
Bupropion
| Contato
Página Inicial
E Philip Perry MBChB FRCS
- Consultant general and vascular surgeon
- Scarborough District Hospital, Scarborough
- Honorary senior lecturer, Hull York Medical School
- Examiner for RCS England, UK
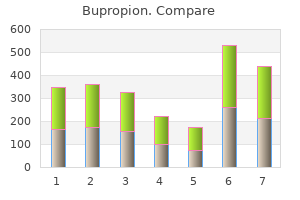
Albumin exerts oncotic activity (colloid osmotic pressure) to retain intravascular water anxiety vs depression symptoms generic 150 mg bupropion mastercard. Hydroxyethyl groups at position C2 inhibit the access of -amylase to the substrate more effectively than those at C6 anxiety zantac buy 150 mg bupropion amex. In hypovolemic patients depression symptoms reddit bupropion 150 mg low cost, there is no evidence that albumin reduces mortality compared with crystalloid or colloid solutions depression zodiac signs buy discount bupropion online. The intravascular retention of albumin is affected by increased vascular permeability depression glass defined cheap 150 mg bupropion with visa. The molar replacement ratio indicates the proportion of glucose molecules replaced with hydroxyethyl units. The C2/ C6 ratio indicates the number of hydroxyethyl units at the C2 relative to the C6 position. Colloid replacement therapy might still be indicated in early volume resuscitation after acute blood loss. Hemostatic Interventions and Coagulation Therapies Platelet Concentrates Platelets are anuclear, granulated cells 2 to 4 µm in diameter derived from bone marrow megakaryocytes. Extravascular (subendothelial) collagen and tissue factor are exposed to the flowing blood. The intact vascular wall (blue), platelets (white ovals), erythrocytes (red circles), and fibrin (green) are depicted. Platelet transfusion and measures to increase von Willebrand factor can augment this process. These factors can be replaced using plasma transfusion or specific factor concentrates (see text for details). Four to 8 random-donor units are pooled to increase platelet count by 5 to 10 × 109/L in the adult. In order to decrease multiple donor exposures, single-donor platelet apheresis is increasingly used. During the apheresis procedure, donor blood is placed in the extracorporeal circuit and centrifuged to separate platelets. One platelet apheresis unit contains 30 to 50 × 1010 platelets in 250 to 300 mL of plasma. Platelet concentrates are agitated and stored at room temperature (2024°C) for up to 5 days (see Table 44. Clinical Uses Platelet transfusion is used to prevent or treat bleeding due to platelet dysfunction or thrombocytopenia. Platelet transfusion can be required even with a normal platelet count if platelet dysfunction is clinically suspected or identified by platelet function testing. The lack of virus reduction procedures for platelet concentrates has been a major concern, and transmissions of Zika virus via platelet transfusion were recently reported. Further clinical validations are needed as to its indications and efficacies against emerging pathogens. Problems due to platelet alloimmunization include refractoriness to platelet transfusion and post-transfusion purpura. This typically occurs after group O platelet transfusion in non-group O recipients. The increment in platelet count was higher after apheresis platelets compared to pooled concentrates, but without impacting clinical bleeding in hemato-oncologyrelated thrombocytopenia. However, other plasma products have been increasingly used to make up the shortfall in plasma supply in the United States. The recovery of coagulation factors after each plasma unit is about 2% to 3% in the adult but can vary with donors, clinical hemorrhage, and/ or ongoing consumption. The bottles of plasma are sealed and refrozen (< -30°C) and subsequently dehydrated under vacuum and gradually rising temperature. Leukoreduced plasma undergoes pathogen reduction steps, including amotosalen and ultraviolet light (Intercept Blood System). The plasma is subsequently aliquoted in an individual flask and freeze-dried over 4 days. Each bottle of powdered plasma is reconstituted with 200 mL of sterile water before transfusion. For congenital factor deficiency, plasma transfusion should be considered only if recombinant or plasma-derived factor concentrate is not available (Table 44. Plasma products are sometimes transfused prophylactically before invasive procedures when risk of bleeding is high, but there is limited evidence and no cut-off level for any coagulation test that clearly indicates the need for plasma. Plasma can be used as a replacement fluid (plasma exchange) in patients undergoing therapeutic plasma exchange (apheresis). The risk of fluid overload owing to a large volume of plasma transfusion should be considered in patients with limited cardiovascular reserve. Hypocalcemia can result from citrate accumulation after plasma transfusion, and is treated with calcium chloride or gluconate. Risk of viral transmission has been reduced significantly since the 1990s by implementing nucleic acid testing for human immunodeficiency virus and hepatitis C virus. Use of pathogeninactivated plasma (S/D or methylene bluetreated plasma) might further reduce viral transmission risks. The minimal level of plasma fibrinogen to minimize perioperative bleeding has not been established. More recently, higher fibrinogen levels (150 to 200 mg/dL) have been recommended in European guidelines for perioperative transfusion10,11 based on clinical data supporting fibrinogen greater than 200 mg/dL in postpartum hemorrhage,93 coronary bypass grafting surgery,46,9496 and cystectomy. Each unit contains 150 to 250 mg of fibrinogen; 5 to 10 units are thawed and pooled before infusion (Table 44. Each unit of cryoprecipitate increases plasma fibrinogen by approximately 100 mg/dL per 5 kg body weight. The volume of cryoprecipitate required to Side Effects Exposure to multiple donors from pooled cryoprecipitate units is a major concern since no viral inactivation procedure is clinically available. Fibrinogen Concentrate Fibrinogen concentrate is a lyophilized product prepared from plasma. It can be rapidly reconstituted and administered intravenously because no thawing or blood type matching is required. The incidence of thromboembolic complications appears to be nearly 7-fold higher in those without congenital factor deficiency. Several small retrospective clinical studies have demonstrated hemostatic effects of fibrinogen replacement after complex cardiac surgical cases,104,105 but the results of recent prospective randomized trials for fibrinogen replacement in cardiac surgery are mixed (Table 44. Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: a phase 3b, open-label, non-inferiority, randomised trial. Elevated systemic thrombin activity thus increases protein C activation as observed in thrombophilia,138 sepsis,139 and traumatic injury. Local and systemic regulation of coagulation and fibrinolysis at a site of vascular injury are shown. Lessons from the aprotinin saga: current perspective on antifibrinolytic therapy in cardiac surgery. The infectious risk of plasma-derived protein C is low owing to viral inactivation steps, including polysorbate-80, vapor-heat, and ion exchange chromatography. Precautions for use include bleeding, sodium overload, rare allergic reactions and heparin-induced thrombocytopenia due to trace amounts of heparin. Clinical use of aprotinin has been resumed but is limited to coronary bypass grafting surgery in Canada and Europe after its suspension from 2007 to 2012 owing to safety concerns. Antifibrinolytic therapy appears to be useful in bleeding associated with menorrhagia 149 and chronic thrombocytopenia. With renal or ureteral bleeding, lysine analogs can increase the risk of ureteral obstruction due to clot formation. In mild to moderate von Willebrand disease and hemophilia A, intravenous desmopressin (0. Desmopressin is often administered to patients with preexisting platelet dysfunction related to antiplatelet drugs and uremia. Disadvantages include inactivation of natural clotting enzymes, such as thrombin, and potential for inflammation and delayed wound healing. Microfibrillar collagen (Avitene, Bard) increases local platelet adhesion and activation, leading to hemostasis within 5 minutes. The collagen particles do not cause much swelling and are reabsorbed within 8 weeks. They are supplied with separate vials of fibrinogen, thrombin, and calcium chloride that are mixed at the wound by a dual-syringe applicator. A patch sponge (TachoSil, Baxter) impregnated with lyophilized human fibrinogen and thrombin is also available for treatment of raw surface bleeding. To prevent viral transmission from the human plasma, fibrinogen and thrombin are treated with solvent-detergent, nanofiltration or vapor-heat. Gelatin forms (Gelfoam, Pfizer; Gelfilm, Pfizer; Surgiform, Surgiform Technology, Ltd. Another gelatin-based sealant (FloSeal, Baxter) is a mixture of human thrombin and bovine-derived gelatin-based matrix. Thrombin generates fibrin from blood fibrinogen and the gelatin particles expand to tamponade bleeding. These topical agents are generally safe and useful adjuncts for hemostasis when used for appropriate indications and anatomic sites. The extent of coagulopathy varies with the type and stage of liver and biliary tract disease. The policy on blood transfusion was changed recently-acceptance of fractionated products of "primary components" was left to the individual believer (Table 44. Improved pathogen detection in donors and pathogen reduction treatments should allow increasingly safer supplies of allogeneic blood products. Proper identifications of the donor unit and patient and careful riskbenefit assessments are essential prior to each component transfusion. Expedited surgical control of bleeding is crucial in improving morbidity and mortality, and there does not appear to be any specific ratio of blood products that can be recommended. The use of thromboelastography/thromboelastometry can be helpful in the selection of hemostatic product(s). Use of factor concentrates in acquired factor deficiency is generally considered to be off-label, but there are some supportive data available for certain indications. The proper indication(s) and site(s) should be considered to reduce untoward complications. Notably, fluid overload or similar cardiac events were more frequent in the plasma group (3% vs. Improved hemostasis was more frequently observed in the 1:1:1 group than in the 1:1:2 group (86. The increased donor exposure was evident in the 1:1:1 group (median 19 U plasma plus platelets vs. This study failed to point to the optimal ratio (or volume) of plasma and platelet transfusion. Fibrinogen or fibrin polymerization was not continuously monitored and cryoprecipitate was seldom used in either group of patients (median, 0 unit). In addition, the incidences of major hemorrhage or cardiac tamponade leading to reoperation were reduced by 50% (P = 0. Thromboelastometry-guided intraoperative haemostatic management reduces bleeding and red cell transfusion after paediatric cardiac surgery. Platelets and plasma were the only 2 products available for hemostatic therapy during the study. Hyperfibrinolysis was evident on thromboelastometry in only 5% of patients, while plasma fibrinolysis markers were elevated in 57% of patients in proportion to the base deficit and hypotension on admission. The 28-day mortality of patients with hyperfibrinolysis on thromboelastometry was 40%, whereas it was 12% in those with elevated plasma fibrinolysis markers. These data suggest that hyperfibrinolysis on thromboelastometry represents a marker of worse prognosis and that antifibrinolytic therapy should be considered according to the injury severity regardless of the thromboelastometry findings. Patient blood management the pragmatic solution for the problems with blood transfusions. Effect of a patient blood management programme on preoperative anaemia, transfusion rate, and outcome after primary hip or knee arthroplasty: a quality improvement cycle. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Cross-sectional guidelines for therapy with blood components and plasma derivatives. Storage, and Transportation, Blood Banking and Transfusion Medicine: Basic Principles and Practice, 2nd Ed. Restrictive versus liberal transfusion strategy in the perioperative and acute care settings: a context-specific 24. Randomised trial of blood transfusion versus a restrictive transfusion policy after hip fracture surgery. Revised Recommendations for Reducing the Risk of Zika Virus Transmission by Blood and Blood ComponentsGuidance for Industry. Efficacy and safety of erythropoietin and intravenous iron in perioperative blood management: a systematic review. A single dose of erythropoietin reduces perioperative transfusions in cardiac surgery: results of a prospective single-blind randomized controlled trial. The role of albumin as a resuscitation fluid for patients with sepsis: a systematic review and meta-analysis. Fibrinogen estimates are influenced by methods of measurement and hemodilution with colloid plasma expanders. Blood platelets are concentrated near the wall and red blood cells, in the center in flowing blood.
The two vertical muscles of the anterolateral abdominal wall depression keeps coming back 150 mg bupropion order visa, contained within the rectus sheath depression negative thoughts order bupropion 150 mg line, are the large rectus abdominis and the small pyramidalis depression kit cheap bupropion 150 mg with amex. The fleshy part of the muscle contributes primarily to the lateral part of the abdominal wall anxiety lymph nodes bupropion 150 mg fast delivery. Thus mood disorder hospitals discount bupropion 150 mg buy, the contralateral external and internal oblique muscles together form a "digastric muscle," a two-bellied muscle sharing a common central tendon that works as a unit (see Introduction chapter). Inferiorly, the external oblique aponeurosis attaches to the pubic crest medial to the pubic tubercle. Palpate your inguinal ligament by pressing deeply into the center of the crease between the thigh and trunk and moving the fingertips up and down. Inferiorly the Chapter 2 · Abdomen 189 Fibers of left external oblique aponeurosis, which run deep on the right side and running superficially on the left side Umbilical ring Deep fibers of right external oblique aponeurosis Deep fibers of left external oblique aponeurosis Fibers passing from superficial to deep (and vice versa) at linea alba Right external oblique muscle Fibers of left internal oblique aponeurosis Fibers of right external oblique aponeurosis Left internal oblique muscle Intramuscular exchange of superficial and deep fibers within aponeuroses of contralateral external oblique muscles. Intramuscular and intermuscular fiber exchanges within the bilaminar aponeuroses of the external and internal oblique muscles are shown. The inferior parts of the two deeper anterolateral abdominal muscles arise in relationship to the lateral portion of the inguinal ligament. The complex modifications and attachments of the inguinal ligament, and of the inferomedial portions of the aponeuroses of the anterolateral abdominal wall muscles, are discussed in detail with the inguinal region (later in this chapter). Observe the anterior cutaneous nerves (T7T12) piercing the rectus abdominis and the anterior layer of the rectus sheath. The neurovascular plane of the anterolateral abdominal wall contains the nerves and arteries supplying the anterolateral abdominal wall. In the anterior part of the abdominal wall, the nerves and vessels leave the neurovascular plane and lie mostly in the subcutaneous tissue. When tensed in muscular people, the areas of muscle between the tendinous intersections bulge outward. Formation of rectus sheath and neurovascular structures of anterolateral abdominal wall. In this deep dissection, the fleshy portion of the external oblique is excised on the right side, but its aponeurosis and the anterior wall of the rectus sheath are intact. The anterior wall of the sheath and the rectus abdominis are removed on the left side so that the posterior wall of the sheath may be seen. It lies anterior to the inferior part of the rectus abdominis and attaches to the anterior surface of the pubis and the anterior pubic ligament. It ends in the linea alba, which is especially thickened for a variable distance superior to the pubic symphysis. When present, surgeons use the attachment of the pyramidalis to the linea alba as a landmark for median abdominal incision (Skandalakis et al. The external oblique aponeurosis contributes to the anterior wall of the sheath throughout its length. The superior two thirds of the internal oblique aponeurosis splits into two layers (laminae) at the lateral border of the rectus abdominis; one lamina passing anterior to the muscle and the Chapter 2 · Abdomen 193 other passing posterior to it. The posterior lamina joins the aponeurosis of the transversus abdominis to form the posterior layer of the rectus sheath. Beginning approximately one third of the distance from the umbilicus to the pubic crest, the aponeuroses of the three flat muscles pass anterior to the rectus abdominis to form the anterior layer of the rectus sheath, leaving only the relatively thin transversalis fascia to cover the rectus abdominis posteriorly. As fat accumulates in the subcutaneous tissue postnatally, the skin becomes raised around the umbilical ring and the umbilicus becomes depressed. When the diaphragm contracts during inspiration, the anterolateral abdominal wall expands as its muscles relax to make room for the organs, such as the liver, that are pushed inferiorly. The transversus abdominis probably has no appreciable effect on the vertebral column (Standring, 2008). The exception occurs at the L1 level, where the L1 anterior ramus bifurcates into two named peripheral nerves. Each dermatome begins posteriorly overlying the intervertebral foramen by which the spinal nerve exits the vertebral column and follows the slope of the ribs around the trunk. Dermatome T10 includes the umbilicus, whereas dermatome L1 includes the inguinal fold. The thoraco-abdominal nerves pass inferoanteriorly from the intercostal spaces and run in the neurovascular plane between the internal oblique and the transversus abdominis muscles to supply the abdominal skin and muscles. The lateral cutaneous branches emerge from the musculature of the anterolateral wall to enter the subcutaneous tissue Chapter 2 · Abdomen 195 along the anterior axillary line (as anterior and posterior divisions), whereas the anterior abdominal cutaneous branches pierce the rectus sheath to enter the subcutaneous tissue a short distance from the median plane. During their course through the anterolateral abdominal wall, the thoraco-abdominal, subcostal, and iliohypogastric nerves communicate with each other. The deeper veins of the anterolateral abdominal wall accompany the arteries, bearing the same name. A deeper, medial venous anastomosis may exist or develop between the inferior epigastric vein (an external iliac vein tributary) and the superior epigastric/internal thoracic veins (subclavian vein tributaries). The superior epigastric artery is the direct continuation of the internal thoracic artery. It runs superiorly in the transversalis fascia to enter the rectus sheath below the arcuate line. For an overview of superficial and deep lymphatic drainage, see the Introduction to Clinically Oriented Anatomy. Cutaneous veins surrounding the umbilicus anastomose with para-umbilical veins, small tributaries of the hepatic portal vein that parallel the obliterated umbilical vein (round ligament of the liver). Between this layer and the deep fascia covering the rectus abdominis and external oblique muscles is a potential space where fluid may accumulate. Although there are no barriers (other than gravity) to prevent fluid from spreading superiorly from this space, it cannot spread inferiorly into the thigh because the deep membranous layer of subcutaneous tissue fuses with the deep fascia of the thigh (fascia lata) along a line approximately 2. Excess fat accumulation owing to overnourishment most commonly involves the subcutaneous fatty layer; however, there may also be excessive depositions of extraperitoneal fat in some types of obesity. The pelvis tilts anteriorly at the hip joints when standing (the pubis descends and the sacrum ascends) producing excessive lordosis (sway back) of the lumbar region. Abdominal Hernias the anterolateral abdominal wall may be the site of abdominal hernias. Most hernias occur in the inguinal, umbilical, and epigastric regions (see the blue box "Inguinal Hernias," p. Umbilical hernias are common in neonates because the anterior abdominal wall is relatively weak in the umbilical ring, especially in low-birth-weight infants. Occasionally, gaps exist where these fiber exchanges occur-for example, in the midline or in the transition from aponeurosis to rectus sheath. The hernial sac, composed of peritoneum, is covered with only skin and fatty subcutaneous tissue. Protuberance of Abdomen A prominent abdomen is normal in infants and young children because their gastrointestinal tracts contain considerable amounts of air. Abdominal muscles protect and support the viscera most effectively when they are well toned; thus the well-conditioned adult of normal weight has a flat or scaphoid (lit. The six common causes of abdominal protrusion begin with the letter F: food, fluid, fat, feces, flatus, and fetus. The location of the incision also depends on the type of operation, the location of the organ(s) the surgeon wants to reach, bony or cartilaginous boundaries, avoidance of (especially motor) nerves, maintenance of blood supply, and minimizing injury to muscles and fascia of the abdominal wall while aiming for favorable healing. Thus, before making an incision, the surgeon considers the direction of the muscle fibers and the location of the aponeuroses and nerves. Instead of transecting muscles, causing irreversible necrosis (death) of muscle fibers, the surgeon splits them in the direction of (and between) their fibers. Generally, incisions are made in the part of the anterolateral abdominal wall that gives the freest access to the targeted organ with the least disturbance to the nerve supply to the muscles. However, because of overlapping areas of innervation between nerves, one or two small branches of nerves may usually be cut without a noticeable loss of motor supply to the muscles or loss of sensation to the skin. Median incisions can be made along any part or the length of the linea alba from the xiphoid process to pubic symphysis. Because the linea alba transmits only small vessels and nerves to the skin, a midline incision is relatively bloodless, and avoids major nerves; however, incisions in some people may reveal abundant and well-vascularized fat. Conversely, because of its relatively poor blood supply, the linea alba may undergo necrosis and subsequent degeneration after incision if its edges are not aligned properly during closure. Paramedian incisions (lateral to the median plane) are made in a sagittal plane and may extend from the costal margin to the pubic hairline. The posterior layer of the rectus sheath and the peritoneum are then incised to enter the peritoneal cavity. The common nerve supply of the skin and muscles of the wall explains why these spasms occur. Palpation of abdominal viscera is performed with the patient in the supine position with thighs and knees semiflexed to enable adequate relaxation of the anterolateral abdominal wall. Otherwise, the deep fascia of the thighs pulls on the membranous layer of abdominal subcutaneous tissue, tensing the abdominal wall. Some people tend to place their hands behind their heads when lying supine, which also tightens the muscles and makes the examination difficult. Superficial Abdominal Reflexes the abdominal wall is the only protection most of the abdominal organs have. With the person supine and the muscles relaxed, the superficial abdominal reflex is elicited by quickly stroking horizontally, lateral to medial, toward the umbilicus. Usually, contraction of the abdominal muscles is felt; this reflex may not be observed in obese people. Similarly, any injury to the abdominal skin results in a rapid reflex contraction of the abdominal muscles. Thus, they are distributed across the anterolateral abdominal wall, where they run oblique but mostly horizontal courses. This muscle may be divided transversely without serious damage because a new transverse band forms when the muscle segments are rejoined. Subcostal incisions provide access to the gallbladder and biliary ducts on the right side and the spleen on the left. Pararectus incisions along the lateral border of the rectus sheath are undesirable because they may cut the nerve supply to the rectus abdominis. The external oblique aponeurosis is incised inferomedially in the direction of its fibers and retracted. The musculo aponeurotic fibers of the internal oblique and transversus abdominis are then split in the line of their fibers and retracted. Carefully made, the entire exposure cuts no musculo-aponeurotic fibers; therefore, when the incision is closed, the muscle fibers move together and the abdominal wall is as strong after the operation as it was before. The linea alba and anterior layers of the rectus sheaths are transected and resected superiorly, and the rectus muscles are retracted laterally or divided through their tendinous parts allowing reattachment without muscle fiber injury. ¨ the subcutaneous layer is modified inferior to the umbilicus to include a superficial fatty layer and a deep membranous layer. ¨ the investing layer is typical of deep fascias ensheathing voluntary muscles, and here reflects the trilaminar arrangement of the flat abdominal muscles and their aponeuroses. ¨ the endoabdominal fascia is of particular importance in surgery, enabling the establishment of an extraperitoneal space that allows anterior access to retroperitoneal structures. The fibers of the aponeuroses interlace in the midline, forming the linea alba, and continue into the aponeuroses of the contralateral muscles. ¨ the aponeurotic fibers of the external obliques are also continuous across the midline with those of the contralateral internal oblique muscles. ¨ Three layers of flat, bilateral digastric muscles encircle the trunk, forming oblique and transverse girdles that enclose the abdominal cavity. Balance in the development and tonus of these partners affects posture (and thus weakness of the abdominal muscles may result in excessive lumbar lordosis-an abnormally convex curvature of the lower vertebral column). ¨ the special arrangements of the anterolateral abdominal muscles enable them to provide flexible containing walls for the abdominal contents, to increase intra-abdominal pressure or decrease abdominal volume for expulsion, and to produce anterior and lateral flexion and torsional (rotatory) movements of the trunk. Nerves: the anterolateral abdominal muscles receive multi-segmental innervation via the anterior rami of lower thoracic (T7T12) and the L1 spinal nerves. ¨ Except for L1, the maps of the abdominal dermatomes and of the peripheral nerves are thus identical. ¨ Cutaneous veins surrounding the umbilicus anastomose with small tributaries of the hepatic portal vein. ¨ the distribution of the deeper abdominal blood vessels reflects the arrangement of the muscles: an oblique, circumferential pattern (similar to the intercostal vessels above) over the anterolateral abdominal wall and a vertical pattern anteriorly. ¨ Vertical vessels include an anastomosis between the superior and the inferior epigastric vessels within the rectus sheath. ¨ A superficial anastomotic channel, the thoraco-epigastric vein, and the deeper medial pathway between the inferior and the superior epigastric veins afford collateral circulation during blockage of superior or inferior vena cava. The location of a hernia in one of these fossae determines how the hernia is classified. The shallow fossae between the umbilical folds are the: · Supravesical fossae between the median and the medial umbilical folds, formed as the peritoneum reflects from the anterior abdominal wall onto the bladder. The level of the supravesical fossae rises and falls with filling and emptying of the bladder. It is an important area anatomically and clinically: anatomically because it is a region where structures exit and enter the abdominal cavity, and clinically because the pathways of exit and entrance are potential sites of herniation. Although the testis is located in the perineum postnatally, the male gonad originally forms in the abdomen. Its relocation out of the abdomen into the perineum through the inguinal canal accounts for many of the structural features of the region. The inguinal ligament is the thickened, underturned, inferior margin of the aponeurosis of the external oblique, forming a retinaculum that bridges the subinguinal space. A slit-like gap between the medial and the lateral crura of the external oblique aponeurosis, bridged by intercrural fibers, forms the superficial inguinal ring. Chapter 2 · Abdomen 203 space, through which pass the flexors of the hip and neurovascular structures serving much of the lower limb. These fibrous bands are the thickened inferolateral-most portions of the external oblique and aponeurosis and the inferior margin of the transversalis fascia.
Effective bupropion 150 mg. Bipolar Disorder.
The prevalence of these variants also varies by race key depression test means discount bupropion 150 mg on line, with 37% of Caucasians and 14% of Africans carrying the A allele hyperinflationary depression definition purchase bupropion 150 mg line. More than 600 drugs reportedly interact the hirudin-like molecules are made by recombinant technology in cultured yeast depression symptoms psychosis buy cheap bupropion 150 mg online. Bayer Healthcare stopped production of lepirudin for business reasons in 2012 so this is no longer available depression glass for sale order bupropion 150 mg visa. This structure together with recombinant desirudin binds to both the active site and an exosite-binding site depression or grief test order generic bupropion on-line. Binding of the C-terminal dodecapeptide is at the anion-binding site used by fibrinogen (brown area), and the 4 amino acid residue D-Phe-Pro-ArgPro binds in the active site (turquoise oval). B shows the effect of thrombin to cleave the Pro-Arg bond of the active site binding moiety to inactivate the direct thrombin inhibition. Stop drug if >2 times control Bivalirudin Intravenous 25 minutes Coagulation tests within normal limits after 2 hr 0. Argatroban is also a synthetic compound derived from arginine but binds only to the active enzymatic site of thrombin and is termed a monovalent inhibitor. All of these compounds inhibit both free and bound thrombin, and none are affected by platelet factor 4. Bivalirudin is also licensed for use during percutaneous coronary intervention/angioplasty procedures. Pharmacokinetics Adverse Effects the major adverse effect of direct thrombin inhibitors is hemorrhage. Hemorrhagic complications, particularly when combined with thrombolytic or antiplatelet agents, can be life threatening. There is no antidote to any of these agents, so the antithrombin effect cannot be reversed pharmacologically. In addition, the recombinant hirudins are associated with allergic/ anaphylactic reactions that limit their use. Oral Direct Thrombin Inhibitors the first oral direct thrombin inhibitor licensed for human use was ximelagatran, a prodrug administered twice daily. Subsequent postmarketing surveillance showed that about 56% of patients given the drug had elevation of hepatic enzymes, even after withdrawal. Excretion of the recombinant hirudins is affected by renal function, whereas argatroban is entirely metabolized by the liver. Although impaired liver function is not a contraindication to the use of argatroban, the dose should be lowered and full reversal of anticoagulant effects might require more than 4 hours. This improves the safety of use of bivalirudin in patients with impaired renal function such as the elderly. This has implications for assessing anticoagulation when transferring patients to long-term anticoagulation with vitamin K antagonists. Manufacturers recommend no loading dose of warfarin, but starting with a dose near the anticipated maintenance dose. The active drug inhibits both free and clot-bound thrombin and thrombin-induced platelet activation. Clinical Pharmacology Pharmacokinetics and Pharmacodynamics Dabigatran has a predictable pharmacokinetic and pharmacodynamic profile, allowing for a fixed-dose regimen. Peak plasma concentrations are reached 2 hours after oral administration in healthy volunteers, with no unexpected accumulation upon multiple dosing. Dabigatran exhibits linear pharmacokinetic characteristics with dose-proportional increases observed in maximum plasma concentration and area under the curve. The dose should be reduced from 150 mg twice daily to 75 mg twice daily if the estimated creatinine clearance is 30 to 50 mL/min. Administration with the P-glycoprotein inhibitors ketoconazole, verapamil, amiodarone, quinidine, or clarithromycin does not require dose adjustments. This is increased to about 75% if the capsule is chewed before swallowing, so patients should be warned to swallow the capsule whole. At the highest dose of 400 mg administered three times daily, maximum prolongations over baseline of 3. If surgery cannot be delayed, a monoclonal antibody to dabagatran has been developed29 and licensed and is discussed in later text. Inhibitors of Activated Factor X Historical Perspective Factor Xa is at the convergence of the extrinsic and intrinsic pathways leading to thrombin activation. The crystal structure of human factor Xa reveals an active site divided into four subpockets (S1-4). The S1 subpocket is the major determinant of selectivity and binding of inhibitors. The first generation of oral factor Xa inhibitors was based on dibasic inhibitors binding to both the primary specificity pocket and a putative cation-binding site. Recent efforts have focused on development of nonpeptide inhibitors of low basicity by screening and rational design. Basic Pharmacology Because of shortcomings of vitamin K antagonists as the only form of oral anticoagulant (Table 45. The major advantage of direct factor Xa inhibitors is their small size and resultant ability to inactivate circulating, as well as bound, forms of factor Xa. In theory, the capacity to inhibit factor Xa within the prothrombinase complex, as well as clot-bound factor Xa, suggests more powerful control over thrombus formation and progression, and therefore potentially greater clinical efficacy. It also seems rational to inhibit the system at this point, because inhibition of one factor Xa moiety can lead to a 50-fold reduction in thrombin production. Inhibitors of activated factor Xa generally bind in an L-shaped conformation involving the anionic S1 pocket and the aromatic S4 pocket. This rational design follows analysis of the binding site by x-ray crystallography. Dabigatran at a dose of 110 mg was associated with rates of stroke and systemic embolism similar to those associated with warfarin, as well as lower rates of major hemorrhage. Dabigatran administered at a dose of 150 mg was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage at 3. These data led to dabigatran being licensed in the United States, Europe, and other countries for use as an alternate to vitamin K antagonists for prevention of stroke with atrial fibrillation. Regulatory authorities are reviewing postmarketing surveillance data after reports of 260 deaths caused by hemorrhage. Special Situations and Adverse Events As with other anticoagulants, the major risk is for bleeding, which can be life threatening, particularly with major trauma. Apixaban is a follow-up compound of the oral direct factor Xa inhibitor razaxaban. All of the agents have protein binding of about 90%, meaning they will be difficult to remove by dialysis. Clinical Pharmacology Pharmacokinetics and Pharmacodynamics the relative pharmacokinetic profiles for the four most clinically advanced factor Xa antagonists are shown in Table 45. The most striking difference between the agents is the very low renal clearance of betrixaban. This should lead to a more consistent effect without dose adjustments in older patients and those with impaired renal function, compared, for example, with rivaroxaban. Longer-term thromboprophylaxis studies center around stroke prevention in patients with atrial fibrillation and prevention of thrombosis in prosthetic heart valves. Results of the studies published thus far have not been universally positive for this class of compound, in part because of the design of the studies and also because of increased bleeding. It may be that this class of compound will replace vitamin K antagonists, but there could be safety issues when the drug is combined with antiplatelet therapy. Spontaneous hemorrhage while taking these compounds appears not to be a problem in the absence of antiplatelet therapy. Both apixaban and rivaroxaban prescribing information warn of the use of neuraxial block when these drugs are being administered. Novel agents are in late stages of development to produce acute reversal of anticoagulation. With increasing knowledge of the mechanisms of action of platelet activation, more recent therapies have concentrated on specific receptor inhibition. The configuration allows the upper part of the molecule to bind to the anionic S1 pocket of the Xa proteolytic site and the lower part to bind to the aromatic S4 pocket. The major targets for pharmacologic intervention have been inhibition of cyclooxygenase with aspirin and phosphodiesterase with dipyridamole. More recent pharmacologic interventions have been to inhibit receptors at the platelet surface. By 1829, the salicin in willow plants was identified as analgesic and this was later converted to salicylic acid. Aspirin was patented in1900; the name Aspirin comes from "A" in acetyl chloride, "spir" in Spiraea ulmaria (the plant the salicylic acid came from), and "in," a familiar name ending for medicines. Thus there is an approximately 100-fold variation in daily doses of aspirin when used as an antiinflammatory rather than as an antiplatelet agent. Peak plasma levels occur 30 to 40 minutes after ingestion, and inhibition of platelet function is evident by 1 hour. In contrast, it can take 3 to 4 hours to reach peak plasma levels after administration of enteric-coated aspirin. The oral bioavailability of regular aspirin tablets is approximately 40% to 50% over a wide range of doses and is less for enteric-coated tablets. There is no substantive evidence for greater efficacy with greater dosage, but there is evidence for increasing morbidity as dose increases. In particular, bleeding is dose dependent in patients treated for stroke and with acute coronary syndrome. Approximately 300 mg/day produce fewer gastrointestinal side effects than 1200 mg/day, and 30 mg/day produces fewer side effects than 300 mg/day. Use of the lowest effective dose (50100 mg/day for long-term treatment) is currently the most appropriate strategy to maximize efficacy and minimize toxicity. The mechanisms of action for the observed benefits in these conditions remain to be elucidated. Following an oral dose of dipyridamole Dipyridamole Basic Pharmacology Mechanism of Action. Dipyridamole is a pyrimido-pyrimidine tablets, the average time to peak concentration is about 75 minutes. The decline in plasma concentration fits a two-compartment model with an half-life (initial decline following peak concentration) of 40 minutes and a half-life of 10 hours. Absorption of dipyridamole from conventional formulations is quite variable and can result in low systemic bioavailability. A modified-release formulation of dipyridamole with improved bioavailability has been developed. Dipyridamole is highly bound to plasma proteins, and is metabolized in the liver where it is conjugated to a glucuronide and excreted in the bile. The P2Y12 receptor acts by inhibiting adenylyl cyclase via a Gi protein and potentiates dense granule secretion, procoagulant activity, and platelet aggregation. Inhibition of the P2Y12 receptor became a recent focus of clinical drug development and licensing. The P2Y1 receptor initiates platelet aggregation and the P2Y12 receptor amplifies and completes the aggregation process. Continued stimulation of P2Y12 receptors is needed to prevent platelet disaggregation. The active metabolite of prasugrel is metabolized to two inactive compounds by S-methylation or conjugation with cysteine. Because the bond is covalent it is essentially irreversible; thus platelets exposed to the active thiol are affected for the remainder of their life span (about 710 days). Return of global platelet function requires the generation of a new platelet pool. For prasugrel and clopidogrel, repeat daily doses do not lead to accumulation of the active metabolite, which has an elimination half-life of about 7 hours in both cases. Approximately 70% of the prasugrel dose is excreted in urine and 30% in feces as inactive metabolites. With both drugs the recommendation is to give a loading dose followed by a once-daily maintenance dose: a 300-mg load and 75 mg/day for clopidogrel and for prasugrel 60 mg and 10 mg/ day, respectively. Dose-dependent inhibition of platelet aggregation occurs about 2 hours after ingestion. With prasugrel, platelet inhibition reaches about 50% 1 hour after a loading dose of 60 mg. Steady-state inhibition of about 70% occurs after 3 to 5 days with a maintenance dose of 10 mg/day. Platelet aggregation returns to baseline over 5 to 9 days, reflecting production of new platelets. With clopidogrel at a dose of 75 mg once daily, platelet inhibition reaches a steady-state of 40% to 60% after 3 to 7 days. Platelet aggregation and bleeding time return to baseline about 5 days after stopping therapy. Because both thienopyridines are prodrugs, their pharmacodynamic effects could be affected by alterations in metabolism. This apparently is the case only with clopidogrel, in that prasugrel has not been shown to have significant metabolic drug interactions. Therapeutic Effects prasugrel and about 50% of clopidogrel is absorbed; this is not affected by food ingestion. The majority of the prodrug is metabolized into inactive metabolites by ubiquitous esterases.
It is active during walking downhill depression verses order 150 mg bupropion free shipping, its eccentric contraction resisting acceleration depression drugs discount bupropion online american express. It often appears to be composed of two layers depression letters order discount bupropion, superficial and deep mood disorder 10 discount 150 mg bupropion visa, and these are generally 1 Because of its anterior position mood disorder dsm 4 code bupropion 150 mg order, the tensor fasciae latae is often studied with the anterior thigh muscles for convenience. The sartorius lies superficially in the anterior compartment, within its own relatively distinct fascial sheath. Damage to one or more of the listed spinal cord segments, or to the motor nerve roots arising from them, results in paralysis of the muscles concerned. The quadriceps femoris (usually shortened to quadriceps) consists of four parts: (1) rectus femoris, (2) vastus lateralis, (3) vastus intermedius, and (4) vastus medialis. Collectively, the quadriceps is a two-joint muscle capable of producing action at both the hip and knee. The medial and lateral vasti muscles also attach independently to the patella and form aponeuroses, the medial and lateral patellar retinacula, which reinforce the joint capsule of the knee joint on each side of the patella en route to attachment to the anterior border of the tibial plateau. In A and B, the suprapatellar bursa, normally a potential space extending between the quadriceps and the femur (exaggerated for schematic purposes in C), is depicted as if injected with latex. The ability of the rectus femoris to extend the knee is compromised during hip flexion, but it does contribute to the extension force during the toe off phase of walking, when the thigh is extended. The rectus femoris is susceptible to injury and avulsion from the anterior inferior iliac spine during kicking, hence the name "kicking muscle. The details of their attachments, nerve supply, and actions of the muscles are provided in Table 5. The adductor magnus is the largest, most powerful, and most posterior muscle in the adductor group. This adductor is a composite, triangular muscle with a thick, medial margin that has an adductor part and a hamstring part. The two parts differ in their attachments, nerve supply, and main actions (Table 5. It acts with the other two "pes anserinus" muscles to From the anatomical position, the main action of the adductor group is to pull the thigh medially, toward or past the median plane. Testing of the medial thigh muscles is performed while the person is lying supine with the knee straight. The roof of the femoral triangle is formed by the fascia lata and cribriform fascia, subcutaneous tissue, and skin. The inguinal ligament actually serves as a flexor retinaculum, retaining structures that pass anterior to the hip joint against the joint during flexion of the thigh. Medial to the arch, the vascular compartment of the retro-inguinal space allows passage of the major vascular structures (veins, artery, and lymphatics) between the greater pelvis and the femoral triangle of the anterior thigh. As they enter the femoral triangle, the names of the vessels change from external iliac to femoral. Compartments of retro-inguinal space and structures traversing them to enter femoral triangle. This dissection of superior end of anterior aspect of the right thigh demonstrates the distal continuation of the structures cut in A. The triangle is bound by the inguinal ligament superiorly, the adductor longus medially, and the sartorius laterally. The femoral nerve and vessels enter the base of the triangle superiorly and exit from its apex inferiorly. Of the neurovascular structures at the apex of the femoral triangle, the two anterior vessels (femoral artery and vein) and the two nerves enter the adductor canal (anterior to adductor longus), and the two posterior vessels (profunda femoris artery and vein) pass deep (posterior) to the adductor longus. The saphenous nerve accompanies the femoral artery and vein through the adductor canal and becomes superficial by passing between the sartorius and gracilis when the femoral vessels traverse the adductor hiatus at the distal end of the canal. It runs antero-inferiorly to supply the skin and fascia on the anteromedial aspects of the knee, leg, and foot. The compartments of the femoral sheath are the: · Lateral compartment for the femoral artery. The femoral canal is the smallest of the three compartments of the femoral sheath. The femoral sheath does not enclose the femoral nerve because it passes through the muscular compartment. The femoral nerve, seen through a window in the iliac fascia, is external and lateral to the femoral sheath, whereas the femoral artery and vein occupy the sheath, as shown where the sheath is incised (B). The femoral septum is pierced by lymphatic vessels connecting the inguinal and external iliac lymph nodes. The pulsations of the femoral artery are palpable within the triangle because of its relatively superficial position deep (posterior) to the fascia lata. The perforating arteries supply muscles of all three fascial compartments (adductor magnus, hamstrings, and vastus lateralis). Orientation drawing showing the adductor canal and the level of the section shown in B. The retinacular arteries are often torn when the femoral neck is fractured or the hip joint is dislocated. The adductor canal provides an intermuscular passage for the femoral artery and vein, the saphenous nerve, and the slightly larger nerve to vastus medialis, delivering the femoral vessels to the popliteal fossa where they become popliteal vessels. In the inferior third to half of the canal, a tough subsartorial or vastoadductor fascia spans between the adductor longus and the vastus medialis muscles, forming the anterior wall of the canal deep to the sartorius. The femoral vein is the continuation of the popliteal vein proximal to the adductor hiatus. The profunda femoris vein (deep vein of thigh), formed by the union of three or four perforating veins, enters the femoral vein approximately 8 cm inferior to the inguinal ligament and approximately 5 cm inferior to the termination of the great saphenous vein. Chapter 5 · Lower Limb 557 Surface Anatomy of Anterior and Medial Regions of Thigh In fairly muscular individuals, some of the bulky anterior thigh muscles can be observed. The patellar ligament is easily observed, especially in thin people, as a thick band running from the patella to the tibial tuberosity. You can also palpate the infrapatellar fat pads, the masses of loose fatty tissue on each side of the patellar ligament. Deep in this depressed area, the large tendon of the adductor magnus can be palpated as it passes to its attachment to the adductor tubercle of the femur. The great saphenous vein enters the thigh posterior to the medial femoral condyle and passes superiorly along a line from the adductor tubercle to the saphenous opening. The femoral triangle, in the supero-anterior aspect of the thigh, is not a prominent surface feature in most people. Contusions cause bleeding from ruptured capillaries and infiltration of blood into the muscles, tendons, and other soft tissues. Another term commonly used is "charley horse," which may refer either to the cramping of an individual thigh muscle because of ischemia or to contusion and rupture of blood vessels sufficient enough to form a hematoma. A psoas abscess should always be considered when edema occurs in the proximal part of the thigh. Such an abscess may be palpated or observed in the inguinal region, just inferior or superior to the inguinal ligament, and may be mistaken for an indirect inguinal hernia or a femoral hernia, an enlargement of the inguinal lymph nodes, or a saphenous varix. Paralysis of Quadriceps A person with paralyzed quadriceps muscles cannot extend the leg against resistance and usually presses on the distal end of the thigh during walking to prevent inadvertent flexion of the knee joint. Chondromalacia patellae may also result from a blow to the patella or extreme flexion of the knee. Ossification abnormalities are nearly always bilateral; therefore, diagnostic images should be examined from both sides. Afferent impulses from the spindles travel in the femoral nerve to the L2L4 segments of the spinal cord. Diminution or absence of the patellar tendon reflex may result from any lesion that interrupts the innervation of the quadriceps. Patellar ligament Abnormal Ossification of Patella the patella is cartilaginous at birth. It ossifies during the 3rd6th years, frequently from more than one ossification center. Because the gracilis is a relatively weak member of the adductor group of muscles, it can be removed without noticeable loss of its actions on the leg. The proximal attachments of these muscles are in the inguinal region (groin), the junction of the thigh and trunk. Some vascular surgeons refer to this part of the femoral artery as the common femoral artery and to its continuation distally as the superficial femoral artery. The femoral artery may be cannulated just inferior to the midpoint of the inguinal ligament. In left cardial (cardiac) angiography, a long, slender catheter is inserted into the artery and passed up the external iliac artery, common iliac artery, and aorta to the left ventricle of the heart. This same approach is used to visualize the coronary arteries in coronary arteriography. Blood may also be taken from the femoral artery for blood gas analysis (the determination of oxygen and carbon dioxide concentrations and pressures with the pH of the blood by laboratory tests). In some cases, an arteriovenous shunt occurs as a result of communication between the injured vessels. When it is necessary to ligate the femoral artery, anastomosis of branches of the femoral artery with other arteries that cross the hip joint may supply blood to the lower limb. Some primary care physicians may not have been taught and/or may not realize that the so-called superficial femoral vein is actually a deep vein, and that acute thrombosis of this vessel is potentially life threatening. Under fluoroscopic control, the catheter is passed superiorly through the external and common iliac veins into the inferior vena cava and right atrium of the heart. A saphenous varix may be confused with other groin swellings, such as a psoas abscess; however, a varix should be considered when varicose veins are present in other parts of the lower limb. Iliopsoas muscle and fascia Femoral nerve External iliac artery and vein (cut) Inferior epigastric artery Location of Femoral Vein the femoral vein is not usually palpable but its position can be located inferior to the inguinal ligament by feeling the pulsations of the femoral artery, which is immediately lateral to the vein. In thin people, the femoral vein may be close to the surface and may be mistaken for the great saphenous vein. It is important therefore to know that the femoral vein has no tributaries at this level, except for the great saphenous vein that joins it approximately 3 cm inferior to the inguinal ligament. Strangulation of a femoral hernia may occur because of the sharp, rigid boundaries of the femoral ring, particularly the concave margin of the lacunar ligament. Strangulation of a femoral hernia interferes with the blood supply to the herniated intestine. ¨ Major muscles of this compartment atrophy rapidly with disease or disuse, requiring physical therapy to retain or restore function. ¨ these muscles are adductors of the thigh, innervated primarily by the obturator nerve. ¨ the primary neurovascular bundle of the thigh, like that of the arm, is placed on the medial side of the limb for protection. Neurovascular structures and relationships in anteromedial thigh: In the upper third of the thigh, the neurovascular bundle is most superficial as it enters deep to the inguinal ligament. ¨ the femoral vessels bisect the femoral triangle, where the primary vessels of the thigh, the profunda femoris artery and vein, arise and terminate, respectively. ¨ the vascular structures then pass through the adductor hiatus, becoming popliteal in name and location in the distal thigh/posterior knee region. The greater sciatic foramen is the passageway for structures entering or leaving the pelvis. These muscles all have proximal attachments to the posterolateral (external) surface and margins of the ala of the ilium, and are mainly extensors, abductors, and medial rotators of the thigh. The gluteal muscles (gluteus maximus, medius, and minimus and tensor fasciae latae) form the bulk of the region. The posterior sacro-iliac ligament is continuous inferiorly with the sacrotuberous ligament. The sacrotuberous and sacrospinous ligaments convert the greater and lesser sciatic notches into foramina. These muscles all have distal attachments on or adjacent to the intertrochanteric crest of the femur. These muscles are lateral rotators of the thigh, but they also stabilize the hip joint, working with the strong ligaments of the hip joint to steady the femoral head in the acetabulum. You do not sit on your gluteus maximus; you sit on the fatty fibrous tissue and the ischial bursa that lie between the ischial tuberosity and skin. The gluteus maximus slopes inferolaterally at a 45° angle from the pelvis to the buttocks. Three bursae (trochanteric, gluteofemoral, and ischial) usually separate the gluteus maximus from underlying bony prominences. The gluteus maximus functions primarily between the flexed and standing (straight) positions of the thigh, as when rising from the sitting position, straightening from the bending position, walking uphill and up stairs, and running. It is used only briefly during casual walking and usually not at all when standing motionless. Paralysis of the gluteus maximus does not seriously affect walking on level ground. Because the iliotibial tract attaches to the femur via the lateral intermuscular septum, it does not have the freedom necessary to produce motion at the knee. Testing the gluteus maximus is performed when the person is prone with the lower limb straight. The person tightens the buttocks and extends the hip joint as the examiner observes and palpates the gluteus maximus. Bursae are membranous sacs lined by a synovial membrane containing a capillary layer of slippery fluid resembling egg white. This bursa is commonly the largest of the bursae formed in relation to bony prominences and is present at birth. The ischial bursa separates the inferior part of the gluteus maximus from the ischial tuberosity; it is often absent.
References
- Lenze EJ, Rogers JC, Martire LM, et al. The association of late-life depression and anxiety with physical disability: A review of the literature and prospectus for future research. Am J Geriatr Psychiatry 2001;9(2):113-35.
- Weinstein MR, Goldfield MD: Cardiovascular malformations with lithium use during pregnancy. Am J Psychiatry 1975; 132:529-531.
- Diel R, Seidler A, Nienhaus A, et al. Occupational risk of tuberculosis transmission in a low incidence area. Respir Res 2005; 6: 35.
- Allen GS, Ahn HS, Preziosi TJ, et al. Cerebral arterial spasm: a controlled trial of nimodipine in patients with subarachnoid hemorrhage. N Engl J Med 1983;308:619-624.