
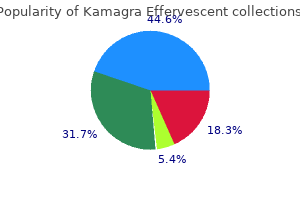
Kamagra Effervescent
| Contato
Página Inicial

"Kamagra effervescent 100 mg discount amex, erectile dysfunction pills at gnc".
Z. Gonzales, M.A., M.D., M.P.H.
Clinical Director, Medical University of South Carolina College of Medicine
These outcomes instructed that a correction of the biochemical defect in adrenoleukodystrophy might be attainable by drug-induced overexpression or ectopic expression of the adrenoleukodystrophy-related gene erectile dysfunction from diabetes treatment for 100 mg kamagra effervescent cheap overnight delivery. Nonsense and frame-shift mutations in addition to massive deletions result in erectile dysfunction louisville ky kamagra effervescent 100 mg purchase with visa a truncated protein doctor for erectile dysfunction in dubai cheap kamagra effervescent 100 mg mastercard. Many missense mutations end in unstable protein whose detection is likely to impotence biking purchase kamagra effervescent 100 mg without prescription be dependent on the specificity and sensitivity of the method used. Epidemiology Screening and diagnostic data recommend that the prevalence is a minimum of 1 in 22 500 to 1 in 62 000. In contrast, the use of the Hardy�Weinberg strategy and genetic frequency information suggests a combined male to feminine frequency of 1 in 18 000 much like phenylketonuria (1 in 12 000). Differential analysis the differential diagnosis of neuropsychiatric abnormalities is shown in Table 12. Similarly, C26:zero accumulates in white matter phosphatidylcholine phospholipids, C24:zero and C24:1 in gangliosides. The diagnostic take a look at depends on measurement of C26:0 ranges and the ratios of C26 to C22:0 (docosahexaenoic acid) and C26:0 to C24:0 (tetracosanoic acid). Results can be confirmed by fibroblast research or by method of sequencing strategies. The N-terminal 73 amino acids and the C-terminal 50 amino acids are largely spared, therefore caution is warranted when interpreting sequencing information suggesting missense mutations outdoors these key regions. The genetic panorama of X-linked adrenoleukodystrophy: inheritance, mutations, modifier genes, and analysis. Prenatal diagnosis is feasible from cultured amniocytes or chorionic villus cells. Eighty per cent of childhood cerebral adrenoleukodystrophy sufferers have symmetric periventricular white matter adjustments within the posterior parietal and occipital lobes with a dorsocaudal development with time. Contrast studies show up areas of active demyelination, inflammation with breakdown of the blood�brain barrier, and gliosis. In childhood illness, 80% present abnormal adrenal stimulation check outcomes, whereas in adrenomyeloneuropathy, between 30 and 50% show regular responses. Levels of follicle-stimulating hormone or luteinizing hormone are elevated in 50 to 70% of sufferers with adrenomyeloneuropathy, while testosterone levels are decreased in 20% with low normal ranges of dehydroepiandrosterone sulphate. Neurophysiology Hearing is regular but brainstem auditory evoked potentials are abnormal in 95% of adrenomyeloneuropathy patients and 42% of heterozygote patients. Abnormalities in visual evoked potentials are additionally found as latencies and are increased in 20% of men with adrenomyeloneuropathy however in more than 70% with childhood cerebral disease. Subtle demyelination and axonal loss patterns of nerve conduction are present in 90% of males and 67% of ladies with adrenomyeloneuropathy, usually affecting the legs greater than the arms. Neuropsychological exams can show up deficits in parieto-occipital perform affecting visuospatial parameters and auditory processing, whereas frontal lobe lesions affect govt functions, emotions, problem fixing, and anticipatory processing. Leukodystrophies are associated with progressive studying difficulties, psychiatric disturbance, and increasing incapacity. Painful muscle spasms are common and ought to be managed with diazepam, baclofen, or gabapentin. Bulbar muscle function could also be lost with disease progression, thus requiring particular attention to feeding to scale back the chance of aspiration pneumonia. Endocrine assessment is carried out at baseline and repeated if the scientific syndrome consists of features of hypoadrenalism. The fatty acid composition of the plasma and liver, but not that of the brain, improves with this remedy, suggesting that. The enhance in frontal exercise correlated with scores from psychological evaluations. Proton spectroscopy utilizing N-acetyl aspartate shows up neuronal loss, whereas choline compound studies assaying phosphocholine and glycerophosphocholine point out membrane turnover and demyelination, and myo-inositol compounds seem to be indices of gliosis. The presence of lactate indicates the anaerobic metabolism of the inflammatory cell infiltrate. Demyelination concerned parietal�occipital lobes in 90%, resulting in visual and auditory processing deficits in many boys. There are few knowledge on the usefulness of bone marrow transplantation in adrenomyeloneuropathy. Adrenal operate should be monitored since 80% of asymptomatic patients with adrenoleukodystrophy develop evidence of adrenal insufficiency and adrenal hormone alternative remedy ought to be offered when indicated by laboratory findings. Studies of cyclophosphamide, immunoglobulin, and interferon- have been unsuccessful. In mice, a sterol regulatory factor exists in the Abcd2 promoter and overlaps sites for liver X receptor/retinoid X receptor heterodimers. Hepatic Abcd2 expression in liver X receptor-/ mice is inducible to levels vastly exceeding wild type. They block the induction of proinflammatory cytokines by way of effects on rho kinase. A combination of the antioxidants tocopherol, N-acetyl-cysteine, and -lipoic acid reduced demyelination in Abcd1-deficient mice. There has been an explosion of curiosity in novel therapeutic methods for inherited errors of metabolism. Neuro-ophthalmic adult peroxisomal problems Introduction Though survival is improving for peroxisomal biogenesis disorders and extra refined defects are now identified, most still present in the neonatal period or in infancy. In distinction to the neuropsychiatric or endocrine presentation associated with adrenoleukodystrophy, these peroxisomal issues present as central and peripheral neuropathies-a neuroophthalmic image. Eventually, the novel defect was recognized as a variant of rhizomelic chondrodysplasia punctata type 1 and attributable to mutations in peroxin 7. In contrast to other Refsum-like syndromes, phytanic acid ranges are normal in this condition. After 10 to 15 years, deafness, ataxia, polyneuropathy, ichthyosis, and cardiac arrhythmias can happen. Other options described have included major hypogonadism, hypothyroidism, spastic paraparesis, epileptic seizures, and mild developmental delay. More severe childhood-onset instances have proven a phenotype of defects in bile acid synthesis allied with fat-soluble vitamin deficiencies, coagulopathy, and cholestatic liver illness and a resemblance to a Niemann�Pick kind C phenotype. It was first described in 1947, but only acknowledged as a syndrome by Refsum in 1962. He described a constellation of indicators comprised of retinitis pigmentosa, anosmia, deafness, ataxia, and polyneuropathy allied with raised ranges of protein in the cerebrospinal fluid. This illness was thought to be unifactorial with admittedly some rare aberrant complementation studies until 1995 when, after the localization of the gene for phytanoyl-CoA hydroxylase, as much as Table 12. Age >30 Axonal/ demyelinating Variable Yes <200 >10 Age >30 Age >5 Absent Age >5 Age >30 Variable progressive Progressive No Normal (<10) Normal (0. Instead, phytanic acid is metabolized both by -oxidation to pristanic acid, or by -oxidation from the other end of the molecule. Using radiolabelled [14C]-phytanic acid as a substrate, an enzyme exercise liable for the -oxidation of phytanic acid in cell lysates was described in 1967. This activity was eventually localized within peroxisomes and, after 30 years, the pathway answerable for -oxidation has been clarified. Unusually, it appears this pathway can metabolize two stereoisomers of its substrate equally well. One carbon atom is then faraway from the latter in a lyase response to give pristanal and formyl-CoA. Pristanal is then oxidized to pristanic acid which is thio-esterified using CoA to give a racemic combination. The action of -methylacylCoA racemase converts the (2R)-epimer to the (2S)-epimer. Further degradation of (2S)-pristanic acid by the stereospecific -oxidation pathway then occurs, with the release of propionyl and acetyl-CoA units. Further -oxidation reactions (including epimerization) are required to generate the dimethylundecanoic and dimethylnonanoic and methyl-heptanoic acid derivatives, that are lastly exported for mitochondrial -oxidation. This pathway produces 3-methyladipic acid as the ultimate metabolite, which is excreted in the urine.

Somatostatin receptor imaging is the most sensitive imaging modality for pancreatic neuroendocrine tumours (80�90%) erectile dysfunction pills herbal kamagra effervescent 100 mg cheap amex. In instances of nonfunctioning pancreatic neuroendocrine tumours presenting as otherwise undifferentiated pancreatic lots erectile dysfunction premature ejaculation treatment cheap kamagra effervescent 100 mg without a prescription, somatostatin receptor imaging is useful in differentiating these from pancreatic adenocarcinomas erectile dysfunction funny images kamagra effervescent 100 mg with visa. Traditionally erectile dysfunction venous leak treatment kamagra effervescent 100 mg discount online, somatostatin receptor imaging has utilized indium-111 octreotide (111In-octreotide), with more than 80% (a) (b). This is important, since 40% of gastrinomas and insulinomas are microadenomas (<1 cm). Visualization of a tumour blush on angiography previous to calcium stimulation additional increases the sensitivity of this investigation. Furthermore, since the hepatic artery is cannulated on the end of the procedure, the presence of microscopic hepatic metastases can also be detected by measuring rises in hormone levels after secretagogue injection into the hepatic artery. Natural historical past the spontaneous course of illness in pancreatic neuroendocrine tumours is tough to verify because of their low incidence, heterogeneous behaviour, and a relative absence of controlled potential scientific trials to assess the efficacy of different therapeutic methods. Those tumours that secrete functionally energetic peptides current early with smaller tumours, morbidity and mortality resulting from the results of peptide hypersecretion rather than tumour bulk. Nonfunctioning pancreatic neuroendocrine tumours are sometimes more superior at prognosis due to the absence of signs attributable to hormone hypersecretion. Poorly differentiated, giant (>3 cm) tumours associated with metastases are indicators of a poor prognosis. Metastatic unfold to liver (in 42% of sufferers at presentation) and bone (in 8% of sufferers at presentation) is the main cause of demise in sufferers with pancreatic neuroendocrine tumours. The general 5year survival for pancreatic neuroendocrine tumours is 50 to 80%, with insulinomas and gastrinomas having as a lot as 94% 5-year survival, primarily as a result of their apparent medical displays prompt early surgical intervention. This operates on the principle of instilling a secretagogue into the primary pancreatic arteries (gastroduodenal, superior mesenteric, inferior pancreaticoduodenal, and splenic) and measuring the secretion of hormonal markers such as insulin and gastrin in the effluent from the hepatic vein. Calcium (chloride or gluconate) is the secretagogue of alternative, having replaced secretin for this objective. Injection of calcium into the artery supplying the tumour causes a marked rise in hormone levels in the hepatic vein, and therefore permits equivocal lesions to be verified, significantly within the presence of multiple pancreatic Specific tumour syndromes Insulinomas Insulinomas are essentially the most frequent useful pancreatic neuroendocrine tumours and are discussed in Chapter 13. Gastrinoma the gastrinoma syndrome was first described in 1955 by Zollinger and Ellison, who reported the triad of fulminating ulcer diathesis, recurrent ulceration with a poor response to remedy, and pancreatic non-cell islet tumours. The syndrome, also called Zollinger� Ellison syndrome, is the results of extra gastrin-stimulated gastric acid secretion. This causes severe, a quantity of peptic ulcers, that are normally duodenal, however may happen in the oesophagus and jejunum, and are sometimes related to problems such as gastric rugal hypertrophy, haemorrhage, perforation, and stricture formation. The excess gastric acid secretion inactivates pancreatic enzymes and damages the intestinal mucosa, leading to diarrhoea and steatorrhoea, which may be prominent features that precede symptoms of peptic ulcer illness. Overall, gastrinomas are the second most frequent functionally energetic pancreatic neuroendocrine tumour. Those arising in the duodenum (50�88%) are frequently a quantity of, comparatively small, and subsequently troublesome to localize. Those gastrinomas arising in the pancreas are most regularly situated in the pancreatic head. The analysis of the gastrinoma syndrome requires the demonstration of a raised fasting plasma gastrin focus (>40 pmol/litre), associated with increased basal gastric acid secretion. However, patients with true gastrinomas could additionally be vulnerable to peptic ulcer perforation if antacids are stopped for plasma gastrin measurements. It is due to this fact often necessary to wean patients off antacids, for example by switching proton pump inhibitors to H2blockers for two weeks earlier than switching the H2-blockers to high-dose calcium/magnesium-based antacids for three days, previous to gastrin sampling. Hypergastrinaemia and raised acid output can also come up from other causes (Table 13. The intravenous secretin test (2 U/kg physique weight) distinguishes these situations from gastrinoma and may help analysis when other investigations are equivocal. In distinction, secretin provokes a paradoxical rise in serum gastrin of at least one hundred twenty pg/ml in sufferers with gastrinoma. Alternatively, an intravenous calcium infusion can be utilized diagnostically, with an increase in plasma gastrin noticed in gastrinoma patients. Since ingestion of meals is a stimulus for gastrin secretion from the antral and duodenal mucosa, it has been proposed that a normal take a look at meal may differentiate hypergastrinaemia of antral and tumoural origin. Endoscopy could additionally be priceless in demonstrating oesophageal and duodenal ulceration and hypertrophy of the gastric mucosa. Localization of microgastrinomas could also be aided preoperatively by endoscopic ultrasound, somatostatin receptor imaging, or selective visceral angiography and venous sampling. Survival depends on the presence of hepatic metastases at presentation, which is more generally seen with pancreatic rather than duodenal gastrinomas. Largevolume diarrhoea with out steatorrhoea is the cardinal symptom, with most patients excreting greater than 3 litres per day. The lack of bicarbonate in the stool leads to a paradoxical acidosis, which can mask the true potassium deficit. Achlorhydria or hypochlorhydria happens in more than 50% of patients and distinguishes this diarrhoeal syndrome from that associated with gastrinoma. Pancreatic polypeptide concentrations levels are elevated in 75% of circumstances and neurotensin in 10%. Occasionally, selective visceral angiography and venous sampling may be essential to detect small pancreatic lesions. Glucagonoma Glucagonomas are rare -cell tumours of the pancreas which secrete varied types of glucagon and other peptides derived from the preproglucagon molecule. Primary glucagonomas mostly come up within the pancreatic tail and extrapancreatic glucagonomas are rare. Smaller glucagonomas are most likely to be benign and elevated tumour measurement correlates with danger of malignancy. Common presenting options of glucagonoma syndrome are weight reduction, diarrhoea, anorexia, and belly discomfort, with the latter usually reflecting tumour bulk from hepatomegaly. Mucous membranes are additionally affected, resulting in angular chelitis, stomatitis, glossitis, and blepharitis. The precise pathogenesis of this unusual pores and skin eruption stays unclear and is more probably to be multifactorial. Hypoaminoacidaemia, zinc deficiency, hypovitaminosis B, and hepatic dysfunction have all been implicated. Diabetes mellitus is current in roughly two-thirds of those with the glucagonoma syndrome and this will likely predate necrolytic migratory erythema. Neurological and psychiatric signs may also be a presenting feature, together with ataxia, dementia, optic atrophy, and proximal muscle weak spot. The diagnosis of glucagonoma is made on the premise of an elevated fasting plasma glucagon (>50 pmol/litre), in association with characteristic scientific features and a demonstrable neuroendocrine tumour and/or metastatic deposits. Endoscopic ultrasonography could additionally be of restricted use in glucagonomas, as these are often positioned within the pancreatic tail. Glucagonomas and their metastases are commonly hypervascular, making selective visceral angiography and venous sampling notably helpful in localizing the tumour and figuring out small hepatic metastases. Although most patients with glucagonoma syndrome current with proof of metastases, the slow-growing nature of those tumours can outcome in a relatively good prognosis. Somatostatinoma Somatostatinomas are extremely rare, with an estimated annual incidence of about 1 in 40 million per yr. Fifty per cent of those tumours are pancreatic, the remainder arising in the duodenum. Pancreatic somatostatinomas are usually massive, greater than 2 cm at prognosis, and thus present with local signs, biliary obstruction, or features relating to excess somatostatin secretion. Somatostatin has pan-inhibitory effects on intestine motility, transit and absorption, gallbladder contraction and secretion, and endocrine and exocrine pancreatic functions. The so-called somatostatin syndrome ensuing from somatostatin hypersecretion due to this fact consists of steatorrhoea (due to inhibition of pancreatic exocrine function), cholelithiasis (due to discount of cholecystokinin secretion and inhibition of gallbladder contraction), hyperglycaemia (due to suppression of insulin secretion), and hypochlorhydria (due to suppression of gastrin secretion). Hypoglycaemia has often been described, probably because of bigger molecular types of somatostatin having a higher inhibitory impact on counterregulatory hormones such as glucagon than on insulin. Duodenal somatostatinomas usually current with obstructive jaundice, pancreatitis, intestinal obstruction, or gastrointestinal haemorrhage.
These molecules are inclined to erectile dysfunction vacuum pump india buy kamagra effervescent 100 mg overnight delivery be massive (150 erectile dysfunction 35 generic 100 mg kamagra effervescent fast delivery,000 to 1 erectile dysfunction at the age of 21 generic 100 mg kamagra effervescent amex,000 erectile dysfunction drugs over the counter uk 100 mg kamagra effervescent generic with amex,000 kd) multimeric and multidomain proteins, with long arms that bind other matrix molecules and assist or modulate cell attachment. They assist to (1) organize tissue topography, (2) help cell migration, (3) orient cells and (4) induce cell conduct. In remodeling, the equilibrium between collagen deposition and degradation is restored. Matrix metalloproteinases are the primary reworking enzymes, although neutrophil protease and serine proteases are also current. They allow cells to migrate via the stroma by degrading matrix proteins at the web site of injury, thereby allowing reorganization of the tissue. In the later phases of the repair course of, inflammatory cells diminish in quantity, and capillary formation is completed. Remodeling of the site of harm into a mechanically strong, mature scar signifies that the stability between collagen deposition and degradation has been restored. For instance, in recovery from a moderate sunburn, small numbers of acute inflammatory cells briefly accompany transient vasodilation beneath the solar-injured dermis. By distinction, sustained acute irritation, with emergence of macrophage-predominant irritation, is a precursor to the sequence of collagen elaboration and restore related to scar formation and fibrosis. Cells of granulation tissue accumulate from labile cell populations, together with circulating leukocytes and basal epithelial cells, and from steady cells, similar to capillary endothelia and resident mesenchymal cells (fibroblasts, myofibroblasts, pericytes and smooth muscle cells). Local and marrow-derived stem cells or committed progenitor cells may also populate wounds, the place they differentiate into endothelial and fibroblast populations. Although tougher to study, therapeutic within hollow viscera and physique cavities usually parallels the repair sequence in pores and skin. Hemostasis A thrombus (clot) is shaped at the site of injury primarily by the conversion of plasma fibrinogen to fibrin. The thrombus additionally contains contracting platelets, an initial source of development components. In the skin, a scab or eschar results from the drying of the uncovered floor of the clot and varieties a barrier to invading microorganisms. For example, the surgical excision of a minor skin lesion leaves little or no devitalized tissue. By distinction, widespread, irregularly defined necrosis is a characteristic of a large third-degree burn. Initially, an acute, neutrophil-dominated, inflammatory response liquefies the necrotic tissue. Plasma-derived fibronectin binds to collagen and cell membranes to facilitate phagocytosis. Fibronectin and mobile debris are chemotactic for macrophages and fibroblasts The look of macrophages as the predominant cell at the website of injury alerts the onset of the restore course of. Macrophages ingest proteolytic products of neutrophils and secrete collagenase, thereby selling further liquefaction. They additionally present development factors that stimulate fibroblast proliferation, collagen secretion and neovascularization. These collagen-secreting cells are concerned in inflammatory, proliferative and remodeling phases of wound repair Fibroblasts are able to further differentiation to contractile cells termed myofibroblasts. Transient acute inflammation could resolve fully, with domestically injured parenchymal elements being regenerated without significant Granulation Tissue Granulation tissue is the transient, specialised tissue of restore that replaces the provisional matrix. Microscopically, a mix of fibroblasts and red blood cells first seems, adopted by the event of provisional matrix and patent capillaries, that are surrounded by fibroblasts and inflammatory cells. A key step in the development of granulation tissue is the recruitment of monocytes to the positioning of injury by chemokines and fragments of broken matrix. Activated macrophages coordinate the event of granulation tissue through the discharge of growth components and cytokines, which (1) direct angiogenesis (see below), (2) activate fibroblasts to kind new stroma and (3) proceed the degradation and removal of the provisional matrix Granulation tissue is fluid-laden, and its mobile constituents provide antibacterial antibodies and growth elements. It is very proof against bacterial an infection, allowing the surgeon to create anastomoses at such nonsterile websites because the colon. Growth issue alerts first arise from platelets, however activated macrophages, resident tissue cells and the matrix itself release a fancy interplay of interacting signals. Capillary blood vessels proliferate, and the epidermal keratinocytes penetrate alongside the granulation tissue below the thrombus. Fibronectin, development components, chemokines, cell debris and bacterial merchandise are chemoattractants for a big selection of cells which would possibly be recruited to the wound site (2 to 4 days). This cross-linking provides a provisional mechanical stabilization of the wound (0 to 4 hours). Integrin receptors act to type polymers of fibronectin, and integrins and fibronectin assist form collagen fibrils. The infiltrating capillaries penetrate a free connective tissue matrix containing mesenchymal cells and occasional inflammatory cells. At its peak, granulation tissue is the most richly vascularized tissue within the body. Once restore has been achieved, many of the newly formed capillaries are reabsorbed, leaving a pale, avascular scar rich in collagen. The release of cytokines by fixed cells in the damaged tissue causes hemorrhage and attracts inflammatory cells to the positioning. About 2 to three days after damage, activated fibroblasts and capillary sprouts are detected. The form of fibroblasts within the wound changes from oval to bipolar, as they start to type collagen and synthesize different matrix proteins Extracellular cross-linking of newly synthesized collagen progressively will increase wound strength. Diminishing anoxia as repair progresses could additionally be key to the arrest of the repair course of. Granulation tissue finally transitions to scar tissue, because the stability between collagen synthesis and collagen breakdown begins inside weeks of damage. Fibroblasts stay active at the wound site, thereby increasing the density of the scar over several years. Tissue regeneration is also driven by signaling networks, which, in cooperation with matrix, help self-renewal, maintenance and differentiation of stem cells. Angiogenesis the Growth of Capillaries At its peak, granulation tissue has extra capillaries per unit volume than another tissue, accounting for the supply of oxygen and vitamins to the cells. Less usually, new blood vessels form de novo from angioblasts (endothelial progenitor cells) by a course of generally identified as vasculogenesis, which is primarily associated with developmental processes. Quiescent capillary endothelial cells are activated by the local release of cytokines and growth components. The endothelial cells and pericytes are bordered by basement membranes, which should be domestically degraded before these cells migrate into the provisional matrix. The growth of new capillaries is supported by the proliferation and fusion of endothelial cells Endothelial progenitor cells which are derived from the bone marrow may be transiently recruited to assist the growing vessel. Migration of cells into the wound site is directed by soluble ligands (chemotaxis) and proceeds alongside adhesive matrix substrates (haptotaxis). These cells, with options intermediate between those of smooth muscle cells and fibroblasts, are characterized by the presence of discrete bundles of myofilaments within the cytoplasm (arrows). The layer of actin that encircles the epithelial cytoplasm creates lateral rigidity and strength and is referred to because the adhesion belt. The shape and the energy of related epithelial sheets result from pressure created by cytoskeletal connections to basement membrane and cell-tocell bonds. Cellular migration is the predominant means by which the wound surface is re-epithelialized. Migrating epidermal cells originate at the margin of the wound, hair follicles and sweat glands. If the basement membrane is lost, cells come in contact with unfamiliar stromal or provisional matrix elements, an impact that stimulates cell locomotion and proteinase expression. Activation of epithelial motility is pushed by the meeting of actin fibers at focal adhesions organized by an integrin receptor, directing the migrating cells alongside the margin of viable dermis. Movement through cross-linked fibrin apposed to the dermis also requires the activation of plasmin from plasminogen to degrade fibrin. Migrating keratinocytes finally resume their normal phenotype after re-forming a confluent layer and attaching to their newly formed basement membranes. Integrins and Angiogenesis Surface integrin receptors sense changes in extracellular matrix and might react by modulating cellular responses to growth factors.
A homozygous defect within the oestrogen receptor in a male led to failure of epiphyseal closure leading to tall stature along with severe osteoporosis impotence and age buy 100 mg kamagra effervescent mastercard. These manifestations recommend that testosterone effects on the male skeleton are causes of erectile dysfunction in youth 100 mg kamagra effervescent generic overnight delivery, in part erectile dysfunction pump amazon 100 mg kamagra effervescent proven, mediated by its enzymatic conversion to oestrogens erectile dysfunction hernia cheap kamagra effervescent 100 mg on line. A growing number of issues associated with defects in transmembrane receptors or their signalling intermediates have been described (Table thirteen. However, in addition to mutations which disrupt protein operate, gain-of-function mutations inflicting constitutive activation of the receptor or signalling protein additionally happen. Constitutive activation of sign transduction can also outcome from G protein mutations. Their secretion is regulated by hypothalamic-releasing and inhibitory components delivered via portal capillaries, and by adverse suggestions inhibition of the cognate hormones produced by goal endocrine glands such as the thyroid and adrenal cortex. Management-the availability of delicate hormonal assays, alternative hormones, and hypothalamic peptides, along with refined neuroimaging strategies and neurosurgical methods, has increased our capability to identify exactly and successfully deal with most sufferers with illnesses of the anterior pituitary gland. Management choices include: (1) surgery-with trans- sphenoidal surgical procedure the remedy of alternative for many sufferers; (2) drugs- together with dopamine receptor agonists, somatostatin receptor ligands Prolactin Prolactinomas are the most common pituitary adenomas and usually present with galactorrhoea and hypogonadism, manifesting in men as impotence, infertility, and decreased libido, and in women as oligo/amenorrhoea and infertility. Secondary causes of hyperprolactinaemia should be excluded in any patient with an elevated serum prolactin and serum prolactin levels normally parallel tumour dimension in those with prolactinomas. First-line treatment usually comprises surgery with or with out adjuvant exterior beam irradiation. Hypophysitis-may be main (granulomatous, xanthomatous or lymphocytic) or caused by a known agent or systemic disease. Optimal remedy for the inflammatory course of has not been established and replacement of defective endocrine function is required. Since the demonstration of the hypothalamic control of pituitary operate by Harris in Oxford in the 1950s, our understanding of the physiology and pathophysiology of the pituitary gland has broadened. The improvement of radioimmunoassays in the Sixties, the extraction of hypothalamic components principally by Schally and Guillemin in the Nineteen Seventies, the advances in immunocytochemistry, electron microscopy, and in situ hybridization strategies, as nicely as the growth of molecular biology have increased this understanding. Finally, the advances in fashionable imaging strategies and in pituitary surgical procedure combined with the development of medical remedies for pituitary tumours have tremendously expanded the therapeutic potentialities, providing successful and protected outcomes in most sufferers. Glucocorticoid deficiency may be life-threatening and hence alternative with hydrocortisone (or different steroid) in a dose and timing to mimic the traditional pattern of cortisol secretion ought to start as quickly as the prognosis is confirmed. Anatomy and embryology the pituitary gland consists of the anterior lobe (adenohypophysis), the posterior lobe (neurohypophysis), and an intermediate zone. A remnant of the pharyngeal hypophysis could additionally be found in adults, forming the pharyngeal pituitary situated within the midline of the nasopharynx. The posterior lobe originates from the neural primordium as an outpouching from the ground of the third ventricle on the fourth week of gestation. The portal system begins developing at the seventh week and is accomplished at around the 20th week of gestation. The body of the sphenoid bone and the sella turcica come up from the fusion of hypophyseal cartilage plates on either facet of the creating pituitary. The sella is nicely formed by the seventh week and matures by endochondral ossification. The pituitary measures around 13 mm transversely, 9 mm anteroposteriorly, and 6 mm vertically. It increases throughout pregnancy to virtually twice its regular measurement, and decreases in older individuals. The gland is centrally located on the base of the mind within the sella turcica inside the sphenoid bone. It is connected to the hypothalamus by the pituitary stalk and a fantastic vascular network. Clinical manifestations depend primarily on the underlying disease, in addition to the sort and the diploma of the hormonal deficits. Pituitary adenomas-the most typical cause of pituitary illness; may be functioning (resulting in syndromes of hormonal excess) or nonfunctioning (presenting with mass effects). Treatment includes surgical procedure, radiotherapy, or medical remedy as described earlier. Pituitary apoplexy-occurs primarily in sufferers with pre-existing pituitary adenomas; outcomes from acute haemorrhage or infarction of the pituitary gland and is characterised by sudden onset of headache, vomiting, visual disturbance, ophthalmoplegia, and altered consciousness. Initial management requires shut monitoring of fluid and electrolyte steadiness and quick substitute of poor hormones, especially corticosteroids. The optic chiasm is positioned superiorly and is separated from the pituitary by the suprasellar cistern and the sellar diaphragm. The anterior lobe includes nearly 80% of the gland and consists of the pars distalis, pars intermedia, and pars tuberalis. On gentle microscopy the cells of the anterior lobe present variation in size, form, and histochemical staining features. They are organized in nests and cords, and are separated by a complex capillary network. The pars intermedia is poorly developed in humans and lies between the pars distalis and the posterior pituitary. The pars tuberalis is an extension of the anterior lobe along the pituitary stalk. It is fashioned by regular acini of pituitary cells distributed around surface portal vessels. The anterior pituitary receives most of its blood supply from the hypothalamo-hypophyseal portal system (primary plexus, lengthy portal venous system, and secondary plexus), which originates from the capillary plexus of the median eminence and superior stalk derived from the terminal ramifications of the superior and inferior hypophyseal arteries. The venous drainage from the anterior pituitary is thru the cavernous sinuses into the petrosal sinuses and the internal jugular veins. The anterior lobe has no direct innervation, apart from a number of sympathetic nerve fibres spreading to the anterior lobe alongside blood vessels. The hypothalamic regulation is exerted through the neurohormonal link with the hypothalamic regulatory peptides reaching the pituitary through the portal vessels. Finally, the anterior pituitary synthesizes several peptides, development factors, and cytokines that play an essential half in autocrine and/or paracrine control of pituitary secretion and/or cell proliferation. Clinical options of pituitary illness the scientific features of pituitary disease, largely associated with a space-occupying lesion, could result from local mass effects and/or pituitary hormone deficits or hypersecretion. The native mass effects depend upon the scale of the tumour and its anatomical place. It can be variable (occipital, retro-orbital, bitemporal) and is commonly nonspecific. The neuro-ophthalmological effects embrace visual subject defects (usually bitemporal hemianopia or upper temporal quadrantanopia or any unilateral or bilateral visual subject defect) from compression of the optic chiasm. Compression of the primary or second branch of the trigeminal nerve could hardly ever lead to facial ache. Very giant pituitary tumours obstructing the fourth ventricle or the foramen of Monro cause hydrocephalus and enlargement of the lateral ventricles. Inferior invasion and erosion of the sellar flooring could end in recurrent sinusitis, cerebrovascular fluid rhinorrhoea, and recurrent meningitis. Extension into the temporal lobe could hardly ever be related to temporal lobe epilepsy and to the cerebral peduncles with motor and/or sensory disturbances. Superior enlargement to the hypothalamus could also be related to hypothalamic dysfunction General physiology the secretion of the anterior pituitary hormones is underneath elegant regulation exerted by hypothalamic peptides and, with the exception of prolactin, by the unfavorable suggestions (at both the hypothalamic and pituitary level) of hormones from the target glands. The hypothalamic peptides are secreted in the median eminence and are transferred to the anterior pituitary gland by way of the hypothalamic� pituitary portal system. They combine environmental and neural data and bind to particular excessive affinity cell membrane receptors of the actual pituitary cell type. Failure of the target gland results in decreased adverse suggestions and increased hypothalamic and pituitary secretion. Primary overactivity of the goal gland ends in increased adverse suggestions and decreased hypothalamic and pituitary secretion. The secretion of these hormones is regulated by hypothalamicreleasing and hypothalamic-inhibiting factors and by negative feedback inhibition of their peripheral hormones. However, any degree of unilateral or bilateral visible deficit can happen depending on the anatomical web site of the lesion.