
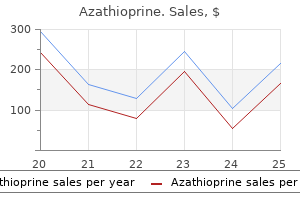
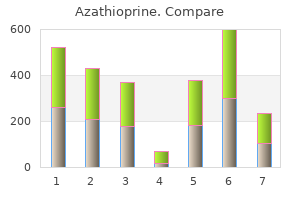
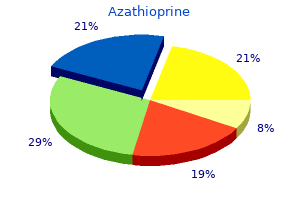
Azathioprine
| Contato
Página Inicial
Tatum Tarin, MD
- Urology Resident,
- Stanford University, Department of Urology,
- Stanford, California
Gastrulation (stages 67) occurs within 3 hours of fertilization muscle relaxant otc meds azathioprine 50 mg order with visa, and by the end of the first day (stages 1617) spasms while going to sleep purchase azathioprine 50 mg on-line, the embryo hatches to enter the first larval stage called the first instar muscle relaxant used in surgery azathioprine 50 mg buy without prescription. An epidermal-derived hardened shell called a cuticle surrounds each instar stage larva spasmus nutans cheap 50 mg azathioprine free shipping. At the end of each instar stage spasms pain rib cage generic azathioprine 50 mg visa, the cuticle sheds to accommodate the growth of the larva. Following the third instar stage, the cuticle contributes to extracellular case that surrounds the prepupa. Adult tissues that are derived from ectoderm, such as the nervous system, arise from pockets of epithelium formed during the larval stages. These pockets of tissue, called imaginal discs, attach to the inside of the larval epidermis and later evert during metamorphosis to form adult structures of the head, thorax, legs, and wings. Unlike most other larval-stage organs, the components of the gut and nervous system persist in the adult fly. Cells of the nervous system proliferate during the larval stages and begin to differentiate in the pupal stage. In Drosophila, the nervous system arises from ventral ectoderm (the ventral neurogenic ectoderm), rather than the dorsal ectoderm as in vertebrates. The arrow indicates the brain region and the arrowhead indicates the ventral nerve cord. These include the subesophageal ganglia (associated with head and neck regions), the thoracic ganglia (associated with legs and wings structures), and the abdominal ganglia (associated with abdominal structures). There are four types of glial cells in Drosophila that are designated cortex, surface, neuropil, and peripheral glia. The three pairs of ganglia that make subesophageal ganglia thoracic ganglia abdominal ganglia up the Drosophila brain are divided into protocerebrum (forebrain), deutocerebrum (midbrain), and tritocerebrum (hindbrain). These ganglia connect to the ventral nerve cord comprised of subesophageal, thoracic, and abdominal ganglia. The nervous system (blue) is shown relative to the digestive (green) and circulatory (yellow) systems. The cortex glia are most like astrocytes, the neuropil glia are similar to oligodendrocytes, and the peripheral glia function similar to Schwann cells. The lineage of each cell has been documented through serial electron micrographs and by following the progeny and fate of individual cells through the translucent body of the tiny worm. The egg cell is fertilized inside the worm and cells begin to divide in a specific sequence beginning about 40 minutes after fertilization. The eggs are laid at the gastrulation 26-cell; beginning of gastrulation 44-cell eggs laid outside synthesis of larval cuticle starts pharyngeal pumping starts 750 800 1. Gastrulation begins when the egg is laid, about 150 minutes after fertilization, when there are 26 cells present. The timing of the migration of founder cells during gastrulation is indicated below the timeline. As the worm continues to elongate and become thinner, the worm folds over itself 1. Under favorable environmental conditions, the adult worm emerges about 56 hours after fertilization. Gastrulation is initiated as cells move inward to form the gut and muscle tissues, while the hypodermis, the equivalent of ectoderm in vertebrates, remains as the outermost layer. Cells of the hypodermis that subsequently move to the inside of the embryo give rise to the majority of the neurons. The remaining cells of the hypodermis migrate over the surface of the embryo to form the epidermis. During the final stages of embryogenesis, the shape of the embryo changes from a spherical structure to the elongated shape of the adult. The resulting larva then progresses through the four larval stages (L1L4) before forming an adult worm. During the larval stages, additional neurons are produced, with the majority born during the late L1 stage. The length of time in each larval stage depends, in part, on environmental conditions such as temperature, food supply, and population density. As shown in the diagram, each dividing cell produces cells in a specific location. The P1 cell (red) establishes the germ line (red cells) and various somatic cells (yellow, orange, purple, and blue). Thus, the P1 founder cell functions like a stem cell in that it gives rise to both somatic and germ cells. However, not all cells of a given body system arise from a single founder cell type. In all cases, however, the individual neuronal types always arise from the same precursor and are always found in the same location in the body. The head region also contains numerous sense organs called sensilla that are comprised of free nerve endings and glial sheath and socket cells. Despite the variations in anatomy and cellular organization among the different animal models, many of the genes and signaling pathways are conserved across species, allowing discoveries in one animal model to impact discoveries in another. This is particularly helpful when a technique is more readily applied to a simpler invertebrate animal model than a more complex vertebrate model. The regulated production of these specialized proteins gives individual neurons their unique characteristics and allows them to perform specific functions in the nervous system. Neurons, like other cells, produce only the proteins required at a particular stage of development. In order to selectively produce these proteins, individual genes must be turned on (expressed) or turned off (repressed) at the correct stage of development. In many instances, gene expression and protein production are influenced by extracellular signals. The extracellular signal is typically a ligand that binds to a cell surface receptor protein to initiate intracellular signal transduction pathways. Cell signaling or signal transduction is the process by which signals originating outside a cell are conveyed to cytoplasmic components or the nucleus to influence cell behavior. Because the ligand is often thought of as the first messenger in a signal transduction pathway, the subsequent intracellular events are often called second messenger pathways. The activation of various signal transduction pathways regulates cellular events such as survival, death, growth, differentiation, movement, and intracellular communication. Once the ligand binds to the receptor, subsequent signaling molecules are activated inside the cell. There are often several sequential signaling molecules influenced before the final cellular response is achieved. A signal is said to activate a target downstream when it influences the next molecule in the signal transduction pathway. The signal transduction pathway eventually regulates effector proteins that serve a variety of different cellular functions. Several examples of specific signal transduction pathways utilized during neural development are detailed in subsequent chapters. The structure of each ligand and receptor is unique so that a given ligand only binds to corresponding receptors. Each step in the cascade stimulates the next molecule in the pathway until an effector protein is influenced. Thus, cells become specialized so they only respond to required signals at each developmental stage and ignore other signals that may also be present at that time. Experimental techniques are used to label genes and proteins in the developing nervous system Because each cell subtype in the nervous system expresses a unique set of genes and proteins, researchers have developed several techniques to identify where and when these molecules are expressed during development and in adulthood. Among the techniques are those that use microscopy to identify the distribution of genes and proteins in tissues or individual cells. These approaches lead not only to understanding the cellular distribution of genes and proteins, but also provide a way to label or mark particular cells and track them over the course of development. This has been especially helpful, because the outward morphological appearance of embryonic neurons is often homogeneous, making it difficult, or impossible, to identify a cell with any certainty following any sort of experimental manipulation. To visualize gene expression in neural tissues, scientist use in situ hybridization. Identifying gene expression patterns often provides insight into the putative function of that gene in a given cell, while also providing a labelling method to track changes in gene expression under normal and experimental conditions. Scientists use immunohistochemistry or immunocytochemistry to label proteins in tissues or cells, respectively. These methods take advantage of the immune response in which an animal develops antibodies to a foreign substance. For example, one method of generating antibodies is to inject rabbits with a protein of interest. The animals develop antibodies to the protein that are then isolated from the blood serum. The resulting antibodies, called primary antibodies, are then added to tissues or cell cultures, where they bind to the target protein. These antibodies are visualized by either adding an enzymatic reporter molecule, such as horseradish peroxidase, or a fluorescent probe directly to the primary antibody, or by adding one of the labels to a secondary antibody that recognizes and binds the primary antibody. These methods often provide fine details on the distribution of a protein within a cellular region. Altering development as a way to understand normal processes One of the most common ways to assess normal developmental events is to alter some aspect of development and see what happens. This allows researchers to test whether a given tissue, cell, or protein is necessary for normal development to occur. Over the past century and a half, a number of methods gene regulatIon In the DevelopIng nervouS SyStem 23 have been used to alter development. Among the common approaches used today are techniques to manipulate tissues in vivo and in vitro and methods to evaluate naturally occurring and experimentally induced genetic mutations. Tissue manipulations have been used since the earliest studies of developmental neurobiology. These methods typically involve surgically removing or rotating a particular region of the developing embryo or grafting extra tissue onto a region of the embryo. Several examples of these types of studies are highlighted in Chapters 2, 4, 7, and 8. Scientists can also observe effects of tissue manipulations in cell culture preparations. In these assays, tissues of interest are surgically dissected from an embryo at a given stage of development and placed into a cell culture dish. The dishes are often coated with substrate molecules that support the attachment and growth of the cells under investigation. The tissues are then covered in a nutrient-containing fluid (cell culture medium). To identify sources of signals that promote the survival, growth, or differentiation of a neural population, the tissues may be grown in the presence of other tissues. In some experiments, specific proteins may be added to test whether they have a direct effect on the developing cells. Cell culture techniques to study neural development were introduced in the 1920s and remain a very popular method for analyzing the development of neural cells. An advantage of cell culture is the ability to test single reagents on a select population of cells. A limitation to the method is that the artificial environment removes other tissue-derived cues that may interact with and alter the effects of the reagent under investigation. Such genetic manipulations have been instrumental in understanding neural development in both invertebrate and vertebrate animal models. A number of these spontaneously occurring mutations have provided an extensive body of data on the development of the nervous system. As detailed in Chapter 6, scientists investigating Drosophila initially relied on naturally occurring mutations, but soon developed methods to experimentally mutate genes of interest. Methods for blocking, reducing, or increasing gene expression were also developed for many vertebrate animal models. A method to experimentally delete, or knock out, individual genes in mice was introduced in the 1980s. The development of a technique for generating gene knockout mice greatly advanced studies of mammalian neural development (Box 1. Researchers continue to refine techniques to selectively alter gene and protein expression in cells at specific stages of development, providing finer resolution of the molecular pathways involved in neural development. There are limits to these approaches, however, and researchers are aware that induced changes represent an artificial environment and that complementary studies are needed to test the role of the molecules during normal development. Despite the inherent limitations of these approaches, to date such tissue and genetic manipulation studies have provided considerable insight into mechanisms underlying normal neural development. The technique has become so widely used and discussed that it may be difficult to imagine what a surprising and significant impact it had when it first emerged in the early 1980s. In fact, when Mario Cappecchi first proposed the technique to a funding agency, the proposal was turned down because reviewers believed the process could not work effectively. Mammalian cells are also capable of the process when foreign genes are intentionally inserted, such as occurs in the process of generating knockout mice. Two commonly used selector genes are the neomycin resistance (neoR) gene-a positive selector gene-and the herpes thymidine kinase (tk) gene-a negative selector gene. The cells are grown in a culture medium that contains the drugs neomycin and glanciclivor. Cells that have inserted the neoR gene in place of the targeted gene will survive in the medium containing the antibiotic neomycin. Glanciclivor will kill any cells that retain the tk gene; thus, the cells that have randomly inserted the targeting vector outside the gene sequence of interest will be eliminated. By using both positive and negative selector genes, all or nearly all of the cells surviving in the culture medium will be those with the targeted gene disrupted. The blastocysts are implanted into a surrogate, or foster, female mouse of a different coat color to develop to term.
Thus P X = (P B - P H 2 O) × F the general gas law (familiar from chemistry courses) states that the product of pressure times volume of a gas is equal to the number of moles of the gas multiplied by the gas constant multiplied by the temperature spasms right upper quadrant buy azathioprine 50 mg visa. The percentages of gases in dry air at a barometric pressure of 760 mm Hg (with the corresponding values for F in parentheses) are as follows: O2 muscle relaxant 5859 azathioprine 50 mg amex, 21% (0 muscle relaxant dogs 50 mg azathioprine buy overnight delivery. Because air is humidified in the airways muscle relaxant for migraine safe azathioprine 50 mg, water vapor pressure is obligatory and equal to 47 mm Hg at 37°C spasms just below ribs azathioprine 50 mg order with visa. To calculate a gas concentration in the liquid phase, the partial pressure in the gas phase first is converted to the partial pressure in the liquid phase; next, the partial pressure in liquid is converted to the concentration in liquid. An important, but not necessarily self-evident, point is that at equilibrium, the partial pressure of a gas in the liquid phase equals the partial pressure in the gas phase. The concentration of a gas in solution is expressed as volume percent (%), or volume of gas per 100 mL of blood (mL gas/100 mL blood). Forms of Gases in Solution In alveolar air, there is one form of gas, which is expressed as a partial pressure. In solution, gas may be dissolved, it may be bound to proteins, or it may be chemically modified. It is important to understand that the total gas concentration in solution is the sum of dissolved gas plus bound gas plus chemically modified gas. In other words, bound gas and chemically modified gas do not contribute to the partial pressure. Of the gases found in inspired air, nitrogen (N2) is the only one that is carried only in dissolved form and it is never bound or chemically modified. Because of this simplifying characteristic, N2 is used for certain measurements in respiratory physiology. The diagram shows that the pulmonary capillaries are perfused with blood from the right heart (the equivalent of mixed venous blood). The blood leaving the pulmonary capillary is delivered to the left heart and becomes systemic arterial blood. In humidified tracheal air, it is assumed that the air becomes fully saturated with water vapor. Again, recall that partial pressures in humidified air are calculated by correcting the barometric pressure for water vapor pressure, then multiplying by the fractional concentration of the gas. It is then pumped from the right ventricle into the pulmonary artery, which delivers it to the pulmonary capillaries. The blood that leaves the pulmonary capillaries has been arterialized (oxygenated) and will become systemic arterial blood. This arterialized blood will now be returned to the left heart, pumped out of the left ventricle into the aorta, and begin the cycle again. This discrepancy is the result of a physiologic shunt, which describes the small fraction of pulmonary blood flow that bypasses the alveoli and therefore is not arterialized. The physiologic shunt has two sources: bronchial blood flow and a small portion of coronary venous blood that drains directly into the left ventricle rather than going to the lungs to be oxygenated. The physiologic shunt is increased in several pathologic conditions (called a ventilation/perfusion defect). When the size of the shunt increases, equilibration between alveolar gas and pulmonary capillary blood cannot adequately occur and pulmonary capillary blood is not fully arterialized. Not shown on the figure, but implied from the differences between systemic arterial blood and mixed venous blood, are the exchange processes that occur in the systemic tissues. This gas exchange in the tissues converts systemic arterial blood to mixed venous blood, which then leaves the capillaries, returns to the right heart, and is delivered to the lungs. Diffusion-Limited and Perfusion-Limited Gas Exchange Gas exchange across the alveolar/pulmonary capillary barrier is described as either diffusion limited or perfusion limited. Diffusion-limited gas exchange means that the total amount of gas transported across the alveolarcapillary barrier is limited by the diffusion process. In these cases, as long as the partial pressure gradient for the gas is maintained, diffusion will continue along the length of the capillary. Perfusion-limited gas exchange means that the total amount of gas transported across the alveolarcapillary barrier is limited by blood flow. In perfusion-limited exchange, the partial pressure gradient is not maintained, and in this case, the only way to increase the amount of gas transported is by increasing blood flow. In the figure, the solid red line shows the partial pressure of a gas in pulmonary capillary blood (Pa) as a function of length along the capillary. The partial pressure of the gas in pulmonary capillary blood is shown as a function of capillary length by the solid red line. The shaded pink area gives the size of the partial pressure difference between alveolar air and pulmonary capillary blood, which is the driving force for diffusion of the gas. The shaded pink area gives the partial pressure gradient between alveolar gas and pulmonary capillary blood along the length of the capillary. Because the partial pressure gradient is the driving force for diffusion of the gas, the larger the shaded area, the larger the gradient, and the greater the net transfer of gas. It is also illustrated by the transport of O2 during strenuous exercise and in pathologic conditions such as emphysema and fibrosis. In fact, if the capillary were longer, net diffusion would continue indefinitely, or until equilibration occurred. N2O is used as the classic example of perfusion-limited exchange because it is not bound in blood at all but is entirely free in solution. Thus initially there is a large partial pressure gradient for N2O between alveolar gas and capillary blood, and N2O rapidly diffuses into the pulmonary capillary. Because all of the N2O remains free in blood, all of it creates a partial pressure. Thus the partial pressure of N2O in pulmonary capillary blood increases rapidly and is fully equilibrated with alveolar gas in the first one-fifth of the capillary. Once equilibration occurs, there is no more partial pressure gradient and therefore no more driving force for diffusion. The much smaller shaded area for N2O illustrates the differences between the two gases. Because equilibration of N2O occurs, the only means for increasing net diffusion of N2O is by increasing blood flow. If more "new" blood is supplied to the pulmonary capillary, then more total N2O can be added to it. Thus blood flow or perfusion determines, or "limits," the net transfer of N2O, which is described as perfusion limited. O2 Transport-Perfusion Limited and Diffusion Limited Under normal conditions, O2 transport into pulmonary capillaries is perfusion limited, but under other conditions. There is a large partial pressure gradient for O2 between alveolar air and capillary blood, which drives O2 diffusion into the capillary. The gradient for diffusion is maintained initially because O2 binds to hemoglobin, which keeps the free O2 concentration and the partial pressure low. Another way of describing perfusionlimited O2 exchange is to say that pulmonary blood flow determines net O2 transfer. This increased diffusion distance slows the rate of diffusion of O2 and prevents equilibration of O2 between alveolar air and pulmonary capillary blood. Because a partial pressure gradient is maintained along the entire length of the capillary, it may seem that the total amount of O2 transferred would be greater in a person with fibrosis than in a person with normal lungs. At high altitude, barometric pressure is reduced, and with the same fraction of O2 in inspired air, the partial pressure of O2 in alveolar gas also will be reduced. Even at the beginning of the pulmonary capillary, the gradient is only 25 mm Hg (50 mm Hg - 25 mm Hg), instead of the normal gradient at sea level of 60 mm Hg (100 mm Hg - 40 mm Hg). This reduction of the partial pressure gradient means that diffusion of O2 will be reduced, equilibration will occur more slowly along the capillary, and complete equilibration will be achieved at a later point along the capillary (two-thirds of the capillary length at high altitude, compared with onethird of the length at sea level). The slower equilibration of O2 at high altitude is exaggerated in a person with fibrosis. Pulmonary capillary blood does not equilibrate by the end of the capillary, resulting in values for PaO2 as low as 30 mm Hg, which will seriously impair O2 delivery to the tissues. Dissolved O2 alone is inadequate to meet the metabolic demands of the tissues; thus a second form of O2, combined with hemoglobin, is needed. Dissolved O2 Dissolved O2 is free in solution and accounts for approximately 2% of the total O2 content of blood. Recall that dissolved O2 is the only form of O2 that produces a partial pressure, which, in turn, drives O2 diffusion. At this concentration, dissolved O2 is grossly insufficient to meet the demands of the tissues. If O2 delivery to the tissues were based strictly on the dissolved component, then 15 mL O2/min would be delivered to the tissues (O2 delivery = cardiac output × dissolved O2 concentration, or 5 L/min × 0. Clearly, this amount is insufficient to meet the demand of 5-Respiratory Physiology · 217 250 mL O2/min. An additional mechanism for transporting large quantities of O2 in blood is needed-that mechanism is O2 bound to hemoglobin. O2 Bound to Hemoglobin O2-Binding Capacity and O2 Content Because the majority of O2 transported in blood is reversibly bound to hemoglobin, the O2 content of blood is primarily determined by the hemoglobin concentration and by the O2-binding capacity of that hemoglobin. The O2-binding capacity is the maximum amount of O2 that can be bound to hemoglobin per volume of blood, assuming that hemoglobin is 100% saturated. The O2 content can be calculated from the O2-binding capacity of hemoglobin and the percent saturation of hemoglobin, plus any dissolved O2. Each subunit contains a heme moiety, which is an iron-binding porphyrin, and a polypeptide chain, which is designated either or. Adult hemoglobin (hemoglobin A) is called 22; two of the subunits have chains and two have chains. Each subunit can bind one molecule of O2, for a total of four molecules of O2 per molecule of hemoglobin. The percent of heme groups bound to O2 is called percent (%) saturation; thus 100% saturation means that all four heme groups are bound to O2. When hemoglobin is oxygenated, it is called oxyhemoglobin; when it is deoxygenated, it is called deoxyhemoglobin. For the subunits to bind O2, iron in the heme moieties must be in the ferrous state. If the iron component of the heme moieties is in the ferric, or Fe3+, state (rather than the normal Fe2+ state), it is called methemoglobin. Methemoglobinemia has several causes including oxidation of Fe2+ to Fe3+ by nitrites and sulfonamides. There is also a congenital variant of the disease in which there is a deficiency of methemoglobin reductase, an enzyme in red blood cells that normally keeps iron in its reduced state. In fetal hemoglobin, the two chains are replaced by chains, giving it the designation of 22. The physiologic consequence of this modification is that HbF has a higher affinity for O2 than hemoglobin A, facilitating O2 movement from the mother to the fetus. HbF is the normal variant present in the fetus and is gradually replaced by hemoglobin A within the first year of life. Hemoglobin S is an abnormal variant of hemoglobin that causes sickle cell disease. In hemoglobin S, the subunits are normal and the subunits are abnormal, giving it the designation A2S2. In its deoxygenated form, hemoglobin S forms sickle-shaped rods in the red blood cells, distorting the shape of the red blood cells. This deformation of the red blood cells can result in occlusion of small blood vessels, causing many of the symptoms of sickle cell crisis. A man who is anemic has a severely reduced hemoglobin concentration of 10 g/100 mL blood. Assume that for a normal hemoglobin concentration of 15 g/100 mL, the O2-binding capacity is 20. It is a given that at a normal hemoglobin concentration of 15 g/100 mL, O2-binding capacity is 20. Thus at a hemoglobin concentration of 10 g/100 mL, O2-binding capacity is 10/15 of normal. If fewer than four molecules of O2 are bound to heme groups, then saturation is less than 100%. For example, if, on average, each hemoglobin molecule has three molecules of O2 bound, then saturation is 75%; if, on average, each hemoglobin has two molecules of O2 bound, then saturation is 50%; and if only one molecule of O2 is bound, saturation is 25%. Sigmoidal Shape (2) Next, calculate the actual amount of O2 combined with hemoglobin by multiplying the O2-binding capacity by the % saturation. O2 content of blood, as already described, is the sum of dissolved O2 (2%) and O2-hemoglobin (98%). A change in the value of P50 is used as an indicator for a change in affinity of hemoglobin for O2. An increase in P50 reflects a decrease in affinity, and a decrease in P50 reflects an increase in affinity. Due to positive cooperativity, affinity is highest and O2 is most tightly bound (the flat portion of the curve). The high affinity makes sense because it is important to have as much O2 as possible loaded into arterial blood in the lungs. O2 is not as tightly bound in this part of the curve, which facilitates unloading of O2 in the tissues. Because oxyhemoglobin and deoxyhemoglobin have different absorbance characteristics, the machine calculates % saturation from absorbance at two different wavelengths. Pulse oximetry measures arterial % saturation because arterial blood "pulses," whereas venous and capillary blood do not; background absorbance from venous and capillary blood is subtracted out. However, knowing % saturation, one can estimate PaO2 from the O2-hemoglobin dissociation curve. Such shifts reflect changes in the affinity of hemoglobin for O2 and produce changes in P50. Shifts can occur with no change in O2-binding capacity, in which case the curve moves right or left, but the shape of the curve remains unchanged.
Because the treatment is described within the note muscle relaxant rocuronium 50 mg azathioprine buy otc, you can easily make your selections and bill without having to memorize a long list of billing codes spasms vitamin deficiency order generic azathioprine on line. One selects a plan from the dropdown menu that includes commonly used treatment instructions muscle relaxant otc cvs azathioprine 50 mg without prescription. If more detail is needed muscle relaxant list azathioprine 50 mg order on-line, one then describes the plan using the expandable box below the dropdown list muscle relaxant 5658 buy 50 mg azathioprine with visa. Development of an inflammatory bowel disease research registry derived from observational electronic health record data for comprehensive clinical phenotyping. Leveraging electronic health record implementation to facilitate clinical and operational quality improvement in an ambulatory surgical clinic. Requirements and access needs of patients with chronic disease to their hospital electronic health record: results of a cross-sectional questionnaire survey. Assessing electronic health record implementation challenges using item response theory. When it comes to securing patient health information from breaches, your best medicine is a dose of prevention: a cybersecurity risk assessment checklist. Impacts of structuring the electronic health record: results of a systematic literature review from the perspective of secondary use of patient data. What are positive and negative aspects of using check boxes, dropdown menus, and smart phrases Provide some examples of what is required in each stage that could be relevant to physical therapy practice. If the clinician has been part of a transition from paper to electronic records, discuss the changes that occurred in the workflow. List components of the Patient/Client Management Model that should be documented in the medical record. Identify tasks that must be documented by the physical therapist and those that can be documented by the physical therapist assistant. Correctly document late entries and appropriate correct errors in written medical records. Documentation begins with the initial examination, evaluation, and plan of care as performed and written by the physical therapist. Subsequent documentation includes interim notes for every encounter with the patient. Interim notes can be written by the physical therapist or the physical therapist assistant. Interim notes are written to record treatment sessions and serve as a record of what was billed. This note often reflects the results of a discharge evaluation, which is also performed and written by the physical therapist. Templates come built into electronic medical records and, in some software, templates can be created or loaded. Avoid making subjective remarks about patients, including anything that cannot be substantiated by the data. Also, avoid subjective terms such as appears and seems to be (eg, "patient seems depressed today"). While the majority of physical therapy documentation occurs electronically, there may be instances when notes must be handwritten and they should be written legibly. When writing in a medical record, or creating documents that will be scanned into a medical record, use black or blue permanent ink. Physical therapy examination, evaluation, diagnosis, prognosis, and plan of care (including interventions) shall be documented, dated, and authenticated by the physical therapist who performs the service. Interventions provided by the physical therapist or selected interventions provided by the physical therapist assistant under the direction and supervision of the physical therapist are documented, dated, and authenticated by the physical therapist or, when permissible by law, the physical therapist assistant. In addition, the medical record should be kept in a secured file to meet confidentiality, privacy, and security requirements. It is important that documentation is completed as soon after the session as possible. In addition, documentation will be necessary so that another physical therapist or physical therapist assistant can treat the patient in the event of an absence. Clinics are likely to have policies in place that require the completion of all patient documentation within a given time frame. A reviewer should be able to examine the medical record and have an accurate, detailed portrayal of the patient and situation. Although it is important to be as concise as possible, you should also still be thorough. The patient required min (a) x 1 for facilitation to the (R) quadriceps during the swing phase of gait and min (a) x 1 for stabilization of the (R) knee during the stance phase. Use only industrystandard and facility-approved medical terminology, symbols, and abbreviations. This can become confusing for the reader, especially if he or she is unfamiliar with the abbreviations. In these cases, one must read the entire note to determine the context of the abbreviation so that it can be interpreted correctly. Most facilities will have policies regarding acceptable abbreviations and their use. Do not skip lines in the middle of entries, such as in between different sections. Skipping lines could allow someone to come back at a later date and fraudulently add information. Headings group relevant information together to indicate new sections and to designate important patient information. When handwriting notes, it is important to use the same headings that were used by the physical therapist in the initial evaluation, when possible. This will help to provide consistency between the initial evaluation and the interim notes and will allow the reader to identify data in specific sections. The use of headings is often necessary in instances when the health care providers must free text their notes into a word processing area. In instances when there are great deals of data that can easily become confusing to the reader, it is appropriate to use tables, columns, or lists. Tables are valuable when documenting range of motion or strength on several joints, such as the hand. After completing the documentation for a particular treatment session and placing it in the medical record, one might realize a need to document additional information about the session. The entry should be placed in chronological order for the date that it is written and should be identified as a "late entry" or "addendum. All physical therapy records should be dated according to the day that the services were provided. Authentication is defined as "the process used to verify that an entry into the medical record is complete, accurate, and final. Document reasons for cancelled or missed appointments or treatment sessions, whether initiated by the patient, the physical therapist, the physical therapist assistant, or another health care provider. For example, one may record the following: "Plan to implement electrical stimulation at the next visit to increase activity of the wrist extensor muscles. This includes documenting any precautions, limitations, restrictions, or instructions provided to the patient. One may document the following, "After reviewing total hip precautions, the patient was able to recite them without correction, and the patient verbalized understanding. Upon licensure, review the practice act to identify any specific requirements related to documentation. One should not use the phrase "continue per plan" for multiple subsequent visits, but instead should be specific as to what skilled intervention will be provided at the next visit. Documenting the same information in the plan on several notes is received as being repetitive. She is performing resisted knee flexion with a pulley system and feels a "pop" in her knee with a moderate increase in pain. For example, one may record the following: "The patient states that his exercises have helped in improving knee motion, and he is noticing improvement in sitting and ascending/descending stairs as a result. Use common, professional terminology consistent with the International Classification of Functioning, Disability and Health Framework. Describe how the impairments are leading to activity limitations and participation restrictions. Also, make comparisons between data collected at the beginning of a treatment session and data collected at the conclusion of the session. Pay by the rules: avoid Medicare audits and reduce payment denials with a sound strategy and proper documentation. What components of the Patient/Client Management Model should be documented in the medical record A physical therapist assistant sees a patient in an acute care setting first thing in the morning. How might an entry be written so that it communicates that the care the patient received is "skilled" When is it appropriate to create your own abbreviations or symbols for use in a medical record What documentation format would be appropriate to document cancellations or missed appointments Give an example of a medical record entry that includes a planned intervention and a rationale. For the following entries, indicate examples that are inappropriate by writing an "I" next to the item. Write the following information in a more clear and concise manner, as it would appear in the medical record. The patient walked 75 feet in the hallway of the hospital with the therapist lightly touching her back. The therapist was needed to help provide the patient with support to maintain balance. The patient demonstrated the following range of motion measurements: active range of motion for the right elbow was 130° flexion and 10° of hyperextension. Chapter 6 the patient propelled his wheelchair around the hospital, outside on the sidewalk, and up and down several ramps with you providing verbal reminders on trunk positioning for going up and down the ramps. The patient was able to put her ankle-foot orthosis on and remove it independently. She was also able to independently check her skin for any irritated areas after she removed the orthosis. You instructed the patient to perform 10 repetitions of each exercise as part of her home exercise program. The exercises included ankle pumps, quadriceps setting, short arc quadriceps strengthening from 45° to 0°, and heel slides. During a busy morning in a hospital, you were working with a patient who told you that she was going to be discharged and wanted home health services, primarily physical therapy. Indicate whether the information would fall into the S, O, A, or P portion of the note. Jones comes into the clinic today and tells you that his fingers became swollen and that he has had pain at a level of 7 out of 10 since the last treatment session. He goes on to say that he has not been able to perform any of the range of motion exercises you gave him because of the incredible amount of pain he has been having. He said that he has changed his postoperative dressing once a day since the last visit, and he has had a little bit of red drainage on the bandages. He also said that he is having trouble eating and shaving due to the swelling and stiffness in the finger joints. She said that her right knee pain is not as bad as it was yesterday and she thinks that she is able to bend it more. She goes on to say that she has performed the range of motion exercises twice already this morning, and she is working on trying to get her knee to bend as much as she can. While walking using a standard walker, she asks if she can begin using a cane soon. Smith comes into the physical therapy department and tells you that he notices improvement in his walking since beginning the active range of motion exercises for his ankle. He goes on to tell you that he still has pain when walking on gravel, carpet, and stairs. His job requires him to do a lot of walking on uneven terrain, and he wants to be able to do this without pain before returning to work. The supervising physical therapist told you that the patient is demonstrating confusion and slurred speech, but her daughter is usually present during the sessions. As you work with the patient, she tells you that she fell in the bathroom last night. She also tells you that she is afraid to get out of bed because of her fear of falling again. He also tells you that he is having trouble getting his mother to walk in the house with him due to pain and fear of making her hip hurt more than it already does. He also says that he has trouble performing the range of motion exercises that you showed him during the last session. The patient tells you that, because of the pain, she feels like her hip is going to give out when she stands on it. The patient went up and down 4 stairs with a handrail that was on the right side going up and on the left coming down; the patient used a straight cane. The patient walked with the therapist at his side (but not touching him) for 100 feet, twice; vital signs before exercise were blood pressure 125/85, 15 for respirations, and 77 for heart rate; vitals after were 135/85 for blood pressure, 17 for respirations, and 87 for heart rate; the patient performed ankle pumping, elbow flexion, shoulder flexion, and knee extension for 10 repetitions before and after exercise. The patient walks independently with crutches, weightbearing as much as he can tolerate on the involved extremity for 100 feet. List the types of information that can be found in each component of an initial evaluation note. List the questions that the physical therapist assistant should ask when reviewing the evaluation note to guide decision related to provision of selected interventions.
As a result of the net movement of positive charge to Solution 2 spasms around heart buy azathioprine master card, an Na+ diffusion potential develops and Solution 2 becomes positive with respect to Solution 1 muscle relaxant for children purchase azathioprine master card. This conversion is accomplished by the various constants: R is the gas constant spasms sleep 50 mg azathioprine buy, this the absolute temperature muscle relaxant modiek order azathioprine 50 mg overnight delivery, and F is Faraday constant; multiplying by 2 muscle relaxant online discount azathioprine 50 mg amex. By convention, membrane potential is expressed as intracellular potential relative to extracellular potential. Hence, a transmembrane potential difference of -70 mV means 70 mV, cell interior negative. If the intracellular [Ca2+] is 10-7 mol/L and the extracellular [Ca2+] is 2 × 10-3 mol/L, at what potential difference across the cell membrane will Ca2+ be at electrochemical equilibrium Another way of posing the question is to ask what the membrane potential will be, given this concentration gradient across the membrane, if Ca2+ is the only permeant ion. Simply complete the calculation either way to arrive at 129 mV, and then determine the correct sign with an intuitive approach. Thus Ca2+ will be at electrochemical equilibrium when the membrane potential is +129 mV (cell interior positive). Be aware that the equilibrium potential has been calculated at a given concentration gradient for Ca2+ ions. With a different concentration gradient, the calculated equilibrium potential would be different. In other words, it is the difference between the actual Em and the value the ion would "like" the membrane potential to be. In other words, ion X "thinks" the membrane potential is too negative and tries to bring the membrane potential toward its equilibrium potential by diffusing in the appropriate direction across the cell membrane. Ions will move across the cell membrane through ion channels when two conditions are met: (1) there is a driving force on the ion, and (2) the membrane has a conductance to that ion. The direction of ionic current is determined by the direction of the driving force, as described in the previous section. The magnitude of ionic current is determined by the size of the driving force and the conductance of the ion. For a given conductance, the greater the driving force, the greater the current flow. For a given driving force, the greater the conductance, the greater the current flow. Lastly, if either the driving force or the conductance of an ion is zero, there can be no net diffusion of that ion across the cell membrane and no current flow. As stated previously, in expressing the membrane potential, it is conventional to refer the intracellular potential to the extracellular potential. The resting membrane potential is established by diffusion potentials, which result from the concentration differences for various ions across the cell membrane. Ions with the highest permeabilities or conductances at rest will make the greatest contributions to the resting membrane potential, and those with the lowest permeabilities will make little or no contribution. The resting membrane potential of most excitable cells falls in the range of -70 to -80 mV. These values can best be explained by the concept of relative permeabilities of the cell membrane. Thus the resting membrane potential is close to the equilibrium potentials for K+ and Cl- because the permeability to these ions at rest is high. The resting membrane potential is far from 1-Cellular Physiology · 19 the equilibrium potentials for Na+ and Ca2+ because the permeability to these ions at rest is low. One way of evaluating the contribution each ion makes to the membrane potential is by using the chord conductance equation, which weights the equilibrium potential for each ion (calculated by the Nernst equation) by its relative conductance. Ions with the highest conductance drive the membrane potential toward their equilibrium potentials, whereas those with low conductance have little influence on the membrane potential. Second, the more important indirect contribution is in maintaining the concentration gradient for K+ across the cell membrane, which then is responsible for the K+ diffusion potential that drives the membrane potential toward the K+ equilibrium potential. Action potentials are the basic mechanism for transmission of information in the nervous system and in all types of muscle. Terminology the following terminology will be used for discussion of the action potential, the refractory periods, and the propagation of action potentials: Depolarization is the process of making the membrane potential less negative. As noted, the usual resting membrane potential of excitable cells is oriented with the cell interior negative. Depolarization makes the interior of the cell less negative, or it may even cause the cell interior to become positive. Such a change in membrane potential should not be described as "increasing" or "decreasing" because those terms are ambiguous. As with depolarization, the terms "increasing" or "decreasing" should not be used to describe a change that makes the membrane potential more negative. An example of an inward current is the flow of Na+ into the cell during the upstroke of the action potential. An example of an outward current is the flow of K+ out of the cell during the repolarization phase of the action potential. Threshold potential is the membrane potential at which occurrence of the action potential is inevitable. Because the threshold potential is less negative than the resting membrane potential, an inward current is required to depolarize the membrane potential to threshold. If net inward current is less than net outward current, the membrane will not be depolarized to threshold and no action potential will occur (see all-or-none response). Overshoot is that portion of the action potential where the membrane potential is positive (cell interior positive). Refractory period is a period during which another normal action potential cannot be elicited in an excitable cell. Each normal action potential for a given cell type looks identical, depolarizes to the same potential, and repolarizes back to the same resting potential. An action potential at one site causes depolarization at adjacent sites, bringing those adjacent sites to threshold. If an excitable cell is depolarized to threshold in a normal manner, then the occurrence of an action potential is inevitable. On the other hand, if the membrane is not depolarized to threshold, no action potential can occur. Indeed, if the stimulus is applied during the refractory period, then either no action potential occurs, or the action potential will occur but not have the stereotypical size and shape. Ionic Basis of the Action Potential the action potential is a fast depolarization (the upstroke), followed by repolarization back to the resting membrane potential. At rest, the membrane potential is approximately -70 mV (cell interior Absolute refractory period +65 mV Relative refractory period Na+ equilibrium potential Action potential Voltage or conductance 0 mV Na+ conductance K+ conductance 70 mV 85 mV Resting membrane potential K+ equilibrium potential 1. The K+ conductance or permeability is high and K+ channels are almost fully open, allowing K+ ions to diffuse out of the cell down the existing concentration gradient. This diffusion creates a K+ diffusion potential, which drives the membrane potential toward the K+ equilibrium potential. The conductance to Cl- (not shown) also is high, and, at rest, Cl- also is near electrochemical equilibrium. At rest, the Na+ conductance is low, and thus the resting membrane potential is far from the Na+ equilibrium potential, and Na+ is far from electrochemical equilibrium. An inward current, usually the result of current spread from action potentials at neighboring sites, causes depolarization of the nerve cell membrane to threshold, which occurs at approximately -60 mV. The increase in Na+ conductance results in an inward Na+ current; the membrane potential is further depolarized toward, but does not quite reach, the Na+ equilibrium potential of +65 mV. Tetrodotoxin (a toxin from the Japanese puffer fish) and the local anesthetic lidocaine block these voltage-sensitive Na+ channels and prevent the occurrence of nerve action potentials. The upstroke is terminated, and the membrane potential repolarizes to the resting level as a result of two events. First, the inactivation gates on the Na+ channels respond to depolarization by closing, but their response is slower than the opening of the activation gates. Thus after a delay, the inactivation gates close, which closes the Na+ channels and terminates the upstroke. Second, depolarization opens K+ channels and increases K+ conductance to a value even higher than occurs at rest. The combined effect of closing of the Na+ channels and greater opening of the K+ channels makes the K+ conductance much higher than the Na+ conductance. For a brief period following repolarization, the K+ conductance is higher than at rest and the membrane potential is driven even closer to the K+ equilibrium potential (hyperpolarizing afterpotential). Eventually, the K+ conductance returns to the resting level, and the membrane potential depolarizes slightly, back to the resting membrane potential. The Nerve Na+ Channel A voltage-gated Na+ channel is responsible for the upstroke of the action potential in nerve and skeletal muscle. This channel is an integral membrane protein, consisting of a large subunit and two subunits. The basic assumption of this model is that in order for Na+ to move through the channel, both gates on the channel must be open. The inactivation gates close in response to depolarization, but slowly, after a time delay. Thus when depolarization occurs, the activation gates open quickly, followed by slower closing of the inactivation gates. At the resting membrane potential, the activation gates are closed and the inactivation gates are open. However, they are "available" to fire an action potential if depolarization occurs. During the upstroke of the action potential, depolarization quickly opens the activation gates and both the activation and inactivation gates are briefly open. At the peak of the action potential, the slow inactivation gates finally close in response to depolarization; now the Na+ channels are closed, the upstroke is terminated, and repolarization begins. In other words, how do they recover, so that they are ready to fire another action potential Repolarization back to the resting membrane potential causes the inactivation gates to open. The Na+ channels now return to the closed, but available state and are ready and "available" to fire another action potential if depolarization occurs. The refractory period includes an absolute refractory period and a relative refractory period. Absolute Refractory Period the absolute refractory period overlaps with almost the entire duration of the action potential. During this period, no matter how great the stimulus, another action potential cannot be elicited. The basis for the absolute refractory period is closure of the inactivation gates of the Na+ channel in response to depolarization. Relative Refractory Period the relative refractory period begins at the end of the absolute refractory period and overlaps primarily with the period of the hyperpolarizing afterpotential. During this period, an action potential can be elicited, but only if a greater than usual depolarizing (inward) current is applied. The basis for the relative refractory period is the higher K+ conductance than is present at rest. Because the membrane potential is closer to the K+ equilibrium potential, more inward current is needed to bring the membrane to threshold for the next action potential to be initiated. Accommodation When a nerve or muscle cell is depolarized slowly or is held at a depolarized level, the usual threshold potential may pass without an action potential having been fired. This process, called accommodation, occurs because depolarization closes inactivation gates on the Na+ channels. The upstroke of the action potential cannot occur because there are insufficient available Na+ channels to carry inward current. An example of accommodation is seen in persons who have an elevated serum K+ concentration, or hyperkalemia. At rest, nerve and muscle cell membranes are very permeable to K+; an increase in extracellular K+ concentration causes depolarization of the resting membrane (as dictated by the Nernst equation). A 48-year-old woman with insulin-dependent diabetes mellitus reports to her physician that she is experiencing severe muscle weakness. She is being treated for hypertension with propranolol, a -adrenergic blocking agent. The physician tapers off the dosage of propranolol, with eventual discontinuation of the drug. This diabetic patient has severe hyperkalemia caused by several factors: (1) Because her insulin dosage is insufficient, the lack of adequate insulin has caused a shift of K+ out of cells into blood (insulin promotes K+ uptake into cells). These mechanisms involve concepts related to renal physiology and endocrine physiology. It is important to understand that this woman has a severely elevated blood [K+] (hyperkalemia) and that her muscle weakness results from this hyperkalemia. The basis for this weakness can be explained as follows: the resting membrane potential of muscle cells is determined by the concentration gradient for K+ across the cell membrane (Nernst equation). At rest, the cell membrane is very permeable to K+, and K+ diffuses out of the cell down its concentration gradient, creating a K+ diffusion potential. This K+ diffusion potential is responsible for the resting membrane potential, which is cell interior negative. When the blood [K+] is elevated, the concentration gradient across the cell membrane is less than normal; resting membrane potential will therefore be less negative. It might be expected that this depolarization would make it easier to generate action potentials in the muscle because the resting membrane potential would be closer to threshold. A more important effect of depolarization, however, is that it closes the inactivation gates on Na+ channels.
As the neural plate curves over to form the neural tube spasms from sciatica cheap azathioprine 50 mg amex, the former apical surface is located surrounding the lumen (the future ventricles) muscle relaxant methocarbamol purchase azathioprine 50 mg amex, while the former basal surface becomes the outer surface of the neural tube located just below the pial membrane muscle relaxer 75 buy generic azathioprine 50 mg. Sauer reported that cells located near the ventricular surface extend thin processes that contact both the apical and basal surfaces spasms above ear 50 mg azathioprine with mastercard. The nuclei of these cells then travel through these processes as the cell cycle progresses muscle relaxant antagonist discount azathioprine 50 mg free shipping. As the neural plate curves over to form the neural tube, the apical surface of the neural plate becomes the ventricular surface surrounding the lumen of the neural tube and the basal surface becomes the outer (pial) surface. Sauer was the first to report that the cells along the ventricular surface extend cytoplasmic processes that contact both the pial and ventricular surface. The nucleus of the cell then migrates through the cytoplasmic process using a mechanism called interkinetic nuclear migration. The nucleus first travels to the basal (pial) surface, then returns to the apical (ventricular) surface, where it undergoes mitosis (cell division). The movement of the nucleus through the cytoplasmic process was called intermitotic migration of nuclei or, as is commonly called today, interkinetic nuclear migration. In the 1950s she and colleagues conducted a number of experiments using nuclear stains and the newly developed tritiated thymidine method that confirmed nuclear migration was linked to phases of the cell cycle. Once chromosomes are copied, the cells progress to the G2 (gap 2) stage, preparing for mitosis. Sauer reported the pattern of nuclear migration in neural precursor cells in the neural tube of the chick. This report was one of the first neurobiology experiments to use the tritiated thymidine labeling technique developed in 1957. Thus, nuclei of cells at the G1 phase of the cell cycle are located at the ventricular zone. When the migrating nucleus reaches the pial surface, the cell is in the S phase of the cell cycle, after which the nucleus travels back to the ventricular surface, where the cell enters the M phase and divides into two dn 5. The resulting daughter cells will either migrate away from the ventricular surface, or extend a process to the pial surface and continue through another series of interkinetic movements in order to divide again. As development progresses and more precursor cells are generated, the wall of the neural tube thickens so that the cell nuclei must travel increasingly greater distances to the pial surface. It is thought that the nucleus may be exposed to growth factors or other signals in the cytoplasm as it travels through the different regions of the cell process during the various stages of the cell cycle. It has also been suggested that the movement of nuclei into different layers provides more space for proliferation to occur in the very small region of the early neural tube. Although the exact purpose is not yet known, interkinetic movements in the developing neural tube are a highly orchestrated and precise mechanism that likely provides essential cues for further development and specification of cellular characteristics. These unique and very precisely ordered patterns of interkinetic movement are seen only in regions of pseudostratified epithelium and the ventricular zone of the neural tube. Other sites of neurogenesis in the nervous system, including the subventricular zone of the cerebrum and external granule cell layer of the cerebellum discussed below, do not undergo nuclear translocation prior to cell division. Thus, the intriguing process of interkinetic movements is restricted to specific regions of the developing embryo. The final stage is the M phase (mitosis) in which the cell divides to produce two daughter cells. Sauer demonstrated that cells that incorporated a radiolabel during the S phase of the cell cycle were located near the pial (basal) surface of the neural tube. Sauer confirmed that the translocation of the nucleus corresponds to different stages of the cell cycle. The cell enters the gap 1 (G1) phase of the cell cycle as its nucleus travels toward the pial (basal) surface. Once the nucleus reaches the ventricular (apical) surface, it enters the mitotic (M) phase in which the cell divides. The plane of cell division and patterns of protein distribution determine whether a cell proliferates or migrates Following interkinetic translocation of the nucleus and its return to the ventricular surface, the precursor cell divides. The cleavage plane of cell division is critical in determining whether a cell continues to divide or migrates away from the ventricular zone. Cell division occurs along a vertical cleavage plane (perpendicular to the ventricular surface) or either a horizontal (parallel to the ventricular surface) or an oblique cleavage plane (at an angle to the ventricular surface). The basal process is either split between the two daughter cells, or one cell inherits the basal process while the other produces a new process. In contrast, with a horizontal or oblique cleavage plane, a cell divides asymmetrically to generate two nonidentical daughter cells. The basal daughter cell (the cell closer to the pial surface) does not inherit the basal process and also loses attachment to the ventricular surface. This daughter cell then migrates away from the ventricular surface as an immature neuron. During this early stage of neurogenesis, the basal cells begin to express proneural genes, the genes that provide a cell with the potential to become a neuron. Later in development, additional genes will be expressed that establish the type of neuron that will form. In contrast to the basal daughter cell, proneural genes are repressed in the apical cells so that they continue to divide. Cells will continue to proliferate until enough neuronal precursors are generated. Distinct proteins are concentrated at the apical and basal poles of progenitor cells At the ventricular surface, the plane of cell division in a progenitor cell is regulated by many factors. Numerous proteins are segregated at the apical and basal poles of cells that function to mediate the attachment of cellular processes to the apical and basal surfaces, direct the orientation of the mitotic spindles, and regulate the expression of genes that allow for either continued proliferation or neural differentiation and migration. For example, adherens junctions are detected in apical cells at the ventricular surface. Adherens junctions contain the calcium-dependent adhesion molecule cadherin and are among the cellular elements required to maintain proliferation. In this case, the cell divides symmetrically, producing two daughter cells (cell 1 and cell 2) that remain at the ventricular (apical) surface of the neural tube. These cells continue to proliferate, producing new daughter cells (cells 1a, 1b, and cells 2a, 2b). In such cases, the cell divides asymmetrically, producing a basal daughter cell that will migrate away from the ventricular region toward the pial (basal) surface (cell 1) and an apical daughter cell (cell 2) that will continue to proliferate at the ventricular (apical) surface (cells 2a and 2b). In the basal daughter, proneural genes begin to be expressed, whereas in the apical daughter cell, proneural genes are repressed. During asymmetrical cleavage, the basal cell down-regulates the expression of cadherins. The orientation of the mitotic spindle determines the position of the cleavage furrow and therefore establishes whether a cell undergoes symmetrical or asymmetrical division. In cells undergoing symmetric division, multiple proteins ensure that the mitotic spindles adhere to the lateral cell membrane. When the mitotic spindle is oriented in a horizontal or oblique plane, an unequal segregation of proteins into apical and basal poles is observed in the daughter cells. Much of what is known about the distribution of apical and basal proteins in vertebrate cells was first discovered in Drosophila, where homologous proteins are found to regulate the formation of neuronal and nonneuronal cells (see Chapter 6). Among the proteins involved during vertebrate neurogenesis are the Notch receptors and their corresponding membrane-bound ligands. The receptors and ligands are expressed in all precursor cells, but at differing levels. The distribution of the apical and basal proteins within a daughter cell helps to establish the level of Notch receptor activity, and therefore determines whether a cell proliferates or migrates. Both cells are attached at the ventricular surface by adherens junctions that are needed to retain a proliferative state. The migrating basal cell will inherit a higher concentration of the basal proteins Numb and Prox 1, while the apical daughter cell will inherit a higher concentration of apical proteins, including those of the Par complex and mInsc (mammalian Inscuteable). In the basal daughter cell, Numb and Prox 1 are able to decrease the activity and expression of Notch, respectively. Decreased Notch activity in the basal daughter cell allows for the expression of proneural genes and cell differentiation. In the apical cell, the Par complex and mInsc allow the Notch receptor to have a higher level of activity. Notch receptor activity also leads to a suppression of proneural genes to help maintain the undifferentiated, proliferative state in that cell. Together these proteins appear to influence the orientation of the mitotic spindle and help keep basal proteins, such as Numb and Prox-1 (prospero homeobox1), concentrated at the opposite pole of the cell. With symmetric cell division, both daughter cells maintain similar levels of Notch receptor activity, so both cells continue to proliferate. With asymmetric division, however, the higher concentration of basal proteins in the basal cell interferes with Notch signaling in that cell. Numb, for example, binds to the intracellular region of the Notch receptor to inhibit its activity and prevent proliferation of the basal daughter cell. As the basal cell begins to migrate out of the ventricular region, Notch gene expression is down-regulated. Prox 1, like the Drosophila homolog Prospero, inhibits the proliferation of precursor cells by binding to the Notch promoter region, preventing Notch expression. Reduced Notch receptor activity or gene expression ends proliferation and allows for the expression of proneural genes in the basal daughter. In the apical daughter cells that arise following asymmetric cleavage, the level of Numb protein is insufficient to interfere with Notch receptor activity. Proneural genes are needed to induce Prox 1 expression, so Notch receptor activity also prevents Prox 1 expression. Thus, Notch and Prox 1 are able to crossinhibit one another to carefully balance the number of proliferating and migrating precursor neurons to ensure the correct number of cells is produced at each phase of neurogenesis. Further details on Notch signaling and the regulation of gene cascades that establish cell fate are described in Chapter 6. What is significant for this stage of development is that the distribution of specific proteins into apical and basal poles during cell division establishes the first step in determining whether a neural progenitor remains in the proliferative state or migrates away from the ventricular surface to begin the differentiation process. The rate of proliferation and the length of the cell cycle change over time the balance of symmetric and asymmetric cleavage changes over the course of development. Such proliferation is particularly evident in the neural plate and early neural tube stages. Over time, as a sufficient number of neuronal precursors are generated, the need for production of new cells lessens. As this happens, more and more cells reach their final cell division (terminal mitosis) and migrate out of the ventricular zone to occupy specific regions of the developing neural tube. Several studies have documented how the cell proliferation rate changes as development progresses. One means of determining the proliferation rate in a given tissue is to monitor the length of the cell cycle. Several methods have been developed for measuring cell cycle length, including tritiated thymidine, BrdU (bromodeoxyuridine, an analog of thymidine), and retroviral labels. As cell cycle time lengthens, fewer cycles per day are possible, and fewer new cells are produced. The length of the cell cycle, which was observed to last about 8 hours on the first day of proliferation, increased to 18 hours by the end of the proliferative phase. Similarly, in the developing chick optic tectum, the cell cycle was found to lengthen from about 8 to 15 hours over a three-day period of proliferation. One hypothesis is that the longer G1 phase allows for exposure to growth factors that influence subsequent developmental events (Box 5. Much of the current understanding of cell cycle regulation originated in work with model systems such as yeast and sea urchins. Scientists soon discovered that knowledge gained from these studies is broadly applicable to most vertebrate neurons as well. Cell cycle regulation is primarily controlled by two families of interacting proteins: cyclins and cyclin-dependent kinases. Both families contain multiple members, including some that are not associated with the cell cycle. The cyclins are a group of proteins that were initially identified on the basis of an unusual expression pattern: Levels of various cyclins oscillate throughout the different stages of the cell cycle. Cyclins were first discovered in the 1980s when scientists studying extracts of fertilized sea urchin eggs noted a decrease in a particular protein band that only occurred at the time of cell division. Cyclin-dependent kinases (Cdks) are a family of serine/threonine protein kinases that must be activated by cyclins before they can phosphorylate downstream proteins to regulate progression through the cell cycle. Cdks are related to the cdc (cell division cycle) genes first identified in yeast. In contrast to the cyclical expression of the cyclins, the expression of the Cdks is stable throughout the cell cycle. It is the changes in A cy cl B in 140 120 100 80 60 40 20 cell division (M) sperm sample every 10 min 35S-methionine extract protein separate proteins on gel cell division (M) suspension of sea urchin eggs 0 minutes autoradiogram urchin eggs radiolabeled with 35S-methionine. Samples were harvested at 10-minute intervals following fertilization and these extracts were then run on a gel. However, one band showed a cyclical pattern of expression in which there was a gradual increase in radiolabel followed by a sudden decrease in signal intensity. Cyclins are proteins that increase through the various stages of the cell cycle, then decrease after mitosis. Cyclin-dependent kinases (Cdks) are serine/threonine kinases that are activated by the cyclins to phosphorylate downstream proteins needed to drive the cell to the next phase of the cell cycle. Growth factors activate cyclin D and Cdk4 or cyclin D and Cdk6 to initiate the G1 phase of the cell cycle. Cyclin A, coupled with Cdk1 or Cdk2 pushes the cell toward G2, from which cyclin B/Cdk1 or cyclin A/Cdk1 drives the cell to mitosis (M). The Cdk inhibitory proteins p15, p21, p27 and p57 can stop the progression of the cell cycle at different phases. All three of these Cdk inhibitory proteins can stop the activity of Cdk4 or Cdk6 associated with cyclin D in the G1 phase. In contrast, p21, p27 and p57 can halt the activity of Cdk2 associated with cyclin E or dn 5.
Azathioprine 50 mg buy with mastercard. Стероиды побочки Ð¡Ñ‚ÐµÑ€Ð¾Ð¸Ð´Ð½Ð°Ñ ÑроÑÑ‚ÑŒ и качок неадекват Ðеадекватное поведение на курÑе Ñтероидов.
References
- Brantly M, Courtney M, Crystal RG. Repair of the secretion defect in the Z form of ?1-antitrypsin by addition of a second mutation. Science 1988;242:1700.
- Steele SR, Goetz LH, Minami S, Madoff RD, Mellgren A, Parker SC. Management of recurrent rectal prolapse: surgical approach influences outcome. Dis Colon Rectum 2006;49(4):440-5.
- Freeman JA, Tarter TA, Esrig D, et al: Urethral recurrence in patients with orthotopic ileal neobladders, J Urol 156:1615n1619, 1996.
- Urban JA. Radical excision of the chest wall for mammary cancer. Cancer. 1951;4:1263-1285.
- Pannu N, Wiebe N, Tonelli M. Prophylaxis strategies for contrast-induced nephropathy. JAMA. Jun 21 2006;295(23):2765-2779.
- MacKenzie EJ, Bosse MJ, Kellam JF, et al. Characterization of patients with high-energy lower extremity trauma. J Orthop Trauma. 2000;14(7):455-466.
- Hall JE: Somatic sensations: I. General organization, the tactile and position senses. In Hall JE, editor: Guyton & Hall textbook of medical physiology, ed 12, Philadelphia, 2011, Saunders, pp 571-582.
- Oohara T, Tohma H, Takezoe K, et al. Minute gastric cancers less than 5 mm in diameter. Cancer 1982;50:801.