as do kidneys from younger compared with older donors. Immunology A primary evaluation of the mechanisms of immune recognition and response to an allograft is helpful to higher understand the affected person who has undergone kidney transplantation as nicely as the pharmacologic brokers used to forestall allograft rejection. Although advances in immunosuppression have narrowed benefits for well-matched transplants, a two-haplotype similar transplant from a member of the family or a zero-antigen mismatched deceased donor transplant confers a graft survival profit compared with transplants with lesser degrees of matching. T cells T cells are processed within the thymus and are central to cellular immunity and allograft recognition and rejection. These properties make them a standard target of medicine designed to stop rejection. They then initiate an immune response to foreign peptides by secreting cytokines important in B-cell proliferation and activation and cytotoxic T-cell activation. Although signal 1 alone will trigger anergy, the addition of signal 2, also called costimulation, will lead to an immune response.
Diseases
- Marfanoid hypermobility
- Oculodental syndrome Rutherfurd syndrome
- Generalized malformations in neuronal migration
- Hypertriglycidemia
- Proteus syndrome
- Autism
- Spinocerebellar ataxia dysmorphism
- Dionisi Vici Sabetta Gambarara syndrome
- Psittacosis
Congenital localized absence of pores and skin and associated abnormalities resembling epidermolysis bullosa gastritis like symptoms order esomeprazole 40 mg online. Extracutaneous manifestations and complications of inherited epidermolysis bullosa: part I gastritis diet ���� 20 mg esomeprazole buy mastercard. Insights from a desmoplakin mutation recognized in deadly acantholytic epidermolysis bullosa gastritis diet ��� cheap esomeprazole 20 mg without prescription. Mutations in the plakophilin 1 gene lead to ectodermal dysplasia/skin fragility syndrome gastritis emedicine esomeprazole 20 mg order amex. Laryngeal involvement within the Dowling-Meara variant of epidermolysis bullosa simplex with keratin mutations of severely disruptive potential. Molecular confirmation of the unique phenotype of epidermolysis bullosa simplex with mottled pigmentation. Tracheolaryngeal complications of inherited epidermolysis bullosa: cumulative expertise of the national epidermolysis bullosa registry. Prenatal prognosis of inherited epidermolysis bullosa in a patient with no family historical past: a case report and literature review. Outcome after surgical restore of junctional epidermolysis bullosa-pyloric atresia syndrome: a report of three instances and evaluate of the literature. Herlitz junctional epidermolysis bullosa: diagnostic features, mutational profile, incidence and population service frequency in the Netherlands. Molecular mechanisms of phenotypic variability in junctional epidermolysis bullosa. The challenges of meeting nutritional requirements in kids and adults with epidermolysis bullosa: proceedings of a multidisciplinary group examine day. Kindler syndrome pathogenesis and fermitin family homologue 1 (kindlin-1) operate. Ankyloblepharon-ectodermal dysplasia-clefting syndrome: a novel p63 mutation related to generalized neonatal erosions. A comparative research between transmission electron microscopy and immunofluorescence mapping in the prognosis of epidermolysis bullosa. Epidermolysis bullosa: management ideas for the neonate, toddler, and young youngster. Assessment of mobility, actions and ache in different subtypes of epidermolysis bullosa. Proceedings of the 5th International Symposium on Epidermolysis Bullosa, Santiago Chile, December 4�6. Treatment decision-making for sufferers with the Herlitz subtype of junctional epidermolysis bullosa. Oral health take care of patients with epidermolysis bullosa � greatest scientific practice pointers. Correction of junctional epidermolysis bullosa by transplantation of genetically modified epidermal stem cells. Neonatal pemphigus in an infant born to a mother with serologic proof of both pemphigus vulgaris and gestational pemphigoid. Neonatal pemphigus vulgaris passively transmitted from a clinically asymptomatic mom. Herpes gestationis in a mother and new child: immunoclinical views based mostly on a weekly follow-up of the enzyme-linked immunosorbent assay index of a bullous pemphigoid antigen noncollagenous area. Linear IgA bullous dermatosis of neonatal onset: case report and evaluation of the literature. Linear IgA bullous dermatosis of childhood with autoantibodies to a 230 kDa epidermal antigen. Clinical options, diagnosis, and pathogenesis of chronic bullous disease of childhood. A study of benign chronic bullous dermatosis of childhood and comparison with dermatitis herpetiformis and bullous pemphigoid occurring in childhood. Chronic bullous disease of childhood, childhood cicatricial pemphigoid, and linear IgA illness of adults. Bullous pemphigoid of childhood: a uncommon disease with diagnostic and administration challenges. Childhood bullous pemphigoid: a clinicopathologic study and evaluate of the literature. Childhood bullous pemphigoid: report of a case with life-threatening course during homeopathy remedy. Childhood bullous pemphigoid: scientific and immunological findings in a collection of 4 circumstances. Childhood bullous pemphigoid: report of a case with characterization of the focused antigens. Bullous pemphigoid in late childhood efficiently handled with mycophenolate mofetil as an adjuvant therapy. A case of juvenile bullous pemphigoid � profitable remedy with diaminodiphenylsulfone and prednisone. Linear IgA illness with scientific and immunopathological options of epidermolysis bullosa acquisita. Childhood IgA-mediated epidermolysis bullosa acquisita responding to mycophenolate mofetil as a corticosteroid-sparing agent. Adjuvant medication in autoimmune bullous illnesses, efficacy versus safety: Facts and controversies. Anaphylaxis in sufferers with mastocytosis: a research on historical past, medical features and danger elements in a hundred and twenty sufferers. Diffuse cutaneous mastocytosis: analysis of 10 circumstances and a brief review of the literature. Bullous impetigo is almost solely caused by Staphylococcus aureus, most commonly phage group 2 (types seventy one and 55) that elaborates toxins. Lesions are probably to be localized in major impetigo, but may turn out to be more widespread when superimposed on diseased pores and skin. Moist intertriginous, periorificial and periumbilical areas are generally involved in both nonbullous and bullous impetigo. Bullous impetigo usually presents through the first 2 weeks of life with flaccid, clear, subcorneal bullae, which can be single or clustered, and sometimes lack underlying cutaneous erythema. Extracutaneous findings Most instances of impetigo, together with neonatal bullous impetigo, are unaccompanied by constitutional signs of sickness. Occasionally, hematogenous spread of bacteria can lead to osteomyelitis, septic arthritis, pneumonia, or septicemia, notably in neonates with bullous impetigo. The staphylococcal organisms that trigger nonbullous impetigo are variable, however are generally not from phage group 2, whereas bullous impetigo is mostly (80%) the end result of S. Infection from hematogenous penetration of the placental barrier or via ruptured amniotic membranes may be more extreme and widespread, involving multiple organ techniques along with the skin, due to the vulnerable state of the creating neonate. Importantly, neonatal cutaneous infections, even these acquired postnatally, are doubtlessly extra serious compared with related cutaneous infections in older kids. The purpose for these variations in severity is multifactorial, involving a fancy interaction between host, pathogen, and environmental components (Box 12. Furthermore, the potential influence of a localized cutaneous infection is of larger concern in neonates, the place alterations of the traditional pores and skin barrier are extra frequent and may function a conduit for systemic infection. This is particularly true for very low-birthweight infants the place organisms that usually colonize the pores and skin are additionally implicated as etiologic agents of sepsis. This suggests that sepsis could also be a consequence of bacterial penetration at websites of skin injury or through the immature epidermal barrier. The medical presentation, pathogenesis, diagnostic modalities and instructed therapeutic interventions are reviewed for numerous common and less frequent neonatal cutaneous infections. The continued emergence of antibiotic resistance has sophisticated the empiric therapeutic options for some bacterial infections. This emergence of resistance has highlighted the importance of obtaining cultures when potential to identify the pathogen and its sensitivity profile. Recommendations regarding antibiotic selections and duration of remedy particular to the an infection are supplied for every clinical situation noting the potential impression of resistance on antibiotic choices.
Diseases
- Keratoderma palmoplantar deafness
- Maxillofacial dysostosis
- Craniostenosis
- X-linked severe combined immunodeficiency
- Hepatic ductular hypoplasia
- Gitelman syndrome
Physical findings with acute drug-induced interstitial nephritis may be lacking gastritis pronounce purchase 20 mg esomeprazole with amex, though fever and a maculopapular or petechial skin eruption may occur with any of the agents chronic superficial gastritis diet 20 mg esomeprazole cheap mastercard, particularly the penicillin derivatives and allopurinol gastritis tylenol cheap esomeprazole 40 mg fast delivery. However gastritis diet 7 up nutrition esomeprazole 20 mg buy overnight delivery, this discovering may be missing, and different clinical clues shall be essential to make the analysis. To distinguish between the 2, quite a few diagnostic indices and formulae have been developed based on their pathophysiologic differences. The elevated reabsorption of water increases urine particular gravity and osmolality. The incidence of nephrotoxicity correlates higher with whole cumulative dose than with plasma ranges. Predisposing factors are old age, preexisting renal illness, quantity depletion, and mixture with other brokers. Nephrotoxicity is often clinically obvious after 5 to 10 days of therapy; early findings are isosthenuria attributable to nephrogenic diabetes insipidus, and magnesium and potassium wasting. It is recommended that, in sufferers with regular kidney function in steady state, aminoglycosides are administered as a single dose daily quite than multiple-dose daily therapy regimens. It can be advised that aminoglycoside drug ranges are monitored when treatment with single day by day dosing is used for more than forty eight hours. Serum creatinine usually peaks at 3 to 4 days and returns to baseline after a few week. Chapter 10 the Patient with Acute Kidney Injury 227 Although quite a few brokers have been studied to forestall contrast nephropathy, the one therapies which have been proven to be helpful are intravenous hydration with either isotonic saline or isotonic sodium bicarbonate earlier than and after the distinction load. Rhabdomyolysis is caused by muscle injury (traumatic or atraumatic) that results in the systemic launch of muscle contents including myoglobin. Rhabdomyolysis ought to be considered in sufferers with trauma, muscle ache, and darkish brown urine. Laboratory clues to the analysis include a speedy rise of serum creatinine, massively elevated creatine phosphokinase, hyperphosphatemia, hyperuricemia, hypocalcemia, elevated anion gap, and disproportionate hyperkalemia. Serum calcium is decreased because of the sequestration of calcium into injured muscle; this calcium is released from the tissue through the restoration section and will cause hypercalcemia. Therefore, alternative of serum calcium ought to be prevented except symptoms of hypocalcemia are current. The solely confirmed remedy within the therapy of rhabdomyolysis is early and vigorous infusion of intravenous isotonic saline. Mannitol administration and urinary alkalinization are often attempted within the therapy of rhabdomyolysis, though their efficacy may not be superior to vigorous hydration with saline alone. Theoretically, forced diuresis with mannitol could help within the washout of obstructing myoglobin pigment. Mannitol administration may be tried only after the correction of volume deficits; saline and mannitol ought to be administered along with a aim urine output of 300 mL/hour. Urinary alkalinization could inhibit myoglobin precipitation; nonetheless, urinary alkalinization is difficult to obtain in apply and requires the administration of a big quantity of bicarbonate. Bicarbonate administration in rhabdomyolysis carries the danger of worsening hypocalcemia because of increased calcium and phosphorus precipitation into injured muscle. Thus, mannitol and urinary alkalinization must be utilized cautiously, if at all, in the management of rhabdomyolysis. The situation usually happens during induction chemotherapy for malignancies with high cell turnover. Clinical options of acute uric acid nephropathy are hyperuricemia, hyperkalemia, hyperphosphatemia, and a urine urate to creatinine ratio larger than 1. Preventive measures embody allopurinol administration (300 to 600 mg/day) and vigorous hydration and compelled diuresis with mannitol. Alkalinization of the urine has been traditionally recommended, but has not been proved more useful than saline administration alone; moreover, bicarbonate therapy carries the risk of elevated calcium precipitation. Rasburicase, a recombinant urate oxidase, can decrease uric acid ranges quickly allowing earlier Chapter 10 the Patient with Acute Kidney Injury 229 institution of chemotherapy, and will cut back the danger of acute uric acid nephropathy. Oral or enema sodium phosphosoda due to this fact is contraindicated in patients with kidney illness. Shape/Appearance Needle formed Envelope formed Diamond shaped, yellow or brown Needle formed or shocks of wheat Needle shaped, birefringent Needle formed, often forming rosettes Uric acid Sulfadiazine Acyclovir Indinavir sulfate or atazanavir 230 Chapter 10 the Patient with Acute Kidney Injury Table 10-11. All supportive measures, including dialysis, ought to be used as warranted by the scientific scenario. Glomerulonephritis and liver cirrhosis are associated with cryoglobulinemia, IgA nephropathy, membranous glomerulonephritis (associated with hepatitis B), and membranoproliferative glomerulonephritis (associated with hepatitis C). A renal biopsy in such circumstances could present the 232 Chapter 10 the Patient with Acute Kidney Injury foundation and justification for aggressive and life-saving therapy. When 1 L of isotonic crystalloid is given, roughly 250 mL remains within the plasma compartment, whereas 750 mL enters the interstitial compartment. After a bolus, the patient ought to be evaluated clinically for indicators of hypovolemia or quantity overload. The presence of basilar crackles or a 3rd heart sound implies too vigorous fluid substitute, Chapter 10 the Patient with Acute Kidney Injury 233 with resultant cardiopulmonary congestion. Prerenal azotemia in this setting is often a secondary drawback overshadowed by main cardiac or liver disease. Ordinarily, nonetheless, the administration goal is to reduce signs and treat ascites and edema with a sodium-restricted food plan (1 to 2 g of salt per day), an aldosterone antagonist. Foley catheter drainage is often successful for acute obstruction secondary to prostatic hypertrophy. The determination relating to further remedy must be made in session with a urologist. Medical remedy with finasteride or an -blocker, or surgical removal of prostatic tissue could additionally be really helpful. With ureteral obstruction, cystoscopy and the position of ureteral drainage catheters or stents may permit passage of obstructing stones, sludge, or pus, but when this fails, surgical intervention is required. With ureteral 234 Chapter 10 the Patient with Acute Kidney Injury obstruction because of extra persistent circumstances like tumor infiltration, prograde stents and nephrostomies are sometimes placed by interventional radiology. A complete dialogue of the remedy of these systemic and vascular problems is beyond the scope of this chapter. Obtaining a renal biopsy early after presentation is crucial to make the analysis and to guide applicable remedy. Therapeutic options embody immunosuppressive remedy with steroids and/or cyclophosphamide. Treatment regimens are varied; however, initiation remedy with 1 mg/kg of prednisone (up to 60 mg/day) for 2 to four weeks with a taper for two to 3 months is a commonly used strategy. In all circumstances, the approach to care must be individualized, with the danger and benefits of steroid therapy and kidney biopsy fastidiously considered. It elicits profound natriuresis and increases urine output in sufferers with regular kidney function. In patients with acute lung harm, conservative fluid management improves outcomes without growing the development of nonpulmonary organ failures such because the kidney. Drug dosages ought to be adjusted based on the measured or best estimate of CrCl, not merely on serum creatinine. Renal factors contributing to the adverse nitrogen balance include uremia, acidosis, parathyroid hormone abnormalities, insufficient protein intake, and protein losses. In this type of dialysis, the affected person is connected to a dialysis machine for four hours at a time, day by day or every second day. Fluid removal and urea clearance for the day is achieved in the course of the interval of some hours. It is well described that delivered doses of dialysis may not match prescribed dose and that underdosing of dialysis is related to worse outcomes. In apply, interruptions in dialysis for patient procedures, radiologic testing, and dialysis membrane clotting are frequent and reduce the amount of time the patient is actually receiving dialysis. Because the elimination of solutes and fluid is slow and steady, hemodynamic instability and hypotensive episodes are reduced. Minimization of hypotension theoretically avoids the perpetuation of renal harm. It can be utilized in patients with minimally elevated catabolism without an immediate or life-threatening indication for dialysis. For short-term dialysis, a inflexible dialysis catheter is inserted into the peritoneum, via the anterior abdominal wall, 5 to 10 cm under the umbilicus. The major risks are bowel perforation throughout insertion of the catheter and peritonitis. The decision may also rely upon facility-specific points, such as expertise, nursing sources, and technical proficiency.