
Asacol
| Contato
Página Inicial
Feroze Mahmood, MD
- Director of Vascular Anesthesia and Perioperative Echocardiography
- Department of Anesthesia and Critical Care
- Beth Israel Deaconess Medical Center
- Boston, Massachusetts
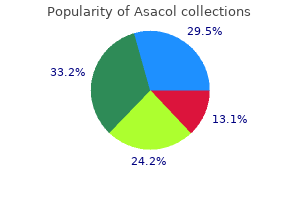
What does hypercalcemia do to neuronal membrane potential treatment of strep throat asacol 400 mg on-line, and why does that effect depress neuromuscular excitability Calcium homeostasis follows the principle of mass balance: Total body calcium = intake - output 1 treatment 6th feb purchase asacol online. In the plasma symptoms detached retina buy 400 mg asacol fast delivery, nearly half the Ca 2+ is bound to plasma proteins and other molecules medicine lake asacol 400 mg for sale. In addition symptoms toxic shock syndrome asacol 800 mg purchase fast delivery, Ca2+ is concentrated inside mitochondria and the sarcoplasmic reticulum. Electrochemical gradients favor movement of Ca2+ into the cytosol when Ca2+ channels open. Bone is the largest Ca2+ reservoir in the body, with most bone Ca2+ in the form of hydroxyapatite crystals. Bone Ca2+ forms a reservoir that can be tapped to maintain plasma Ca2+ homeostasis. Usually only a small fraction of bone Ca2+ is ionized and readily exchangeable, and this pool remains in equilibrium with Ca2+ in the interstitial fluid. Only about one-third of ingested Ca2+ is absorbed, and unlike organic nutrients, Ca2+ absorption is hormonally regulated. Many people do not eat enough Ca2+containing foods, however, and intake may not match output. Intestinal calcium absorption is apparently both transcellular and paracellular (between the cells). Once inside the cell, Ca2+ binds to a protein called calbindin that helps keep free intracellular [Ca2+] low. This is necessary because of the role of free Ca2+ as an intracellular signal molecule. Of these, parathyroid hormone and calcitriol are the most important in adult humans. The parathyroid glands, which secrete parathyroid hormone para-, alongside of, were discovered in the 1890s by physiologists studying the role of the thyroid gland. These scientists noticed that if they removed all of the thyroid gland from dogs and cats, the animals died in a few days. In contrast, rabbits died only if the little parathyroid "glandules" alongside the thyroid were removed. The scientists then looked for parathyroid glands in dogs and cats and found them tucked away behind the larger thyroid gland. If the parathyroid glands were left behind when the thyroid was surgically removed, the animals lived. The scientists concluded that the parathyroid glands contained a substance that was essential for life, although the thyroid gland did not. The absence of parathyroid hormones causes hypocalcemic tetany and respiratory paralysis, as mentioned in the section on functions of calcium. Parathyroid hormone raises plasma Ca2+ in three ways: Parathyroid hormone Four small parathyroid glands lie on the Calcium Balance 771 fiG. Increased bone resorption by osteoclasts takes about 12 hours to become measurable. These paracrine factors are receiving intense scrutiny as potential pharmacological agents. As we mentioned previously, regulated Ca2+ reabsorption takes place in the distal nephron. If the concentrations exceed that level, calcium phosphate crystals form and precipitate out of solution. High concentrations of calcium phosphate in the urine are one cause of kidney stones. The body makes calcitriol from vitamin D that has been obtained through diet or made in the skin by the action of sunlight on precursors made from acetyl CoA. People who live above 37 degrees of latitude north or below 37 degrees south do not get enough sunlight to make adequate vitamin D except in the summer, and they should consider taking vitamin supplements. Vitamin D is modified in two steps-first in the liver, then in the kidneys-to make vitamin D3 or calcitriol. Calcitriol is the primary hormone responsible for enhancing Ca2+ uptake from the small intestine. In addition, calcitriol facilitates renal reabsorption of Ca2+ and helps mobilize Ca2+ out of bone. This action ensures maximal absorption of Ca2+ from the diet at a time when metabolic demands for calcium are high. Experiments in animals have shown that calcitonin decreases bone resorption and increases renal calcium excretion. Calcitonin apparently plays only a minor role in daily calcium balance in adult humans. Patients whose thyroid glands have been removed show no disturbance in calcium balance, and people with thyroid tumors that secrete large amounts of calcitonin also show no ill effects. However, phosphates have other significant physiological roles, including energy transfer and storage in highenergy phosphate bonds, and activation or deactivation of enzymes, transporters, and ion channels through phosphorylation and dephosphorylation. Enhances kidney excretion Signal transduction pathways appear to vary during cell cycle Experimentally decreases plasma Ca2+ but has little apparent physiological effect in adult humans. Osteoporosis Is a Disease of Bone Loss One of the best-known pathologies of bone function is osteoporosis, a metabolic disorder in which bone resorption exceeds bone deposition. Most bone resorption takes place in spongy trabecular bone, particularly in the vertebrae, hips, and wrists. Osteoporosis is most common in women after menopause, when estrogen concentrations fall. Bone loss and small fractures and compression in the spinal column lead to kyphosis hump-back, the stooped, hunchback appearance that is characteristic of advanced osteoporosis in the elderly. Risk factors include small, thin body type; postmenopausal age; smoking; and low dietary Ca2+ intake. The most effective drugs for preventing or treating osteoporosis act more directly on bone metabolism. Currently clinical studies are investigating whether some combination of bisphosphonates and teriparatide is more effective in combating osteoporosis than either drug alone. To avoid osteoporosis in later years, young women need to maintain adequate dietary calcium intake and perform weightbearing exercises, such as running or aerobics, which increase bone density. Loss of bone mass begins by age 30, long before people think they are at risk, and many women suffer from low bone mass (osteopenia) before they are aware of a problem. He goes on a low-calcium diet, avoiding milk, cheese, and other dairy products, but several months later he returns to the emergency room with another painful kidney stone. Spinks sends him to an endocrinologist, who recommends surgical removal of the overactive parathyroid glands. He must have his plasma Ca2+ levels checked regularly for the rest of his life to ensure Question Q1: What role does Ca2+ play in the normal functioning of muscles and neurons Integration and Analysis Muscle weakness in hyperparathyroidism is the opposite of what you would predict from knowing the role of Ca2+ in muscles and neurons. Hypercalcemia Q2: What is the technical term for "elevated levels of calcium in the blood" Filtration at the glomerulus is a selective process that excludes blood cells and most plasma proteins [p. A significant amount of plasma Ca2+ is bound to plasma proteins and therefore cannot filter. Each hormone has stimuli that initiate its secretion, and feedback signals that modulate its release. Molecular interactions and communication across membranes are also essential to hormone activity. In many instances, such as calcium and phosphate homeostasis, the principle of mass balance is the focus of homeostatic regulation. Cortisol is a typical steroid hormone in its synthesis, secretion, transport, and action. It promotes gluconeogenesis, breakdown of skeletal muscle proteins and adipose tissue, Ca2+ excretion, and suppression of the immune system. Basic components of endocrine pathways include hormone receptors, feedback loops, and cellular responses. Hypercortisolism usually results from a tumor or therapeutic administration of the hormone. The thyroid follicle has a hollow center filled with colloid containing thyroglobulin and enzymes. Tetraiodothyronine (thyroxine, T4) is converted in target tissues to the more active hormone triiodothyronine (T3). Thyroid hormones are not essential for life, but they influence metabolic rate as well as protein, carbohydrate, and fat metabolism. Long bone growth occurs at epiphyseal plates, where chondrocytes produce cartilage. Calcium acts as an intracellular signal for second messenger pathways, exocytosis, and muscle contraction. Calcitonin from the thyroid gland plays only a minor role in daily calcium balance in adult humans. Normal growth requires growth hormone, thyroid hormones, insulin, and sex hormones at puberty. The adrenal cortex secretes hormones, and the adrenal medulla secretes hormones. For (a) cortisol, (b) growth hormone, (c) parathyroid hormone, and (d) T3 and T4: Draw the full control pathway and show feedback where appropriate. Make a table showing the effects of cortisol, thyroid hormones, growth hormone, insulin, and glucagon on protein, carbohydrate, and lipid metabolism. Explain why the deficiency of parathyroid hormone causes hypocalcemic tetany and respiratory paralysis. Draw an osteoclast and diagram this process, including enzymes and the appropriate transporters on each membrane. How many different transporters can you think of that could be used to reabsorb bicarbonate Boston is located at 42 degrees north latitude, and weak sunlight in winter there does not allow skin synthesis of vitamin D. A lady with a history of smoking and a poor appetite fractures her hand and leg as the result of a fall. As part of the treatment, a doctor initiates a therapy that includes bisphosphonate and teriparatide. One diagnostic test to determine the cause of hypercortisolism is a dexamethasone suppression test. The following table shows the results from two patients given a dexamethasone suppression test. Plasma Cortisol Concentration Patient A Patient B Before Test High High After Test High Low 20 10 0 1829 3039 4049 50+ Age (years) 15. When blood test results came back last week, someone in the office spilled a cup of coffee on them, smearing the patient names and some of the numbers. Your tentative diagnoses, based on physical findings and symptoms, for those three patients are: Mr. The following graph shows the results of a study done in Boston that compared blood vitamin D levels during summer and winter. On graph A, plot the effect of plasma parathyroid hormone concentration on plasma Ca2+ concentration. On graph B, plot the effect of plasma Ca2+ concentration on plasma parathyroid hormone concentration. Although, at first sight, the immune system may appear to be autonomous, it is connected by innumerable structural and functional bridges with the nervous system and the endocrine system, so as to constitute a multisystem. Cell infected with poxvirus (650x) 777 778 chaPter 24 the Immune System " aughter is the best medicine. But even as our list of immune cytokines grows, scientists are coming to recognize that the immune system is only one part of a complex communication network that includes the nervous and endocrine systems. The brain-immune connection has even been given its own name: psychoneuroimmunology. The connections between the immune system and other body systems are becoming more important in our understanding of physiology. For example, we have learned that bacteria are not always harmful, and that the symbiotic bacteria permitted by our immune system to live inside our gut play an important role in metabolism. Inflammation created by the immune system is a factor in many disease states, including atherosclerosis [p. And on the flip side, the brain can assist or derail the immune system, depending on our psychological state. Together specif icity and memory in immune cells enable the body to distinguish normal from abnormal and to mount a targeted response. The human immune system consists of the lymphoid tissues of the body, the immune cells, and chemicals (both intracellular and secreted) that coordinate and execute immune functions. Most immune functions depend heavily on cell-to-cell communication, particularly local communication by cytokines and contact-dependent signaling that relies on cells binding to surface receptors on other cells [p. It tries to recognize and remove abnormal "self " cells created when normal cell growth and development go wrong. For example, the diseases we call cancer result from abnormal cells that multiply uncontrollably, crowding out normal cells and disrupting function.
Duct branches are present in the interlobar treatment spinal stenosis asacol 400 mg buy on line, interlobular symptoms 2dp5dt 400 mg asacol buy amex, and intralobular connective tissue septa as interlobar ducts 300 medications for nclex generic asacol 400 mg with visa, interlobular ducts medicine world asacol 400 mg on line, and intercalated/striated ducts connected to the secretory units (acini) medicine tour purchase asacol 800 mg mastercard. A gland with a secretory unit with a rounded form is called simple acinar or alveolar gland. The acini and alveoli of the salivary glands and the mammary glands contain contractile basket-like myoepithelial cells. The acinar cellular organization can be part of the wall of short tubular ducts and also form their endings. The gland is then called branched tubuloacinar gland (for example, mammary gland). Mixed glands contain both mucous and serous cells, the latter forming a crescentic or half-moonshaped region (serous demilunes) capping the acini. A gland in which the apical region of a cell is pinched off and released into the lumen is called apocrine gland (an example is the mammary gland). When the whole cell is released and is part of the secretion, the gland is called holocrine gland (such as the sebaceous glands of the skin). Intracellular membranes, called cytomembranes, separate diverse cellular processes into compartments. Multicellular glands form the parenchyma of organs such as the pancreas and the prostate. Larger glands have a branched duct system and are called branched or compound glands. Branched glands are surrounded by a connective tissue capsule that Essential concepts 85 reticulum and Golgi apparatus. The nucleus, mitochondria, lysosomes, and peroxisomes are bound by cytomembranes and are called organelles. The nucleus and mitochondria are surrounded by a double membrane; lysosomes and peroxisomes are surrounded by a single membrane. Phospholipids (phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine and sphingomyelin) form a bilayer consisting of outer and inner leaflets. Phosphatidylinositol is another phospholipid, with an important role in cell signaling, localized to the inner leaflet of the plasma membrane. Cholesterol is inserted into the phospholipid bilayer and modulates membrane fluidity. Integral membrane proteins are transmembrane proteins spanning the lipid bilayer through -helical regions. Peripheral membrane proteins are indirectly linked to the plasma membrane by protein-protein interactions. Peripheral membrane proteins exposed to the cytosol interact with cytoskeletal components. The extracellular portion of integral and peripheral membrane proteins is generally glycosylated. A frozen and fractured specimen is used to produce a thin metal replica of the two surfaces of a membrane and its two artificial faces. The lipid bilayer membranes are frozen at liquid nitrogen temperature (196oC) and "split" along the middle of the hydrophobic core. As a result, two complementary halves of a membrane are produced and the hydrophobic face exposed. Gases (such as oxygen and carbon dioxide) can cross membranes by passive diffusion. Glucose, electrically charged molecules, and small ions require transport proteins and channel proteins for facilitated diffusion across a membrane. Channel proteins can be ligand-gated channels (gates which open upon ligand binding) or voltage-gated channels (which open in response to changes in electrical potential across the membrane). The lumen of cisternae, tubules, and vesicles is continuous with the extracellular space. The membranous wall separates the luminal compartment from the cytosolic compartment. Products released into the lumen of the endoplasmic reticulum are transported to the Golgi apparatus by transporting vesicles and eventually to the cell exterior by exocytosis. Imagine that there is a continuum in this secretory sequence and that all the luminal spaces are virtually interconnected and continuous with the cell exterior. The freeze-fracture technique takes advantage of this virtual arrangement if you consider that the membrane splitting knife can jump from the exocytoplasmic leaflet of a membranebound vesicle to the exocytoplasmic leaflet of the plasma membrane exposed to the environment. The rough endoplasmic reticulum participates in protein synthesis and transport to the Golgi apparatus. The smooth endoplasmic reticulum has a significant role in cell detoxification reactions required for converting harmful lipid-soluble substances into water-insoluble material. The smooth endoplasmic reticulum is generally adjacent to glycogen deposits and lipid droplets (nonmembrane-bound inclusions). Proteins targeted to the nucleus, mitochondria, or peroxisomes and cytoskeletal proteins are synthesized on free ribosomes (polyribosomes) and released in the cytosol. It consists of four compartments: (1) A cis-Golgi, the receiving site from the endoplasmic reticulum. Golgins, a family of coiled-coil proteins, stabilize the flattened stacks of sacs of the Golgi apparatus. Golgi-derived products can be released from the cell by exocytosis or sorted to lysosomes. Certain classes of Golgi-derived cargos are stored into secretory granules and released by exocytosis under control of a chemical or electrical signal. The sorting mechanism of lysosomes involves two steps: (1) the insertion of mannose-6-phosphate (M6P) into glycoproteins destined to lysosomes. This mechanism separates M6P-containing lysosomal enzymes from other glycoproteins. Two types of lysosomes are recognized: (1) Primary lysosomes (inactive), the primary storage of lysosomal enzymes. Lysosomes target internalized extracellular material for degradation through the activity of lysosomal hydrolytic enzymes operating at an acidic pH (5. There are three major pathways involved in intracellular degradation of materials: (1) Phagocytosis (the pagocytosed material is enclosed within a phagosome that fuses with a lysosome to form a phagolysosome). Lysosomal storage disorders occur when hereditary deficiency in lysosomal enzymes prevents the normal breakdown of cell components that accumulate progressively in cells. Endocytosis involves the internalization of virus or bacteria by phagocytosis using clathrin-independent vesicles and the uptake of small macromolecules utilizing clathin-coated vesicles. The ligand-receptor complex is internalized by the process of receptor-mediated endocytosis. This process involves: (1) the formation of a clathrin-coated pit (to concentrate ligand-receptor complexes in a small surface area). High levels of cholesterol in blood plasma result in the formation of atheromas in the intima of blood vessels. The outer mitochondrial membrane is separated by an intermembrane space from the inner mitochondrial membrane. Mitochondria participate in apoptosis (programmed cell death), steroidogenesis, and thermogenesis in brown fat. Both males and females can be affected by mitochondrial disease, but males never transmit the disorder. Peroxisomes contain crystaloid cores containing oxidases and catalases, enzymes that oxidize organic compounds and decompose hydrogen peroxide into water. Peroxisomes are involved in the synthesis of bile acids and biosynthesis of lipids. Peroxisome biogenesis involve two pathways: (1) De novo generation pathway, consisting in pre-peroxisomal vesicles budding off from the endoplasmic reticulum and fusing to form mature peroxisomes. Peroxisomes contain peroxins, receptor proteins shuttling between the cytosol and the peroxisome, matrix proteins, and peroxisomal membrane proteins. Peroxins bind to the peroxisome targeting signal of the matrix proteins to be imported across transporting pores or channels. In fact, peroxisomal membrane proteins build the pores serving as transporting gates for proteins that need to gain access inside the peroxisome. Zellweger syndrome, a severe and fatal cerebrohepatorenal disorder, is determined by the failure of peroxisomal enzymes to be imported from the cytosol into the peroxisome. Deficient peroxisomal assembly in hepatocytes is associated with fibrosis and cirrhosis. Cell Signaling Cells respond to extracellular signals produced by other cells or by themselves. This mechanism, called cell signaling, allows cell-cell communication and is necessary for the functional regulation and integration of multicellular organisms. Our discussion in this chapter not only provides the basis for understanding cell signaling pathways but serves also as an introduction to General Pathology, including aging, cell senescence and neoplasia and the role of cell injury in human disease, including necrosis, apoptosis and necroptosis and the mechanisms of autophagy, ubiquitin-proteasome proteolysis and mitophagy. Signaling molecules can transmit information by acting as ligands binding to receptors expressed by their target cells. Some signaling molecules can act on the cell surface after binding to cell surface receptors; others can cross the plasma membrane and bind to intracellular receptors in the cytoplasm and nucleus. An understanding of the molecular aspects of cell signaling is clinically relevant to uncover potential targets of novel therapeutics for the treatment of metabolic dysfunctions and diseases. Types of cell signaling and feedback action cells of the immune system to foreign antigens or growth factors that trigger their own proliferation and differentiation. Endocrine cell signaling involves a signaling molecule, a hormone, secreted by an endocrine cell and transported through the circulation to act on distant target cells. An example is the steroid hormone testosterone produced in the testes, that stimulates the development and maintenance of the male reproductive tract using the vascular route. Neuroendocrine cell signaling is a specific form of endocrine signaling involving a product secreted by a nerve cell into the bloodstream and acting on distant cells. Paracrine cell signaling is mediated by a molecule acting locally to regulate the behavior of a nearby cell. Neurotransmitter or synaptic cell signaling is a specialized form of paracrine signaling. Neurons secrete neurotransmitters that diffuse short distances and bind to receptors on target cells. It requires the contact of proteins of adjacent plasma membranes for signaling to occur. Autocrine cell signaling is defined by cells responding to signaling molecules that they themselves produce. A classic example is the response of Binding of a hormone or ligand to its receptor initiates a cascade of intracellular reactions (called signal transduction) to regulate critical functions such as embryonic and fetal development, cell proliferation and differentiation, movement, metabolism, and behavior. Steroid hormones are synthesized from cholesterol and include testosterone, estrogen, progesterone and corticosteroids. Steroid hormones are usually secreted as they are synthesized and are transported in the bloodstream bound to protein carriers. Testosterone, estrogen, and progesterone are sex steroids and are produced predominantly by the gonads. Signaling mechanisms Hormone secreted into the blood Endocrine gland Blood vessel Membrane receptor Endocrine signaling Cytosol receptor Endocrine cells secrete a polypeptide or steroid hormone into a blood vessel. The hormone is then carried to a target cell, which may be located at a considerable distance from the secreting cell. An example of a polypeptide hormone is thyrotrophic hormone, secreted by the hypophysis and acting on the thyroid gland. An example of a steroid hormone is estradiol, produced by the ovaries and acting on the endometrium. Neuroendocrine signaling Hormone In response to a neural signal, neuroendocrine cells secrete a hormone into the blood to travel to a target organ. Blood vessel Neuroendocrine cell Hormone or growth factor secreted into the extracellular space Distant target cell Paracrine signaling Paracrine cells secrete hormones or growth factors that act on an adjacent cell. Examples are glucagon and somatostatin acting on adjacent cells of the islets of Langerhans that secrete insulin. A ligand secreted by one cell binds to the receptor of the other cell to trigger a response. Distant target cell Stimulus from axon terminal Adjacent target cell Membrane receptor Synapse Adjacent target cell Cytokine Autocrine signaling Some hormones, growth factors and cytokines can act on the originating cell and exert an autocrine control. Although genetically male, the individual develops the secondary sexual characteristics of a female. We discuss their functional roles in Chapter 20, Spermatogenesis, and Chapter 22, Follicle Development and the Menstrual Cycle. Corticosteroids are synthesized in the cortex of the adrenal gland and include two major classes: glucocorticoids, which stimulate the production of Box 3-A Steroid hormones · They derive from cholesterol. Positive and negative feedback Feedback loops Hypothalamus Various feedback loops coordinate the secretion of Positive hormones. For example, a feedback negative feedback loop prevents the unregulated release Hypophysis of a hormone from the hypophysis into the blood circulation when the target cell or tissue may be nonresponsive. A positive feedback loop occurs when the hypophysis senses a decrease in the blood Target cells levels of a hormone produced by the target cell or tissue. The synthetic pathway of thyroid hormones and some of their actions are presented in Chapter 19, Endocrine System. Peptide hormones and growth factors Negative feedback glucose, and mineralocorticoids, which act on the kidneys to regulate water and salt balance. We address structural and functional aspects of corticosteroids in Chapter 19, Endocrine System.
Although bone fractures are a common characteristic in patients with osteomalacia and osteoporosis medicine 4839 discount generic asacol uk, note that there is defective osteogenesis in osteomalacia in contrast to bone weakening of a previous normal osteogenesis process in patients with osteoporosis symptoms xanax addiction buy asacol 400 mg low cost. Essential concepts Connective Tissue An extension of the adult connective tissue classification is based on which fibers predominate medicine 4 the people buy asacol now. Elastic connective tissue symptoms 8 days past ovulation buy asacol 800 mg online, found in the form of sheets or laminae in the wall of the aorta treatment xanthelasma eyelid 800 mg asacol order overnight delivery, is rich in elastic fibers. The fibroblast synthesizes the precursor molecules of various types of collagens and elastin and proteoglycans. Procollagen, the initial collagen precursor which contains hydroxyproline and hydroxylysine, is secreted by fibroblasts in the form of a triple helix flanked by nonhelical domains. Procollagen peptidase cleaves the nonhelical domains and procollagen becomes tropocollagen. Tropocollagen molecules self-assemble in a staggered array in the presence of lysyl oxidase to form a cross-banded collagen fibril. Osteoblasts, chondroblasts, odontoblasts and smooth muscle cells can also synthesize collagens. Defects in the processing of procollagen and tropocollagen and the assembly of collagen fibrils give rise to variations of the Ehlers-Danlos syndrome, characterized by hyperelasticity of the skin and hypermobility of the joints. Elastin, the precursor of elastic fibers, is also synthesized and processed sequentially. Fibroblasts or smooth muscle cells secrete desmosine- and isodesmosine-containing proelastin, which is partially cleaved to give rise to tropoelastin. Tropoelastin, fibrillins and fibulin 1 assemble into elastic fibers that aggregate to form bundles of elastic fibers. A defect in fibrillin 1 affects the assembly of mature elastic fibers, a characteristic of Marfan syndrome. Their function in connective tissue is the turnover of fibers and extracellular matrix and, most important, the presentation of antigens to lymphocytes as an essential step of immune and inflammatory reactions. Mast cells acquire metachromatic granules · Connective tissue provides support, or stroma, to the functional component, or parenchyma, of tissues. The functions of connective tissue include the storage of metabolites, immune and inflammatory responses and tissue repair after injury. Connective tissue consists of thee basic components: cells, fibers and extracellular matrix (called ground substance). The proportion of these three components contributes to the classification of connective tissue. Connective tissue can be classified into three major groups: (1) Embryonic connective tissue. The embryonic connective tissue, or mesenchyme, consists predominantly of extracellular matrix. The adult connective tissue can be subclassified as: (1) Loose or areolar connective tissue (more cells than fibers, found in the mesentery or lamina propria of mucosae). The latter is subdivided into two categories: · Dense irregular connective tissue (with a random orientation of collagen bundles, found in the dermis of the skin). Finally, tumor cells can produce chemokine molecules on their surface that facilitate their transendothelial migration to metastasize. There are two types of adipose tissue: (1) White fat, the major reserve of long-term energy. Mesenchymal stem cells give rise to white fat preadipocytes and common myoblast/ brown fat preadipocyte precursors. White fat can transdifferentiate into brown fat-like adipocytes following cold exposure and -adrenergic signaling. Lipoprotein lipase is transferred to endothelial cells in the adjacent blood vessels to enable the passage of fatty acids and triglycerides into the adipocytes. Fat can accumulate in a single lipid-strorage droplet (unilocular) or multiple small lipid droplets (multilocular). The granules contain vasoactive mediators (histamine, heparin, and chemotactic mediators), chymases and other proteases. Leukotrienes are vasoactive agents not present in granules; they are metabolites of the plasma membraneassociated arachidonic acid. Like most vasoactive agents, they induce an increase in vascular permeability leading to edema. Mast cells and basophils circulating in blood derive from the same progenitor in the bone marrow. Mast cells play a role in allergic hypersensitivity reactions associated with asthma, hay fever, and eczema. Three characteristics define the structure of a plasma cell: a well-developed rough endoplasmic reticulum, an extensive Golgi apparatus, and a prominent nucleolus. These features define the plasma cell as an actively protein-producing cell, whose main product are immunoglobulins. The extracellular matrix is a combination of collagens, noncollagenous glycoproteins, and proteoglycans. Each proteoglycan consists of a core protein attached to a linear hyaluronan molecule by a linker protein. Attached to the core protein are numerous glycosaminoglycan chains (keratan sulfate, dermatan sulfate and chondroitin sulfate). Malignant cells originated in a lining epithelium (carcinoma) or a glandular epithelium (adenocarcinoma) can break down the basement membrane and invade the underlying connective tissue. The histologic sequence of epithelial tumor invasion starts with dysplasia (increased cell proliferation and incomplete cell maturation), followed by carcinoma in situ (loss of epithelial normal organization within the limits of the basement membrane), microinvasive carcinoma (decreased expression of cadherins and breakdown of the basement membrane) and invasive carcinoma. Cessation in the expression of cadherins weakens the cohesive nature of the epithelial tumor. The production of proteinases allows the tumor cells to invade and attach to components of the connective tissue. Then, tumor cells produce autocrine motility factors, to enable tumor cell motility; vascular permeability Essential concepts 157 deposits can increase by inhibition of lipase activity (antilipolytic effect) determined by insulin and prostaglandins. Phosphorylated perilipin changes its conformation and enables lipolysis by lipases. Leptin, a peptide produced by adipocytes, regulates appetite, energy balance, and feeding. Leptin-deficient mice are obese and infertile, conditions that are reversible when leptin is administered to the mutants. Like a typical connective tissue member, cartilage consists of cells, fibers, and extracellular matrix. Cartilage lacks blood vessels and is surrounded by the perichondrium (except in fibrocartilage and articular hyaline cartilage, which lack a perichondrium). The perichondrium consists of two layers: an outermost fibrous layer, consisting of elongated fibroblastlike cells and blood vessels, and the innermost chondrogenic cell layer. Chondrogenesis (cartilage growth) takes place by two mechanisms: (1) Interstitial growth (within the cartilage). During interstitial growth, centers of chondrogenesis, consisting of chondroblasts located in lacunae and surrounded by a territorial matrix, divide by mitosis without leaving the lacunae and form isogenous groups. During appositional growth, the cells of the perichondrial chondrogenic layer differentiate into chondroblasts following activation of the gene encoding the transcription factor Sox9. A lack of Sox9 gene expression causes campomelic dysplasia characterized by bowing and angulation of long bones, hypoplasia of the pelvis and scapula, and abnormalities of the vertebral column. Macroscopically, a mature long bone consists of a shaft or diaphysis, and two epiphyses at the endings of the diaphysis. During bone growth, a cartilaginous growth plate is present at the epiphysismetaphysis interface. The diaphysis is surrounded by a cylinder of compact bone housing the bone marrow. The epiphyses consist of spongy or cancellous bone covered by a thin layer of compact bone. The periosteum covers the outer surface of the bone (except the articular surfaces and the tendon and ligament insertion sites). Microscopically, there is: (1) Lamellar bone, with a regular alignment of collagen fibers, typical of mature bone. Blood vessels are present in the central canal, which is surrounded by concentric lamellae. Each lamella contains lacunae and radiating canaliculi occupied by osteocytes and their cell processes. Osteoblasts synthesize type I collagen, noncollagenous proteins, and proteoglycans. These are the components of the bone matrix or osteoid deposited during bone formation. In mature bone, the bone matrix consists of about 35% organic components and about 65% inorganic components (calcium phosphate with the crystalline characteristics of hydroxyapatite). Osteopontin contributes to the development of the sealing zone during osteoclast bone resorption activity. Under the influence of the transcription factor Sox9, mesenchymal stem cells give rise to preosteoblasts, the mitoticallyactive osteoprogenitor cells expressing the transcription factor Runx2. Preosteoblasts differentiate into postmitotic osteoblasts expressing the transcription factors Runx2 and Osterix (Osx). Note that the osteoblast differentiation process requires the participation of three transcription factors: Sox9, Runx2, and Osx. Runx2-deficient mice have a skeleton consisting of cartilage and lack osteoclasts. In humans, cleidocranial dysplasia, characterized by hypoplastic clavicles and delayed ossification of sutures of certain skull bones, is associated with defective expression of the Runx2 gene. The function of osteoclasts is regulated by calcitonin, produced by C cells located in the thyroid gland. The free domain has a sealing zone, a tight belt consisting of v 3 integrin with its intracellular domain linked to F-actin and the extracellular domain attached to osteopontin on the bone surface. The osteoclast is a multinucleated cell resulting from the fusion of several monocytes during osteoclastogenesis. You should be aware that the bone marrow contains megakaryocytes that may be confused with the osteoclasts. Osteoclasts are intimately associated to bone and are multinucleated; megakaryocytes are surrounded by hematopoietic cells and their nucleus is multilobed. Bone removal occurs in two phases: First, the mineral component is mobilized in an acidic environment (~pH 4. Because of the significant H+ transport, a parallel bicarbonate-chloride ion transport mechanism is required to maintain intracellular electroneutrality. The osteoclast precursor is a member of the monocyte-macrophage lineage present in the adjacent bone marrow. Osteoblasts recruit monocytes and differentiate them into osteoclasts, the cell in charge of bone remodeling and mobilization of calcium. Osteoclastogenesis consists of several phases under strict control by the osteoblast. Osteoporosis is the loss of bone mass leading to bone fragility and susceptibility to fractures. The major factor in osteoporosis is the deficiency of the sex steroid estrogen that occurs in postmenopausal women. Osteopetrosis is a clinical syndrome caused by a failure of osteoclasts to remodel bone. Osteomalacia is characterized by a progressive softening and bending of the bones. Softening occurs because of a defect in the mineralization of the osteoid due to lack of vitamin D or renal tubular dysfunction. Osteogenesis Bone, including associated ligaments, tendons and articular cartilage, withstand the forces of compression, tension and shear stress. The two processes of bone formationosteogenesis or ossificationobserved in the embryo are: (1) intramembranous ossification, in which bone tissue is laid down directly in embryonic connective tissue or mesenchyme, and (2) endochondral ossification, in which bone tissue replaces a preexisting hyaline cartilage, the templateor anlageof the future bone. In addition to a description of the two major processes of ossification, this chapter addresses pathologic conditions, such as the sequence of bone fracture healing, metabolic and hereditary disorders and rheumatoid arthritis, within an integrated histologic and clinical context. Intramembranous ossification the mechanism of bone formation during intramembranous and endochondral ossification is essentially the same: A primary trabecular network, called primary spongiosa, is first laid down and then transformed into mature bone. But there is a difference in the nature of the template that becomes bone: a mesenchymal template is the starting point of intramembranous ossification, in contrast to a cartilage template of endochondral ossification. Intramembranous ossification 1 Mesenchymal cells aggregate without a cartilage intermediate. This process is controlled by patterning signals from polypeptides of the Wnt, hedgehog, fibroblast growth factor, and transforming growth factor families. Osteocytes within the core of the blastema are interconnected by cell processes forming a functional syncytium. Later, Ca2+, transported by blood vessels, is used in the mineralization process and primary bone tissue is formed. Mesenchyme Patterning signals 1 Bone blastema Primary bone tissue Ca2+ 3 2 Osteocyte Blood vessel Mesenchymal cell Bone matrix (osteoid) Osteoblast Osteoclast Mineralization Blood vessels Organization of a primary ossification center Multiple individual trabeculae enlarge by appositional growth and eventually fuse together as a primary ossification center organized during the first stage of intramembranous ossification. Although primary bone tissue formation begins as an interstitial process, it soon becomes appositional. At the surface of the osteoid, osteoblasts continue the appositional deposit of matrix, mainly type I collagen and noncollagenous proteins. Intramembranous ossification the mesenchymal cells located near the surface condense to form the periosteum 1 Blood vessel 2 the continued deposition of bone on trabecular surfaces determines the occlusion of the intertrabecular spaces, and compact bone is formed. In other areas, the thickening of the trabeculae does not occur and the connective tissue in the intertrabecular space differentiates into hematopoietic tissue. Intramembranous ossification Monolayer of osteoblasts 3 Blood vessel the frontal and parietal bones and parts of the occipital, temporal, mandible, and maxilla bones develop by intramembranous ossification. Intramembranous ossification requires: 1 A well-vascularized primitive connective tissue. Osteoblasts organize thin trabeculae of woven bone, forming an irregular network called primary spongiosa.
Syndromes
- Benzene
- Barium enema
- Laser or heat therapy to shrink the prostate if the problem is due to an enlarged prostate
- Fibrocystic breast disease
- Temporary or permanent weakness, numbness, difficulty speaking
- Venomous bites and stings (see snake bite)
- Muscular dystrophy
- If you find active lice, talk to your health care provider before doing another treatment.
- Thinning of eyebrows
- Naphtha
In most people medications ocd asacol 400 mg order amex, their natural immune response finds the virus and clears it from the body symptoms nicotine withdrawal buy discount asacol line. The direct medical costs of following these women may be as much as $6 billion a year treatment quadriceps tendonitis cheap asacol 400 mg amex, and the emotional cost of the abnormal test reports cannot be measured medications in carry on luggage cheap asacol 800 mg buy line. Antibodies work in the extracellular compartment and cannot affect viruses inside cells medications given during labor asacol 400 mg purchase without prescription. This problem was written by Claire Conroy when she was an undergraduate student at the University of Texas at Austin. MasteringA&P Chapter Summary 807 chaPter summary In this chapter, you learned how the immune system protects the body from pathogens and how it removes damaged tissue and abnormal cells. An immune response requires detection of the foreign substance, communication with other immune cells, and coordination of the response. These functions depend on chemical communication and molecular interactions between receptors, antibodies, and antigens. The compartmentation of the body affects how the immune system fights pathogens: Some pathogens hide inside cells, while others remain in the extracellular compartment. Physical and chemical barriers, such as skin and mucus, are the first line of defense. Phagocytosis requires that surface molecules on the pathogen bind to membrane receptors on the phagocyte. Inflammatory cytokines include acute-phase proteins, histamine, interleukins, bradykinin, and complement proteins. The complement cascade forms membrane attack complex, poreforming molecules that cause pathogens to rupture. The human immune system consists of lymphoid tissues, immune cells, and cytokines. Antigens are substances that trigger an immune response and react with products of that response. First exposure to an antigen activates a naïve lymphocyte clone and causes it to divide (clonal expansion). Additional exposure to the antigen creates a faster and stronger secondary immune response. Lymphocyte cytokines include interleukins and interferons, which interfere with viral replication. Activated B lymphocytes differentiate into plasma cells, which secrete soluble antibodies. The five classes of immunoglobulins (Ig), or antibodies, are IgG, IgA, IgE, IgM, and IgD, collectively known as gamma globulins. Soluble antibodies act as opsonins; serve as a bridge between antigens and leukocytes; activate complement proteins, cytotoxic cells, and mast cells; and disable viruses and toxins. The immune response includes: (1) detection and identification, (2) communication among immune cells, (3) recruitment of assistance and coordination of the response, and (4) destruction or suppression of the invader. Neutrophils are phagocytic cells that release pyrogens and cytokines that mediate inflammation. B cell antibodies bind antigens to activate B lymphocytes and initiate the production of additional antibodies. T lymphocytes are responsible for cell-mediated immunity, in which the lymphocytes bind to target cells using T-cell receptors. T lymphocytes react to antigen bound to major histocompatibility complex proteins on the target cell. Cytotoxic Tc cells release perforin, a pore-forming molecule that allows granzymes to enter the target cell and trigger it into committing suicide (apoptosis). In addition, lymphocytes produce antibodies keyed to the specific type of bacterium. Innate immune responses and antibodies help control the early stages of a viral infection. Immediate hypersensitivity reactions to allergens are mediated by antibodies and occur within minutes of exposure to antigen. Delayed hypersensitivity reactions are mediated by T lymphocytes and may take several days to develop. When self-tolerance fails, the body makes antibodies against its own components, creating an autoimmune disease. The theory of immune surveillance proposes that cancerous cells develop on a regular basis but are detected and destroyed by the immune system before they can spread. The nervous, endocrine, and immune systems are linked together by signal molecules and receptors. The link between inability to cope with stress and the development of illnesses is believed to result from neuroimmunomodulation. What is the mononuclear phagocytic system, and what role does it play in the immune system Match each of the following cell types with its description: (a) (b) (c) (d) (e) (f) lymphocyte neutrophil monocyte dendritic cell eosinophil basophil 7. Define the following terms and explain their significance: (a) (b) (c) (d) (e) (f) (g) anaphylaxis agglutinate extravascular degranulation acute-phase protein clonal expansion immune surveillance 1. Summarize the effects of histamine, interleukin-1, acute-phase proteins, bradykinin, complement, and interferon-g. A compatibility check before blood transfusion is important in order to avoid immune reaction in the recipient. Every semester around exam time, the number of students visiting the Student Health Center with colds and viral infections increases. Barbara has rheumatoid arthritis, characterized by painful, swollen joints from inflamed connective tissue. Why do lymph nodes often swell and become tender or even painful when you are sick One fascinating aspect of the physiology of the human being at work is that it provides basic information about the nature and the range of the functional capacity of different organ systems. Per-Olof Åstrand and Kaare Rodahl, Textbook of Work Physiology, 1977 25 integrative physiology iii: exercise MetabolisM and exercise 811 lo 25. The work done by Phelps and the hundreds of other Olympic athletes from around the world represents one of the most common challenges to body homeostasis: exercise. Distance running, swimming, and cycling are examples of a dynamic endurance exercise. In this chapter, we examine dynamic exercise as a challenge to homeostasis that is met with an integrated response from multiple body systems. In many ways, exercise is the ideal example for teaching physiological integration. Everyone is familiar with it, and unlike high-altitude mountaineering or deep-sea diving, it involves no special environmental conditions. Moreover, exercise is a normal physiological state, not a pathological one-although it can be affected by disease and (if excessive) can result in injury. In addition to being an excellent teaching example, exercise physiology is a very active area of integrative physiology research. The coordinated functioning of multiple body systems is still not well understood in many instances because of complex interactions between neural and local control mechanisms. Researchers use a combination of animal models and studies with human subjects, including elite athletes, in their quest to explain how the body adapts to the metabolic demands of exercise. For further information, you might want to consult an exercise physiology textbook. Others must be mobilized from the liver and adipose tissue and then transported to muscles through the circulation. If the oxygen requirement of a muscle fiber exceeds its oxygen supply, energy production from fatty acids decreases dramatically, and glucose metabolism shifts to anaerobic pathways. In low-oxygen conditions, when the cell lacks oxygen for oxidative phosphorylation, the final product of glycolysis-pyruvate-is converted to lactate 3 instead of being converted to acetyl CoA and entering the citric acid cycle [p. In general, exercise that depends on anaerobic metabolism cannot be sustained for an extended period. The body has three sources: the plasma glucose pool, intracellular stores of glycogen in muscles and liver, and "new" glucose made in the liver through gluconeogenesis [p. Muscle and liver glycogen stores provide enough energy substrate to release about 2000 kcal (equivalent to about 20 miles of running in the average person), more than adequate for the exercise that most of us do. About 30 minutes after aerobic exercise begins, the concentration of free fatty acids in the blood increases significantly, indicating that fats are being mobilized from adipose tissue. When exercise exceeds about 70% of maximum, carbohydrates become the primary source of energy. Endurance training also increases the activity of enzymes for b-oxidation and converts muscle fibers from fast-twitch glycolytic to fast-twitch oxidative-glycolytic [p. During high-intensity exercise (levels greater than 70% of maximum), glucose becomes the main energy source. Oxygen supply to exercising cells lags behind energy use, creating an oxygen deficit. Hormones Regulate Metabolism during Exercise Several hormones that affect glucose and fat metabolism change their pattern of secretion during exercise. Plasma concentrations of glucagon, cortisol, the catecholamines (epinephrine and norepinephrine), and growth hormone all increase during exercise. Cortisol and the catecholamines, along with growth hormone, promote the conversion of triglycerides to glycerol and fatty acids. Glucagon, catecholamines, and cortisol also mobilize liver glycogen and raise plasma glucose levels. A hormonal environment that favors the conversion of glycogen into glucose is desirable, because glucose is a major energy substrate for exercising muscle. Curiously, although plasma glucose concentrations rise with exercise, the secretion of insulin decreases. This response is contrary to what you might predict, because normally an increase in plasma glucose stimulates insulin release. During exercise, however, insulin secretion is suppressed, probably by sympathetic input onto the beta cells of the pancreas. For one thing, less insulin means that cells other than muscle fibers reduce their glucose uptake, sparing blood glucose for use by muscles. Actively contracting muscle cells, on the other hand, are not affected by low levels of insulin because they do not require insulin for glucose uptake. Oxygen Consumption Is Related to Exercise Intensity the activities we call exercise range widely in intensity and duration, from the rapid and relatively brief burst of energy exerted by a sprinter or power lifter, to the sustained effort of a marathoner. Oxygen consumption is a measure of cellular respiration and is usually measured in liters of oxygen consumed per minute. When exercise begins, muscle oxygen consumption increases so rapidly that it is not immediately matched by the oxygen supplied to the muscles. The use of these muscle stores creates an oxygen def icit because their replacement requires aerobic metabolism and oxygen uptake. Other factors that play a role in elevating postexercise oxygen consumption include increased body temperature and circulating catecholamines. Q1: Where is the RyR found in skeletal muscle fibers and what is its role in muscle contraction Ventilatory responses to exercise Think about what happens to your breathing when you exercise. Exercise is associated with both increased rate and increased depth of breathing, resulting in enhanced alveolar ventilation [p. Exercise hyperventilation, or hyperpnea, results from a combination of feedforward signals from central command neurons in the motor cortex and sensory feedback from peripheral receptors. As muscle contraction continues, sensory information feeds back to the respiratory control center to ensure that ventilation and tissue oxygen use remain closely matched. Pulmonary stretch receptors were once thought to play a role, but recipients of heartlung transplants display a normal ventilatory response to exercise even though the neural connections between lung and brain are absent. This observation means that the once-accepted causes of increased ventilation during mild to moderate exercise- 811 814 818 819 821 such as strength training depends heavily on anaerobic metabolism to meet energy needs. Is the limiting factor for aerobic exercise the ability of the exercising muscle to use oxygen efficiently Or is it the ability of the cardiovascular system to deliver oxygen to the tissues One possible limiting factor in exercise is the ability of muscle fibers to obtain and use oxygen. Data suggest that muscle metabolism is not the limiting factor for maximum exercise capacity, but muscle metabolism has been shown to influence submaximal exercise capacity. This finding explains the increase in numbers of muscle mitochondria and capillaries with endurance training. The question of whether the pulmonary system or the cardiovascular system limits maximal exercise was resolved when research showed that ventilation is only 65% of its maximum when cardiac output has reached 90% of its maximum. From that information, exercise physiologists concluded that the ability of the cardiovascular system to deliver oxygen and nutrients to the muscle at a rate that supports aerobic metabolism is a major factor in determining maximum oxygen consumption. Next, we examine the reflexes that integrate breathing and cardiovascular function during exercise. Exercise Ventilation (L/min) 40 20 0 0 Exercise begins 5 Time (min) Exercise ends 10 Modified from P. The center responds with sympathetic discharge that increases cardiac output and causes vasoconstriction in many peripheral arterioles. In untrained individuals, cardiac output goes up fourfold, from 5 L/ min to 20 L/min. In trained athletes, it may go up six to eight times, reaching as much as 40 L/min. Because oxygen delivery by the cardiovascular system is the primary factor determining exercise tolerance, trained athletes are therefore capable of more strenuous exercise than untrained people.
Purchase asacol 400 mg with amex. ìƒì‚¬ë³‘ (Symptoms) - SHINee (Sub español).
References
- Browning A: Risk factors for developing residual urinary incontinence after obstetric fistula repair, BJOG 113(4):482n485, 2006.
- Prasad K, Mohanty S, Bhatia R, et al. Autologous intravenous bone marrow mononuclear cell therapy for patients with subacute ischaemic stroke: a pilot study. Indian J Med Res 2012; 136:221-8.
- De Palo G, Mariani L, Camerini T, et al. Effect of fenretinide on ovarian carcinoma occurrence. Gynecol Oncol 2002;86(1):24-27.
- Handa T, Nagai S, Miki S, et al: Incidence of pulmonary hypertension and its clinical relevance in patients with sarcoidosis, Chest 129(5):1246-1252, 2006.