
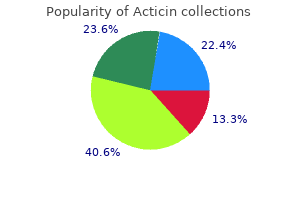
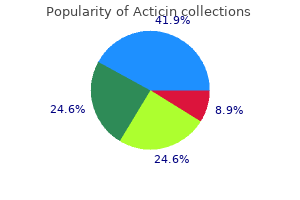
Acticin
| Contato
Página Inicial
David William Butterly, MD
- Associate Professor of Medicine
https://medicine.duke.edu/faculty/david-william-butterly-md
The lip pits may be an isolated nding (33%) or be ound with cle lip palate (67% o cases) acne 3 step order discount acticin line. Associated anomalies o the extremities may include talipes equinovarus tazorac 005 acne 30 gm acticin purchase with visa, syndactyly skin care market buy cheap acticin 30 gm on line, and popliteal pterygia acne jeans mens buy acticin online pills. Congenital lip pits have also been seen in association with the oral- acial-digital syndrome skin care giant crossword 30 gm acticin order amex. Cockayne Syndrome Cockayne syndrome is autosomal recessive, progressive bilateral sensorineural hearing loss, associated with dwar sm, acial disharmony, microcephaly, mental de ciency, retinitis pigmentosa, optic atrophy, intracranial calci cation, and multiple dental caries. Patients succumb to respiratory or genitourinary in ection in the teens or twenties. Cogan Syndrome Nonsyphilitic interstitial keratitis and vestibuloauditory symptoms are characteristics o Cogan syndrome. Symptoms include episodic severe vertigo accompanied by tinnitus, spontaneous nystagmus, ataxia, and progressive sensorineural hearing loss. Cyclophosphamide and azathioprine have been used in addition to prednisone (40 mg daily). This syndrome is not to be con used with Ménière disease despite vertiginous symptoms and uctuating hearing loss. Vogt-Koyanagi-Harada syndrome is also similar but involves alopecia, poliosis, and exudative uveitis. Syphilis is also con used with this syndrome, but in syphilis, the interstitial keratitis is old and usually does not demonstrate active in ammatory changes. Follow-up treatment o patients must be thorough in order to detect more extensive involvement, such as systemic vasculitis or aortitis. Collet-Sicard Syndrome The 9th, 10th, and 11th nerves are involved with normal sympathetic nerves. The etiology is usually a meningioma or other lesion involving the nerves in the posterior cranial ossa. Clinical eatures include saddle nose de ormity, micromelia, rhizomelia, short stature, exion contractures, and dermatoses. This syndrome is also known as chondrodystrophia epiphysialis punctata, stippled epiphysis disease, dysplasia epiphysialis punctata, chondroangiopathia calcarea punctata, and Conradi disease. Some cases point to sporadic mutations and others to autosomal dominant patterns o inheritance. The clinical eatures 10 Pa rt 1: General Otolaryngology o this syndrome are so varied rom case to case that only a complete workup can exclude other versions o this syndrome. A er a care ul workup to rule out other abnormalities, the patient is treated with aspirin, heat, and slow exercise o the joint. The joint has a gliding motion between the meniscus and the temporal bone (upper compartment). It is innervated by the auriculotemporal nerve, masseter nerve, lateral pterygoid nerve, and temporal nerve. It is supplied by the super cial temporal artery and the anterior tympanic branch o the internal maxillary artery. The lateral pterygoid muscle protracts the jaw, and the masseter, medial pterygoid, and temporalis muscles act as elevators. Creutz eldt-Jakob Disease Creutz eldt-Jakob disease is a rare spongi orm encephalopathy. Cha pter 1: Syndromes and Eponyms 11 Curtius Syndrome Curtius syndrome is a orm o hypertrophy that may involve a single small part o the body or an entire system (ie, muscular, nervous, or skeletal systems). Dandy Syndrome Oscillopsia or jumbling o the panorama common in patients a er bilateral labyrinthectomy is characteristic o this syndrome. Darier Disease (Keratosis Follicularis) Autosomal dominant, this skin disorder o the external auditory canal is characterized by keratotic debris in the canal. Déjérine Anterior Bulbar Syndrome this syndrome is evidenced by thrombosis o the anterior spinal artery, resulting in either an alternating hypoglossal hemiplegia or an alternating hypoglossal hemianesthetic hemiplegia. Demarquay-Richter Syndrome Demarquay-Richter syndrome is a congenital oro acial disorder characterized by cle lip, cle palate, lower lip stulas, and progeria acies. The diabetes insipidus has a varied time o onset and is vasopressin sensitive, indicative o degeneration o the hypothalamic cells or o the supraopticohypophyseal tract. The hearing loss is sensorineural and progressive, and primarily a ects the higher tones. Urinary tract abnormalities ranging rom atonic bladder to hydronephrosis and hydroureter have been reported with this disorder. T ird and ourth pharyngeal pouch syndrome, characterized by cardiovascular and cranio acial anomalies as well as abdominal visceral abnormalities B. Partial DiGeorge syndrome (thymic hypoplasia in which the thymus gland weighs less than 2 g) The patients have small mal ormed pinnae with narrow external auditory canals and abnormal ossicles. The patients also have shortened cochlea o the Mondini type as well as an absence o hair cells in the hook region, hypertelorism with nasal cle, shortened philtrum, and micrognathia. Other middle ear anomalies include an absence o stapedial muscle, hypoplastic acial nerve, and absent oval window. Pa rt 1: General Otolaryngology Dysphagia Lusoria Dysphagia lusoria is secondary to an abnormal right subclavian artery. The right subclavian arises abnormally rom the thoracic aorta by passing behind or in ront o the esophagus, thus compressing it. Symptoms include recurrent nonspeci c throat discom ort, oreign body sensation, dysphagia, acial pain, and increased salivation. Carotidynia may result rom impingement o the styloid process on the carotid artery, producing regional tenderness or headaches. The only e ective treatment or Eagle syndrome is surgical shortening o the styloid process. Ectodermal Dysplasia, Hypohidrotic this syndrome consists o hypodontia, hypotrichosis, and hypohidrosis. Eisenlohr Syndrome Numbness and weakness in the extremities; paralysis o the lips, tongue, and palate; and dysarthria are evidenced. Elschnig Syndrome Extension o the palpebral ssure laterally, displacement o the lateral canthus, ectropion o the lower lid, and lateral canthus are observed. Cha pter 1: Syndromes and Eponyms 13 The primary empty sella syndrome is due to congenital absence o the diaphragm sella, with gradual enlargement o the sella secondary to pulsations o the brain. Secondary empty sella syndrome may be due to necrosis o an existing pituitary tumor a er surgery, postirradiation directed at the pituitary, or pseudotumor cerebri. Face-Hand Syndrome Face-hand syndrome is a re ex sympathetic dystrophy that is seen a er a stroke or myocardial in arction. There may be edema and erythema o the involved parts along with persistent burning. Fanconi Anemia Syndrome Patients have aplastic anemia with skin pigmentation, skeletal de ormities, renal anomalies, and mental retardation. The bleeding time is prolonged, the platelet count is decreased, and the bone marrow megakaryocytes vary rom decreased to absent. Congenital anomalies o the inner, middle, and external ear could be causes o the dea ness that accompanies this syndrome. Felty Syndrome Felty syndrome is a combination o leukopenia, arthritis, and enlarged lymph nodes and spleen. Aural atresia, hearing impairment, tissue tags rom the tragus to the oral commissure, coloboma o the upper eyelid, malar hypoplasia, and cle palate also may be present. Cardiovascular, renal, and nervous system abnormalities have been noted in association with this disorder. A challenge test with either choline bitartrate or trimethylamine is diagnostic o this disease. Fordyce Disease Fordyce disease is characterized by pseudocolloid o the lips, a condition marked by the presence o numerous, small yellowish-white granules on the inner sur ace and vermilion border o the lips. Foster Kennedy Syndrome Patients with this disorder show ipsilateral optic atrophy and scotomas and contralateral papilledema occurring with tumors or other lesions o the rontal lobe or sphenoidal meningioma. Loss o taste o the anterior two-thirds o the tongue with decreased salivary and lacrimal secretions is seen with involvement o the nervus intermedius. Frey Syndrome In the normal person, the sweat glands are innervated by sympathetic nerve bers. A er parotidectomy, the auriculotemporal nerve sends its parasympathetic bers to innervate the sweat glands instead. The incidence o Frey syndrome a er parotidectomy in children has been estimated to be about 20%. Also called preauricular gustatory sweating, parotidectomy is considered the most common etiology. It may be the result o invasion by neoplasm, granulomas, or in ections in the retropharyngeal space. Gard-Gignoux Syndrome Gard-Gignoux syndrome involves paralysis o the eleventh nerve and the tenth nerve below the nodose ganglion. The symptoms include vocal cord paralysis and weakness o the trapezius and sternocleidomastoid muscles. Gardner Syndrome Gardner syndrome is an autosomal dominant disease whose symptoms include broma, osteoma o the skull, mandible, maxilla, and long bones, with epidermoid inclusion cysts in the skin and polyps in the colon. Gaucher Disease As an autosomally recessive inherited disorder o lipid metabolism, this syndrome results in a decrease in activity o the glucocerebrosidase. This leads to an increased accumulation o glucocerebrosides, particularly in the retroendothelial system. There are three classi cations o the disease: (1) the chronic non-neuronopathic orm, characterized by joint pain, aseptic necrosis, pathologic ractures, hepatosplenomegaly, thrombocytopenia, anemia, and leukopenia; (2) the acute neuronopathic Gaucher disease (in antile orm), causing increased neurologic complications that o en end in death be ore the rst 2 years o li e; and (3) the juvenile and less severe orms than the in antile orm. Cha pter 1: Syndromes and Eponyms 15 Gerlier Disease With the presence o vertigo and kubisagari, it is observed among cowherds. It is marked by pain in the head and neck with visual disturbances, ptosis, and generalized weakness o the muscles. Gilles de la ourette Syndrome Characterized by chorea, coprolalia, and tics o the ace and extremities, it a ects children (usually boys 5-10 years old). Repetitive acial grimacing, blepharospasms, and arm and leg contractions may be present. Compulsive grunting noises or hiccupping subsequently become expressions o rank obscenities. Goldenhar Syndrome A rare, nonhereditary congenital variant o hemi acial microsomia, Goldenhar syndrome is a congenital syndrome o the rst and second arch. It is characterized by underdevelopment o cranio acial structures, vertebral mal ormations, and cardiac dys unction. Clinical eatures o this syndrome are malar and maxillary hypoplasia, poor ormation o external auditory canal, supernumerary ear tags and antetragal pits, orbit, enlarged mouths, renal anomalies, and missing growth centers in the condyle, causing delayed eruption o teeth and teeth crowding. Maxillo acial reconstruction in young patients demands consideration o uture growth and development. It is also recommended or psychologic reasons as well as reasons involving the proper expansion o the skin that will later aid in urther reconstruction. This syndrome is not to be con used with reacher Collins, Berry, or Franceschetti-Zwahlen-Klein syndromes. These tend to show well-de ned genetic patterns (irregular but dominant), whereas Goldenhar syndrome does not. Goodwin umor (Benign Lymphoepithelial Lesion) this syndrome is characterized by in ammatory cells, lymphocytes, plasma cells, and reticular cells. Gradenigo Syndrome Gradenigo syndrome is due to an extradural abscess involving the petrous bone. The symptoms are suppurative otitis, pain in the eye and temporal area, abducens paralysis, and diplopia. Grisel Syndrome Grisel syndrome, also known as nasopharyngeal torticollis, is the subluxation o the atlantoaxial joint and is usually associated with children. It is associated with pharyngitis, nasopharyngitis, adenotonsillitis, tonsillar abscess, parotitis, cervical abscess, and otitis media. Proposals or etiology include overdistention o the atlantoaxial joint ligaments by e usion, rupture o the transverse ligament, excessive passive rotation during general anesthesia, uncoordinated re ex action o the deep cervical muscles, spasm o the prevertebral muscles, ligamentous relaxation rom decalci cation o the vertebrae, and weak lateral ligaments. Clinical eatures include spontaneous torticollis in a child, a exed and rotated head with limited range o motion, at ace, 16 Pa rt 1: General Otolaryngology and Sudeck sign (displacement o the spine o the axis to the same side as the head is turned). Guillain-Barré Syndrome Guillain-Barré syndrome is in ectious polyneuritis o unknown etiology ("perhaps" viral) causing marked paresthesias o the limbs, muscular weakness, or a accid paralysis. Hallermann-Strei Syndrome Hallermann-Strei syndrome consists o dyscephaly, parrot nose, mandibular hypoplasia, proportionate nanism; hypotrichosis o scalp, brows, and cilia; and bilateral congenital cataracts. Hanhart Syndrome A orm o acial dysmorphia, Hanhart syndrome is characterized by (1) bird-like pro le o ace caused by micrognathia, (2) opisthodontia, (3) peromelia, (4) small growth, (5) normal intelligence, (6) branchial arch de ormity resulting in conductive hearing loss, (7) tongue de ormities and o en a small jaw, and (8) possibly some limb de ects as well. Ear surgery should be care ully considered because o the abnormal course o the acial nerve due to this syndrome. Heer ordt Syndrome or Disease In Heer ordt syndrome, the patient develops uveoparotid ever. Hick Syndrome Hick syndrome is a rare condition characterized by a sensory disorder o the lower extremities, resulting in per orating eet and by ulcers that are associated with progressive dea ness due to atrophy o the cochlear and vestibular ganglia. Hippel-Lindau Disease Hippel-Lindau disease consists o angioma o the cerebellum, usually cystic, associated with angioma o the retina and polycystic kidneys. Homocystinuria Homocystinuria is a recessive hereditary syndrome secondary to a de ect in methionine metabolism with resultant homocystinemia, mental retardation, and sensorineural hearing loss. Cha pter 1: Syndromes and Eponyms 17 Horton Neuralgia Patients have unilateral headaches centered behind or close to the eye accompanied or preceded by ipsilateral nasal congestion, su usion o the eye, increased lacrimation and acial redness, and swelling. Cerebellar tumor, an intention tremor that begins in one extremity gradually increasing in intensity and subsequently involving other parts o the body B. Facial paralysis, otalgia, and aural herpes due to disease o both motor and sensory bers o the seventh nerve C. A orm o juvenile paralysis agitans associated with primary atrophy o the pallidal system Hunter Syndrome A hereditary and sex-linked disorder, this incurable syndrome involves multiple organ systems through mucopolysaccharide in ltration. Death, usually by the second decade o li e, is o en caused by an in ltrative cardiomyopathy and valvular disease leading to heart ailure. Chondroitin sul ate B and heparitin in urine, mental retardation, beta-galactoside de ciency, and hepatosplenomegaly are also eatures o this syndrome.
Must assess or septal hematoma and manage i present-untreated may lead to loss o septal support and saddle nose de ormity skin care qualifications buy acticin 30 gm on-line. Loss o support o the upper lateral cartilages is common and may lead to internal valve stenosis and nasal obstruction acne jeans cheap acticin 30 gm buy line. Angle ractures typically extend rom the region o the posterior body posterior to or through the region o the third molar acne 5 skin jeans buy acticin 30 gm, so that they occur behind the dentition acne images discount acticin 30 gm with mastercard. I the posterior edge o the racture is behind the angle o the mandible acne meaning order acticin 30 gm line, it is in the ramus. Fractures that traverse the sigmoid notch (between the coronoid and condylar segments) and exit the posterior mandible behind the angle are subcondylar ractures. The presence or absence o teeth (as well as their quality) has signi cant implications or racture repair. Over time, the edentulous mandible atrophies rom the top down, leaving the bone thin and atrophic and both vulnerable to racture and dif cult to repair. Alveolar ractures involve the tooth bearing segments and separate them rom the remainder o the mandible. Fracture may be repaired to avoid de ormity or i de ormity is present, or a depression may be covered with an implant to correct any de ormity (camou age). Small ractures with overlying lacerations can be repaired using the laceration (uncommon). Larger ractures or i no laceration is present, a coronal approach is generally utilized to avoid scarring on the orehead (the brow or gull wing incision is rarely used today due to the likelihood o unsightly scarring as well as injury to the supraorbital and supratrochlear nerves). Repair involves the use o small plates or mesh screwed in place so as to hold the bones in position and reestablish the proper contour o the orehead. I the racture is nondisplaced and the sinus is ully aerated and clear on C, exploration is not required. When the posterior wall o the rontal sinus(es) is disrupted, some orm o obliteration o the sinus should be considered. This requires complete removal o all mucosa ollowed by obliteration o the rontal sinus out ow tracts. Damage to the oor o the rontal sinus implies injury to the rontal sinus outow tract. Note that this approach requires care ul ollow-up and a low threshold or intervention i the sinus remains cloudy or sinusitis develops. Orbital roo ractures rarely require repair, and these may require intracranial repair. Medial wall, lateral wall, and oor ractures are repaired to restore the correct orbital volume and correct/prevent enophthalmos or exophthalmos as well as to relieve any entrapment o the extraocular muscles and correct diplopia and/or limitation o eye movement. Entrapment requires release o any tissue trapped in the racture-i it is a crack in the bone, a small implant or even a piece o ascia or cartilage or Gel lm may adequately resolve the problem and prevent recurrence. De ects must be repaired with implants or gra s to restore both orbital contour and volume. The medial wall may be approached via transcutaneous ortranscaruncular (through orbital mucosa) approach or transnasally using an endoscopic approach. The orbital oor may be approached via a transcutaneous approach through the lower lid or a transconjunctival approach through the lower lid. It may also be approached through the maxillary sinus or the nose using endoscopes, though this is more controversial. For simple ractures, rigid xation with plates in this area a er proper reduction may be adequate. Use small (mini, not micro) plates and screws and ensure at least two or three screws in each side o the racture, taking care to avoid injury to the in raorbital nerve. In raorbital rim may be reached via the gingivobuccal sulcus incision, but this puts the in raorbital nerve at risk. In raorbital rim should be repaired using microplates or wires, since xation o the skin to the plate may lead to lid malposition. Frontozygomatic racture may be reached via an upper lid crease incision or an in ra or supra brow incision (incision generally should not violate the brow, as the scar may separate the hair and be more visible). When coronal incision has been used, the rontozygomatic region is reached via this approach. Generally exposure is enough to ensure position, though, occasionally, this suture may be plated inside the orbit. Generally done with wires or microplates Critical to ensure proper reconstruction o the arch-note that it is usually not a true arch, but rather has a straight portion anteriorly and becomes an arch posteriorly (c) Zygomatic arch ractures: Generally repaired percutaneously. An instrument is advanced under the arch and is used to li the arch into position, where it typically stays. Elevation between the ascia and muscle allows access to the arch medially since the ascia inserts on the arch and the muscle continues to the coronoid process o the mandible. Once rigid xation has been properly applied, the surgeon may decide to remove the appliance used to establish occlusion. I the maxillae are impacted, Rowe disimpaction orceps or a wire through the nasal root may be necessary to ensure that proper reduction is accomplished prior to placing any rigid xation appliances. Thus repair o all areas where the mobile acial skeleton is separated rom the nonmobile cranial skeleton should be per ormed rst. Fixation is then continued rom the top down, completing the repair at the Le Fort I level. I acial symmetry and occlusion have been established and there is a minor bony discrepancy persisting at the Le Fort I level, this may be disregarded. Ellis has even recommended racturing at the Le Fort I level i symmetry has been established above and there is occlusal discrepancy present at this nal point o the procedure. For both types 2 and 3, it is critical to properly reposition the ligament posteriorly, medially, and superiorly, as the natural tendency o the ligament is to move anteriorly, laterally, and in eriorly when le unattached. When the medal anterior orbit is de cient, repair is best per ormed by rst bone gra ing the medial orbital wall de ect. A drill hole in the gra will allow proper placement o the transcanthal/ transnasal repair. Closed reduction is done by analyzing the de ormity and attempting to correct it by manipulating the bones into their native position manually using instruments. Cha pter 50: Craniomaxillofacial Trauma 969 · Lower third (a) The lower third is essentially the mandible. In the dentate patient, most, i not all, ractures through the tooth-bearing bone will be compound (open into the mouth) and there ore contaminated-the use o prophylactic antibiotics is there ore advocated by most surgeons rom the time o the racture until the time o repair. Fractures behind the dentition in dentate patients, and most ractures in edentulous patients will be closed. The orces o mastication are such that there are large orces o compression and distraction acting on the bone during unction. Arch bars are the most common means o establishing and maintaining the correct occlusal relationships (though other means may be used; see the preceding text). Once occlusion has been established, the key to stabilization o mandible ractures is to apply xation so that the orces o distraction during unction are overcome and may even be converted into compressive orces. This much less likely due to pain and splinting that tend to occur at the racture site. For ractures o the mandibular body rom angle to angle, monocortical mini-plates may be used along the so-called "ideal line o osteosynthesis. Open reduction o subcondylar ractures may be per ormed transorally or rom an external approach. For overlapping ragments, the use o lag screws is important to x the ragments together without distracting them. Note that or managing mandible ractures, amiliarity with the locations o the tooth roots and the in erior alveolar nerves is important. Most American surgeons do not open ractures o the condylar head at this time, so this will not be addressed. For the edentulous mandible: * I there is no atrophy, it can be treated in a manner similar to the dentate mandible. Cha pter 50: Craniomaxillofacial Trauma 971 A note about pediatric ractures: The presence o mixed dentition makes the use o arch bars more dif cult, and dental splints may be very help ul Note the presence o the tooth buds in the bone during the period o deciduous dentition. T ough this approach has allen out o vogue in recent years, it should be in the surgical armamentarium. Best treated by removing hardware, debriding bone, replacing a longer, stronger repair, with or without a cancellous bone gra (b) Malposition A malposition may be signi cant or minimal I signi cant, early reoperation and repositioning and restabilization can rescue an inadequate repair. Since atrophic, edentulous mandibles are very small in height, when the body o such a mandible is ractured, it is best repaired using which o the ollowing techniques When the orbit is ractured along with a zygomatic racture, and there is clinical evidence o enophthalmos, which o the ollowing represents the best approach to repair First attend to the de ect in the orbital loor, and once this is repaired, the zygoma can be ixed. When managing subcondylar ractures o the mandible, which o the ollowing is most correct When the anterior wall o the rontal sinus is ractured, which o the ollowing is most likely to be true Chapter 51 Orbital Fractures Orbital ractures are injuries requently encountered both acutely in the emergency room as well as in the o ce as chronic conditions. This chapter covers the clinical presentation, evaluation, examination ndings, and management o orbital ractures organized rom an anatomical perspective. The bulk o the discussion ocuses on oor ractures, as these are the most requent orbital ractures encountered. Other orbital ractures are then discussed in a more succinct ashion to highlight the unique eatures based on their anatomic location. Basic orbital anatomy is not discussed; or a review o orbital anatomy, re er to Chapter 6. Most common location is posteromedial oor (maxillary bone), medial to in raorbital neurovascular bundle. Blunt trauma (usually object smaller in diameter than orbit) pushes orbital contents posteriorly. Resultant increase in intraorbital pressure causes racture at weakest point: posteromedial orbital oor (hydraulic theory). Buckling theory: direct blow to orbital rim causes buckling at weakest point o orbital oor. Blow-in racture: direct trauma to orbital rim causing bone ragment to be displaced into orbit (rather than into maxillary sinus); presents with exophthalmos, not enophthalmos. Lens dislocation: blurred vision; may occlude pupil causing angle closure glaucoma v. Commotio retinae: injury to outer retinal layers caused by shockwave rom blunt trauma with resultant edema; may cause blurred vision i macula involved vii. Most common in children due to more exible bones (greenstick racture- "white eyed" blow-out racture). Visual acuity: vision assessed with one eye at a time, using near card with ull spectacle correction. Pupillary examination: assess or af erent pupillary de ect, anisocoria, and peaked/ irregular pupil. Diplopia elds: Have patient ollow your nger in horizontal and vertical directions. Increase in intraocular pressure (1-15 mm Hg) on upgaze compared to primary position suggests entrapment o in erior rectus. Ophthalmic examination: slit lamp biomicroscopy and dilated unduscopic examination. Forced ductions: used to distinguish paretic muscle rom entrapped (restricted) muscle i. Patient is asked to look in direction being examined and globe is then rotated in the same direction. In acute setting this test may not be help ul as edema and hemorrhage o muscle capsule may cause restriction and simulate an entrapped muscle. This test may be most help ul intraoperatively, done both at the beginning o surgery and then a er orbital contents have been reposited and racture has been reduced to ensure that all so tissue has been reed. Smith and Converse advocated early surgical intervention, within 2 to 3 weeks o injury, to minimize late enophthalmos and diplopia. Putterman (1974) argued that all cases may be ollowed or 4 to 6 months or longer prior to surgical intervention. Found that patients with diplopia had resolution in unctional positions o gaze without surgical intervention. One-quarter o patients had persistent diplopia, but in extremes o gaze, and were without unctional limitations. Dutton proposed the ollowing recommendations that are generally accepted as guidelines or surgical intervention: i. Symptomatic persistent diplopia with positive orced ductions, computed tomography (C) evidence o orbital tissue or muscle entrapment, and no clinical improvement over 1 to 2 weeks ii. Persistent diplopia inter ering with occupational demands: pilots, painters, mechanics or pro essional athletes. Nasal precautions: avoid nose blowing, sneezing with a closed mouth, sucking through a straw. Timing o racture repair: ractures are general observed or 7 to 10 days to allow edema and hemorrhage to decrease. Pre erably repaired within 2 weeks o injury; injuries greater than 6 weeks become increasingly di cult to repair. Delayed repair o oor racture may result in persistent enophthalmos, secondary to brosis and contracture o traumatized orbital so tissue. Jaeger plate is used to protect globe and provide gentle retraction, as lower lid is retracted by traction suture.
Cephalosporins with side chains may undergo hepatic metabolism skin care gadgets discount acticin 30 gm mastercard, but the major elimination mechanism for drugs in this class is renal excretion via active tubular secretion skin care usa cheap acticin online visa. Most first- and second-generation cephalosporins do not enter the cerebrospinal fluid even when the meninges are inflamed acne treatment during pregnancy generic acticin 30 gm buy on line. Structural differences from penicillins render cephalosporins less susceptible to penicillinases produced by staphylococci acne 14 dpo buy on line acticin, but many bacteria are resistant through the production of other betalactamases that can inactivate cephalosporins acne vulgaris cause buy acticin line. First-generation drugs-Cefazolin (parenteral) and cephalexin (oral) are examples of this subgroup. They are active against gram-positive cocci, including staphylococci and common streptococci. Clinical uses include treatment of infections caused by these organisms and surgical prophylaxis in selected conditions. These drugs have minimal activity against gram-negative cocci, enterococci, methicillin-resistant staphylococci, and most gramnegative rods. Second-generation drugs-Drugs in this subgroup usually have slightly less activity against gram-positive organisms than the first-generation drugs but have an extended gram-negative coverage. Examples of clinical uses include infections caused by the anaerobe Bacteroides fragilis (cefotetan, cefoxitin) and sinus, ear, and respiratory infections caused by H influenzae or M catarrhalis (cefamandole, cefuroxime, cefaclor). Third-generation drugs-Characteristic features of thirdgeneration drugs (eg, ceftazidime, cefoperazone, cefotaxime) include increased activity against gram-negative organisms resistant to other beta-lactam drugs and ability to penetrate the blood-brain barrier (except cefoperazone and cefixime). Most are active against Providencia, Serratia marcescens, and beta-lactamaseproducing strains of H influenzae and Neisseria; they are less active against Enterobacter strains that produce extended-spectrum beta-lactamases. Individual drugs also have activity against Pseudomonas (cefoperazone, ceftazidime) and B fragilis (ceftizoxime). Drugs in this subclass should usually be reserved for treatment of serious infections. Ceftriaxone (parenteral) and cefixime (oral), currently drugs of choice in gonorrhea, are exceptions. Likewise, in acute otitis media, a single injection of ceftriaxone is usually as effective as a 10-day course of treatment with amoxicillin. Fourth-generation drugs-Cefepime is more resistant to beta-lactamases produced by gram-negative organisms, including Enterobacter, Haemophilus, Neisseria, and some penicillinresistant pneumococci. Cefepime combines the gram-positive activity of first-generation agents with the wider gram-negative spectrum of third-generation cephalosporins. Ceftaroline has activity in infections caused by methicillin-resistant staphylococci. Allergy-Cephalosporins cause a range of allergic reactions from skin rashes to anaphylactic shock. Complete cross-hypersensitivity between different cephalosporins should be assumed. Cross-reactivity between penicillins and cephalosporins is incomplete (510%), so penicillin-allergic patients are sometimes treated successfully with a cephalosporin. However, patients with a history of anaphylaxis to penicillins should not be treated with a cephalosporin. Other adverse effects-Cephalosporins may cause pain at intramuscular injection sites and phlebitis after intravenous administration. They may increase the nephrotoxicity of aminoglycosides when the two are administered together. Drugs containing a methylthiotetrazole group (eg, cefamandole, cefoperazone, cefotetan) may cause hypoprothrombinemia and disulfiram-like reactions with ethanol. Aztreonam Aztreonam is a monobactam that is resistant to beta-lactamases produced by certain gram-negative rods, including Klebsiella, Pseudomonas, and Serratia. Aztreonam is administered intravenously and is eliminated via renal tubular secretion. Adverse effects include gastrointestinal upset with possible superinfection, vertigo and headache, and rarely hepatotoxicity. Imipenem, Doripenem, Meropenem, and Ertapenem these drugs are carbapenems (chemically different from penicillins but retaining the beta-lactam ring structure) with low susceptibility to beta-lactamases. They have wide activity against gram-positive cocci (including some penicillin-resistant pneumococci), gram-negative rods, and anaerobes. With the exception of ertapenem, the carbapenems are active against P aeruginosa and Acinetobacter species. For pseudomonal infections, they are often used in combination with an aminoglycoside. The carbapenems are administered parenterally and are useful for infections caused by organisms resistant to other antibiotics. Carbapenems are currently co-drugs of choice for infections caused by Enterobacter, Citrobacter, and Serratia species. Imipenem is rapidly inactivated by renal dehydropeptidase I and is administered in fixed combination with cilastatin, an inhibitor of this enzyme. Cilastatin increases the plasma halflife of imipenem and inhibits the formation of a potentially nephrotoxic metabolite. Meropenem is similar to imipenem except that it is not metabolized by renal dehydropeptidases and is less likely to cause seizures. Ertapenem has a long half-life but is less active against enterocci and Pseudomonas, and its intramuscular injection causes pain and irritation. Beta-Lactamase Inhibitors Clavulanic acid, sulbactam, and tazobactam are used in fixed combinations with certain hydrolyzable penicillins. They are most active against plasmid-encoded beta-lactamases such as those produced by gonococci, streptococci, E coli, and H influenzae. They are not good inhibitors of inducible chromosomal beta-lactamases formed by Enterobacter, Pseudomonas, and Serratia. Vancomycin is also a backup drug for treatment of infections caused by Clostridium difficile. Teicoplanin and telavancin, other glycopeptide derivatives, have similar characteristics. Vancomycin-resistant enterococci are increasing and pose a potentially serious clinical problem because such organisms usually exhibit multiple-drug resistance. Vancomycinintermediate strains of S aureus resulting in treatment failures have also been reported. Vancomycin is not absorbed from the gastrointestinal tract and may be given orally for bacterial enterocolitis. When given parenterally, vancomycin penetrates most tissues and is eliminated unchanged in the urine. Toxic effects of vancomycin include chills, fever, phlebitis, ototoxicity, and nephrotoxicity. Rapid intravenous infusion may cause diffuse flushing ("red man syndrome") from histamine release. Fosfomycin Fosfomycin is an antimetabolite inhibitor of cytosolic enolpyruvate transferase. This action prevents the formation of N-acetylmuramic acid, an essential precursor molecule for peptidoglycan chain formation. Resistance to fosfomycin occurs via decreased intracellular accumulation of the drug. In a single dose, the drug is less effective than a 7-day course of treatment with fluoroquinolones. Fosfomycin may be synergistic with beta-lactam and quinolone antibiotics in specific infections. Bacitracin Bacitracin is a peptide antibiotic that interferes with a late stage in cell wall synthesis in gram-positive organisms. Cycloserine Cycloserine is an antimetabolite that blocks the incorporation of d-Ala into the pentapeptide side chain of the peptidoglycan. Because of its potential neurotoxicity (tremors, seizures, psychosis), cycloserine is only used to treat tuberculosis caused by organisms resistant to first-line antituberculous drugs. Daptomycin Daptomycin is a novel cyclic lipopeptide with spectrum similar to vancomycin but active against vancomycin-resistant strains of enterococci and staphylococci. Vancomycin Vancomycin is a bactericidal glycoprotein that binds to the d-Ala-d-Ala terminal of the nascent peptidoglycan pentapeptide side chain and inhibits transglycosylation. This action prevents elongation of the peptidoglycan chain and interferes with crosslinking. The primary mechanism of antibacterial action of the penicillins involves inhibition of (A) Beta-lactamases (B) Cell membrane synthesis (C) N-acetylmuramic acid synthesis (D) Peptidoglycan cross-linking (E) Transglycosylation Questions 2 and 3. A 33-year-old man was seen in a clinic with a complaint of dysuria and urethral discharge of yellow pus. He had a painless clean-based ulcer on the penis and nontender enlargement of the regional lymph nodes. Gram stain of the urethral exudate showed gram-negative diplococci within polymorphonucleocytes. The patient informed the clinic staff that he was unemployed and had not eaten a meal for 2 d. The most appropriate treatment of gonorrhea in this patient is (A) A single intramuscular dose of ceftriaxone (B) Amoxicillin orally for 7 d (C) Procaine penicillin G intramuscularly as a single dose plus oral probenecid (D) Meropenem orally for 7 d (E) Vancomycin intramuscularly as a single dose 3. Immunofluorescent microscopic examination of fluid expressed from the penile chancre of this patient revealed treponemes. Because he appears to be infected with Treponema pallidum, the best course of action would be to (A) Administer a single oral dose of fosfomycin (B) Give no other antibiotics because drug treatment of gonorrhea provides coverage for incubating syphilis (C) Inject intramuscular benzathine penicillin G (D) Treat with oral tetracycline for 7 d (E) Treat with vancomycin 4. A 36-year-old woman recently treated for leukemia is admitted to the hospital with malaise, chills, and high fever. The records of the patient reveal that she had a severe urticarial rash, hypotension, and respiratory difficulty after oral penicillin V about 6 mo ago. The most appropriate drug regimen for empiric treatment is (A) Aztreonam (B) Ceftriaxone (C) Meropenem (D) Oxacillin (E) Ticarcillin plus clavulanic acid Questions 68. A 52-year-old man (weight 70 kg) is brought to the hospital emergency department in a confused and delirious state. He has had an elevated temperature for more than 24 h, during which time he had complained of a severe headache and had suffered from nausea and vomiting. Lumbar puncture reveals an elevated opening pressure, and cerebrospinal fluid findings include elevated protein, decreased glucose, and increased neutrophils. Gram stain of a smear of cerebrospinal fluid reveals gram-positive diplococci, and a preliminary diagnosis is made of purulent meningitis. The microbiology report informs you that for approximately 15% of S pneumoniae isolates in the community, the minimal inhibitory concentration for penicillin G is 20 mcg/mL. Treatment of this patient should be initiated immediately with intravenous administration of (A) Amoxicillin (B) Cephalexin (C) Ceftriaxone plus vancomycin (D) Nafcillin (E) Piperacillin 7. Resistance of pneumococci to penicillin G is due to (A) Alterations in porin structure (B) Beta-lactamase production (C) Changes in chemical structure of target penicillin-binding proteins (D) Changes in the d-Ala-d-Ala building block of peptidoglycan precursor (E) Decreased intracellular accumulation of penicillin G 8. If this patient had been 82-years-old and the Gram stain of the smear of cerebrospinal fluid had revealed gram-positive rods resembling diphtheroids, the antibiotic regimen for empiric treatment would include (A) Ampicillin (B) Cefoxitin (C) Ceftriaxone (D) Fosfomycin (E) Vancomycin 9. A patient needs antibiotic treatment for native valve, culturepositive infective enterococcal endocarditis. His medical history includes a severe anaphylactic reaction to penicillin G during the last year. The best approach would be treatment with (A) Amoxicillin-clavulanate (B) Aztreonam (C) Ceftriaxone (D) Ticarcillin (E) Vancomycin 10. The beta-lactam antibiotics also activate autolysins, which break down the bacterial cell wall. Vancomycin inhibits transglycolase, preventing elongation of peptidoglycan chains. Treatments of choice for gonorrhea include a single dose of ceftriaxone (intramuscularly). Because of the high incidence of beta-lactamase-producing gonococci, the use of penicillin G or amoxicillin is no longer appropriate for gonorrhea. Alternative drugs (not listed) for gonorrhea include cefixime, azithromycin (see Chapter 44) or spectinomycin (see Chapter 45). The penile chancre, the enlarged nontender lymph nodes, and the microscopic identification of treponemes in fluid expressed from the lesion are essentials of diagnosis. Although a single dose of ceftriaxone may cure incubating syphilis, it cannot be relied on for treating primary syphilis. The most appropriate course of action in this patient is to administer a single intramuscular injection of 2. For penicillin-allergic patients, oral doxycycline or tetracycline for 15 d (not 7 d) is effective in most cases (see Chapter 44). First- and second-generation cephalosporins are not effective in meningitis because they do not readily enter the cerebrospinal fluid. The elimination half-lives of many beta-lactam antibiotics are prolonged by probenecid, which inhibits their proximal tubular secretion. All penicillins should be avoided in patients with a history of allergic reactions to any individual penicillin drug. Cephalosporins should also be avoided in patients who have had anaphylaxis or other severe hypersensitivity reactions after use of a penicillin. There is partial cross-reactivity between penicillins and the carbapenems such as imipenem and meropenem, but no crossreactivity between the penicillins and aztreonam. Pneumococcal isolates with a minimal inhibitory concentration for penicillin G of greater than 2 mcg/mL are highly resistant. Such strains are not killed by the concentrations of penicillin G or ampicillin that can be achieved in the cerebrospinal fluid. Nafcillin has minimal activity against penicillin-resistant pneumococci and piperacillin is mainly used for infections caused by gram-negative rods.
Ethmoid Roo and Cribri orm Plate ypically skin care vitamin e discount 30 gm acticin with visa, the ethmoid roo slopes in eriorly and medially acne inversa cheap acticin 30 gm amex, and is thinner medially than laterally (by a actor o 10×) skin care zinc oxide acticin 30 gm buy cheap. This should be care ully evaluated preoperatively by comparing the ratio o the ethmoid height to that o the height o the maxillary sinus acne and birth control acticin 30 gm buy overnight delivery. Sphenoethmoidal (Onodi) Cell · Onodi stressed that when the most posterior ethmoid cell was highly pneumatized skin care 2012 buy discount acticin, it could extend posteriorly along the lamina papyracea and superiorly into the anterior wall o the sphenoid sinus. Sphenoid Sinus · Located centrally within the skull, the sphenoid sinuses are separated by an intersinus septum that is highly variable in position. Laterally, the sinus may pneumatize or a variable distance under the middle cranial ossa (lateral recess), in eriorly it may pneumatize to a variable extent into the pterygoid processes, and posteriorly it may pneumatize or a variable distance in erior to the sella turcica. The cell above the septum (E) represents a sphenoethmoidal cell (Onodi cell) that has pneumatized above the sphenoid sinus (S), bringing the ethmoid sinus into close proximity to the optic nerve and carotid artery. Environmental Progression o Acute Rhinosinusitis · Multiple episodes o acute rhinosinusitis may ultimately lead to mucosal dys unction and chronic in ections. Bio lms · Bacterial bio lms are a complex organization o bacteria anchored to a sur ace. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 469 · Bio lms elicit a considerable immunologic reaction and can be di cult to eradicate rom the paranasal sinuses. Bacterial Superantigen · Bacteria possess the ability to elicit pathogenic exotoxins that can activate large subpopulations o the -lymphocyte pool. Mucociliary Dys unction · Mucociliary clearance is especially important in maintaining the homeostasis o the paranasal sinuses. The gel and sol layers o the mucus blanket are severely af ected, thereby hindering bacterial removal. Odontogenic Sinusitis · Dental pathology can occasionally lead to maxillary sinusitis with subsequent spread to adjacent sinuses and should always be considered in unilateral sinusitis. Alteration in Sinus Microbiome · There has been a signi cant amount o interest recently in the role o microbes in various health diseases (ie, Clostridium dif cile colitis). Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 471 · The microbiome re ers to the totality o all microbes in given environment. Airway Hyperactivity · Although the nature o the relationship between the paranasal sinuses and the lungs is still unclear, the lungs and the upper airway share contact with inhaled pathogens and include many o the same epithelial properties. Immune Barrier Hypothesis · Recently, a uni ying theory on the pathogenesis o chronic sinusitis has been proposed to help explain the plethora o potential etiologies as previously discussed. Diagnostic Nasal Endoscopy · The development o the modern rigid nasal endoscope represents a major advance in rhinologic diagnostic capability. The overall anatomy, presence o pathologic secretions or polyps, and the condition o nasal mucosa may be identi ed. In some cases it may also be possible to identi y the nasolacrimal duct within the in erior meatus. T erea er, the scope is advanced through the nasal cavity and toward the nasopharynx. As the scope is advanced into the nasopharynx, the entire nasopharynx, including the contralateral eustachian tube ori ce, can be examined by rotating the telescope. While directing the scope posteriorly, the in erior portion o the middle meatus, ontanelles, and accessory maxillary ostia can be examined. The scope is then passed medial to the middle turbinate and advanced posteriorly to examine the sphenoethmoidal recess. Rotating the scope superiorly and slightly laterally allows or visualization o the superior turbinate and meatus as well as the slit-like or oval ostia o the sphenoid sinus. As the scope is brought back anteriorly, it can requently be rotated laterally under the middle turbinate into the posterior aspect o the middle meatus. The bulla ethmoidalis, hiatus semilunaris, and in undibular entrance are inspected. Withdrawing the telescope urther can provide an excellent view o the middle turbinate, uncinate process, and surrounding mucosa. In selected patients this portion o the examination can be conducted rom an anterior approach, i the anatomy is avorable. Alternatively, additional topical anesthesia may be placed within the middle meatus and in the region o the anterior insertion o the middle turbinate. Diagnostic and T erapeutic Applications · A crucial application o nasal endoscopy is to evaluate patient response to medical treatment, such as topical nasal steroids, antibiotics, oral steroids, and antihistamines. A small malleable Calgiswab is care ully directed to the middle meatus or other site o origin o purulent drainage and submitted or culture. Preoperative Patient Management · Minimizing the risks or complications and optimizing surgical planning are o critical importance in patient management. Not exceeding this s 476 Pa rt 3: Rhinology dosage is very important as seizures and other complications have been noted at higher dosage. C Evaluation · Regardless o the reason or surgery, all patients should have at least a coronal C with 3-mm cuts. In these latter situations, or in revision surgery, the use o computer-aided surgical navigation is also a reasonable consideration. In any case, the surgeon should have a 3D conceptualization o the anatomy be ore starting endoscopic sinus surgery. On the le t side the skull base has been violated (curved arrow), apparently as a result o the limited vertical height posteriorly. Preparation o the Nasal Cavity · Under local or general anesthesia, the nose is decongested prior to surgery with oxymetazoline. The needle tip is used to eel or the oramen and the injection must be per ormed very slowly, a ter aspiration. Surgical echnique Uncinectomy · Anterior attachment recognized by a semilunar depression in the lateral nasal wall. I site o attachment not evident, it is pre erable to make the incision posterior to its attachment and remove any residual uncinate later. Maxillary Antrostomy · Identi y the in erior cut edge o the uncinate process and pull it medially with a balltipped seeker. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 479 Ethmoidectomy · Use 0° telescope until the major landmarks have been identi ed (to avoid disorientation). I the posterior ethmoid cells are to be entered: · Withdraw telescope slightly to provide overview o basal lamella. In general, the cells here are larger and the skull base is more horizontal, making identi cation signi cantly easier and sa er than in the anterior ethmoid sinus. Frontal Recess Surgery (Dra ype 1) Because o the di cult anatomic relationships, it is very important to rereview the C and have a 3D conceptualization o the anatomy be ore working in the region o the rontal sinus. The rontal sinus may then be accessed as ollows: · Dissect rom posterior to anterior along the skull base, skeletonizing the medial orbital wall. Dra ype 2 Frontal Sinusotomy · In a Dra 2A, the rontal sinus is opened between the lamina papyracea and the insertion o the middle turbinate. The septal mucosa that is removed to create a window can be used as a ree gra over the exposed bone anteriorly. At the time o surgery, tumor was attached extensively to the anterior wall and was burred with a 70° diamond burr. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 483 Surgical Steps · Care ully evaluate the axial, coronal, and sagittal C to evaluate anatomic suitability and the extent o bone that may need to be removed by drill. The size o the rontal opening created will depend on the degree o bony thickening and mucosal in ammation present. Management o the Nasal Septum · The nasal septum is addressed during sinus surgery i it is markedly deviated to where it signi cantly inter eres with nasal air ow or i the deviation is such that access to the anterosuperior attachment o the middle turbinate is not possible with the 0° telescope. This allows the deviated nasal septum to be addressed under excellent visualization, without the necessity to either change to a headlight or to change instrumentation. We have ound the 1-mm Acu ex orthopedic punch particularly help ul in this regard. The septal aps are then quilted with a running chromic suture on a small straight needle. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 485 Endoscopic Sinus Surgery or Neoplasms and Skull Base De ects General guidelines or mucoceles are as ollows: · Identi y skull base posteriorly (or rontal). General guidelines or inverted papillomas are as ollows: · Obtain permission to convert to an open procedure. However, rontal sinus and supraorbital ethmoid de ects may require an adjunctive external approach. Laterally placed de ects may be approached with ligation or cauterization o the internal maxillary artery and a transpterygoid approach. Avoiding and Managing Complications Prevention o Bleeding · Provide care ul topical and in ltrative vasoconstriction. Approximately 40% are dehiscent as the artery can travel beneath the ethmoid roo along a bony mesentery, in some cases l to 3 mm rom the roo. Care must be taken not to mistake the artery or a bony septae o an ethmoid cell and attempt resection. Care should be taken to avoid dissecting the basal lamella too ar in eriorly when entering the posterior ethmoids. Bleeding can result as the sphenopalatine artery lies just behind the in erior aspect o the basal lamellae in most patients. Management o Intraoperative Bleeding · Pack the surgical cavity with cottonoid pledgets soaked in vasoconstrictive agents. Management o Postoperative Epistaxis · Application o topical hemostatic vasoconstrictive agents. Prevention o Orbital Injury · Identi y the lamina orbitalis positively and do so early in the dissection. This extremely important in cases where a sphenoethmoidal cell (Onodi cell) is present. Should this artery be inadvertently divided during surgery, the lateral aspect o the vessel can retract within the orbit and bleed with a resultant and dramatic orbital hematoma. Management o Orbital Complications · I the lamina papyracea is entered during intranasal ethmoidectomy and orbital at is exposed, urther dissection should be terminated in the immediate region and the at should not be removed or resected. Medical measures such as topical timolol; intravenous acetazolamide; mannitol; and high-dose steroids, globe massage, and C scan should be considered. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 487 Prevention o Skull Base Injury · Conceptualize the C anatomy. Identi y the ethmoid roo positively and then work anteriorly eeling behind bony partitions be ore they are removed. Management o Intraoperative Skull Base Injury/Cerebrospinal Fluid Rhinorrhea · Inspect the area endoscopically to determine the site and size and determine i intradural injury has occurred. Local Management o the Postoperative Cavity · Merocel sponges are typically removed on the rst postoperative day and the cavities suctioned ree o blood under local anesthetic. At each visit, crusts are debrided, the cavity is examined or areas o persistent in ammation, and any residual ragments o exposed or osteitic bone are removed. Scars are divided and particular attention is paid to the all important rontal recess region. However, sinus cavities opened around the repair are debrided in the standard ashion. Long- erm Management · Symptoms, with the exception o postnasal discharge, usually resolve early ollowing endoscopic sinus surgery. Indeed, patients should be instructed to ollow their sense o smell and to obtain additional medical therapy and ollow-up endoscopic examination, i they experience a signi cant decrease in their ability to smell. Cha pter 26: Paranasal Sinuses: Embryology, Anatomy, Endoscopic Diagnosis, and Treatment 489 · Advances in nasal endoscopy, radiologic imaging, medical treatments, and surgical technique have allowed or signi cant improvements in patient management. However, recalcitrant sinus disease is a particular problem and continues to await new therapeutic approaches. Practice Guidelines · A thorough understanding o paranasal sinus anatomy and embryology is required or success ul and sa e sinus surgery. Sinus microbiome diversity depletion and Coryne, bacterium tuberculostearicum enrichment mediates rhinosinusitis. Functional endoscopic sinus surgery: anesthesia, technique, and postoperative management. Perspectives on the etiology o chronic rhinosinusitis: an immune barrier hypothesis. Middle meatal spacers or the prevention o synechiae ollowing endoscopic sinus surgery: a systematic review and meta-analysis o randomized controlled trials. A systematic review and meta-analysis o asthma outcomes ollowing endoscopic sinus surgery or chronic rhinosinusitis. Management o an acute orbital hematoma in the recovery room includes all o the ollowing except: A. Anatomy o the Nose Nasal Skeleton · Bone (a) wo paired nasal bones, which attach laterally to nasal process o maxilla · Cartilage (a) Paired upper lateral, lower lateral cartilages (b) Accessory sesamoid cartilages Nasal Septum · Bone: vomer, perpendicular plate o ethmoid bone, maxillary crest, palatine bone · Cartilage: quadrangular cartilage Lateral Nasal Wall · T ree turbinates and corresponding space (meatus) · In erior, middle, and superior turbinates · In erior meatus: drains nasolacrimal duct 491 492 Pa rt 3: Rhinology · Middle meatus: drains maxillary, anterior ethmoid, and rontal sinuses · Superior meatus: drains posterior ethmoid sinuses Arterial Blood Supply · External nose (a) Primary supply rom external carotid artery to acial artery (b) Superior labial artery: columella and lateral nasal wall (c) Angular artery: nasal side wall, nasal tip, and nasal dorsum · Nasal cavity (a) Both external and internal carotid artery (b) External carotid artery system Internal maxillary artery Sphenopalatine artery via sphenopalatine oramen: divides into lateral nasal artery, supplying lateral nasal wall; and posterior septal artery, supplying posterior aspect o septum Descending palatine artery: orms the greater and lesser palatine arteries; supplies lower portion o the nasal cavity Greater palatine artery: passes in eriorly through greater palatine canal and oramen, travels within hard palate mucosa; bilateral arteries meet in midline and travel through single incisive oramen back into nasal cavity (c) Internal carotid artery system Ophthalmic artery enters orbit and gives o anterior and posterior ethmoid arteries; courses via anterior and posterior ethmoidal canal, takes an intracranial course and then turns in eriorly over the cribri orm plate Anterior ethmoid artery: supplies lateral and anterior one-third o nasal cavity; anastomoses with sphenopalatine artery (also known as nasopalatine artery; most common artery injured in septoplasty surgery, causing hematomas) Posterior ethmoid artery: supplies small portion o superior turbinate and posterior septum · Kiesselbach plexus (Little area) (a) Con uence o vessels along the anterior nasal septum where the septal branch o sphenopalatine artery, anterior ethmoidal artery branches, greater palatine artery, and septal branches o superior labial artery anastomose · Woodru plexus (naso-nasopharyngeal plexus) (a) Anastomosis o posterior nasal, posterior ethmoid, sphenopalatine, and ascending pharyngeal arteries along posterior lateral nasal wall in erior to the in erior turbinate Venous Drainage · Venous system is valveless. Lymphatic Drainage · Anterior portion o nose drains toward external nose in the subcutaneous tissue to the acial vein and submandibular nodes. Ol actory mucosa Lamina propria (d) Di erent cell types: Bipolar receptor cell Sustentacular cell Microvillar cell Cells lining Bowman gland Horizontal basal cell Globose basal cell · Unmyelinated axons rom ol actory receptor neurons orm myelinated ascicles which become ol actory la that passes through the oramina o cribri orm plate; each axon synapses in ol actory bulb. Four basic theories are: (a) Persistence o buccopharyngeal membrane (b) Abnormal persistence o bucconasal membrane (c) Abnormal mesoderm orming adhesions in nasochoanal region (d) Misdirection o neural crest cell migration 496 Pa rt 3: Rhinology · Bilateral choanal atresia usually presents with airway distress at birth since newborns are obligate nasal breathers; classic presentation is cyclic cyanosis relieved by crying (paradoxical cyanosis). Glioma · Comprised o ectopic glial tissue; 15% to 20% have intracranial connection. Cysts Rathke Pouch Cyst · Rathke pouch is an invagination o the nasopharyngeal epithelium in the posterior midline; the anterior pituitary gland develops rom this in etal li. T ornwaldt Cyst (ornwaldt Cyst) · Benign nasopharyngeal cyst · Develops rom remnant o notochord · Symptoms: postnasal drainage, aural ullness, serous otitis media, and cervical pain · Examination: smooth submucosal midline mass in nasopharynx · Treatment: none i asymptomatic; i symptomatic, marsupialization through surgical correction via endoscopic approach 498 Pa rt 3: Rhinology Intra-Adenoidal Cyst · Occlusion o adenoid crypts, leading to retention cyst in adenoids; asymptomatic; in midline; rhomboid shape on imaging Branchial Cle Cyst · Can be ormed by either the rst or second branchial arch · Relative lateral position in nasopharynx · reatment is surgical excision Allergic Rhinitis · Nasal symptoms: nasal congestion, rhinorrhea (anterior and posterior), nasal pruritus, palate pruritus, postnasal drainage, anosmia, or hyposmia · Ocular symptoms: ocular pruritus, watery eyes · Pathophysiology: (a) Gell and Coombs type I hypersensitivity. Upon subsequent exposure to the same antigen, these cells are stimulated to di erentiate into either more -helper cells or B cells.
Diagnosis: Laryngeal examination shows waxy lesions that may be gray or orange acne face chart discount 30 gm acticin, typically on the epiglottis acne quizlet best purchase for acticin, but sometimes glottic or subglottic skin care not tested on animals acticin 30 gm low price. Specimens should be processed with Congo red stain and viewed under polarized light to show apple green bire ringence skin care natural order acticin 30 gm mastercard. Blunt trauma to the larynx can cause laryngeal ractures without signi cant external signs acne 5dpo purchase acticin on line. Laryngeal ractures are not common, since the larynx is protected posteriorly by the spine, and anteriorly, the chin and sternum provide some shielding. Laryngeal ractures usually result rom a direct anterior blow with the head extended. Nearly hal o patients who sustain a laryngeal racture asphyxiate at the scene o the accident. In other cases, airway obstruction develops a er a airly asymptomatic interval, and can be suddenly atal. Proceed directly to operating room or tracheotomy with local anesthesia, ollowed by direct laryngoscopy under general anesthesia to assess the injury. Be prepared to per orm emergency tracheotomy en route should the airway be suddenly lost. Orotracheal intubation is not recommended, as laryngeal distortion makes this dif cult, and the tube may create a alse passage. Flexible laryngoscopy to assess vocal old motion and look or lacerations and exposed cartilage. I beroptic examination is normal, manage conservatively with observation, humidi cation, and steroids. I beroptic examination shows hematoma, swelling, decreased motion, or other distortion, per orm C scan. I examination shows lacerations or exposed cartilage, proceed directly to operating room or urgent tracheotomy under local, ollowed by direct laryngoscopy under general anesthesia. I an arytenoid cartilage is completely avulsed and displaced, it is better to remove it than attempt to reposition it. Laryngeal stents may be used to add stability, but can stimulate granulation tissue. Of ce endoscopy to evaluate supraglottic and glottic airway and vocal old motion iii. Direct laryngoscopy and bronchoscopy to determine extent o lesion and palpate immobile vocal olds E. I obstructive symptoms are present nearly always involves xation o the vocal olds due to posterior scarring, anterior stenosis usually a ects voice more than respiration. I vocal old mobility cannot be restored, then the airway can only be restored by static enlargement o the airway, which impairs the voice. Can be managed by endoscopic excision i the scar is thin and not circum erential, and the cricoid support is intact. Can per orm with or without radial incision and balloon dilation or rigid dilation c. Reconstructive surgery can be considered with either laryngotracheoplasty, or cricotracheal resection. Airway stenosis that involves multiple sites or that occurs in patients with complex medical conditions is very dif cult to treat. Expanding endotracheal stents are not advised, due to complications o granulation and potential erosion into the mediastinum. Pathophysiology: Supraglottis is accid, and epiglottis or interarytenoid tissue collapse during inspiration to obstruct the airway. However because o the current "Back to Sleep" initiative to prevent sudden in ant death syndrome, parents o en do not place child in supine position. Flexible endoscopy in the of ce: Epiglottis is classically described as "omega" shaped and alls backward during inspiration. Operative endoscopy is indicated i other anomalies are suspected or i stridor is very severe, with cyanosis. Proton pump inhibitor treatment can help temporize symptoms to avoid surgical procedure. Causes: idiopathic, birth trauma, cardiomegaly, Arnold-Chiari mal ormation, ligation o persistent ductus arteriosis ii. E ective or decreasing synkinetic inspiratory stridor, which can occur later in li. Direct laryngoscopy and bronchoscopy show compressible erythematous most o en involving the anterior subglottis. Observation: Natural history is expansion or several months ollowed by involution. Laryngeal atresia presents with complete obstruction at birth, unless a distal -E stula provides some connection rom trachea to outer air. Diagnosis and treatment are accomplished by endoscopy with rupture or marsupialization o the cyst. Recurrence is in requent, but subsequent endoscopy is required to monitor or such an occurrence. Presentation: stridor and respiratory ailure, usually a er attempts to extubate C. Laryngeal cle is a rare anomaly caused by incomplete usion o the laryngotracheal septum. There are multiple other accompanying anomalies including mental retardation, acial abnormalities, hypotonia, and strabismus. Choking on ood causes about 3000 deaths per year in the United States, predominantly between the ages o 1 and 3. In in ants less than 1 year o age, su ocation rom oreign body aspiration is the leading cause o accidental death. Presentation: Foreign bodies that do not cause obstruction present with wheezing or chronic cough. Fluoroscopy or inspiratory and expiratory lms show atelectasis on inspiration, hyperin ation on expiration on the side o the oreign body. Per orming a negative endoscopy is much better than neglecting an occult oreign body. Removal requires teamwork and communication, with all equipment available, assembled, and working. General anesthesia is required, with spontaneous ventilation, may be supplemented by topical anesthesia. Pulmonary insuf ciency that bene ts rom reduction o upper airway resistance and dead space v. It is best to intervene early rather than wait or late signs o upper airway obstruction. Secure tube tightly, pre erably with direct sutures, to prevent accidental dislodgement. Immediate: bleeding, pneumothorax, pneumomediastinum, subcutaneous emphysema, dislodged or obstructed tube, alse passage with tube outside trachea, postobstructive pulmonary edema, apnea due to loss o hypoxic drive, tube too short or inappropriate shape (especially in morbidly obese patients) ii. Delayed: granulation tissue, stomal in ection, subglottic or tracheal stenosis, tracheomalacia, tracheoesophageal stula, displacement o tube, tracheoinnominate stula, persisting tracheocutaneous stula a er decannulation Cha pter 44: the La rynx 799 Swallowing and Management o Dysphagia Stages o Swallowing A. Muscle is under tonic contracted to prevent air ingestion with inhalation and re ux rom esophagus ii. Signs and symptoms: coughing, choking, recurrent pneumonia, malnutrition, dehydration, weight loss, regurgitation, globus sensation, ood impaction B. Patient questionnaire indicating the severity o dysphagia and e ect on quality o li e b. Screening tool used to assess whether patient needs urther testing or is cleared or oral intake b. Uses trial with water and various consistencies monitoring outcomes o oxygen saturation or coughing to pass or ail patient c. Probes with graded pressure sensors placed in of ce and patient observed with numerous swallows b. Good or detection o penetration, aspiration, pooling, retained secretions, e ectiveness o cough d. Start with pharyngeal squeeze (high pitched strained phonation in rising crescendo) 2. Pre-swallow · Secretion level: assess amount and location o secretion prior to swallow · Can indicate patients who are at high risk or aspiration due to open glottis during bolus ormation and transit 4. Post swallow · Assess whether ood contents have penetrated larynx or i the patient aspirated the contents. Can use light touch with endoscope, presence o residue without patient attempt to clear or air pu s d. Assess all phases o swallowing and allows or visualization o structural movement c. Stimulation · Electrical stimulation (a) Percutaneous hook wire electrodes to target muscles (b) ranscutaneous stimulated sensory bers in skins and target muscles · T ermal tactile (a) Rubbing anterior tonsillar pillars with cold (b) Increases sensitivity minimizing pharyngeal delay ii. Pathophysiology: causes mechanical obstruction and can produce in ammation, which can cause associated neck and back sti ness and pain c. Symptoms: Solid ood dysphagia due to mechanical obstruction and aspiration o retained secretions post swallow d. Symptoms: intermittent dysphagia to solids, do not start until diameter < 13 mm b. Symptoms: regurgitation o ood, chest pain, cough, dysphagia to solids and liquids, heartburn, b. Esophageal motility disorder due to dys unction o inhibitory neurons o myenteric plexus 2. Pathophysiology: neuroinhibitory dys unction with normal peristaltic contractions with high amplitude contraction o esophageal smooth muscle c. Symptoms: dysphagia, regurgitation, halitosis, neck swelling, aspiration, gurgling a er eating, dysphonia b. Pathophysiology: pseudodiverticulum at Killian triangle between in erior constrictor and cricopharyngeus 1. Diverticulopexy open procedure with suturing intact diverticulum superiorly to prevertebral ascia to prevent entrance o ood 2. Killian Jamieson diverticulum is between in erior cricopharyngeus and esophagus viii. Pathophysiology: hypertrophy o muscle, inability to relax muscle due to neuromuscular disorder (muscular dystrophy, stroke, Parkinson, vagus nerve palsy), brosis rom radiation c. Esophagram or Video Oropharyngeal Swallow Study · Will show Cricopharyngeal bar · Can help identi y poor surgical candidates (a) Impaired pharyngeal strength (b) Impaired hyolaryngeal elevation Manometry tonic contraction o cricopharyngeus without relaxation d. Singers Formant or "Ring"-Resonance that allows singers to be heard over the orchestra vi. Baseline examination-including stroboscopy-per ormers may have asymptomatic nodules or other lesions, which could be "red herrings" i there is a subsequent voice disorder viii. Pro essional voice users have the same pathologies as nonpro essional voice patients, but a. Singing outside range Vocal Emergency: Sudden Voice Change Just Be ore Per ormance A. These are all short-term measures or an important limited per ormance that cannot or should not be canceled. Ideal management o laryngitis includes voice rest, as continued per ormance perpetuates the problem. Morphology and development o the human vocal tract: a study using magnetic resonance imaging. Advances in understanding the relationship between the skull base and larynx with comments on the origins o speech. Spontaneous laryngeal reinnervation a er recurrent laryngeal or vagus nerve injury. A patient with adductor spasmodic dysphonia will have the most di iculty with which o the ollowing words Between these arches are the grooves or cle s externally and the pouches internally. These nerves are anterior to their respective arteries, except in the h arch where the nerve is posterior to the artery. The sternocleidomastoid muscles are derived rom the cervical somites posterior and in erior to the above arches. During the course o embryonic development, the rst and second arch arteries degenerate. The second arch artery has an upper branch that passes through a mass o mesoderm, which later chondries and ossi es as the stapes. The third arch artery is the precursor o the carotid artery in both le and right sides. The rest o the right subclavian and the le subclavian are derivatives o the seventh segmental arteries. Hence when it arises too ar rom the le, an anterior compression o the trachea results (anomalous innominate). As the connection on the right side between the h arch artery (pulmonary) and the dorsal aorta degenerates, the nerve (recurrent laryngeal nerve) loops around the ourth arch artery, which subsequently becomes the subclavian. Ventral wing Each pouch Dorsal wing Ventral wing and accessory wing Dorsal wing Dorsal Ventral Middle ear cavity Dorsal onsillar ossa and palatine tonsil Ventral Dorsal Parathyroid 3 Fourth pouch First pouch Second pouch B. During embryonic development the thymus descends caudally, pulling with it parathyroid 3. The ultimobranchial body becomes in ltrated by cells o neural crest origin, giving rise to the inter ollicular cells o the thyroid gland. As these "out-pocketing" pouches develop into glandular elements, their connections with the pharyngeal lumen, re erred to as pharyngobranchial ducts, become obliterated.
Acticin 30 gm buy with visa. HOW TO: CREATE YOUR OWN SKINCARE PRODUCTS! (MixNature Review).
References
- Wilensky GR. Cost-effectiveness information: yes, it's important, but keep it separate, please! Ann Intern Med 2008;148(12):967-968.
- Schaffner A. Therapeutic concentrations of glucocorticoids suppress the antimicrobial activity of human macrophages without impairing their responsiveness to gamma interferon. J Clin Invest. 1985;76:1755-1764.
- Griepp RB: Panel discussion: Session IIóaortic arch, Ann Thorac Surg 83:S824, 2007.
- Kumral E, Evyapan D, Keser G, et al. Detection of microembolic signals in patients with neuropsychiatric lupus erythematosus. Eur Neurol 2002;47:131-5.
- Skinner J, Weinstein JN, Sporer SM, Wennberg JE. Racial, ethnic, and geographic disparities in rates of knee arthroplasty among Medicare patients. N Engl J Med 2003; 349(14):1350-9.