
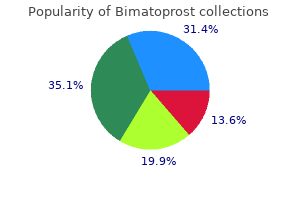
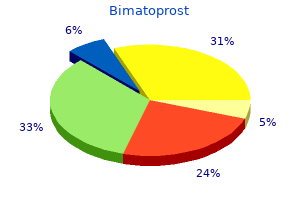
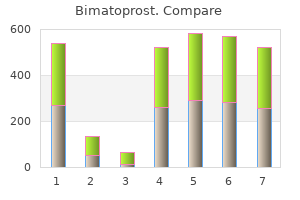
Bimatoprost
| Contato
Página Inicial
Stephen Joseph Balevic, MD
- Assistant Professor of Pediatrics
- Assistant Professor of Medicine
- Member of the Duke Clinical Research Institute
https://medicine.duke.edu/faculty/stephen-joseph-balevic-md
Bacterial nongonococcal infections or fungal disease requires some kind of joint drainage as the initial step of treatment 10 medications generic 3 ml bimatoprost free shipping, regardless of the cause and timing of the infection treatment tmj bimatoprost 3 ml buy amex, and the condition of the host aquapel glass treatment order discount bimatoprost on-line. In contrast treatment 7th march 3 ml bimatoprost order with amex, viral medicine 2015 lyrics order bimatoprost on line amex, mycobacterial, or gonococcal infections usually do not require surgical washout. Surgical Drainage versus Arthrocentesis Current literature suggests that any form of drainage is valid to reduce the infectious burden. In animal models, it has been shown that septic arthritis destroys cartilage within days [37]. Thus, rapid and effective drainage is needed, even though the exact duration until clinically significant destruction is unknown for humans, and might be influenced by several factors such as preexisting degeneration, rheumatological comorbidities, as well as the nature and inoculum size of pathogens. While surgeons usually prefer joint lavage by arthrotomy or arthroscopy [38], many rheumatologists and internists prefer joint drainage outside of the operating theater by (repeated) arthrocentesis. The discussion about the therapeutic value of each of these approaches is as old as the existence of the different medical and surgical specialities. To the best of our knowledge, there is no direct prospective head-to-head comparison in the literature, which might be difficult because of the large case mix of the arthritis population. As a rule, physicians prefer surgical drainage in lifethreatening conditions such as sepsis or in joints, which are inconvenient for repeated arthrocentesis such as the hip. Conversely, many nonsurgical specialists prefer arthrocentesis for elbow and knee arthritis that is technically easier to aspirate. Resection, Arthrodesis, or Amputation When the infection has already destroyed the articular surface and the underlying bone, resection of the infected area becomes an option. This is mainly performed in severe hip arthritis by resection of the femoral head (Girdlestone hip), which subsequently requires joint reconstruction by arthroplasty. The mechanical removal of a nonfunctional joint and adjacent bone with cavernous infectious foci allows treating all hidden foci inside porous bone before a prosthetic joint can be implanted after 4Â6 weeks of antibiotic therapy, and a 2-week free interval for observation. Antibiotic-loaded spacers may mechanically fill the gap until definitive arthroplasty [41], which is not the only mechanical solution for a destroyed articulation. Arthrodesis (the operative fusion of bones across the former synovial space) can provide a stable, generally painless, limb with some expected shortening. Arthrodesis is often performed after septic arthritis of the knee, ankle, or fingers, without major limitations in daily life, while a prosthesis approach is more applicable for the hip joint. Amputation is indicated only for life-threatening infection or persistent local infection with massive bone loss not amenable to arthrodesis or prosthesis. Frequently, vascular and arterial insufficiencies may lead to the decision of amputation. Choice of Antibiotic Agents Standard antimicrobial regimens for the most commonly encountered microorganisms are listed in Table 6. Intravenous -lactam antibiotics can be used as long as the pathogen is susceptible. Two important drawbacks of this large class of antibiotics are their low oral bioavailability and limited synovial penetration [44]. Another cell wall synthesis inhibitor is the glycopeptide vancomycin, which has a serum half-life of 6 h. While it is believed that trough serum levels of 20 mg/ml are required for optimal treatment of bone infections [45], there is no similar consensus for optimal glycopeptide therapy of arthritis. Additional arguments against high-dose vancomycin are the nephrotoxic side effects. This issue may have been exaggerated in the past, since it was frequently confounded with the use of concomitant nephrotoxic medication in patients with chemotherapy. When used in continuous perfusion, the changes in vancomycin serum levels are less important than for intermittent application. The target concentrations are achieved faster with less adverse drug effects [46]. However, continuous perfusion does not automatically provide a better outcome in terms of remission. Vancomycin should be administered over at least 1 h to prevent a histamine-mediated "red man" syndrome, which should not be confounded with a true, but rare allergy. Another glycopeptide antibiotic is teicoplanin, which is available in Europe and several other countries outside Europe, but not in the United States. Teicoplanin, which has an extended serum half-life of 72 h, can be administered within 30 min, generally at a dose of 400 mg once a day parentally (after a loading dose of 2 Ч 400 mg the first day). Alternatively, teicoplanin can be administered three times a week or intramuscularly. For synovial infections, high serum levels may be required, although optimal trough levels and daily regimens remain to be established. Another category of antibiotics includes daptomycin, which depolarizes bacterial membranes and yields a rapid, dose-dependent bactericidal effect. It can be administered once a day at a dose of 6Â8 mg/kg [47] in the absence of renal dysfunction, which makes it suitable for outpatient treatment. Some adverse events are known, in particular muscular toxicity detected by an elevation of creatinine phosphokinases. Tigecycline, which belongs to the class of glycylcyclines, is a substance that has been developed from tetracyclines, but it exhibits a fivefold higher affinity to the target. In osteoarticular infections, tigecycline is still considered an experimental drug. Among other antibiotics, aminoglycosides might be used in combination therapy for sustained bacteremia, but are not recommended for systemic monotherapy for osteoarticular infections. Aminoglycosides have a suboptimal activity in synovial fluid or bone [44], and their activity is known to be substantially reduced in a low-pH and low-oxygen environment. Linezolid inhibits ribosomal protein synthesis and can be administered parenterally or orally at a dose of 600 mg twice daily without adjustment for renal insufficiency. It is an antiÂGram-positive bacteriostatic antibiotic displaying no cross-resistance to other 84 Bone and Joint Infections Table 6. It has an excellent bioavailability of 100%, which makes it a feasible and convenient choice for outpatient treatment [44]. Disadvantages of linezolid are its high cost, and some serious side effects include reversible bone marrow suppression (mainly thrombopenia), especially during prolonged administration for more than 2 weeks. Most serious adverse events are optic neuropathy and nonreversible peripheral neuropathy, which have been reported in 2Â4% of patients 6 Native Joint Arthritis 85 with prolonged administration of linezolid. A severe serotonin syndrome in comedication with certain antidepressant drugs, such as monoamine oxidase inhibitors, has been described [48]. It may be less active for some severe infections, releasing significant amounts of thymidine from damaged host tissues and bacteria, which might antagonize its activity. Indeed, thymidine is known to antagonize the antistaphylococcal effects of both trimethoprim and sulfamethoxazole. Thus, failure with trimethoprim/ sulfamethoxazole may well depend on the extent of tissue damage and organism burden [50]. Main adverse events during prolonged administration are nausea, rash, myelosuppression, allergy, and hepatitis. Tetracyclines (doxycycline and minocycline; both 100 mg twice daily) are lipophilic, facilitating their uptake into tissues. Tetracyclines may be combined with rifampin, in order to get bactericidal activity against staphylococci [51]. Oral fusidic acid administered 500 mg three times daily has demonstrated efficacy in osteoarticular infections [52] and inhibits protein synthesis. Most experts do not recommend fusidic acid monotherapy because of the development of (potentially reversible) resistance [53]. The time interval between onset of therapy and emergence of fusidic acid resistance is not defined and is quite variable. Hepatic failure has been reported when using fusidic acid and rifampin combinations, which may require a regular monitoring of liver function. QuinupristinÂdalfopristin administration requires central venous access and dextrose infusion. However, adverse effects, such as myalgias, arthralgias, and nausea, limit their use [44]. In patients with anaerobic, streptococcal, and staphylococcal infection, bacterial protein synthesis inhibitors such as clindamycin (600Â900 mg three times daily) may be an option. The clinical efficacy of clindamycin in arthritis can be explained by its excellent penetration despite its classification as a bacteriostatic agent [44]. In isolates tested as susceptible to clindamycin but resistant to erythromycin in routine testing, resistance may be induced during ongoing clindamycin treatment [54]. Although staphylococci may be susceptible to fosfomycin and chloramphenicol, these antibiotics have not been recommended for osteoarticular infections and should be avoided, due to the potential risk of agranulocytosis under chloramphenicol administration. Fluoroquinolones are the most important antimicrobial agents against Gram-negative infections. Because of their excellent bioavailability, they can be used by the oral route; practically from the start. A multicenter study in Switzerland proved that oral combination therapy with fluoroquinolones plus rifampicin was an alternative to standard parenteral therapy (cure rates; 86% versus 84%, respectively) for staphylococcal infections, including joint infections in 35 cases [55]. Pseudomonas aeruginosa and other nonfermenting Gram-negative rods may rapidly develop fluoroquinolone resistance in monotherapy. However, to the best 86 Bone and Joint Infections of our knowledge, no antibiotic treatment adapted to this situation has been studied so far. Of note, the optimal oral dose of ciprofloxacin for synovial and bone [44] infections is set at 750 mg twice daily orally [44] for patients with good renal function. Other authors recommend parenteral treatment for 2 weeks, followed by 2 additional weeks of oral treatment [56], or for 4 weeks without indicating the route of administration [57]. Noteworthy, many surgeons prescribe antimicrobials for longer periods without evidence-based arguments [40, 59]. The current opinion is that a standard course of 6 weeks, such as used for chronic osteomyelitis [44] or periprosthetic joint infections after implant removal, might be excessive for native joint infections. In addition, 2 weeks of total antibiotic treatment had the same outcome as 2Â4 weeks (0. Since prospective randomized trials are lacking, the current view of initial parenteral antibiotic treatment administered for 2 weeks for all severe orthopedic infections can hardly be modified, with the exception of fluroquinolone use, which enables oral therapy from day 1 or 2 [55]. Like in our study, an early switch from parenteral to oral antibiotics after a median duration of 7 days was equally effective in the treatment of pediatric arthritis among 186 children [63]. This cutoff of 7 days was supported by another trial where 7 versus 14 days of parenteral antibiotics yielded an equivalent outcome after surgical drainage in 130 cases with infectious arthritis [64]. A reduced duration of antibiotic treatment for a total of 2Â3 weeks may decrease not only antibiotic consumption, but also related costs, adverse effects, and selective pressure for antibiotic resistance among bacterial pathogens. This uniform duration of concomitant antimicrobial treatment has remained constant for the last three decades. Supportive Therapy Besides surgical and antimicrobial chemotherapy, several adjunctive therapies are widely used or are under investigation for the treatment of septic arthritis. The most important aspect of arthritis therapy is to keep the joint mobility despite infection. Traditionally, many experts used to recommend bed rest or at least interdiction of weight bearing to patients with septic arthritis of the lower extremities. Although there are theoretical reasons for reducing the weight load, there is no scientific evidence for this practice. On the contrary, there is even increased cartilage damage if the infected joint is immobilized [67, 68]. Thus, patients should be allowed to move and stand, as long as the pain can be handled. This is especially important, because prolonged immobilization results in stiffening, which subsequently leads to additional morbidity and costs in the treatment of arthritis patients. A novel approach to the treatment of infectious arthritis, and a field of emerging research so far in children, has been the addition of systemic steroid therapy for native joint infections, especially to reduce the incidence of mechanical sequels due to infection [69]. Several animal studies indicate that injection of steroids in the infected joint (additional to systemic antibiotics) may reduce cartilaginous destruction without other deleterious effects [70]. Corticosteroids are supposed to diminish the number of T cells and macrophages in the synovial space, thus leading to improved cartilage preservation [70]. In the clinical situation, two randomized pediatric trials have examined this topic by randomizing in double-blind conditions 49 [71] or 123 infants [72] to receive antibiotics with or without systemic dexamethasone (the latter for 4 days) (see Chapter 5). Children on steroids showed a more rapid cure, a shorter hospital stay, and a significantly better functional outcome scale than those without steroids. Since there are no robust published data on corticosteroid therapy in septic arthritis of adults, we do not recommend their use in this population. Outcome of Native Joint Septic Arthritis the outcome of septic arthritis depends on the pathogenesis, the infecting agent, and the type of joint. In a literature review of posttraumatic cases, mortality equals zero and microbiological cure is achieved in 96%. In this particular population and according to our literature review, severe mechanical sequelae with arthrodesis, amputation, or invalidating pain were witnessed in 15% patients (12/82) [3]. There were considerable differences in outcome according to setting and the microorganism involved. However, the worst functional outcome was seen in bite-inflicted cases with notably persistent pain in 5/6 of documented cases. Interestingly, fungal or mycobacterial infections resulted in relatively modest residual morbidity. In a patient population with a majority of primary 88 Bone and Joint Infections cases and a high prevalence of S. In 21 episodes (21/169, 12%), arthritis relapsed after the end of antibiotic treatment.
Camellia thea (Green Tea). Bimatoprost.
- Green Tea Dosing »
- How does Green Tea work?
- Green Tea Safety and Side Effects »
- Reducing abnormal development and growth of cells of the cervix (cervical dysplasia) caused by human papilloma virus (HPV) infection.
- Is Green Tea effective?
- Preventing bladder, esophageal, ovarian, and pancreatic cancers.
- What other names is Green Tea known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96923
Multifocal atrial tachycardia Multifocal atrial tachycardia is less common than focal atrial tachycardia and occurs most often in acutely unwell patients and those with pulmonary disease and/or digoxin toxicity medications mexico purchase bimatoprost 3 ml mastercard. The commonest is "typical" atrial flutter where the re-entrant loop circles the right atrium (fig 5) treatment dry macular degeneration cheap bimatoprost 3 ml. The incidence in a large cohort in the United States was found to be 35/100 000 patient years symptoms 3 days after conception purchase bimatoprost on line amex, with a prevalence of 0 medicine valium order bimatoprost online. Common symptoms include palpitations symptoms thyroid problems bimatoprost 3 ml fast delivery, chest pain, anxiety, lightheadedness, pounding in the neck, shortness of breath, and uncommonly syncope. Electrocardiography Attempts should always be made to capture the arrhythmia during an episode of palpitations. We recommend giving the patient a copy to ensure it is never lost and is easily available to health professionals. A rhythm strip should be recorded if 12 lead electrocardiography is not available, and Echocardiography Echocardiography is an important investigation for patients presenting with palpitations. The presence of structural heart disease such as left ventricular impairment should prompt urgent referral and investigation. Patients troubled by recurrent symptomatic episodes should be offered treatment; options include medication or catheter ablation. Patients can be taught the Valsalva manoeuvre and some find this helpful in controlling their symptoms. Atrial flutter: the characteristic flutter waves are seen clearly after administration of adenosine, and tachycardia continues because it does not depend on the atrioventricular node. However, data from prospective non-randomised studies suggest that catheter ablation results in a greater reduction in symptoms and higher quality of life scores compared with medical treatment. Such patients are at risk of sudden cardiac death from ventricular fibrillation induced by rapidly conducted atrial fibrillation. The findings from a recent meta-analysis suggest that in patients who do not have palpitations, this risk seems to be relatively low (1. Drug treatment In general drug treatment is reserved for minimising symptoms while awaiting catheter ablation or for long term management of patients who decline catheter ablation or in whom the procedure carries an unacceptably high risk. In one small placebo controlled study 79% of patients in the flecainide group and 15% in the placebo group did not experience symptoms, though the follow-up period was only eight weeks. Catheters capable of recording electrical activation in the heart are inserted via the femoral vessels and manipulated under x ray guidance. Radiofrequency energy delivered via a catheter is used to create small localised areas of scar. If the arrhythmia was or had the potential to be incapacitating, the restriction is six weeks after successful ablation. Wolff-ParkinsonWhite syndrome and atrioventricular nodal re-entry tachycardia in a Swedish population: consequences on health-related quality of life. Adenosine for paroxysmal supraventricular tachycardia: dose ranging and comparison with verapamil: assessment in placebo-controlled, multicenter trials. The relative efficacy of adenosine versus verapamil for the treatment of stable paroxysmal supraventricular tachycardia in adults: a meta-analysis. Comparison of the efficacy and safety of esmolol, a short-acting beta blocker, with placebo in the treatment of supraventricular tachyarrhythmias. Radiofrequency catheter ablation versus medical therapy for initial treatment of supraventricular tachycardia and its impact on quality of life and healthcare costs. Long-term outcomes on quality-of-life and health care costs in patients with supraventricular tachycardia (radiofrequency catheter ablation versus medical therapy). Flecainide acetate prevents recurrence of symptomatic paroxysmal supraventricular tachycardia. Preliminary report: effect of encainide and flecainide in a randomized trial of arrhythmia suppression after myocardial infarction. In recent years, publication of several randomised controlled trials and meta-analyses have improved our understanding of the advantages and inconveniences of rate and rhythm control strategies, and effective, new non-pharmacological treatments have been introduced. An individual can have different types of atrial fibrillation over time-for example, it can evolve from paroxysmal to persistent. In most cases, atrial fibrillation is associated with hypertension, coronary disease, heart failure, valvular diseases, or cardiomyopathies that result in a dysfunctional heart muscle. Atrial fibrillation is characterised by a chaotic electrical activity in the atria that induces an irregular and usually rapid contraction of the ventricles (figure 1). Patients may be asymptomatic; may have mild symptoms, such as palpitations, weariness, and reduced effort capacity; or may present with syncope, heart failure, or angina. Many of the presenting symptoms, as well as their intensity, are related to the degree of associated tachycardia. Aside from tachycardia, the major complication of atrial fibrillation is systemic embolism, usually cerebral. Atrial fibrillation may be self limiting (paroxysmal, which may recur) or sustained (termed "persistent" if lasting more than seven days). We selected well conducted systematic reviews, metaanalyses, and large randomised controlled trials. When no study of those types was available, we considered small randomised controlled trials and cohort studies How should we investigate a patient presenting with atrial fibrillation? In patients with suspected symptoms but in sinus rhythm at the time of consultation, ambulatory electrocardiography (a 24 hour monitor or an event recorder) may be needed. History taking and physical examination are important for defining whether the atrial fibrillation is paroxysmal or persistent and which symptoms it produces, and for enabling detection of possible causes and precipitating factors, as well as any underlying heart disease (table 2). Managing acutely unwell patients Current guidelines for atrial fibrillation agree in several aspects. It is usual to admit to hospital any patient with symptomatic atrial fibrillation of recent onset, even if stable, to expedite investigation and treatment. Some experts advocate trying early restoration of sinus rhythm in these patients to prevent further atrial remodelling and reduce the risk of persistence and recurrence of the arrhythmia. Additionally, adequate treatment of cardiovascular risk factors, especially of hypertension, and avoiding hypokalaemia when using diuretics, can contribute to reduce recurrences of atrial fibrillation. A systematic review of randomised trials found that first generation calcium channel blockers, blockers, digoxin, or a combination of these drugs are more effective than placebo in slowing tachycardia associated with atrial fibrillation. A randomised trial found that intravenous diltiazem was better than intravenous digoxin (90% versus 74% of patients were well controlled at 24 hours) for rapid rate control of acute, symptomatic, uncomplicated atrial fibrillation. Full anticoagulation is warranted whenever pharmacological or electrical cardioversion is considered, for at least three weeks before and four weeks after the procedure, except when atrial fibrillation has existed for less than 48 hours. Recommended in chronic, stable systolic heart failure Hypotension, bradycardia, atrioventricular block, heart failure, bronchospasm, impotence, asthenia, depression Intravenously 0. Systematic reviews of randomised trials show that aspirin reduces the risk of stroke by about 22-36%. In well conducted systematic reviews warfarin reduced rate of stroke by 65-68% compared with placebo and 32-47% compared with aspirin, at the expense of increasing haemorrhages (2. It is important to (a) explain clearly to patients that their disease carries a risk of embolism and stroke and that they need to take a treatment continuously to reduce this risk and (b) describe the relative advantages and inconveniences of aspirin and warfarin (especially the needs of regular monitoring and dose adaptations). A large randomised trial13 and a cohort studyw5 have found that elderly patients obtain greater net benefit from warfarin despite their higher haemorrhagic risk. Cohort studies have found that thromboembolic risk in recurrent paroxysmal atrial fibrillation is closely similar to persistent or permanent atrial fibrillation. In one of them, aspirin plus clopidogrel proved inferior to warfarin in preventing embolism. In rate control, in which the aim of treatment is to slow the heart rate and prevent emboli, atrial fibrillation is tolerated. To restore sinus rhythm, pharmacological or electrical cardioversion can be used, always after adequate anticoagulation. Pharmacological cardioversion can be tried with antiarrhythmic drugs, administered intravenously or orally; patients receive the treatment usually as inpatients but sometimes as outpatients. In electrical cardioversion, a low voltage electric current, synchronised with the R wave, is delivered through pads placed appropriately on the chest and back. After cardioversion, atrial fibrillation often recurs (70-85% of patients at one year15), so most patients need treatment with antiarrhythmic drugs to stay in sinus rhythm. Several good quality randomised trials,16 17 w9 pooled in meta-analysis,18 19 have compared rate and rhythm control in a variety of patients with atrial fibrillation. No study found any difference between the strategies in terms of mortality, major cardiovascular events, or stroke. Rate control was better for some secondary outcomes: it produced fewer side effects and fewer admissions to hospital. Regardless of whether patients received rate control or rhythm control, those who were in sinus rhythm reported better scores for quality of life. However, when the results were analysed on the basis of intention to treat, quality of life scores did not differ for rate control and rhythm control. Other specialists believe that rhythm control might provide better outcomes or quality of life in some subgroups of patients. Current guidelines recommend considering rhythm control in patients with (a) lone atrial fibrillation, especially younger patients; (b) symptomatic atrial fibrillation, such as frequent symptomatic paroxysmal atrial fibrillation or symptoms despite rate control; or (c) atrial fibrillation secondary to a corrected precipitant. Nevertheless, rhythm control in those subgroups has not yet been proved in controlled trials to be better than rate control. However, a recent large randomised trial in patients with systolic heart failure found no difference between rate and rhythm control for any outcome, including worsening heart failure. Amiodarone does not increase mortality, can be given to patients with heart failure, and seems to be more effective than other drugs in maintaining sinus rhythm. Unfortunately, amiodarone causes frequent and varied adverse effects, which can be severe. Patients with infrequent paroxysmal atrial fibrillation may receive no treatment between episodes. If their atrial fibrillation recurs they may have repeated electrical or pharmacological cardioversion, sometimes following a "pill in the pocket" approach (that is, patients who have been given flecainide or propafenone in hospital to reduce paroxysmal atrial fibrillation, and tolerate them well, can be prescribed a single, oral loading dose of flecainide or propafenone for them to take outside hospital if they experience sudden and persistent heart palpitations). A prospective non-controlled trial found that this approach was effective and safe in patients with no underlying heart disease. Atrioventricular nodal catheter ablation with permanent ventricular pacing is used as a palliative approach for controlling ventricular rate in patients with symptomatic atrial fibrillation refractory to medical treatment. A metaanalysis of randomised and non-randomised studies showed that this technique is highly effective and significantly improves quality of life. Non-pharmacological interventions aiming to "cure" atrial fibrillation have been tried, initially using open surgery. In experienced centres, the success rates are above 70% at one year for paroxysmal atrial fibrillation. In persistent atrial fibrillation, pulmonary vein isolation alone is not sufficient to achieve acceptable success rates, and atrial substrate modification (discrete ablation and/or linear ablations) is usually necessary. Catheter ablation for patients with atrial fibrillation has become widely used only recently and has not yet been tested in large randomised studies with a mortality end point. However, several well conducted randomised trials and systematic reviews have shown that, in both paroxysmal and persistent atrial fibrillation, catheter ablation is better than antiarrhythmic drugs at preventing recurrences of atrial fibrillation. In such patients, catheter ablation can be considered for "severely symptomatic recurrent atrial fibrillation after failure of greater than or equal to one antiarrhythmic drug plus rate control. In a randomised trial, vernakalant, a new atrial selective agent, was effective for rapid cardioversion of recent onset atrial fibrillation. New oral anticoagulant drugs not requiring blood tests for monitoring are being developed. In a recent large randomised trial, dabigatran, a direct thrombin inhibitor, was as good as warfarin for the primary end point of stroke or systemic embolism and was associated with comparable or lower rates of major haemorrhage. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Echographic predictors of stroke in patients with atrial fibrillation: a prospective study of 1066 patients from three clinical trials. Bleeding risk index in an anticoagulation clinic assessment by indication and implications for care. Mixed comparison of stroke prevention treatments in individuals with nonrheumatic atrial fibrillation. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Oral anticoagulants versus antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no history of stroke or transient ischemic attacks. Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial fibrillation. Rate-control vs rhythm-control in patients with atrial fibrillation: a meta-analysis. Efficacy of agents for pharmacologic conversion of atrial fibrillation and subsequent maintenance of sinus rhythm: a metaanalysis of clinical trials. Meta-analysis of randomised controlled trials of the effectiveness of antiarrhythmic agents at promoting sinus rhythm in patients with atrial fibrillation. Benefits and risks of long-term amiodarone therapy for persistent atrial fibrillation: a meta-analysis. Outpatient treatment of recent-onset atrial fibrillation with the "pillin-the-pocket" approach. Clinical outcomes after ablation and pacing therapy for atrial fibrillation: a meta-analysis. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. The use of oral anticoagulation in patients with atrial fibrillation at moderate or high risk of stroke, estimated by established criteria, improves outcomes. However, to ensure that the benefits exceed the risks of bleeding, appropriate patient selection is essential. Vitamin K antagonism has been the mainstay of treatment; however, newer drugs with novel mechanisms are also available.
Removal of both the ovaries is unlikely to cause any problem in this case as she has completed her family and is postmenopausal symptoms zoloft bimatoprost 3 ml amex. There is no ascites containing malignant cells; no tumor is present on the external surface; and capsule is intact medicine quetiapine purchase cheapest bimatoprost and bimatoprost. Tumor is limited to the true pelvis medications prescribed for ptsd bimatoprost 3 ml for sale, but with histologically proven extension to small bowel or omentum symptoms 2 months pregnant 3 ml bimatoprost with mastercard. Chemotherapy is the more commonly used option and the treatment is usually administered in the form of either cisplatin or carboplatin or combination therapy including either of these drugs with paclitaxel for three to four cycles treatment 2 stroke cheap bimatoprost 3 ml mastercard. This involves an initial exploratory procedure with the removal of as much disease as possible (both tumor and the associated metastatic disease). Postoperative chemotherapy and radiotherapy in advanced cases may help improve the survival and quality of life. What are the potential benefits of cytoreduction in women with epithelial ovarian cancer? Potential benefits of cytoreduction in women with epithelial ovarian cancer are as follows: · Removal of bulky disease helps in rapidly improving the disease-related symptoms. The use of carboplatin is associated with reduced toxicity in comparison with cisplatin. Therefore recent trend is to replace cisplatin with carboplatin and use it in combination with taxane, paclitaxel. Exfoliation of the cancer cells that implant along the surfaces of the peritoneal cavity tends to follow the circulatory path of the peritoneal fluid. As a result, metastases are typically seen on the posterior cul-de-sac, paracolic gutters, right hemidiaphragm, liver capsule and peritoneal surfaces of the intestine, their mesenteries and the omentum. Other less common modes of spread of ovarian cancer include lymphatic and hematogenous spread. Lymphatic spread can lead to the involvement of pelvic and paraaortic group of lymph nodes. Lymphatic spread above the diaphragm can result in the involvement of supraclavicular lymph nodes. Ultrasonography (both transabdominal and transvaginal) is accurate in differentiating tumors of the ovary from other types of tumors of the pelvis, in more than 90% of the patients. Discrimination between benign and malignant lesions of the ovary can be made on the basis of ultrasonic patterns. As the percentage of echogenic material in the cyst increases, the likelihood of malignancy also increases. In general, benign lesions are likely to be unilateral, unilocular and thin walled with no papillae or solid areas. In contrast, malignant lesions are often multilocular with thick walls, thick septae and mixed echogenicity due to the presence of solid areas. Doppler flow studies of the ovarian artery may also help in differentiating between benign and malignant growths. In malignant tumors due to increased blood supply, the resistance index is usually low (< 0. Other signs suggestive of malignancy include presence of irregular solid parts within the mass, indefinite margins, papillary projections extending from inner wall of the cyst, presence of ascites, hydronephrosis, pleural effusion, matted bowel loops, omental implants, other evidence of peritoneal disseminated disease and lymphadenopathy. Larger tumors, usually greater than 8 cm in size have been thought to be associated with higher risk of malignancy in comparison to the smaller ones. Since there are no follicles or corpus luteum in postmenopausal ovary, no such cysts can arise. Therefore, palpable ovary in postmenopausal women must be considered as a significant finding. The pain is mainly present in the lower back and abdomen and typically exacerbates at the time of menstrual periods. During this time, the pain becomes severe enough to interfere with the quality of life. The patient gives history of experiencing mild-to-moderate pain at the time of sexual intercourse. On bimanual pelvic examination, localized areas of tenderness were felt in the pelvic region. However, no nodularity or thickness of uterosacral ligaments, cul-de-sac or rectovaginal septum was felt. Diagnosis of endometriosis is suspected on the basis of history and clinical examination. However, it needs to be confirmed by performing various investigations (imaging studies and laparoscopy). In this patient, the history points towards the likelihood of endometriosis as the likely diagnosis. Common sites for endometriotic lesions include uterine scars, uterosacral ligaments and pelvic side walls. The ectopic endometrial tissue, both the glands and the stroma, are capable of responding to cyclical hormonal stimulation and has the tendency to invade the normal surrounding tissues. Endometriosis is a disease, which is largely encountered in the women belonging to the reproductive age group. It is a leading cause of disability in women of reproductive age, responsible for causing dysmenorrhea, pelvic pain and subfertility. The common sites for the occurrence of endometriosis include the ovaries, the pouch of Douglas, uterosacral ligaments and serosal surface of the uterus, bladder, sigmoid colon, appendix, cecum, uterine scars, etc. The classic lesion is a chocolate cyst of the ovary that contains old blood that has undergone hemolysis. Involvement of uterine serosa and formation of dense adhesions can lead to fixed retroversion of the uterus. Posteriorly, the disease may cause obliteration of the cul-de-sac and form dense adhesions between the posterior vaginal wall or cervix and the anterior rectum. Deep endometriotic nodules can also cause infiltration of the uterosacral ligaments and rectovaginal septum. Through contiguous spread, endometriosis may invade the rectovaginal septum and the anterior rectal wall, the ileum, appendix and cecum may also be involved, resulting in intestinal obstruction. In the beginning, the endometriotic lesions appear as red colored, papular vesicles. With the passage of time, these lesions progressively change their appearance from dark-red to bluish-black appearance. What are the likely causes of infertility in a patient with endometriosis and how must be such patients managed? The diagnosis of endometriosis should be considered especially if a patient develops dysmenorrhea after years of pain-free menstrual cycles. Relation of pain with deep penetration during intercourse or dyspareunia needs to be asked. Previous Treatment History · the patient needs to be asked if she has ever undergone an assessment or treatment for pain in the past. What are main considerations which must be kept in mind before evaluating a case of chronic pelvic pain? This would enable the clinician to institute the most appropriate course of further investigations and management. A definite diagnosis and the cause of the pain cannot always be elicited clinically. If the gynecological cause of pain cannot be established with surety, the clinician can make use of the hormonal suppression test to distinguish between the gynecological and nongynecological causes of pain. The hormonal suppression test is a functional study that provides a practical means of making this distinction and uses progestogens to create a hypoestrogenic environment. Limitation in forward flexion may be indicative of underlying orthopedic or musculoskeletal disease gluteal folds and knee creases also needs to be assessed. If hypovolemia is present, an intravenous access must be established prior to completion of the examination. Specific Systemic Examination Abdominal Examination · Both abdominal and pelvic examinations must proceed slowly and gently because both the abdominal and pelvic components of the examination may be painful. Presence of previous surgical scars increases the possibility of postoperative adhesions, which could be an important cause of pelvic pain. A positive test occurs when the pain increases during this maneuver and is typical of anterior abdominal wall pathology and indicates myofascial cause of the pain. On the other hand, tenderness originating from inside the abdominal cavity usually decreases with this maneuver. Pelvic Examination Detailed description of the method for conducting the pelvic examination has been described in Chapter 8. Per Speculum Examination Vagina and vulva must be inspected for presence of generalized changes and any local lesions. Bimanual Pelvic Examination Tenderness upon pelvic examination is best detected at the time of menses when the endometrial implants are likely to be the largest and most tender. A moistened cotton swab should be used to elicit point tenderness in the vulva and vagina. Following the single-digit examination, a bimanual examination should be performed. The bimanual examination may reveal the following findings:  Nodularity and thickening of the uterosacral ligaments and the cul-de-sac may be present in cases of moderate to severe endometriosis. Women with minimal or mild endometriosis may have focal tenderness of the uterosacral ligaments or cul-de-sac without palpable nodules. The patient should be checked for point tenderness along the bladder or other musculoskeletal structures. While an irregularly enlarged uterus is indicative of leiomyomas, a regularly enlarged uterus with softening could indicate adenomyosis or pregnancy. A rectal examination may show rectal or posterior uterine masses, presence of nodules in the uterosacral ligaments, cul-de-sac or rectovaginal septum and/or pelvic floor point tenderness. Various investigations which help in establishing the diagnosis of endometriosis are as follows: Ultrasound examination: Ultrasound examination (both transabdominal and transvaginal) is the most commonly used investigation, which may help in revealing the pelvic pathology responsible for producing pain. Laparoscopy detects small nodules of endometriosis which may remain undetected clinically. Laparoscopy can also detect pelvic adhesions and small inflammatory pelvic masses. Varied appearance of the lesions of endometrosis as observed on laparoscopic examination is described in Table 9. Therapeutic treatment such as adhesiolysis and cauterization of endometriotic lesions can be applied in the same sitting. Perhaps the strongest reason for beginning with surgical treatment is the apparently lower recurrence rate compared with medical treatment. The likelihood of subsequent conception can be significantly increased by undertaking surgery in infertile patients. Since medical treatment has not been shown to help these patients conceive, surgical treatment is usually preferred in patients desiring fertility. Furthermore, pregnancy is contraindicated in patients receiving medical treatment and is in fact unlikely, because the drugs that are used may interfere with ovulation and endometrial implantation. On the other hand, both medical and surgical approaches have been used successfully for reducing the pain associated with endometriosis. Algorithm for treatment of patients with endometriosis is described in Flow chart 9. However, for severe endometriosis, the efficacy of hormonal treatment has not yet been established. Since no pharmacologic method appears to restore fertility, medical treatment should be reserved for use in patients with Table 9. Endometrial atrophy is the most likely mechanism, which provides relief from pain due to endometriosis. Danazol therapy is started when the patient is menstruating, usually on the 1st day of the menses. Patients with less severe symptoms may be given 200Â400 mg/day, in two divided oral doses. Treatment is usually administered for 6 months, but can be extended to 9 months in responsive patients with severe disease. Laparoscopy can help in establishing the diagnosis of endometriosis by identifying the lesions such as endometriotic nodules or lesions having blue-black or a powder-burned appearance. Laparoscopycanalsodetect presence of blood or endometriotic deposits in cul-de-sac and its obliteration. Besides diagnosis of endometriotic lesions at various locations, laparoscopy can also help in treating the patient. Powder-burn lesions over the uterine surface may be amenable to laser obliteration. Until recently, surgery in infertile patients with limited disease was thought to be no better than expectant management. However, according to the recent evidence, laparoscopic surgery has been found to significantly improve the fertility rate among infertile women with minimal or mild endometriosis. The usefulness of conservative surgery for pain relief is unclear, but it appears that immediate postoperative efficacy is at least as high as that with medical treatment and long-term outcomes may be considerably higher. Since laparoscopy is much more expensive in comparison to the medical treatment, some physicians advocate that the overall costs can be reduced by making aggressive use of empiric medical treatment before surgery is considered. Definitive surgery, which includes hysterectomy and oophorectomy, is reserved for use in women with intractable pain who no longer desire pregnancy. In summary, surgical treatment improves pregnancy rate and is the preferred initial treatment for infertility caused by endometriosis. Surgery also appears to provide better longterm pain relief than medical treatment. Per vaginal examination revealed a bulky soft uterus and the urine pregnancy test was positive.
These patients have concomitant retinitis pigmentosa treatment 02 3 ml bimatoprost overnight delivery, which is slowly progressive and bilateral medicine reminder alarm purchase bimatoprost 3 ml on line, with retinal degeneration symptoms zithromax order bimatoprost 3 ml with visa. Rods are affected treatment 4 stomach virus generic bimatoprost 3 ml without a prescription, leading to defective night vision that becomes symptomatic in early childhood treatment of pneumonia buy bimatoprost online pills. It incorporates other classifications (Mainz, Heidelberg) and describes entities based on both pathologic and genetic analyses. Senior-Loken syndrome: A syndromic form of retinal dystrophy associated with nephronophthisis. Individual renal veins can be sampled to isolate ischemic individual renal segments using this same technique. Normal, morning plasma renin activity for seated subjects ranges from about 1Â 4 ng/mL/h (0. Renin is increased with diuretics (including spironolactone), dihydropyridine calcium channel blockers, angiotensin converting enzyme inhibitors and angiotensin receptor antagonists. Levels are decreased by -blockers, clonidine, or -methyldopa (all of which reduce -sympathetic stimulation of renin release), or nonsteroidal anti-inflammatory agents (which promote salt retention and also inhibit renal prostaglandin production). Renal vein renin measurements accurately identify renovascular hypertension caused by total occlusion of the renal artery. It can involve pleural space alone or erode into lung parenchyma and bronchial tree. Its usual presentation is in a young female with severe, refractory, frequently paroxysmal hypertension with hypokalemia, hyperaldosteronism, and elevated plasma renin levels. Surgical intervention (open or laparoscopic) may be curative and in high-risk patients, radiofrequency ablation may be a less invasive alternative to radical nephrectomy (Image). Oncologic outcomes and complications in partial nephrectomy without clamping are similar to those with clamping. The clinical sequelae of warm ischemia reperfusion renal injury of approximately 30 min in one study of laparoscopic partial nephrectomy are minimal, however advanced age and pre-existing azotemia increase the risk of renal dysfunction after partial nephrectomy, especially when the warm ischemia time exceeds 30 min. No renoprotective drug therapy has proven clinical utility and renal cooling has not been proven uniformly beneficial. If renal vascular clamping is necessary, it seems that this should be for <30 min to limit renal reperfusion injury. The impact of warm ischaemia on renal function after laparoscopic partial nephrectomy. Renomedullary interstitial cell tumor arises from interstitial cells of the medulla. At gross exam, medullary fibromas are white or gray nodules within the renal pyramid. At histologic exam, this tumor is characterized by stellate spindle cells in the background of a basophilic stroma. Although it is a benign tumor, it is difficult to differentiate this lesion from other malignancies of the kidney on radiologic basis and hence many patients undergo radical nephrectomy (Image). Urinary retention and postvoid residual urine in men: Separating truth from tradition. It used to evaluate upper tract urinary obstruction as well as graft function in transplanted kidneys. Mesenchymal neoplasms of the kidney in Adults: Imaging spectrum with radiologic-pathologic correlation. Although reperfusion is essential for the survival of ischemic tissue, there is evidence that reperfusion itself causes additional cellular injury after a period of ischemia. This can occur during renal transplantation and with vascular clamping during partial nephrectomy. Doppler ultrasonographic indices after renal transplantation as renal function predictors. Pathology reveals papillary adenocarcinoma in the rete testis, commonly with local invasion. May be associated with maldescended testis or adenomatous hyperplasia of the rete testis. Not all retrocaval/circumcaval ureters are obstructed, but if obstruction exists, surgical repair is typically warranted. Despite its congenital origin, symptoms are usually absent in childhood and present later in life. They are usually identified incidentally or at a locally advanced stage when they cause symptoms from adjacent tissue invasion or compression. Compression of ureters can cause obstruction, but other symptoms can include early satiety, obstruction, or retroperitoneal bleeding. Computed tomography manifestations of common inferior vena cava dysplasia and its clinical significance. Primary adenocarcinoma of the rete testis: Diagnostic problems and therapeutic dilemmas. It is commonly performed by inserting a Foley catheter or Brodney clamp into the Fossa Navicularis. Then 50 cc of contrast solution is injected into the urethra under low pressures while obtaining a series of x-rays. Ovoid cluster of anechoic cystic spaces located peripherally in the mediastinum testis (without any solid component) and no flow within the lesion on Doppler imaging and normal adjacent testicular parenchyma are pathognomic for tubular ectasia of the rete testis. It is believed that this is secondary to obstruction of the epididymis as 85% of cases have coexisting epididymal abnormalities like epididymal cysts. Vasectomy, spermatoceles or epididymitis, may also be associated with dilatation of the rete testis. Cystic dysplasia of the rete testis is similar sonographically and histologically, but it is a congenital lesion that occurs in children. It is associated with ipsilateral renal or urogenital excretory duct malformations. Both of these lesions (tubular ectasia and cystic dysplasia) must be differentiated from benign intratesticular varicocele and tumors such as adenocarcinoma of the rete testis. Differential diagnosis may include retroperitoneal fibrosis, retroperitoneal fat necrosis, lymphangiomas, ganglioneuroma, sarcomas, metastasis form other tumors such as prostate, or bladder or germ cell tumor metastasis. Ecchymosis may be observed around the umbilicus (Cullen sign) or flank (GreyÂTurner sign). Management is primarily conservative, including frequent hemoglobin levels, resuscitation, and transfusion, as necessary. However, if the patient is hemodynamically unstable and the bleeding is from a renal source, and they have an expanding pulsatile hematoma, or renal hemorrhage cannot be stopped with selective embolization, then surgical exploration is indicated. Further evaluation of the underlying pathology and follow-up imaging for resolution is warranted. They have been reported in numerous other locations, including blood vessels, larynx, pharynx, sclera, and extradural space. Retroperitoneal occurrence has been reported and can cause ureteral compression and obstruction requiring ureterolysis and repair. Approximately 1/2 of retroperitoneal sarcomas are high-grade tumors, with the most common type being liposarcoma, followed by leiomyosarcoma. They are typically incidentally diagnosed but when patients do present with symptoms they are abdominal or back pain and increased abdominal girth. Differential diagnosis of a retroperitoneal mass includes neoplasm from a retroperitoneal visceral structure, lymphoma, or a metastatic lesion. Retroperitoneal sarcomas carry a worse prognosis than extremity sarcomas due to the difficulty of complete resection, involvement of critical structures, and delay of diagnosis. In patients whom systemic therapy or radiation is deemed to be potentially beneficial, a biopsy is mandatory. Neoadjuvant chemotherapy or radiation should be based on optimizing the patient for surgical resection. The most common presentation is an abdominal mass detected in these young patients. Extrarenal sites include central nervous system (35%), liver, and gastrointestinal tract. This condition occurs as a result of marked thinning of the parenchyma due to end-stage obstructive atrophy, and it usually denotes irretrievable renal function. Hydronephrosis in infants and children: Value of high dosage excretory urography in predicting renal salvageability. It is manifested by ocular anomalies such as glaucoma; cardiovascular outflow tract malformations, craniofacial abnormalities and pituitary abnormalities which can result in severe endocrinologic sequelae. It is characterized by short stature, limb shortening, genital hypoplasia (micropenis), and craniofacial abnormalities. Local injury to fat cells from trauma appears to be the initiating event of fat necrosis in the retroperitoneum. In addition, an inflammatory trigger such as acute pancreatitis may also be an initiating event. Its presentation is similar to that of retroperitoneal fibrosis with insidious onset of abdominal or flank pain with the possibility of extrinsic ureteral obstruction. Improvements in patient survival Journal of Hepato-Biliary-Pancreatic Surgery 1996, Volume 3, Issue 3, pp. It comprises 2% of all renal tumors and primarily affects children and 85% are diagnosed before the age of 5. The condition is usually discovered during evaluation of a normal-appearing girl who presents with failure of menstruation at the time of expected puberty. The syndrome may be caused by the lack of development of the mullerian ducts between the 5th and 6th wk of Ð gestation. In some patients, cyclic abdominal pain suggestive of some functional endometrium is noted. A continuous or cycling mode of electrical pulses are generated by an implanted device to activate or inhibit neural reflexes associated with lower urinary tract function via stimulation of the sacral nerves, which innervate the lower urinary tract and pelvic floor. An alternate theory is that stimulation may inhibit involuntary reflex voiding by altering the transmission of sensory input from the bladder to the pontine micturition center, inhibiting ascending afferent pathways but not the descending pathways. Stage I consists of percutaneous placement of temporary wire leads into the S3 foramina. A 1Â2-wk trial period occurs with the leads in place and voiding symptoms are reevaluated. Several histologic subtypes are described, the classic pattern, which is present in over 90% of tumors, is characterized by round/oval cells with clear cytoplasm with uniform nuclei. Not infrequently, tubular and peritubular fibrosis is associated with germ cell aplasia. The mechanism of action is not completely understood, but may include alteration of cholesterol metabolism, anti-inflammatory, antiestrogenic, and anti-androgenic effects, and decrease in available sex hormone-binding globulin. This procedure does not prevent deterioration of renal function but may improve flank pain if the cysts cause obstruction of the collecting system. Patients are stratified based on predicted survival into low-risk, intermediate-risk and high-risk groups for appropriate treatment regimens and for prospective trials of new therapies. It is due to compression of the isthmus of the fused kidney on the vena cava and aorta, accentuated by hypertension and accompanied by a sensation of fullness. Diagnosis can be made by identifying the mite (Sarcoptes scabiei), expressed from the papular or linear burrow-like lesion. Scoring algorithm to predict survival after nephrectomy and immunotherapy in patients with metastatic renal cell carcinoma. Typically, patients will exhibit polypoid urothelial mucosal lesions (active infection) or "sandy patch" flat, tan lesions (inactive infection). It is characterized by a cellular proliferation of variably sized glands and solid nests surrounded by basement membrane material in a cellular stroma. The contours of the lesion can be well circumscribed or infiltrative, raising concern for carcinoma. The specimen will be immunoreactive with S-100 and smooth muscle actin, indicating a myoepithelial differentiation. Other features differentiating this condition from cancer are that cells have bland nuclei and are sometimes surrounded by a hyaline-like sheath. The upper apex of the flap is then flipped down to the apex of the ureterotomy, where a 5-0 chromic stay suture is placed. The lateral edge of the flap is sutured to the lateral aspect of the ureterotomy, and the pelvis is closed. Schwannomas of renal origin are very rare with only 20 reported cases in the literature. They typically appear as spherical, solid, and well-circumscribed encapsulated lesions. Partial or radical nephrectomy (open or laparoscopic technique) is the treatment of choice as there are no reliable preoperative diagnostic methods. Using the urodynamic parameters of pressure (p) and flow rate (Q), a ratio is plotted and every data point reflects bladder contractility outflow conditions. Using a linear approximation to the p/Q data, an assessment can be made of outflow conditions. Usually diagnosed by ultrasound, these are described as a hyperechoic density in the scrotal wall that demonstrates acoustic shadowing. Scrotal pearls can occur from infection or trauma and themselves are rarely symptomatic. They may also be noticed as artifacts after torsion of the appendix testis or epididymis. Schwannoma of the kidney with magnetic resonance images of non-homogenous renal mass-a case presentation. The condition commonly affects kidneys, with renal disease affecting 10Â50% of patients. Lower urinary tract manifestations are also reported, including bladder fibrosis, microscopic hematuria, urodynamic abnormalities, such as poor compliance and obstructive uropathy. Hepatoid yolk sac tumors of the mediastinum: A clinicopathologic and immunohistochemical study of four cases.
Purchase 3 ml bimatoprost visa. Your Brain on Social Anxiety Disorder.
References
- Glantz MJ, LaFollette S, Jaeckle KA, et al. Randomized trial of a slow release versus a standard formulation of cytarabine for the intrathecal treatment of lymphomatous meningitis. J Clin Oncol 1999; 17:3110-3116.
- Tyni T, Kivela T, Lappi M, et al. Ophthalmologic findings in long-chain 3-hyroxyacyl-CoA dehydrogenase deficiency caused by the G1528C mutation: a new type of hereditary metabolic choriorentinopathy. Ophthalmology 1998;105:810.
- Lauwers GY, Ban S, Mino M, et al. Endoscopic mucosal resection for gastric epithelial neoplasms: a study of 39 cases with emphasis on the evaluation of specimens and recommendations for optimal pathologic analysis. Mod Pathol 2004;17:2.
- Mikami Y, Nakajima M, Hashimoto H, et al. Primary poorly differentiated monophasic synovial sarcoma of the lung. A case report with immunohistochemical and genetic studies. Pathol Res Pract 2003;199(12):827-33.