
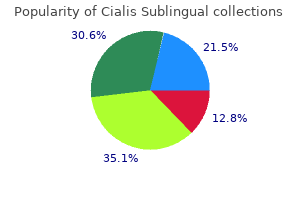
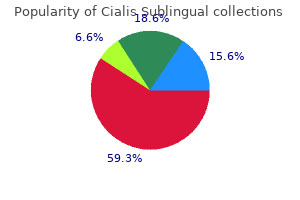
Cialis Sublingual
| Contato
Página Inicial
Angelo Michael DeMarzo, M.D., Ph.D.
- Associate Director of Cancer Research Pathology, Sidney Kimmel Comprehensive Cancer Center
- Professor of Pathology
https://www.hopkinsmedicine.org/profiles/results/directory/profile/0007730/angelo-demarzo
They are called "opportunistic infections" and pose a risk to the patient but not to the care provider what food causes erectile dysfunction cialis sublingual 20 mg lowest price. Most individuals have this yeast-like fungus in their lungs erectile dysfunction protocol scam or real purchase on line cialis sublingual, but it does not cause illness because a healthy immune system prevents it from causing infection erectile dysfunction and stress purchase 20 mg cialis sublingual visa. This is a medical issue for the patient but does not pose a risk to the healthy health-care worker impotence female cialis sublingual 20 mg buy mastercard. Although the virus has been cultured from a variety of body fluids erectile dysfunction causes prostate cialis sublingual 20 mg buy lowest price, only blood has been implicated in the transmission of the virus in the workplace. This is because other body fluids do not carry enough virus particles to transmit the disease. Semen and vaginal secretions have been shown to transmit the virus during sexual activity only. Transmission to health-care workers has been documented only after accidental parenteral exposure (needlestick) or exposure of mucous membranes and open wounds to large amounts of infected blood. There is one documented case of transmission from infected blood on nonintact skin. You should also wear a mask especially if the patient requires oxygen and cannot wear a mask. In general, large-gauge hollow-needle exposures are more significant than solid instruments (such as a scalpel). Recommendations are for early post-exposure treatment to reduce the risk of acquiring the disease. Exposed personnel need to be counseled about the side effects and other issues involving the use of these drugs before they are started. In other areas of the world, treating physicians should follow facility protocols before the drugs are prescribed. Remember, all post-exposure medical follow-up begins with testing the source patient, not the exposed emergency care provider. It is the responsibility of the physician treating the exposed emergency care provider to assess the risk of transmission and to provide guidance to the exposed emergency care provider. Public Law 101-381, required inclusion of all emergency response employees-firefighters, emergency medical technicians, paramedics, law enforcement officers, and volunteers-in the postexposure medical notification process in the event of an exposure to a bloodborne or airborne transmissible disease. From 1985 to 1993, the incidence of active tuberculosis increased significantly to over 25,000 cases in the United States. Because of better public health measures, tuberculosis has been declining in the past several years. In fact, the number of cases in 2012 was the lowest ever reported in the United States. Tuberculosis is caused by a bacterium, Mycobacterium tuberculosis, which is spread from an infected person to susceptible people through the air, especially by coughing or sneezing. Contracting tuberculosis requires prolonged direct contact, as in a family living situation. Infections outside the lung are called extrapulmonary and are not communicable to the care provider. Signs and symptoms of active tuberculosis are most prominent in the lungs and include a productive cough that lasts longer than three weeks in conjunction with two or more of the following: pain in the chest, coughing up bloody sputum, weakness or fatigue, unexplained weight loss, loss of appetite, fever, chills, night sweats, or hoarseness. It should be noted that to continue annual testing in low-risk areas leads to false-positive tests. Chickenpox-Varicella Zoster Chickenpox is considered to be a highly communicable disease. It is transmitted from one person to another by inhalation of aerosols or by touching drainage from the lesions. An infected person may be able to transmit the disease one to two days before the rash appears. A person with chickenpox is considered to be communicable until all the lesions become crusted and dried. Signs and symptoms of chickenpox include fever and a rash that progresses to a plump lesion or lesions, and photosensitivity (the patient wants to be in the dark). The primary prevention measure for chickenpox is vaccination if the person is not immune. Immunity is documented by written diagnosis, a titer or documentation of vaccination with two doses of vaccine given one month apart. Protection from acquiring chickenpox helps reduce the chance of a person developing shingles (Zoster). A person who is not protected against chickenpox and cares for a patient with shingles is at risk for developing chickenpox. Women of childbearing age are to be counseled not to become pregnant for four weeks after each dose of vaccine, which needs to be documented. Rubeola (Red Measles/Hard Measles) Rubeola is a virus primarily transmitted by the airborne route. Health care personnel are considered a higher risk for becoming infected than members of the general public. This disease has been preventable since measles vaccination programs started in 1963. Immunity is documented by evidence per written documentation showing the person has received two doses of live measles vaccine, a titer showing immunity, or written documentation of disease. Of special note: Persons who were vaccinated between 1963 and 1967, need to be revaccinated with live-measles vaccine because the killed-virus vaccine that was used previously has been shown not to be protective. Signs and symptoms of measles include rash, fever, coryza and conjunctivitis, and Koplik spots (whitish/gray spots on the buccal mucosa). The secondary prevention method is placing a surgical mask on the suspect patient, or, health-care workers should wear a surgical mask. As this text goes to press, increasing numbers of cases are being reported, with several significant outbreaks in the United States. Pertussis is characterized by uncontrollable, violent coughing spells that often make it difficult to breathe. After a coughing attack, someone with pertussis often needs to take deep breaths, which makes the whooping sound from which the disease gets its name. Pertussis more commonly affects infants and young children whose smaller airways are at risk for compromise. Most adults and health-care workers have not been vaccinated against pertussis since they were 11 to 14 years of age. If pertussis is contracted or a provider exposed, the person can be treated with antibiotics. Signs and symptoms of this disease include fever and swelling and inflammation of the salivary glands. Care providers should make sure they have received two doses of mumps vaccine if they have not had the mumps. This is a live virus vaccine, so women of childbearing age need to be counseled not to become pregnant for four weeks after each dose of vaccine. If not immune and need to transport a suspect patient, put a surgical mask on the patient. However, this illness in pregnant women can lead to birth defects in the fetus, including blindness, deafness, mental retardation, and congenital heart defects. Primary protection is afforded by vaccination in the absence of history of the disease. Meningitis, Viral or Bacterial Meningitis is a disease caused by the inflammation of the protective membranes (the meninges) covering the brain and spinal cord. Those who have had significant exposure to a patient with meningococcal meningitis need to be treated with a short course of antibiotics. Meningitis infections are characterized by a sudden onset of fever, headache, and stiff neck. It is often accompanied by other symptoms, such as nausea, vomiting (projectile), photophobia (sensitivity to light), altered mental status, sudden onset severe headache, and neck stiffness. Influenza Influenza (flu) is a communicable respiratory illness caused by influenza viruses (Type A or Type B viruses). Worldwide, influenza kills over 200,000 people each year, more than any of the other diseases discussed in this chapter. The elderly, young children, pregnant women, and people with lowered immune systems are at high risk for serious flu complications. Flu complications can include bacterial pneumonia, ear infections, sinus infections, and dehydration. Flu can also exacerbate chronic medical conditions such as congestive heart failure, asthma, and diabetes. People who have the flu often feel some or all of the following symptoms: fever or feeling feverish/chills, cough, sore throat, headache, body aches (myalgias), fatigue, and runny nose. Flu viruses spread mainly by droplets made when people with the flu cough or sneeze. A person might get flu by touching a surface or object that has flu virus on it and then touching his or her own mouth, eyes, or nose. The importance of work restriction was stressed during the H1N1 flu outbreak in 2009 and 2010. Flu vaccine is viewed not only as emergency care provider protection but as patient protection as well. There are new influenza vaccines available that do not contain mercury or antibiotics and are not egg based. Have appropriate barrier devices with you so you are not required to do mouth-tomouth breathing. However, you have an obligation to perform mouth-to-mouth resuscitation if your patient needs it and you forgot your equipment. Since the early 1960s the number of multidrug-resistant organisms has been increasing. First reported in the hospital care setting, such infections are now also in the general population. It is transmitted by close personal contact with nonintact skin, close contact sports (wrestling, football), and poor personal hygiene. Generally, it presents as a localized soft-tissue infection (abscess) and is easily treated by incision and drainage. Gloves, good hand washing, and clean surfaces and equipment are important for protection of patients and care providers. Enterococci are common bacteria of the gastrointestinal and urinary tracts and sometimes cause infection. Clostridium Difficile (C-diff) Clostridium difficile (C-diff) is not a multidrug-resistant organism, but it is treated as if it were. C-diff replaces "good" bacteria in the intestines and leads to watery, green, and foul-smelling diarrhea, fever, nausea, loss of appetite, and abdominal tenderness/pain. Generally, this illness resolves in two to three days after discontinuing antibiotics. Glove use, good hand washing with warm water and soap, and cleaning contaminated surfaces with an appropriate cleaning agent is important for reducing transmission risks. Multidrug-resistant organisms will continue to be an issue until several key influencing factors are addressed. They include good hand washing practice, cleaning of vehicles and equipment, education regarding the nonuse of antibiotics when not needed, removal of antibiotics from animal foods, and altering prescription habits. With the advent of new and emerging resistant organisms, obtaining a travel history on all patients is important. Difficile Cleaning Alcohol-based products are not effective for decontaminating surfaces that have been exposed to C-diff. C-diff is a spore-forming agent so a chlorine-based cleaning solution is required. Precautions for Prevention of Transmission of Infectious Agents Standard precautions refer to treating everyone (including you) as if they are infectious. Your goal is to prevent the spread of infection from you to the patient and from the patient to you. Consider the use of personal protection based on the task being performed (Table 22-1). Understand their etiologies, signs and symptoms, routes of transmission, and epidemiology (relationships of the various factors determining the frequency and distribution of a disease). Avoid invasive procedures, other direct patient care activities, and handling of equipment used for patient care. Emergency care providers should not have artificial nails or extensions because they can be hard to clean and can trap potentially infectious materials. Become immunized against the hepatitis B virus, chickenpox, measles, mumps, and rubella if you are not protected by acquired immunity. Procedure Transmission-Based Precautions When the way in which a disease is transmitted is identified, there are specific methods to prevent that transmission. There are three categories of transmission precautions-contact, droplet, and airborne precautions. Wear gown when in contact with the individual, surfaces, or objects within the immediate environment. Clean and disinfect all reusable items, such as blood pressure cuff and stethoscope. Follow surface cleaning protocol for the vehicle and stretcher, using appropriate viricidal or germicidal agents. So, in addition to standard precautions use the following droplet precautions: · Wear a surgical mask when within three feet (one meter) (for smallpox six feet or two meters) of persons known or suspected of having diseases spread by droplets. The plastic bags should then be disposed of according to governmental definitions of medical waste in proper waste containers available in hospital emergency departments or other health-care locations.
Experimental Design Question: You wish to knockout the expression of a particular gene impotence when trying to conceive buy cheap cialis sublingual 20 mg, only in B cells impotence kidney buy cialis sublingual mastercard, and you want to do the knockout only after you have exposed your B cells to antigen erectile dysfunction hand pump order cialis sublingual cheap. Because they are often expressed selectively on particular cell types erectile dysfunction and prostate cancer order discount cialis sublingual online, and sometimes alter their expression according to the developmental and/or activation state of those cells erectile dysfunction pills nz 20 mg cialis sublingual order amex, they can serve as markers for particular cell types at specific stages of their differentiation. The molecular weights that are shown are those of the human versions of the proteins, as listed on the UniProt or BioLegend websites (see below). Note that the molecular weight is calculated on the basis of the protein sequence and does not include the molecular weight of any associated carbohydrate. Where there are two isoforms, both molecular weights are shown; where there are more than two, only the first molecular weight is shown in the table, and the reader is alerted to the number of known isoforms. Recall that type 1 membrane proteins present the amino terminus to the external face of the membrane, and type 2 membrane proteins conversely present the carboxyl terminus to the external membrane face. Multipass proteins may cross the membrane many times, but most cross the membrane seven times. However, many of these antigens are also expressed in other cell types, and we also give some (but not exhaustive) examples of these. Recall that these numbers are based on antigenic determinants detected by monoclonal antibodies. Most determinants have been confirmed by the binding of more than one monoclonal antibody. The website and international workshops are the product of a collaborative effort by numerous researchers and biomedical supply companies around the world and are updated regularly. The PubMed site allows searches of published articles by keywords as well as other variables, such as author name or year of publication. For a more comprehensive search on a particular antigen, the synonyms listed in this table can be included as alternative keywords. This table was updated on the basis of information in the websites mentioned above, along with some recent literature references. There is also a secreted form Neutrophils, stimulated eosinophils Low-affinity Fc receptor, binds IgG, especially in complexes or aggregates. Expressed in monocytes, neutrophils, macrophages, basophils, eosinophils, Langerhans cells, B cells, platelets, and placenta (endothelial cells) Binds Fc region of IgG. Involved in phagocytosis of immune complexes and modulation of antibody production by B cells. Provides essential costimulatory signals for B-cell activation, proliferation, differentiation, and isotype switching; apoptosis rescue signal for germinal center B cells. Stimulates cytokine production by macrophages and dendritic cells and upregulates adhesion molecules on dendritic cells. Also involved in lymphocyte activation, recirculation and homing to lymphoid tissues and sites of inflammation, and in hematopoiesis. Plays an important role in memory formation and synaptic plasticity in the hippocampus. The main protein product is cleaved into the following three chains: integrin 6 heavy chain, integrin 6 light chain, processed integrin 6; type 1 membrane protein. Adhesion molecule; contributes to antigenspecific T-cell activation by antigen-presenting cells; contributes to the extravasation of leukocytes from blood vessels, particularly in areas of inflammation. Protective barrier against inappropriate complement activation and deposition on plasma membranes. Binds to C8 and/or C9, thereby preventing incorporation of C9 into the structure of the osmolytic pore. Binds to tissue- and organspecific lectins or selectins, allowing homing of macrophage subsets to particular sites. Also expressed on melanosomes Endothelium, stem-cell subsets Control of endothelial cell-cell adhesion, permeability, and migration Follicular dendritic cells, endothelium, melanoma, smooth muscle, intermediate trophoblast, a subpopulation of activated T cells Adhesion molecule All leukocytes, red blood cells, platelets, endothelial cells. Detected at high levels in heart and lung, and at low levels in brain, placenta, liver, skeletal muscle, pancreas, and kidney Cell surface receptor for fibrillar collagen; regulates cell differentiation, remodeling of the extracellular matrix, cell migration, and cell proliferation. Myeloid progenitor cells, fibroblasts, chondrocytes, osteoclasts, osteocytes, subsets of endothelial and macrophage cells May affect cell motility and remodeling of the extracellular matrix. Expressed in many lymphoma cell lines 1582 B-cell development and differentiation. May be immunoregulatory in marginal zone B cells and on hairy cell leukemia cells. Expression more elevated in peripheral blood leukocytes than in bone marrow, and in normal than in malignant cells. Expressed at low levels in early hematopoiesis and in the promonocytic stage and at high levels in mature 1588 Stimulates neutrophil and monocyte inflammatory responses; amplifies inflammatory responses; mediates septic shock monocytes. In some instances, a given cytokine may have biological activities in addition to those listed here or may be produced by other sources as well as the ones cited here. Major references used for the information in this appendix: GeneCards Human Gene Database: Induces epithelial cell release of antimicrobial peptides and enhances tight junction integrity. Also shown to function in ontogenesis and promote survival and regeneration of nerves Bone marrow stromal cells and macrophages Essential for growth and differentiation of neutrophils T cells, macrophages, fibroblasts, and endothelial cells Growth factor for hematopoietic progenitor cells and differentiation factor for granulocytic and monocytic cell lineages Many cell types, including lymphocytes, monocytes, fibroblasts, epithelial cells, and others Growth, differentiation, and survival factor for macrophage progenitors, macrophages, and granulocytes Cells activated by viral and other microbial components: macrophages, dendritic cells, and lymphocytes, virus-infected cells Induces resistance to virus infection. Induces class switching to IgA Strong mediator of inflammatory and immune functions. Note that this table is not comprehensive; investigators are not in full agreement about groupings. Chemokines (family, old and new nomenclature), their receptors, and predominant receptor repertoires in various leukocyte populations are listed. Chemokine names in bold identify inflammatory chemokines, names in italics identify homeostatic chemokines, and underlined names refer to molecules belonging to both realms. Chemokine receptors to which the leukocyte expression lists pertain are underlined. This is the first step in the processes of both somatic hypermutation and class switch recombination. Active immunity Adaptive immunity that is induced by natural exposure to a pathogen or by vaccination. Acute phase protein One of a group of serum proteins that increase in concentration in response to inflammation. Acute phase response proteins Proteins synthesized in the liver in response to inflammation; serum concentrations of these proteins increase in inflammation. Acute rejection Refers to the process of allo- or xenograft recognition and rejection that occurs after hyperacute rejection and that involves the action of both activated T and B cells. This stage of rejection can begin as early as 7 days after engraftment (following sensitization and effector cell engagement) and can continue for a year 1608 or more. Adapter Proteins Proteins that connect to other effector proteins in a signaling pathway and create a signaling scaffold. Adaptive immunity Host defenses that are mediated by B cells and T cells following exposure to antigen and that exhibit specificity, diversity, memory, and self-nonself discrimination. Addressin A cell-surface protein or set of cell-surface proteins that are ligands for specific homing receptors on immune cells; they help guide immune cell trafficking. Adhesion molecules Families of surface proteins that regulate cell interactions with tissues, vessels, and with each other; they are important players in immune cell trafficking. Adjuvant cancer therapy A supplement or secondary treatment for cancer applied after the primary treatment (typically, surgical removal), which can include radiation and/or chemical/drug therapy meant to target residual tumor cells. Adjuvants Factors that are added to a vaccine mixture to enhance the immune response to antigen by activating innate immune cells. Dead mycobacterium were among the original adjuvants, but more refined preparation include alum, cytokines, and/or lipids. Adoptive transfer the transfer of the ability to make or participate in an immune response by the transplantation of cells of the immune system. Affinity the strength with which a monovalent ligand interacts with a binding site. Affinity constant the ratio of the forward (k1) to the reverse (k-1) rate constant in an antibody-antigen reaction. High affinity interactions result in death by negative selection, lower affinity interactions in positive selection and maturation, and very low or no affinity interactions result in death by neglect. Affinity maturation 1609 the increase in average antibody affinity for an antigen that occurs during the course of an immune response or in subsequent exposures to the same antigen. Agent-induced immunodeficiency A state of immune deficiency induced by exposure to an environmental agent/s. Agglutination inhibition the reduction of antibody-mediated clumping of particles by the addition of the soluble forms of the epitope recognized by the agglutinating antibody. Agglutinin titer the reciprocal of the greatest serum dilution that elicits a positive agglutination reaction. It is expressed by a subset of medullary epithelial cells and regulates transcription. Alarmins A diverse group of molecules, released in response to cellular stress, that summon protective inflammatory responses. Alleles Two or more alternative forms of a gene at a particular locus that confer alternative characters. Allelic exclusion A process that permits expression of only one of the allelic forms of a gene. For example, a B cell expresses only one allele for an antibody heavy chain and one allele for a light chain. Allergy A hypersensitivity reaction that can include hay fever, asthma, serum sickness, systemic anaphylaxis, or contact dermatitis. Allotypes A set of allotypic determinants characteristic of some but not all members of a species. Allotypic determinant An antigenic determinant that varies among members of a species or between different inbred strains of animals. Allotypic marker A genetic marker that defines the presence of an allele on one strain of mouse that is not shared by other strains. Altered peptide model A proposal stating that developing T cells encounter different sets of peptides in the cortical region versus the medullary region of the thymus. Advanced to help explain differences in the subsets of cells that undergo positive versus negative selection. Alternative pathway of complement activation A pathway of complement activation that is initiated by spontaneous hydrolysis of the C3 component of complement, resulting in the formation of a fluid-phase C3 convertase enzyme. This spontaneous initiation distinguishes the alternative pathway from the classical and lectin-mediated pathways that are both initiated by specific antigen binding by either antibodies or lectins respectively. However, one recently-discovered branch of the alternative pathway may begin with Properdin binding to the surface of bacteria from the Neisseria genus. Alternative tickover pathway the alternative pathway of complement activation that is initiated by spontaneous hydrolysis of C3 molecule in the serum. Alveoli the clusters of sacs at the end of the bronchiolar branches where gas exchange takes place; alveoli are lined by a single layer of epithelial cells and are in contact with capillaries. Amphiregulin 1611 A protein factor, produced by epithelial cells as well as several types of immune cells, which contributes to tolerance and promotes healthy epithelial barriers; in the skin, amphiregulin helps promote keratinocyte proliferation. Anaphylactic shock An acute, life threatening (Type I) whole-body allergic response to an antigen. Anaphylatoxins the complement split products C3a and C5a, which mediate degranulation of mast cells and basophils, resulting in release of mediators that induce contraction of smooth muscle and increased vascular permeability. Anaphylaxis An immediate type I hypersensitivity reaction, which is triggered by IgE-mediated mast cell. Anti-Fab antibodies Antibodies directed towards the Fab regions of other antibodies. Anti-idiotypic antibodies Antibodies directed towards antigenic determinants located in the antigen binding site of other antibodies. Anti-isotype antibodies Antibodies directed towards antigenic determinants located in the constant regions of antibodies, that are shared among all members of a species. Antibodies 1612 Immunoglobulin proteins consisting of two identical heavy chains and two identical light chains, that recognize a particular epitope on an antigen and facilitates clearance of that antigen. Membrane-bound antibody is expressed by B cells that have not encountered antigen; secreted antibody is produced by plasma cells. Antigen Any substance (usually foreign) that binds specifically to an antibody or a T-cell receptor; often is used as a synonym for immunogen. Antigenic drift A series of spontaneous point mutations that generate minor antigenic variations in pathogens and lead to strain differences. Antigenic shift Sudden emergence of a new pathogen subtype, frequently arising due to genetic reassortment that has led to substantial antigenic differences. Antigenically committed the state of a mature B cell displaying surface antibody specific for a single immunogen. Antimicrobial peptides Peptides/small proteins, such as defensins, less than 100-amino acids long that are produced constitutively or after activation by pathogens. Antimicrobial proteins Enzymes and other proteins that directly damage pathogens, induce phagocytosis, or inhibit pathogen infectivity or replication. Antiserum Serum from animals immunized with antigen that contains antibodies to that antigen. Apical surface the portion of the membrane of an epithelial cell that faces the lumen of a tissue. Apoptosis A process, often referred to as programmed cell death, where cells initiate a signaling pathway that results in their own demise. Apoptosome A wheel-like assemblage of molecules that regulate cell death initiated via the mitochondrial (intrinsic) pathway. Atopic Pertaining to clinical manifestations of type I (IgE-mediated) hypersensitivity, including allergic rhinitis (hay fever), eczema, asthma, and various food allergies. Atopic (allergic) march 1614 the natural history or typical progression of allergic diseases that often begin early in life, starting with atopic dermatitis (eczema) and progressing to food allergy, allergic rhinitis (hay fever), and possibly asthma. Atopy the genetic tendency to develop allergic diseases such as allergic rhinitis, asthma, and atopic dermatitis (eczema); typically associated with heightened immune responses to common allergens, especially inhaled and food allergens. Attenuate To decrease the virulence of a pathogen and render it incapable of causing disease.
Importantly erectile dysfunction pills review cialis sublingual 20 mg order, these first two stages in the transformation process can last for long periods and the cells are still susceptible to immune-mediated detection and chemopreventive agents erectile dysfunction hiv cheap 20 mg cialis sublingual with amex, with the potential to reverse the course of disease impotence curse 20 mg cialis sublingual purchase free shipping. Genetic alterations occurring here allow for rampant cell proliferation and the acquisition of new mutations to 1377 potential cancer-promoting genes erectile dysfunction shots cheap cialis sublingual 20 mg overnight delivery, exacerbating the cycle erectile dysfunction self injection purchase 20 mg cialis sublingual otc. When one or more of these rapidly dividing cells acquire mutations that allow invasion of nearby tissue, the situation has progressed to the final stage, metastasis. By definition, metastatic cancers that come from solid tissues have lost adhesion with neighboring cells and no longer exhibit contact inhibition. This allows them to move outside the original site and even enter blood or lymphatic vessels, where they can then spread through the body. Colon cancer begins as small, benign tumors called adenomas in the colorectal epithelium. Each of the stages indicated in (a) is morphologically distinct, as illustrated in (b), allowing researchers to determine the sequence of genetic alterations. Studies with transgenic mice also support the role of multiple steps in the induction of cancer. Transgenic mice expressing high levels of Bcl-2, a protein encoded by the anti-apoptotic gene bcl2, develop a population of small resting B cells (derived from secondary lymphoid follicles) that have greatly extended life spans. Analysis of 1378 lymphomas from these animals has shown that approximately half have a c-myc translocation (a proto-oncogene) to the immunoglobulin H-chain locus. The synergism of Myc and Bcl-2 is highlighted in double-transgenic mice produced by mating the bcl-2 + transgenic mice with myc+ transgenic mice. Hallmarks of Cancer Examples of the genetic mutations typical of cellular transformation have helped scientists to establish some interesting common denominators for cancer. By definition, all neoplastic cells display a selective growth advantage over their peers. The four conditions later added to this picture of cancer include genome instability, altered metabolic pathways, chronic inflammation, and immune avoidance patterns. As discussed below, these observations are linked to a burst of immune-based therapies aimed at the treatment of cancer. Shown in the center are the six original hallmarks proposed as common characteristics of cancer. Later, two enabling characteristics were added as an overlay or microenvironmental factor: genome instability and protumor inflammation. Finally, two newly emerging hallmarks were added to the observed cancer profile: changes in cellular energetics and 1380 immune evasion. In the face of these unifying themes related to cancer, evidence has emerged also for heterogeneity within the cancer cell population. Clinical studies of at least three different types of tumors, including those originating in the gut, brain, and skin, suggest that a subset of cells within a tumor may be the real engines of tumor growth. This subset, called cancer stem cells, displays true unlimited regenerative potential and is the major producer of new cells to feed the tumor. Nonstem cells constitute the bulk of the growing edges of the tumor and thus serve as the primary immune targets-like decoys. These rapidly mutating cells express an ever-evolving set of new protein markers, with the potential to serve as targets for the immune response. However, there is little risk if these proteins are recognized and lead to immune destruction; their undifferentiated stem cell parent remains as a source of replacement. Key Concepts: Cellular transformation occurs as the result of multiple gene mutations that accumulate in several genes over time, and gradually subvert the normal checks on cell growth and survival. Malignant cells display alterations in key cellular processes and microenvironmental conditions: cell fate decisions, genome maintenance, cell survival, genetic instability, metabolic changes, and immune response patterns. As such, all or most of the antigens associated with these cells are subject to the same tolerance-inducing processes that maintain homeostasis and inhibit the development of autoimmunity elsewhere in the body. However, in some instances, cancer cells may produce unique or inappropriately expressed antigens that can be detected by the immune system. As one can imagine, many clinical research studies aim to utilize these antigens as diagnostic or prognostic indicators, as well as therapeutic targets for tumor elimination. These unique sequences will be shared by all tumors induced by the same virus, making their characterization simpler. For example, when mice are injected with killed polyoma virusinduced tumor cells from a syngeneic mouse (see Chapter 7) the recipients are protected against subsequent challenge with live tumor cells from any polyomainduced tumors. This suggests that the mice mounted an immune response against virus-specific antigens present on these tumor cells. Likewise, when lymphocytes are transferred from mice with a virus-induced tumor into normal syngeneic recipients, the recipients reject subsequent transplants of all syngeneic tumors induced by the same virus. In some cases, the presence of virus-specific tumor antigens is an indicator of neoplastic transformation. Over 500,000 women each year develop cervical cancer (80% of them are in developing countries), and approximately 275,000 women die of the disease annually. Periodic cervical examination (using the Papanicolaou test, or Pap smear) to detect abnormal cervical cells significantly reduces the risk for women. However, a health care program that includes regular Pap smears is commonly beyond the means of the less advantaged and is largely unavailable in many developing countries. Most infections are resolved without disease; it is persistent infection leading to cervical or anal intraepithelial neoplasia that is associated with high cancer risk. Conclusive evidence that this will translate into significantly reduced rates of cervical cancer in women, which can take many years to develop, will not be available until longterm follow-up studies have been completed. Although the committee did not recommend routine immunization for boys at that time, it did suggest that Gardasil be offered to males ages 9 to 26. As of 2007, 25% of 13- to 17-year-old girls in the United States reported receiving at least one dose of this vaccine. In 2011, this number rose to 53% in girls, still far short of targeted numbers (about 80%) and significantly lower than the rates of compliance for most other routine childhood vaccines (somewhere around 90%, depending on the age of the child). The hope is that this will curb the rising tide of anal and oropharyngeal cancers among men, but also cut back the infection cycle and impact rates of cervical cancer in women. The idea was that, with Gardasil in particular, the ability to reduce the incidence of unsightly genital warts might provide added incentive for male vaccination. With a safe and effective vaccine against a common and deadly cancer available for several years, why are the rates of immunization in young people still so low The answer depends somewhat on the country in question, as well as social and economic factors. In the group that had received a provider recommendation, 85% were immunized, compared with only 5% among women who did not receive a physician recommendation. Naturally, these antigens can be quite diverse and are identified only by their ability to induce T cellmediated rejection. The immune response to such tumors typically eliminates all of the tumor cells bearing sufficient numbers of these unique antigens, and thus selects for cells bearing few or no antigens. Instead, these represent normal cellular proteins and thus are prone to the usual self-tolerance mechanisms. Those derived from reactivation of certain fetal or embryonic genes, called oncofetal tumor antigens, normally only appear early in embryonic development, before the immune system acquires immunocompetence. When transformation of cells causes these fetal proteins to appear at later stages of development on the neoplastic cells of the adult, they can be recognized as aberrant and induce an immunologic response. Elevated levels of this glycoprotein can also be found in women, 1386 especially during the early stages of pregnancy. These proteins, although transcribed in the healthy adult, are normally tightly regulated and expressed only at low levels. Another, melanotransferrin, designated p97, has fibroblast growth factorlike activities. Whereas normal cells express fewer than 8000 molecules of p97 per cell, melanoma cells express 50,000 to 500,000 molecules per cell. The gene that encodes p97 has been cloned, and a recombinant vaccinia virus vaccine has been prepared that carries the cloned gene. When this vaccine was injected into mice, it induced both humoral and cell-mediated immune responses, which protected the mice against live melanoma cells expressing the p97 antigen. Key Concept: Cancer-associated antigens are normal cellular proteins that display abnormal expression patterns and thus are not foreign. In some instances these can be recognized by the immune system, or used clinically to monitor or therapeutically target the cancer. Some said that the immune response played no role, since these cancer cells arise from self and are therefore protected from immune recognition by ongoing tolerance processes. Others insisted that one of the essential roles of the immune response was to protect us from cancer. Data collected in the past few decades from both animal models and clinical studies have clearly defined a role for the immune response in tumor cell identification and eradication. The evolving data concerning the relationship between the immune system and cancer will be covered in this section. However, before we discuss the role of the immune system it is worth mentioning that there are several intrinsic and extrinsic mechanisms designed to prevent cancer. Should this or other intrinsic systems fail there are still extrinsic or cell external control mechanisms at work to inhibit transformation. At their most basic, these extrinsic mechanisms involve environmental signals that instruct a cell to activate internal pathways leading to growth arrest and/or apoptosis in order to prevent neoplastic cell spread. For instance, disruption of epithelial cell associations with the extracellular matrix due to malignant transformation triggers death signals that block proliferation and spread of these contactdependent cells. Thus, these extracellular attachments normally serve as inhibitors of cell death, which when broken set off a safety mechanism promoting apoptosis. However, if unregulated growth continues despite this safety net, identification and rejection of tumor cells by components of the immune system may help salvage homeostasis. Although several key immune cell types and effector molecules that participate in this response have been identified in recent years, much still remains to be learned about natural mechanisms of antitumor immunity and how best to harness or induce these in clinical settings. Immunoediting Can Both Protect Against and Promote Tumor Growth To date, there are three proposed mechanisms by which the immune system is thought to control or inhibit cancer: By destroying viruses that are known to transform cells By rapidly eliminating pathogens and regulating inflammation By actively identifying and eliminating transformed cells the first two constitute the typical purview of immunity outside of a role in cancer: find and destroy foreign infectious agents. The third mechanism, involving tumor cell identification and eradication, is termed immunosurveillance. It posits that the immune system continually monitors for and destroys neoplastic cells. However, significant evidence from animal models, immune deficiency disorders, and induced immune suppression regimens in humans supports the notion that immunosurveillance is an important inhibitor of cancer. Likewise, in animal models, almost any form of immunosuppression leads to increases in the incidence of both spontaneous and induced cancers. These observations and experiments clearly demonstrate the power of the immune system to hold cancer at bay. Exactly how the immune system recognizes and targets neoplastic cells is the topic of the following section. However, recent data also point to potential protumor influences of the immune response on cancer. For instance, chronic inflammation and immune-mediated selection for malignant cells may actually contribute to cancer cell spread and survival. Contemporary studies of immunity to cancer have now generated a more nuanced hypothesis of immune involvement in neoplastic regulation, including both tumor-inhibiting and tumor-enhancing processes. In the mid-1990s, research using animal models of cancer suggested that natural immunity could eliminate tumors. Armed with this understanding, researchers identified some of the key cell types and effector molecules involved. This suggested that tumors growing in immune-deficient environments are more immunogenic, that is, they are easier for the immune system to recognize than those arising in an immunocompetent environment. These observations led to the idea that the immune system exerts a dynamic influence on cancer, inhibiting some tumor cells but also sculpting or editing them in a Darwinian process of selection: those that survive immune winnowing are better able to outwit the immune response and thus have a survival advantage. Thus was born the term immunoediting, to describe how the immune system engages in both positive (antitumor) and negative (protumor) actions that help to sculpt the tumor, determining which cells will be eliminated and which will remain. The first phase, elimination, is the traditional view of the role 1389 of the immune system in cancer, roughly analogous to immunosurveillance-identification and destruction of newly formed cancer cells. Equilibrium is the next phase, characterized by a state of balance between moderate destruction of neoplastic cells with survival of a small number of cancer cells. Ample clinical evidence now suggests that the equilibrium phase can continue for decades after the emergence of a tumor, whether it is treated or not. In fact, equilibrium states of cancer may be much more common than previously appreciated. During this process of survival of the fittest, environmental conditions that influence immune reactivity can have a significant role in lengthening or shortening this time period. Clinical identification of transformed cells at this stage can be tricky, despite the fact that this likely represents a fruitful window of time for intervention. When this is in balance, unhealthy cells are eliminated and new cells take their place. However, once this balance is tipped in favor or more cellular expansion than loss, tumors can arise. Recognition and targeting of tumor cells by the immune system is believed to occur in three phases. In the process, some cells acquire mutations that allow them to resist immune destruction. Over time, inhibitory immune responses begin to dominate and immune activity shifts from anti- to protumor. Tan cells are normal; pink to red cells 1390 represent progressive development of decreased immunogenicity in tumor cells. Immune escape is the final phase of immunoediting, when the most aggressive and least immunogenic of the residual tumor cells begin to thrive and spread, often thanks to help from immune pathways.
Syndromes
- Blood culture
- The time it was swallowed
- CT scan of the head with contrast dye
- Drug and medication intoxication
- Down syndrome
- If there is no response, shout for help. Tell someone to call 911 or your local emergency number. Do not leave the infant yourself to call 911 until you have done CPR for about 2 minutes.
- Bunionectomy and hammer toe repair
- Urge to urinate often
- Family history of AMD
- Malaise
Most fungal infections prevalent in the general population do not lead to severe disease and are dealt with by innate immune mechanisms and lead to protective adaptive responses erectile dysfunction lack of desire purchase discount cialis sublingual on-line. Other features of modern life that may contribute include mass distribution of food erectile dysfunction doctors minneapolis discount cialis sublingual 20 mg online, which exposes 1748 large populations to potentially contaminated food erectile dysfunction medication free samples buy genuine cialis sublingual on line, and unhygienic food preparation erectile dysfunction treatment mayo clinic buy cialis sublingual with a mastercard. The answer comes from the concept of original antigenic sin cheap erectile dysfunction pills uk cialis sublingual 20 mg otc, which posits that we only mount a primary response once we have exhausted the potential to use memory cells to eradicate the infection. Since most of our first encounters with influenza will vary, the years in which "all" of the key influenza epitopes are significantly "new" to each of us will also vary. It is only in these years that we experience a new primary response to influenza virus, and therefore symptoms of the flu are most severe. The limited growth of attenuated organisms within the host often eliminates the need for booster doses of the vaccine. Also, if the attenuated organism is able to grow along mucous membranes, then the vaccine will be able to induce the production of secretory IgA. The major disadvantage of attenuated whole-organism vaccines is that they may revert to a virulent form. They also are more unstable than other types of vaccines, requiring refrigeration to maintain their activity. The antitoxin was necessary because the girl had not been previously immunized and, therefore, did not have circulating antibody to tetanus toxin or memory B cells specific for tetanus toxin. Therefore, after the second injury 3 years later, she will require another dose of antitoxin. The Sabin polio vaccine is live and attenuated, whereas the Salk vaccine is heat killed and inactivated. The Sabin vaccine thus has the usual advantages of an attenuated vaccine compared with an inactivated one (see the answer to question 15). Moreover, since the Sabin vaccine is capable of limited growth along the gastrointestinal tract, it induces production of 1749 secretory IgA. Now that polio is rarely if ever seen in the United States, continuing use of a vaccine with the potential to revert to a more virulent form introduces an unwarranted element of risk to both the vaccinee and others who might contract the disease from them. The virus strains used for the nasally administered vaccines are temperature-sensitive mutants that cannot grow at human body temperature (37°C). The live attenuated virus can grow only in the upper respiratory tract, which is cooler, inducing protective immunity. These mutant viruses cannot grow in the warmer environment of the lower respiratory tract, where they could replicate and mutate into a disseminated influenza infection. T-cell epitopes generally are internal peptides, which commonly contain a high proportion of hydrophobic residues. Thus, synthetic hydrophobic peptides are most likely to represent T-cell epitopes and induce a cellmediated response, whereas synthetic hydrophilic peptides are most likely to represent accessible B-cell epitopes and induce an antibody response. In this hypothetical situation, the gene can be cloned into an expression system and the protein expressed and purified in order to test it as a recombinant protein vaccine. However, the plasmid containing the gene for the protective antigen must be suitably purified for use in human trials. Protection against such pathogens is achieved by repeated immunizations to maintain high levels of neutralizing antibody. Bacterial capsular polysaccharides, inactivated bacterial exotoxins (toxoids), and surface protein antigens. In addition, most vaccinated individuals, if exposed to the disease, will develop mild illness. Exposure of unvaccinated individuals to either source of disease would put them at 1750 risk for serious illness. Epidemics within adult populations would have more serious consequences, and infant mortality due to these diseases would increase. The antiserum you received 1 year ago protected you temporarily, but those antibodies are now gone and you have no memory B cells to produce new antibodies during this second exposure. Because the snake venom was coated with antibodies, naïve B cells were not activated during this first exposure and therefore no adaptive immune response was mounted. There are no residual cells or antibodies that were involved in the original encounter with this snake venom and, therefore, no recall response. Any connection between vaccination and a subsequent adverse reaction must be evaluated by valid clinical trials involving sufficient numbers of subjects in the control group (those given a placebo) and experimental group (those receiving the vaccine). This is needed to give a statistically correct assessment of the effects of the vaccine versus other possible causes for the adverse event. Such clinical studies must be carried out in a double-blind manner; that is, neither the subject nor the caregiver should know who received the vaccine and who received the placebo until the end of the observation period. In the example cited, it is possible that the adverse event (increased incidence of arthritis) was caused by an infection occurring near the time when the new vaccine was administered. Determining the precise cause of this side effect may not be possible, but ascertaining whether it is likely to be caused by this vaccine is feasible by appropriate studies of the vaccinated and control populations. The longer they presented antigen, the longer the host would respond to produce antigen-specific T cells. As discussed in Chapter 8, the thymus is the location for differentiation and maturation of helper and cytotoxic T cells. Thus, the thymocytes produced in the bone marrow of patients with DiGeorge syndrome do not have the ability to mature into effector cell types. In the adult, effector-cell populations have already been produced (peak thymus size occurs during puberty); therefore, a defect after this stage would cause less severe T-cell deficiency. After birth, these IgG molecules will supply the newborn with passive immune protection from many common bacterial infections, which can then be quickly dispatched by antibody-mediated mechanisms. Without the common chain, this does not occur and the development of lymphocytes is blocked. Some components of the immune system are responsible for regulating or suppressing the activity of leukocytes. When these pathways are defective, overactive immune responses can occur, leading to breaks in self tolerance that lead to attacks on self molecules, or autoimmune syndromes. Without this protein, the negative selection of T cells in the thymus that recognize self antigen is disrupted and autoreactive T cells emerge and instigate organspecific autoimmune attacks. Cytokines that activate T cells stimulate infection because they increase expression of receptors used by the virus. These cells can be activated and begin producing virus, thus causing a relapse of the disease. A third challenge is that the generation of broadly neutralizing antibodies that will react with most viral strains requires many somatic hypermutations that need to occur and be selected for over time. This example of the complexity of the immune system demonstrates that specific responses are not always easily predictable. However, based on the data presented in the table accompanying this question, one might predict that in the absence of T-cell help, there will be a significant impact on class switching. Clinical Focus Answer All individuals needing antiretroviral therapy are supposed to receive combination drugs to lessen the chance that resistant viral variants will survive. These drugs cross the placenta, which will prevent the fetus from becoming infected in utero. Treatment should continue for several weeks, and longer if the infant is breastfeeding. You could also perform fluorescence staining with antibody specific for the cytoplasmic heavy chain. Tumor antigens may be encoded by genes expressed only by tumors, may be products of genes overexpressed by the tumor or of genes normally expressed only at certain stages of differentiation, or may be products of normal genes that are altered by mutation. While some patients with metastatic melanoma had a positive response to this therapy it did not help all, possibly due to the inadvertent expansion of regulatory T cells. These are expanded ex vivo and reinfused into the patient, as a means to activate T cells specific for this prostatespecific antigen. These T cells should then home to the site of the tumor and help to eradicate prostate cancer cells expressing these antigens at high levels. These danger or damage signals would help to recruit leukocytes to the site (inflammation) and activate local antigen-presenting cells. The antigens presented by these cells might include both bacterial and local tumor antigens, acquired via phagocytosis of dead or damaged tumor cells. If antigens from the tumors were presented to naïve T cells, this could activate antitumor-specific adaptive responses. Other cancers that may be targets for such prevention include adult T-cell leukemia/lymphoma and the liver cancer that is linked to hepatitis B infection. Most cancers have not been clearly 1758 linked to an agent of infection, and therefore a preventive vaccine is not an option. If I wished to precipitate my antigen, I might elect to use a polyclonal preparation, as it would contain antibodies toward multiple different determinants on the antigen and therefore many antibody molecules could bind per antigen molecule, maximizing the chances that at least some of the antibodies could bind more than one antigen and facilitate precipitation. With time, the population of B-cell clones that respond to an antigen in an individual will change. Overall, the affinity of the antibodies in the serum will increase according to the methods described in Chapter 12. However, this means that the proteins with which individual antibodies will cross-react will change as the range of binding sites modulates, and this is what has happened in your experiment. I will have the most effective agglutination if antibodies can cross-link multiple sites on the bacterial surface. However, a monoclonal antibody would also work, as most antigens are repeated many times on the bacterial surface. If each only has a single site at which an antibody can bind, a bivalent antibody can cross-link only two proteins, and that would be insufficient to create a precipitate. If I am precipitating a protein with multiple copies of the same site, then monoclonal antibodies could still work. The antibody binds to the band, localizing an enzymatic reaction at the band and causing substrate conversion to product. A polyclonal antibody mixture would have the advantage that different antibodies could bind at different antigenic determinants on the target protein and therefore could give rise to a stronger signal. However, different bleeds of polyclonal sera would have different levels of cross-reactivity with other, structurally similar determinants on other proteins. Monoclonal antibodies will bind to predictable determinants, and, although they might still cross-react with structurally similar determinants on other proteins, those cross-reactivities are predictable and will not change from batch to batch. To achieve this, the heart and blood vessels must work in tandem with the respiratory and haematological systems to achieve adequate tissue and organ perfusion. Contracting at an average rate of 75 beats per minute (bpm), the human heart is said to contract up to 3 billion times in an average 80-year lifespan. Bridge to clinical medicine Anatomy · the heart is covered by a fibroserous sac called the pericardium and is located in the thorax between the lungs, in an area known as the mediastinum · the heart is a four-chambered, muscular structure comprising two atria and two ventricles, which serve to pump deoxygenated (largely venous) blood to the lungs and transport oxygenated (largely arterial) blood to organs and tissues. Aortic arch Ascending aorta Right coronary artery Right atrium Atrial arteries Anterior cardiac veins Small cardiac vein Marginal artery Circum ex artery Great cardiac vein Marginal artery Coronary sinus 12 Small cardiac vein Right coronary artery Marginal artery Middle cardiac vein Posterior interventricular artery Posterior cardiac vein Left ventricle 13 14 15 Anterior view Posterior view. When the heart is contracting, the intramuscular blood vessels are compressed and blood flow is at its lowest. Any increase in the heart rate reduces diastolic time more than systolic time, thus reducing coronary artery perfusion time. In patients with pre-existing disease (such as coronary artery disease or aortic stenosis), tachycardia may lead to reduced myocardial perfusion. W Cardiac pain is not found exclusively in the chest, but often radiates down the medial side of the left arm and up to the neck and jaw. This is because radiation occurs to areas that send sensory impulses to the same level of the spinal cord that receives cardiac sensation. The sensory fibres from the heart then travel up to T1T4, and radiation occurs in the medial left arm via dermatomes T1T4. When the arterial pressure falls, renin is released from the juxtaglomerular cells of the kidney. Cardiac catheterisation Involves passing catheters into the heart under radiographic guidance May be diagnostic or therapeutic Site of entry is identified, followed by administration of local anaesthetic; a guide wire is used to ensure correct placement of the catheter Classically, the right radial (preferred) or right femoral arteries are used for arterial access in angiography Haemodynamics may be measured during the process Relatively safe procedure, with a mortality rate <0. Myocardial perfusion scanning Form of nuclear stress testing Observes passage of gadolinium contrast through the heart via T1-weighted sequencing Contrast absorbed by myocardium; low signal indicates hypoperfusion Assesses for the presence of coronary artery disease Agents such as adenosine, dipyridamole and regadenoson are used as vasodilators in myocardial perfusion imaging stress tests. Vasodilator agents (such as dipyridamole and adenosine) should be used with caution in patients with a history of bronchospasm or carotid stenosis and dobutamine should not be used in patients with a history of ventricular arrhythmia. Beta blockers exert their effect by antagonising the action of epinephrine and norepinephrine at beta adrenergic receptors. They are prescribed to treat heart failure, arrhythmias and coronary artery disease, and should be used with caution in asthmatics. Antiplatelet agents prevent thrombus formation and are indicated in the prevention and treatment of cardiovascular events. Diuretics are used to treat oedema and heart failure by increasing urinary sodium excretion and urine output. Other lipid-lowering agents include ezetimibe (which inhibits intestinal absorption of 1. However, it should be borne in mind that, unlike statins, these medications do not lower mortality. P Atherosclerosis Atherosclerotic cardiovascular disease is the number one worldwide cause of death and disability. Pathologically, there is focal accumulation within the intimal layer of the arterial wall of cells, lipids, fibrous tissue and complex proteoglycans, eventually leading to the formation of an atherosclerotic plaque. Smoking is by far the greatest cause of preventable mortality and has been implicated as a risk factor in the development of numerous disease processes. This discrepancy is most commonly caused by atherosclerotic disease, although possible non-atherosclerotic causes, such as coronary artery anomalies (younger individuals) and systemic vasculitides (older individuals), should also be kept in mind. Ischaemic heart disease can be categorised as either stable angina or acute coronary syndrome.
Cheap cialis sublingual 20 mg. How To Treat Itchy Skin in Dogs Naturally at Home || Home Remedies for Itchy skin.
References
- Armstrong AJ, Garrett-Mayer ES, Yang YC, et al: A contemporary prognostic nomogram for men with hormone-refractory metastatic prostate cancer: a TAX327 study analysis, Clin Cancer Res 13:6396n6403, 2007.
- Hartford A, Zietman A, Shipley W: Proton radiotherapy. In DiAmico AV, Hanks GE, editors: Radiotherapeutic management of prostate cancer, New York, NY, 1999, Oxford University Press, pp 61n72. Haustermans KM, Hofland I, Van Poppel H, et al: Cell kinetic measurements in prostate cancer, Int J Radiat Oncol Biol Phys 37(5):1067n1070, 1997.
- Doglietto GB, Papa V, Tortorelli AP, et al. Nasojejunal tube placement after total gastrectomy: a multicenter prospective randomized trial. Arch Surg 2004;139(12):1309-1313.
- Yazar S, Eser B, Yalcin S, Sahin I, Koc AN. A case of pulmonary Microsporidiasis in an acute myeloblastic leukemia (AML) - M3 patient. Yonsei Med J 2003;44(1):146-9.
- Joviasis A, Kraag G. Acute gastrointestinal manifestations of systemic lupus erythematosus. Can J Surg 1987;30:185.
- McNeal JE: Significance of duct-acinar dysplasia in prostatic carcinogenesis, Urology 34(6 Suppl):9n15, 1989.
- Kang ES, Gerald PS. Hereditary tyrosinemia and abnormal pyrrole metabolism. J Pediatr 1970;77:397.
- Clowes AW, Clowes MM, Reidy MA: Kinetics of cellular proliferation after arterial injury. I. Smooth muscle growth in the absence of endothelium, Lab Invest 49:327, 1983.