
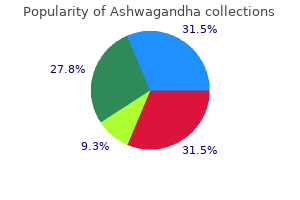
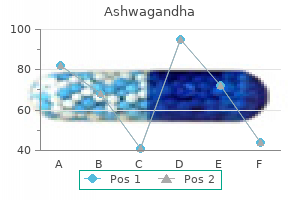
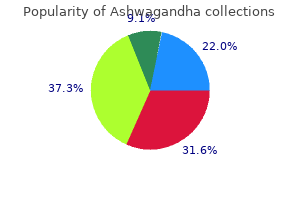
Ashwagandha
| Contato
Página Inicial
Mark K. Wax, MD, FACS, FRCSC
- Professor, Otolaryngology/Head and Neck Surgery
- Professor, Oral and Maxillofacial Surgery
- Program Director
- Director, Microvascular Reconstruction
- Coordinator, Education, AAOHNS(F)
- Department of Otolaryngology/Head and Neck Surgery
- Oregon Health Sciences University
- Portland, Oregon
Phleboviruses are assigned to at least 10 serocomplexes; human pathogens are found in at least four of these serocomplexes anxiety 0 technique discount ashwagandha 60 caps otc. The flaviviruses discussed here belong to two phylogenetically and antigenically distinct groups and are transmitted among vertebrates by mosquitoes and ixodid ticks anxiety symptoms feeling cold ashwagandha 60 caps order on line, respectively 8 tracks anxiety ashwagandha 60 caps buy on-line. Vectors are usually infected when they feed on viremic hosts; as in the case of most other viruses discussed here anxiety symptoms unsteadiness discount 60 caps ashwagandha otc, humans are accidental hosts who usually are infected by arthropod bites anxiety symptoms everyday best order ashwagandha. Arthropods maintain flavivirus infections horizontally, although transovarial transmission has been documented. Under certain circumstances, flaviviruses can also be transmitted by aerosols or via contaminated food products; in particular, raw milk can transmit tick-borne encephalitis virus. Quaranjaviruses are transmitted among birds by ixodid ticks, whereas thogotoviruses have a predilection for mammalian host reservoirs and can be transmitted by both ixodid ticks and mosquitoes. These viruses produce particles that have icosahedral symmetry and are 6080 nm in diameter. In contrast to all other virions discussed here, reovirions are not enveloped and thus are insensitive to detergent inactivation. Human arthropod-borne viruses are found among the genera Coltivirus (subfamily Spinareovirinae), Orbivirus, and Seadornavirus (subfamily Sedoreovirinae). Coltiviruses are transmitted by numerous tick types transstadially but not transovarially. Overall maintenance of the transmission cycle, therefore, involves viremic mammalian hosts infected by tick bites. Arthropod-borne orbiviruses have 10 genome segments and are transmitted by mosquitoes or ixodid ticks, whereas relevant seadornaviruses have 12 genome segments and are transmitted exclusively by mosquitoes. Only the genus Vesiculovirus includes human arthropod-borne viruses, all of which are transmitted by insects (biting midges, mosquitoes, and sandflies). The togaviruses discussed here are all members of the genus Alphavirus and are transmitted among vertebrates by mosquitoes. Unknown Unknown Unknown Unkown Unknown Unknown Unknown Ixodid ticks (Amblyomma, Dermacentor, Haemaphysalis, Hyalomma, Rhipicephalus spp. Abbreviations are placed in parentheses when cases are either extremely rare or controversial. Table 233-2 lists the approximate geographic distribution of most arthropod-borne and rodent-borne infections. Many of these diseases can be acquired in either rural or urban settings; these diseases include yellow fever, dengue (previously called dengue fever), severe dengue (previously called dengue hemorrhagic fever and dengue shock syndrome), chikungunya virus disease, hemorrhagic fever with renal syndrome caused by Seoul virus, sandfly fever caused by sandfly fever Naples and Sicilian viruses, and Oropouche virus disease. Exposure to rodents is sometimes reported by persons infected with arenaviruses or hantaviruses. Laboratory diagnosis is required in all cases, although epidemics occasionally provide enough clinical and epidemiologic clues for a presumptive etiologic diagnosis. For most arthropod-borne and rodent-borne viruses, acute-phase serum samples (collected within 3 or 4 days of onset) have yielded isolates. These tests can provide a diagnosis based on a single serum sample within a few hours and are particularly useful in patients with severe disease. Hantavirus infections differ from other viral infections discussed here in that severe acute disease is immunopathologic; patients present with serum IgM that serves as the basis for a sensitive and specific test. Infection with any dengue virus type (1, 2, 3, or 4) is considered as a cause of fever and myalgia because this syndrome is by far the most common manifestation worldwide. Unfortunately, most of the known arthropod- or rodent-borne viral diseases have not been studied in detail with modern medical approaches; thus available data may be incomplete or biased. The reader must be aware that data on geographic distribution are often fuzzy: the literature frequently is not clear as to whether the data pertain to the distribution of a particular virus or the areas where human disease has been observed. In addition, the designations for viruses and viral diseases have changed multiple times over decades. Two ungrouped bunyaviruses, Gan Gan virus and Trubanaman virus, and the flavivirus Kokobera virus have been associated with single cases of polyarthritic disease. Arthropodborne alphaviruses are also common causes of arthritides-usually acute febrile diseases accompanied by the development of a maculopapular rash. Most alphavirus infections are less severe and have fewer articular manifestations in children than in adults. The most important alphavirus arthritides are Barmah Forest virus infection, chikungunya virus disease, Ross River disease, and Sindbis virus infection. Mayaro, Semliki Forest, and Una viruses have caused isolated cases or limited and infrequent epidemics (30 to several hundred cases per year) in the past. Signs and symptoms of infections with these viruses often are similar to those observed with chikungunya virus disease. Chikungunya Virus Disease Disease caused by chikungunya virus is endemic in rural areas of Africa. In 2004, a massive epidemic began in the Indian Ocean region (in particular on the islands of Réunion and Mauritius) and was most likely spread by travelers; Aedes albopictus was identified as the major vector of chikungunya virus during that epidemic. Between 2013 and 2014, several thousand chikungunya virus infections were reported (and several tens of thousands of cases were suspected) from Caribbean islands. The virus was imported to Italy, France, and the United States by travelers from the Caribbean. Chikungunya virus poses a threat to the continental United States as suitable vector mosquitoes are present in the southern states. The disease is most common among adults, in whom the clinical presentation may be dramatic. The abrupt onset of chikungunya virus disease follows an incubation period of 210 days. Fever (often severe) with a saddleback pattern and severe arthralgia are accompanied by chills and constitutional symptoms and signs, such as abdominal pain, anorexia, conjunctival injection, headache, nausea, and photophobia. Migratory polyarthritis mainly affects the small 1313 joints of the ankles, feet, hands, and wrists, but the larger joints are not necessarily spared. Rash may appear at the outset or several days into the illness; its development often coincides with defervescence, which occurs around day 2 or 3 of the disease. Young children develop less prominent signs and are therefore less frequently hospitalized. Children also often develop a bullous rather than a maculopapular/ petechial rash. Maternalfetal transmission has been reported and in some cases has led to fetal death. Recovery may require weeks, and some elderly patients may continue to experience joint pain, recurrent effusions, or stiffness for several years. Treatment of chikungunya virus disease relies on nonsteroidal anti-inflammatory drugs and sometimes chloroquine for refractory arthritis. Barmah Forest Virus Infection and Ross River Disease Barmah Forest virus and Ross River virus cause diseases that are indistinguishable on clinical grounds alone (hence the previously common disease designation epidemic polyarthritis for both infections). Ross River virus has caused epidemics in Australia, Papua New Guinea, and the South Pacific since the beginning of the twentieth century and continues to be responsible for ~4800 cases of disease in rural and suburban areas annually. In 19791980, the virus swept through the Pacific Islands, causing more than 500,000 infections. Ross River virus is predominantly transmitted by Aedes normanensis, Aedes vigilax, and Culex annulirostris. Barmah Forest virus is transmitted by both Aedes and Culex mosquitoes and has been isolated from biting midges. The vertebrate hosts remain to be determined, but serologic studies implicate horses and possums. Of the human Barmah Forest and Ross River virus infections surveyed, 5575% were asymptomatic; however, these viral diseases can be debilitating. The incubation period is 79 days; the onset of illness is sudden, and disease is usually ushered in by disabling symmetrical joint pain. A nonitchy, diffuse, maculopapular rash (more common in Barmah Forest virus infection) generally develops coincidentally or follows shortly, but in some patients it can precede joint pains by several days. Constitutional symptoms such as low-grade fever, asthenia, headache, myalgia, and nausea are not prominent or are absent in many patients. Most patients are incapacitated for considerable periods (6 months) by joint involvement, which interferes with grasping, sleeping, and walking. Ankle, interphalangeal, knee, metacarpophalangeal, and wrist joints are most often involved, although elbows, shoulders, and toes may also be affected. Periarticular swelling and tenosynovitis are common, and one-third of patients have true arthritis (more common in Ross River disease). Only half of all patients with arthritis can resume normal activities within 4 weeks, and 10% still must limit their activity after 3 months. Occasional patients are symptomatic for 13 years but without progressive arthropathy. In the diagnosis of either infection, clinical laboratory values are normal or variable. Tests for rheumatoid factor and antinuclear antibodies are negative, and the erythrocyte sedimentation rate is acutely elevated. Joint fluid contains 100060,000 mononuclear cells/L, and viral antigen can usually be detected in macrophages. IgM antibodies are valuable in the diagnosis of this infection, although such antibodies occasionally persist for years. Isolation of the virus from blood after mosquito inoculation or growth of the virus in cell culture is possible early in the illness. Because of the great economic impact of annual epidemics in Australia, an inactivated Ross River virus vaccine is under development. Nonsteroidal anti-inflammatory drugs such as naproxen or acetylsalicylic acid are effective for treatment. Infections with northern European or southern African variants are particularly likely in rural environments. After an incubation period of <1 week, Sindbis virus infection begins with rash and arthralgia. Constitutional clinical signs are not marked, and fever is modest or lacking altogether. The rash, which lasts ~1 week, begins on the trunk, spreads to the extremities, and evolves from macules to papules that often vesiculate. The arthritis is multiarticular, migratory, and incapacitating, with resolution of the acute phase in a few days; the ankles, elbows, knees, phalangeal joints, wrists, and-to a much lesser extent-proximal and axial joints are involved. Persistence of joint pain and occasionally of arthritis is a major problem and may continue for months or even years despite lack of deformities. Zika Virus Infection Zika virus is an emerging pathogen that is transmitted among nonhuman primates and humans by Aedes mosquitoes. Human infections are usually benign and are most likely misdiagnosed as dengue or influenza. Zika virus infection is characterized by influenza-like clinical signs, including fever, headaches, and malaise. A maculopapular rash, conjunctivitis, myalgia, and arthralgia usually accompany or follow those manifestations. Zika virus infection was first documented in Africa in 1947 and was later recognized in southeastern and southern Asia. In recent years, the number of Zika virus infections reported from Micronesia and Polynesia has increased steadily. However, individual agents of other families, including Dhori virus and thogotovirus (Orthomyxoviridae) as well as Banna virus (Reoviridae), have been known to cause isolated cases of encephalitis as well. Arboviral encephalitides are seasonal diseases, commonly occurring in the warmer months. Their incidence varies markedly with time and place, depending on ecologic factors. All the viral encephalitides discussed in this section have a similar pathogenesis. During the viremic phase, there may be little or no recognizable disease except in tick-borne flavivirus encephalitides, which may manifest with clearly delineated phases of fever and systemic illness. The usual pathologic features of arboviral encephalitides are focal necroses of neurons, inflammatory glial nodules, and perivascular lymphoid cuffing. The typical patient presents with a prodrome of nonspecific constitutional signs and symptoms, including fever, abdominal pain, sore throat, and respiratory signs. The severity of human infection varies from an absence of signs/symptoms to febrile headache, aseptic meningitis, and full-blown encephalitis. The proportions and severity of these manifestations vary with the infecting virus. Involvement of deeper brain structures in less severe cases may be signaled by lethargy, somnolence, and intellectual deficit (as disclosed by the mental status examination). More severely affected patients are obviously disoriented and may become comatose. Tremors, loss of abdominal reflexes, cranial nerve palsies, hemiparesis, monoparesis, difficulty swallowing, limb-girdle syndrome, and frontal lobe signs are all common. Spinal and motor neuron diseases are documented after West Nile and Japanese encephalitis virus infections. Seizures and focal signs may be evident early or may appear during the course of the disease. The infections may be fatal, or recovery may be slow, with weeks or months required for the return of maximal recoupable function, or incomplete, with persisting long-term deficits. Leptospirosis, neurosyphilis, Lyme disease, catscratch disease, and more recently described viral encephalitides. Early in the process, a significant proportion of these leukocytes may be polymorphonuclear, but mononuclear cells are usually predominant later.
Prompt triage is vital to provide aggressive support with high-dose intravenous catecholamine therapy and sometimes with temporary mechanical circulatory support anxiety 18 year old generic ashwagandha 60 caps without prescription. Recognition of patients with this fulminant presentation is potentially life-saving as more than half can survive anxiety joint pain ashwagandha 60 caps with amex, with marked improvement demonstrable within the first few weeks anxiety symptoms upset stomach 60 caps ashwagandha order with mastercard. The ejection fraction function of these patients often recovers to near-normal anxiety symptoms jittery buy discount ashwagandha 60 caps, although residual diastolic dysfunction may limit vigorous exercise for some survivors anxiety symptoms tingling buy generic ashwagandha 60 caps line. Chronic viral myocarditis is often invoked, but rarely proven, as a diagnosis when no other cause of dilated cardiomyopathy can be identified. However, some cases of otherwise unexplained cardiomyopathy will later be recognized to have a genetic basis, or ultimately found to have resulted from excess alcohol consumption or illicit drugs. The prevalence of previous or persistent viral infection as the cause for chronic dilated cardiomyopathy remains highly controversial. Magnetic resonance imaging is increasingly used for the diagnosis of myocarditis, which is supported by evidence of increased tissue edema and gadolinium enhancement. Endomyocardial biopsy is not often indicated for the initial evaluation of suspected viral myocarditis unless ventricular tachyarrhythmias suggest possible etiologies of sarcoidosis or giant cell myocarditis. The indications and benefit of endomyocardial biopsy for evaluation of myocarditis or new-onset cardiomyopathy remain controversial. It is not known to what degree persistent infection and/or ongoing immune responses contribute to ongoing myocardial injury in the chronic phase. The Dallas Criteria for myocarditis on endomyocardial biopsy include lymphocytic infiltrate with evidence of myocyte necrosis. Negative Dallas Criteria can reflect sampling error or early resolution of lymphocytic infiltrates, but also the insensitivity of the test when inflammation results from cytokines and antibodymediated injury. Routine histologic examination of endomyocardial biopsy rarely reveals a specific infective etiology, such as toxoplasmosis or Cytomegalovirus. An increase in circulating viral titers between acute and convalescent blood samples supports a diagnosis of acute viral myocarditis with potential spontaneous improvement. There is no established role for measuring circulating anti-heart antibodies, which may be the result, rather than a cause, of myocardial injury and have been found also in patients with coronary artery disease and genetic cardiomyopathy. Patients with recent or ongoing viral syndromes can be classified into three levels of diagnosis: 1. Microscopic image of an endomyocardial biopsy showing massive infiltration with mononuclear cells and occasional eosinophils associated with clear myocyte damage. Such extensive involvement of the myocardium would lead to extensive replacement fibrosis even if the inflammatory response could be suppressed. Probable acute myocarditis is diagnosed when the above criteria are met and accompanied also by cardiac symptoms, such as shortness of breath or chest pain, which can result from pericarditis or myocarditis. Definite myocarditis is diagnosed when there is histologic or immunohistologic evidence of inflammation on endomyocardial biopsy (see below) and does not require any other laboratory or clinical criteria. However, their contribution to chronic cardiomyopathy is uncertain, as serologic evidence of exposure is present in many children and most adults. The clinical picture may be complicated by pericardial effusions and pulmonary hypertension. There is a high frequency of lymphocytic myocarditis found at autopsy, and viral particles have been demonstrated in the myocardium in some cases, consistent with direct causation. Hepatitis C has been repeatedly implicated in cardiomyopathy, particularly in Germany and Asia. As this cytokine itself often depresses cardiac function transiently, careful coordination of administration and ongoing clinical evaluation are critical. Involvement of the heart with hepatitis B is uncommon, but can be seen when associated with systemic vasculitis (polyarteritis nodosa). Additional viruses implicated specifically in myocarditis include mumps, respiratory syncytial virus, the arboviruses (dengue fever and yellow fever), and arenaviruses (Lassa fever). However, for any serious infection, the systemic inflammatory response can cause nonspecific depression of cardiac function, which is generally reversible if the patient survives. During acute infection, therapy with antiinflammatory or immunosuppressive medications is avoided, as their use has been shown to increase viral replication and myocardial injury in animal models. Therapy with specific antiviral agents (such as oseltamivir) has not been studied in relation to cardiac involvement. There is ongoing investigation into the impact of antiviral therapy to treat chronic viral persistence identified from endomyocardial biopsy. Large trials of immunosuppressive therapy for Dallas Criteriapositive myocarditis have been negative. There are some initial encouraging results and ongoing investigations with immunosuppressive therapy for immune-mediated myocarditis defined by immunohistologic criteria on biopsy or circulating anti-heart antibodies in the absence of myocardial viral genomes. However, neither antiviral nor antiinflammatory therapies are currently recommended. Until we have a better understanding of the different phases of viral myocarditis and its sequelae and the effects of timed or targeted therapies, treatment will continue to be directed to the clinical cardiovascular stage of the disease, for dilated cardiomyopathy in general. Transmission can also occur through blood transfusion, organ donation, from mother to fetus, and occasionally orally. While programs to eradicate the insect vector have decreased the prevalence from about 16 million to less than 10 million in South America, cases are increasingly recognized in Western developed countries. Approximately 100,000 affected individuals are currently living in the United States, most of whom contracted the disease in endemic areas. The parasite itself can cause myocyte lysis and primary neuronal damage, and specific immune responses may recognize the parasites or related antigens and lead to chronic immune activation in the absence of detectable parasites. Further evidence for persistent infection is the eruption of parasitic skin lesions during immunosuppression after cardiac transplantation. As with viral myocarditis, the relative roles of persistent infection and of secondary autoimmune injury have not been resolved. In the absence of antiparasitic therapy, the silent stage progresses slowly over 1030 years in almost half of patients to manifest in the cardiac and gastrointestinal systems in the chronic stages. These dilated ventricles are particularly thrombogenic, giving rise to pulmonary and systemic emboli. The serologic tests for specific IgG antibodies against the trypanosome lack sufficient specificity and sensitivity, thereby requiring two separate positive tests required to make a diagnosis. Treatment of the advanced stages focuses on clinical manifestations of the disease and includes heart failure medications, pacemakerdefibrillators, and anticoagulation. Increasing attention is directed to antiparasitic therapy even in chronic disease without obvious active infection. The most common effective antiparasitic therapies are benznidazole and nifurtimox, both associated with multiple severe reactions, including dermatitis, gastrointestinal distress, and neuropathy. Survival is less than 30% at 5 years after the onset of overt clinical heart failure. Patients without major extracardiac disease have occasionally undergone transplantation, after which they may require lifelong therapy to suppress reactivation of infection. African trypanosomiasis infection results from the tsetse fly bite and can occur in travelers exposed during trips to Africa. The West African form is caused by Trypanosoma brucei gambiense and progresses silently over years. The diagnosis is made by identification of trypanosomes in blood, lymph nodes, or other affected sites. Antiparasitic therapy has limited efficacy and is determined by the specific type and the stage of infection (hemolymphatic or neurologic). Immunocompromised hosts are most likely to experience reactivation of latent infection from cysts. Toxoplasmosis may present with encephalitis or chorioretinitis and, in the heart, can cause myocarditis, pericardial effusion, constrictive pericarditis, and heart failure. The diagnosis in an immunocompetent patient is made when the IgM is positive and the IgG becomes positive later. Active toxoplasmosis may be suspected in an immunocompromised patient with myocarditis and a positive IgG titer for toxoplasmosis, particularly when avidity testing identifies high specificity of the antibody. Trichinellosis is caused by Trichinella spiralis larva ingested with undercooked meat. Periorbital and facial edema and conjunctival and retinal hemorrhage may also be seen. Although the larva may occasionally invade the myocardium, clinical heart failure is rare and, when observed, attributed to the eosinophilic inflammatory response. The diagnosis is made from the specific serum antibody and is further supported by the presence of eosinophilia. Treatment includes antihelminthic drugs (albendazole, mebendazole) and glucocorticoids if inflammation is severe. Cardiac involvement with Echinococcus is rare, but cysts can form and rupture in the myocardium and pericardium. Bacterial Infections Most bacterial infections can involve the heart occasionally through direct invasion and abscess formation, but do so rarely. More commonly, systemic inflammatory responses depress contractility in severe infection and sepsis. Diphtheria specifically affects the heart in almost one-half of cases, and cardiac involvement is the most common cause of death in patients with this infection. The prevalence of vaccines has shifted the incidence of diphtheria from children worldwide to countries without routine immunization and to older populations who have lost their immunity. The bacillus releases a toxin that impairs protein synthesis and may particularly affect the conduction system. The specific antitoxin should be administered as soon as possible, with higher priority than antibiotic therapy. Other systemic bacterial infections that can involve the heart include brucellosis, chlamydophila, legionella, meningococcus, mycoplasma, psittacosis, and salmonellosis, for which specific treatment is directed at the systemic infection. Gas bubbles can be detected in the myocardium, and occasionally abscesses can form in the myocardium and pericardium. Streptococcal infection with -hemolytic streptococci is most commonly associated with acute rheumatic fever and is characterized by inflammation and fibrosis of cardiac valves and systemic connective tissue, but it can also lead to a myocarditis with focal or diffuse infiltrates of mononuclear cells. Tuberculosis can involve the myocardium directly as well as through tuberculous pericarditis, but rarely does so when the disease is treated with antibiotics. The usual manifestations are in the gastrointestinal tract, but pericarditis, coronary arteritis, valvular lesions, and occasionally clinical heart failure may also occur. Multidrug antituberculous regimens are effective, but the disease tends to relapse even with appropriate treatment. Other Infections Spirochetal myocarditis has been diagnosed from myocardial biopsies containing Borrelia burgdorferi that causes Lyme disease. Lyme carditis most often presents with arthritis and conduction system disease that resolves within 12 weeks of antibiotic treatment, only rarely implicated in chronic heart failure. Fungal myocarditis can occur due to hematogenous or direct spread of infection from other sites, as has been described for aspergillosis, actinomycosis, blastomycosis, candidiasis, coccidioidomycosis, cryptococcosis, histoplasmosis, and mucormycosis. However, cardiac involvement is rarely the dominant clinical feature of these infections. The paradigm of noninfective inflammatory myocarditis is cardiac transplant rejection, from which we have learned that myocardial depression can develop and reverse quickly, that noncellular mediators such as antibodies and cytokines play a major role in addition to lymphocytes, and that myocardial antigens are exposed by prior physical injury and viral infection. The most commonly diagnosed noninfective inflammation is granulomatous myocarditis, including both sarcoidosis and giant cell myocarditis. Although classically presenting with higher prevalence in young African-American men, the epidemiology appears to be changing, with increasing recognition of sarcoidosis in Caucasian patients in nonurban areas. Patients with pulmonary sarcoid are at high risk for cardiac involvement, but cardiac sarcoidosis also occurs without clinical lung disease. Regional clustering of the disease supports the suspicion that the granulomatous reaction is triggered by an infectious or environmental allergen not yet identified. The sites and density of cardiac granulomata, the time course, and the degree of extracardiac involvement are remarkably variable. Patients may present with rapid-onset heart failure and ventricular tachyarrhythmias, conduction block, chest pain syndromes, or minor cardiac findings in the setting of ocular involvement, an infiltrative skin rash, or a nonspecific febrile illness. They may also present less acutely after months to years of fluctuating cardiac symptoms. When ventricular tachycardia or conduction block dominates the initial presentation of heart failure without coronary artery disease, suspicion should be high for these granulomatous myocarditides. There is often right ventricular predominance of both dilation and ventricular arrhythmias, sometimes initially attributed to arrhythmogenic right ventricular dysplasia. Computed tomography of the chest often reveals pulmonary lymphadenopathy even in the absence of clinical lung disease. To rule out chronic infections, such as tuberculosis or histoplasmosis as the cause of adenopathy, the diagnosis usually requires pathologic confirmation. Immunosuppressive treatment for sarcoidosis is initiated with highdose glucocorticoids, which are often more effective for arrhythmias than for the heart failure. Patients with sarcoid lesions that persist or recur during tapering of corticosteroids are considered candidates for other immunosuppressive therapies, frequently with agents also used for cardiac transplantation. Pacemakers and implantable defibrillators are generally indicated to prevent life-threatening heart block or ventricular tachycardia, respectively. Because the inflammation often resolves into extensive fibrosis that impairs cardiac function and provides pathways for reentrant arrhythmias, the prognosis for improvement is best when the granulomata are not extensive and the ejection fraction is not severely reduced. Giant cell myocarditis is less common than sarcoidosis, but accounts for 1020% of biopsy-positive cases of myocarditis. Giant cell myocarditis typically presents with rapidly progressive heart failure and tachyarrhythmias. Diffuse granulomatous lesions are surrounded by extensive inflammatory infiltrate unlikely to be missed on endomyocardial biopsy, often with extensive eosinophilic infiltration. Associated conditions are thymomas, thyroiditis, pernicious anemia, other autoimmune diseases, and occasionally recent infections. Microscopic image of an endomyocardial biopsy showing a noncaseating granuloma and associated interstitial fibrosis typical of sarcoidosis.
Supportive diagnostic virology and fluorescent staining of skin scrapings with monoclonal antibodies are helpful in ensuring the proper diagnosis anxiety symptoms gastro cheap 60 caps ashwagandha mastercard. A rapid impression can be obtained by a Tzanck smear anxiety symptoms muscle tension cheap ashwagandha express, with scraping of the base of the lesions in an attempt to demonstrate multinucleated giant cells; however anxiety symptoms 4dp5dt buy discount ashwagandha 60 caps, the sensitivity of this method is low (~60%) anxiety symptoms twitching ashwagandha 60 caps line. Direct immunofluorescent staining of cells from the lesion base or detection of viral antigens by other assays (such as the immunoperoxidase assay) is also useful anxiety attacks symptoms order ashwagandha online pills, although these tests are not commercially available. Medical management of chickenpox in the immunologically normal host is directed toward the prevention of avoidable complications. Acyclovir (800 mg by mouth five times daily), valacyclovir (1 g three times daily), or famciclovir (250 mg three times daily) for 57 days is recommended for adolescents and adults with chickenpox of 1186 24 h duration. Patients with herpes zoster benefit from oral antiviral therapy, as evidenced by accelerated healing of lesions and resolution of zoster-associated pain with acyclovir, valacyclovir, or famciclovir. However, valacyclovir and famciclovir are superior in terms of pharmacokinetics and pharmacodynamics and should be used preferentially. Famciclovir, the prodrug of penciclovir, is at least as effective as acyclovir and perhaps more so; the dose is 500 mg by mouth three times daily for 7 days. For low-risk immunocompromised hosts, oral therapy with valacyclovir or famciclovir appears beneficial. Persons with zoster ophthalmicus should be referred immediately to an ophthalmologist. Therapy for this condition consists of the administration of analgesics for severe pain and the use of atropine. The management of acute neuritis and/or postherpetic neuralgia can be particularly difficult. In addition to the judicious use of analgesics ranging from nonnarcotics to narcotic derivatives, drugs such as gabapentin, pregabalin, amitriptyline hydrochloride, lidocaine (patches), and fluphenazine hydrochloride are reportedly beneficial for pain relief. In one study, glucocorticoid therapy administered early in the course of localized herpes zoster significantly accelerated such quality-of-life improvements as a return to usual activity and termination of analgesic medications. Two doses are recommended for all children: the first at 1215 months of age and the second at ~46 years of age. Furthermore, inactivation of the vaccine virus significantly decreases the occurrence of herpes zoster after hematopoietic stem-cell transplantation. Hospital Varicella: same 2- to 4-bed room or adjacent beds in large ward, faceto-face contact with infectious staff member or patient, visit by a person deemed contagious Zoster: intimate contact. Immunocompromised susceptible children without a history of varicella or varicella immunization 2. Newborn infants whose mother had onset of chickenpox within 5 days before or within 48 h after delivery 4. Hospitalized premature infant (28 weeks of gestation) whose mother lacks a reliable history of chickenpox or serologic evidence of protection against varicella 5. This product should be given within 96 h (preferably within 72 h) of the exposure. Lastly, antiviral therapy can be given as prophylaxis to individuals at high risk who are ineligible for vaccine or who are beyond the 96-h window after direct contact. While the initial studies have used acyclovir, similar benefit can be anticipated with either valacyclovir or famciclovir. By adulthood, more than 90% of individuals have been infected and have antibodies to the virus. In lower socioeconomic groups and in areas of the world with deficient standards of hygiene. While B cells may become infected after contact with epithelial cells, studies suggest that lymphocytes in the tonsillar crypts can be infected directly. A prodrome of fatigue, malaise, and myalgia may last for 12 weeks before the onset of fever, sore throat, and lymphadenopathy. Fever is usually low-grade and is most common in the first 2 weeks of the illness; however, it may persist for >1 month. Lymphadenopathy and pharyngitis are most prominent during the first 2 weeks of the illness, while splenomegaly is more prominent during the second and third weeks. Lymphadenopathy most often affects the posterior cervical nodes but may be generalized. Pharyngitis, often the most prominent sign, can be accompanied by enlargement of the tonsils with an exudate resembling that of streptococcal pharyngitis. A morbilliform or papular rash, usually on the arms or trunk, develops in ~5% of cases. Many patients treated with ampicillin develop a macular rash; this rash is not predictive of future adverse reactions to penicillins. Most patients have symptoms for 24 weeks, but nearly 10% have fatigue that persists for 6 months. Laboratory Findings the white blood cell count is usually elevated and peaks at 10,00020,000/L during the second or third week of illness. The latter cells are enlarged lymphocytes that have abundant cytoplasm, vacuoles, and indentations of the cell membrane. Serum levels of aminotransferases and alkaline phosphatase are usually mildly elevated. Meningitis and encephalitis are the most common neurologic abnormalities, and patients may present with headache, meningismus, or cerebellar ataxia. The cerebrospinal fluid contains mainly lymphocytes, with occasional atypical lymphocytes. In most cases, the anemia is Coombs-positive, with cold agglutinins directed against the red blood cell antigen. Splenic rupture is more common among male than female patients and may manifest as abdominal pain, referred shoulder pain, or hemodynamic compromise. Others develop hypogammaglobulinemia, malignant B cell lymphomas, aplastic anemia, or agranulocytosis. In the test for this antibody, human serum is absorbed with guinea pig kidney, and the heterophile titer is defined as the greatest serum dilution that agglutinates sheep, horse, or cow erythrocytes. Tests usually remain positive for 3 months after the onset of illness, but heterophile antibodies can persist for up to 1 year. False-positive monospot results are more common among persons with connective tissue disease, lymphoma, viral hepatitis, and malaria. Excessive physical activity during the first month should be avoided to reduce the possibility of splenic rupture, which often necessitates splenectomy. Infusions of donor lymphocytes are often effective for stem cell transplant recipients, although graftversus-host disease can occur. All are associated with the production of characteristic enlarged cells-hence the name cytomegalovirus. Viral replication is associated with the production of large intranuclear inclusions and smaller cytoplasmic inclusions. Data generated in specific regions should be considered in the context of local seropositivity rates, when appropriate. However, clinical disease in the fetus or newborn is related almost exclusively to primary maternal infection (Table 219-1). The sites of persistent infection probably include multiple cell types and various organs. Transmission via blood transfusion or organ transplantation is due primarily to latent infections in these tissues. Cytomegalic cells are found in a wide variety of organs, including the salivary gland, lung, liver, kidney, intestine, pancreas, adrenal gland, and central nervous system. The cellular inflammatory response to infection consists of plasma 1191 cells, lymphocytes, and monocyte-macrophages. Cytomegalic inclusion disease develops in 5% of infected fetuses and is seen almost exclusively in infants born to mothers who develop primary infections during pregnancy. Microcephaly with or without cerebral calcifications, intrauterine growth retardation, and prematurity are reported in 3050% of cases. Laboratory abnormalities include elevated alanine aminotransferase levels in serum, thrombocytopenia, conjugated hyperbilirubinemia, hemolysis, and elevated protein levels in cerebrospinal fluid. Of asymptomatically infected infants, 525% develop significant psychomotor, hearing, ocular, or dental abnormalities over the next several years. Of infants who are breast-fed for >1 month by seropositive mothers, 4060% become infected. Prolonged high fevers, sometimes with chills, profound fatigue, and malaise, characterize this disorder. Occasional patients develop rubelliform rashes, often after exposure to ampicillin or certain other antibiotics. Less common are interstitial or segmental pneumonia, myocarditis, pleuritis, arthritis, and encephalitis. Heterophile antibodies are absent; however, transient immunologic abnormalities are common and may include the presence of cryoglobulins, rheumatoid factors, cold agglutinins, and antinuclear antibodies. Hemolytic anemia, thrombocytopenia, and granulocytopenia complicate recovery in rare instances. Without prophylaxis, the period of maximal risk is between 1 and 4 months after transplantation. Disease likelihood and viral replication levels generally are greater after primary infection than after reactivation. The risk is greatest 513 weeks after transplantation, and identified risk factors include certain types of immunosuppressive therapy, an allogeneic (rather than an autologous) graft, acute graft-versus-host disease, older age, and pretransplantation recipient seropositivity. The development of tachypnea, hypoxemia, and unproductive cough signals respiratory involvement. Radiologic examination of the lung often shows bilateral interstitial or reticulonodular infiltrates that begin in the periphery of the lower lobes and spread centrally and superiorly; localized segmental, nodular, or alveolar patterns are less common. Early lesions consist of small, opaque, white areas of granular retinal necrosis that spread in a centrifugal manner and are later accompanied by hemorrhages, vessel sheathing, and retinal edema. Progressive pulmonary infiltrates, pancytopenia, hyperamylasemia, and hypotension are characteristic features that are frequently found in conjunction with a terminal bacterial, fungal, or protozoan superinfection. Such assays may yield a positive result several days earlier than culture methods. Virus excretion or viremia is readily detected by culture of appropriate specimens on human fibroblast monolayers. With universal prophylaxis, antiviral drugs are used for a defined period, often 3 or 6 months. Because of the bone marrowsuppressive effects of universal prophylaxis, preemptive therapy is more commonly employed in hematopoietic stem cell transplant recipients. Studies in hematopoietic stem cell transplant recipients have produced conflicting results. Prophylactic or suppressive ganciclovir may be useful in high-risk hematopoietic stem cell or organ transplant recipients. Furthermore, the adverse-event profiles and rates of resistance for the two drugs are similar. Peripheral-blood neutropenia develops in roughly one-quarter of treated patients but may be ameliorated by granulocyte colonystimulating factor or granulocyte-macrophage colony-stimulating factor. Whether to use maintenance therapy should depend on the overall level of immunocompromise and the risk of recurrent disease. Although this intraocular device provides good local protection, contralateral eye disease and disseminated disease are not affected, and early retinal detachment is possible. A combination of intraocular and systemic therapy may be better than the intraocular implant alone. Because this agent does not require phosphorylation to be active, it is also effective against most ganciclovir-resistant isolates. With aggressive hydration and dose adjustments for renal dysfunction, the toxicity of foscarnet can be reduced. Most postnatally infected children develop symptoms (fever, fussiness, and diarrhea). In low-prevalence areas, infections typically occur in adults, probably with sexual transmission. Among individuals with intact immunity, chronic asymptomatic infection is the rule, and neoplastic disorders generally develop only after subsequent immunocompromise. The poxviruses responsible for infections in humans, the geographic locations in which these infections are found, the host reservoirs, and the main manifestations are listed in Table 220e-1. These lesions measure 25 mm in diameter and are pearly, flesh-colored, and umbilicated, with a characteristic dimple at the center. Lesions may be found-singly or in clusters-anywhere on the body except on the palms and soles and may be associated with an eczematous rash. Molluscum contagiosum is highly prevalent among children and is the most common human disease resulting from poxvirus infection. Genital lesions are more common in adults, to whom the virus may be transmitted by sexual contact. The incubation period ranges from 2 weeks to 6 months, with an average of 27 weeks. The diagnosis of molluscum contagiosum is typically based on its clinical presentation and can be confirmed by histologic demonstration of the cytoplasmic eosinophilic inclusions (molluscum bodies) that are characteristic of poxvirus replication. Cidofovir displays in vitro activity against many poxviruses, and case reports suggest that parenteral or topical cidofovir may have some efficacy in the treatment of recalcitrant molluscum contagiosum in immunosuppressed hosts. Human infections with monkeypox virus typically occur in Africa when humans come into direct contact with infected animals. Human disease is characterized by a systemic illness and vesicular rash similar to those of variola. Compared with the lesions of this herpesvirus infection, monkeypox lesions tend to be more uniform. The first outbreak of human monkeypox infection in the Western Hemisphere occurred during 2003, when more than 70 cases were reported in the midwestern United States. The outbreak was linked to contact with pet prairie dogs that had become infected while being housed with rodents imported from Ghana.
It therefore must regulate the entry of molecules and cells into tissues in a selective manner anxiety journal order 60 caps ashwagandha free shipping. The ability of endothelial cells to serve as a selectively permeable barrier fails in many vascular disorders anxiety symptoms for dogs generic ashwagandha 60 caps on line, including atherosclerosis anxiety symptoms skin ashwagandha 60 caps order with amex, hypertension anxiety symptoms vs adhd symptoms generic ashwagandha 60 caps mastercard, and renal disease anxiety symptoms vs heart attack symptoms buy cheap ashwagandha. This dysregulation of permeability also occurs in pulmonary edema and other situations of "capillary leak. Hence, an understanding of the fundamentals of vascular biology furnishes a foundation for understanding the normal function of all organ systems and many diseases. The smallest blood vessels-capillaries-consist of a monolayer of endothelial cells apposed to a basement membrane, adjacent to occasional smooth-muscle-like cells known as pericytes. Unlike larger vessels, pericytes do not invest the entire microvessel to form a continuous sheath. The intima consists of a monolayer of endothelial cells continuous with those of the capillaries. The middle layer, or tunica media, consists of layers of smooth-muscle cells; in veins, the media can contain just a few layers of smooth-muscle cells. The outer layer, the adventitia, consists of looser extracellular matrix with occasional fibroblasts, mast cells, and nerve terminals. Larger arteries have their own vasculature, the vasa vasorum, which nourishes the outer aspects of the tunica media. The tone of muscular arterioles regulates blood pressure and flow through various arterial beds. These smaller arteries have a relatively thick tunica media in relation to the adventitia. The larger elastic arteries have a much more structured tunica media consisting of concentric bands of smooth-muscle cells, interspersed with strata of elastin-rich extracellular matrix A. Larger muscular arteries have a prominent media with smooth-muscle cells embedded in a complex extracellular matrix. Larger elastic arteries have cylindrical layers of elastic tissue alternating with concentric rings of smooth-muscle cells. Measurement of flow-mediated dilatation can assess endothelial vasodilator function in humans. By contrast, endothelial cells also produce potent vasoconstrictor substances such as endothelin in a regulated fashion. Excessive production of reactive oxygen species, such as superoxide anion (O2-), by endothelial or smoothmuscle cells under pathologic conditions. The normal endothelium resists prolonged contact with blood leukocytes; however, when activated by bacterial products such as endotoxin or by proinflammatory cytokines released during infection or injury, endothelial cells express an array of leukocyte adhesion molecules that bind various classes of leukocytes. The endothelial cells appear to recruit selectively different classes of leukocytes in different pathologic conditions. The gamut of adhesion molecules and chemokines generated during acute bacterial infection tends to recruit granulocytes. In chronic inflammatory diseases such as tuberculosis and atherosclerosis, endothelial cells express adhesion molecules that favor the recruitment of mononuclear leukocytes that characteristically accumulate in these conditions. The surface of endothelial cells contains heparan sulfate glycosaminoglycans that furnish an endogenous antithrombotic coating to the vasculature. They express receptors for plasminogen and plasminogen activators and produce tissue-type plasminogen activator. Thus, in pathologic circumstances, the endothelial cell may promote local thrombus accumulation rather than combat it. Inflammatory stimuli also induce the expression of the potent procoagulant tissue factor, a contributor to disseminated intravascular coagulation in sepsis. Lysis of endothelial cells mediated by complement provides an example of immunologically mediated tissue injury. The presentation of foreign histocompatibility complex antigens by endothelial cells in solid-organ allografts can promote allograft arteriopathy. In addition, immune-mediated endothelial injury may contribute in some patients with thrombotic thrombocytopenic purpura and patients with hemolytic-uremic syndrome. Thus, in addition to the involvement of innate immune responses, endothelial cells participate actively in both humoral and cellular limbs of the immune response. Upon deflation of the cuff, an ultrasound probe monitors changes in diameter (A) and blood flow (B) of the brachial artery (C). Heparan sulfate glycosaminoglycans elaborated by endothelial cells can inhibit smooth-muscle proliferation. In contrast, when exposed to various injurious stimuli, endothelial cells can elaborate growth factors and chemoattractants, such as platelet-derived growth factor, that can promote the migration and proliferation of vascular smoothmuscle cells. Dysregulated elaboration of these growth-stimulatory molecules may promote smooth-muscle accumulation in atherosclerotic lesions. Vascular Smooth-Muscle Cell the vascular smooth-muscle cell, the major cell type of the media layer of blood vessels, also contributes actively to vascular pathobiology. Contraction and relaxation of smooth-muscle cells at the level of the muscular arteries controls blood pressure and, hence, regional blood flow and the afterload experienced by the left ventricle (see below). The vasomotor tone of veins, which is governed by smooth-muscle cell tone, regulates the capacitance of the venous tree and influences the preload experienced by both ventricles. Smooth-muscle cells in the adult vessel seldom replicate in the absence of arterial injury or inflammatory activation. Proliferation and migration of arterial smooth-muscle cells, associated with functional modulation characterized by lower content of contractile proteins and greater production of extracellular matrix macromolecules, can contribute to the development of arterial stenoses in atherosclerosis, arteriolar remodeling that can sustain and propagate hypertension, and the hyperplastic response of arteries injured by percutaneous intervention. In the pulmonary circulation, smooth-muscle migration and proliferation contribute decisively to the pulmonary vascular disease that gradually occurs in response to sustained high-flow states such as left-to-right shunts. Excessive production of collagen and glycosaminoglycans contributes to the remodeling and altered functions and biomechanics of arteries affected by hypertension or atherosclerosis. In larger elastic arteries, the elastin synthesized by smooth-muscle cells serves to maintain not only normal arterial structure, but also hemodynamic function. The ability of the larger arteries, such as the aorta, to store the kinetic energy of systole promotes tissue perfusion during diastole. Arterial stiffness associated with aging or disease, as manifested by a widening pulse pressure, increases left ventricular afterload and portends a poor outcome. Like endothelial cells, vascular smooth-muscle cells do not merely respond to vasomotor or inflammatory stimuli elaborated by other cell types but can themselves serve as a source of such stimuli. For example, when exposed to bacterial endotoxin or other proinflammatory stimuli, smooth-muscle cells can elaborate cytokines and other inflammatory mediators. Smoothmuscle cells also elaborate autocrine growth factors that can amplify hyperplastic responses to arterial injury. Vascular Smooth-Muscle Cell Function Vascular smooth-muscle cells govern vessel tone. Those cells contract when stimulated by a rise in intracellular calcium concentration by calcium influx through the plasma membrane and by calcium release from intracellular stores. Calcium sparks directly augment intracellular calcium concentration and indirectly increase intracellular calcium concentration by activating chloride channels. In addition, calcium sparks reduce smooth-muscle contractility by activating largeconductance calcium-sensitive K+ channels, hyperpolarizing the cell membrane and thereby limiting further voltage-dependent increases in intracellular calcium. These membrane lipid derivatives in turn activate protein kinase C and increase intracellular calcium concentration. Vascular smooth-muscle cell contraction depends principally on the phosphorylation of myosin light chain, which in the steady state, reflects the balance between the actions of myosin light chain kinase and myosin light chain phosphatase. Calcium activates myosin light chain kinase through the formation of a calciumcalmodulin complex. Phosphorylation of the myosin-binding subunit (thr695) of myosin light chain phosphatase by Rho kinase inhibits phosphatase activity and induces calcium sensitization of the contractile apparatus. These agents in turn activate protein kinase A and protein kinase G, respectively, which inactivate myosin light chain kinase and decrease vascular smooth-muscle cell tone. In addition, protein kinase G can interact directly with the myosinbinding substrate subunit of myosin light chain phosphatase, increasing phosphatase activity and decreasing vascular tone. Control of Vascular Smooth-Muscle Cell Tone the autonomic nervous system and endothelial cells modulate vascular smooth-muscle cells in a tightly regulated manner. Autonomic neurons enter the blood vessel medial layer from the adventitia and modulate vascular smoothmuscle cell tone in response to baroreceptors and chemoreceptors within the aortic arch and carotid bodies and in response to thermoreceptors in the skin. These regulatory components include rapidly acting reflex arcs modulated by central inputs that respond to sensory inputs (olfactory, visual, auditory, and tactile) as well as emotional stimuli. Norepinephrine activates receptors, and epinephrine activates and receptors (adrenergic receptors); in most blood vessels, norepinephrine activates postjunctional 1 receptors in large arteries and 2 receptors in small arteries and arterioles, leading to vasoconstriction. Acetylcholine released from parasympathetic neurons binds to muscarinic receptors (of which there are five subtypes, M15) on vascular smooth-muscle cells to yield vasorelaxation. The release of these endothelial effectors of vascular smooth-muscle cell tone is stimulated by mechanical (shear stress, cyclic strain, etc. Guidance molecules, including members of the semaphorin family of secreted peptides, direct blood vessel patterning by attracting or repelling nascent endothelial tubes. The development of collateral vascular networks in the ischemic myocardium, an example of angiogenesis, can result from selective activation of endothelial progenitor cells, which may reside in the blood vessel wall or home to the ischemic tissue from the bone marrow. True arteriogenesis, or the development of a new blood vessel that includes all three cell layers, normally does not occur in the cardiovascular system of adult mammals. The molecular mechanisms and progenitor cells that can recapitulate blood vessel development de novo are under rapidly advancing study (Chaps. Many investigators have focused on receptors and enzymes associated with neurohumoral modulation of vascular function as well as hepatic enzymes that metabolize drugs that affect vascular tone. The genetic polymorphisms thus far associated with differences in vascular response often (but not invariably) relate to functional differences in the activity or expression of the receptor or enzyme of interest. Within the confines of the sarocytes, normally 60140 m in length and 1725 m in diameter. Each cell contains multiple, rodlike cross-banded strands fibers their striated appearance under the light microscope. At the (myofibrils) that run the length of the cell and are composed of seri- center of the sarcomere is a dark band of constant length (1. The cytoplasm between A band, which is flanked by two lighter bands, the I bands, which are the myofibrils contains other cell constituents, including the single of variable length. The sarcomere of heart muscle, like that of skeletal muscle, consists of two sets of interdigitating myofilaments. Thicker filaments, composed principally of the protein myosin, traverse the A band; they are about 10 nm (100 Å) in diameter, with tapered ends. Thinner filaments, composed primarily of actin, course from the Z lines through the I band into the A band; they are approximately 5 nm (50 Myofiber Å) in diameter and 1. Thus, thick and thin filaments overlap only within the (dark) A A Myocyte 10 m band, whereas the (light) I band contains only thin filaments. On electron-microscopic examination, Ca2+ bridges may be seen to extend between the thick enters and thin filaments within the A band; these are Na+ Ca2+ myosin heads (see below) bound to actin filaments. B illustrates the critical role played by the changing [Ca2+] in the myocardial cytosol. Ca2+ ions are schematically shown as entering through the calcium channel that opens in response to the wave of depolarization that travels along the sarcolemma. The varying actin-myosin overlap is shown for (B) systole, when [Ca2+] is maximal, and (C) diastole, when [Ca2+] is minimal. In the process, the A band remains constant in length, whereas the I band shortens and the Z lines move toward one another. In forming the thick myofilament, which is composed of ~300 longitudinally stacked myosin molecules, the rodlike segments of the myosin molecules are laid down in an orderly, polarized manner, leaving the globular portions projecting outward so that they can interact with actin to generate force and shortening. A group of regulatory proteins-troponins C, I, and T-are spaced at regular intervals on this filament. Therefore, even though the crossbridges are energized, they cannot interact with actin. This cycle continues until calcium is dissociated from troponin C in the thin filament, which causes the contractile proteins to return to the resting state with the cross-bridge in the energized state. Mutations in components of the dystrophin complex lead to muscular dystrophy and associated cardiomyopathy. During activation of the cardiac myocyte, Ca2+ becomes attached to one of three components of the heterotrimer troponin C, which results in a conformational change in the regulatory protein tropomyosin; the latter, in turn, exposes the actin cross-bridge interaction sites. Repetitive interaction between myosin heads and actin filaments is termed cross-bridge cycling, which results in sliding of the actin along the myosin filaments, ultimately causing muscle shortening and/or the development of tension. Intracytoplasmic Ca2+ is a principal determinant of the inotropic state of the heart. Most agents that stimulate myocardial contractility (positive inotropic stimuli), including the digitalis glycosides and -adrenergic agonists, increase the [Ca2+] in the vicinity of the myofilaments, which in turn triggers cross-bridge cycling. Its longitudinally disposed tubules closely invest the surfaces of individual sarcomeres but have no direct continuity with the outside of the cell. Thus, intracellular [K+] is relatively high and [Na+] is far lower; conversely, extracellular [Na+] is high and [K+] is low. The absolute quantity of Ca2+ that crosses the sarcolemma and the T system is relatively small and by itself appears to be insufficient to bring about full activation of the contractile apparatus. The major determinants of preload, afterload, and contractility are shown in Table 265e-2. This length provides the optimum configuration for the interaction between the two sets of myofilaments. According to this concept, termed length-dependent activation, myofilament sensitivity to Ca2+ is also maximal at the optimal sarcomere length. The latter acts via protein kinase A to stimulate metabolism (left) and phosphorylate the Ca2+ channel protein (right). In isolated heart and heart-lung preparations, the stroke volume varies directly with the end-diastolic fiber length (preload) and inversely with the arterial resistance (afterload), and as the heart fails-i.
One of the simplest ways to estimate exposure clinically is to measure the time of prodromal appearance anxiety from weed order ashwagandha 60 caps with visa. The earlier the prodromal signs and symptoms appear anxiety disorders ashwagandha 60 caps purchase free shipping, the higher is the dose of radiation exposure anxiety symptoms flushing order 60 caps ashwagandha free shipping. A few laboratory tests need to be done routinely anxiety symptoms 35 buy ashwagandha us, such as complete blood count and urinalysis anxiety symptoms hypertension generic ashwagandha 60 caps buy line. If internal contamination is suspected, specific treatment should be given as outlined below. Treatment for internal radionuclide contamination, also referred to as decorporation, should be started as soon as possible after suspected or known exposure. The approximate upper limit of radionuclide contamination that can reasonably be ignored from a radiation safety point of view is not well defined. These are judgments that will depend on the circumstances of the event and the resources available. The gastrointestinal tract may be cleared by stomach lavage, with emetics (such as apomorphine, 510 mg; or ipecac, 1- to 2-g capsules or 15 mL in syrup), or by use of purgatives, laxatives, ion exchangers, and aluminum antacids. Prussian blue (1 g tid for a minimum of 3 weeks) is an ion exchanger used to treat cesium-137 internal contamination. Aluminum antacids (such as aluminum phosphate gel) may reduce strontium uptake in the gut if given immediately after exposure. Radionuclide interaction with tissues can be prevented or reversed through use of agents that block absorption; dilute, mobilize, or release radionucleotides from tissues; or chelate radionucleotides. Adults between the ages of 18 and 40 should receive 130 mg/d for 714 days if exposed to 10 cGy of radioactive iodine. Other thyroidblocking agents include propylthiouracil (100 mg tid for 8 days) and methimazole (10 mg tid for 2 days followed by 5 mg tid for 6 days). Diluting agents decrease the absorption of the radionuclide; for example, water may be used as a diluting agent in the treatment for tritium (3H) contamination. Mobilizing agents are most effective when given immediately; however, they may be effective for up to 2 weeks after exposure. These agents include antithyroid drugs, parathyroid extract, glucocorticoids, ammonium chloride, diuretics, expectorants, and inhalants. Chelating agents can bind many radioactive materials, after which the complexes are excreted from the body. The duration of chelation treatment depends on the amount of internal contamination and the individual response to treatment. Lung lavage can reduce radiation-induced pneumonitis and is indicated only when a large amount of radionuclide enters the lungs and has the potential to cause acute radiation injury. Immediately after a terrorist event, when victims are being triaged, information regarding source, dose, and exposure time is unlikely to be available. Victims who arrive at the hospital reporting severe weakness, nausea, vomiting, diarrhea, or seizures probably will not survive despite supportive measures. A very limited number of tests can be performed to estimate radiation exposure and contamination. The patient should be observed for clinical symptoms, and the severity and time of onset of nausea, vomiting, headache, anorexia, fever, hypotension, tachycardia, weakness, cognitive changes, skin desquamation, diarrhea, and bloody stools should be recorded. Baseline tests should include a complete blood count with differential and platelet count, renal evaluation, and determination of electrolytes, serum amylase, and serum C-reactive protein. Urine and stool samples should be obtained if internal contamination is suspected. Nasal swabs taken from each nostril within the first 12 h after the exposure may be useful for determination of radionuclide inhalation. After exhalation, each swab is labeled, sealed in a plastic bag, and sent for analysis to appropriate laboratories. Lymphocytes show the most rapid decline, whereas counts of other leukocytes and platelets decline less rapidly. Absolute lymphocyte counts should be repeated every 46 h for 56 days; they are the most valuable early indicator because they constitute a sensitive marker for radiation damage and correlate with both the exposure and the prognosis. A 50% drop in absolute lymphocyte count within the first 24 h indicates a significant injury. Radiation-induced chromosomal aberrations visible in peripheralblood lymphocytes include dicentric chromosomes and ring forms that last for a few weeks. Calibration of a dose-response curve makes it possible to assess the radiation dose on the basis of the presence of these aberrations. Dicentric quantification requires multiple days to perform and is available only in select centers. Another method for estimating exposure is the in vitro cytokinesis block micronucleus assay. Micronuclei can be the result of small acentric chromosome fragments that arise during exposure to radiation. The technique to score the micronuclei in peripheral-blood lymphocytes has been standardized in the last few years. It can be a useful tool in small-scale exposures but is not feasible in a mass casualty setting. In general, only persons who are exposed to <810 Gy of whole-body irradiation have a chance to survive in the long term, and they are at risk of developing cataracts, sterility, and cancers as well as lung, kidney, and bone marrow problems. In light of their age, their gender, and the amount and type of exposure, they should be followed for many years. A major public health issue is the risk of secondary malignancy in individuals and populations that have been exposed to low doses of radiation. Leukemia and breast, brain, thyroid, and lung cancer develop most commonly, but the exposed population is at increased risk for many other cancers as well. Appropriate follow-up protocols should be based on the type of exposure and the exposed population. In cases of internal contamination, long-term follow-up should be focused on the organ at risk. Substantial psychosocial support will likely be needed for a community in the years after an attack including radiologic agents. Obstruction to blood flow, as occurs in valvular stenosis, can cause symptoms resembling those of myocardial failure (Chap. Cardiac arrhythmias often develop suddenly, and the resulting symptoms and signs-palpitations (Chap. Although dyspnea, chest discomfort, edema, and syncope are cardinal manifestations of cardiac disease, they occur in other conditions as well. Thus, dyspnea is observed in disorders as diverse as pulmonary disease, marked obesity, and anxiety (Chap. Edema, an important finding in untreated or inadequately treated heart failure, also may occur with primary renal disease and in hepatic cirrhosis (Chap. Syncope occurs not only with serious cardiac arrhythmias but in a number of neurologic conditions as well (Chap. Whether heart disease is responsible for these symptoms frequently can be determined by carrying out a careful clinical examination (Chap. Myocardial or coronary function that may be adequate at rest may be insufficient during exertion. Thus, dyspnea and/or chest discomfort that appear during activity are characteristic of patients with heart disease, whereas the opposite pattern, i. It is important, therefore, to question the patient carefully about the relation of symptoms to exertion. Age-adjusted death rates for coronary heart disease have declined by two-thirds in the last four decades in the United States, reflecting the identification and reduction of risk factors as well as improved treatments and interventions for the management of coronary artery disease, arrhythmias, and heart failure. Nonetheless, cardiovascular diseases remain the most common causes of death, responsible for 35% of all deaths, almost 1 million deaths each year. In addition, cardiovascular diseases are highly prevalent, diagnosed in 80 million adults, or ~35% of the adult population. For many years cardiovascular disease was considered to be more common in men than in women. In fact, the percentage of all deaths secondary to cardiovascular disease is higher among women (43%) than among men (37%) (Chap. In addition, although the absolute number of deaths secondary to cardiovascular disease has declined over the past decades in men, this number has actually risen in women. Inflammation, obesity, type 2 diabetes mellitus, and the metabolic syndrome appear to play more prominent roles in the development of coronary atherosclerosis in women than in men. Exercise electrocardiography has a lower diagnostic accuracy in the prediction of epicardial obstruction in women than in men. However, the alert physician may recognize the patient at risk for these complications long before they occur and often can take measures to prevent their occurrence. For example, a patient with acute myocardial infarction will often have had risk factors for atherosclerosis for many years. Had these risk factors been recognized, their elimination or reduction might have delayed or even prevented the infarction. Similarly, a patient with hypertrophic cardiomyopathy may have had a heart murmur for years and a family history of this disorder. These findings could have led to an echocardiographic examination, recognition of the condition, and appropriate therapy long before the occurrence of a serious acute manifestation. Patients with valvular heart disease or idiopathic dilated cardiomyopathy, by contrast, may have a prolonged course of gradually increasing dyspnea and other manifestations of chronic heart failure that is punctuated by episodes of acute deterioration only late in the course of the disease. Familial clustering of cardiovascular diseases not only may occur on a genetic basis but also may be related to familial dietary or behavior patterns, such as excessive ingestion of salt or calories and cigarette smoking. The breathlessness that occurs after running up two long flights of stairs denotes far less functional impairment than do similar symptoms that occur after taking a few steps on level ground. Also, the degree of customary physical activity at work and during recreation should be considered. The development of two-flight dyspnea in a well-conditioned marathon runner may be far more significant than the development of one-flight dyspnea in a previously sedentary person. For example, the persistence or development of edema, breathlessness, and other manifestations of heart failure in a patient who is receiving optimal doses of diuretics and other therapies for heart failure (Chap. Similarly, the presence of angina pectoris despite treatment with optimal doses of multiple antianginal drugs (Chap. In an effort to determine the progression of symptoms, and thus the severity of the underlying illness, it may be useful to ascertain what, if any, specific tasks the patient could have carried out 6 months or 1 year earlier that he or she cannot carry out at present. In general, electrocardiographic changes should be interpreted in the context of other abnormal cardiovascular findings. When such a murmur occurs in an asymptomatic child or young adult without other evidence of heart disease on clinical examination, it is usually benign and echocardiography generally is not required. Failure by the noncardiologist to recognize important cardiac manifestations of systemic illnesses. One example may serve to illustrate the importance of establishing a complete diagnosis. In a patient who presents with exertional chest discomfort, the identification of myocardial ischemia as the etiology is of great clinical importance. The establishment of a correct and complete cardiac diagnosis usually commences with the history and physical examination (Chap. Indeed, the clinical examination remains the basis for the diagnosis of a wide variety of disorders. Mendelian transmission of single-gene defects may occur, as in hypertrophic cardiomyopathy (Chap. Although familial transmission may be less obvious than in the monogenic disorders, it is helpful in assessing risk and prognosis in polygenic disorders, as well. Several examples may be used to demonstrate some of the 1441 principles of cardiovascular therapeutics: 1. In the absence of evidence of heart disease, the patient should be clearly informed of this assessment and not be asked to return at intervals for repeated examinations. If there is no evidence of cardiovascular disease but the patient has one or more risk factors for the development of ischemic heart disease (chap. Early signs of deterioration of ventricular function may signify the need for surgical treatment before the development of disabling symptoms, irreversible myocardial damage, and excessive risk of surgical treatment (chap. Mechanical revascularization may be employed too frequently in the United States and too infrequently in Eastern Europe and developing nations. The mere presence of angina pectoris and/or the demonstration of critical coronary arterial narrowing at angiography should not reflexively evoke a decision to treat the patient by revascularization. For example, hyperthyroidism should be considered in an elderly patient with atrial fibrillation and unexplained heart failure, and Lyme disease should be considered in a patient with unexplained fluctuating atrioventricular block. For example, an unexplained pericardial effusion may provide an early clue to the diagnosis of tuberculosis or a neoplasm. Overreliance on and overutilization of laboratory tests, particularly invasive techniques, for the evaluation of the cardiovascular system. Although a great deal of attention has been directed to these examinations, it is important to recognize that they serve to supplement, not supplant, a careful examination carried out with clinical and noninvasive techniques. A coronary arteriogram should not be performed in lieu of a careful history in patients with chest pain suspected of having ischemic heart disease. Despite the value of invasive tests in certain circumstances, they entail some small risk to the patient, involve discomfort and substantial cost, and place a strain on medical facilities. Prevention begins with risk assessment, followed by attention to lifestyle, such as achieving optimal weight, physical activity, and smoking cessation, and then aggressive treatment of all abnormal risk factors, such as hypertension, hyperlipidemia, and diabetes mellitus (chap. Larger arteries have a clearly demarcated internal elastic lamina that forms the barrier between the intima and the media. An external elastic lamina demarcates the media of arteries from the surrounding adventitia. Some upper-body arterial smooth-muscle cells derive from the neural crest, whereas lower-body arteries generally recruit smooth-muscle cells from neighboring mesodermal structures during development. Derivatives of the proepicardial organ, which gives rise to the epicardial layer of the heart, contribute to the vascular smooth-muscle cells of the coronary arteries.
Order ashwagandha online. Doctor Mom Separation Anxiety | Wyatt's First Day of School.
References
- Basile DP, Donohoe D, Roethe K, et al. Renal ischemic injury results inpermanent damage to peritubular capillaries and influences long-term function. Am J Physiol. 2001;281:F887.
- Sarin YK. Pyloric atresia associated with intestinal atresia. Indian Pediatr 2000;37:206.
- Kao JH. Hepatitis B vaccination and prevention of hepatocellular carcinoma. Best Pract Res Clin Gastroenterol 2015;29(6):907-917.
- Johansen K, Lynch K, Paun M, Copass M. Non-invasive vascular tests reliably exclude occult arterial trauma in injured extremities. J Trauma. 1991;31:515-522.
- Anderson C, Teo K, Gao P, for the ONTARGET and TRANCEND Investigators, et al. Renin-angiotensin system blockade and cognitive function in patients at high risk of cardiovascular disease: analysis of data from the ONTARGET and TRANSCEND studies. Lancet Neurol 2010.
- Lal R, Bhatnagar V, Mitra DK: Long-term prognosis of renal function in boys treated for posterior urethral valves, Eur J Pediatr Surg 9(5):307n311, 1999.
- Tomai F, Crea F, Gaspardone A, et al: Ischemic preconditioning during coronary angioplasty is prevented by glibenclamide, a selective ATP-sensitive K+ channel blocker. Circulation 1994;90:700-705.