
Rogaine 5
| Contato
Página Inicial

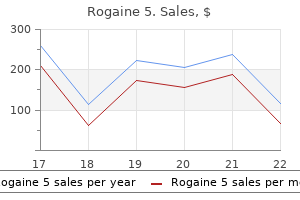
"Buy rogaine 5 60 ml with amex, prostate cancer vitamin d".
H. Yasmin, M.A., M.D.
Co-Director, University of Texas at Tyler
Invasive pathology might instantly infiltrate the cranial nerves or nuclei and induce neurological deficits mens health arm workout rogaine 5 60 ml purchase with visa, which might be less likely to prostate cancer early symptoms rogaine 5 60 ml otc enhance from operative intervention prostate cancer fund generic rogaine 5 60 ml without a prescription. Along this path prostatic urethra rogaine 5 60 ml discount with amex, it variably interacts with the origins of the ninth, tenth, or eleventh cranial nerves. It then divides into medial and lateral branches to provide the vermis or the tonsils and hemisphere, respectively. Originating in shut proximity to and usually inferior to the interior auditory meatus, it typically abuts the seventh and eighth cranial nerve complex. This includes the cerebellar cortex and cerebellar nuclei and, by proxy, tumors within these areas. It curves across the pons, inferior to the third, fourth, and fifth cranial nerves. Along its course, perforators provide the superior and middle cerebellar peduncles and the colliculi. The venous drainage can also be distinguished in the posterior fossa, with brainstem, bridging, superficial, and deep veins. These veins drain into the superior petrosal sinus, the transverse sinus, and the sigmoid sinus. The deep veins are alongside the roof and partitions of the fourth ventricle; they function periventricular constructions. The veins of the brainstem are on the anterior surface and drain into the petrosal and jugular sinuses and generally the sigmoid sinus. The transverse and sigmoid sinuses are usually the widespread last drainage outlet for the sagittal sinus, petrosal sinuses, and deep venous drainage pathways. Skull-base approaches, together with petrosal bone resection, alter these limitations by offering alternative angles to posterior fossa lesions, significantly these situated in the anterolateral posterior fossa. Early access to vascular buildings in the course of the initial dissection is necessary to decrease hemorrhage and to keep away from the problems of each blood loss and alternative, including anemia, coagulopathy, and transfusion reactions. Furthermore, although mannitol and dexamethasone throughout induction and surgery may assist in controlling edema, securing arterial entry provides definitive control of edema within the lesion and surrounding tissue, which can turn into acutely worsened within the setting of venous compromise. In certain circumstances deep provide or supply derived from a quantity of distributions can complicate surgical procedure. In the postoperative setting it is necessary to pay attention to vascular compromise in circumstances that may benefit explicit vigilance for hypoperfusion or venous congestion and venous infarction. Venous constructions are important in posterior fossa surgical procedure, and fixed consciousness of their location is crucial from the initial tumor method to keep away from venous damage. The junction between the transverse and sigmoid sinuses is commonly quoted to lie on the asterion, where the parietal, occipital, and temporal bone meet with three sutures. Perioperative Considerations Key Concepts the scientific examination, cerebrovascular perfusion, radiographic imaging, and echocardiographic outcomes guide intraoperative monitoring necessities. Although clinically important adjustments could also be undetected on intraoperative monitoring, these techniques might usually present helpful further data to guide the aggressiveness of operative objectives. For all positions, areas uncovered to strain require padding, such as the orbit, ankles, heels, knees, iliac crests, pelvis, breasts, axilla, elbow, wrist, and vascular access websites. During any surgical positioning, the neck is prone to structural damage, and avoidance of this requires shut consideration to element in the process. The inclined place retains the top in the impartial position with slight flexion to preserve standard anatomical distances and ease of orientation. The lateral place could involve turning of the head and can be achieved in a lateral physique place or with the patient supine with vital angulation. It is imperative to assess both structural neck pressure and preservation of cerebral venous return. Further specific considerations for the prone place embrace the turning approach, thoracic strain, and retinal damage. Turning of the patient can lead to injury, particularly to the neck or extremities. All extremities and the neck ought to be maintained in a neutral position throughout turning, which can require additional staff in the course of the turn. Once within the inclined place with commonplace cushioning points addressed, the thoracic pressure also must be addressed as a outcome of the susceptible place could limit air flow in addition to venous return, leading to hypoventilation and hypotension. This ought to be mentioned before the beginning of the case in order that the team is appropriately ready for such a maneuver. However, anatomical changes, edema, dural retraction, and dural shrinkage (even within the setting of frequent irrigation) may lead to inadequate material for closure. Dural substitutes include cadaveric pores and skin processed into tissue matrix, cadaveric tensor fasciae latae, or pericranium. The suture closure of the dural opening can be additional strengthened with artificial brokers, which differ in availability at every establishment. These brokers, which embrace totally different biological and chemical glues and bonding material, can be challenging to apply within the operative area, resulting in irregular bonding and inconsistent layering, and can be value prohibitive. Clinical Pearl Clinical danger elements for poor wound healing embrace diabetes, prior irradiation, upcoming irradiation, corticosteroid usage, smoking, and malnutrition. Although not yet evaluated, a heterologous supply such as a lyophilized bone, plastic implant, or mesh with cement or bone fragments could also be used instead of bone flap alternative. Soft tissue closure should emphasize reducing potential spaces and achieving a watertight closure. Postoperative Complications Complications may turn out to be obvious either during the operation or after an in any other case successful operation 20 Infratentorial and Cerebellar Tumors 213 Box 20. Whereas direct damage to neurological structures sometimes manifests on initial examination, the effects of edema, corresponding to from venous injury and subsequent congestion, usually have a delayed onset. Therefore early postoperative neurological examination is important to establish a primary time point. Therefore many institutional and operatorspecific policies may dictate the need for an intensive care unit for no less than the preliminary postoperative interval. Although intraoperative complications would typically have been stabilized before exiting the operating room, they might have continued monitoring requirements or ongoing impact on scientific status. Arterial harm in the course of the operation, whether because of unintended vessel damage and have to sacrifice the artery for hemostasis or intentional sacrifice to control tumor perfusion, may result in infarct of wholesome tissue. Posterior fossa infarction with cytotoxic edema might result in mass impact, obstructive hydrocephalus, and compression of the brainstem, with catastrophic outcomes. This edema may progress over the course of hours, and hemorrhagic conversion can hasten this process and make clinical deterioration precipitous. Venous injury, whether or not from bridging veins or sinuses, causes a very fulminant edema, with venous congestion usually accompanied by hemorrhagic conversion. Delayed improvement of focal neurological deficits localizing to the posterior fossa, corresponding to deficits of the lower cranial nerves, ataxia, or nystagmus, may point out a delayed damage to neurological buildings through a congestive process. Edema and mass effect from hemorrhage may also result in obstructive hydrocephalus. In the absence of hydrocephalus, the clinical examination and serial radiographic imaging might present the one reliable technique of monitoring infratentorial strain, similar to demonstration of upward herniation or tonsilar herniation through the foramen magnum. Clinical Pearl Hydrocephalus may not be synonymous with ventriculomegaly, notably in operations of the posterior fossa the place the dural opening lies in a dependent position. Blood from the operation may enter the ventricular areas, which is associated with a speaking hydrocephalus. Postoperative hematomas can happen inside the resection cavity, in the extradural compartment, or within the subcutaneous compartment. In the absence of clinically significant mass effect, remark of the spontaneously resolving hematoma might provide the most effective risk�benefit stability. An extradural hematoma can also necessitate evacuation, however may be a definite entity from the epidural hematoma in the setting of an intact calvarium. Optimal dural closure is achieved when using native dura or harvested autologous material. Rare however extreme complications embrace perioperative cranial nerve damage with the problems these suggest, corresponding to corneal abrasions from facial weakness or aspiration pneumonia from decrease cranial nerve injury. Deficits in lower cranial nerves may result in issue swallowing and lack of ability to protect the airway. In many circumstances, patients may require feeding tube placement and a tracheostomy to forestall aspiration pneumonia until they sufficiently recuperate perform. A formal method to decide extubation readiness and swallowing perform is perfect. Intraoperative monitoring might serve as a useful adjunct in the evaluation of swallowing or airway compromise. These issues are more widespread for surgery for extraaxial lesions but could be seen sometimes from any approach in the posterior fossa.
Visual area preservation after multisession cyberknife radiosurgery for perioptic lesions man health 6 health 60 ml rogaine 5 proven. Radiographic findings and morbidity in patients handled with stereotactic radiosurgery prostate cancer treatment drugs rogaine 5 60 ml without a prescription. Pertreatment radiation induced oedema causing acute hydrocephalus after radiosurgery for a number of cerebellar metastases androgen hormone in pregnancy order 60 ml rogaine 5 with amex. Initial expertise with bevacizumab remedy for biopsy confirmed cerebral radiation necrosis mens health 20 worst drinks 60 ml rogaine 5 cheap with amex. Bevacizumab as therapy for radiation necrosis in 4 kids with pontine gliomas. Randomized double-blind placebocontrolled trial of bevacizumab therapy for radiation necrosis of the central nervous system. Bevacizumab as a remedy for radiation necrosis of brain metastases post stereotactic radiosurgery. Bevacizumab for refractory antagonistic radiation results after stereotactic radiosurgery. Long-term outcomes amongst grownup survivors of childhood central nervous system malignancies within the Childhood Cancer Survivor Study. New primary neoplasms of the central nervous system in survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. This abrupt motion leads to a spectrum of neurological harm ranging from mild concussion to severe axonal damage or hemorrhagic lesions that may cause swelling, herniation, and dying. The location and severity of the lesion produced after head trauma is determined by the mechanism of injury, the magnitude of the utilized drive, and the movement of the brain and cerebral vasculature throughout the skull. The healthy brain is suspended throughout the skull by the cerebral spinal fluid, the buoyancy of which reduces its efficient weight from 1500 g to 50 g. The meninges and vasculature also restrict volumetric distortion of the mind, causing it to be primarily prone to shear strain in response to external forces. Brain motion inside the skull results in the coupcontrecoup phenomena the place injuries happen directly beneath factors of impression (coup) as properly as on the surface of the mind reverse to the purpose of harm (contrecoup). Impacts with oblique components to their trajectory exert rotational forces on the brain, causing damage at excessive shear strain points along with the coup-contrecoup places. The anterior frontal and inferior temporal poles are the most common locations of injury. These areas have high shear strains and are adjacent to irregular inside cranium anatomy, growing the risk of both parenchymal and vascular damage. Occipital impacts sometimes trigger contrecoup accidents to the frontal lobe with little coup harm. The dura is supplied by the middle meningeal artery, whereas the mind is equipped by the inner carotid and vertebral arteries, which come collectively at the circle of Willis before branching out to supply the cerebrum. The distal arteries and arterioles travel alongside the floor of the brain before turning into the parenchyma. There is a wealthy capillary network with many anastomoses within the parenchyma, which offers a rich and redundant vascular supply to the neurons and glia. Points of maximal shear strain correlate with the traditional anatomical locations for traumatic hemorrhagic or axonal accidents. When this barrier is disrupted, blood can escape into the encircling areas, where it units off a chain of biochemically poisonous actions. Extravascular blood can result in parenchymal swelling, whereas subarachnoid blood could cause arterial vasospasm and subsequent downstream ischemia. Consistent with this, the arteries can stand up to twice as much axial pressure as veins previous to rupturing. However, arteries can only stretch half as a lot as veins, making them susceptible to rupture when stretched. The aged vasculature can be at greater threat for compromise because of hypertension, amyloid deposition, and decreased compliance. Classically, these lesions come up after impact to the temporal bone inflicting rupture of the center meningeal artery. They are sometimes accompanied by a lucid interval of a quantity of hours previous to neurological deterioration. The arachnoid is avascular, and the only vessels that cross between the arachnoid and dura are the bridging veins, which traverse the potential subdural area between the cortex and venous sinuses. Head trauma causes translation of the brain and arachnoid relative to the dura, stretching, and subsequently rupturing, the bridging veins. They occur primarily at the crowns of gyri as nicely as at places with excessive shear strain described earlier, notably the anterior temporal poles and inferior frontal lobes. Notice how the diploma of midline shift decreases with growing chronicity of the bleed. It occurs after high-speed deceleration injuries, which commonly occur throughout motor vehicle collisions. Primary injury to mind tissue occurs at the time of influence; however, secondary harm additionally occurs due to tissue hypoxia after the primary insult and might contribute to longterm morbidity. A skin incision is made with a scalpel, and a twist drill is used to drill through the cranium. Posterior fossa hemorrhage: Urgent surgical evacuation of hemorrhagic mass lesions in the posterior fossa with suboccipital craniectomy ought to be performed for patients with neurological indicators attributable to the lesion and fourth ventricle compression, basal cistern compression, or obstructive hydrocephalus. The Decompressive Craniectomy in Patients with Severe Traumatic Brain Injury trial lately showed that bifrontal craniectomy resulted in worse outcomes for patients with diffuse intracranial hypertension, which has led to that operation falling out of favor in most facilities. Burr holes are drilled in the cranium and connected with a side-cutting drill, permitting elevation of the bone flap. Dural tack-up sutures are positioned across the edges of the flap to maintain the peripheral dura closely apposed to the cranium, preventing epidural hematoma. The temporal bone is removed laterally until reaching the floor of the middle fossa. The hematoma is evacuated, and any sources of bleeding are identified and controlled. If the swelling is significant, the bone is shipped to a tissue financial institution till cranioplasty could be performed-typically at least three months postoperatively. Initial Management from Trauma bay to Scanner to Operating Room As with all traumas, management of airway, respiration, and hemodynamic stability must be achieved first. If intracranial hemorrhage is suspected as evidenced by pupil dilation, loss of pupil reactivity, or lack of brainstem reflexes, then hyperosmolar remedy may be initiated. If venous sinus harm is suspected, as with penetrating trauma or skull fracture, a delayed postcontrast scan can assess sinus patency. If surgically amenable hematoma is identified, the affected person must be rapidly transported to the working room. If the affected person is hemodynamically secure, 1 g/kg intravenous mannitol must be began. In addition, recombinant elements and concentrated cryoprecipitate may be administered for extreme coagulopathy. Brain tissue oxygenation monitoring permits titration of FiO2 to guarantee adequate tissue oxygenation. Some centers additionally place microdialysis catheters, which allows assessment of metabolites whose levels can replicate native metabolism. These metabolites embrace glucose, lactate, pyruvate, and glycerol, molecules whose levels are altered during hypoperfusion or ischemia. New multimodal neuromonitoring units allow trending of those variables simultaneously over time and facilitate optimal visualization of information tendencies, permitting the intensivist to respect correlations between particular person parameters, which can be utilized to information therapy for every affected person. In addition to the particular neurosurgical issues, these sufferers have similar wants as other critically ill patients, including nutritional help, ventilator help, and long-term care planning, together with rehabilitation, tracheostomy, and percutaneous gastrostomy tube placement. Functional evaluation at discharge showed that 82% of patients have been impartial in expression, 66% have been independent in feeding, and 29% had been unbiased in locomotion. Interestingly, latest knowledge looking at trends of withdrawal of care between multiple facilities noticed that the speed of withdrawal of care varied considerably between facilities. Interestingly, prehospital administration of hypertonic saline, which can temporize patients with hemorrhagic mass lesions until surgical evacuation, additionally increased blood stress.
Buy rogaine 5 60 ml with visa. Dr. Rishma Dhillon Pai - Mens Health.
This may be notably true in the scenario of refractory bupivacaine toxicity prostate 7 price cheap rogaine 5 60 ml overnight delivery,111 hypothermia mens health leg workout rogaine 5 60 ml buy discount online,112 large venous or thrombotic or air embolism mens health gift guide 60 ml rogaine 5 generic with mastercard,113�115 or different potentially reversible causes mens health no gym workout discount rogaine 5 60 ml with mastercard. Ongoing hemorrhage requires steady vigilance and therapy for hemorrhage, coagulopathy, and thrombocytopenia. Post�anoxic ischemic encephalopathy is a direct postoperative concern and can be troublesome to verify early after surgical procedure. The beforehand famous issues regarding utility of hypothermic remedy continue into the postoperative period. A new animal mannequin of cerebral venous infarction: ligation of the posterior a part of the superior sagittal sinus within the cat. Does the impression of elective momentary clipping on intraoperative rupture really influence neurological outcome after surgery for ruptured anterior circulation aneurysms Asymptomatic, unruptured carotid-ophthalmic artery aneurysms: angiographical differentiation of every sort, operative outcomes, and indications. Endovascular embolization of outstanding intercavernous sinuses for profitable transsphenoidal resection of cushing microadenoma: case report. Original memoirs: the control of bleeding in operations for brain tumors: with the description of silver "clips" for the occlusion of vessels inaccessible to the ligature. Spinal metastases from renal cell carcinoma: effect of preoperative particle embolization on intraoperative blood loss. Blood loss in major backbone surgical procedure: are there effective measures to lower massive hemorrhage in major spine fusion surgical procedure Prone versus knee-chest position for microdiscectomy: a prospective randomized research of intra-abdominal pressure and intraoperative bleeding. The effect of patient positioning on intraabdominal strain and blood loss in spinal surgical procedure. A comparability of move charges and warming capabilities of the Level 1 and fast infusion system with varioussize intravenous catheters. Reversal of rivaroxaban and dabigatran by prothrombin complex focus: a randomized, placebo-controlled, crossover study in wholesome subjects. Discontinue volatile agents and succinylcholine; get assist; get dantrolene; notify surgeon 2. Consideration could be given to reversal of some anesthetic results with naloxone or flumazenil, however with cautious consideration of potential unwanted effects of hypertension116 and/or seizure. Dangerously low temperature needs to be treated due to risk of arrhythmias, central nervous system melancholy, and coagulopathy. Conversely these sufferers are susceptible to fever,118 and this must be aggressively prevented or treated. Typically the affected person will arrive with the surgical wound rapidly closed, full of gauze or fabric, or simply coated with a drape. Administration of antibiotics seems applicable, and as quickly as possible a return to the working room may be wanted to complete the surgical procedure, complete hemostatic procedures, or just present for sterile wound closure. They usually arise from a wide selection of commonly interacting components related to affected person anatomy and pathology; surgical position; expertise of anesthesia and neurosurgery groups; and disparate hospital elements related to experience, protocols in place, and resource availability. Severe blood loss throughout spinal reconstructive procedures: the potential usefulness of topical hemostatic agents. Determinants of neurological end result after surgery for mind arteriovenous malformation. Hypothermic coagulopathy in trauma: impact of varying ranges of hypothermia on enzyme velocity, platelet perform, and fibrinolytic exercise. Regional anesthesia in the patient receiving antithrombotic or thrombolytic remedy: American Society of Regional Anesthesia and Pain Medicine EvidenceBased Guidelines (third edition). The significance of thrombocytopenia within the development of postoperative intracranial hematoma. Critical care issues in the management of the trauma patient following initial resuscitation. Transfusion strategies and improvement of acute respiratory distress syndrome in combat casualty care. Severe intraoperative air embolism throughout convexity meningioma surgical procedure in the supine place: case report. An unusual entrance web site of venous air embolism throughout operations in the sitting place. Effect of air exposure and suction on blood cell activation and hemolysis in an in vitro cardiotomy suction model. The pathophysiology of mind swelling produced by mechanical trauma and hypertension. Is ligation and division of anterior third of superior sagittal sinus really safe Craniotomy for supratentorial brain tumors: risk elements for mind swelling after opening the dura mater. Acute intraoperative brain herniation during elective neurosurgery: pathophysiology and administration considerations. A review of mind retraction and recommendations for minimizing intraoperative brain injury. Anesthesia considerations and intraoperative monitoring throughout surgery for arteriovenous malformations and dural arteriovenous fistulas. Traumatic bilateral jugular vein thrombosis: case report and evaluate of the literature. Monitoring and intraoperative management of elevated intracranial strain and decompressive craniectomy. Brain oedema in focal ischaemia: molecular pathophysiology and theoretical implications. Delayed emergence from anesthesia resulting from posterior cerebral artery infarction after Guglielmi detachable coil embolization. Tongue necrosis and cleft after extended transesophageal echocardiography probe placement. Unilateral transient sialadenopathy: one other complication of oropharyngeal airway. Brief review: airway rescue with insertion of laryngeal mask airway units with sufferers within the susceptible place. Emergency airway management with fiberoptic intubation in the prone place with a exhausting and fast flexed neck. Major vascular harm during anterior lumbar spinal surgical procedure: incidence, risk components, and administration. Retroperitoneal hematoma as a severe complication of endovascular aneurysmal coiling. Practice guidelines for administration of the difficult airway: an up to date report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Successful resuscitation of bupivacaine-induced cardiac arrest utilizing cardiopulmonary bypass. When should cardiopulmonary bypass be used within the setting of severe hypothermic cardiac arrest Surgical treatment of acute large pulmonary embolism using momentary cardiopulmonary bypass. Fulminant pulo monary embolism handled by extracorporeal membrane oxygenation in a affected person with traumatic mind harm. Massive carbon dioxide fuel embolism: a near catastrophic scenario averted by use of cardiopulmonary bypass. Impact of fever on consequence in sufferers with stroke and neurologic injury: a comprehensive metaanalysis. Mild therapeutic hypothermia to improve the neurologic end result after cardiac arrest. Delayed emergence from anesthesia ensuing from bilateral epidural hemorrhages during cervical backbone surgery. Delayed emergence from anesthesia ensuing from cerebellar hemorrhage throughout cervical spine surgery. A case of delayed emergence from anesthesia caused by postoperative mind edema associated with sudden cerebral venous sinus thrombosis. Endovascular therapy of venous sinus thrombosis: a case report and evaluate of the literature. A prospective audit of critical incidents in anaesthesia in a university instructing hospital.
The ribbon is coloured from blue to pink because the polypeptide goes from N- to C-terminus prostate volume calculator rogaine 5 60 ml generic free shipping. The energetic web site is identified by the catalytic product galactose prostate oncology qpi buy cheap rogaine 5 60 ml on-line, shown in sphere Corey-Pauling-Koltun format prostate frequent urination 60 ml rogaine 5 purchase with amex. Electron microscopy showing lamellated membrane inclusion our bodies with both "myelin-like" (C) or "zebroid" (D) look in secondary lysosomes mens health 2012 grooming awards 60 ml rogaine 5 purchase mastercard. Acroparesthesia or neuropathic pain in hands or ft starting in later childhood, precipitated by sickness, fever, exercise, emotional stress, or exposure to heat 2. Any combination of two or more of these issues is extremely suggestive of Fabry illness in both intercourse. The index case (arrow) was diagnosed by a nationwide case-finding study amongst Austrian patients undergoing dialysis. His mom and the 2 daughters (dot) carry the identical mutation and were asymptomatic at the time of screening. Results of a nationwide screening for Anderson-Fabry illness amongst dialysis sufferers. Pain (and depression) management brokers embrace gabapentin, carbamazepine, phenytoin, amitriptyline, and other antidepressants. The 5-year survival after kidney transplantation can also be decrease than that of controls. It can be thought-about for each adult male affected person, for symptomatic boys, and for symptomatic girls. Two preparations are presently out there, with other merchandise in clinical improvement. The first, Agalsidase alfa (Replagal, Shire Human Genetic Therapies, Lexington, Massachusetts), is produced in human skin fibroblasts with gene activation technology. The other product, agalsidase beta (Fabrazyme, Sanofi Genzyme, Cambridge, Massachusetts), is produced in Chinese hamster ovary cells and is registered to be used at 1. Fabrazyme is the one currently available enzyme alternative in the United States. Side effects of enzyme substitute therapy include fever, rigors, and chills, sometimes delicate to average in nature. These occur in more than half of the sufferers during the first months of remedy. Infusion-related reactions may be because of IgG or IgE antibodies that have been detected in several sufferers. In case of reactions, the infusion fee ought to be decreased or stopped, and the administration of antihistamines and/ or corticosteroids should be thought-about. Some sufferers want premedication with antihistamines, paracetamol/ acetaminophen, or corticosteroids. In sufferers receiving upkeep dialysis remedy, the infusion could be administered throughout dialysis treatment. The medical effect of both merchandise was examined in two small pivotal trials, a couple of controlled studies, and numerous uncontrolled research and registry reports. Neuropathic ache, the first endpoint, improved throughout remedy with Agalsidase alpha as assessed by a ache questionnaire. After 20 weeks of treatment (11 infusions), 20 of the 29 individuals (69%) within the Agalsidase beta group had no microvascular endothelial Gb3 deposits, as in contrast with zero of 29 individuals within the placebo group. Among secondary endpoints, there was no distinction in ache between energetic therapy and placebo. A per-protocol evaluation, adjusted for baseline proteinuria, nevertheless, suggested an impact of Agalsidase beta as in contrast with placebo. Uncontrolled studies recommend stabilization and even improvement of kidney and coronary heart illness manifestations during enzyme alternative therapy in plenty of sufferers. Quality-of-life, gastrointestinal signs, hypohidrosis, pulmonary obstruction, and different clinical signs additionally confirmed improvement. Kidney function, proteinuria, and blood strain are necessary predictors of the kidney response to enzyme replacement remedy. In a current analysis of 213 patients treated with Agalsidase beta for at least 2 years enrolled in the Fabry Registry, a higher urinary protein stage, worse initial kidney function, and delayed initiation of enzyme substitute remedy after the onset of signs were robust predictors of kidney disease progression in males. Patients with 24-hour protein excretion higher than 1 g/24 hour had worse kidney function at baseline and follow-up in contrast with patients with protein excretion of 500 to one thousand mg/24 hour or lower than 500 mg/24 hour. Kidney function was worse in sufferers with baseline hypertension, and there was a more fast annual decline in contrast with normotensive patients. Thus novel therapeutic methods are wanted to improve outcomes in sufferers with Fabry illness. An in vitro assay can be used to determine topics with mutations which may be prone to reply to chaperone remedy. Kidney biopsy samples have been obtainable for sixty four patients and showed a 50% discount within the number of Gb3 inclusions per kidney interstitial capillary in 41% of sufferers who acquired migalastat hydrochloride and 28% of patients who obtained placebo (P = zero. Of note, among 45 patients with responsive mutations, therapy with migalastat hydrochloride was related to a larger reduction within the imply variety of Gb3 inclusions per kidney interstitial capillary compared with placebo (-0. Among different secondary endpoints, therapy with migalastat hydrochloride lowered plasma levels of lyso-Gb3 and gastrointestinal signs however confirmed no effect on urinary Gb3, kidney operate, or left ventricular mass. In the lysosome, dissociation of migalastat restores enzyme exercise and permits degradation of Gb3. Taken collectively, these knowledge suggest an essential medical potential for this new therapeutic device, alone or together with enzyme replacement remedy. Natural history of Fabry renal disease: influence of alpha-galactosidase A activity and genetic mutations on medical course. Cardiac manifestations of Anderson-Fabry illness: outcomes from the international Fabry consequence survey. Neonatal screening for lysosomal storage issues: feasibility and incidence from a nationwide study in Austria. Fabry illness: development of nephropathy, and prevalence of cardiac and cerebrovascular occasions before enzyme replacement remedy. Perazella Primary interstitial kidney disease makes up a various group of ailments that elicit interstitial irritation related to renal tubular cell injury. Traditionally, interstitial nephritis has been classified morphologically and clinically into acute and persistent forms. This process sometimes spares each glomerular and vascular buildings, and is mentioned more fully in Chapter 33. Over time, glomerular and vascular constructions are involved, with progressive fibrosis and sclerosis within the kidney. As the renal epithelium develops from the metanephric mesenchyme by way of a means of mesenchymalepithelial transition, observations recommend a novel paradigm of tubulointerstitial response to damage whereby dedifferentiation pathways are activated inside the epithelium, leading to a transition to cells of more mesenchymal characteristics. The ability of renal tubular epithelial cells to transform in vitro to fibroblasts and myofibroblasts is nicely documented. Future studies will likely higher characterize pathways that both initiate and propagate renal fibrogenic processes. Glomerular and vascular structures could also be comparatively preserved early in the midst of disease but ultimately turn into involved in progressive fibrosis and sclerosis. All forms of progressive kidney disease eventually end in persistent and progressive interstitial fibrosis. One hypothesis regarding immune recognition of the interstitium suggests that portions of infectious particles or drug molecules may cross-react with or alter endogenous kidney antigens. An immune response directed towards these inciting agents would subsequently also goal the interstitium. Light microscopy findings demonstrate focal collections of lymphocytes and pronounced lack of normal tubulointerstitial architecture. There is proof of tubular dilation and atrophy, as properly as interstitial fibrosis and relative sparing of glomerular structures. Laboratory findings in these patients include low-grade (tubular) proteinuria, microscopic hematuria, and sterile pyuria. The paradigm of tubular epithelial-mesenchymal transition suggests an additional pathway to kidney fibrosis, in that tubular epithelium undergoes profound phenotypic modifications after publicity to fibrogenic stimuli (center box). This leads to loss of epithelial traits and acquire of mesenchymal traits. The transitioning cells might stay within the tubular wall or migrate into the interstitium.