
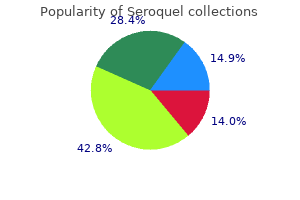
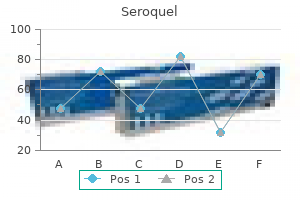
Seroquel
| Contato
Página Inicial

"Purchase 300 mg seroquel, medicine head".
K. Gorn, M.B.A., M.B.B.S., M.H.S.
Vice Chair, Texas A&M Health Science Center College of Medicine
Otitis Externa the time period otitis externa refers to a set of illnesses involving primarily the auditory meatus symptoms you may be pregnant buy seroquel 50 mg with visa. Otitis externa normally outcomes from a combination of heat symptoms 8 days after ovulation generic seroquel 200 mg, retained moisture symptoms uric acid 50 mg seroquel cheap mastercard, and desquamation and maceration of the epithelium of the outer ear canal medicine 801 300 mg seroquel cheap free shipping. Heat, humidity, and the lack of protective cerumen lead to extreme moisture and elevation of the pH in the ear canal, which in turn lead to skin maceration and irritation. Infection may then happen; the predominant pathogen is P aeruginosa, although different gram-negative. The sickness often starts with itching and progresses to severe pain, which is usually triggered by manipulation of the pinna or tragus. The onset of pain is generally accompanied by the development of an erythematous, swollen ear canal, typically with scant white, clumpy discharge. Treatment consists of cleansing the canal to take away debris and to improve the exercise of topical therapeutic agents-usually hypertonic saline or mixtures of alcohol and acetic acid. Clinicians should contemplate inflammatory issues as a potential cause of exterior ear irritation, particularly within the absence of local or regional adenopathy. Aside from the extra salient causes of inflammation, such as trauma, insect chew, and overexposure to daylight or extreme cold, the differential analysis should include much less common situations, corresponding to autoimmune issues. It presents with the everyday signs and symptoms of a skin/ delicate tissue infection, with tenderness, erythema, swelling, and warmth of the exterior ear (particularly the lobule), but without apparent involvement of the ear canal or inside structures. Treatment consists of warm compresses and oral antibiotics such as dicloxacillin that are lively against typical pores and skin and gentle tissue pathogens (specifically, S. Chronic otitis externa is triggered primarily by repeated native irritation, mostly arising from persistent drainage from a persistent middle-ear infection. Other causes of repeated irritation, corresponding to insertion of cotton swabs or other foreign objects into the ear canal, can lead to this situation, as can uncommon continual infections corresponding to syphilis, tuberculosis, or leprosy. Chronic otitis externa typically presents as erythematous, scaling dermatitis in which the predominant symptom is pruritus somewhat than pain; this situation must be differentiated from a quantity of others that produce an identical clinical image, similar to atopic dermatitis, seborrheic dermatitis, psoriasis, and dermatomycosis. Invasive otitis externa, also recognized as malignant or necrotizing otitis externa, is an aggressive and doubtlessly lifethreatening disease that occurs predominantly in aged diabetic sufferers and different immunocompromised sufferers. The illness begins within the external canal, progresses slowly over weeks to months, and often is difficult to distinguish from a severe case of continual otitis externa due to the presence of purulent otorrhea and an erythematous swollen ear and exterior canal. Severe, deep-seated otalgia is often noted and might help differentiate invasive from persistent otitis externa. If left unchecked, the infection can migrate to the base of the cranium (resulting in skull-base osteomyelitis) and on to the meninges and brain, with a high associated mortality price. Cranial nerve involvement is often seen, with the facial nerve often affected first and most often. In all cases, the exterior ear canal must be cleansed, and a biopsy specimen of the granulation tissue within the canal (or of deeper tissues) ought to be obtained for culture of the offending organism. A fluoroquinolone antibiotic is regularly used instead of the aminoglycoside and may even be administered orally, given the excellent bioavailability of this drug class. Cases of invasive Pseudomonas otitis externa recognized within the early stages can typically be handled with oral and otic fluoroquinolones alone, albeit with shut follow-up. The inflammatory response to these circumstances results in the event of a sterile transudate inside the middle-ear and mastoid cavities. Infection might occur if micro organism or viruses from the nasopharynx contaminate this fluid, producing an acute (or generally chronic) sickness. The proliferation of those pathogens on this house results in the development of the typical signs and symptoms of acute middle-ear infection. The diagnosis of acute otitis media requires the demonstration of fluid in the center ear (with tympanic membrane immobility) and the accompanying signs or signs of native or systemic sickness (Table 16-2). Viruses, corresponding to these talked about above, have been recovered either alone or with micro organism in 17�40% of circumstances. Clinical Manifestations Fluid in the center ear is often demonstrated or confirmed with pneumatic otoscopy. In the absence of fluid, the tympanic membrane strikes visibly with the appliance of constructive and adverse stress, but this movement is dampened when fluid is current. With bacterial infection, the tympanic membrane can be erythematous, bulging, or retracted and sometimes can spontaneously perforate. The indicators and symptoms accompanying an infection could be local or systemic, together with otalgia, otorrhea, diminished listening to, fever, or irritability. Other indicators and signs which might be occasionally reported include vertigo, nystagmus, and tinnitus. Sources: American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media, 2004; Dowell et al, 1998. Although most cases resolve clinically 1 week after the onset of illness, antibiotics seem to be of some benefit. A higher proportion of treated than of untreated sufferers are freed from illness 3�5 days after diagnosis. The difficulty of predicting which patients will benefit from antibiotic therapy has led to totally different approaches. In distinction, many specialists in the United States continue to recommend antibiotic remedy for youngsters <6 months old in light of the higher frequency of secondary complications in this younger and functionally immunocompromised population. However, observation without antimicrobial remedy is now typically considered an affordable possibility within the United States for gentle to moderate illness in children 6 months to 2 years of age with an uncertain prognosis and for kids 2 years of age (Table 16-2). Given that nearly all research of the etiologic agents of acute otitis media constantly document similar pathogen profiles, remedy is mostly empirical, besides in those few instances the place tympanocentesis is warranted-e. Therapy for uncomplicated acute otitis media is usually administered for 5�7 days to patients 6 years old; longer programs. Recurrent Acute Otitis Media Recurrent acute otitis media (more than three episodes inside 6 months or 4 episodes within 12 months) is mostly due to relapse or reinfection, although knowledge point out that nearly all of early recurrences are new infections. In general, the same pathogens responsible for acute otitis media trigger recurrent disease; even so, the beneficial remedy consists of antibiotics active in opposition to -lactamase-producing organisms. Other approaches, together with placement of tympanostomy tubes, adenoidectomy, and tonsillectomy plus adenoidectomy, are of questionable total value, given the relatively small benefit compared with the potential for issues. Serous Otitis Media In serous otitis media (otitis media with effusion), fluid is present in the center ear for an extended period and in the absence of indicators and symptoms of an infection. In some circumstances, nonetheless (in explicit after an episode of acute otitis media), effusions can persist for months. These persistent effusions are often associated with a big hearing loss in the affected ear. In youthful youngsters, persistent effusions and decreased listening to may be associated with impairment of language acquisition expertise. Antibiotic therapy or myringotomy with insertion of tympanostomy tubes is typically reserved for sufferers in whom bilateral effusion (1) has endured for a minimal of three months and (2) is associated with important bilateral listening to loss. Chronic Otitis Media Chronic suppurative otitis media is characterised by persistent or recurrent purulent otorrhea in the setting of tympanic membrane perforation. Inactive illness is characterized by a central perforation of the tympanic membrane, which permits drainage of purulent fluid from the middle ear. When the perforation is more peripheral, squamous epithelium from the auditory canal might invade the center ear through the perforation, forming a mass of keratinaceous particles (cholesteatoma) on the web site of invasion. Treatment of chronic energetic otitis media is surgical; mastoidectomy, myringoplasty, and tympanoplasty can be performed as outpatient surgical procedures, with an overall success fee of 80%. Chronic inactive otitis media is tougher to cure, often requiring repeated programs of topical antibiotic drops during times of drainage. Mastoiditis Acute mastoiditis was relatively common among kids earlier than the introduction of antibiotics. Early and frequent therapy of acute otitis media is most likely the explanation that the incidence of acute mastoiditis has declined to just one. In countries just like the Netherlands, the place antibiotics are used sparingly for acute otitis media, the incidence price of acute mastoiditis is roughly twice that in nations like the United States. However, neighboring Denmark has a fee of acute mastoiditis similar to that in the Netherlands however an antibiotic-prescribing rate for acute otitis media more much like that in the United States. Patients usually present with pain, erythema, and swelling of the mastoid process together with displacement of the pinna, normally along side the typical signs and signs of acute middle-ear infection. Initial empirical remedy is usually directed in opposition to the typical organisms associated with acute otitis media, corresponding to S. Some sufferers with more severe or extended programs of illness must be handled for an infection with S. Broad empirical therapy is often narrowed as quickly as culture results become obtainable.
![Meadows syndrome[disambiguation needed]](https://cmaan.pa.gov.br/pharmshop/seroquel/katyarog/galqo1.jpg)
Regulation of Virulence Gene Expression In each toxin-mediated and non�toxin-mediated illnesses because of medicine bobblehead fallout 4 seroquel 100 mg cheap line S treatment lower back pain discount 50 mg seroquel with amex. The regulatory gene agr is part of a quorum-sensing sign transduction pathway that senses and responds to bacterial density medicine in the middle ages 200 mg seroquel buy. In contrast 10 medications doctors wont take 50 mg seroquel free shipping, many secreted proteins, such as toxin, the enterotoxins, and assorted enzymes, are launched during the postexponential progress part. The subsequent release of varied enzymes permits the colony to acquire nutritional support and permits bacteria to spread to adjacent tissues. Studies with mutant strains by which these regulatory genes are inactivated present reduced virulence in several animal fashions of S. For these organisms to invade the host and trigger an infection, some or the entire following steps are necessary: inoculation and native colonization of tissue surfaces, invasion, evasion of the host response, and metastatic spread. The initiation of staphylococcal infection requires a breach in cutaneous or mucosal obstacles. Colonizing strains or strains transferred from other individuals are inoculated into damaged pores and skin, a wound, or the bloodstream. After their introduction right into a tissue website, micro organism replicate and colonize the host tissue surface. Binding to these units typically involves staphylococcal adherence to serum constituents that have coated the gadget surface. The lipases may facilitate survival in lipid-rich areas such as the hair follicles, the place S. The staphylococcal cell wall- consisting of alternating N-acetylmuramic acid and N-acetylglucosamine units together with an additional cell wall part, lipoteichoic acid-can provoke an inflammatory response that features the sepsis syndrome. Staphylococcal toxin, which causes pore formation in varied eukaryotic cells, can also initiate an inflammatory response with findings suggestive of sepsis. Evasion of Host Defense Mechanisms the anterior nares is the principal site of staphylococcal colonization in people. Other elements which will contribute to colonization embody the influence of other resident nasal flora and their bacterial density, nasal mucosal injury. It additionally results in mobile modifications, such because the expression of integrins and Fc receptors that will contribute to systemic manifestations of disease, together with sepsis and vasculitis. These menadione and hemin auxotrophic mutants are usually poor in toxin and may persist inside endothelial cells. Small-colony variants are sometimes chosen after aminoglycoside therapy and are more commonly found in websites of persistent infections. These variants represent one other mechanism for extended staphylococcal survival that will improve the chance of recurrences. Groups at Increased Risk of Infection Some illnesses seem to entail a quantity of threat factors for S. Other teams in danger embrace people with skin abnormalities and people with prosthetic gadgets. The enterotoxins can then bind T-cell receptors via the v chain, leading to a dramatic overexpansion of T-cell clones (up to 20% of the entire T-cell population). A different area of the enterotoxin molecule is liable for the symptoms of food poisoning. The enterotoxins are heat secure and may survive circumstances that kill the micro organism. Although the mechanism of this disruption stays unsure, studies counsel that the toxins possess serine protease activity, which-through undefined mechanisms-triggers exfoliation. These infections are characterised by the formation of pus-containing blisters, which regularly begin in hair follicles and unfold to adjoining tissues. Folliculitis is a superficial infection that includes the hair follicle, with a central area of purulence (pus) surrounded by induration and erythema. Furuncles (boils) are extra in depth, painful lesions that are inclined to happen in bushy, moist areas of the physique and prolong from the hair follicle to turn into a true abscess with an area of central purulence. The infection, which typically presents within 2�3 weeks after delivery, is characterized by findings that vary from cellulitis to abscess formation. It should be famous that many of those syndromes may also be as a result of group A streptococci or, much less commonly, to other streptococcal species. When needed, bone biopsies for tradition and histopathologic examination are normally diagnostic. These infections may present as intense again pain and fever, however can also be clinically occult, presenting as persistent back ache and low-grade fever. Contamination of tradition material from adjoining tissue can make the prognosis of osteomyelitis difficult within the absence of pathologic affirmation. This an infection is quickly progressive and may be associated with intensive joint destruction if left untreated. In adults, arthritis may result from trauma, surgery, or hematogenous dissemination. Infection incessantly develops in joints previously broken by osteoarthritis or rheumatoid arthritis. Iatrogenic infections resulting from aspiration or injection of brokers into the joint also happen. In these settings, the affected person experiences elevated pain and swelling within the concerned joint in association with fever. Distinguishing bacterial pneumonia from respiratory failure of different causes or new pulmonary infiltrates in critically sick patients is often difficult and depends on a constellation of clinical, radiologic, and laboratory findings. Patients could present with fever, bloody sputum production, and midlung-field pneumatoceles or multiple, patchy pulmonary infiltrates. The frequency of metastatic seeding during bacteremia has been estimated to be as excessive as 31%. Recognition of those problems by scientific and laboratory diagnostic strategies alone is often difficult. The well-described progression of hemodynamic changes- starting with respiratory alkalosis and clinical findings of hypotension and fever-is generally seen. Other components related to an elevated risk of endocarditis are injection drug use, hemodialysis, the presence of intravascular prosthetic gadgets, and immunosuppression. Despite the availability of efficient antibiotics, mortality rates from these infections proceed to range from 20 to 40%, relying on each the host and the nature of the an infection. In each of those settings, the analysis is established by recognition of clinical stigmata suggestive of endocarditis. In the absence of antecedent antibiotic remedy, blood cultures are almost uniformly optimistic. Chest x-rays reveal proof of septic pulmonary emboli (small, peripheral, circular lesions that may cavitate with time). Individuals with antecedent cardiac valvular harm extra generally current with left-sided native-valve endocarditis involving the previously affected valve. These patients tend to be older than those with right-sided endocarditis, their prognosis is worse, and their incidence of problems (including peripheral emboli, cardiac decompensation, and metastatic seeding) is larger. This an infection is especially fulminant within the early postoperative interval and is associated with a high mortality price. These infections usually contain intravascular catheters, prosthetic valves, orthopedic gadgets, peritoneal or intraventricular catheters, left-ventricularassist units, and vascular grafts. It is comparatively frequent for a pyogenic collection to be current on the gadget site. Aspiration of these collections and efficiency of blood cultures are necessary parts in establishing a analysis. As in most prosthetic-device infections, successful remedy often entails removal of the device. Left in place, the system is a possible nidus for both persistent or recurrent infections. Hypotension: systolic blood stress of ninety mmHg, or orthostatic hypotension (orthostatic drop in diastolic blood strain by 15 mmHg, orthostatic syncope, or orthostatic dizziness) three. Diffuse macular rash with subsequent desquamation in 1�2 weeks after onset (including the palms and soles) 4. Renal: blood urea nitrogen or serum creatinine stage 2 occasions the normal upper restrict d. Muscular: severe myalgias or serum creatine phosphokinase degree 2 instances the upper limit g. Negative serologic or other checks for measles, leptospirosis, and Rocky Mountain spotted fever, in addition to adverse blood or cerebrospinal fluid cultures for organisms aside from S.
Asymptomatic bacteriuria is extra frequent amongst elderly men and women medications safe during breastfeeding cheap seroquel 100 mg without prescription, with rates as excessive as 40�50% in some studies symptoms of strep throat generic 300 mg seroquel mastercard. The incidence of acute uncomplicated pyelonephritis among community-dwelling girls 18�49 years of age is 28 circumstances per 10 3 medications that cannot be crushed seroquel 300 mg buy generic on line,000 women medications covered by medicare purchase 300 mg seroquel free shipping. Escherichia coli causes 80% of acute infections (both cystitis and pyelonephritis) in patients without catheters, urologic abnormalities, or calculi. About one-third of ladies with dysuria and frequency have either an insignificant number of bacteria in midstream urine cultures or completely sterile cultures and have been beforehand defined as having the urethral syndrome. These agents are discovered most frequently in younger, sexually active ladies with new sexual partners. Adenoviruses cause acute hemorrhagic cystitis in youngsters and in some young adults, typically in epidemics. Colonization of the urine of catheterized or diabetic sufferers by Candida and other fungal species is common and generally progresses to symptomatic invasive an infection (Chap. Ascent of micro organism from the bladder might observe and is probably the pathway for most renal parenchymal infections. In females vulnerable to the development of cystitis, nevertheless, enteric gram-negative organisms residing in the bowel colonize the introitus, the periurethral skin, and the distal urethra nedasalamatebook@gmail. The elements that predispose to periurethral colonization with gramnegative bacilli remain poorly understood, however alteration of the conventional vaginal flora by antibiotics, different genital infections, or contraceptives (especially spermicide) appears to play an essential role. Loss of the usually dominant H2O2-producing lactobacilli from the vaginal flora appears to facilitate colonization by E. Small numbers of periurethral micro organism in all probability acquire entry to the bladder frequently, and this process is facilitated in some instances by urethral massage during intercourse. Whether bladder infection ensues is dependent upon interacting effects of strain pathogenicity, inoculum measurement, and local and systemic host protection mechanisms. Under regular circumstances, bacteria positioned in the bladder are rapidly cleared, partly by way of the flushing and dilutional effects of voiding, but also on account of the antibacterial properties of urine and the bladder mucosa. Owing largely to a high urea concentration and high osmolarity, the bladder urine of many wholesome persons inhibits or kills bacteria. Metastatic staphylococcal or candidal infections of the kidney might observe bacteremia or fungemia, spreading from distant foci of an infection in the bone, skin, or vasculature or elsewhere. An important issue predisposing to bacteriuria in males is urethral obstruction because of prostatic hypertrophy. Insertive rectal intercourse can be related to an increased threat of cystitis in males. Symptomatic higher tract infections, in particular, are unusually frequent throughout being pregnant; absolutely 20�30% of pregnant ladies with asymptomatic bacteriuria subsequently develop pyelonephritis. This predisposition to higher tract an infection during pregnancy results from decreased ureteral tone, decreased ureteral peristalsis, and momentary incompetence of the vesicoureteral valves. Infection superimposed on urinary tract obstruction might result in rapid destruction of renal tissue. It is of utmost significance, therefore, when an infection is present, to identify and repair obstructive lesions. The an infection could additionally be initiated by means of catheters for bladder drainage and is favored by the prolonged stasis of urine within the bladder. An additional factor typically operative in these circumstances is bone demineralization because of immobilization, which causes hypercalciuria, calculus formation, and obstructive uropathy. Vesicoureteral Reflux Defined as reflux of urine from the bladder cavity up into the ureters and typically into the renal pelvis, vesicoureteral reflux occurs throughout voiding or with elevation of strain within the bladder. In practice, this situation is detected as retrograde movement of radiopaque or radioactive materials throughout a voiding cystourethrogram. Voiding after intercourse reduces the risk of cystitis, most likely as a result of it promotes the clearance of micro organism launched throughout intercourse. Use of spermicidal compounds with a diaphragm or cervical cap or use of spermicide-coated condoms dramatically alters the conventional introital bacterial flora and has been associated with marked increases in vaginal colonization with E. Vesicoureteral reflux is common amongst children with anatomic abnormalities of the urinary tract or with anatomically normal however infected urinary tracts. These uropathogenic clones have accrued a quantity of virulence genes that are often intently linked on the bacterial chromosome in "pathogenicity islands. The quantity and type of receptors on uroepithelial cells to which micro organism might connect are, at least partly, genetically decided. Many of these structures are components of blood group antigens and are current on both erythrocytes and uroepithelial cells. Conversely, P blood group�negative individuals, who lack these receptors, are at decreased risk of pyelonephritis. Fever or an elevated C-reactive protein degree usually accompanies acute pyelonephritis and is present in uncommon cases of cystitis, but in addition occurs in infections other than pyelonephritis. Cystitis Patients with cystitis normally report dysuria, frequency, urgency, and suprapubic ache. The urine typically turns into grossly cloudy and malodorous and is bloody in 30% of circumstances. White cells and bacteria can be detected by examination of unspun urine generally. Physical examination usually reveals only tenderness of the urethra or the suprapubic space. If a genital lesion or a vaginal discharge is obvious, particularly in conjunction with <105 bacteria per milliliter on urine culture, then pathogens that may cause urethritis, vaginitis, or cervicitis. Acute Pyelonephritis Symptoms of acute pyelonephritis typically develop quickly over a few hours or a day and embody fever, shaking chills, nausea, vomiting, stomach ache, and diarrhea. Besides fever, tachycardia, and generalized muscle tenderness, bodily examination generally reveals marked tenderness on deep stress in one or both costovertebral angles or on deep abdominal palpation. Some patients have mild disease; in others, signs and signs of gram-negative sepsis predominate. Most sufferers have significant leukocytosis and bacteria detectable in Gram-stained unspun urine. Leukocyte casts are present in the urine of some patients, and the detection of those casts is pathognomonic. Hematuria may be demonstrated through the acute phase of the disease; if it persists after acute manifestations of an infection have subsided, a stone, a tumor, or tuberculosis must be considered. Except in individuals with papillary necrosis, abscess formation, or urinary obstruction, the manifestations of acute pyelonephritis normally respond to applicable remedy inside 48�72 h. In extreme pyelonephritis, fever subsides extra slowly and may not disappear for a number of days, even after acceptable antibiotic therapy has been instituted. Persistence of fever or of signs and indicators beyond 72 h suggests the need for urologic imaging. Urethritis Of women with acute dysuria, frequency, and pyuria, 30% have midstream urine cultures with either no growth or insignificant bacterial progress. In this case, a distinction ought to be made between women contaminated with sexually transmitted pathogens. Chlamydial or gonococcal an infection must be suspected in women with a gradual onset of illness, no hematuria, no suprapubic pain, and >7 days of signs. The additional historical past of a recent sex-partner change, particularly if the partner has just lately had chlamydial or gonococcal urethritis, should heighten the suspicion of a sexually transmitted an infection, as ought to the finding of mucopurulent cervicitis (Chap. Infection occurs when micro organism attain the bladder by certainly one of two routes: migration through the column of urine in the catheter lumen (intraluminal route) or up the mucous sheath exterior the catheter (periurethral route). Bacteria normally enter the catheter system at the catheter�collecting tube junction or on the drainage bag portal. Bacterial progress in biofilms on the catheter ultimately produces encrustations consisting of bacteria, bacterial glycocalyces, host urinary proteins, and urinary salts. These encrustations present a refuge for bacteria and may defend them from antimicrobial agents and phagocytes. Clinically, catheter-associated infections often trigger minimal signs without fever and often resolve after withdrawal of the catheter. The frequency of higher tract infection associated with catheter-induced bacteriuria is unknown. The catheterized urinary tract has repeatedly been shown to be the most typical source of gramnegative bacteremia in hospitalized sufferers, typically accounting for 30% of cases. The use of catheters impregnated with antimicrobial brokers reduces the incidence of asymptomatic bacteriuria in sufferers catheterized for <2 weeks. Despite precautions, nearly all of sufferers catheterized for >2 weeks eventually develop bacteriuria.
This information will undoubtedly lead to medications 319 buy 300 mg seroquel visa a better understanding of the pathogenesis of leptospirosis medications you cant take with grapefruit buy seroquel 200 mg with mastercard. The pathogenic leptospires are divided into serovars based on medicine man 1992 seroquel 200 mg buy cheap on-line their antigenic composition treatment 4 ulcer 300 mg seroquel discount mastercard. Leptospires are coiled, thin, highly motile organisms with hooked ends and two periplasmic flagella that let burrowing into tissue. They stain poorly however could be seen microscopically by dark-field examination and after silver impregnation staining. Leptospires require special media and situations for progress; it might take weeks for cultures to become positive. Rodents, particularly rats, are the most important reservoir, though different wild mammals in addition to home and farm animals may harbor leptospires. For example, a large outbreak occurred in 1998 amongst athletes after a triathlon in Illinois. Ingestion of one or more swallows of lake water was a distinguished threat factor for sickness. Heavy rains that preceded the triathlon, with consequent agricultural runoff, are likely to have increased the level of leptospiral contamination in the lake water. In 2000, eighty members contracted leptospirosis throughout an Eco-Challenge multisport endurance race in Malaysian Borneo. In a study in the Netherlands, 14% of patients with confirmed leptospirosis had acquired the infection whereas traveling in tropical countries, most often in Southeast Asia. Leptospirosis develops sometimes after unanticipated immersion in contaminated water. The most necessary identified pathogenic properties of leptospires are adhesion to cell surfaces and cellular toxicity. Although leptospires primarily infect the kidneys and liver, any organ may be affected. In the kidney, leptospires migrate to the interstitium, renal tubules, and tubular lumen, inflicting interstitial nephritis and tubular necrosis. Hypovolemia due to dehydration or altered capillary permeability might contribute to the development of renal failure. Invasion of skeletal muscle by leptospires ends in swelling, vacuolation of the myofibrils, and focal necrosis. In extreme leptospirosis, vasculitis could in the end impair the microcirculation and improve capillary permeability, leading to fluid leakage and hypovolemia. When antibodies are formed, leptospires are eliminated from all sites within the host except the attention, the proximal renal tubules, and maybe the mind, where they may persist for weeks or months. The persistence of leptospires in the aqueous humor often causes persistent or recurrent uveitis. The systemic immune response is efficient in eliminating the organism but can also produce symptomatic inflammatory reactions. A rise in antibody titer coincides with the event of meningitis; this association suggests that an immunologic mechanism is accountable. After the start of antimicrobial therapy for leptospirosis, a Jarisch-Herxheimer response similar to that seen in different spirochetal illnesses might develop. Although frequently described in older publications, this response appears to be a uncommon event in leptospirosis and is certainly less frequent on this infection than in other spirochetal ailments. Leptospires enter the host by way of abrasions in the skin or by way of intact mucous membranes, especially the conjunctiva and the liner of the oro- and nasopharynx. Drinking of contaminated water could introduce leptospires by way of the mouth, throat, or esophagus. After entry of the organisms, leptospiremia develops, with subsequent spread to all organs. In symptomatic circumstances of leptospirosis, medical manifestations range from delicate to serious and even deadly. More than 90% of symptomatic individuals have the comparatively gentle and usually anicteric form of leptospirosis, with or with out meningitis. The concept that distinct clinical syndromes are related to particular serogroups has been refuted, although some serovars are probably to trigger more extreme illness than others. Typically, an acute leptospiremic section is followed by an immune leptospiruric phase. Specimens 1 and a pair of for serology are acute-phase serum samples, specimen three is a convalescent-phase serum pattern which will facilitate detection of a delayed immune response, and specimens 4 and 5 are follow-up serum samples that may provide epidemiologic data, such as the presumptive infecting serogroup. Muscle pain, which especially affects the calves, back, and abdomen, is a crucial feature of leptospiral infection. The affected person often has an intense headache (frontal or retroorbital) and sometimes develops photophobia. The most typical finding on physical examination is fever with conjunctival suffusion. Less widespread findings embody muscle tenderness, lymphadenopathy, pharyngeal injection, rash, hepatomegaly, and splenomegaly. The begin of this second (immune) part coincides with the event of antibodies. Usually the symptoms final for only some days, but occasionally they persist for weeks. Often the fever is less pronounced and the myalgias are much less severe than within the leptospiremic section. An important event in the course of the immune section is the event of aseptic meningitis. Similarly, pleocytosis typically disappears inside 2 weeks but often persists for months. Iritis, iridocyclitis, and chorioretinitis-late issues that may persist for years-can become obvious as early as the third week but usually current a number of months after the initial illness. Mortality charges in anicteric leptospirosis are low, though death as a result of pulmonary hemorrhage occurred in 2. In Europe, this syndrome is incessantly but not solely related to an infection because of serovar Icterohaemorrhagiae/ Copenhageni. Although some degree of defervescence could also be famous after the first week of illness, a biphasic illness pattern like that seen in anicteric leptospirosis is lacking. Hypovolemia and decreased renal perfusion contribute to the development of acute tubular necrosis with oliguria or anuria. Dialysis is usually required, although a fair variety of instances could be managed without dialysis. Rhabdomyolysis, hemolysis, myocarditis, pericarditis, congestive coronary heart failure, cardiogenic shock, grownup respiratory misery syndrome, necrotizing pancreatitis, and multiorgan failure have all been described throughout extreme leptospirosis. Related findings vary from urinary sediment changes (leukocytes, erythrocytes, and hyaline or granular casts) and delicate proteinuria in anicteric leptospirosis to renal failure and azotemia in severe disease. Mild thrombocytopenia occurs in up to 50% of patients and is associated with renal failure. In distinction to sufferers with acute viral hepatitis, these with leptospirosis sometimes have elevated serum levels of bilirubin and alkaline phosphatase in addition to delicate will increase (up to 200 U/L) in serum ranges of aminotransferases. Levels of creatine phosphokinase, which are elevated in as a lot as 50% of sufferers with leptospirosis during the first week of sickness, could help to differentiate this infection from viral hepatitis. When a meningeal reaction develops, polymorphonuclear leukocytes predominate initially and the variety of mononuclear cells increases later. In extreme leptospirosis, pulmonary radiographic abnormalities are more widespread than could be expected on the premise of bodily examination. The most typical radiographic finding is a patchy alveolar sample that corresponds to scattered alveolar hemorrhage. Radiographic abnormalities most frequently affect the decrease lobes within the periphery of the lung fields. These checks usually can be found solely in specialized laboratories and are used for determination of the antibody titer and for tentative identification of the serogroup-and in some cases the serovar-involved (thus the significance of using antigens representative of the serovars prevalent in the specific geographic area). However, in endemic areas, pooled serum samples from the local inhabitants are required as positive and unfavorable controls. Cultures most frequently turn out to be positive after 2�4 weeks, with a spread of 1 week to 6 months. Sometimes urine cultures stay positive for months or years after the beginning of sickness. When sufferers have a flulike illness with disproportionately extreme myalgia or aseptic meningitis, a prognosis of leptospirosis ought to be considered.