
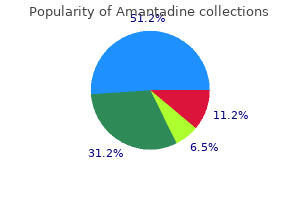
Amantadine
| Contato
Página Inicial
Michael J. Gonyeau, BS Pharm, PharmD, MEd, FNAP, FCCP, BCPS, RPh
- Clinical Professor
- Acting Chair, Department of Pharmacy and Health Systems Sciences
- Director of Undergraduate and Professional Programs, Northeastern University School of Pharmacy
- Clinical Pharmacist, Integrated Teaching Unit, Brigham and Womenメs Hospital, Boston, Massachusetts
https://bouve.northeastern.edu/bchs/directory/michael-gonyeau/
Acute inflammation may appear after a person has worn occlusive clothing for an extended period antiviral brand crossword order 100 mg amantadine fast delivery. Topical steroid creams are frequently prescribed for inflammatory skin disease of the groin antiviral plot 100 mg amantadine purchase, and they modify the typical clinical presentation of tinea antiviral condoms purchase amantadine 100 mg otc. This modified form (tinea incognito) may not be immediately recognized as tinea; the only clue is the history of a typical hiv infection statistics by country discount amantadine 100 mg with visa, half moonshaped plaque treated with cortisone cream hiv infection rate south africa purchase amantadine amex. Tinea cruris usually presents as a unilateral half moonshaped plaque that does not extend onto the scrotum. They infect the scrotum and show the typical fringe of scale at the border and satellite pustules. The sharp borders touch where the apposed surfaces of the skin folds of the groin and thigh meet. Obesity contributes to this inflammatory process, which may be infected with a mixed flora of bacteria, fungi, and yeast. Groin intertrigo recurs after treatment unless weight and moisture are controlled. Psoriasis and seborrheic dermatitis of the groin may mimic intertrigo (see the section Candidiasis of Large Skin Folds, p. Erythrasma differs in that it is noninflammatory, it is uniformly brown and scaly, and it has no advancing border. The most common site of erythrasma is in the fourth interdigital toe space, but infection is also seen in the inframammary fold and the axillae. Gram stain of the scale shows Gram-positive, rod-like organisms in long filaments. One technique is to strip the scale with clear tape and then carefully stain the taped-scale preparation. Erythrasma responds to erythromycin (250 mg four times a day for 5 days) or clarithromycin (single 1-g dose) or topically to miconazole, clotrimazole, and econazole creams (but not ketoconazole). Topical acne medication such as clindamycin or erythromycin applied two times a day for 2 weeks is effective. Some topical antibiotics contain alcohol and may be irritating when applied to the groin. Tinea cruris is effectively treated by 50 to 100 mg of fluconazole daily or 150 mg once weekly for 2 to 3 weeks. Itraconazole 100 mg twice daily immediately after meals on days 1 and 8 or on days 1 and 2 may be effective. Tinea of the Body and Face Tinea of the face (excluding the beard area in men), trunk, and limbs is called tinea corporis ("ringworm of the body"). There is a broad range of manifestations, with lesions varying in size, degree of inflammation, and depth of involvement. This variability is explained by differences in host immunity and the species of fungus. An epidemic of tinea corporis caused by Trichophyton tonsurans was reported in student wrestlers. Tinea of the groin responds to any of the topical antifungal creams listed in the Formulary. Lesions may appear to respond quickly, but creams should be applied twice a day for at least 10 days. The fungicidal allylamines (naftifine and terbinafine) and butenafine (allylamine derivative) allow for a shorter duration of treatment compared with fungistatic azoles (clotrimazole, econazole, ketoconazole, oxiconazole, miconazole, and sulconazole). Moist intertriginous lesions may be contaminated with dermatophytes, other fungi, or bacteria. The wet dressings are discontinued when the skin is dry, but the cream is continued for at least 14 days or until all evidence of the fungal infection has disappeared. A limited amount of topical steroid cream is prescribed to discourage long-term use. Betamethasone dipropionate/clotrimazole cream or solution may be used for initial treatment if lesions are red, inflamed, and itchy. Prolonged use of this steroid/antifungal preparation may not cure the infection and may cause striae in this intertriginous area. In classic ringworm, lesions begin as flat, scaly spots that then develop a raised border that expands at varying rates in all directions. Clear, central areas of the larger lesions are yellow-brown and usually contain several red papules. Pityriasis rosea and multiple small annular lesions of ringworm may appear to be similar. However, the scaly ring of pityriasis rosea does not reach the edge of the red border as it does in tinea. Other distinguishing features of pityriasis rosea include rapid onset of lesions and localization of the trunk. Tinea from cats may appear suddenly as multiple round to oval plaques on the trunk and extremities. Tinea Corporis (Tinea Gladiatorum) Tinea corporis has become common in competitive wrestling. The infection is more common in northern regions, where cattle are confined in close quarters during the winter. Intracutaneous and subcutaneous granulomatous nodules arise from these initial inflammatory tinea infections. Lesions have necrotic areas containing fungal elements; they are surrounded by epithelioid cells, giant cells, lymphocytes, and polymorphonuclear leukocytes, and they are believed to result from the rupturing of infected follicles into the dermis and subcutis, thus the term "granuloma. These variations may be a factor in allowing the dermatophytes to persist and grow in an abnormal manner. The area involved covers a few to 10 cm and may be red and scaly, but it is not as intensely inflamed as the T. Skin biopsy with special stains for fungi is required for diagnosis if hyphae cannot be demonstrated in scale or hair. The superficial lesions of tinea corporis respond to the antifungal creams described in the Formulary. Lesions usually respond after 2 weeks of twicea-day application, but treatment should be continued for at least 1 week after resolution of the infection. Extensive superficial lesions or those with red papules respond more predictably to oral therapy (see Table 13. Tinea corporis is treated by 50 to 100 mg of fluconazole daily or 150 mg once weekly for 2 to 4 weeks, or by 100 mg of itraconazole daily for 2 weeks or 200 mg daily for 7 days. Attempts at treatment with topical steroids extended infection into the follicular structures producing red papules. The patient responded to one month of twice daily application of econazole 1% topical cream. Dermatophytes are typically confined within the keratinized, epithelial layer of the skin. The pathogenic potential is dependent, however, on a variety of local and systemic factors affecting the natural host resistance to dermatophytic infection. Underlying systemic conditions that cause depressed cellular immunity, such as malignant lymphomas and Cushing disease, as well as the administration of exogenous steroids or immunosuppressive agents, can lead to atypical, generalized, or invasive dermatophyte infection. Invasive dermatophyte infection should be included in the differential diagnosis of nodular, firm, or fluctuant masses (particularly on the extremities). Several dermatophyte species have caused a deep, generalized infection in which the organism invaded various visceral organs. The dry keratotic form may be asymptomatic and the patient may be unaware of the infection, attributing the dry, thick, scaly surface to hard physical labor. Some authors believe that oral or topical antifungal agents do not alter the course of highly inflammatory tinea. However, oral antifungals are safe, and few physicians would withhold such therapy. This was followed by a trial of topical steroids and the infection became more intense. A potassium hydroxide examination revealed numerous fungal hyphae and the patient cleared with a 2-week course of oral terbinafine. The patient is often unaware of the infection and feels that these changes are secondary to dry skin or hard physical labor. A clinical diagnosis of psoriasis was made and the patient was treated with clobetasol cream. Fingernail infection often accompanies infection of the dorsum of the hand or palm. Treatment is the same as that for tinea pedis and, as with the soles, a high recurrence rate can be expected for palm infection. Tinea Incognito Fungal infections treated with topical steroids often lose some of their characteristic features. Topical steroids decrease inflammation and give the false impression that the rash is improving while the fungus flourishes secondary to cortisone-induced immunologic changes. Treatment is stopped, the rash returns, and memory of the good initial response prompts reuse of the steroid cream, but by this time the rash has changed. Inappropriate treatment of groin tinea with topical steroids has allowed the once localized infection to extend over a wide area. The diagnosis was difficult to make because a sharp border characteristic of a fungal infection disappeared with long-term use of the group V topical steroid. Large family size, crowding, and low socioeconomic status increase the chance of infection. Infectious fungal particles that have fallen from the infected person may be viable for months. Tinea capitis can be transmitted by infected persons, fallen hairs, animals, fomites. The animals may harbor the pathogen in their fur (colonization) although clinical symptoms may not be visible. Of the 3775 cases of tinea capitis reported to the European Confederation of Medical Mycology, 37. Asymptomatic scalp carriage of dermatophytes by classmates and adults is probably an important factor contributing to disease transmission and reinfection. Hair shaft infection is preceded by invasion of the stratum corneum of the scalp (see Chapter 24). The fungus grows down through this dead protein layer into the hair follicle and gains entry into the hair in the lower intrafollicular zone, just below the point where the cuticle of the hair shaft is formed. Because of the cuticle, the fungi cannot cross over from the perifollicular stratum corneum into the hair but must penetrate deep into the hair follicle to circumvent the cuticle. This may explain why topical antifungal agents are ineffective for treating tinea capitis. The fungi then invade the keratinized outer root sheath, enter the inner cortex, and digest the keratin contained inside the hair shaft. The growth of hyphae occurs within the hair above the zone of keratinization of the hair shaft and keeps pace with the growth of hair. Distal to this zone of active growth, arthrospores are formed within or on the surface of the hair, depending on the species of dermatophytes. Large spores can be seen as separate structures with the lowpower microscope objective. The fungus grows completely within the hair shaft, and the cuticle surface of the hair remains intact. A well-defined border may not be present and a once-localized process may have expanded greatly. Tinea incognito is most often seen on the groin, on the face, and on the dorsal aspect of the hand. Tinea infections of the hands are often misdiagnosed as eczema and treated with topical steroids. Hyphae are easily demonstrated, especially a few days after discontinuing use of the steroid cream when scaling reappears. Tinea of the Scalp Tinea of the scalp (tinea capitis) occurs most frequently in prepubertal children between 3 and 7 years of age. The species of dermatophyte likely to cause tinea capitis varies among different countries, but anthropophilic species (found in humans) predominate in most areas. Each animal is associated with a limited number of fungal species; therefore an attempt should be made to identify the fungus by culture to help locate and treat a possible animal source. Unlike other fungal infections, tinea of the scalp may be contagious by direct contact or from contaminated clothing; this provides some justification for briefly isolating those with proven infection. Large-spore endothrix pattern of hair invasion (Trichophyton tonsurans, "a sack of marbles"). Arthrospores inside the shafts of infected hairs weaken the hair and cause it to break off at or below the scalp surface, resulting in the "black dot" appearance of the surface. Pediatr Dermatol 1985;2(3):22437; reproduced by permission of Blackwell Scientific Publications. The arthrospores are located both on the inside of the hair shaft and on the outer surface to produce the ectothrix pattern seen under the microscope. There are three patterns of hair invasion: small-spored ectothrix, largespored ectothrix, and large-spored endothrix. An approach for the clinical diagnosis, laboratory investigations, and management of tinea capitis is presented in Boxes 13. A severe, inflammatory reaction with a boggy, indurated, tumor-like mass that exudes pus is called a kerion; it represents a hypersensitivity reaction to fungus and heals with scarring and some hair loss.
A translucent yellow-red discoloration resembles a drop of oil beneath the nail plate hiv infection rates nigeria order amantadine 100 mg online. It occurs from psoriasis of the nail bed herpes zoster antiviral drugs 100 mg amantadine purchase fast delivery, which causes serum to be trapped under the nail plate hiv infection urine buy amantadine 100 mg with mastercard. Other features can include enthesitis antiviral eye ointment order 100 mg amantadine, dactylitis hiv symptoms three months after infection order 100 mg amantadine with visa, iritis, peripheral arthritis (oligoarticular asymmetric and polyarticular symmetric), spondylitis, and a variable clinical course. The heterogeneity in clinical presentation and course makes PsA difficult to classify and differentiate from other forms of SpA and inflammatory arthropathies. Dactylitis presents as the "sausage digit" diffuse swelling of the entire digit. T-cell subpopulations Th1, Th2, Th17, Th9, Th22, and Treg cells secrete proinflammatory or antiinflammatory cytokines. These proinflammatory mediators activate resident cells, including synovial fibroblasts, chondrocytes, and osteoblasts, which in turn secrete more proinflammatory mediators that can further recruit immune cells into the joins, creating a selfperpetuating inflammatory response. The inflamed synovial microenvironment leads to the formation of the synovial pannus, entheseal inflammation, and joint destruction. The Moll and Wright classification was developed more than 30 years ago and is still used today to divide PsA into five clinical subtypes (Table 8. These criteria were established for patients with long-standing disease duration (mean, 12. The small joints of the hands and feet, wrists, ankles, knees, and elbows may be involved. The most severe form of psoriatic arthritis involves osteolysis of any of the small bones of the hands and feet. Severe osteolysis leads to digital telescoping, producing the "opera glass" deformity. Gout is often associated with periarticular inflammation, which is not seen in PsA. Classification criteria for psoriatic arthritis and ankylosing spondylitis/axial spondyloarthritis. Magnetic resonance imaging and ultrasonography detect enthesitis (inflammation at the point of insertion of skeletal muscle to bone). For peripheral arthritis, conventional disease modifying antirheumatic drugs are considered early in the treatment of PsA. Methotrexate may also be given as a single dose or divided into two doses taken 12 hours apart. The amount is increased to 25 to 30 mg/week, until control is obtained, and then tapered to a maintenance dose of around 5 to 15 mg/week. Etanercept (Enbrel), Adalimumab (Humira), Infliximab (Remicade), Golimumab (Simponi). Group for research and assessment of psoriasis and psoriatic arthritis 2015 treatment recommendations for psoriatic arthritis. Apremilast, an oral inhibitor of phosphodiesterase, is effective for moderate to severe plaque psoriasis and PsA. Patients become discouraged with moderately effective expensive topical treatment that lasts weeks or months. One intralesional steroid injection (510 mg/mL triamcinolone acetonide) can heal a small plaque and keep it in remission for months. Topical steroid creams and ointments, calcitriol, calcipotriene, tazarotene, and tar are the mainstays of topical treatment. Effective programs can be designed for patients who do not have access to a therapeutic light source and for patients who have limited disease. Without light, tar is moderately effective, but persistent use of calcipotriene or tazarotene can clear the disease and offers the patient substantial remission periods. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. Guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions. Stains hair and clothes Irritating, expensive; pregnancy category X; excreted in mammalian milk Only moderately effective in a few patients Expensive, office-based therapy Effective, long remissions possible New preparations are pleasant Insurance may cover part or all of treatment, effective for 70% of patients, no need for topical steroids Tape or occlusive Convenient, no mess dressing Intralesional steroids Excimer laser Convenient, rapidly effective, long remissions Useful for palmoplantar, scalp and nail psoriais Expensive, only for limited disease Only for limited areas, atrophy and telangiectasia occur at injection site Only for limited areas, office-based treatment May be used to occlude topical steroids Ideal for chronic scalp and body plaques when small and few in number Best utilized for isolated plaques and as a adjunct treatment for topical and systemic agents work quickly, but total eradication of the plaques is difficult to accomplish; remission times are short, and the creams become less effective with continued use. Patients with psoriasis covering more than 5% of the body need special treatment programs (see Table 8. Residual erythema, hypopigmentation, or brown hyperpigmentation is common when the plaque clears; patients frequently mistake the residual color for disease andcontinuetreatment. Iftheplaquecannotbefeltby drawing the finger over the skin surface, treatment may be stopped. Patients should apply an emollient to the previously treated areas to keep the skin healthy and prevent recurrence. Some treatments are better suited for rapid clearing; others are better suited to be maintenance treatment. The optimum management involves the sequential use of therapeutic agents involving three steps, namely: the clearing phase, the transitional phase, and the maintenance phase. Topical Therapy Topical Steroids Topical corticosteroids are first-line drugs for limited disease (Box 8. Corticosteroids are antiinflammatory, antiproliferative, immunosuppressive, and vasoconstrictive. Toxicities · Local skin atrophy, telangiectasia, striae, purpura, contact dermatitis, rosacea · Systemic hypothalamicpituitaryadrenal axis suppression may occur with use of medium- and high-potency topical steroids. Increasedintraocularpressure,glaucoma,and cataracts have been reported with use around the eye. Ongoing monitoring · Assessment of growth in children using long-term topical corticosteroids · Regular skin checks for all patients receiving longterm therapy to assess for atrophy Pregnancy: Category C Nursing: Unknown safety Pediatric use: Because of the increased skin surface/ body mass ratio, the risks to infants and children may be higher for systemic effects secondary to enhanced absorption. Patients with thick, chronic plaques require treatment with the highest potency corticosteroids,suchasclobetasol. ForclassIcorticosteroids, the available data allow for 2 to 4 weeks of use with increased risk of both cutaneous side effects and systemic absorption if used continuously for longer periods of time. A gradual reduction in the frequency of usage following clinical response is accepted practice. Initially,whenthepatientisintroduced to topical steroids, the results are most gratifying. However, tachyphylaxis, or tolerance, occurs, and the medication becomes less effective with continued use. Patients remember the initial response and continue topical steroids in anticipation of continued effectiveness. Plastic occlusion of topical steroids is much more effective than simple application. Augmented betamethasone dipropionate and clobetasol are extremely potent, and occlusion is not used with these drugs. Group V topical steroids applied once or twice a day should be used in the intertriginous areas and on the face. Some plaques resolve completely, but most remain only partially reduced with continued application. Remissions are usually brief and the plaques may return shortly after treatment is terminated. Topical steroid creams applied under an occlusive plastic dressing promote more rapid clearing, but remissions are not extended. The rapid appearance of atrophy and telangiectasia occurs when the group I topical steroids are occluded. Multiple small intralesional injections of plaques with triamcinolone acetonide 5 to 10 mg/mL almost invariably clears the lesion and accords long-term remission. Betamethasone valerate foam and clobetasol propionate foam are available in 50-g and 100-g containers. These formulations are very effective and preferred by many patients to creams, ointments, and solutions for treating scalp lesions and plaque psoriasis on the trunk and extremities. Intralesional Steroids Patients with a few, small, chronic psoriatic plaques of the scalp or body can be effectively treated with a single intralesional injection of triamcinolone acetonide 5 to 10 mg/mL. The 10 mg/mL solution may be diluted with saline or 1% lidocaine with epinephrine. Topical Calcineurin Inhibitors the topical calcineurin inhibitors tacrolimus and pimecrolimus block the synthesis of inflammatory cytokines. They are useful for thinner skin areas such as facial and intertriginous psoriasis. They do not cause atrophy or hypopigmentation as do topical corticosteroids in these regions. The most common side effect is burning and itching that reduces with ongoing usage and can be reduced by not applying immediately after bathing. Both are pregnancy category C, are found in human milk, and are not recommended for nursing mothers. Vitamin D Analogues (Calcipotriene, Calcitriol) Vitamin D3 analogues inhibit epidermal cell proliferation and enhance cell differentiation. They are effective and safe and well tolerated for the short- and long-term treatment of psoriasis. It is not as effective as betamethasone valerate, but it does not have the corticosteroid sideeffectofatrophy. Most patients now use the following regimen: calcipotriene is applied in the morning and a group I corticosteroid is applied in the evening for 2 weeks. Application for 6 to 8 weeks gives a 60% to 70% improvement in plaquetype psoriasis. Application of calcipotriene twice a day is much more effective than once-a-day application. Calcipotriene treatment can produce a mild irritant contact dermatitis at the site of application. Hypercalcemia is reported with excessive quantities of calcipotriene applied over large surface areas. Use with caution in patients receiving medications known to increase serum calcium levels, such as thiazide diuretics. Caution should also be exercised in patients receiving calcium supplements or high doses of vitamin D. Itisappliedonceeachday and is indicated for the topical treatment of psoriasis in adults 18 years of age and older. The solution can be used acutely for 4 to 8 weeks to bring psoriasis under control. After this, control of the disease can be maintained with once-daily application as needed. Irritationmay be reduced by use of the cream formulation, use of the lower concentration product, combination use with moisturizers, application on alternate days, short-contact (30 to 60 minutes) treatment, and application in combination with topical corticosteroids. Treatment consists of application of tazarotene once a day and a topical steroid approximately 12 hours later. Remission of psoriasis may be maintained for at least 5 months with a regimen of tazarotene gel 0. Tazarotene causes thinning of the stratum corneum of the epidermis, allowing patients to burn more easily. Tazarotene is a teratogenic retinoid and is pregnancy category X; therefore use in pregnancy is avoided. Thirty-six to 45% of patients experience clear to almost clear skin after 8 weeks of application. The Goeckerman regimen consists of the combination of crude coal tar alongwithultravioletlight. Coal tar formulations are often poorly tolerated because ofstainingofclothesandtarodor. The response is unpredictable but many patients are gratified with this safe, inexpensive treatment. Anthralin Antralin cream (Anthralin 1% cream) is applied to the skin and scalp daily for 30 minutes and then washed off. Antralin is more effective when used along with phototherapy and or a topical steroid. Nonmedicated Topical Moisturizers Nonmedicated topical moisturizers may be effective treatment. Patients who are dissatisfied with irritating, expensive prescription topical medications often turn to use of just topical moisturizers with a gratifying effect. They are more effective at maintaining skin health and thereby decrease skin inflammation. Ultraviolet Light Therapy Ultraviolet light therapy has been used for decades to successfullytreatpsoriasis. Guidelines of care for the treatment of psoriasis with phototherapy and photochemotherapy have been published. Complete clearing occurred in 47% of the cases in an average of 5 weeks; another 41% of those tested showed improvement. Waterproof tape with low-moisture vapor transmission applied continually for 1 week gave similar results. An adhesive hydrocolloid dressing (Duoderm) may be applied alone or over topical steroids and changed every 1 to 7 days. Treating the Scalp the scalp is difficult to treat because hair interferes with the application of medicine and shields the skin from ultraviolet light. Superficial scale can be removed with shampoos that contain tar and salicylic acid. When used at least every other day, tar shampoos (see the Formulary) may be effective in controlling moderate scaling. Treatment is repeated each night for 1 to 3 weeks until itching and erythema are controlled. Betamethasone valerate foam and clobetasol foam become a liquid upon contact with the skin. Small plaques are effectively treated with intralesional steroid injections of triamcinolone acetonide 5 to 10 mg/ mL.
Typically there is diffuse swelling of an arm or leg and intense pain on palpation hiv infection rates manchester order generic amantadine canada. About 1 or 2 days after symptom onset antiviral us release generic amantadine 100 mg without prescription, the patient has high fever side effects of antiviral medication amantadine 100 mg purchase line, leukocytosis hiv infection uk buy amantadine 100 mg mastercard, edema with central patches of dusky blue discoloration hiv infection game order cheapest amantadine and amantadine, weeping blisters, and borders with cellulitis. Septicemia may develop secondarily and should be strongly suspected in the presence of fever, anorexia, nausea, diarrhea, confusion, and hypotension. Progression to gangrene, sometimes with myonecrosis, and an extension of the inflammatory process along fascial planes are possible. Mortality in this group approaches 50% to 70% in patients with hypotension and organ failure. The polymicrobial necrotizing infection is associated with: (1) surgical procedures involving the bowel or penetrating abdominal trauma, (2) decubitus ulcers or perianal abscesses, (3) sites of injection in injection drug users, and (4) extension from a Bartholin abscess or a minor vulvovaginal infection. Gas may be present in clostridial and mixed aerobic/anaerobic infections but it is never present in group A streptococcal infections. Direct inspection at surgery shows the fascia is swollen and dull gray in appearance, with stringy areas of necrosis. Gram-positive cocci in chains suggest Streptococcus organisms (either group A or anaerobic). Patients in whom the etiologic agents cannot be definitively identified should be treated with broad-spectrum antimicrobial regimens. Surgical exploration is indicated when the diagnosis of infection is in doubt and the patient is very ill. Surgery can establish a diagnosis by providing material for culture, Gram staining, and histopathologic examination. Options for treatment include simple drainage, radical debridement, or amputation. Wounds can discharge copious amounts of tissue fluid and administration of fluid is often necessary (Table 9. Gas Gangrene Gas gangrene is a rapidly progressive infection caused by Clostridium perfringens, Clostridium septicum, Clostridium histolyticum, or Clostridium novyi. Penetrating trauma or crush injuries associated with interruption of the blood supply are the usual predisposing factors. Necrotizing fasciitis and gas gangrene may cause necrosis of skin, subcutaneous tissue, and muscle. There is no response to antibiotics, no reduction in fever or toxicity, or no lack of advancement. Profound toxicity, fever, hypotension, or advancement of the skin and soft tissue infection during antibiotic therapy occurs. When the local wound shows any skin necrosis with easy dissection along the fascia by a blunt instrument, more complete incision and drainage are required. Any soft tissue infection accompanied by gas in the affected tissue suggests necrotic tissue and requires operative drainage and/or debridement. Parenteral clindamycin and penicillin are used for severe group A streptococcal and clostridial necrotizing infections. Antimicrobials directed against aerobic Gram-positive, Gram-negative bacteria and anaerobes are used in mixed necrotizing infections. Folliculitis is very common and is seen as a component of a variety of inflammatory skin diseases, which are listed in Table 9. In superficial folliculitis, the inflammation is confined to the upper part of the hair follicle. Inflammation of the entire follicle or the deeper portion of the hair follicle initially appears as a swollen, red mass, which eventually may point toward the surface, becoming a somewhat larger pustule than that seen in superficial folliculitis. Staphylococcal Folliculitis Staphylococcal folliculitis is the most common form of infectious folliculitis. Staphylococcal folliculitis may occur because of injury, abrasion, or nearby surgical wounds or draining abscesses. Follicular pustules are cultured, not by touching the pustule with a cotton swab, but by scraping off the entire pustule with a no. If cut below the surface by shaving, the sharp-tipped whisker may curve into the follicular wall or emerge and curve back to penetrate the skin. A tender, red papule or pustule occurs at the point of entry and remains until the hair is removed. Generally, the problem is more severe in the neck area where hair follicles are more likely to be oriented at low angles to the skin surface, making repenetration of the skin more likely. Normal bacterial flora may eventually be replaced by pathogenic organisms if the process becomes chronic. Pseudofolliculitis of the beard is a significant problem in the armed services and in professions in which individuals are required to shave. Prevention and Treatment Programs for treatment and prevention are outlined in Boxes 9. Folliculitis keloidalis nuchae and pseudofolliculitis barbae: are prevention and effective treatment within reach Wash the beard for several minutes in a circular motion with a washcloth or toothbrush to dislodge ingrown hairs. Dislodge embedded hair shafts by inserting a firm, pointed instrument such as syringe needle under the hair loop and firmly elevating it. Corticosteroids (prednisone at 40 to 60 mg/day for 5 to 10 days) may be used in moderate to severe cases to reduce inflammation around the hair follicles until the hair grows and is no longer an aggravating factor. For a long-term solution to pseudofolliculitis barbae, laser hair removal may be the best option. The only definitive cure is permanent removal of the hair follicle with laser-assisted hair removal. Use techniques that avoid close shaves and the production of sharply angled hair tips. Hydrating the beard before shaving by washing with soap and warm water softens the whiskers. The softened hairs are cut off directly, leaving a blunt hair and making the development of ingrown hairs less likely. Shaving closely with multiple razor strokes and shaving against the grain should be avoided. Depilatories with barium sulfide (Magic Shave and Royal Crown powders) or calcium thioglycolate (Nair lotion, Magic Shave gold powder) are available online and in pharmacies. This hydrates the hair so that it cuts more easily and leaves a tip that is not sharp. Use a soft-bristled toothbrush, in a circular motion, to dislodge hair tips that are piercing the skin. This special razor cuts the hair at the correct length and prevents hair tip reentry into the skin. Rinse blade after each shaving stroke to prevent the traction that occurs with buildup of hair between the blade and guard. Defining pseudofolliculitis barbae in 2001: a review of the literature and current trends. A group of small, pinpoint, follicular pustules remains in the same areas for years. Scratching, wearing tightfitting clothing, or treating with abrasives may infect these sterile pustules and cause a diffuse eruption. The weakened hair fibers shear when the material is removed, leaving a soft, fluffy hair tip that is less likely to become ingrown. Several different lasers are available for the permanent removal of the beard hair. Clinically, a group of small, pinpoint, follicular pustules remains in the same area for years. Histologic studies show that the inflammation actually occurs outside of the hair follicle. It is important to recognize this entity to avoid unnecessary and detrimental treatment. Group V topical steroids provide temporary relief when the area becomes dry and inflamed. Sycosis Barbae Sycosis implies follicular inflammation of the entire depth of the hair follicle and may be caused by infection with S. In chronic cases, the pustules may remain confined to one area, such as the upper lip or neck. The hairs are epilated with difficulty in staphylococcal sycosis and with relative ease in fungal sycosis. Hairs should be removed and examined for fungi and the purulent material should be cultured. Fungal infections tend to be more severe, producing deeper and Keratosis Pilaris With Folliculitis Keratosis pilaris is a common finding on the posterolateral aspects of the upper arms and anterior thighs. Recurrences are not uncommon and require an additional course of oral antibiotics. Acne Keloidalis Acne keloidalis (see Chapter 24) is a primary form of scarring alopecia. It is a chronic scarring folliculitis of unknown etiology located on the posterior neck that eventually results in the formation of a group of keloidal papules. Histologically there is inflammation, fibroplasia, and disappearance of sebaceous glands. Extensive subclinical disease may be present and can account for some of the permanent hair loss. Keloidal papules may eventually form on the back of the neck after chronic inflammation of the hair follicles. Several hairs may protrude from a single follicle and look like tufted hair folliculitis. Overgrowth of microorganisms does not appear to play an important role in the pathogenesis. Treatment A bacterial etiology has never been proven but acne keloidalis usually responds to short- or long-term courses of oral antibiotics. Control with one antibiotic may diminish with time and the patient may need to be treated with a different antibiotic for continued long-term suppression. Topical steroid foams applied twice daily in short courses may control inflammation and reduce the keloids. An intralesional injection of triamcinolone reduces the keloids, but this treatment should be delayed until infection has been controlled. Successful surgical therapy of advanced cases can be carried out using a number of methods as long as subfollicular destruction of the process is achieved. Excision with primary closure is an excellent surgical treatment for extensive and refractory cases. An abscess is a cavity formed by finger-like loculations of granulation tissue and pus that extends outward along planes of least resistance. Furunculosis occurs as a self-limited infection in which one or several lesions 9 Bacterial Infections 355 are present or as a chronic, recurrent disease that lasts for months or years, affecting one or several family members. Most patients with sporadic or recurrent furunculosis appear to be otherwise healthy and have an intact immune system. Location Lesions may occur at any site but favor areas prone to friction or minor trauma, such as underneath a belt, the anterior thighs, buttocks, groin, axillae, and waist. The infecting strain may be found during quiescent periods in the nares and perineum. There is evidence that the anterior nares and perineum are the primary sites from which the staphylococcus is disseminated to the skin. In general, the microbiology of abscesses reflects the microflora of the anatomic part of the body involved. Bacteria colonize the skin in patients with atopic dermatitis, eczema, and scabies. Predisposing Conditions Occlusion of the groin and buttocks by clothing, especially in patients with hyperhidrosis, encourages bacterial colonization. Follicular abnormalities, evident by the presence of comedones and acneiform papules and pustules, are often found on the buttocks and axillae of patients with recurrent furunculosis of those areas; these findings suggest the diagnosis of hidradenitis suppurativa (see p. Pain is most intense in areas where expansion is restricted, such as the neck and external auditory canal. The abscess either remains deep and reabsorbs or points and ruptures through the surface. The abscess cavity contains a surprisingly large quantity of pus and white chunks of necrotic tissue. The infection originates deep in the dermis and the subcutaneous tissue, forming a broad, red, swollen, slowly evolving, deep, painful mass that points and drains through multiple openings. Deep extension into the subcutaneous tissue may be followed by sloughing and extensive scarring. Enlarged swollen mass with purulent material beginning to exude from several points on the surface. A large mass of white, amorphous material and pus exudes after a linear incision is made over the surface. An intense, foreign-body, inflammatory reaction occurs in hours, forming a sterile abscess. Treatment of a ruptured cyst consists of making a linear incision over the surface and evacuating the white material with manual pressure and a curette. In many cases the wall cannot be removed because it is fused to the dermis during the inflammatory process. Treatment of Furuncles Many furuncles are self-limited and respond well to frequent applications of a moist, warm compress, which provides comfort and probably encourages localization and pointing of the abscess. Hidradenitis suppurativa Cystic acne Primary immunodeficiency diseases* Secondary immunodeficiency Others: diabetes, alcoholism, malnutrition, severe anemia, debilitation *Syndrome of hyperimmunoglobulinemia E associated with staphylococcal abscesses (Job syndrome), chronic granulomatous disease, ChédiakHigashi syndrome, C3 deficiency, C3 hypercatabolism, transient hypogammaglobulinemia of infancy, immunodeficiency with thymoma, WiskottAldrich syndrome. For simple abscesses or boils, incision and drainage alone is likely to be adequate. Antibiotic therapy is recommended for abscesses associated with the following conditions: presence of severe or extensive disease.
Syndromes
- Blurred vision and slow vision loss over time
- Psoriasis
- Rheumatoid arthritis
- Muscle aches
- Coma
- Ehlers-Danlos syndrome
- Pediatrics
- The doctor may also order periodic computed tomography (CT) scans of your chest, abdomen, and pelvic area.
- You feel a lump in the scrotum
- Low blood pressure
Sclerodactyly evolves through three phases: the edematous phase hiv infection experiences 100 mg amantadine order otc, indurative phase hiv virus infection process order amantadine master card, and atrophic phase hiv symptoms days after infection discount amantadine. The edematous phase begins with finger swelling hiv infection rates in los angeles order amantadine 100 mg line, morning stiffness antiviral gel for chickenpox cheap amantadine express, and arthralgias. A subset of patients with antibodies to centromere and histone have severe pulmonary or vascular disease. Office Nail Fold Capillary Microscopy A technique has been described for characterizing the telangiectasias seen in the proximal nail fold of the various connective tissue diseases. The technique used by Minkin and Rabhan is as follows: A drop of mineral oil is placed on each nail fold. Because the field of observation is smaller than in wide-field microscopy, the ophthalmoscope must be moved over the entire nail fold. A technique for using a television camera to record nail fold capillary characteristics has been described. In scleroderma and dermatomyositis the capillary loops are enlarged, deformed, and dilated. In lupus the capillaries are tortuous but there is little dilation of capillary loops. Cutaneous ulcers are protected with an occlusive dressing such as hydrocolloid dressings. Pruritus tends to occur early in the course of diffuse disease, especially over the forearms, and disappears after months or several years. Simple surgical excision may be performed if the overlying skin is intact and is not infiltrated with calcium, which may interfere with wound healing. When skin breakdown and draining fistulous tracts occur from deeper deposits in deeper levels, primary wound closure is not possible. Intense, sterile, inflammatory reactions surrounding hydroxyapatite deposits, along with constitutional symptoms such as low-grade fever, may be dramatically improved by a course of oral colchicine 0. A daily physical therapy program emphasizing full range of motion of all large joints is important. Therapies for scleroderma target the immune system, with the goal of reducing inflammation and secondary tissue injury and fibrosis. Therapy targeting underlying vascular disease is designed to improve the symptoms of Raynaud phenomenon and to reduce ischemic injury to involved organs. Prostacyclins are a therapeutic option in patients with secondary Raynaud phenomenon. The presence of bushy capillaries is suggestive of mixed connective tissue disease. Loss of capillaries produces many avascular areas and disruption of the orderly appearance of the capillary bed. Patients with Raynaud phenomenon who present with avascularity and/or a mean of more than two megacapillaries per digit are likely to progress to a scleroderma spectrum disorder. The scleroderma pattern is present in 63%, the lupus pattern in 22%; 73% have bushy capillary formation. In lupus there are tortuous, "meandering" capillary loops, but there is relatively little dilation of the capillary limbs. There is usually some disorganization of the capillary pattern, but only rarely are avascular areas seen. There is a close association between the degree of visible capillary abnormalities and organ involvement. Recent trials demonstrate promising results in the treatment of interstitial lung disease with cyclophosphamide, and treatment of vascular disease of the lungs and digits with endothelin receptor antagonists, the phosphodiesterase inhibitor sildenafil, and prostacyclins. Rituximab and stem Morphea (Localized Scleroderma) Morphea, also known as localized scleroderma, is a rare fibrosing disorder. Patients with morphea may have systemic symptoms, such as malaise, fatigue, arthralgias, and myalgias, and positive autoantibody serologies. The first was proposed in 1995 and classifies morphea into five groups: plaque, generalized, bullous, linear, and deep (Table 17. Like scleroderma, morphea begins spontaneously and involves thickening or sclerosis of the skin. The two diseases differ in appearance, in the extent of the lesions, and in evolution. Scleroderma appears as a bound-down skin thickening with minor skin color change, progresses to involve large contiguous areas of skin, and does not improve with time. The lesions of morphea begin as one to several circumscribed areas of purplish induration. After weeks or months, the major portion of the central region of discoloration becomes thickened, firm, hairless, and ivorycolored. The smooth, dull, white, waxy surface is elevated, in contrast to the diffusely bound-down skin of scleroderma. During the active stage, the round to oval plaques slowly extend peripherally but do not increase very much in size. AC, A single or a few oval areas of nonpitting erythema and edema typically appear on the trunk. The center of the lesion then develops smooth, ivory-colored hairless or hyperpigmented plaques, and the ability to sweat is lost. Oval or round, circumscribed deep induration of skin involving subcutaneous tissue extending to fascia and may involve underlying muscle. Sometimes primary site of involvement is in subcutaneous tissue without involvement of skin. Linear induration involving dermis, subcutaneous tissue, and, sometimes, muscle and underlying bone; affects limbs and trunk. Linear induration that affects face and scalp and sometimes involves muscle and underlying bone. ParryRomberg syndrome or progressive hemifacial atrophy: loss of tissue on one side of face that may involve dermis, subcutaneous tissue, muscle, and bone. Induration of skin starting as individual plaques (4 or more and larger than 3 cm) that become confluent and involve at least 2 out of 7 anatomic sites (head and neck, right upper extremity, left upper extremity, right lower extremity, left lower extremity, anterior trunk, posterior trunk). Circumferential involvement of limb(s) affecting skin, subcutaneous tissue, muscle, and bone. Order of concomitant subtypes, specified in bracket, will follow their predominant representation in individual patients. Patients with localized scleroderma, especially those with morphea, should be carefully screened for concomitant lichen sclerosus, including inspection of the anogenital region. Extracutaneous manifestations of morphea are most common with generalized morphea and include myalgia, arthralgia, and fatigue. In a review of 750 children with morphea, 22% of the children had extracutaneous manifestations. The most common extracutaneous symptom was arthralgia, affecting 10% of the children. Of children with morphea, 2% to 5% have an autoimmune disease (vitiligo, insulin-dependent diabetes mellitus, Hashimoto thyroiditis, Graves disease, and ulcerative colitis); 30% of adults with morphea have an autoimmune disease, including psoriasis. Most reported cases are probably cases of lichen sclerosus et atrophicus; in fact, the 17 Connective Tissue Diseases 711 factor. Antihistone antibodies are more prevalent in childhood-onset than in adult-onset morphea. Antihistone antibodies have been detected in 42% of patients with localized scleroderma and in 87% of patients with generalized morphea. Early active lesions show inflammatory cells in the dermis and subcutaneous tissue. The collagen becomes eosinophilic and increases to occupy portions of the subcutaneous fat. Inducing atrophy by infiltrating with triamcinolone acetonide (10 mg/mL) may be useful in areas where skin thickening has resulted in discomfort or limitation of motion. Thickened tissue offers great resistance to infiltration, and scattered pitted areas of atrophy rather than a uniform decrease in plaque thickness may result. Early inflammatory lesions resolved and late sclerotic lesions softened without improvement in atrophy and scarring. The fundi should be examined by an ophthalmologist before antimalarials are started and should be monitored periodically. Linear Scleroderma Lesions of linear scleroderma have bands of sclerotic skin that often cross joint lines and lead to mild, but occasionally severe and disabling, joint contractures. The female-to-male ratio is 4: 1, and 83% of patients are younger than 25 years old when the disease begins. Most lesions occur on the extremities, and two or more lesions appear simultaneously (61%), often bilaterally (46%). It remains controversial whether linear scleroderma follows the lines of Blaschko. In one study, peripheral blood eosinophilia (200 to 2500 cells/mm3) occurred in 50% of patients with early active disease and declined with time. This may explain why lesions may be fixed to underlying structures and extend to muscle or bone. Early and continued physical therapy is crucial to maintain adequate joint motion. Methotrexate should be used early in juvenile localized scleroderma, especially in linear, generalized, pansclerotic, and mixed subtypes. The treatment is generally well tolerated with rare occurrence of significant adverse events. In time, atrophy of one side of the face may occur, giving the impression that a blade was turned to the side to remove a thickness of skin after landing vertically. Photoprotective effects of a broad-spectrum sunscreen in ultravioletinduced cutaneous lupus erythematosus: a randomized, vehicle-controlled, double-blind study. Response to antimalarial agents in cutaneous lupus erythematosus: a prospective analysis. Efficacy of mycophenolate mofetil in antimalarial-resistant cutaneous lupus erythematosus. Low blood concentration of hydroxychloroquine in patients with refractory cutaneous lupus erythematosus: a French multicenter prospective study. Management of cutaneous lupus erythematosus with low-dose methotrexate: indication for modulation of inflammatory mechanisms. Incidence of dermatomyositis and clinically amyopathic dermatomyositis: a population-based study in Olmsted County, Minnesota. Calcinosis cutis occurring in association with autoimmune connective tissue disease: the Mayo Clinic experience with 78 patients, 1996-2009. Novel classification of idiopathic inflammatory myopathies based on overlap syndrome features and autoantibodies: analysis of 100 French Canadian patients. Juvenile localized scleroderma: clinical and epidemiological features in 750 children. Coexistence of lichen sclerosus and morphea: a retrospective analysis of 472 patients with localized scleroderma from a German tertiary referral center. Pulsed high-dose corticosteroids combined with low-dose methotrexate in severe localized scleroderma. A long-term follow-up study of methotrexate in juvenile localized scleroderma (morphea). Histopathologic manifestations of systemic diseases: the example of cutaneous lupus erythematosus. Subacute cutaneous lupus erythematosus: a cutaneous marker for a distinct lupus erythematosus subset. Overlapping syndromes, undifferentiated connective tissue disease, and other fibrosing conditions. Updating the American College of Rheumatology preliminary classification criteria for systemic sclerosis: addition of severe nailfold capillaroscopy abnormalities markedly increases the sensitivity for limited scleroderma. Systemic sclerosis sine scleroderma: an unusual presentation in scleroderma renal crisis. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Clinical and histopathologic features and immunologic variables in patients with severe chilblains. Bullous morphea: clinical, pathologic, and immunopathologic evaluation of thirteen cases. Symmetrical pigmented sclerosis enclosed by pruritic erythema: a new variant of morphoea Keloid morphea and nodular scleroderma: two distinct clinical variants of scleroderma Clinical Manifestations the prodromal symptoms, morphologic configuration of the lesions, and intensity of systemic symptoms vary. Differential Diagnosis of Erythema Multiforme Bullous pemphigoid Dermatitis herpetiformis Drug eruptions Leukocytoclastic vasculitis Lupus erythematosus Pityriasis rosea Polymorphic light eruption StevensJohnson syndrome Toxic epidermal necrolysis Urticaria Urticarial vasculitis Viral exanthems forms of the disease may be preceded by malaise, fever, or itching and burning at the site where the eruption will occur. The cutaneous eruptions are most distinctive, and classification is based on their form. Dusky red, round maculopapules appear suddenly in a symmetric pattern on the backs of the hands and feet and on the extensor aspect of the forearms and legs. The mature target lesion consists of two distinct zones: an inner zone of acute epidermal injury with necrosis or blisters and an outer zone of erythema. Partially formed targets with annular borders or target lesions on the palms and soles are less distinctive and clinically resemble urticaria. Patients with many target lesions respond rapidly to a 1- to 3-week course of prednisone.
Order amantadine 100 mg. The Ebola Virus Explained — How Your Body Fights For Survival.
References
- Powell PH, Smith PJ, Feneley RC: The identification of patients at risk from acute retention, Br J Urol 52(6):520n522, 1980.
- Aksoy Y, Ozbey I, Atmaca AF, et al: Extracorporeal shock wave lithotripsy in children: experience using a mpl-9000 lithotriptor, World J Urol 22:115, 2004.
- Grams ME, Sang Y, Ballew SH, et al. CKD Prognosis Consortium. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Age, Race, and Sex With Acute Kidney Injury. Am J Kidney Dis. 2015;66(4):591-601.
- Shalaby-Rana E, Lowe LH, Blask AN, et al: Imaging in pediatric urology, Pediatr Clin North Am 44(5):1065-1089, 1997.
- Farpour-Lambert NJ, Aggoun Y, Marchand LM, et al. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J Am Coll Cardiol 2009;54(25):2396-2406.
- Tan RT, McGahan JP, Link DP, et al: Bronchial artery embolisation in management of haemoptysis, J Intervent Radiol 6:67, 1991.
- Banday AA, Lokhandwala MF. Dopamine receptors and hypertension. Curr Hypertens Rep. 2008;10(4):268-275.
- Kellum JA, Song M, Li J. Science review: extracellular acidosis and the immune response: clinical and physiologic implications. Crit Care. 2004;8(5):331-336.