
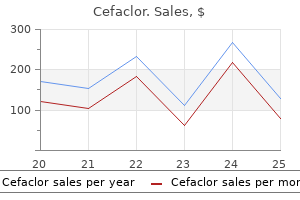
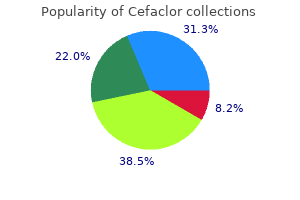
Cefaclor
| Contato
Página Inicial
Ralph Augostini, MD, FACC
- Co-Director, Electrophysiology Fellowship Program
- Assistant Professor of Clinical Medicine
- Department of Cardiovascular Medicine
- The Ohio State University
- Columbus, Ohio
Newborn infants may exhibit vasoconstriction of the extremities (acrocyanosis) and may have wide fluctuations in red blood cell content (hematocrit) medicine 93 3109 250 mg cefaclor fast delivery, as well as blood volume medicine ketorolac generic 500mg cefaclor. The formation of a superficial vascular plexus is also associated with increased convolution of the undersurface of the epidermis (rete peg formation) symptoms xeroderma pigmentosum buy cheapest cefaclor, which is a hallmark of the mature human epidermis treatment centers for alcoholism buy 250mg cefaclor fast delivery. Abnormal development of the cutaneous vasculature medications you cannot eat grapefruit with buy cefaclor 250 mg low cost, such as infantile hemangiomas, and the role of growth factors, such as vascular endothelial growth factor, have been reviewed elsewhere. This organism rapidly colonizes the skin surface and is the predominate organism on the skin of most neonates. Normally, commensal bacterial flora plays a protective role, and recent evidence suggests that organisms such as Staphylococcus epidermidis may up-regulate expression of antimicrobial peptides, such as human -defensin 2 and phenol-soluble modulins. Natural skin products, such as vernix caseosa, have been reported to function as an endogenous skin cleansers that readily remove topical soils, such as carbon particles. These natural functions should be incorporated into the design of exogenous skin cleansing regimens. Vernix caseosa has also been demonstrated to contain multiple antimicrobial peptides, including lactoferrin and lysozyme. In addition to terminal differentiation and formation of the stratum corneum, keratinocytes have been reported to internalize bacteria, leading to bacterial death and containment of infection. Breach of the epidermal barrier leads to exposure of Langerhans cells to microorganisms and other potentially pathogenic material. Their density and function within preterm epidermis have not been extensively explored. Thegradualdevelopment of papillary buds and organization of the subpapillary plexus from birth (A) to 3 months of age (B-D) and the vascular pattern at 3 monthsofage(E). Immaturity of the dermis and the cutaneous appendages poses problems of lesser magnitude for very-low-birth-weight infants. This effect is believed to be secondary to xeric stress imposed by the dry environment. The rapid transition from the sticky, wet, translucent skin surface of a very-low-birth-weight infant to the dry, opaque stratum corneum of an older preterm infant is familiar to infant caregivers. Such rapid formation of the stratum corneum often results in excessive desquamation and scaling several weeks after preterm birth. Measurements of transepidermal water loss and surface electrical capacitance have been used to track the rate of barrier formation after preterm birth. Other skin conditions characterized by rapid epidermal turnover, such as atopic dermatitis and psoriasis, have similar high water loss rates. Care must be exercised to avoid toxic substances, which can enter the body via a transdermal route. Gaseous movement across the skin surface, facilitated by local skin heating, is the basis for the use of transcutaneous gas electrodes in clinical practice. The first week of life is a vulnerable period, particularly in developing countries, when 50% to 70% of fatal and life-threatening neonatal illnesses occur, many of which are infectious complications associated with preterm birth. Increasing the humidity within a convective incubator, for example, creates a microenvironment in which transepidermal water loss is lessened. A similar microenvironment can be created under semipermeable membranes with the infant lying beneath radiant warming devices. High humidities, however, may result in "rain-out" with obscuration of the infant. Radiant warming devices increase transepidermal water loss and require a concomitant increase in fluid replacement rates. The increase in transepidermal water loss with infrared warmers is due entirely to the low humidity of the overlying air rather than any direct drying effect of the infrared radiation. Vohra and colleagues142 studied the use of polyethylene films on premature infants in the delivery room. This study reported better temperature stability and a significant decrease in mortality in extremelylow-birth-weight infants treated with vapor-reducing occlusive membranes at birth. This approach highlights the "golden hour" concept of care originally developed for treatment of adult patients after stroke and myocardial infarction. Attention to environmental temperature, humidity, adhesive application, and the presence or absence of surface biomaterials such as vernix plays a role in delivery room management. One innovative approach for enhancing epidermal barrier function is application of topical lipid-rich emollients to the skin surface. Darmstadt and colleagues150 examined the effects of a variety of naturally occurring vegetable oils on the skin barrier. The goal was to identify safe, inexpensive vegetable oils available in developing countries that might improve epidermal barrier function in very-low-birth-weight infants. When vegetable oils were applied to barrier-compromised skin of adult hairless mice, oils rich in linoleic acid enhanced epidermal barrier formation. In contrast, mustard oil, a topical emollient used routinely in newborn care throughout South Asia, had toxic effects on the epidermal barrier. The investigators noted that emollients containing a physiologic balance of epidermal lipids (3: 1: 1 molar ratio of cholesterol, ceramide, and fatty acids) may be optimal for barrier repair. Such oils provide a simple, inexpensive, and effective alternative for topical use. A recent metaanalysis of seven studies in preterm infants in low-resource countries using topical emollients (sunflower oil, coconut oil, soybean oil) concluded that such traditional intervention significantly reduces infection and mortality and improves weight gain in moderately preterm infants. Transepidermal water loss, skin hydration, rate of moisture accumulation, and erythema were measured. This finding is consistent with a role for vapor permeability to regulate epidermal barrier formation. Using the same model in adults, Visscher and colleagues153 demonstrated that the application of vernix caseosa results in improved initial hydration (compared with no intervention) and an improved moisture accumulation rate as compared with the use of an oil-in-water cream. Vernix-mediated improvement in epidermal barrier function was also demonstrated in a tapestripped murine model. Therapeutic strategies may result from a combination of individual methods optimized for a specific infant. For example, the efficacy of prenatal glucocorticoid therapy to accelerate epidermal barrier maturation is well documented for rodent skin and for fetal lung maturation. This material is self-cleaning and self-assembling and possesses sensing and actuating properties putatively secondary to the piezoelectric and piezomechanical properties of the contained keratin filaments. Interfacing with the environment is a function of the material in which the nerve endings are embedded. This perspective applies an engineering view to the material properties of the skin surface and is important for understanding innovative approaches to interactions between the skin and the central nervous system as suggested by Ansel and colleagues169 Thus the stratum corneum and the epidermal/dermal matrix are potential mediators of sensory signal processing. Biophysical properties of the skin can be easily measured with noninvasive instrumentation. In particular, study of the electrical properties of the skin may be relevant for very-low-birth-weight preterm infants. By contrast, the electrical resistance of the epidermal barrier in verylow-birth-weight preterm infants is likely to be low owing to relative deficiency of vernix and stratum corneum. Wakai and colleagues174 demonstrated the development of a high electrical impedance barrier in utero during the last trimester of pregnancy. During the first half of gestation, the amplitude of the fetal electrocardiogram can be measured directly from the surface of the maternal abdomen. After 26 to 27 weeks of gestation, the amplitude gradually disappears, concomitant with the intrauterine development of an epidermal barrier consisting of vernix caseosa and the stratum corneum. Evaluation of sensory competency is difficult; however, studies in newborn infants typically use developmental scoring systems, which rely heavily on tests of motor skills or behavior. The idea that the sensory system is precocious in early human development places the skin in a strategic location to affect subsequent development. Neonatal animals, such as kittens and rodents, have proved to be useful models to study the effect of sensory inputs on central nervous system development. In humans, clinical studies have demonstrated various effects of tactile stimulation during infancy. Field and colleagues showed that massage of hospitalized preterm infants results in greater weight gain, shorter length of hospital stay, and improved behavorial scores. Division of Research and Advanced Studies, College of Pharmacy, Cincinnati, Ohio, 1995, University of Cincinnati, p 173. This process presumably reflects growing fetal autonomy with electrical isolation of the fetus from the mother. After birth, the electrical resistance of the skin of the term newborn is relatively high. New advances in monitoring, such as evoked potential testing of the brain, hold great promise for the assessment of multiple clinical conditions such as birth asphyxia. From a practical standpoint, the field of evoked potential testing in newborns could be improved by focus on the electrode-skin interface and the development of a seamless electrical contact, which avoids wounding the skin. Experimental interference with several sensory modalities, such as vision, touch, and hearing, results in profound anatomic, functional, and biochemical impairment of the central nervous system structures that regulate such modalities. Schanberg and colleagues163-165,180 have studied the link between tactile stimulation and the molecular regulation of internal cellular growth-promoting enzymes, such as ornithine decarboxylase, which is a sensitive index of the maturation and growth of internal organs such as the heart, liver, and brain. Brain, liver, and heart ornithine decarboxylase levels are decreased by 35%, 81%, and 53%, respectively, when rat pups are removed from their mothers for periods as short as 1 hour. In other work, tactile stimulation of neonates influences circulating levels of lactate, an important energy substrate for brain metabolism. These same stimuli fail to elicit an increase in serum lactate levels at 1 week of age. These results are noteworthy because the brain of the early suckling rat uses lactate in preference to other metabolic fuels such as glucose and 3-hydroxybutyrate. This experiment demonstrates, in an animal model, that sensory interaction between the organism and the environment is a potential regulator of the availability of cerebral energy substrates. The concept that the human newborn infant is precocious in terms of sensory capabilities and relatively helpless in terms of motor capabilities159 provides a conceptual framework within which to investigate the complex maturation of sensorimotor feedback loops. Ruffini organs are deep, slowly adapting structures for stretch and/or warmth sensing. Free nerve endings are associated with crude touch, itch, pain,andtemperaturesensations. Skinconductancemeasured on the sole of the foot shows a sharp increase over the first minute in response to a heel prick on the other side. The cutaneous flexor response is elicited by stimulation of the foot with nylon filaments (von Frey hairs) of graded thickness. The accessibility of the skin surface and the availability of multiple biomedical instruments for noninvasive measurement provide an open area for skin-based research in neonatology, with potential relevance for central nervous system organization and control. The concept of a smart material interface presumes that changes in the biophysical properties of the skin surface will have a direct influence on adaptive environmental interfacing and sensorimotor response loops. This "emotional" sweating is easily measured from the palm or sole with a skin evaporimeter185 but is usually estimated indirectly by measurement of skin electrical conductance or resistance. Various instruments are now available for directly, simply, and noninvasively measuring skin surface conductance at the bedside. This response is characteristic of the change in skin conductance caused by arousal in a neonate. Confirmatory measurements can also be made using different techniques, such as transepidermal water loss. Results are displayed according to equivalent gestational age(gestationpluspostnatalage). Thevaluesare10to30g/m2/hour until the equivalent gestational age of 36 weeks is reached. This skin-based method, combined with sensory evoked potential testing, offers a new technique for assessment of central nervous system functioning in developing preterm infants. Studies of epidermal barrier function may exhibit not only short-term responses secondary to autonomic nervous system activation of eccrine sweating but also long-term consequences related to stress and glucocorticoid secretion. Denda and colleagues191,192 showed that stressful events such as immobilization, overcrowding, and abrupt change in physical environment can result in impaired epidermal barrier function in murine skin. Similarly, Garg and colleagues193 demonstrated a delay in recovery of epidermal barrier function after induced trauma in a group of psychologically stressed graduate students. These studies indicate a link between physiologic stress of the organism and epidermal barrier function. As presented earlier, a very-low-birthweight preterm infant exhibits compromised barrier function up to 28 days after delivery. The idea of the skin as an information-rich surface can be extended to the intensive care or emergency department setting. Given the ready accessibility of the skin surface and the plethora of noninvasive measurement techniques that have yet to be applied to the study of newborn physiology,171 it seems reasonable to assume that a number of innovative and useful skin-based sensing systems will be designed for clinical decision making in the future. De Felice and colleagues197 for example, used skin colorimetry to provide a significant quan- titative predictor of illness severity in hospitalized newborns. This work supports the hypothesis that noninvasive measurements of skin physical properties directly reflect the pathophysiologic state of infants. Such measurements can be used as objective adjuncts to clinical decision making and bedside assessment. Given the close embryologic connection of the skin and the brain, it is not surprising that there is a strong functional overlap between perception of the body surface and correlative neurobehavior. The most commonly used clinical assessment tool for determining gestational age. Best estimates of gestational age are important for prediction of clinical outcomes and as a guide for physiologic development and expectant management by the newborn caregiver. Finally, recent advances in three-dimensional/four-dimensional fetal ultrasound imaging have resulted in an unprecedented ability to image the body surface in utero. Four-dimensional reconstruction allows temporal visualization of fetal behavior such as yawning and response to external stimuli such as touch. This technology forms the basis for a new prenatal correlate of the postnatal Ballard score. These technologic advances require further research regarding safety and efficacy but point to a possible new frontier in fetal skin research and correlative neurobehavior.
Whether plugging in the first trimester can completely block intervillous blood flow or possibly retains cellular elements of the blood remains subject to further discussion 5 medications generic cefaclor 250mg amex. This functional separation ensures unrestricted maternal blood supply to the placenta treatment yeast infection home remedies cefaclor 500mg order online, regardless of maternal attempts to regulate the blood flow distribution within her own body; the mother cannot reduce the nutrient supply to the placenta without decreasing the nutrient supply to her own tissues medicine list buy cefaclor 500 mg on line. However medicine look up drugs buy cefaclor 250mg without a prescription, several different hypotheses concerning the nature of this impairment have been proposed treatment 6 month old cough purchase cefaclor 250 mg overnight delivery. The classic view is that of a general defect of trophoblast invasion,45 possibly resulting from impaired integrin expression. It is still unclear what features of the human placenta during the second half of pregnancy are connecting the early events to the late appearance of the symptoms. They are interpreted as dislocations of basal plate tissue into the intervillous space, caused by lateral movement and folding of the uterine wall and basal plate over each other. Parts of such septa detached from the basal plate and then attached to neighboring villi are called cell islands. Similar islands, without decidual contribution, may be formed from villous tips that have not been opened up by connective tissue and fetal vessels during transition from primary to tertiary villi. In such cases, the cytotrophoblastic core proliferates and subsequently becomes largely transformed into fibrinoid. These cell islands are growth zones for the attached villous stems comparable with cell columns. With complete implantation, the decidua recloses over the blastocyst, bulging into the uterine lumen, and is called the capsular decidua. With the increasing diameter of the chorionic sac, the capsular decidua locally touches the parietal decidua of the opposing uterine wall. Between weeks 15 and 20 after conception, both decidual layers fuse with each other, thereby obstructing the uterine cavity. From this point onward, the smooth chorion has contact over nearly its entire surface with the decidual surface of the uterine wall and may function as a paraplacental exchange organ. Owing to the absence of fetal vascularization in the smooth chorion and the amnion, all paraplacental material exchanged between fetal membranes and fetus has to pass through the amniotic fluid. The mean thickness of the membranes, after separation from the uterine wall during labor, is approximately 200 to 300 µm. Amniotic epithelium may be involved in the production of the latter and even partially responsible for its resorption. The next layer consists of chorionic connective tissue, which is directly adherent to a cytotrophoblastic layer of variable thickness. Attached to the outer surface of the cytotrophoblast is a decidual layer approximately 50 µm thick. The latter finding indicates that the separation of membranes does not take place along the maternofetal interface but instead occurs at a somewhat deeper level. Between 8 and 10 weeks after conception, the amniotic sac has expanded to such a degree that the amniotic mesenchyme comes into close contact with the mesenchymal surface of the chorionic plate and the chorion laeve (smooth chorion). As part of the same process, the expanding amniotic sac surrounds the connective stalk and the allantois and joins them to form the umbilical cord. The allantoic vessels-two arteries and one vein-grow in thickness and length and convert into the umbilical vessels. The allantoic epithelium gradually disappears; small vesicular remnants of the allantois, however, may persist until term. The allantoic mesenchyme differentiates into a complex system of myofibroblasts that probably help in regulating turgor of the cord and avoid bending of the latter with fatal consequences for the fetus. The cord is characterized by a spiral twisting, the number of spiral turns increasing as pregnancy progresses, up to a maximum of 380 turns. The other parts of the blastocystic circumference, implanted a few days later, undergo a corresponding although delayed development that is quickly followed by regressive changes. The newly formed villi degenerate, and the surrounding intervillous space is obliterated. As a consequence of obliteration of the intervillous space, the chorionic plate, villous remnants, and the basal plate fuse into a multilayered compact lamella, the smooth chorion (chorion laeve). Formation of the smooth chorion starts opposite to the implantation pole at the so-called anti-implantation pole. From there it spreads over Chapter10-PlacentalDevelopment 113 movements of the fetus resulting from asymmetric uterine contractions. Demir R, Kaufmann P, Castellucci M, et al: Fetal vasculogenesis and angiogenesis in human placental villi. Castellucci M, Schweikhart G, Kaufmann P, et al: the stromal architecture of the immature intermediate villus of the human placenta. Kohnen G, Kertschanska S, Demir R, et al: Placental villous stroma as a model system for myofibroblast differentiation. Graf R, Matejevic D, Schuppan D, et al: Molecular anatomy of the perivascular sheath in human placental stem villi: the contractile apparatus and its association to the extracellular matrix. Graf R, Neudeck H, Gossrau R, et al: Elastic fibres are an essential component of human placental stem villous stroma and an integrated part of the perivascular contractile sheath. Castellucci M, Kosanke G, Verdenelli F, et al: Villous sprouting: fundamental mechanisms of human placental development. Castellucci M, Scheper M, Scheffen I, et al: the development of the human placental villous tree. Graf R, Schonfelder G, Muhlberger M, et al: the perivascular contractile sheath of human placental stem villi: its isolation and characterization. Gauster M, Huppertz B: the paradox of caspase 8 in human villous trophoblast fusion. Lamkanfi M, Festjens N, Declercq W, et al: Caspases in cell survival, proliferation and differentiation. Baczyk D, Drewlo S, Proctor L, et al: Glial cell missing-1 transcription factor is required for the differentiation of the human trophoblast. Frendo J, Cronier L, Bertin G, et al: Involvement of connexin 43 in human trophoblast cell fusion and differentiation. Castellucci M, Theelen T, Pompili E, et al: Immunohistochemical localization of serine-protease inhibitors in the human placenta. Kemp B, Kertschanska S, Kadyrov M, et al: Invasive depth of extravillous trophoblast correlates with cellular phenotype: a comparison of intra- and extrauterine implantation sites. Lacey H, Haigh T, Westwood M, et al: Mesenchymally-derived insulin-like growth factor 1 provides a paracrine stimulus for trophoblast migration. Moll W, Nienartowicz A, Hees H, et al: Blood flow regulation in the uteroplacental arteries. Mühlhauser J, Crescimanno C, Rajaniemi H, et al: Immunohistochemistry of carbonic anhydrase in human placenta and fetal membranes. Rosenfeld Pregnancy is associated with numerous alterations to the maternal cardiovascular system; however, it is the development of the low-resistance, high-flow placental vascular bed that characterizes this physiologic state. Moreover, this vascular bed is unique in that it is composed of maternal and fetal components separated by several cell layers that differ in structure and function among the mammalian species studied. Thus conclusions about the relative importance of the mechanisms responsible for the control of blood flow to these vascular beds in the human continue to require careful interpretation. Thus sheep studies provide an excellent basis for characterizing this aspect of pregnancy and improving our understanding of clinical data obtained in Doppler flow velocity studies in women. Both vascular beds undergo substantial independent modification throughout pregnancy. For example, the maternal uterine vasculature undergoes remodeling,12 and the fetal vasculature exhibits ongoing vasculogenesis, angiogenesis, and branching morphogenesis. Understanding these independent yet parallel modifications will facilitate our knowledge of fetal growth, maintenance of fetal well-being, and possibly the origins of some pregnancy-related diseases. In women the uteroplacental vascular bed is composed of cotyledons, lobes, or placentomes similar to those seen in many species. Nonetheless, they can be identified as individual structures when viewed from the basal or maternal side of the placenta after its delivery. Each placentome receives its maternal arterial blood by way of a single spiral artery, and alterations in the tone of these and/or more proximal branches of the uterine artery are responsible for modifying the magnitude and distribution of maternal uteroplacental blood flow. Therefore the rise in maternal uteroplacental blood flow during pregnancy is initially due to the development of the placenta. This increase is coincident with a doubling of maternal cardiac output and an increase in the proportion of cardiac output directed to the uterus, increasing from less than 1% of cardiac output in nonpregnant sheep to nearly 25% at term. The first is associated with relatively low absolute blood flows, which on the basis of uterine plus conceptus wet weight is actually high, achieving values of 0. This increase in uterine blood flow is believed to reflect vasodilation secondary to the increased production of maternal ovarian and possibly fetal hormones. The second phase is associated with the development of the fetal placentomes and, in the primate, with the development of the intravillous spaces or the maternal placental vascular bed. At this time the anatomic maternal placental vascular bed achieves its maximum size. If this does not occur, placentation will be restricted, resulting in a small placenta and a fetus characterized by proportionate growth restriction. In sheep, total uterine blood flow plateaus at this time, averaging approximately 500 mL/minute; however, blood flow expressed on a weight basis at the same point in gestation, which takes into account metabolically active tissues, has fallen by 50% to 0. The final phase in the "growth" of uterine blood flow is exponential and associated with a threefold increase in fetal weight that occurs in the last third of pregnancy or after 110 days in sheep (75% of gestation) and beyond 30 weeks in humans (75%). Fetal growth is attenuated until adaptation has occurred and this ratio is reestablished, at which time a new growth curve is established that lies below the curve for normally growing fetuses. The dramatic rise in total uterine blood flow during pregnancy actually reflects changes in three separate vascular beds within the gravid uterus: the placentomes, endometrium, and myometrium. The change in distribution of blood flow to these tissues cannot be determined in women but has been studied in sheep and other species. As pregnancy progresses, a gradual redistribution of uterine blood flow occurs, such that at term the placentomes (cotyledons) receive nearly 90% of total uterine blood flow. Thus in the last third of pregnancy, perfusion of the placentomes accounts for most of the observed increase in uterine blood flow. The placentome is the site of nutrient and gas exchange; therefore fetal well-being is determined by changes in placental development, growth, and perfusion. This discordance in placental growth and blood flow occurs earlier in pregnancy in women and other primates compared with sheep. In contrast to the high value for total uterine blood flow 100 Placental cotyledons (R = 0. Closed circle, twin pregnancy; open circle, singleton pregnancy; square,nonpregnant. Placental weight and blood flow in the twin gestations are the sum for the two placentas. Closed circle, twin pregnancy; open circle, singleton pregnancy; square, nonpregnant. For example, a villous stem originating from the fetal side of the placenta contains a distal branch of the umbilical artery and vein. As pregnancy progresses, a villous tree (in the human) or vascular bed originating from this villous stem undergoes angiogenesis and branching morphogenesis throughout pregnancy, providing an ever-enlarging fetal placental vascular bed and surface area for nutrient and gas exchange by term pregnancy. Although the sheep has no villous tree, continued growth of the fetal placental vascular bed occurs as in the human. Thus umbilicoplacental blood flow remains approximately 100 to 200 mL/minute per kilogram of fetal weight throughout gestation in most species. Although this correlation is not well studied, Doppler technology has shown increases in umbilical artery resistance associated with decreased fetal growth. This section reviews how these agents may affect placental perfusion and fetal well-being. The rise in perfusion pressure also exceeds that of uterine vascular resistance; thus uteroplacental blood flow increases throughout this dosage range. Importantly, maternal placental blood flow is minimally affected, and the reproductive tissues as a group are more refractory than early in pregnancy followed by a fall and leveling off, placental blood flow falls in mid pregnancy and then progressively increases from about 0. This increase in placental blood flow is due to progressive vasodilation, because maternal arterial blood pressure. Of note, the volume of placental blood flow greatly exceeds that required for normal fetal growth. Uterine arteries from pregnant ewes demonstrate a three-fold rise in the basal synthesis of prostacyclin. Modifications of these agonist-antagonist interactions likely occur in hypertensive pregnant women, resulting in uteroplacental hypoperfusion and eventually fetal growth restriction. The pressor responses to infused catecholamines- epinephrine and norepinephrine-are also attenuated in normal pregnancies44 and increased in hypertensive pregnant women. During labor, circulating catecholamine levels are elevated, and this enhanced responsiveness of the placental arteries to catecholamines can potentially endanger the growth-restricted fetus or a normally grown fetus with a small or borderline "margin of safety" by decreasing uterine oxygen delivery to dangerous levels, resulting in fetal heart rate decelerations. Thus fetal responses to catecholamines are associated with the maintenance of umbilicoplacental perfusion, as well as cerebral and myocardial blood flow. This interest stems from observations of increased circulating levels of vasodilating prostanoids in normotensive pregnant women and animals. First, prostanoids may not be circulating hormones but rather mediate their effects through paracrine mechanisms. Third, although cyclooxygenase inhibition enhances systemic and uterine vascular responses to vasoconstrictors in pregnant women and sheep, this effect does not alter basal uteroplacental blood flow commensurate with the fall in plasma prostaglandin levels. Similar controversy exists regarding the role of prostaglandins in the fetal compartment. These hormones have profound vascular effects and play important roles in promoting implantation and placentation19 and modulating placental blood flow and other aspects of maternal cardiovascular adaptation during pregnancy. Unfortunately, few investigators have examined the effects of these hormones on umbilicoplacental blood flow.
Hu X-Q medications john frew discount 250 mg cefaclor overnight delivery, Xiao D symptoms jock itch order discount cefaclor online, Zhu R medications like tramadol discount cefaclor uk, et al: Pregnancy upregulates large-conductance Ca2+activated K+ channel activity and attenuates myogenic tone in uterine arteries treatment 31st october discount cefaclor 500mg mastercard. In the last third of pregnancy medications mobic discount cefaclor 250 mg buy, fetal and maternal placental blood flows increase logarithmically, paralleling the increase in fetal weight. In conjunction with increases in placental function and surface area, the rise in blood flows increases the capacity to deliver and transfer oxygen and nutrients to the fetus. Maternal uteroplacental blood flow normally exceeds fetal-placental metabolic needs, providing a large "margin of error"; thus blood flow may acutely fall by 50% without altering oxygen and nutrient delivery. There also is enhanced local synthesis of vasodilators by the uterine and umbilicoplacental vasculature that not only increase blood flow but may also antagonize vasoconstrictor responses. In the presence of maternal hypertension, one or more of these systems may be dysfunctional, placing the fetus at risk for long-term and shortterm episodes of hypoxia via increased sensitivity to intracellular calcium and circulating vasoconstrictors. The contribution of each mechanism remains to be determined in order to develop new strategies to maintain placental blood flows and ensure fetal well-being. Hu X-Q, Xiao D, Zhu R, et al: Pregnancy upregulates large-conductance Ca2+-activated K+ channel activity and attenuates myogenic tone in uterine arteries. Italian Study of Aspirin in Pregnancy: Low-dose aspirin in prevention and treatment of intrauterine growth retardation and pregnancy-induced hypertension. Sibley 12 It has been known since the eighteenth century that the circulation of the human fetus is kept separate from that of the mother by intervening placental tissue. The evidence linking altered placental transporter activities with anomalous fetal growth is also reviewed. Corresponding functional differences are recognized in the mechanisms and degree of transfer of certain solutes, notably immunoglobulin G (IgG) (transferred by the yolk sac in rabbits, by the placenta in women, and not transferred in sheep) and iron (transferred by red blood cells in sheep and cats, and by receptor-mediated transfer from plasma transferrin in women). Most other transport systems have been observed in the majority of species studied, but few extensive cross-species sets of data are available. An additional major interspecies difference is in the balance between diffusional and carrier-mediated transplacental transport. Hemochorial placentas are considerably more permeable than epitheliochorial placentas to lipid-insoluble molecules for which no specific transport systems exist-such molecules are presumed to leak across the placenta by diffusion through "pores. These differences must be borne in mind when one is extrapolating conclusions drawn from one species to another. This article provides examples of the main mechanisms of transplacental transfer and focuses predominantly on data obtained in humans and on those substances with net transfer toward the fetus. In the case of urea, carbon dioxide, and bilirubin, for example, net transfer is in the opposite direction. The methodological approaches used in humans on which the results discussed hereafter are based are summarized in Table 12-1. Accordingly, definitions of commonly used anatomic descriptions and terms are provided in Table 12-2. Their transfer is slow, owing to the small surface area of this pathway, and is limited by both the size of the molecule and the membrane characteristics (permeability and pore size); thus it is said to be membrane limited. Nonphysiologic hydrophobic permeants (including mannitol, sucrose, inulin, chromium-labeled ethylenediaminetetraacetic acid, and high-dose vitamin B12) have been used to assess placental permeability because they do not possess specific transporters (or because, as in the case of vitamin B12, the transport systems were saturated during studies). The net rate (Jnet) of diffusional transfer of a given solute from maternal to fetal blood is influenced by the surface area available for transfer, the permeability of the placenta, and the maternal-fetal concentration difference. Two pathways are available for diffusion: a hydrophilic route for lipid-insoluble molecules and a lipophilic route. Their relative importance in determining Jnet is determined by the degree of solubility in lipid of the molecule of interest. Such a relationship is most easily explained by diffusion through paracellular channels or pores sufficiently wide to allow free diffusion of low-molecular-weight substances (smaller than proteins). The epitheliochorial sheep placenta has reduced permeability to larger hydrophilic molecules,39 possibly because the channels have a radius some 10 to 20 times smaller than in human and other hemochorial placentas. For calcium, in vitro data suggest that the paracellular route contributes approximately 50% of total maternal-fetal transfer,57 with the remainder due to active transcellular transfer. Chloride, phosphate, and sulfate are maintained at higher concentrations in fetal plasma than in maternal plasma,11 and therefore transcellular active transport is likely to be involved in the translocation of these ions; the components of such routes certainly exist. These workers hypothesized that under normal conditions of hydrostatic pressure, the channels are too narrow to be resolved by electron microscopy. They failed, however, to show channels that are simultaneously open to both the maternal side and the fetal side of the syncytiotrophoblast; the absence of such channels may not be surprising in view of the small number of channels overall required to explain the permeability data. Because of the large surface area involved, the placenta is highly permeable to such substances, and the transport rate depends predominantly on Cm and Cf, which, in turn, depend on the geometric relationships of the maternal and fetal bloodstreams and their flow rates. Therefore, relatively lipophilic molecules, such as respiratory or anesthetic gases, are said to demonstrate flow limitation in their permeability pattern. The human placenta probably belongs to an anatomically intermediate type of exchanger5 in that, on the fetal side, there are hairpin-like capillary loops, with opposite flow directions in each limb. Placental structure may include a population of extracellular channels small enough to exclude mannitol (the smallest extracellular tracer studied so far in humans) but large enough to let through some excess sodium (indicating heterogeneity of pore size). Paracellular diffusion of sodium may be accelerated by a transplacental potential difference between the fetal capillary and the intervillous space (with the fetal side negative). Some evidence suggests a potential difference in certain species but other data are contradictory. Maternal-fetal sodium transport may be partly transcellular, affected by the various sodium-linked transport systems demonstrable in trophoblast membrane vesicle preparations. In sheep and monkeys, however, these two values are not identical64 because of shunting (some maternal and fetal blood does not pass close to the site of exchange) or uneven perfusion (maternal-fetal blood flow ratios that are different between different segments of the placenta). In addition, the placenta and membranes can consume considerable amounts of oxygen from the uterine circulation. In receptor-mediated transport, the specific receptors always become associated with specialized regions of the plasma membrane called coated pits, which on electron microscopy can be seen to be covered with a "coat" of the protein clathrin. In other tissues, many vesicles fuse with lysosomes, and for some macromolecules, such as low-density lipoproteins in fibroblasts, this is the last step of the process. Transsyncytial movement of vesicles may occur by diffusion down a concentration gradient from the site of endocytosis to the other side. Alternatively, as in secretory cells, microtubules and other components of the cytoskeletal system may direct vesicle shuttling. It is well known that in most species fetal hemoglobin has a higher affinity for oxygen than does maternal hemoglobin (the oxyhemoglobin dissociation curve is shifted to the left). Generally, endocytosis cannot occur without exocytosis, as areas of plasma membrane that are continuously lost from a cell surface must be continuously replaced to maintain the polarity of the epithelium. Although investigations of the role of endocytosis and exocytosis in the placental transfer of proteins and other macromolecules have generally focused on the syncytiotrophoblast, the fetal capillary endothelium also provides a considerable barrier to the exchange of such molecules. Endocytosis is classically divided into two types: phagocytosis, the process by which large particles are ingested; and pinocytosis, the process by which small solutes and water are absorbed. Iron transport may use the former process in the sheep,68 but in the human the latter process is relevant to placental transport. Low-density lipoprotein, the transferrin-iron complex, and IgG all probably gain entry to the human placental syncytiotrophoblast by endocytosis. Transfer of iron to the fetus may involve an exocytotic process as well, but not until after some intracellular processing has occurred that results in the return of transferrin to the maternal plasma. In other species, particularly rabbits, guinea pigs, and rodents, this function is served by the yolk sac placenta rather than by the chorioallantoic placenta. The pioneer of these studies, Brambell,87 suggested that uptake of IgG is by a nonselective process, but subsequent binding to receptors selectively prevents its degradation in phagolysosomes, allowing release of the intact molecule on the fetal side. The identification of specific Fc receptors by placental cells,73 however, suggests that IgG transfer is accomplished through receptor-mediated endocytosis (reviewed by Wild86). This proposed mechanism is supported by the fact that maternal-fetal immunoglobulin transfer is highly selective (IgG, but not immunoglobulin A or immunoglobulin M, crosses the placenta, and transfer of IgG1 is greater than that of other IgG subclasses). Interference with this pathway by inactivation of mutations of FcRn reduces IgG transfer to the fetus. As Barcroft91 pointed out, the net molar flux of water into the fetus is greater than that of any other substance, including oxygen. From kinetic analysis of plasma and amniotic fluid deuterium oxide concentrations, Hutchinson and colleagues92 concluded that at 40 weeks of gestation, the unidirectional flux of water across the human placenta is approximately 60 mL/minute in both directions, some 10,000 times the net flux. The main reasons for asymmetrical unidirectional fluxes and thus for net water flux across the placenta are likely to be hydrostatic and osmotic pressure differences between fetal and maternal placental microcirculations. For example, acutely increasing the osmotic pressure of either maternal or fetal plasma by injection of hypertonic solutions leads to net flux of water out of the fetus or mother in primates,94 rabbits,95 and sheep. The factors regulating water acquisition remain somewhat obscure for at least two reasons. First, the reflection coefficients across placenta for the many solutes present in plasma are unknown. Accordingly, calculation of the total effect of osmotic pressure of fetal and maternal plasma from knowledge of their individual solute concentrations,4 or from freezing point depression or colloid osmometry data, cannot be accomplished. Second, solute concentrations in plasma of the microcirculation may be different from those in the large vessels from which samples have been collected. In women it is not even clear whether fetal plasma total osmolarity is higher than103 or equal to4 maternal plasma osmolarity, whereas hydrostatic pressure in the intervillous space (insofar as it can be estimated) is lower than that in the umbilical vein. A further area of uncertainty is the extent to which transplacental water flow is transcellular as opposed to paracellular. Both Faber and Hart,105 using the fetal sideperfused rabbit placenta, and Meschia and colleagues,35 using an in vivo sheep preparation, showed that the clearance of 3H2O was much greater than that predicted on the basis of molecular size alone if water had been restricted to the same paracellular route as, for example, for sodium. Illsley and Verkman106 measured the osmotic water permeability of a microvillous membrane vesicle preparation from which the paracellular route was excluded. Although uptake was found to be low compared with that of other plasma membranes, these investigators calculated that it was sufficiently high to account for the entire transplacental water flux93 without the need to invoke a paracellular route for water. Despite the many probable inaccuracies in such a calculation, it does at least appear that a proportion of transplacental water movement in the human placenta is likely to be transcellular. Such transcellular fluxes may be mediated by aquaporins, a family of membrane proteins functioning as water channels and found in the syncytiotrophoblast. On this basis, these workers further suggested that solute-free water is driven transcellularly across the placenta, driven by osmotic gradients set up by active transport of solutes. Water and dissolved solutes then return from the fetus to the mother by paracellular filtration across the placenta, the whole system runs to ensure that the net flux of water to the fetus is exactly correct. Reports of asymmetrical transfer across the perfused human placental cotyledon,109 together with the hydrostatic gradient as noted previously, suggest that a similar model could apply in humans. Despite this and several other attempts to model fetal water acquisition,93,110 the nature and control of water transfer across the placenta are poorly understood. It also remains possible that an important fraction of net water transfer between the mother and the fetus occurs extraplacentally by way of the amniochorion. These include carriers, which translocate solutes by a saturable mechanism and use energy either from prevailing electrochemical gradients (facilitated diffusion-e. Many such transporter proteins in the microvillous (maternal-facing) and basal (fetal-facing) plasma membranes of the human syncytiotrophoblast have been characterized. These transporter proteins are important for transplacental transfer or are involved in solute supply to the trophoblast for its own metabolism. Transplacental active transport can occur by means of a pump-leak or leak-pump mechanism. In the former process, the active step, localized to the microvillous membrane, generates a higher intracellular concentration of the substance than in maternal plasma, followed by a leak across the opposite plasma membrane (as is probably the case for many amino acids). In a leak-pump system, the substance is pumped out of the trophoblast at the basal plasma membrane, thereby lowering its intracellular concentration so that a leak from maternal plasma into the syncytium occurs (as is perhaps the case for calcium). Two solutes for which transporter proteins are recognized to play an essential role in maternal-fetal transfer are glucose and amino acids. This mechanism is highly efficient, and it has been shown in the isolated perfused human placental cotyledon that transplacental glucose flux is directly proportional to the maternal arterial concentration. The transporter systems are characterized on the basis of competitive interactions and are analogous to those described for other epithelia. Expression patterns across gestation indicate highly specific regulation of placental amino acid transfer; however, despite differences in substrate specificity, localization (microvillous membrane or basal plasma membrane) and predominant direction of flux, the transporters have overlapping actions. Uptake of amino acids by vesicles prepared from either the microvillous membrane or the basal plasma membrane of the syncytiotrophoblast of the human placenta has been extensively investigated. This observation suggests active transport into the syncytiotrophoblast from maternal blood, followed by a passive leak down the concentration gradient to fetal plasma. However, no intrinsic reason exists to suggest that a passive leak should not also occur from the syncytiotrophoblast into maternal plasma. The observed asymmetrical transcellular transport (maternal-fetal flux) is explained by the differential expression or activity of carriers on the microvillous and basal plasma membranes of the syncytiotrophoblast. Studies with perfused placental cotyledons have confirmed preferential maternal-fetal transfer of the neutral amino acids 154 L-leucine and L-alanine in the human placenta. In addition, a faster rate of maternal-fetal transfer has been demonstrated for aminoisobutyric acid (a nonmetabolizable amino acid analogue), 155 L-leucine, and the basic amino acid L-lysine. The fetal-maternal transfer rates of aminoisobutyric acid, L-leucine, and L-lysine are all nearly half the maternal-fetal transfer rate. Transport of these amino acids in the fetal-maternal direction is thought to occur by the paracellular route, because the transfer rates are not different from those for the extracellular marker L-glucose. These experiments have been performed with equal maternal and fetal perfusate amino acid concentrations, and the importance of paracellular transfer may be even greater in vivo because fetal plasma amino acid concentrations are higher than maternal levels. Further studies using the placental perfusion model have demonstrated that there are amino acid exchangers present on both membranes of the syncytiotrophoblast, which transport one amino acid in place of another. This helps to maintain the high concentration of amino acids within the placenta, while preventing changes in cell osmolality and sustaining a homeostatic environment for optimal placental function. It could be that the pump-leak hypothesis is an oversimplification and is not always applicable. Tryptophan, which may have an important role in immune evasion by the placenta and fetus,166 is also transported by system L. However, the fetus clearly has varying nutrient demands across pregnancy, and because fetal growth in the third trimester far exceeds that of the placenta, increased expression or activity of transporters must account for the more efficient uptake of nutrients.
American College of Obstetricians and Gynecologists Committee on Genetics: Committee Opinion No treatment hypercalcemia cefaclor 250mg buy overnight delivery. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units medicine examples discount cefaclor 250mg on line. Rizzo G medications 1-z order generic cefaclor online, Arduini D medicine to calm nerves 500 mg cefaclor order otc, Romanini C: Uterine artery Doppler velocity waveforms in twin pregnancies treatment 3rd stage breast cancer discount cefaclor 250 mg with visa. Goodnight W, Newman R: Society of Maternal-Fetal Medicine: optimal nutrition for improved twin pregnancy outcome. Luke B: the changing pattern of multiple birth in the United States: maternal and infant characteristics, 1973 and 1990. El-Chaar D, Yang Q, Gao J, et al: Risk of birth defects increased in pregnancies conceived by assisted human reproduction. Rychik J, Ayres N, Cuneo B, et al: American Society of Echocardiography guidelines and standards for performance of the fetal echocardiogram. Gratacos E, Carreras E, Becker J, et al: Prevalence of neurological damage in monochorionic twins with selective intrauterine growth restriction and inter- 176. House M, et al: Intensive management of monoamniotic twin pregnancies improves perinatal outcome. Spencer R: Anatomic description of conjoined twins: a plea for standardized terminology. Sogaard K, Skibsted L, Brocks V: Acardiac twins: pathophysiology, diagnosis, outcome and treatment. Cabassa P, Fichera A, Prefumo F, et al: the use of radiofrequency in the treatment of twin reversed arterial perfusion sequence: a case series and review of the literature. In contrast, failure of nutritional supply in the second half of pregnancy leads to asymmetric growth restriction in which fetal body weight is more affected than body length. Low amniotic fluid volume with intact membranes is most commonly associated with placental insufficiency, whereas normal or increased amniotic fluid volume implies normal placental perfusion and points to different causes, such as infections or fetal chromosomal abnormalities. In particular, it is difficult to perform mechanistic studies in pregnant women, and placental function can be explored only after delivery, typically in late gestation. Detailed studies in carefully validated animal models can provide critical pieces of information that help us better understand the pathophysiology of placental insufficiency and facilitate the development of tools for early diagnosis and specific interventions. Thus, although this chapter is focused on the human, numerous key animal experiments will be referenced and briefly discussed. Maternal calorie restriction also poses a significant problem in the United States, with nearly 50 million Americans experiencing food shortage or hunger at some time during the year. Smoking during pregnancy, an example of a modifiable risk factor, increases the risk for growth restriction 3. In addition, the mouse is the model of choice for mechanistic studies because of well-established techniques for gene targeting in this species. However, rodents are polytocous, and their metabolism differs significantly from that of the human, which needs to be taken into account when one is extrapolating data obtained in the rodent to pregnant women. Thus, in response to decreased fetal oxygen and/or nutrient availability, the fetus signals to up-regulate placental growth and nutrient transport as a compensatory mechanism. Other macroscopic placental abnormalities include unusual paleness, infarction, and loss of parenchyma. The area of unusual paleness is believed to represent decreased vascularization of chorionic villi, whereas the infarction can be recognized by a pale and indurated region in placental parenchyma. If ambient temperature is increased, maternal body temperature is elevated, which interferes with placental development, causing decreased placental oxygen diffusion and nutrient transport capacity. Mediated by a process of vascular proliferation and branching, the composition of the placenta shifts from few, large and poorly vascularized primary villi to numerous, small and highly vascularized tertiary villi. These changes could compromise placental oxygen transfer and contribute to fetal hypoxia. Notably, in normal pregnancies intraplacental thrombosis is uncommon, suggesting that factors within the placenta itself may offset the hypercoagulability observed in normal pregnancies. The proteoglycans and their glycosaminoglycan side chains play an important role in preventing thrombosis within the placenta. These aberrant patterns of umbilical artery Doppler findings are predictive of perinatal and long-term outcomes. In uteroplacental insufficiency, the changes in uterine artery resistance are reflected by an elevated pulsatility index, an elevated systolicto-diastolic ratio, and the presence of a diastolic notch in Doppler ultrasonogaphy. Genomic imprinting refers to silencing of one parental allele by methylation, leading to monoallelic expression of the gene. Decidual leukocytes, particularly uterine natural killer cells and macrophages, participate in the process of vascular smooth muscle cell apoptosis, contributing to vascular remodeling. It is possible that hypoxia/oxidative stress activates trophoblast apoptotic pathways. Placental corticotrophinreleasing hormone secreted into the fetal circulation may act via cortisol as an inhibitor of fetal growth. Although the mechanisms remain to be fully established, emerging evidence suggests that complex trophoblast signaling pathways are involved. Because fetal growth and development are critically dependent on nutrient and oxygen availability, and therefore placental function, changes in placental transport may directly alter the fetal growth trajectory. The syncytiotrophoblast is the transporting epithelium of the human placenta and constitutes the primary barrier for nutrient and oxygen flux across the placental barrier. They are the key receptors for cholesterol uptake from maternal lowdensity lipoprotein and/or high-density lipoprotein. Oxygen, which is highly lipophilic, diffuses rapidly across the placental barrier, and placental oxygen transfer is therefore primarily limited by the rate of blood flow on the two sides of the barrier, and to some degree the barrier thickness. In contrast, transplacental transport of nutrients such as glucose and amino acids is less affected by changes in blood flow because transport across the barrier is the primary limiting factor for effective transfer of these molecules. Because changes in fetal nutrient availability "program" the fetus for future disease, placental function determines lifelong health. Maternal signals conveying nutritional information to the placenta may include metabolic hormones such as cortisol, insulin, leptin, and adiponectin, which are known to reflect maternal nutritional status and regulate placental transport. Matching fetal growth to maternal resources in severe maternal undernutrition will produce an offspring that is smaller but that, in most instances, will survive and reproduce. Rather than excess extraction of nutrients from the deprived mother, which would jeopardize the survival of both the mother and her fetus, fetal growth restriction was a necessary evolutionary compromise. However, if the initial perturbation is prolonged and severe, placental dysfunction (such as impaired capacity to eliminate metabolic acid) and injury. Brosens I, Pijnenborg R, Vercruysse L, Romero R: the "great obstetrical syndromes" are associated with disorders of deep placentation. Roos S, Jansson N, Palmberg I, et al: Mammalian target of rapamycin in the human placenta regulates leucine transport and is down-regulated in restricted foetal growth. Jansson N, Pettersson J, Haafiz A, et al: Down-regulation of placental transport of amino acids precedes the development of intrauterine growth restriction in rats fed a low protein diet. Jansson T, Persson E: Placental transfer of glucose and amino acids in intrauterine growth retardation: studies with substrate analogs in the awake guinea pig. If the initial perturbation is prolonged and severe, placental dysfunction and injury may occur. Kingdom J, Huppertz B, Seaward G, Kaufmann P: Development of the placental villous tree and its consequences for fetal growth. Struwe E, Berzl G, Schild R, et al: Microarray analysis of placental tissue in intrauterine growth restriction. Harding K, Evans S, Newnham J: Screening for the small fetus: a study of the relative efficacies of ultrasound biometry and symphysiofundal height. Pereira L, Petitt M, Fong A, et al: Intrauterine growth restriction caused by underlying congenital cytomegalovirus infection. Committee on Practice Bulletins-Obstetrics, American College of Obstetricians and Gynecologists: practice bulletin no. Ego A, Subtil D, Grange G, et al: Customized versus population-based birth weight standards for identifying growth restricted infants: a French multicenter study. Dessi A, Ottonello G, Fanos V: Physiopathology of intrauterine growth retardation: from classic data to metabolomics. Todros T, Sciarrone A, Piccoli E, et al: Umbilical Doppler waveforms and placental villous angiogenesis in pregnancies complicated by fetal growth restriction. Sugimura M, Ohashi R, Kobayashi T, Kanayama N: Intraplacental coagulation in intrauterine growth restriction: cause or result Plaisier M, Rodrigues S, Willems F, et al: Different degrees of vascularization and their relationship to the expression of vascular endothelial growth factor, placental growth factor, angiopoietins, and their receptors in first-trimester decidual tissues. Lyall F, Young A, Boswell F, et al: Placental expression of vascular endothelial growth factor in placentae from pregnancies complicated by pre-eclampsia and intrauterine growth restriction does not support placental hypoxia at delivery. Wallner W, Sengenberger R, Strick R, et al: Angiogenic growth factors in maternal and fetal serum in pregnancies complicated by intrauterine growth restriction. Dunk C, Shams M, Nijjar S, et al: Angiopoietin-1 and angiopoietin-2 activate trophoblast Tie-2 to promote growth and migration during placental development. Todros T, Piccoli E, Rolfo A, et al: Review: feto-placental vascularization: a multifaceted approach. Gudmundsson S, Marsal K: Umbilical artery and uteroplacental blood flow velocity waveforms in normal pregnancy-a cross-sectional study. Gudmundsson S, Marsal K: Blood velocity waveforms in the fetal aorta and umbilical artery as predictors of fetal outcome: a comparison. Brodszki J, Hernandez-Andrade E, Gudmundsson S, et al: Can the degree of retrograde diastolic flow in abnormal umbilical artery flow velocity waveforms predict pregnancy outcome Nevo O, Many A, Xu J, et al: Placental expression of soluble fms-like tyrosine kinase 1 is increased in singletons and twin pregnancies with intrauterine growth restriction. Sagol S, Ozkinay E, Oztekin K, Ozdemir N: the comparison of uterine artery Doppler velocimetry with the histopathology of the placental bed. Hata T, Tanaka H, Noguchi J, Hata K: Three-dimensional ultrasound evaluation of the placenta. Reik W: Stability and flexibility of epigenetic gene regulation in mammalian development. McMinn J, Wei M, Schupf N, et al: Unbalanced placental expression of imprinted genes in human intrauterine growth restriction. Cecconi D, Lonardoni F, Favretto D, et al: Changes in amniotic fluid and umbilical cord serum proteomic profiles of foetuses with intrauterine growth retardation. Wolter M, Rower C, Koy C, et al: A proteome signature for intrauterine growth restriction derived from multifactorial analysis of mass spectrometrybased cord blood serum profiling. Huppertz B, Kingdom J, Caniggia I, et al: Hypoxia favours necrotic versus apoptotic shedding of placental syncytiotrophoblast into the maternal circulation. Huppertz B, Weiss G, Moser G: Trophoblast invasion and oxygenation of the placenta: measurements versus presumptions. Endo H, Okamoto A, Yamada K, et al: Frequent apoptosis in placental villi from pregnancies complicated with intrauterine growth restriction and without maternal symptoms. Randhawa R, Cohen P: the role of the insulin-like growth factor system in prenatal growth. Fowler D, Albaiges G, Lees C, et al: the role of insulin-like growth factor binding protein-1 phosphoisoforms in pregnancies with impaired placental function identified by doppler ultrasound. Dalcik H, Yardimoglu M, Vural B, et al: Expression of insulin-like growth factor in the placenta of intrauterine growth-retarded human fetuses. Laviola L, Perrini S, Belsanti G, et al: Intrauterine growth restriction in humans is associated with abnormalities in placental insulin-like growth factor signaling. Desai M, Guang H, Ferelli M, et al: Programmed upregulation of adipogenic transcription factors in intrauterine growth-restricted offspring. Wadsack C, Tabano S, Maier A, et al: Intrauterine growth restriction is associated with alterations in placental lipoprotein receptors and maternal lipoprotein composition. Bhosle Gabriel Altit Julie Autmizguine Sylvain Chemtob 18 [18-1] Pharmacology is a science concerned with the interaction of substances. The in vivo efficacy of a drug is guided by two principles of pharmacology, namely pharmacokinetics and pharmacodynamics. The former is concerned with the processes of drug concentration in the tissue compartments and therefore involves absorption, distribution, biotransformation, and excretion; pharmacodynamics applies to study of the mechanism of action of drugs. Application of these concepts to the newborn requires one to take into account developmental changes in pharmacokinetics and pharmacodynamics. In this articler, we present basic pharmacologic principles and introduce how drug disposition and actions can be altered by developmental changes and disorders of the immature subject. Regardless of the route of administration, drugs must often cross cell membranes to reach their sites of action. Therefore the mechanisms governing the passage of drugs across cell membranes and the physicochemical properties of molecules and membranes are important to consider in drug transfer. Among the most important physicochemical properties of drug molecules are lipid solubility, degree of ionization (pKa), molecular weight, and protein binding. Although some drugs (those with molecular weight < 200 Da) cross the cellular lipid membranes by diffusion,1 it is now well known that many require transporters. Furthermore, because the active molecule is believed to be the nonproteinbound portion, drugs that have a lower protein binding have greater access to their site of action. This equation does not take into account the ionization state of the drug molecule, the effect of regional blood flow, or the influence of tissue affinity on drug partitioning. The ionization state is affected by the pH on both sides of the membrane, according to the Henderson-Hasselbalch equation: pH = pK A + log ([base] [acid]) [18-3] Therefore acidic compounds, such as salicylic acid, diffuse across cell membranes more readily when the environmental pH is low because they are less ionized at low pH. Regional blood flow also influences the rate of diffusion by altering the delivery and consequently the local concentration of the drug. Finally, some drugs demonstrate increased affinity for a particular tissue component, which influences the concentration of drug on either side of the membrane. Active transport is a carrier-mediated transmembrane process that plays an important role in the renal, intestinal, and biliary secretion and absorption of many drugs and metabolites.
Rasola A symptoms stroke discount cefaclor 500 mg with mastercard, Sciacovelli M symptoms renal failure cheapest cefaclor, Pantic B shinee symptoms mp3 cefaclor 500 mg buy visa, et al: Signal transduction to the permeability transition pore medications in canada discount cefaclor 250mg. Bonora M medications requiring central line order cefaclor online from canada, Pinton P: the mitochondrial permeability transition pore and cancer: molecular mechanisms involved in cell death. Puka-Sundvall M, Gilland E, Hagberg H: Cerebral hypoxia-ischemia in immature rats: involvement of mitochondrial permeability transition Wang X, Carlsson Y, Basso E, et al: Developmental shift of cyclophilin D contribution to hypoxic-ischemic brain injury. Wang X, Han W, Du X, et al: Neuroprotective effect of Bax-inhibiting peptide on neonatal brain injury. Modjtahedi N, Giordanetto F, Madeo F, et al: Apoptosis-inducing factor: vital and lethal. Krantic S, Mechawar N, Reix S, et al: Apoptosis-inducing factor: a matter of neuron life and death. Riley T, Sontag E, Chen P, et al: Transcriptional control of human p53regulated genes. Lassus P, Opitz-Araya X, Lazebnik Y: Requirement for caspase-2 in stressinduced apoptosis before mitochondrial permeabilization. Carlsson Y, Schwendimann L, Vontell R, et al: Genetic inhibition of caspase-2 reduces hypoxic-ischemic and excitotoxic neonatal brain injury. Chauvier D, Renolleau S, Holifanjaniaina S, et al: Targeting neonatal ischemic brain injury with a pentapeptide-based irreversible caspase inhibitor. Gill R, Soriano M, Blomgren K, et al: Role of caspase-3 activation in cerebral ischemia-induced neurodegeneration in adult and neonatal brain. Hagberg H, Gressens P, Mallard C: Inflammation during fetal and neonatal life: implications for neurologic and neuropsychiatric disease in children and adults. Potrovita I, Zhang W, Burkly L, et al: Tumor necrosis factor-like weak inducer of apoptosis-induced neurodegeneration. Fiers W, Beyaert R, Declercq W, et al: More than one way to die: apoptosis, necrosis and reactive oxygen damage. Galluzzi L, Vanden Berghe T, Vanlangenakker N, et al: Programmed necrosis from molecules to health and disease. Vercammen D, Beyaert R, Denecker G, et al: Inhibition of caspases increases the sensitivity of L929 cells to necrosis mediated by tumor necrosis factor. He S, Liang Y, Shao F, et al: Toll-like receptors activate programmed necrosis in macrophages through a receptor-interacting kinase-3-mediated pathway. Takahashi N, Duprez L, Grootjans S, et al: Necrostatin-1 analogues: critical issues on the specificity, activity and in vivo use in experimental disease models. Wu J, Huang Z, Ren J, et al: Mlkl knockout mice demonstrate the indispensable role of Mlkl in necroptosis. Declercq W, Takahashi N, Vandenabeele P: Dual face apoptotic machinery: from initiator of apoptosis to guardian of necroptosis. Degterev A, Huang Z, Boyce M, et al: Chemical inhibitor of nonapoptotic cell death with therapeutic potential for ischemic brain injury. Shimizu S, Kanaseki T, Mizushima N, et al: Role of Bcl-2 family proteins in a non-apoptotic programmed cell death dependent on autophagy genes. Chen Y, McMillan-Ward E, Kong J, et al: Oxidative stress induces autophagic cell death independent of apoptosis in transformed and cancer cells. Yu L, Wan F, Dutta S, et al: Autophagic programmed cell death by selective catalase degradation. Kuma A, Hatano M, Matsui M, et al: the role of autophagy during the early neonatal starvation period. Hoyer-Hansen M, Bastholm L, Szyniarowski P, et al: Control of macroautophagy by calcium, calmodulin-dependent kinase kinase-, and Bcl-2. Zhu C, Xu F, Wang X, et al: Different apoptotic mechanisms are activated in male and female brains after neonatal hypoxia-ischaemia. Carloni S, Buonocore G, Longini M, et al: Inhibition of rapamycin-induced autophagy causes necrotic cell death associated with Bax/Bad mitochondrial translocation. Tsukada M, Ohsumi Y: Isolation and characterization of autophagy-defective mutants of Saccharomyces cerevisiae. Suzuki K, Ohsumi Y: Molecular machinery of autophagosome formation in yeast, Saccharomyces cerevisiae. Pattingre S, Tassa A, Qu X, et al: Bcl-2 antiapoptotic proteins inhibit beclin 1-dependent autophagy. Luisa IruelaArispe Ann Zovein 8 the vasculature, composed of endothelial cells and their support cells, is critical not only for circulation of blood, but also for the organization, maintenance, and regeneration of multiple organ systems. Developmentally, blood vessels first arise through a process called vasculogenesis, which encompasses the differ entiation of angioblastic progenitors from mesenchymal cells and their subsequent organization into primitive channels. The first vascular structures to form emerge in the extraembryonic yolk sac, where mesodermal cells differentiate into angioblast precursors that quickly coalesce into uniform vascular struc tures. The coincident emer gence of vessels and blood cells in the early embryonic yolk sac gave the impression that a common progenitor, termed the hemangioblast, was responsible for both hematopoietic and endothelial lineages. The first hematopoietic stem cells capable of adult engraftment arise later in development from endothelial precur sor cells that are called hemogenic endothelium. However, the intraembryonic vessels arise from another vasculogenic pool of mesodermal precursors. The terminal expansions of these vascular networks organize an evensized vascular plexus that later remodels extensively into a hierarchic tree of characteristic arteries, capillaries, and veins. In the vasculature, the Notch pathway is responsible for defining arte rial and venous identity. An important repulsive signaling cascade in the vasculature involves the ephrin ligands and Eph receptors. Designated venous cells express high levels of EphB4 receptor, and alternatively, arterial cells express high levels of ephrinB2. Loss of ephrins results in a loss of repulsive cues between the two endothelial cell types and subsequent mixing of circulations. In addition to arterial and venous circulation, a third circula tory system of lymph vessels develops through the assembly of lymphatic endothelial cells. Angiogenic expansion of a primary capillary plexus, created by vasculogenesis, contributes a great deal to the functional circulatory bed. It is the mechanism by which subse quent growth of the vascular tree is achieved in coordination with physiologic expansion of tissues. The close association of growing blood vessels with parenchymal cells during develop ment also imposes unique heterotypic interactions in distinct organs. These tissuespecific interactions further induce vascular adaptations, resulting in an array of molecular and physiologic variations known as endothelial heterogeneity. In this manner, the capillaries of the liver are formed by disconnected endothe lium and differ significantly from those in the brain, which form highly specialized bloodbrain barrier structures to ensure a tight blockade between the blood and the central nervous system. How endothelial cells know to start migrating and form a new vessel begins with detection of hypoxia and hypoxic cues in the surrounding tissue. Hypoxia is sensed by the tissue and triggers cellular production of hypoxiainducible factor, a transcription factor that activates many downstream pathways. Coordination of angiogenic outgrowth toward a hypoxic source needs to be balanced by the stability of the existing vessel. To achieve that balance, endothelial cells within the exist ing vessel selfselect which endothelial cell will migrate out of the vessel. The initiating event is a vascular sprout that emerges and is composed of a leading tip cell followed by stalk cells. Large amounts of Dll4 ligand correlate with low Notch1 receptor expression in the same tip cell. In turn, Dll4 in tip cells activates Notch in neighboring cells, blocking formation of filopodia. The process prevents multiple endothelial cells from an established vessel from migrating concurrently toward a hypoxic source and resulting in catastrophic vascular disruption. In this manner the departing tip cell inhibits its neighbors from migrating-ensuring vascular stability in the pre existent vessel while promoting vascular expansion. The process of angiogenic sprouting can become deranged or overactive in hypoxic tumor environments or even in the premature retina. It was generally believed that as premature infants are exposed to higher levels of oxygen, large fluctuations in the retinal oxygen environment trigger a hypoxic cascade, such that overgrowth of the retinal vasculature occurs. The same programs of arteryvein specification, as well as tip and stalk cell selection, are recapitu lated in the retina for proper vascularization. The investment of smooth muscle cells around naked endothelial tubes provides mechanical resistance against the continuous force imposed by rapid and pulsatile blood flow. The progenitors for these vascular smooth muscle cells are broad, and depending on the location of the blood vessel and the time, they originate from the neural crest (mostly head vessels) or somitic or lateral mesoderm. These proteins bind with smooth muscle cells to form a highly integrated tissue that is able to respond to and regulate intravascular pressure. The types of extracellular matrix proteins (elastic fibers, collagen fibers, and several types of glycoproteins) are distinctly depos ited in different vessels. Part of the difficulty results from extensive diversity of vascular smooth muscle phenotypes. Furthermore the vascular smooth muscle cells retain a level of cellular plasticity not observed in other systems. Notch is required for the development of vascular smooth muscle and the initial association of undifferentiated mesenchymal cells with endothelial tubes. Additionally, it drives a program of differentiation in cholangio cytes that is critical for their full differentiation into the epithe lium of the biliary tree. A wellpatterned and physiologically responsive circu latory system ensures proper nutrient and oxygen delivery for the growth and development of the embryo. It requires de novo formation of major vessels (vasculogenesis), in addition to rapid, organized expansion of vascular beds from preexisting vessels (angiogenesis). We have reviewed the overarching principles governing the formation of the vascular system within the embryo and the main signaling cascades responsible for its organization. Foremost to the importance of a functioning vas cular system is the specification of endothelial cells into arterial, vein, and lymphatic cell subsets and the establishment of their respective circulatory systems. In the adult, the expansion of the vasculature addresses the needs of growing tissues and, when necessary, promotes repair and regeneration. Interest ingly, similar signaling mechanisms are echoed throughout each vascular process. The intersection of these pathways, combined with the increased ability to detect human gene and genomic variants, will continue to reveal the complex and interwoven system of signaling cascades in normal vascular formation and function. In addition to forming a circulatory system on the organismal level, the regulation and formation of the vasculature are also respon sible for proper formation and maintenance of specific organs. As antiangiogenic agents continue to be created and tested as cancer therapies, new opportunities will arise for therapeutic exploration in vascular disease. Heterotypic cell interactions between vascular cells (endothelial and smooth muscle) and cells making up the developing organ are required. The developing vascula ture provides critical spatial information and differentiation signals to parenchymal cells for proper organ formation. This instructive role of the endothelium has been studied specifically in the pancreas using elegant genetic models that either elimi nate or perturb the vascular endothelium. In smooth muscle cells, inactiva tion of Jagged 1, a ligand for Notch receptors, arrests the forma tion of biliary ducts in the liver and results in liver failure. Moyon D, Pardanaud L, Yuan L, et al: Plasticity of endothelial cells during arterialvenous differentiation in the avian embryo. Fukushima Y, Okada M, Kataoka H, et al: Sema3EplexinD1 signaling selec tively suppresses disoriented angiogenesis in ischemic retinopathy in mice. Domenga V, Fardoux P, Lacombe P, et al: Notch3 is required for arterial iden tity and maturation of vascular smooth muscle cells. Lammert E, Cleaver O, Melton D: Induction of pancreatic differentiation by signals from blood vessels. One reason why is that the human genome is more complicated than originally postulated. Counterintui tively, this complexity partially arises from the finding that the human genome has approximately only one third of the pre dicted number of genes. As a result, the regulatory processes that control the expression of these genes are complex4,5 and involve multiple layers of regulation, much of which still remains to be discovered and described. Traditionally, it had been assumed that inherited genes control gene expression and ultimately phenotype. This definition leaves out the concept of inheritance, instead emphasizing the effect on the final cell type and how small nongenetic changes in development can lead to measurable differences in adult pheno type. As previously mentioned, it is through the epigenetic changes that each individual modifies his or her phenotype to better suit the environment. This regulatory control occurs through mechanisms that utilize epigenetic signals to affect nuclear. Thus genetic changes tend to occur slowly, taking many genera tions for a single mutation to become dominant in a population. This means that epigenetics provides a mechanism for rapid responses to environmental changes. This difference in "mutation rates" is due to a reduction in the fidelity of maintenance of epigenetic features when compared with genetic features throughout the cell cycle. However, the influence of genes and environment on the development of phenotypic traits is not mutually exclusive but rather a result of their constant interaction. For example, twin studies suggest that genetic factors have a substantial effect on variations in body weight, particularly in children and adolescents. Nonetheless, the fact that obesity is rapidly increasing worldwide shows that environment also plays a significant role in the likelihood of becoming obese. Thus, in most cases the resulting manifestation of noncommunicable disease is a combination of nature and nurture.
500mg cefaclor fast delivery. How to cure Pigeon Neck Twisting and treatment - lakwe or jhoole ka desi ilag (PMV).
References
- Hugo W, Zaretsky JM, Sun L, et al. Genomic and transcriptomic features of response to anti-PD-1 therapy in metastatic melanoma. Cell 2016;165(1):35-44.
- Wilson A, Pillay S, Greenwell T: How and why to take a Martius labial interposition flap in female urology, Transl Androl Urol 6(Suppl 2):S81nS87, 2017.
- Benchekroun, A., Alarm, M., Ghadouan, M. et al. Urinary candidiasis revealed by ureteral obstruction: report of 2 cases. Ann Urol (Paris) 2000;34:171-174.
- Walley KR, Lewis TH, Wood LD. Acute respiratory acidosis decreases left ventricular contractility but increases cardiac output in dogs. Circ Res. 1990;67:628-635.
- Levitsky J, Kalil A, Meza JL, et al. Herpes zoster infection after liver transplantation: a case-control study. Liver Transpl. 2005;11: 320-325.
- Rajfer J, Ehrlich RM, Goodwin WE: Reduction clitoroplasty via ventral approach, J Urol 128(2):341n343, 1982.
- Esnaola NF, Rubin BP, Baldini EH, et al. Response to chemotherapy and predictors of survival in adult rhabdomyosarcoma. Ann Surg 2001;234(2):215-223.
- Claahsen-van der Grinten HL, Otten BJ, Hermus ARMM, et al: Testicular adrenal rest tumors in patients with congenital adrenal hyperplasia can cause severe testicular damage, Fertil Steril 89:597n601, 2008.