
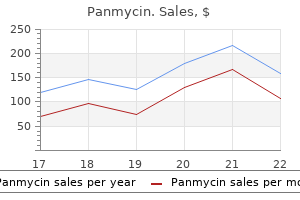
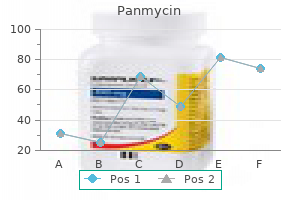
Panmycin
| Contato
Página Inicial

"Order panmycin 500 mg otc, antibiotic ear drops".
C. Torn, M.A., Ph.D.
Co-Director, Idaho College of Osteopathic Medicine
However hpv virus 500 mg panmycin discount mastercard, as a outcome of mitotic figures are uncommon and no invasive growth is current bacteria 3d model 500 mg panmycin cheap with visa, a designation of "atypical pleomorphic adenoma" is acceptable infection behind the eye purchase panmycin 250 mg fast delivery. The epithelial element is most frequently a squamous cell carcinoma or adenocarcinoma antibiotics linked to type 2 diabetes buy discount panmycin 500 mg on-line, and the most common malignant mesenchymal element is chondrosarcoma, followed by fibrosarcoma, leiomyosarcoma, osteosarcoma, liposarcoma, and rhabdomyosarcoma. The carcinomatous element contains cohesive polygonal cells (right decrease field), and the sarcomatous component includes loosely dispersed spindle to stellate cells. A, the tumor is surrounded by a fibrous capsule without evidence of invasion, as is attribute of adenoma. This exhibits the prototypic structure of basal cell adenoma-interconnected jigsaw puzzle�like islands of basaloid cells. B, Typical jigsaw puzzle�like islands of basaloid cells, interspersed by occasional vacuolar or small cystic areas. Some true glandular lumens lined by cells with eosinophilic cytoplasm are also seen. In contrast to pleomorphic adenoma, the cell islands are sharply demarcated from the stroma. This case additionally shows spindle cells within the stroma in the left field, according to myoepithelium-derived stroma. This tumor is distinguished from pleomorphic adenoma by the sharp demarcation of the basaloid islands from the stroma, without transition to the spindle cells. In our experience, focal myoepitheliumderived stroma (S100+) is in fact a very common and attribute finding in basal cell adenoma, and its presence may assist within the distinction from adenoid cystic carcinoma. Interspersed small glandular lumens lined by cells with eosinophilic cytoplasm are current. Because membranous basal cell adenoma generally grows in a multinodular style with entrapment of regular salivary gland tissue, it could be misinterpreted as a malignant tumor. Membranous basal cell adenoma (also known as dermal analogue tumor) is histologically identical to dermal cylindroma. Familial instances accompanied by multiple cylindromas, trichoepithelioma, eccrine spiradenoma, and milia constitute an autosomal BrookeSpiegler syndrome (familial cylindromatosis or turban tumor syndrome). Somatic mutations of this gene are additionally incessantly present in sporadic instances of membranous basal cell adenoma. A, the tumor islands comprise uniform basaloid cells with focal nuclear palisading at the periphery. In the left area, a glandular lumen lined by cells with eosinophilic cytoplasm is present. A, this variant could additionally be mistaken for adenoid cystic carcinoma due to the presence of many cribriform buildings. B, Besides absence of invasive tumor borders (not shown), the cribriform islands seem to be shaped by expanded jigsaw puzzle�like lobules punctuated by multiple cystic areas, they usually merge with the characteristic basaloid lobules of basal cell adenoma (lower field). A, the fibrous stroma between the islands of tumor harbors bland-looking plump spindle cells (most evident in the left upper field). Adenoid cystic carcinoma: the cribriform variant of basal cell adenoma is commonly mistaken for adenoid cystic carcinoma. The islands of basaloid cells are usually surrounded by thick eosinophilic hyaline sheaths made up of basement membrane materials and likewise interspersed with hyaline droplets. Periodic acid�Schiff�diastase stain dramatically highlights the thick hyaline sheaths around the tumor islands, in addition to the interposed hyaline material among the many tumor cells. Note the remarkable identification of histologic appearances of the 2 tumor sorts, which explains the choice name of "dermal analogue tumor" for membranous basal cell adenoma. Basal Cell Adenocarcinoma Definition Basal cell adenocarcinoma is a low-grade malignant neoplasm with cytoarchitectural resemblance to basal cell adenoma. The apparent infiltrative growth of this basal cell neoplasm unequivocally locations it into the malignant category. Basal cell adenocarcinoma typically grows in the type of lobules, usually with a jigsaw puzzle�like high quality. However, tumors arising in minor salivary glands seem to have a higher recurrence price (71%), metastatic rate (21%), and mortality (29%) compared with those arising in main glands (corresponding figures 37%, 11%, 3%). Well-defined tubular structures with two-cell type of lining are typically present focally. Cases displaying nuclear atypia and readily recognized mitotic figures are simple to recognize as being malignant. However, most circumstances have a relatively bland cytologic appearance, and the diagnosis of malignancy relies solely on the identification of infiltrative development. Perineural infiltration or intravascular invasion is present in 25% to 35% of instances. It is indistinguishable from basal cell adenoma were it not for the presence of unequivocally infiltrative development. B, this example exhibits more apparent nuclear atypia and mitotic exercise within the basaloid tumor cells. Clinical Features Myoepithelioma most frequently impacts the parotid gland and palate. Pathologic Features Myoepithelioma is usually thinly encapsulated and has a strong, tan or yellow cut floor. The neoplastic myoepithelial cells may be spindled, plasmacytoid hyaline, epithelioid, clear, or oncocytic, with the primary two cell sorts being commonest. Either a single cell kind predominates in a tumor, or a mix of cell sorts could be present. Myoepitheliomas of the minor glands are inclined to be composed of plasmacytoid hyaline cells, and those of the parotid gland, spindled or epithelioid cells. The central portion of the tumor island exhibits squamous differentiation with keratinization. Although the presence of a minor ductal element was previously acceptable,124-127 the newest definition is stricter, with no ductal part being allowed. E, Solid to trabecular development sample with distinguished interspersed hyaline materials. F, Prominent hyalinization and presence of irregular clefts lead to an pseudoangiomatous pattern. Plasmacytoid hyaline cells in myoepithelioma are equivalent to those seen in pleomorphic adenoma. They type nondescript islands and sheets or are suspended in myxoid matrix within the type of isolated cells, cords, or aggregates, and in the absence of true chondroid matrix. Although it has been disputed that plasmacytoid hyaline cells lack immunohistochemical and ultrastructural proof of myoepithelial differentiation,133 optimistic staining for calponin, actin, and p63 helps their myoepithelial nature. C, Plasmacytoid hyaline cells (left field) and semiplasmacytoid hyaline cells (right field). They are normally present only focally however can occasionally be so outstanding as to pose difficulties in distinction from different clear cell tumors. However, the presence of rare enlarged hyperchromatic nuclei in a background of benignappearing cells is appropriate. Ultrastructural research can help verify myoepithelial differentiation by identifying each epithelial (hemidesmosomes) and myoid options (myofilaments with focal densities, pinocytotic vesicles). Tyrosine crystals (resembling daisy heads) are present within the stroma of this case. Various mesenchymal lesions, for instance, nerve sheath tumor, nodular fasciitis, solitary fibrous tumor Myoepithelial Carcinoma (Malignant Myoepithelioma) Definition Myoepithelial carcinoma is a pure myoepithelial tumor that demonstrates cytologic atypia and a potential for aggressive behavior. A designation "myoepithelial neoplasm of unsure malignant potential" may be appropriate for a tumor that reveals some worrisome features but falls wanting frank infiltrative progress. Clinical Features the height age is within the sixth decade, about 10 years older than for the benign counterpart. Approximately one half of cases arise from a preexisting pleomorphic adenoma or myoepithelioma, significantly in recurrences. Approximately one third of patients die; another third have recurrences, principally multiple; and the remaining third are illness free. Pathologic Features Myoepithelial carcinoma is usually unencapsulated and may exhibit areas of necrosis and cystic degeneration, although uncommon examples could also be predominantly encapsulated.
Diseases
- Mental retardation arachnodactyly hypotonia telangiectasia
- Hypertriglycidemia
- Cerebro oculo genital syndrome
- Vitreoretinochoroidopathy dominant
- Bronchiolitis obliterans with obstructive pulmonary disease
- Baker Vinters syndrome
- Knuckle pads, leuconychia and sensorineural deafness
- Acyl-CoA dehydrogenase, short chain, deficiency of
Other delicate variations in the pathologic features and conduct of these lesions have additionally been famous antibiotic 3 2 250 mg panmycin cheap overnight delivery. Clinically bacteria never have 500 mg panmycin buy amex, they most often current as endobronchial lesions that trigger signs related to bronchial obstruction bacteria kid definition buy panmycin 250 mg cheap, including cough 801 antibiotic purchase 500 mg panmycin overnight delivery, dyspnea, and hemoptysis. Peripheral lesions are more doubtless to be asymptomatic and therefore found incidentally on routine chest radiograph. As a group, salivary gland�type tumors are inclined to behave as low-grade neoplasms with a good clinical outcome when fully resected. In specific, salivary gland� type blended tumors, acinic cell carcinoma, low-grade mucoepidermoid carcinoma, and epithelial-myoepithelial carcinoma are curable by surgical excision alone. However, some exceptions exist; for instance, adenoid cystic carcinomas might follow an aggressive course with distant spread and excessive mortality, depending on the stage of the illness at the time of initial prognosis. Tumors discovered to be at a complicated stage on the time of prognosis will often prove deadly, unbiased of the histologic features. Poorly differentiated salivary gland�type combined tumors and mucoepidermoid carcinomas of high-grade histology will also present extremely aggressive habits resulting in death because of widespread metastases. Adenoid Cystic Carcinoma Adenoid cystic carcinoma of the bronchus could demonstrate a wide selection of histologic development patterns: (1) cribriform (cylindromatous), (2) tubular, and (3) strong. The islands of tumor cells are separated by fibrous bands and include cells with round nuclei displaying clear nuclear outlines and scant eosinophilic cytoplasm. The cystic areas are composed of two rows of cells, and mitotic figures are usually absent. The solid development sample is probably probably the most uncommon and is characterised by similar cells that kind diffuse sheets. Mitotic figures are found more incessantly in affiliation with the latter growth sample. The only parameter that has been discovered to predict the prognosis for these tumors reliably is staging at the time of preliminary analysis. Immunohistochemical stains will establish both a glandular secretory and a myoepithelial component. Several morphologic growth patterns have been identified in these tumors, including acinar, cystic or papillocystic, nesting, and oncocytic. Some tumors could also be composed predominantly of oncocytic cells exhibiting a strikingly nested growth pattern, thus intently resembling a neuroendocrine neoplasm. The most important feature for analysis, nevertheless, is the finding of 600- to 800-nm membrane-bound intracellular zymogen granules by electron microscopy. Mucoepidermoid Carcinoma Mucoepidermoid carcinoma represents the most common major salivary gland�type tumor of the lung and is amongst the most common major lung tumors in children. They are characterised by sheets of cells showing epidermoid differentiation admixed with mucocytes containing intracellular and extracellular mucin. The more strong component could also be composed predominantly of clear cells embedded in a fibrous stroma. In the low-grade tumors, the solid or epidermoid element is devoid of serious cellular atypia or mitotic activity. The presence of marked mobile atypia and mitotic exercise, as nicely as areas of necrosis and hemorrhage, are options indicative of a high-grade tumor. Transitions between areas of low- and high-grade malignancy could additionally be seen in any given tumor. High-grade mucoepidermoid carcinoma may be unimaginable to distinguish from poorly differentiated squamous cell carcinoma in the absence of a well-differentiated mucoepidermoid carcinoma component in the same tumor. The epithelial components usually take the form of ductal, glandular, and solid areas composed of rather small, eosinophilic or clear cells with spherical to oval nuclei and inconspicuous nucleoli. In some circumstances the strong mobile proliferation can undertake a plasmacytoid appearance. In the majority of cases, the predominant component is a solid proliferation of myoepithelial cells. Immunohistochemical stains demonstrate the myoepithelial nature of these cells by exhibiting coexpression of keratin and actin filaments. The mesenchymal stromal part in combined tumors is characterized by loose chondromyxoid tissue and more hardly ever by the formation of cartilaginous matrix. The tumors may be very stable and show low to reasonable mitotic activity, yet still behave in a low-grade trend with full surgical excision generally being curative. The presence of increased mitotic exercise, necrosis, vascular invasion, and pronounced cellular atypia ought to alert the pathologist to the potential of a malignant mixed tumor. Epithelial-Myoepithelial Carcinoma that is an unusual tumor characterised by glandular or tubular structures made up of cells with abundant clear cytoplasm showing characteristic displacement of the nuclei toward the periphery102. Immunohistochemical stains show the myoepithelial nature of the clear cells; coexpression of actin and keratin is seen, in addition to focal positivity for vimentin and S-100 protein. Oncocytoma Rare circumstances of oncocytoma resembling those seen in the salivary glands have been reported up to now as major lung neoplasms. The two most necessary lesions in this class are carcinosarcoma and pulmonary blastoma. For the analysis of pulmonary carcinosarcoma, both the epithelial and the mesenchymal element have to be simply acknowledged as malignant on routine microscopic examination. Carcinosarcoma must also be distinguished from sarcomatoid or spindle cell carcinoma. In the latter, the tumor is composed totally of a malignant proliferation of epithelial cells, as demonstrated by immunohistochemical or ultrastructural proof of epithelial differentiation within the sarcomatoid or spindle cell element, whereas in carcinosarcoma the 2 separate parts show unequivocal features of both epithelial or mesenchymal differentiation by light microscopic, immunohistochemical, and ultrastructural studies. A male predominance appears to exist, in addition to a direct correlation with the usage of tobacco. The tumor appears to present a predilection for adults, with a mean age of 60 years. On the other hand, tumors arising in the periphery of the lung usually have a tendency to reach a big measurement before they produce signs. Therefore the prognosis for these tumors, although poor, can be linked to their anatomic location. Among the most typical scientific symptoms are cough, hemoptysis, and obstructive pneumonia for the central lesions and chest pain for the peripheral lesions. Although the tumors are usually solitary, satellite tv for pc nodules can be noticed within the vicinity of the main lesion. Histologically the epithelial element may take the type of an adenocarcinoma, squamous cell carcinoma, small cell carcinoma, or anaplastic giant cell carcinoma. The mesenchymal part often corresponds to one of many well-defined types of differentiated soft tissue sarcomas such as chondrosarcoma, osteosarcoma, or 5 Tumors of the Lung and Pleura 221 rhabdomyosarcoma. As acknowledged previously, these components must be acknowledged simply by routine light microscopy; the function of immunohistochemistry for diagnosis will often solely be confirmatory. Pulmonary Blastoma this kind of tumor corresponds to a blended epithelialmesenchymal neoplasm in which each elements appear to correspond to immature or primitive glandular or stromal components suggestive of embryonal structures. Two histologic variants are identified: (1) predominantly epithelial (monophasic) and (2) mixed epithelial-mesenchymal (biphasic blastoma). The predominantly epithelial tumors have additionally been designated under a wide selection of other phrases, including adenocarcinoma of fetal lung sort, welldifferentiated fetal adenocarcinoma, pulmonary endodermal tumor resembling fetal lung, and pulmonary embryoma. Tumors located centrally are extra probably to produce signs of bronchial obstruction, whereas these situated within the periphery of the lung most often stay asymptomatic until the tumor reaches a bigger dimension. Grossly, the tumors are often properly circumscribed, unencapsulated, and solitary and should range in measurement from 1 cm to over 20 cm in diameter. On reduce section, these lesions are firm and rubbery and in about 50% of instances show areas of necrosis. Histologically, the biphasic tumors are characterized by a glandular proliferation composed of tubular structures of various sizes separated by a densely cellular spindle cell stromal element. The tubular structures could resemble endometrial glands or might present clear cell options with hanging subnuclear vacuolization paying homage to fetal lung. More lately, a high-grade type of the monophasic epithelial sort has been described. In the biphasic tumors, the spindle cell part may be completely undifferentiated or present features of a conventional sarcoma. Other components that may occasionally be encountered in pulmonary blastoma embody cartilage, bone, and multinucleated trophoblast-like big cells. However, it has been noticed that monophasic tumors have a better prognosis than the biphasic ones. Theoretically, any given type of tumor affecting the soft tissue may happen within the lung as a primary tumor. Because the lung is a common site of metastases from delicate tissue sarcomas, care must be taken to obtain a whole clinical history and examination earlier than rendering a analysis of main sarcoma of the lung to rule out the potential of metastasis from a delicate tissue major.
Diseases
- Diabetes insipidus, nephrogenic type 1
- Pseudoachondroplasia
- Aplasia cutis congenita recessive
- Maternal hyperphenylalaninemia
- Hing Torack Dowston syndrome
- Osteomyelitis
- Sclerosing bone dysplasia mental retardation
- Deafness c Deafness s
- Delayed ejaculation
A infection rates in hospitals panmycin 250 mg online, this determine exhibits the prototypic appearance of this tumor type: invasion in pushing fronts antibiotics yes or no panmycin 250 mg discount visa, violaceous staining high quality of the tumor cells antibiotic used for acne 250 mg panmycin buy mastercard, microcystic areas infection nail bed 500 mg panmycin buy with mastercard, and interspersed lymphoid aggregates. Note the typical microcystic sample of the big tumor islands, that are separated by sclerotic septa. Nonspecific glandular cells are also present that are generally small, with eosinophilic to amphophilic cytoplasm, often forming sheets. Uncommon cell types embody vacuolated cells with a solitary or multiple clear vacuoles. They are susceptible to ischemia and infarction, which happens spontaneously or after fine-needle aspiration. This rare variant is characterised by giant cystic areas lined by simple or stratified cuboidal epithelium with some papillary projections. A, the tumor is punctuated by irregular-shaped small cystic spaces (empty or containing blood in this case). Note also the violaceous color of the cytoplasm, as commonly observed in acinic cell carcinoma. B, Tumor islands interspersed with many microcystic areas, some containing eosinophilic secretion. D, Rarely, some microcystic spaces have a microglandular appearance (upper field), with lining cells regularly aligned around the areas. A, Some cells contain abundant basophilic granules, consistent with acinar cell differentiation. Smaller cuboidal cells are admixed with apparent differentiation toward intercalated ducts. C, Polygonal tumor cells with amphophilic cytoplasm and sparse small basophilic granules. This uncommon variant contains closely packed spherical cystic areas full of homogeneous eosinophilic colloid-like materials, extremely reminiscent of thyroid follicles. The follicles are lined by intercalated duct-like cells and nonspecific glandular cells. Immunostaining for thyroglobulin is useful for ruling out a thyroid follicular neoplasm. Dedifferentiated Acinic Cell Carcinoma Dedifferentiation of acinic cell carcinoma to a high-grade adenocarcinoma, poorly differentiated carcinoma, or undifferentiated carcinoma can rarely happen at presentation or in the recurrent tumor. This rare variant is characterised by follicles containing eosinophilic colloid-like material. C, the intraluminal component consists of pseudopapillae with no fibrovascular cores. D, the intraluminal component might take the form of a protruding nodule with a microcystic sample. A, the left area reveals a typical acinic cell carcinoma with microcystic growth sample. The right field exhibits a high-grade carcinoma with a solid development pattern (dedifferentiated component). B, the tumor cells of acinic cell carcinoma are bland wanting (left), whereas those of the high-grade carcinoma exhibit bigger nuclei with vital nuclear pleomorphism. Dedifferentiated acinic cell carcinoma is associated with fast tumor progress, significant pain, facial nerve palsy, cumbersome tumor, and an especially poor prognosis. However, the value of amylase staining is restricted as a result of solely 15% of instances are optimistic. The normal serous cells show moderate apical membranous staining, and the distal intercalated duct cells present variable weak to moderate apical staining. A, the most common progress patterns are microcystic (left field) and papillary-cystic (right field), occurring alone or together. B, Tumor islands punctuated by microcysts, which are empty or include eosinophilic or basophilic secretion. In distinction to acinic cell carcinoma, basophilic cytoplasmic granules are conspicuously absent. The mainstay of therapy is full surgical excision with or with out postoperative radiotherapy. Microscopic Features the tumor is basically circumscribed with focally invasive borders. The tumor grows within the form of microcystic to cribriform islands, tubulocystic glands, papillary cystic buildings, and typically thyroidlike follicles. Bluish mucin and eosinophilic secretions are readily discovered within the glandular lumens. The tumor cells are cuboidal to polygonal, with eosinophilic granular or multivacuolated cytoplasm. The nuclei are oval with finely granular chromatin and/or small distinct nucleoli. The cytologic composition corresponds to the intercalated duct, vacuolated, and nonspecific glandular cells as initially described in acinic cell carcinoma, whereas acinar cells with basophilic zymogen granules are conspicuously absent. In occasional instances, some tumor islands are surrounded by a layer of p63+ abluminal cells, indicating the presence of a focal intraductal (in situ) element. The tumor characteristically shows extensive and powerful staining for S100 protein. Each nucleus accommodates one regular fused red-green (or yellow) signal, one separate purple sign, and one separate green signal. Macroscopic and Microscopic Appearances Grossly, most tumors are circumscribed but nonencapsulated, with a lightweight tan to grey glistening minimize surface. Despite the gross circumscription, infiltrative growth is apparent histologically, with invasion of salivary gland lobules or adjacent adipose tissue or muscle. The cribriform plates seem as islands of tumor cells interrupted by round, rarefied areas which are empty or crammed with mucoid materials. Papillary or papillary-cystic pattern consists of dilated cysts with small intraluminal papillary projections. Extensive and robust immunoreactivity for S100 and mammaglobin can assist additional in the distinction. Other designations embody lobular carcinoma,369 terminal duct carcinoma,370 and low-grade papillary adenocarcinoma. Only hardly ever does it occur in the main glands, the place it mostly represents the malignant part in carcinoma ex pleomorphic adenoma. Highly variable growth patterns are current in different areas of the same neoplasm. The tumor cells have round pale nuclei with evenly distributed fantastic chromatin and indistinct nucleoli. The tumor cells could assume cuboidal, columnar, spindled, or polygonal shapes, however the bland cytologic features are at all times maintained. Although some authors contemplate myoepithelium to be an integral component of this tumor sort,321,384 myoepithelial cells are absent or at most current very focally on the lightmicroscopic level. A, this exhibits a extremely characteristic swirling pattern, resembling sclerosing adenosis of the breast. A, the tubules are lined by ductal cells solely, without an underlying layer of basal or myoepithelial cells. The tumor cells show a excessive nucleus to cytoplasm ratio and more hyperchromatic nuclei. The most commonly involved site is the tongue, but the soft palate, buccal mucosa, tonsils, and lip may also be involved. The tumor cells are bland looking and possess uniform, often overlapping, nuclei with vesicular or "ground-glass" chromatin reminiscent of papillary thyroid carcinoma. Epithelial-Myoepithelial Carcinoma Definition Epithelial-myoepithelial carcinoma is a malignant tumor composed of ductal structures lined by a single layer of ductal cells that are surrounded by a single or multiple layers of clear myoepithelial cells. The counterparts in the breast are adenomyoepithelioma and adenomyoepithelial carcinoma. The tumor has additionally been reported to happen in lacrimal gland, lung, bronchus, trachea, and liver. Recurrence is reported in 30% to 40% of instances, which may occur as late as 28 years after initial surgery.