
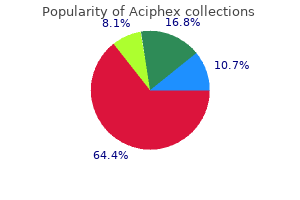
Aciphex
| Contato
Página Inicial
Kyle Melin, PharmD, BCPS
- Assistant Professor
- School of Pharmacy
- University of Puerto Rico
Planning computer Simple planning can be carried out using tables or plots of measured beam data gastritis and gastroparesis diet buy aciphex in united states online. Calculations are based on measured beam data but also depend on algorithms that allow for varying attenuation and scatter of X-rays in tissues of different densities gastritis diet ���� buy aciphex 20 mg low price. Target drawing the most important step in planning radiotherapy is defining the target gastritis bad breath aciphex 10 mg low cost, i gastritis blood test order discount aciphex line. For less sophisticated treatments chronic gastritis biopsy quality 10 mg aciphex, the target and critical organs are defined clinically. Dose planning the objective of dose planning is to design a treatment plan, such that the target is uniformly irradiated to an appropriate dose, whilst ensuring that critical organs do not exceed tolerance doses. Treatment verification It is essential that beams are correctly positioned and critical organs not over-irradiated. For this, thermoluminescence dosimeters are attached to relevant sites on the patient during one fraction of radiotherapy. Treatment prescription and delivery the clinical oncologist prescribes the appropriate dose and fractionation schedule. Together with beam configuration information, these form a dataset completely describing the intended treatment. They are entered into a computer verification system on the linear accelerator and control set-up and delivery of each treatment. Normal practice until the 1990s was to use rectangular beams, with limited use of blocking. By minimizing the amount of normal tissue irradiated to high dose, it may be possible to deliver higher doses to the target, thereby improving tumour control without increasing morbidity. The tumour volume for even palliative treatments can now be accurately defined in 3D. Image-guided radiotherapy Radiotherapists have always recognized the need to allow for discrepancies between the planned treatment volume and the volume of tissue that actually receives irradiation. Previously, confirmation of the accuracy of treatment required the taking of a megavoltage X-ray of the exit beam during a small part of the treatment exposure. So-called online imaging can be performed at the start of a treatment fraction in order to correct any misalignment, whilst offline images can be reviewed by radiographers or clinicians after the treatment fraction has been delivered. This treatment requires careful voluming of the tumour and all surrounding normal tissues on each slice of the planning scan, with typical times for volume definition of at least 2h per patient, and considerably increases the workload of the physics team. Stereotactic radiotherapy Since the 1990s, this treatment modality has become established for the treatment of a number of intracranial conditions, including benign tumours and arteriovenous (aV) malformations. Recently, this approach has been used successfully in the treatment of small malignancies in the brain, lung, and liver. Dosimetric characteristics of electron beams the various dosimetric aspects of electron beams in homogeneous tissue are as follows. Depth dose characteristics the dose builds up slowly to a maximum value and then falls off rapidly, reaching nearly zero at a depth equal to the practical electron range. Effect of incident energy the depth of penetration of an electron beam is determined by its incident energy. Beam profile and penumbra the beam penumbra tends to be larger for electron beams than for photon beams. Thus, a larger electron beam is required to cover a given target to a clinically useful dose. This property of electron beams makes abutting of photon and electron beams problematical, since a uniform dose across a field junction cannot be achieved at all depths. Brachytherapy allows the delivery of a localized high radiation dose to a small tumour volume, increasing the chance of local control. The constant low-dose irradiation takes advantage of the different rates of repair and repopulation of normal and malignant tissues to produce differential cell killing, enhancing the therapeutic ratio. Reoxygenation may occur during low-dose rate radiotherapy, with initially resistant hypoxic cells becoming oxygenated and more radiosensitive during the course of brachytherapy. Treatment is often prescribed to the minimum dose received around the periphery of the treated volume. Staff exposure can be minimized by after-loading techniques or the use of low-energy radionuclides. In order to treat the required tissue volume adequately, accurate geometric positioning of the sources is critical. The spatial arrangement of sources used varies, depending on the type of source applicator, the anatomical position of the tumour, and the surrounding dose-limiting normal tissue. Implants can be classified as manually inserted, after-loading, or remote after-loading. Manual insertion of radiation sources should be avoided, if possible, owing to the radiation hazards to operating staff and nurses. For remote after-loading, stainless steel pellets containing, for example, caesium in glass are moved pneumatically from a computer-controlled, lead-lined safe into intrauterine and vaginal applicators. Low-dose rate brachytherapy may require the sources to remain in place for many hours. The rays produced are relatively high-energy (average of 830keV), and thick lead shields are required to provide adequate radiation protection. Caesium-137 has no gaseous daughter products, a useful half-life of 30y, and a less penetrating 660keV ray, and it has largely replaced radium, especially for gynaecological work. Iridium-192 is manufactured in the form of flexible wires and has many advantages over traditional radium or caesium needles for interstitial brachytherapy. Iridium is also available in the form of seeds sealed in thin plastic coating, used frequently for gynaecological treatments with the Microselectron. Iridium produces a ray of 330keV, and lead shields of 2cm in thickness provide good protection for medical and nursing staff. The major disadvantage of iridium is the relatively short half-life (74 days), so that fresh material should be used for each interstitial implant. Dosimetry Radioactive material is implanted into tissues, according to distribution rules that vary according to the system used. In a volume implant, sources in cross-section should be arranged in either equilateral triangles or squares. The dose to the tumour can be calculated manually, using graphs, such as oxford cross line curves, or by computer. The basal dose rate (the mean of minimum values between sources) is first calculated. The most frequently used prescribing point is the Manchester a point, defined as a point 2cm lateral to the uterine canal and 2cm above the cervical os. The dose calculated at this point is a good predictor of late radiation damage to the ureter, bladder, rectum, and other pelvic organs. Radiation exposure to staff has been reduced by the increased use of high-dose rate remote after-loading machines. The complication rate following fractionated high-dose gynaecological insertions is less than that following manually inserted low-dose sources. Report 38: dose and volume specification for reporting intra-cavity therapy in gynecology. Issues, such as treatment planning, are clearly complex, as only limited treatment volume data can be available preoperatively. The distribution of the radiopharmaceutical may vary from the normal because of a pathological process. Examples are iodine-123 and -131, which localize avidly in functioning thyroid tissue. The ideal radionuclide for scintigraphic imaging does not exist, but technetium-99m (99mTc) has many favourable characteristics. Planar images and whole-body images are acquired during a period of several minutes by a stationary camera. Glucose utilization is measured with 18F-labelled fluorodeoxyglucose, and cerebral blood flow has been studied with 15 o-labelled water. Thyroid scintigraphy 131 I as radioiodine, 123I as sodium iodide, and 99mTc as sodium pertechnetate are the radionuclides used for scintigraphic visualization of the thyroid gland. Therapy with unsealed radioactive sources Targeted radiotherapy using tumour-seeking radiopharmaceuticals has been employed for almost half a century. Some of the clinically useful radiopharmaceuticals for therapy are 131I, 89Sr, 32P, 186Re, 153Sm, and 90y. Iodine-131 therapy in differentiated thyroid cancer 131 I has been used extensively in the treatment of thyrotoxicosis and in differentiated thyroid carcinoma after thyroidectomy. Post-therapy scintigrams, 1wk after administration, can be obtained for further documentation. Bone-seeking radiopharmaceuticals have pharmacokinetic properties similar to those of either calcium or phosphate. Colloids and monoclonal antibodies labelled with 32P, 90y, or 131I can be used for this purpose. The goal has been to develop antibodies that target active tumour cells specifically and act as carriers of radiation to treat the disease. This can be compensated for by using bolus or lung shielding but is unnecessary using schedules described here where doses do not exceed tolerance for any normal tissues. Calculation of dose Paired lithium fluoride dose meters or diodes are used to measure the dose distribution throughout the body. These are placed on the skin at defined sites in the upper and lower lung, mediastinum, abdomen, and pelvis. The maximum lung dose is preferred, as this is the dose-limiting organ, and should not exceed 14. Many other dose schedules are in common use and have been found by experience to be satisfactory. Chapter 5 83 Principles of chemotherapy Rationale for combination therapy 84 Alkylating agents 85 Anti-tumour antibiotics 86 Anti-metabolites 88 Cisplatin and derivatives 94 Topoisomerase inhibitors 98 Anti-microtubule agents 100 Drug resistance 104 Dose intensification 106 Chemo-irradiation 108 84 ChApTeR 5 Principles of chemotherapy Rationale for combination therapy Cytotoxic chemotherapy destroys cancer cells. The discovery and development of cytotoxic agents has paralleled the understanding of the chemical processes involved. The lack of selectivity inherent in this approach has limited the ability to kill cancer cells, whilst leaving normal dividing cells unscathed. Clinical use extensively used to treat leukaemia and lymphoma, and they are also active in a wide range of solid cancers. The rationale behind this is that dividing cells might take up amino acids more rapidly (and hence melphalan), thus providing some tumour selectivity. As a result of its relative lack of non-haematological toxicities, it is used in high-dose chemotherapy regimens. The dose-limiting toxicities are myelosuppression and hepatic veno-occlusive disease. Pharmacology the anthracyclines have several effects, and their specific mode of action is unclear. The characteristic cardiotoxicity of anthracyclines appears due to the generation of free radicals in the heart where defence systems are less active. Drug resistance Some tumours are inherently resistant to anthracyclines, whereas others initially respond but later become resistant. Though expression is increased in some human cancers before treatment or at relapse, attempts to manipulate pgp have had limited success. Subsequent metabolism and elimination lead to a slow fall in plasma concentrations over several days. Dose reductions are recommended for patients with abnormal liver biochemistry, as they are at risk of increased toxicity. Cumulative cardiotoxicity is specific to anthracyclines and appears to be caused by the accumulation of free radicals in the heart. The main clinical use of mitoxantrone has been as an alternative to doxorubicin in advanced breast cancer, as it is substantially less cardiotoxic and less vesicant and causes less alopecia. They include some of the most widely prescribed cytotoxic agents, the indications of which are not confined to treating malignancies. Anti-folates Understanding anti-metabolite action necessitates the knowledge of folate biochemistry. Fluoropyrimidines these pro-drugs are intracellularly activated, and their products inhibit pyrimidine synthesis. Fluorouracil this is a widely prescribed agent, with particular activity in breast cancer, Gi cancers, and head and neck tumours. Toxicities of fluorouracil include myelosuppression and, particularly with longer administration schedules, stomatitis and diarrhoea. Further development and clinical trial work is ongoing to try to substitute this drug for fluorouracil in other clinical scenarios. Modulation of fluorouracil A number of agents have been combined with fluorouracil in order to increase either its efficacy or therapeutic index. Although more toxic, it has a higher response rate in advanced colorectal cancer with combined treatment than single-agent fluorouracil. Anti-purines purine analogues are widely used to treat leukaemias and as immunosuppressives (azathioprine) and antivirals (aciclovir, ganciclovir). Variable oral bioavailability may contribute to some treatment failures in childhood acute lymphoblastic leukaemia (All). Both drugs have a short half-life and are primarily metabolized-the important difference is that 6-Mp is a substrate for xanthine oxidase, and dose alterations are necessary when co-administered with allopurinol. There is renal excretion of the deaminated compound, and, because of rapid clearance, better activity is observed when cytarabine is given by continuous infusion. Toxicities include flu-like symptoms, transaminitis, peripheral oedema, myelosuppression, and possible nephrotoxicity. There is some evidence for synergy with cisplatin, the extent of which appears to be schedule-dependent.
As with the description of brain and liver pathology with the preeclampsia syndrome gastritis diet vegan cheap aciphex 10 mg overnight delivery, we chose to discuss alterations in liver pathology and function in their clinical context rather than anatomically gastritis diet ���������� purchase aciphex with a visa. In his usual thorough fashion gastritis or ulcer 10 mg aciphex otc, he reviewed data that had accrued up to that time gastritis symptoms remedy purchase 20 mg aciphex, and he concluded that there was evidence for slightly increased coagulation and fibrinolysis during normal pregnancy gastritis symptoms heart attack buy aciphex 20 mg low cost. He went on to say, however, that many women with severe preeclampsia and eclampsia show no detectable evidence of increased coagulation and fibrinolysis. He concluded that disseminated intravascular coagulation did not appear to be a fundamental feature of the disease. Although observed as early as 1924, it had been proven by that time that platelet concentrations were decreased in some women with preeclampsia syndrome  especially severe cases that included those with eclampsia. In a fourth of these, the platelet count was <150,000/L, in 15% it was <100,000 L, and in 3% it was <50,000/L. From these and other studies, Chesley concluded that thrombocytopenia is a feature of the preeclampsia syndrome, but that it was not caused by consumptive coagulopathy. Somewhat parallel to the coagulation story, it had been long known that severe preeclampsia and eclampsia were associated with gross and microscopical changes in the liver. And while hepatocellular damage is a known cause of coagulopathy, Chesley concluded that damage to the liver was generally not severe enough to cause significant liver dysfunction. But the link between thrombocytopenia and liver involvement characterized by elevated serum transaminase levels did evolve as a marker for the severity of preeclampsia. Thus coagulation, thrombocytopenia, and hepatic changes of the preeclampsia syndrome became accepted as interrelated. As with any review concerning preeclampsia, a major difficulty is the use of variable or imprecise criteria for its diagnosis, as discussed in Chapter 1. Platelets are extremely complex morphologically and biochemically, and have myriad functions. Some of these myriad changes in platelet numbers, morphology, and function are shown in Table 17. Several large, populationbased studies have demonstrated that in uncomplicated pregnancies, the platelet count decreases by about 10% by term. The genesis of this decrease is not known for certain, but is likely to be related to the larger total blood volume as well as the expanded splenic volume, which may be as much as 35%. Up to half of women with preeclampsia develop thrombocytopenia, the extent of which is generally proportional to the severity of disease. The elevated levels of thromboxane A2 metabolites in the urine of preeclamptic patients, as well as the increased plasma levels of the platelet -granule proteins -thromboglobulin and platelet factor 4, supports the argument that platelet activation contributes to accelerated platelet clearance in this disorder. Thus, increased generation of thrombin may be one mechanism that promotes platelet activation. Platelets may also be stimulated through contact with dysfunctional endothelium and/or exposed subendothelium underlying the injured placental vasculature. Numerous membrane receptors serve to discharge platelet functions, the primary one being their adaptation to adhere to damaged blood vessels, with one another, and to stimulate thrombin generation, all of which generate a hemostatic plug  the clot. Critical to platelet function are platelet surface receptors that bind adhesive glycoproteins. Others receptors bind additional matrix glycoproteins, while the P-selectin receptor mediates interactions with leukocytes to incite a proinflammatory response. Ligand binding by platelet cell surface receptors may induce platelet activation, through "outside-in" signaling. An idea of the complexity of this process comes from consideration of the multiple agonists shown in Table 17. When endothelium is disrupted, platelets adhere to exposed subendothelial collagen. This process requires von Willebrand factor and results in platelet shape change from a discoid to a tiny sphere with numerous fine filopodia or pseudopodia. Inherent to the platelet activation process is secretion of the contents of dense granules and alpha granules that contain a variety of substances, such as some of those shown in Table 17. Optimal methods to investigate platelet lifespan require radiolabeling, which is prohibited in pregnancy. Using the method of platelet malondialdehyde production, disparate findings have been reported. The demonstration of a shorter platelet production time is consistent with a shorter platelet half-life. These changes are found only with maternal platelets because, even with marked maternal thrombocytopenia with severe preeclampsia, neither cord blood nor fetal platelet counts are affected. Despite this, the absolute platelet count is of limited predictive or prognostic value. The platelet nadir is usually reached approximately 24 hours postpartum, with normalization occurring within 6Â11 days. Thus, likely events operative include platelet activation by contact with damaged endothelium, platelet consumption secondary to thrombin generation, and microangiopathic hemolysis. Moreover, this activation is increased further in women with preeclampsia Table 17. Circulating levels of factors stored within platelets reflect platelet activation  specifically, platelet aggregation and release of granule contents. Plasma levels of -thromboglobulin, a platelet -granule protein, are increased in normal pregnant women. There are increased expressions of other platelet membrane antigens that signify activation. They reported a higher frequency of abnormal platelet antiglobulin found in preeclamptic women compared with normotensive pregnant women. Alterations in plateletbound immunoglobulins might be from the deposition of autoreactive antibodies or immune complexes caused by placental tissue antigens. Alternatively, platelet activation at sites of microvascular injury could lead to the externalization of IgG and other proteins in platelet -granules. They reported that activated platelets were detected prior to the development of preeclampsia. The most reliable method of assessing in vivo thromboxane production is by measurement of urinary metabolites of thromboxane A. Urinary excretion of 2,3-dinor-thromboxane B and 11-dehydro-thromboxane B is increased in normal pregnancy. These latter compounds are both a substrate for lipid oxidation and participate in thromboxane formation. Increased thromboxane production may thus reflect altered platelet membranes in preeclampsia. Summary of Platelet Activation Taken together, there is ample evidence for platelet activation in preeclampsia. There is reduced platelet concentration, increased size, reduced lifespan, increased -granule release, enhanced expression of cell adhesion molecules, and increased thromboxane production. This increased activation, which occurs early in the disease, may either result from an extrinsic factor such as endothelial damage with platelet activation, or it might be intrinsic and antedate pregnancy. Evidence that intrinsic platelet alterations are at least partly responsible comes from findings of platelet binding-site alterations. This would lead to decreased platelet-activating factor in normally pregnant compared with nonpregnant women, but not in those with preeclampsia. Specifically, these studies demonstrate increased platelet activation in normal pregnancy compared with nonpregnant women; however, reduced activation is consistently reported in vitro with preeclampsia. Platelet aggregation decreased somewhat in early pregnancy, but thereafter it was increased throughout the latter two trimesters. As indicated, however, others have reported decreased platelet aggregation in women with eclampsia. When whole blood is studied in vitro, platelets from women with preeclampsia release less serotonin in response to epinephrine compared with platelets from normally pregnant women. This mirrors the in vitro reduction in platelet aggregation in response to this agonist in preeclampsia. Taken together, these findings suggest that the platelet content of serotonin is reduced in preeclampsia, suggesting that platelets have become activated and released their granule contents prior to in vitro studies. Thus, most in vitro studies demonstrate reduced platelet reactivity in preeclampsia compared with normal pregnancy. One possible explanation of the disparate in vivo and in vitro observations is that preeclampsia leads to in vivo activation which results in circulating "exhausted" platelets which are hyporeactive when tested in vitro. There have been other in vitro studies designed to elucidate mechanisms responsible for increased in vivo platelet activation in preeclampsia. For example, there is evidence that the inhibitory mechanisms that switch off platelet activation responses may be less effective in preeclampsia. In reports focusing on preeclampsia, however, pregnancy-induced diminished susceptibility to prostacyclin inhibition was significantly more marked  up to 50%  in preeclampsia. Expression of Platelet Receptors in Pregnancy and Preeclampsia the platelet surface is decorated by a plethora of glycoprotein receptors that function to mediate signals from the extracellular milieu to the platelet signaling machinery, often using specific G-protein-coupled receptors as an intermediary. The integrated function of these receptors regulates the platelet activation response, and antiplatelet therapies, either approved or in development, target many of these receptors. However, there are very few data available on the expression of these receptors in normal pregnancy or hypertensive pregnancy disorders. Platelet Second Messengers In an attempt to further elucidate mechanisms underlying in vivo and in vitro changes in platelet behavior, studies have been done to investigate platelet second messenger systems in normal pregnancy and in preeclampsia. They used the calcium-sensitive indicator quin-2, which is known to quench increases in platelet [Ca2+] resulting from platelet stimulation. It had been previously shown that 5-hydroxytryptamine responses were easily suppressed as a result of prior platelet activation. Whether this increase in platelet [Ca2+] reflects a population of partially activated platelets in preeclampsia, or is a cause of altered platelet reactivity, is unclear. There is some evidence that alteration in stimulated platelet [Ca2+] precedes clinical signs of preeclampsia. They used a sensitive assay based on prelabeling of the metabolic adenine nucleotide pool in platelets with hydrogen 3-adenine. In a cross-sectional study, no differences were found between normal and a heterogeneous group of women including those with nonproteinuric gestational hypertension and preeclampsia. They speculated that upregulation of platelet guanylate cyclase activity may be a compensatory response to impaired nitric oxide production in preeclampsia. Classically, this enzyme sequence is divided into the intrinsic and extrinsic pathways, which both converge in a final common pathway. The major distinction between the two pathways is that the intrinsic pathway is activated from within the bloodstream while the extrinsic pathway begins in the blood vessel walls. This in turn leads to a series of reactions culminating with the activation of factor X. There is considerable evidence that preeclampsia is accompanied by a number of coagulopathic changes when compared with normal pregnant women. Despite this, except for the rare case of preeclampsia complicated by overt clinical disseminated intravascular coagulation, routine coagulation tests are usually normal. There have been reports, however, of covert activation of both the intrinsic and extrinsic coagulation pathways in preeclampsia. Although fibrinogen levels are the same or only slightly increased in women with preeclampsia compared with normal pregnant women,96 the turnover of radiolabeled fibrinogen is increased in preeclamptic women. The action of thrombin on fibrinogen is a crucial step in the coagulation cascade. Thrombin cleaves two pairs of peptides  fibrinopeptide A and B  from fibrinogen to produce soluble fibrin monomer, which rapidly polymerizes to fibrin. Determination of free fibrinopeptides in blood can be used to measure thrombin activity and fibrinopeptide concentrations are considered to be the best markers of accelerated thrombosis or coagulopathy. Levels of fibrinopeptide A are either elevated or they are unchanged in normal pregnancy; however, most investigators describe increased fibrinopeptide levels in women with preeclampsia compared with normal pregnant women. It seems indisputable that many of the mutations of these factors are associated with a substantively increased risk of venous thromboembolism. Any association between these and adverse pregnancy outcomes is, however, controversial, as recently reviewed by the American College of Obstetricians and Gynecologists. Protein C levels appear to be unchanged in normal pregnancy compared with the nonpregnant state. This reduces the sensitivity of the factor V protein to inactivation by activated protein C  hence, activated protein C resistance  resulting in a procoagulant state and an increased risk of thrombosis. The trait is inherited in an autosomal dominant manner with the risk of thrombosis increased seven-fold in heterozygotes and 80-fold in homozygotes. One metaanalysis of many of these studies suggested that factor V Leiden is associated with a 2. Antiphospholipid Syndrome these autoimmune antibodies include lupus anticoagulant, anticardiolipin antibodies, and anti-2-glycoprotein. Amongst other adverse effects, these autoantibodies are associated with recurrent pregnancy loss, preeclampsia, and fetal-growth restriction. Fibrinolytic System the end-product of the coagulation cascade is fibrin formation. Plasmin, which is the main protease enzyme in this system, originates from plasminogen secreted by the liver. The activation of plasminogen into plasmin is through plasminogen activators which are serine proteases. Both act upon plasminogen to convert it to plasmin and in so doing trigger a proteolysis cascade that causes thrombolysis. It results from a G-to-A mutation at nucleotide 20210 in the prothrombin gene that causes excessive production and increased circulating prothrombin levels. Like the factor V Leiden variant, this mutation shows significant ethnic variation, being most prevalent in southern European populations, with an overall population prevalence of 2Â3%. In a number of case-control studies there does not appear to be a significant association. Finally, 2-macroglobulin  2-M  is synthesized mainly by the liver and is a general inhibitor of both coagulation and fibrinolysis, acting as a scavenger. In the fibrinolytic system, 2-M inhibits the action of plasmin and kallikrein, while in coagulation it inhibits thrombin.
Renal agenesis in one-third of patients is associated with cystic seminal vesicles or unilateral seminal vesicle agenesis gastritis labs order aciphex 10 mg line. Hypoplasia A hypoplastic kidney appears sonographically as an abnormal development of the renal tissue gastritis symptom of pregnancy aciphex 20 mg order without prescription, which is usually of less than normal size gastritis diet ����� buy cheap aciphex 20 mg online, but with a normal structure gastritis anxiety buy 20 mg aciphex with visa. In dysplasia there are additional disturbances of normal renal architecture gastritis diet plan foods buy generic aciphex 20 mg line, with the kidney presenting as small or very small: some hypoplastic kidneys are too small to be defined with ultrasound. Differentiation from an atrophic kidney is not always possible, but most hypoplastic kidneys exhibit normal parenchyma and normal central hilar echoes. The apparent "missing left kidney" is probably a tiny hypoplastic kidney (cursors). Dysplasia Because of the common association of dysplastic kidneys with a urinary tract obstruction and other extrarenal syndromes, they are found more often in children than in adults. In ultrasound imaging the kidney is small and shows a dysplastic parenchyma with single or multiple small or large cysts and a dissolved corticomedullar differentiation without a regular architecture. About 50% of the population have renal cysts, which appear more often and are larger in advanced age. A specific pathologic explanation for this has not yet been established; however, ischemic changes, interstitial medullary fibrosis, and tubular obstruction at the basal membrane of the distal tubulus are all under discussion. Renal and often liver and splenic cysts can also be commonly found in parents of affected children, especially in the father. They are caused by increased intratubular pressure due to distal tubular obstructions and by tubular epithelial dysplasia. Because the cysts are small in infancy and only later become increasingly larger, it is difficult to make a diagnosis in children. Renal cysts in children aged 6 years and older should indicate an examination of the parents (as the mother can often have multiple renal cysts). Secondary cysts (involutional cysts) may be found in chronic renal diseases (see below), especially in terminal kidney insufficiency, which is frequently associated with renal cancer. The kidney is still of normal size, and the parenchyma is clearly visible; dialysis. Renal cysts appear sonographically as round, anechoic, smooth-bordered masses that are lined with epithelium, forming a cyst wall. Polycystic kidneys contain multiple anechoic masses of varying size, usually causing considerable organ enlargement. The cysts produce an undulating renal outline with no discernible capsule, causing poor delineation of the kidney. Large bullous cysts obscure the residually intact parenchyma through a "blooming effect," so that the kidney appears to consist almost entirely of cystic areas. Anomalies of Number, Position, or Rotation Kidneys Anomalies, Malformations Aplasia, Hypoplasia Cystic Malformation Anomalies of Number, Position, or Rotation Fusion Anomaly Anomalies of the Renal Calices Vascular Anomaly Diffuse Changes Circumscribed Changes Duplex Kidney Ectopic Kidney Malrotation Duplex Kidney Duplex kidney is the most common renal anomaly, occurring in 1% of the general population. It is characterized by duplicated renal pelvises and two ureters that unite somewhere between the kidney and bladder. When the ureters have different insertions, the ureter with the more distal insertion belongs to the upper moiety, according to the MeyerÂWeigert rule. The ureter belonging to the lower moiety consistently empties proximate to that site. But if the lower ureter is affected, the obstruction is due not to an ectopic insertion but to some other obstructive process. It is common to find an ectopic insertion of the lower moiety with an associated ureterocele, leading to vesicorenal reflux or ureteral obstruction that again affects the upper moiety. The two moieties are separated by a parenchymal band (B), where a notch is visible in the renal outline (arrows; the lower arrow marks the hilum of the lower renal segment). Ectopic Kidney A lumbar kidney is the most common form of renal ectopia, with ultrasound revealing the ectopic kidney in the anterior iliac fossa. The key sonographic landmark is the iliac artery- the ectopic kidney will generally be found anterior to that vessel. The less common pelvic kidney lies anterior to the sacrum and below the aortic bifurcation. Malrotation Malrotation is an anomaly in which the renal hilum faces anteriorly (caution: this makes the vessels vulnerable to a percutaneous needle). Fusion Anomaly Kidneys Anomalies, Malformations Aplasia, Hypoplasia Cystic Malformation Anomalies of Number, Position, or Rotation Fusion Anomaly Anomalies of the Renal Calices Vascular Anomaly Diffuse Changes Circumscribed Changes Horseshoe Kidney Fetal Lobulation Horseshoe Kidney In the most common fusion anomaly, the symmetrical horseshoe kidney, the lower poles of the kidneys are fused together across the midline. It is not unusual for horseshoe kidney to be missed in ultrasound, as the scan planes may not completely define the inferior outline of the lower pole. Ultrasound may occasionally suggest a misdiagnosis of preaortic lymphoma unless horseshoe kidney is considered in the differential diagnosis. Color Doppler ultrasound usually establishes the diagnosis by demonstrating the typical vascular configuration. Incomplete horseshoe kidney is diagnosed when ultrasound shows the typical medial extension of the lower pole, often crossing the aorta, but the contralateral kidney is absent. A cake-shaped kidney results when the fusion occurs over broader areas, producing an irregularly shaped organ. They require differentiation from caliectasis due to obstructing caliceal stones, which are more common in older patients. Megacalicosis this is a congenital dilatation of the calices, which is usually asymptomatic. Vascular Anomaly Kidneys Anomalies, Malformations Aplasia, Hypoplasia Cystic Malformation Anomalies of Number, Position, or Rotation Fusion Anomaly Anomalies of the Renal Calices Vascular Anomaly Diffuse Changes Circumscribed Changes Aberrant Vessels Renovascular Malformations Aberrant Vessels A crossing interlobar artery will occasionally narrow the neck of the calix, causing prestenotic dilatation of the upper calix. Ultrasound then shows an abnormal expansion of the affected calix with no visible outflow obstruction (stone). A more common aberrant configuration is a lower pole artery arising separately from the aorta and narrowing the upper ureter, causing pyelectasis. Ultrasound shows an anechoic mass in the pyelocaliceal system obstructing the proximal ureter but does not demonstrate a causative lesion (tumor, stone). The differential diagnosis should also include pyelectasis due to an ampullary renal pelvis and a hypermobile kidney with proximal kinking of the ureter. Whether a kidney appears large or small in ultrasonography depends very much on the selected field of view, i. For some examinations, then, it is necessary to measure at least the longiThe individual scatter of measurement is about 0. The parenchymal thickness is in the range 13Â18 mm; small kidneys have less than 12 mm. For specific examinations, volume analysis is preferable: the product of the largest longitudinal, transverse, and anteroposterior tudinal renal diameter and parenchymal thickness. Anatomically, the adult kidney measures 1 cm over the sonographic diameter, 10Â11. For physical reasons, radiographic measurements of the kidney add approximately 1. Sonographic measurements, by contrast, are slightly smaller than the true dimensions because the kidneys occupy planes that are angled laterally and anteromedially and do not coincide precisely with the planes used for routine scanning. One of the most common types of renal enlargement involves duplex kidneys, whose sonographic features are described above. The longitudinal diameter may be normal or increased up to 15 cm, with a normal width. The moieties can be distinguished from a tumor by color Doppler sonography, which shows a normal duplex vascular pattern. In the early stage, which marks the onset of a progressive function impairment leading to manifest renal failure, the kidneys are enlarged as a result of hyperperfusion. According to studies of diabetic nephropathy in type 1 diabetics, the enlargement is based on a volume increase affecting both the longitudinal diameter and thickness of the organ. In ultrasound, the renal parenchyma is thickened and often shows increased sonodensity. Six months later, persistent diarrhea and reversible decompensation with creatinine of 8 mg/ dL. The kidney should therefore be measured in patients evaluated for diabetic nephropathy. It is not until an advanced stage, when the patient requires hemodialysis, that the kidney shrinks in size and shows obvious structural changes. The kidneys tend to show increased echogenicity, probably due to a suppurative leukocytic reaction to septicopyemic foci in the organs. Acute Urinary Retention, Acute Outflow Obstruction In this situation as well, the kidneys often react with enlargement and decreased echogenicity due to interstitial edema. The sonographic renal changes are the same as those seen in renal congestion resulting from heart failure. Renal Congestion Due to Heart Failure the fluid build-up that occurs in severe congestive heart failure leads to swelling and increased echogenicity of the renal parenchyma secondary to edema and hemorrhage. Acute Pyelonephritis A different picture is seen with severe acute septic pyelonephritis, in which one or both kidneys are enlarged and generally show a decrease in parenchymal echogenicity. Often there are accompanying abscesses, pyonephrosis, or merely circumscribed anechoic to hyperechoic lesions in the parenchyma, renal pelvis, or renal sinus representing abscesses or infected, purulent urine. Enlarged kidney (N) shows slightly increased echogenicity relative to the liver (L). The medullary pyramids (arrows) are markedly swollen and show patchy low echogenicity due to proteinfilled tubules, with the formation of hyaline casts in the distal tubules (creatinine 3. Pyonephrosis If the purulent collection in the renal pelvis takes up the entire central echo complex, the pyonephrotic mass leads to overall renal enlargement. With extensive tumor infiltration, the kidney appears substantially enlarged and broadened. Renal Allograft, Allograft Rejection As a solitary functioning kidney, the renal allograft is enlarged owing to adaptive hypertrophy. A more definitive sign is occlusive vasculopathy, which can be demonstrated with Doppler ultrasound. Complications consist of renal artery stenosis, renal vein thrombosis, and arteriovenous fistulas. Small Kidneys Kidneys Anomalies, Malformations Diffuse Changes Large Kidneys Small Kidneys Hypoechoic Structure Hyperechoic Structure Irregular Structure Circumscribed Changes Hypoplasia Renal Artery Stenosis, Embolism Arteriosclerosis, Arteriolosclerosis (Ischemic Nephropathy) Chronic Pyelonephritis Analgesic Nephropathy Chronic Glomerulonephritis Diabetic Nephropathy Hypoplasia Renal hypoplasia is characterized by a small kidney with essentially normal parenchyma accompanied by compensatory contralateral enlargement and often showing ectopia or malrotation. Renal Artery Stenosis, Embolism When a small kidney is due to renal artery stenosis, generally the stenosis is severe and of long duration and is associated with chronic hypertension. Renal artery stenosis may be classified as atherosclerotic (85% of cases) or fibromuscular (15%). Accessory renal arteries occur in up to 28% of cases, so that when renovascular hypertension is diagnosed, these vessels should be included in diagnostic considerations. The length of the kidney may be reduced to less than 9 cm in highergrade stenosis, and the parenchyma may appear normal or thinned in ultrasound. The maximum flow velocity rises to values in excess of 180 cm/s at the stenosis, and there is concomitant spectral broadening and aliasing. Arteriosclerosis, Arteriolosclerosis (Ischemic Nephropathy) While arteriolosclerosis leads to a decrease in renal size with thinning of the cortex, arteriosclerosis causes an irregular surface with areas of parenchymal thinning, but an overall normal renal size. The echogenicity is normal or slightly hyperechoic (due to sclerosis) and the parenchyma is frequently narrowed. The surface appears smooth when arteriolosclerosis is predominant; in arteriosclerosis the surface appears coarse, with a scarred contour, and thickened segmental arteries showing bright double echoes with a central, narrow echofree band can be seen in the renal sinus. In bilateral cases that have progressed to a stage requiring dialysis, the kidneys are significantly smaller than normal, especially in their longitudinal dimension. In interstitial renal diseases, a correlation exists between the echogenicity of the renal cortex and histological changes such as sclerosis, tubular atrophy, hyaline casts, and focal leukocyte infiltration. In the advanced stage of renal atrophy when the longitudinal size of the kidney has dwindled to approximately 6Â7 cm, ultrasound is generally no longer helpful in diagnosing the cause. In addition to these changes, abscesses may form in the renal pelvis, appearing as hypoechoic masses. The histological features are a lumen-occluding capillary sclerosis, tubular and papillary necrosis, and papillary necrosis with calcification of the papillary tips. The sonographic features reflect the histological changes in the form of decreased renal size, increased echogenicity, wavy contours, and fine calcifications at the tips of the medullary pyramids. Marked parenchymal rarefaction with a hazy structure and fine calcifications projected over the papillary tips (arrows). Chronic Glomerulonephritis Chronic glomerulonephritis and diabetic nephropathy (glomerulosclerosis) are both characterized by a decrease in renal size that does not occur until an advanced stage. In both diseases, the longitudinal diameter of the kidney is within normal limits in patients who have reached the dialysis stage. Sonographically, the kidney shows markedly increased echogenicity due to glomerular hyalinization and tubular atrophy. The medullary pyramids may still be appreciated as hypoechoic areas, but in most cases they disappear owing to histologically demonstrable tubular atrophy. In stage V disease, the kidneys return to either a normal or slightly decreased size, and small kidneys are not seen until the later dialysis stage. Ultrasound at that stage demonstrates rarefied areas in the cortex and increased echogenicity. Microcysts are also found, consisting mainly of medullary pyramids that have undergone cystic degeneration. The kidney, which is very difficult to identify, has an irregular structure and contains calcifications with acoustic shadows (S). Thus, some of the following disor- ders have already been described above and will be merely outlined here. It should also be noted that while the features listed are sugges- tive of the various diseases, they do not necessarily mean that ultrasound can definitely detect the disease in question. Acute Renal Failure If there are any characteristic changes in acute renal failure, they are renal enlargement and decreased echogenicity. An increase in echogenicity is to be found in many acute and chronic renal diseases. It indicates no special nephropathy, but it is an important sonographic sign indicating disturbed Table 9.
Syndromes
- You have a headache that gets worse when you sit up, especially if you have recently had a head injury, surgery, or childbirth involving epidural anesthesia.
- Start CPR or rescue breathing, if necessary and if you know the proper technique.
- Climate
- The needle is removed.
- Uterine prolapse is mild when the cervix drops into the lower part of the vagina.
- Eflornithine (for T. b. gambiense only)
- Stuttering
- Lumbar puncture (spinal tap)
- Muscle biopsy
The connective tissue disorder will usually be pre-existing and therefore easily identified as a possible or likely cause of the effusion 7 day gastritis diet cheap 10 mg aciphex. Occasionally gastritis diet and treatment discount 10 mg aciphex mastercard, one of these conditions may present for the first time with pleuritis treating gastritis over the counter 20 mg aciphex amex, and this could occur in pregnancy gastritis symptoms diarrhoea aciphex 20 mg without a prescription, especially as they are generally more common in young women chronic gastritis journal purchase aciphex with a visa. The pleural fluid aspirate and a blood sample should be analysed for the relevant autoantibodies (rheumatoid factor, antinuclear factor, Ro and La antibodies) following a diagnostic tap. Thoracic malignancy occurs rarely in pregnancy, and if involving the pleura would tend to cause breathlessness more often than chest pain. Pleural effusion may occur but is due to involvement of the visceral pleura, which is not innervated, and/ or blockage of lymphatics. Breast cancer frequently spreads to bone and pleura and is the most common malignancy of young women. Bronchial carcinoma usually occurs in later life at an age beyond that of most pregnancies and has rarely been reported. A combination of these tests including culture of the biopsy specimen itself will give the highest possible yield for diagnosis. Pneumothorax usually presents with the sudden onset of pleuritic chest pain and breathlessness. The pain often subsides quite rapidly, as it is probably due to the sudden shearing off from the chest wall of the parietal pleura. Although primary spontaneous pneumothorax can occur in anyone, it is 9Â22 times more common in smokers and usually occurs in those with a tall, thin body habitus. There is no reason to suppose that pneumothorax should be any more common in pregnancy with the exception of during labour, when repeated strenuous Valsalva manoeuvres could theoretically increase the risk of subpleural bleb (a small bulla-like structure) rupture, which is the main cause of spontaneous pneumothorax. The clinical diagnosis may be difficult, as physical examination reveals a hyperresonant percussion note and significantly reduced breath sounds on the affected side only when the pneumothorax is of a sufficiently large size. Chest X-ray is essential to the diagnosis and should be reviewed by a skilled practitioner, as small pneumothoraces are easily missed. Pneumomediastinum has also been described in pregnancy and may present with chest pain and breathlessness. This condition is even less common than pneumothorax, although the two may coexist owing to a similar underlying cause. Pneumomediastinum may be due to oesophageal rupture and has been reported in association with hyperemesis gravidarum. Empyema may present with pleuritic or nonspecific chest pain and occurs most frequently as a complication of pneumonia, developing from a simple parapneumonic effusion. Up to two-thirds of pregnant women may have reflux, caused by relaxation of the gastro-oesophageal sphincter owing to high progesterone levels. However, the expression of heartburn may be different in individual women who may complain of chest pain indistinguishable from other causes. Usually the diagnosis can be made on clinical grounds alone (see Heartburn in pregnancy). Extrathoracic Peptic ulcer disease is less common in pregnant women, but the resultant upper abdominal pain may manifest as lower chest pain instead. Endoscopy may be necessary if symptoms fail to clear with drug treatment or complications such as gastrointestinal bleeding are apparent (see Epigastric pain in pregnancy). Other abdominal diseases, such as cholecystitis, gallstones, kidney stones, pyelonephritis, and acute pancreatitis, for example, may occasionally present with lower chest pain, which leads to diagnostic difficulty. One of these disorders might be suspected if there are other typical features in the history, such as pain occurring shortly after eating meals (especially with a high fat content) for gallstones; fever and/or rigors with cholecystitis and pyelonephritis; frequency, dysuria and haematuria with pyelonephritis and sometimes kidney stones; spasmodic pain with gallstones and kidney stones; or the presence of possible triggers for acute pancreatitis such as alcohol or known gallstones. The following provides an approach to the history and examination in the pregnant patient with chest pain (refer also to Chest pain in pregnancy: cardiac causes). Physical examination  key findings to look for General examination: fever, sweating, cyanosis, lymphadenopathy, jaundice, anaemia, inflamed throat, evidence of connective tissue disease. Respiratory system: increased respiratory rate, chest wall tenderness, chest wall masses, tracheal deviation, dullness to percussion, crackles, bronchial breathing, reduced or absent breath sounds on auscultation. History  key features to be elucidated History of the presenting complaint investigations Chest radiography delivers negligible radiation and is crucial to diagnosing or excluding important conditions such as pneumonia and pleural effusion. The consequences of misdiagnosis are potentially far Duration, onset, severity, nature and radiation of chest pain. Typically in pregnancy the woman becomes agitated, possibly short of breath, and then confused before losing consciousness and collapsing. Immediate assessment will determine whether the woman is conscious and breathing and whether there is any blood loss. Resuscitation should follow the standard Advanced Life Support protocols, and the diagnosis may only become clear as resuscitation proceeds. Ultrasonography is usually the first investigation of choice for possible abdominal pathology. The most common causes will be non-specific, and often no definite aetiology will be found. More serious causes should be apparent from the history, examination, and simple investigations. Venous pooling occurs in the lower limbs, and greater muscle activity is more necessary than in the non-pregnant state to ensure adequate venous return. Standing still for prolonged periods, standing up quickly, and lying supine in late pregnancy are more likely to cause fainting than in the non-pregnant woman. Hot weather increases peripheral vasodilatation and may contribute to the process. Loss of consciousness is not sudden and is preceded by a feeling of light-headedness or dizziness, cold sweating, and nausea. If the woman does not sit or lie down, these signs and symptoms will be rapidly followed by complete loss of consciousness and collapse. There may be injury from falling and, less commonly, seizures from cerebral anoxia if the woman is kept in an upright or semi-recumbent position. Consciousness usually returns quickly when the woman is placed in the recovery position. Pregnant women have a significant increase in blood volume and may lose 35 per cent of their blood volume without showing signs of hypovolaemia. When they decompensate, it may be more rapid than in non-pregnant women, and the degree of blood loss may be concealed. Fetal distress may be the first sign of hypovolaemia, as maternal blood flow is diverted from the abdominal and pelvic organs to maintain blood pressure and cerebral perfusion. Blood loss Ectopic pregnancy usually presents between 6 and 10 weeks of pregnancy, and 50 per cent of women presenting to hospitals will have been previously seen by a doctor who did not make the diagnosis. One in 80Â90 pregnancies are ectopic, though rates vary geographically, and this increases to one in 20 if the woman has conceived with assistance. Other risk factors for ectopic pregnancy are previous ectopic pregnancy, tubal damage including previous sterilisation and infection, and a history of fertility problems. Any woman of reproductive age admitted to hospital with shock and a loss of consciousness should be assumed to a) be pregnant, and b) have a ruptured ectopic pregnancy until proven otherwise. The woman will have signs of shock with tachycardia, rapid respirations, pallor, cold skin, and hypotension. Her abdomen is likely to be distended, and, depending on the level of consciousness, very tender with signs of peritonism  guarding and rebound. The latter are not invariable, however, and distension and tenderness may be difficult to assess if the woman is unconscious. A large intra-abdominal bleed causing shock is usually a straightforward diagnosis, and immediate surgery is required. In women of this age group without a history of trauma, ruptured ectopic pregnancy is the most likely diagnosis and is confirmed by a positive pregnancy test of bloods taken during resuscitation. In the second half of pregnancy, placental abruption is the most likely cause of blood loss sufficient to cause collapse, with a combination of concealed and overt bleeding. Hypovolaemia does not, of itself, usually cause collapse; however, the extravasation of blood into the myometrium can lead to a severe coagulopathy, disseminated intravascular coagulation with diffuse bleeding, and consequent haemorrhagic shock. The uterus is usually tender and firm and the fundus may be higher than expected, while the fetal heart rate is either abnormal or absent. While resuscitation is taking place, bloods should be taken for full blood count, group and cross match, Kleihauer and coagulation tests. The woman must be closely observed once she is haemodynamically stable, as a coagulopathy may not be evident at first and develop subsequently. Spontaneous uterine rupture is rare during pregnancy but more likely if the woman has a history of myomectomy or classical caesarean section. Distinguishing between amniotic fluid embolism and pulmonary embolism may be difficult, as the initial presentation will be similar, and adequate resuscitation will be the first priority. When stable, the woman should have a chest X-ray to exclude intrathoracic pathology such as pneumothorax, and a low dose ventilation/perfusion (V/Q) scan to confirm the diagnosis of pulmonary embolism. The V/Q scan is very likely to be diagnostic because of the profound disturbance of maternal physiology in this situation. A history of uterine surgery and the degree of abdominal pain suggest uterine rupture or a major intra-abdominal bleed. The fetus is usually dead unless the rupture occurs in hospital and delivery is accomplished very quickly. Abdominal trauma in pregnancy, whether due to automobile accidents, falls, or domestic violence, may lead to abruption, uterine rupture, or significant intra-abdominal bleeding resulting in collapse. Other causes of intra-abdominal bleeding are rare in pregnancy, but the rupture of congenital or pregnancy-related vascular aneurysms. It usually occurs during labour after rupture of the membranes; however, it has been reported after amniocentesis and first trimester curettage. Classically it is thought to be associated with hypertonic uterine activity and abruption, but these factors are not invariable. If the woman survives longer, a coagulopathy invariably develops rapidly and contributes to the haemorrhagic shock. The presentation is similar to pulmonary embolism, with shortness of breath and rapid collapse. Provided the woman survives the initial collapse following embolism, the developing coagulopathy distinguishes it from venous thromboembolism. The diagnosis is clinical and the purpose of investigations is to guide treatment. Blood should be taken for a full blood count, coagulation studies, and cross match. The detection of fetal squames in central venous blood confirms the diagnosis but does not usually assist management. Coagulopathy Serious blood loss causing collapse is often exacerbated by coagulopathy in pregnancy. Coagulation factors should be measured in severe pre-eclampsia but are unlikely to be abnormal if the platelet count is normal. Coagulopathy can be expected if collapse has occurred from abruption, amniotic fluid embolism, or massive haemorrhage of any cause. Embolism Pulmonary Venous thromboembolism occurs in 1 in 1,000 2,000 pregnancies and is a leading cause of maternal death in developed countries. Confirming the diagnosis of pulmonary embolism takes second place to resuscitation. This may occur as a result of trauma or spontaneously as seen in a subarachnoid haemorrhage. If traumatic in origin, the case will usually be obvious and should be suspected in any pregnant woman presenting with a significant head injury. In most cases, the blood pressure will be normal or elevated, and signs of raised intracranial pressure will be detected with papilloedema and cranial nerve abnormalities. The abrupt history, the clinical signs, and the absence of bleeding all indicate an intracranial cause that will normally need immediate neurosurgical review and probable intervention, though the outlook for many of these cases is poor. The diagnosis is often obvious in women with a history of preceding severe pre-eclampsia. These women may present with symptoms and signs of imminent eclampsia: severe headache, persistent visual disturbances, epigastric pain, and hyperreflexia. In these circumstances the seizures are likely to be caused by a hypertensive encephalopathy. However, in 20 per cent of cases the fit is the initial presentation with a normal or only mildly elevated blood pressure. Supportive care should be undertaken during the fit, and magnesium sulphate infusion commenced to prevent recurrence. As a result of the fit there may be external trauma or damage to the mouth or tongue. Failure to recognise the symptoms and signs of sepsis or respond appropriately may lead to septic shock, which can be rapidly fatal. As the condition worsens she will become shocked with poor tissue perfusion, hypoxia, hypotension, and oliguria. The diagnosis is made by noting the preceding history of infection and the diverse signs, as well as having an increased awareness of the protean nature and danger of sepsis in pregnant women. Blood should be taken for a full blood count, culture, biochemistry, liver function tests, and coagulation studies before treatment. However, treatment with broad-spectrum antibiotics and multi-system support as necessary should be instituted as quickly as possible without awaiting the results of the blood tests. Myocardial infarction Although most pregnant women are young and healthy, increasingly, older and less medically fit women are having babies. Women with ischaemic heart disease are at risk of myocardial infarction, although it remains a very rare cause of cardiac arrest in pregnancy. The diagnosis should be suspected when significant chest pain precedes the collapse. There may be a history of cardiac disease, but the diagnosis must be made as resuscitation continues. She appeared to be postictal, and it was assumed she had suffered an eclamptic seizure. The increased signal would be even more marked if the changes were a result of infarction.
Aciphex 10 mg order on-line. पेट जलà¥à¤¦à¥€ कैसे कम करें || How to loss belly fat at home || Rajiv dixit.
References
- Newman JP, LaFerriere KA, Koch RJ, et al. Transcalvarial suture fixation for endoscopic brow and forehead lifts. Arch Otolaryngol Head Neck Surg 1997;123:313.
- Cronenwett J, Johnston K: The United Kingdom Small Aneurysm Trial: implications for surgical treatment of abdominal aortic aneurysms, J Vasc Surg 29:191, 1999.
- Lowry LY, Evans DJ, Lowry RJ, et al. Under-registration for dental care of children with heart defects in the north-east of England: a comparative study. Prim Dent Care. 1996;3:68-70.
- Nowycky MC, Fox AP, Tsien RW: Three types of neuronal calcium channel with different calcium agonist sensitivity, Nature 316:440, 1985.
- Whyman MR, Fowkes FG, Kerracher EM, et al. Randomised controlled trial of percutaneous transluminal angioplasty for intermittent claudication. Eur J Vasc Endovasc Surg 1996;12(2):167-172.
- Nakamura H, Makino K, Yano S, et al. Epidemiological study of primary intracranial tumors: a regional survey in Kumamoto prefecture in southern Japan -20-year study. Int J Clin Oncol 2011; 16:314-321.