
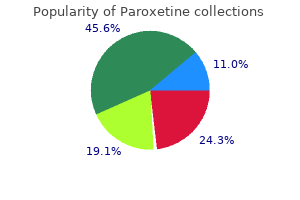
Paroxetine
| Contato
Página Inicial

"Order paroxetine 20 mg with amex, symptoms ear infection".
P. Jerek, M.B. B.CH. B.A.O., Ph.D.
Vice Chair, Touro College of Osteopathic Medicine
Nonselective angiography is most well-liked to avoid trauma when participating the ostium of the vertebral artery with an angled catheter (Judkins right coronary medicine 773 buy paroxetine 20 mg online, Berenstein medicine naproxen paroxetine 20 mg purchase line, Cobra medicine plies buy paroxetine 20 mg with mastercard, or internal mammary artery catheter) symptoms bacterial vaginosis paroxetine 20 mg buy free shipping. Typically the catheter is positioned very near the ostium, and hand injections of distinction are made to visualize the vertebral artery. After penetrating the foramen of the atlas, it enters the cranial cavity via the foramen magnum. The vertebral artery joins with the contralateral vertebral artery to type the basilar artery. Nonselective angiography is carried out with hand injections, using a coronary manifold with stress monitoring, analogous to selective coronary angiography. Similar to views of the anterior cerebral circulation, it is essential to determine the contribution of the posterior circulation to the circle of Willis. Complications of Peripheral Vascular Angiography Complications of peripheral vascular angiography could result in significant morbidity and even mortality. Access website bleeding is the most frequent complication following femoral arterial entry. In general, entry website bleeding may be managed by guide or mechanical compression and reversal of anticoagulation. If bleeding continues despite these steps, extra aggressive therapies-including percutaneous intervention or surgical therapy-may be thought of. If retroperitoneal bleeding is suspected, anticoagulation ought to be reversed and discontinued. Volume resuscitation with crystalloid solutions and/or blood merchandise ought to be administered if volume depletion is clinically evident. If bleeding causes hemodynamic embarrassment (hypotension), emergency angiography from the contralateral femoral artery access site should be carried out to identify the bleeding site. Surgical correction is reserved for those patients who fail a less invasive method. Vascular entry closure devices are designed to facilitate hemostasis, scale back time to ambulation, and reduce length of hospital stay. Allergic or anaphylactic reactions happen in fewer than 3% of instances, and fewer than 1% require hospitalization. Nonoliguric creatinine elevation, which peaks inside 2 to three days and returns to baseline by 7 days, is the standard medical scenario of contrast-induced nephrotoxicity. Patients in danger for contrast-induced nephropathy are these with baseline persistent renal insufficiency, diabetes mellitus, a number of myeloma, and individuals who are receiving different nephrotoxic drugs. All sufferers in general, but these at risk to develop contrast-induced nephropathy specifically, ought to be well hydrated before and after the procedure, and the quantity of contrast quantity should be minimized. One randomized trial reported that in patients with renal insufficiency, Iodopaque (iso-osmolar, nonionic) is much less nephrotoxic than Omnipaque (low osmolar, nonionic) distinction, but there are conflicting studies. However, it demonstrated that acetylcysteine was ineffective in preventing contrast-induced nephropathy. Hydration with half-normal saline for 12 hours earlier than and after the process offers better safety against creatinine rise than the mixture of hydration and diuretics. Other risk factors include feminine intercourse, age older than 70 years, diabetes mellitus, and weight problems. Patients with pseudoaneurysms usually present with ache at the access site several days following the intervention. On bodily examination, a pulsatile hematoma could also be current with a systolic bruit. Management of a femoral pseudoaneurysm is dependent on its size, severity of symptoms, and want for continued anticoagulation. A small pseudoaneurysm (<2 cm) could also be observed and often will resolve spontaneously. Larger pseudoaneurysms could also be handled with ultrasound-guided compression, percutaneous offlabel thrombin injection, endovascular coil insertion, or coated stents. Surgical repair of pseudoaneurysms is normally reserved for failure of less invasive approaches. In some cases, there may be a swollen and tender extremity due to venous dilation, and in severe circumstances, arterial insufficiency (steal syndrome) might occur. When catheters are manipulated within the aorta or brachiocephalic vessels during a thoracic aortogram, stroke is a rare however doubtlessly devastating complication. If an embolic stroke has occurred, one choice is to perform catheter-directed thrombolysis and/or angioplasty. In the presence of intracerebral hemorrhage, anticoagulants and antiplatelet agents must be reversed. Unlike contrast-induced nephropathy, renal dysfunction after atheroembolization usually develops slowly (weeks to months) and a few of these patients progress to renal failure. Diagnosis is confirmed by tissue examination (biopsy), and remedy is supportive. Systemic manifestations of atheroembolism include livedo reticularis, abdominal or foot ache, and purple toes associated with systemic eosinophilia (blue toe syndrome). Spinosa D, Angle J, Hagspiel K, et al: Feasibility of gadodiamide in contrast with dilute iodinated distinction material for imaging of the abdominal aorta and renal arteries, J Vasc Interv Radiol 11:733, 2000. Ledneva E, Karie S, Launay-Vacher V, et al: Renal safety of gadolinium-based contrast media in patients with chronic renal insufficiency, Radiology 250:618�628, 2009. Armstrong P, Han D, Baxter J, et al: Complication rates of percutaneous brachial artery entry in peripheral vascular angiography, Ann Vasc Surg 17:107, 2003. Beales J, Adcock F, Frawley J, et al: the radiological assessment of illness of the profunda femoris artery, Br J Radiol 44:854, 1971. Singh H, Cardella J, Cole P, et al: Quality enchancment pointers for diagnostic arteriography, J Vasc Interv Radiol 13:1, 2002. Waigand J, Uhlich F, Gross C, et al: Percutaneous remedy of pseudoaneurysms and atriovenous fistulas after invasive vascular procedures, Catheter Cardiovasc Interv 47:157, 1999. Toursarkissian B, Mejia A, Smilanich R, et al: Changing patterns of access website complications with the use of percutaneous closure gadgets, Vasc Surg 35:203, 2001. Aspelin P, Aubry P, Fransson S, et al: Nephrotoxic results in high-risk patients undergoing angiography, N Engl J Med 348:491, 2003. Willinsky R, Taylor S, Terbrugge K, et al: Neurologic problems of cerebral angiography: potential analysis of 2,899 procedures and evaluate of the literature, Radiology 227:522, 2003. Fayed A, White C, Ramee S, et al: Carotid and cerebral angiography performed by cardiologists: cerebrovascular complications, Catheter Cardiovasc Interv fifty five:277, 2002. Peripheral artery disease is related to most of the similar danger components as atherosclerotic cardiovascular and cerebrovascular diseases, and is quite common among the many elderly. Peripheral artery illness that exhibits typical symptomatology, usually in the type of leg pain brought about by walking, has been conservatively estimated to reduce high quality of life in at least 2 million Americans, and in some circumstances leads to a need for surgical revascularization or amputation. This type of ache is named intermittent claudication and is characterized as leg ache or discomfort associated with walking and relieved by rest. A number of affected person questionnaires have been developed to uniformly determine claudication and distinguish it from different forms of leg pain. The first of these was the Rose questionnaire, additionally referred to as the World Health Organization questionnaire. Classic: 1 = yes and 2 = no and three = sure and four = yes and 5 = cease or slow down and 6 = lessened or relieved 5. Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Stop or slow down Continue on Stop or decelerate Continue on Lessened or relieved Unchanged Lessened or relieved Unchanged traditional threat factors and comorbidities. Pressure measurements are made with the patient at relaxation in a supine place for five minutes previous to measurement. Ankle stress is measured in both legs at the dorsalis pedis and posterior tibial arteries. In epidemiological analyses, the unit of analysis is either the leg, with appropriate statistical adjustments for intrasubject correlation, or the subject, with illness standing classified primarily based on the "worst" limb. With respect to claudication, information from the Framingham Study show claudication in men rising from lower than 0. The design and period of this research had been uniquely suited to estimating long-term tendencies in disease incidence; comparable studies for different populations are unavailable.
Syndromes
- Collapse
- Syphilis (small, painless open sore or ulcer (called a chancre) on the genitals)
- Respiratory failure
- Abdominal pain or cramps, nausea, vomiting, and diarrhea
- Chest x-ray
- Abdominal pain
- Seizures
The femoral pulse is situated deep symptoms meaning paroxetine 20 mg discount on-line, beneath the inguinal ligament symptoms zoloft dosage too high paroxetine 10 mg cheap free shipping, about halfway between the symphysis pubis and iliac backbone medications kidney failure discount paroxetine 20 mg without a prescription. Lateral rotation of the leg symptoms 3 months pregnant paroxetine 10 mg order on line, pannus retraction, and two arms could additionally be required for enough palpation. The popliteal pulse must be palpated with three fingers from each hand while the thumbs are making use of moderate opposing force to the highest of the knee. The popliteal pulse typically could be discovered at the junction of the medial and lateral thirds of the fossa. In contrast to superficial pulses like the radial or dorsalis pedis pulse, the popliteal pulse is diffuse and deep. The posterior tibial pulse could be found slightly below and behind the medial malleolus. Examiner, utilizing three or 4 fingers, lightly palpates the superficial radial pulse over stylus of radius close to base of thumb. Examiner uses both thumbs for reasonable opposing pressure whereas placing digits two, three, and four in lateral third of popliteal fossa. In contrast, the dorsalis pedis pulse, which could be appreciated just lateral to the extensor tendon on the dorsum of the foot, usually may be absent in 2% to 12% of individuals. Each compo- eleven nent of the bundle could additionally be affected, including the brachial plexus, subclavian/axillary artery, and subclavian/axillary vein. Thoracic outlet maneuvers search to elicit positional interruption of arterial move. During the examination, the doctor holds the radial pulse in one hand and maneuvers the arm with the other. An irregular thoracic outlet maneuver is characterized by improvement of a subclavian bruit followed by loss of the radial pulse. Several thoracic outlet maneuvers have been described, and each may be relevant to compression at completely different websites in the thoracic outlet. The Adson maneuver assesses the section of the subclavian artery in the scalene triangle. The costoclavicular maneuver assesses the section of the subclavian artery coursing between the clavicle and first rib. The hyperabduction maneuver evaluates the subclavian artery because it courses near the insertion of the pectoralis main muscle. Abduction of the arm to ninety degrees may be mixed with external rotation in evaluating signs suggestive of thoracic outlet syndrome. This maneuver is commonly used to assess subclavian venous or arterial compression throughout ultrasonography or angiography. For patients in whom clinical suspicion for thoracic outlet syndrome is present, sensitivity and specificity for these provocative tests are 72% and 53%, respectively. Indeed, in a single study of sixty four randomly chosen subjects, software of these maneuvers in a nonspecific method overdiagnosed the syndrome more than threefold. It ought to be approached from the lateral facet, with digits utilized to lower curvature of malleolus. Within the hand, these arteries type the superficial and deep palmar arches, enabling blood supply to the digits from either vessel; 5% to 10% of the population has a congenitally incomplete arch. Persistent pallor is indicative of an incomplete palmar arch or occluded artery distal to the remaining pulse occluded by the examiner. Both radial and ulnar pulses are occluded whereas affected person opens and closes hand to create palmar pallor. In this example, affected person presented with persistent fifth digit and hypothenar cyanosis. A, Release of radial artery pulse leads to expected hyperemia and palmar erythema. Patient initially sits wanting ahead whereas arms are abducted 90 degrees, elbows are abducted ninety degrees, and affected person repeatedly makes a clenched fist. During maneuver, radial pulse should be palpated while subclavian artery is auscultated. Digital ischemia could additionally be apparent in sufferers with fastened obstructive lesions of the digital arteries. Fissures, pits, ulcerations, or necrosis or gangrene could also be evident on the ischemic digits. The "laces" might differ in colour from purple to blue and encompass a central space of clearing. The secondary forms are usually related to vasculitis, atheroemboli, hyperviscosity syndromes, endocrine abnormalities, and infections. In the secondary types of livedo reticularis, lesions could additionally be more diffuse and ominous. Purpuric lesions and cutaneous nodules that progress to ulceration in response to cold might develop. The commonest location is in the legs, adjoining to the malleoli and over the tibia. With deep digital palpation, improvement of a divot or finger impression is indicative of pitting edema. Edema could be graded in each leg or arm as absent, mild, average, or severe or on a numerical scale of 4, with 0 being the absence of edema. A common femoral vein wire is detected by palpating alongside its course slightly below the inguinal ligament vein, and a femoral vein twine can be appreciated along the anteromedial side of the thigh. In the absence of obvious edema, a subtle clue could also be unilateral absence of contours of the thigh, calf, or ankle. Muscular teams subtended by the thrombosed vein may be edematous because of poor venous drainage, conferring a boggy feeling to the affected calf or thigh muscles. The ft, palms, fingers and toes must be examined for temperature and pores and skin shade, and the nails for evidence of fragility and pitting. Temperature adjustments of adjacent segments on the ipsilateral limb and comparisons with the contralateral limb may be made. Presence of foot pallor whereas the leg is horizontal is indicative of poor perfusion and could also be an indication of ischemia. To qualitatively assess collateral blood circulate, the leg is then lowered because the affected person strikes to the seated place. This is completed to elicit rubor, indicative of reactive hyperemia, and decide pedal vein refill time. Neurotrophic ulcers that develop in patients with diabetes typically happen at sites of trauma, corresponding to areas of callus formation, bony prominence, or elements of the foot uncovered to mild chronic trauma caused by ill-fitting footwear. Without correct therapy, ulceration might progress to tissue necrosis and gangrene. Gangrene may be characterized as an area of dead tissue that blackens, mummifies, and sloughs. Chronic venous insufficiency and edema end in deposition of hemosiderin, causing darkening and toughening of skin and giving calf a brawny look. The patient might present with local venous engorgement, a palpable twine, warmth, erythema, or tenderness. Chronic venous edema could impart hemosiderin deposition in the skin and confer a brawny appearance, typically in the pretibial calf. In contrast to arterial ulcers, which are circumscribed and pallid, venous ulcers are giant with irregular borders, erythematous, and moist, giving the pores and skin a shiny appearance. Areas of erythema, tenderness, or induration might determine superficial thrombophlebitis. Superficial venous varicosities may be primary or outcome from deep venous thrombosis or insufficiency. An examiner can distinguish between superficial venous insufficiency and deep venous insufficiency at the bedside utilizing the Brodie-Trendelenburg take a look at. With the patient mendacity supine, the leg is elevated to 45 levels and a tourniquet utilized after the veins have drained. If venous refill distal to the positioning of tourniquet application occurs in less than 30 seconds, this is proof of an incompetent deep and perforator system. Superficial venous insufficiency shall be confirmed with rapid retrograde superficial venous filling. The Perthes check can differentiate between deep venous insufficiency and a deep venous obstruction as the cause for varicose veins. The patient is requested to stand, and as quickly as the superficial veins are engorged, a tourniquet is utilized across the mid-thigh. If the varicose veins collapse below the extent of the tourniquet, the perforator veins are 146 pinch pores and skin on the toes, the Stemmer sign, additionally may differentiate early lymphedema from venous edema.
Syndromes
- Strongyloidiasis
- Low blood pressure
- Corneal ulcers -- Ulcers on the outer covering of the eye, usually because of a bacterial or viral infection.
- Stiffness
- Sore throat
- It is difficult or painful to move the eye
- Severe headache
- Overall appearance
- Two weeks before surgery you may be asked to stop taking drugs that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), Naprosyn (Aleve, Naproxen), and others.
- Headaches
Judicious use of heparin medicine education paroxetine 20 mg generic with amex, notably if the patient is on multiple antiplatelet agent treatment juvenile arthritis discount paroxetine 20 mg with amex, is essential medicine on time 20 mg paroxetine order mastercard. Carotid Endarterectomy Compared to Carotid Angioplasty/Stenting Carotid artery angiography and stenting is described intimately in Chapter 32 treatment kennel cough order paroxetine 20 mg free shipping. These variations endured for 1 12 months, however by 4 years, there was no difference between the 2 teams relating to eventfree survival. The study patients were adopted for 4 years, at which time the dying and stroke charges were 6. It involved 50 academic centers within the United Kingdom, Europe, Australia, New Zealand, and Canada. Between the years 2000 and 2008, 2502 patients had been randomized; 47% were asymptomatic, and 53% had been symptomatic. The preliminary evaluation occurred after the last group of patients had no much less than 1 yr of followup, and median follow up was 2. Hunt J: the function of the carotid arteries in the causation of vascular lesions of the mind, with remarks on certain special options of symptomatology, Am J Med Sci 147:704�713, 1914. Carrea R, Molins M, Murphy G: Surgical treatment of spontaneous thrombosis of the interior carotid artery within the neck: carotid-carotidal anastomosis. An index of tolerance to momentary carotid occlusion, Arch Surg 106:521�523, 1973. Halliday A, Mansfield A, Marro J, et al: Prevention of disabling and deadly strokes by profitable carotid endarterectomy in patients with out recent neurological signs: randomised managed trial, Lancet 363:1491�1502, 2004. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery, Circulation 124:e54�e130, 2011. North American Symptomatic Carotid Endarterectomy Trial Collaborators: Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis, N Engl J Med 325:445�453, 1991. Gowers W: On a case of simultaneous embolism of central retinal and middle cerebral arteries, Lancet 2:794, 1875. The terms speaking and noncommunicating check with the presence or absence, respectively, of blood flow between the true and false lumens of the aorta. Aortic dissection is acute if presentation happens inside 14 days of the onset of symptoms and persistent if more than 2 weeks have elapsed. In practice, analysis of aortic dissection depends on demonstration with imaging of an intimal flap with separation of true and false lumens. In type A dissection, the true lumen is normally displaced along the internal curvature of the aortic arch and continues caudally alongside the medial side of the descending thoracic aorta. Aortic department vessel blood move might derive from both the true or false lumen; alternatively, circulate could also be sluggish or absent inside the false lumen, or department vessels could additionally be utterly occluded at or close to their origins. Acute aortic dissection is an uncommon but life-threatening emergency that requires immediate analysis, speedy triage, and quick medical, endovascular, or surgical treatment. A unified effort across several international centers over the previous 15 years has led to the institution of a detailed registry that describes major aspects of presentation, administration, and outcomes of sufferers with acute aortic dissection. Although gains have been made in the delivery of life-saving care to sufferers with acute aortic dissection, hospital mortality rates stay distressingly high. Enhanced consciousness of danger factors for aortic dissection, presentation options, diagnostic pathways, and medical, endovascular, and surgical therapy strategies is a crucial first step toward bettering outcomes. Analysis of the Swedish National Cause of Death Register between 1987 and 2002 estimated the incidence of thoracic aortic aneurysm or dissection to be 16. In classic acute aortic dissection, the initiating event is an intimal tear through which blood rapidly surges distally in to the media under systolic pressure, splitting the layers of the aortic wall and creating an intimal flap that separates the true from the false lumen. Classification Classifying aortic dissection in accordance with anatomical location and time from onset of symptoms helps stratify risk and information number of preliminary therapy technique. The Stanford classification system designates dissections that involve the aorta proximal to the brachiocephalic artery. In the older DeBakey classification scheme, a type I dissection originates within the ascending aorta and extends for a variable distance beyond the take-off the innominate artery. It is most frequently situated a few centimeters above the level of the aortic valve alongside the higher curvature of the aorta in instances of kind A dissection and accounts for almost 60% of all instances. Compared with other locations within the ascending aorta, the proximal few centimeters of the greater curvature are uncovered to comparatively larger hemodynamic, shear, and torsional pressure. By this mechanism, as many as 20% of dissections that originate in the distal arch or descending thoracic aorta might contain the ascending aorta. Blood inside the false lumen might reenter the true lumen wherever alongside the length of the dissection. Reentry may be protective due to spontaneous decompression of the false lumen which will cut back the dangers of rupture and/or growth of malperfusion syndromes. Acquired Aortic Rupture and End-Organ Malperfusion Aortic rupture, outlined as tearing within the vessel wall that results in extravascular hemorrhage, most commonly happens with trauma. Dissection-mediated end-organ ischemia or infarction happens from (1) mechanical compression of aortic department vessels by false lumen hematoma, (2) extension of the dissection airplane throughout the ostium of the branch vessel, or (3) dynamic vessel inlet obstruction attributable to an oscillating intimal flap. The stomach aorta is the least frequent site for entry (3% of cases), despite the high prevalence of intima media ulcers in sufferers with atherosclerotic illness on this phase. A, Computed tomographic picture demonstrates three-channel descending aortic dissection in Marfan syndrome patient. B, Schematic illustration of dissection is offered: region 1 represents thrombosed false lumen, area 2 is true lumen considerably diminished in measurement, and area three designates contrast-enhanced false lumen. False Lumen Thrombosis Thrombosis of blood throughout the false lumen might seal the entry tear, thus eliminating communication with the true lumen and interruption of false lumen growth. Partial thrombosis of the false lumen, however, has been identified as a danger factor for long-term demise in sufferers with type B dissection. Alternatively, it has been proposed that partial thrombosis of the false lumen is related to worse clinical outcomes by promoting vascular irritation, hypoxia, and/or neovascularization with weakening of adjoining vascular constructions and an elevated risk for aortic rupture. A, Hematoxylin and eosin microscopic section of aorta reveals fragmentation and lack of elastin fibers with cyst-like structures current inside media. This phenotype is felt to be associated with aortic wall weakening and increased predisposition to dissection. Deceleration harm from high-speed accidents leads to aortic transection with false aneurysm formation and rupture, mostly in the region of the aortic isthmus just past the origin of the left subclavian artery. In many instances, being pregnant unmasks primary circumstances that predispose to aortic dissection. Decreased aortic compliance and vulnerability to pulsatile forces predispose to harm and create a substrate for dissection. Drug Use and Other Acquired Conditions Recent cocaine use, notably among younger men who smoke tobacco, is an additional risk issue for aortic dissection. Chronic amphetamine use and/or dependence seem to improve the chance of growing a thoracoabdominal aortic dissection in these aged 18 to forty nine years. Retrograde dissections created on the time of catheterization normally seal spontaneously on withdrawal of the catheter. Aortic atherosclerotic plaques could forestall longitudinal propagation of a dissection. Pheochromocytoma and weight lifting (believed due to intense or repetitious Valsalva maneuvers) additionally predispose to aortic dissection. Absent an appreciation for the cardinal options of dissection, the analysis may be missed in a considerable number of patients. Simple scientific prediction guidelines have been developed to estimate probability of acute aortic dissection. These markers, assessed at bedside, had been divided in to three distinct classes: predisposing components, traits of the ache at time of presentation, and key bodily examination findings. Visceral discomfort or limb pain may be indicative of aortic department vessel ischemia from malperfusion. Syncope is a very ominous presenting symptom and will reflect cardiac tamponade from intrapericardial aortic rupture, cerebral malperfusion, and/or neurally mediated hypotension in response to the intense ache of the dissection. For instance, paraplegia might develop when important impairment of circulate to the anterior spinal artery, thoracic intercostals, or the artery of Adamkiewicz happens. A retrospective evaluation of the International Registry of Acute Aortic Dissection decided that among 2538 sufferers with acute aortic dissection, ninety five. Hypertension is present in more than two thirds of kind B dissection patients and in roughly one third of sort A sufferers. Additional auscultatory findings embody a gentle first coronary heart sound and a grade 1 or 2 midsystolic murmur at the base or alongside the left sternal border.