
Imuran
| Contato
Página Inicial

"Imuran 50 mg purchase free shipping, back spasms 4 weeks pregnant".
S. Olivier, MD
Co-Director, Howard University College of Medicine
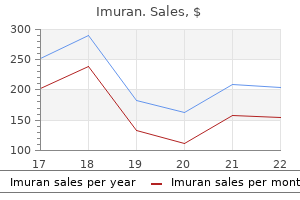
In: Radiology of the Heart: Cardiac Imaging in Infants spasms after stroke discount imuran 50 mg on-line, Children muscle relaxant whiplash imuran 50 mg purchase with visa, and Adults: New York spasms hip order 50 mg imuran amex, Berlin Heidelberg Tokyo: Springer-Verlag; 1985:525�532 infantile spasms 2 year old generic imuran 50 mg with visa. Burns and Hugo Spindola-Franco Definition In truncus arteriosus, a single arterial trunk arises from a single semilunar valve at the base of the heart. The widespread arterial trunk (truncus) offers rise to the systemic, coronary, and pulmonary arteries. Clinical Features the amount of blood move and the degree of pulmonary resistance decide the clinical options of truncus arteriosus. Truncus arteriosus with ostial or branch pulmonary arterial stenosis or increased pulmonary resistance normally presents with cyanosis. Truncus arteriosus with out pulmonic stenosis or elevated pulmonary resistance might not have apparent cyanosis, but quite may present with congestive heart failure. The severity of congestive heart failure is expounded to the degree of both pulmonary overcirculation and truncal valve insufficiency. Any type of truncus arteriosus may present with a murmur usually at the decrease left sternal border, radiating to the whole precordium. Anatomy and Physiology Normally, the aorta arises from the left ventricle and the pulmonary trunk from the proper ventricle. The regular aortic and pulmonary (semilunar) valves have an analogous tricuspid structure. Characteristically, the pulmonary valve is supported by the best ventricular infundibulum. In different phrases, the common arterial trunk has a biventricular origin and is located over each the proper and left ventricles. In some cases, the truncus might arise completely from the right or left ventricle. In rare situations, communication between the ventricles is impeded by dysplastic tissue arising from the interventricular septum and attaching to the commissures of the truncal valve. The proper ventricle turns into dilated and hypertrophied secondary to systemic strain within the widespread arterial trunk. In 60�70% of sufferers with truncus arteriosus, the truncal valve is tricuspid, though it might have between one and six cusps. The truncal valve leaflets could also be thickened and dysplastic, predisposing to stenosis, insufficiency (prolapse), or each. About half of patients with truncus arteriosus have truncal valve insufficiency and about one-third have truncal valve stenosis. Just because the aortic valve is in fibrous continuity with the mitral valve, so is the truncal valve. The tricuspid and truncal valves, against this, are usually discontinuous, separated by the ventriculoinfundibular fold. Rarely, the mitral, tricuspid, and truncal valves could all be in continuity, or, even more rarely, they may lack continuity altogether. The origins and proximal programs of the coronary arteries are extremely variable and have an elevated incidence of a single coronary artery origin. Approximately one-third of patients with truncus arteriosus have a right-sided aortic arch. Unilateral absence of a pulmonary artery might happen in up to 16% of patients and often occurs on the facet of the aortic arch. This is in contradistinction to tetralogy of Fallot, during which absence of the pulmonary artery happens on the other facet of the aortic arch. In one sequence, 10% of sufferers with truncus arteriosus had interruption of the aortic arch. Other associated anomalies embody aortic arch hypoplasia, aortic coarctation, persistent left superior vena cava, aberrant proper subclavian artery from the descending thoracic aorta, and atrial septal defects (especially secundum type). How to Approach the Image Radiographic features of truncus arteriosus depend upon the quantity of pulmonary blood circulate and pulmonary resistance. Patients with truncus arteriosus with unrestricted blood circulate to the lungs present with pulmonary overcirculation and heart failure. In distinction, sufferers with truncus arteriosus with pulmonic stenosis show pulmonary undercirculation. Chest radiograph of a 2-day-old boy with type 1 truncus arteriosus and interruption of the aortic arch who offered with a murmur at the left lower sternal border. There is cardiomegaly with rounding and upward rotation of the cardiac apex suggestive of proper ventricular enlargement. Pulmonary vascular redistribution and indistinctness of the pulmonary vessels are according to reasonable congestive coronary heart failure. The presence of a right aortic arch and pulmonary overcirculation should alert the radiologist to the potential of truncus arteriosus. Cross-sectional imaging can clearly reveal abnormal truncal valvular morphology and the connection of the truncal valve to the interventricular septum. Postoperative cross-sectional imaging could additionally be useful for anatomic and functional downside solving. Type I: the primary pulmonary artery is a branch of the common trunk and provides rise to proper and left pulmonary arteries. A combined kind of truncus arteriosus happens with unilateral absence of a pulmonary artery. Complete major surgical restore is performed within the neonatal interval to stop pulmonary vascular obstructive disease brought on by elevated stress within the pulmonary arteries. Moderate to extreme truncal valve insufficiency earlier than repair and interruption of the aortic arch are circumstances associated with decreased postoperative survival. Conduit alternative or revision is kind of all the time necessary after full restore of truncus arteriosus with a median time to reoperation of 5 to 6 years. For sufferers with truncal valve insufficiency earlier than full restore, truncal valvuloplasty method could also be carried out. The proximal right subclavian artery (arrow) is occluded with distal reconstitution via the proper vertebral artery (dotted arrow). Key Points In truncus arteriosus, a single arterial trunk arises from a single semilunar valve at the base of the center, which supplies rise to the systemic, coronary, and pulmonary arteries. All types of truncus arteriosus may be sophisticated by ostial or branch pulmonary arterial stenosis or increased pulmonary vascular resistance, leading to cyanosis. Truncal valve insufficiency is probably considered one of the commonest problems and should present concurrently with pulmonary arterial stenosis. If truncal valve insufficiency is extreme, heart failure will be present shortly after start. Late follow-up of 1095 patients present process operation for advanced congenital coronary heart disease utilizing pulmonary ventricle to pulmonary artery conduits. Persistent truncus arteriosus: pathologic, diagnostic and therapeutic concerns. Selection of patients with truncus arteriosus for surgical correction: anatomic and hemodynamic considerations. The anatomy of widespread aorticopulmonary trunk (truncus arteriosus communis) and its embryologic implications: a research of fifty seven necropsy circumstances. Conduction abnormalities including first-degree to full coronary heart block could develop. Unrepaired adult survivors normally develop pulmonary hypertension, which results in Eisenmenger syndrome and preferential move into the aorta. Anatomy and Physiology Normally, the aorta arises from the left ventricle and the pulmonary trunk originates from the proper ventricle. The pulmonary valve is located anterior, superior, and to the left of the aortic valve. The aortic and mitral valves and aortic and tricuspid valves are in fibrous continuity. In contradistinction, the pulmonary and tricuspid valves are discontinuous, separated by the crista supraventricularis. Persistent left superior vena cava drainage into the coronary sinus or left atrium (20%), coronary artery anomalies (20%), and situs anomalies (10%) are much less common associations. A lack of fibrous continuity of the aortic and mitral valves can be attribute. The thoracic aorta should be examined for coarctation, hypoplasia of the arch, or interruption. Additionally, a valved conduit from the right ventricle to the pulmonary artery (Rastelli procedure) is often wanted for sufferers with pulmonary stenosis. The arterial switch process has largely changed the influx (Mustard and Senning) procedures, by which an interatrial baffle is constructed to redirect pulmonary venous return into the proper ventricle and systemic venous blood into the left ventricle.
Diseases
- Hip dysplasia (canine)
- Nose polyposis, familial
- Korula Wilson Salomonson syndrome
- Chromosome 3, monosomy 3p
- Gamborg Nielsen syndrome
- Frontonasal dysplasia Klippel Feil syndrome
- Landouzy Dejerine muscular dystrophy
- Lopez Hernandez syndrome
- Tracheoesophageal fistula symphalangism
- Hyperreflexia
The uterine tube lies in the anterosuperior free border of the broad ligament quadricep spasms imuran 50 mg order visa, inside a small mesentery referred to as the mesosalpinx muscle relaxant cyclobenzaprine high imuran 50 mg cheap overnight delivery. The principal supports of the uterus holding it in this place are both passive and lively or dynamic spasms 1983 youtube imuran 50 mg discount. Its tone during sitting and standing and energetic contraction during periods of increased intraabdominal stress (sneezing muscle relaxant walgreens imuran 50 mg buy fast delivery, coughing, and so on. When intra-abdominal pressure is increased, the uterus is pressed towards the bladder. The cervix is generally fibrous and is composed primarily of collagen with a small quantity of clean muscle and elastin. Posteriorly, the uterine body and supravaginal a half of the cervix are separated from the sigmoid colon by a layer of peritoneum, and the peritoneal cavity and from the rectum by the recto-uterine pouch. The vaginal orifice, exterior urethral orifice, and ducts of the greater and lesser vestibular glands open into the vestibule of the vagina, the cleft between the labia minora. The peritoneum is unbroken, lining the pelvic cavity and masking the superior side of the bladder, fundus and physique of uterus, and far of the rectum. The round ligament of the uterus follows the identical subperitoneal course because the ductus deferens of the male. The orifice is normally collapsed toward the midline in order that its lateral walls are in touch on each side of an anteroposterior slit. The posterior vaginal fornix is the deepest part and is intently related to the recto-uterine pouch. These veins are steady with the uterine venous plexus because the uterovaginal venous plexus, and drain into the inner iliac veins by way of the uterine vein. Only the inferior one fifth to one quarter of the vagina is somatic in phrases of innervation. Only this somatically innervated half is delicate to touch and temperature, even though the somatic and visceral afferent fibers have their cell our bodies in the identical (S2�S4) spinal ganglia. Most of the vagina (superior three quarters to four fifths) is visceral in terms of its innervation. The uterovaginal nerve plexus is likely considered one of the pelvic plexuses that extends to the pelvic viscera from the inferior hypogastric plexus. Sympathetic innervation originates in the inferior thoracic spinal cord segments and passes by way of lumbar splanchnic nerves and the intermesenteric-hypogastric-pelvic sequence of plexuses. The two different routes followed by visceral ache fibers is clinically important in that it provides moms a variety of forms of anesthesia for childbirth (see the blue box "Anesthesia for Childbirth," on p. All visceral afferent fibers from the uterus and vagina not concerned with ache (those conveying unconscious sensations) also comply with the latter route. Pelvic splanchnic nerves, arising from the S2�S4 anterior rami, provide parasympathetic motor fibers to the uterus and vagina (and vasodilator fibers to the erectile tissue of the clitoris and bulb of the vestibule; not shown). Presynaptic sympathetic fibers traverse the sympathetic trunk and cross by way of the lumbar splanchnic nerves to synapse in prevertebral ganglia with postsynaptic fibers; the latter fibers travel via the superior and inferior hypogastric plexuses to attain the pelvic viscera. Visceral afferent fibers conducting ache from intraperitoneal constructions (such because the uterine body) journey with the sympathetic fibers to the T12�L2 spinal ganglia. Visceral afferent fibers conducting ache from subperitoneal constructions, such as the cervix and vagina. Somatic sensation from the opening of the vagina additionally passes to the S2�S4 spinal ganglia by way of the pudendal nerve. Conversely, inflammation of a tube (salpingitis) might result from infections that spread from the peritoneal cavity. Accumulation of radiopaque fluid or the looks of gasoline bubbles within the pararectal fossae area of the peritoneal cavity indicates that the tubes are patent. Arrowheads, uterine tubes; c, catheter within the cervical canal, vs, vaginal speculum. Ectopic Tubal Pregnancy In some women, collections of pus could develop in a uterine tube (pyosalpinx) and the tube may be partly occluded by adhesions. Tubal being pregnant is the most common kind of ectopic gestation; it happens in approximately 1 of each 250 pregnancies in North America (Moore et al. In both circumstances, the parietal peritoneum is inflamed in the identical common area, and the pain is referred to the best lower quadrant of the stomach. The scenario is exacerbated in the presence of a disrupted perineal body or with atrophic ("relaxed") pelvic flooring ligaments and muscles (see the blue box "Disruption of Perineal Body," p. The measurement and different characteristics of the uterus can be decided in this way. Because of the small measurement of the pelvic cavity during infancy, the uterus is mainly an stomach organ. The cervix remains comparatively giant (approximately 50% of whole uterus) throughout childhood. All these levels represent normal anatomy for the actual age and reproductive status of the lady. Because no peritoneum intervenes between the anterior cervix and the bottom of the bladder, cervical cancer could unfold by contiguity to the bladder. Hysterectomy Owing to the frequency of uterine and cervical most cancers, hysterectomy, excision of the uterus (G. Cervical Cancer, Cervical Examination and Pap Smear Until 1940, cervical most cancers was the main explanation for demise in North American ladies (Krebs, 2000). Lateral distension is proscribed by the ischial spines, which project posteromedially, and the sacrospinous ligaments extending from these spines to the lateral margins of the sacrum and coccyx. Urine enters the vagina from both vesicovaginal and urethrovaginal fistulas, but the flow is continuous from the former and happens only during micturition from the latter. Digital Pelvic Examination Because of its relatively thin, distensible partitions and central location throughout the pelvis, the cervix, ischial spines, and sacral promontory could be palpated with the gloved digits within the vagina and/or rectum (manual pelvic examination). Chapter three � Pelvis and Perineum Forceps 397 Culdoscopy and Culdocentesis An endoscopic instrument (culdoscope) can be inserted by way of the posterior part of the vaginal fornix to examine the ovaries or uterine tubes. Although it involves less disruption of tissue, culdoscopy has been largely changed by laparoscopy, which, however, supplies higher flexibility for operative procedures and better visualization of pelvic organs (see the blue box "Laparoscopic Examination of Pelvic Viscera," p. Anesthesia for Childbirth Laparoscopic Examination of Pelvic Viscera Visual examination of the pelvic viscera is especially helpful in diagnosing many circumstances affecting the pelvic viscera, such as ovarian cysts and tumors, endometriosis (the presence of functioning endometrial tissue exterior the uterus), and ectopic pregnancies. Insufflation of inert fuel creates a pneumoperitoneum to present space to visualize, and the pelvis is elevated so that gravity will pull the intestines into the abdomen. The uterus may be externally manipulated to facilitate visualization, or further openings (ports) can be made to introduce other instruments for manipulation or to allow therapeutic procedures. General anesthesia has advantages for emergency procedures and for ladies who select it over regional anesthesia. Clinicians monitor and regulate maternal respiration and each maternal and fetal cardiac perform. Childbirth happens passively underneath the control of maternal hormones with the assistance of an obstetrician. Women who choose regional anesthesia, similar to a spinal, pudendal nerve, or caudal epidural block, often want to take part actively. The anatomical foundation of the administration of a pudendal block is supplied in the blue box "Pudendal and Ilio-inguinal Nerve Blocks," p. The anesthetic agent circulates into the cerebral subarachnoid area in the cranial cavity when the affected person lies flat following the delivery. Pudendal nerve Key Intraperitoneal viscera Subperitoneal viscera Somatic constructions Chapter 3 � Pelvis and Perineum 399 anesthesia bathes the S2�S4 spinal nerve roots, including the ache fibers from the uterine cervix and superior vagina, and the afferent fibers from the pudendal nerve. � Coursing in a peritoneal fold (mesosalpinx) that makes up the superior margin of the broad ligament, every uterine tube has a fimbriated, funnel-like infundibulum, a large ampulla, a slender isthmus, and a short uterine part that traverses the uterine wall to enter the cavity. The ovaries and uterine tubes receive a double (collateral) blood provide from the abdominal aorta by way of the ovarian arteries and from the inner iliac arteries through the uterine arteries. � this collateral circulation allows the ovaries to be spared to provide estrogen when a hysterectomy necessitates ligation of the uterine arteries. Uterus: Shaped like an inverted pear, the uterus is the organ by which the blastocyst (early embryo) implants and develops into a mature embryo after which a fetus. The uterus is normally anteverted and anteflexed so that its weight is borne largely by the urinary bladder, although it additionally receives vital passive support from the cardinal ligaments and energetic support from the muscle tissue of the pelvic flooring. Vagina: the vagina is a musculomembranous passage connecting the uterine cavity to the exterior, allowing the entrance/insertion of the penis, ejaculate, tampons, or examining digits and the exit of a fetus or menstrual fluid.
Diseases
- Leucinosis
- Hutteroth Spranger syndrome
- Christian Demyer Franken syndrome
- Thanatophoric dysplasia cloverleaf skull
- Complement component receptor 1
- Anterograde amnesia
- Pashayan syndrome
Following a Jatene restore gastric spasms 50 mg imuran purchase, the primary pulmonary artery is positioned anterior to the neoaortic root muscle relaxant veterinary imuran 50 mg generic mastercard, with the right and left major pulmonary arteries extending posteriorly "hugging" the neoaorta muscle relaxant soma discount imuran 50 mg visa. The baffle separates the "neo-right atrium" (long thin arrow) muscle spasms 7 little words imuran 50 mg buy cheap on-line, which receive the systemic venous return, from the "neo-left atrium (thick arrow)," which receives the pulmonary venous return. After an arterial swap process, pulmonary arterial stenosis ought to be evaluated. There is stenosis of the left pulmonary artery (arrow), a recognized complication of this process. Quantitative flow assessment of the proper and left pulmonary arteries demonstrated two-thirds of the pulmonary blood circulate supplying the proper lung and one-third supplying the left lung. The neonatal goals of therapy are to hold shunts open to permit mixing between the parallel pulmonary and systemic circuits. This is done medically with prostaglandin, to keep the ductus arteriosus open, or interventionally with a balloon atrioseptostomy, known as the Rashkind procedure, which permits mixing on the atrial stage. However, it is a temporary answer and definitive surgical procedure must be undertaken; the arterial change operation is currently favored. The timing bolus reveals early enhancement of the "neo-left atrial appendage" (arrow) before pulmonary venous enhancement indicating a leak in the superior limb of the baffle. Some of those terms have totally different shades of that means and levels of precision, but they are going to be used interchangeably in this chapter. Key determinants of poor outcomes are tricuspid regurgitation and proper (systemic) ventricular failure. Anatomy and Physiology During the third week of embryonic growth, the guts tube loops, with the cranial end looping ventrally and caudally. In addition to the anatomic concerns, there are also physiological considerations. How to Approach the Image During the neonatal interval and even later, echocardiography generally provides an entire analysis of the cardiac chambers and great arteries. Still, there could also be lack of the aortic knob contour, narrowing of the mediastinum from the pulmonary artery and aorta being superimposed on the frontal projection, and mesocardia or dextrocardia. Common Variants Congenitally corrected transposition might exist in two varieties: S,L,L, the more frequent form, the place the atria are in situs solitus but the ventricles and nice arteries are each inverted, and I,D,D, where the atria are inverted and the ventricles and great arteries are each inverted relative to these inverted atria. Note the parallel course of the pulmonary artery (black arrow) and the aorta (white arrow). Note the crossing pattern of the aorta (white arrow) and the pulmonary artery (dotted black arrow), which crosses posterior to the aircraft of this image. Before attempting surgical repair, coronary artery anatomy should be delineated to prevent catastrophic coronary artery damage. Cardiac venous anatomy, such as absence of the coronary sinus, may happen and be clinically related when making an attempt to insert a pacing lead into an epicardial vein for biventricular pacing. A Mustard/Senning process can be used to reroute blood at the atrial stage, and a Jatene process can be utilized to reroute blood on the degree of the great arteries. The aorta is anterior and to the left of the pulmonary artery, greatest seen on axial images. The nomenclature, definition and classification of discordant atrioventricular connections. Congenitally corrected transposition of the good arteries presenting in a nonagenarian. Congenital Heart Surgery Nomenclature and Database Project: corrected (discordant) transposition of the great arteries (and related malformations). Burns and Hugo Spindola-Franco Definition Ebstein anomaly is congenital displacement of the posterior and septal leaflets of the tricuspid valve towards the best ventricular apex. More than 90% of neonates current with cyanosis secondary to an associated proper to left atrial degree shunt or within the presence of pulmonary valve stenosis or atresia. Older adults with delicate forms of Ebstein anomaly might present with arrhythmias or proper heart failure from long-standing tricuspid insufficiency. Supraventricular tachycardia and Wolff-Parkinson-White syndrome are generally associated with Ebstein anomaly. There is a robust affiliation of Ebstein anomaly with maternal oral lithium therapy throughout pregnancy. Severe displacement of the tricuspid valve leaflets presents early in the neonatal and childhood period, whereas less extreme displacement could be tolerated into adulthood. Neonates with extreme Ebstein anomaly and an related right-to-left atrial degree shunt usually current on the first day of life with cyanosis and a tricuspid insufficiency murmur. Older youngsters or young adults could current with Anatomy and Physiology the traditional tricuspid valve has three leaflets: septal, anterior, and posterior. The anterior portion of the septal leaflet inserts into the membranous septum, whereas the mid and posterior parts insert into the muscular septum. In Ebstein anomaly (b), the septal leaflet of the tricuspid valve is displaced toward the right ventricular apex. There is atrialization of a half of the best ventricle (white asterisk) with abnormal thinning of the affected portion of the septal wall. The black asterisk is within the remaining functional portion of the right ventricle distal to the insertions of the leaflet. The presence of noncompaction of the left ventricular apex and adjoining lateral wall is incidentally noted. For this reason, the anterior tricuspid valve leaflet is usually described as "sail-like. The vast majority of patients with Ebstein anomaly could have tricuspid insufficiency. Rarely, redundancy of the anterior leaflet might trigger obstruction of the right ventricular outflow tract during systole, whereas an imperforate valve leads to tricuspid atresia. Displacement of the posterior and septal tricuspid leaflets towards the best ventricular apex also ends in atrialization of part of the proper ventricle. In different phrases, the portion of the proper ventricle proximal to the irregular attachments of the tricuspid valve adapts to function as part of the best atrium. Consequently, the remainder of the practical right ventricle distal to the tricuspid valve has decreased pumping capability. The native right atrium and the atrialized right ventricle are dilated and thin-walled. With elevated proper coronary heart pressures, a generally associated secundum atrial septal defect or patent foramen ovale will result in right-to-left atrial shunting and variable levels of cyanosis. Pulmonary stenosis or atresia may also be related to Ebstein anomaly, additional impeding pulmonary blood circulate and worsening the degree of cyanosis. In the overwhelming majority of circumstances, there might be an associated secundum atrial septal defect or a patent foramen ovale. In contrast, in Ebstein anomaly, the tricuspid valve is rotated relative to the short-axis airplane. What Not to Miss Atrial septal defect or patent foramen ovale Pulmonary stenosis or atresia Additional cardiovascular anomalies, together with ventricular septal defect, patent ductus arteriosus, endocardial cushion defect, mitral valve abnormalities. The main pulmonary artery and aortic arch are inconspicuous, leading to a relatively narrow-appearing vascular pedicle. Pulmonary vascularity is usually decreased secondary to right-to-left atrial shunting but can be normal. If present, it signifies the current of a left-to-right shunt typically because of ventricular septal defect or patent ductus arteriosus. The most attribute findings of Ebstein anomaly are displacement of the posterior and septal tricuspid valve leaflets into the best ventricular cavity, leading to an atrialized, thin-walled Differential Diagnosis Tricuspid insufficiency: Congenital tricuspid valve dysplasia (rare, but consider in children) Acquired causes are more widespread in adults Secondary from tricuspid valve annular dilatation (most common) Right coronary heart failure (any cause) Pulmonary hypertension Primary tricuspid abnormality Rheumatic tricuspid valve illness (usually associated with mitral valve disease) Endocarditis Chest trauma with ruptured chordae tendinae or papillary muscle tissue Carcinoid heart disease Common Variants No universal classification system is used for Ebstein anomaly. Chest radiographs (a, b) and right ventriculogram (c) of an adolescent boy with fatigue on exertion and paroxysmal supraventricular tachycardia. The frontal chest radiograph (a) demonstrates the basic box-like configuration of the cardiac silhouette in Ebstein anomaly. There is severe cardiomegaly with squaring of the decrease section of the best coronary heart border (right atrium), a convex left coronary heart border (dilated outflow tract of the right ventricle), and a slender vascular pedicle. On the lateral chest radiograph (b), the proper atrium varieties the anterior and posterior coronary heart borders.