
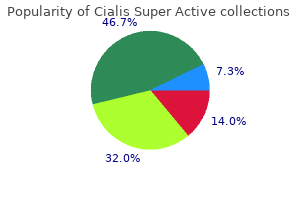
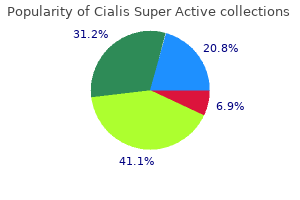
Cialis Super Active
| Contato
Página Inicial
Louis Flancbaum, M.D., FACS, FCCM, FCCP
- Associate Professor of Surgery, Anesthesiology,
- and Human Nutrition
- The Ohio State University Hospitals
- Columbus, OH
Successful treatment of a child with a primary intracranial rhabdomyosarcoma with chemotherapy and radiation therapy erectile dysfunction protocol food lists cialis super active 20 mg buy amex. Malignant fibrous histiocytoma originating at the site of a previous fronto-temporal craniotomy erectile dysfunction diabetes viagra discount cialis super active 20 mg buy. Primary thalamic malignant fibrous histiocytoma of the dominant hemisphere causing severe neuropsychological symptoms erectile dysfunction treatment aids buy cialis super active 20 mg overnight delivery. Primary intracerebral malignant fibrous histiocytoma: immunohistochemical findings and etiopathogenetic considerations erectile dysfunction pills from china generic 20 mg cialis super active. Sarcoma: a possible late result of effective radiation therapy for pituitary adenoma erectile dysfunction statistics worldwide purchase line cialis super active. Patient outcome at longterm follow-up after aggressive microsurgical resection of cranial base chondrosarcomas. Bifrontal meningeal fibrosarcoma in a patient with metastases to the liver, kidneys and suprarenal glands. On the primary meningeal tumors with special concern to the hemangiopericytoma pathology and biology. Hemangiopericytoma of the meninges (angioblastic meningioma of Cushing and Eisenhardt): clinicopathologic aspects and follow-up studies in 8 cases. Intracranial hemangiopericytoma: radiology, surgery, radiotherapy, and outcome in 21 patients. Hemangiopericytoma of the meninges: histopathological variability and differential diagnosis. Meningeal hemangiopericytoma: histopathological features, treatment, and long-term follow-up of 44 cases. Anaplastic meningioma versus meningeal hemangiopericytoma: immunohistochemical and genetic markers. Meningiomas: Their Classification, Regional Behavior, Life History, and Surgical Results. Morbidity, mortality, and quality of life following surgery for intracranial meningiomas: a retrospective study in 257 cases. Meningioma: analysis of recurrence and progression following neurosurgical resection. Excision of a large pineal region hemangiopericytoma (angioblastic meningioma, hemangiopericytoma type). Meningioma and intracranial hemangiopericytoma: a comparative electron microscopic study. Analysis of hemangiopericytic meningiomas by immunohistochemistry, electron microscopy and cell culture. Immunohistochemical staining for claudin-1 can help distinguish meningiomas from histologic mimics. Aberrations of chromosome segment 12q13-15 characterize a subgroup of hemangiopericytomas. Atypical and anaplastic meningiomas: radiology, surgery, radiotherapy and outcome. Meningeal hemangiopericytoma manifesting as massive intracranial hemorrhage-two case reports. Primary intracranial meningeal and spinal hemangiopericytoma: radiologic manifestations. Intracranial hemangiopericytomas: angiography, pathology, and differential diagnosis. Intracranial meningeal hemangiopericytoma: the role of radiotherapy: report of 29 cases and review of the literature. Anti-angiogenic treatment (sunitinib) for disseminated malignant haemangiopericytoma: a case study and review of the literature. Activity of temozolomide and bevacizumab in the treatment of locally advanced, recurrent, and metastatic hemangio-pericytoma and malignant solitary fibrous tumor. Adjuvant fractionated radiotherapy after resection of intracranial hemangiopericytoma. The role of radiotherapy in the management of malignant hemangiopericytoma: report of eleven new cases and review of the literature. Fortunately, over the past few decades our understanding of the natural history of the disease has dramatically progressed, coupled with refinements in surgical techniques and the advent of radiation options. This combination of advances has led to improved outcomes for our patients both oncologically and in terms of quality of life and functional outcome. Radiation options are then considered, and the chapter concludes with a discussion of surgical and radiationrelated complications, as well as strategies for avoidance and management. The later discovery of Schwann cells as the oncologic cells of origin2 and the finding that the lesions were typically confined to the vestibular division of the eighth cranial nerve3 led to the recommendation by a consensus meeting in 1992 to use the term vestibular schwannoma, which is used throughout this chapter. In the literature, the terms acoustic neurinoma, acoustic neuroma, and vestibular schwannoma are used interchangeably. Several reports followed, and in 1830 the British physician Charles Bell provided the first detailed, accurate description of these lesions. The unilateral suboccipital craniectomy, the predecessor to the modern retrosigmoid craniotomy, was described by Woosley in 1903. Cushing also advocated for subtotal removal of the mass in order to avoid paralysis of the facial nerve. An advantage to the bilateral suboccipital approach was that the contralateral side could be explored in the same setting should a lesion not be found at the expected location. House went on to popularize the translabyrinthine and middle cranial fossa approaches. In the early 20th century the mortality rate was as high as 86%, but was reduced to 20% by Harvey Cushing. For similar reasons, the mean tumor size at time of diagnosis in the same data set declined over the years and leveled out around 10 to 15 mm, with large and giant tumors representing 6% of all tumors. In a review of the literature by Sughrue and colleagues,24 among 982 patients the mean initial tumor size was 11. This was further confirmed when the same findings were noted in a prospectively followed group of 59 patients treated conservatively by the same group. Of extrameatal tumors, 1% decreased in size, 70% remained unchanged, and 29% increased in size. Notably, none of the tumors demonstrated growth after the fifth year of observation. The presence of tinnitus at presentation increases the odds of tumor growth threefold. Cystic lesions have been reported to have the potential to undergo sudden and dramatic growth28,29; some series have reported higher rates of facial palsy with surgical treatment of cystic lesions,27,30,31 and others reported reduced rates of hearing preservation. Furthermore, in the past decade, rates of microsurgical resection have dropped from greater than 90% to 53%, and rates of radiosurgery have increased from 5% to 24%. Additionally, quality of life for patients undergoing observation did not significantly change over the observation period. The relationship between the facial nerve (light yellow) and the vestibulocochlear complex (dark yellow) is shown. The structures of the inner ear are shown in purple, while the tympanic membrane and the ossicles are shown in blue. As the tumor grows, the normal fascicles are displaced and flattened along the capsule. The lesions arise near the transition point between glial and Schwann cells, known as the Obersteiner-Redlich zone,44 which occurs near or at the porus acusticus. In over 90% of cases, the lesions arise from, and remain confined to , the inferior division of the vestibular nerve. In contrast, Antoni B tissue consists of loosely arranged cells with multipolar processes, with frequent microcyst formation. With rare exceptions, residual nerve fibers are not dispersed through the substance of the lesion. As the tumor volume increases, the pons and lateral medulla are compressed with resultant initial effacement, and eventual obliteration, of the fourth ventricle and resultant obstructive hydrocephalus. Oftentimes, the initial symptoms result from local irritation of the vestibular or cochlear portion of the eighth cranial nerve and are episodic. B, Schwannomas contain Antoni A tissue, composed of compact spindle cells, and loose-textured Antoni B areas. C, the juxtaposition of cellular Antoni A and loose Antoni B patterns is classic for conventional schwannoma. D, Verocay bodyrich schwannomas are frequent in the spinal intradural compartment. American Academy of OtolaryngologyHead and Neck Surgery Hearing Classification Class Pure-Tone Average(dB) 30 >30 >50 Any and and 50 and and level Speech Discrimination(%) 70 50 50 <50 and patient adaptation, it is not unusual for symptoms to be neglected for a long period of time prior to presentation. The examination findings in the series by Ojemann and colleagues55 are summarized in Table 149-1; these results are commensurate with the findings by Harner and Laws56 and Pulec and coworkers57 in similar series. The audiologic A: Useful B: Useful C: Capable of aid D: Nonfunctional examination will typically show loss of hearing at high frequencies with speech discrimination being more affected than pure tone, indicating a retrocochlear lesion. As tumors grow into the extrameatal space, they acquire the characteristic "ice-cream cone appearance. In addition, there is a homogeneous pattern in small noncystic tumors, and a heterogeneous pattern in large and cystic lesions. Although meningioma has a similar appearance on T1- and T2-weighted sequences, calcifications are more common and a broad dural base can sometimes be seen. In addition, hyperostosis of the adjacent bone may be seen and is a hallmark of meningioma. Schwannoma may occur in another cranial nerve, of which the trigeminal nerve would be the next most common. Vascular lesions, including vertebrobasilar dolicoectasia and aneurysms, demonstrate flow voids and are well delineated on vascular imaging, such as magnetic resonance angiography. Metastasis should be suspected in the patient with a known primary malignancy, especially in the presence of multiple intracranial lesions and/or suspicious leptomeningeal enhancement. A bidirectional tool for the conversion of volumetric and linear indices of tumor size has been devised in order to facilitate grouping of data from disparate sources. Using a volume-doubling time model, Varughese and colleagues demonstrated prospectively that a 5-year cutoff is adequate to distinguish growing from nongrowing tumors. In particular, the proportion of intrameatal to extrameatal tumor is important for surgical approach selection (see "Surgical Approaches" section later in the chapter). The use of optimal monitoring techniques, along with the ability to correctly interpret and troubleshoot intraoperative signal changes, is critical for maximizing neural preservation. During the operation, a direct stimulation probe is applied to the area of the facial nerve and an electrical stimulus is delivered. Multiple waveforms of motor potentials have been described, and can be studied by the electrophysiologist in the operating room to provide additional feedback regarding the health of the nerve. Furthermore, there is the risk of overstimulation of the nerve as well as iatrogenic injury from the probe. To minimize this risk, low stimulation frequency and the use of a pulsed (noncontinuous) stimulus are recommended, and electrocautery should be avoided when possible. After placement of a negative electrode at the contralateral mastoid and a scalp reference electrode, a recording electrode is placed directly on the nerve proximal to the tumor resection and an external auditory stimulus is applied. The resulting action potential is measured, and typically results in two negative peaks with high amplitude designated "N1" and "N2. The main factors influencing surgical approach choice are tumor size, extent of cisternal versus intracanalicular growth, and baseline hearing function. Stimulation is then performed in the opposite ear in order to subtract the signals from the contralateral side. Utilizing the same anatomic landmarks and a smaller craniotomy, an endoscope is used in place of the microscope, resulting in the potential for less cerebellar retraction with the ability to look around corners. Gross total resection rates of 94% with retention of serviceable hearing in 57% of cases have been reported (tumor size range: 0. A shoulder roll is avoided if possible to maximize the space between the operative field and the ipsilateral shoulder, although one is used if head rotation is limited by cervical spondylosis. Attention must be paid so as to not overrotate the head and impair jugular venous drainage. All potential pressure points should be adequately padded, and the patient must be well secured to the operating table to allow freedom of table rotation during surgery. Typically, 1 g/kg of mannitol, 2 g of cefazolin, and 10 mg of dexamethasone are administered prior to skin incision. Intraoperative monitoring is employed routinely; at our institution we used motor evoked potentials, somatosensory evoked potentials, and direct stimulation of the facial nerve. The design of the surgical incision depends on the target pathology: for tumors with a significant intracanalicular component, a curvilinear incision starting at the level of the top of the pinna and extending down to the bottom of the mastoid is preferred. This incision allows for a larger craniotomy with the ability to take a more oblique look toward the porus acusticus. B, A suboccipital craniotomy is performed medial to the sigmoid sinus, including exposure of the sigmoid and transverse sinuses and their junction. C, the posterior wall of the porus can be drilled to expose the internal auditory canal. The dissection is complete when key bony anatomic landmarks are identified: the base of the mastoid, the digastric groove, and the tip of the mastoid. A single self-retaining retractor, such as a curved cerebellar retractor, is used. Neuronavigation may be used to confirm and mark the location of the transverse sinus, the sigmoid sinus, and the transversesigmoid junction. Our preferred method for the craniotomy is to drill away the outer table along the sinuses using a 6-mm cutting bur and then skeletonize the sinuses using a 5-mm diamond bur.
Such symptoms can also accompany the neurological effects of the complex and often harsh therapies that are commonly used to delay progression or improve survival in patients with malignant disease erectile dysfunction 18 cialis super active 20 mg. Given the highly structured nature of the nervous system erectile dysfunction treatment psychological causes purchase cialis super active 20 mg amex, neurological symptoms can be used at the time of presentation of the patient to often accurately localize the lesion erectile dysfunction overweight buy cialis super active 20 mg amex, which can enable the clinician to efficiently choose the most optimal tests for confirming diagnosis impotence world association buy cialis super active 20 mg. Neurological symptoms associated with malignancies can be classified in several ways erectile dysfunction new treatments purchase cialis super active 20 mg without prescription. First, from a temporal perspective, the presentation of such symptoms can be acute, subacute, or chronic. For instance, primary brain tumors can sometimes present with slowly progressive decline of cognitive function whose relationship to the tumor is often recognized in retrospect after diagnosis. In the case of low-grade gliomas, such a presentation may span over months and even years. Conversely, patients may present suddenly with a seizure or a sudden severe headache, heralding the diagnosis. However, unlike tension-type headaches, they are worsened with changes in position, particularly on bending down. The International Headache Society Classification of Headache Disorders in its second edition distinguished headaches attributed to increased intracranial pressure or tumorinduced hydrocephalus from those attributed directly to the brain tumor (Box 120-1). Meninges and their associated portions of the cerebral vasculature are the only intracranial sites from which pain can be evoked7; their distortion by increased intracranial pressure due to tumor mass, surrounding edema, or hydrocephalus can generate headaches. An anecdotal report of transient response of headaches related to a glioblastoma to sumatriptan, a serotonin receptor agonist, suggest the possible existence of neurotransmittermediated mechanisms for some of these headaches. In a retrospective study, seizures were reported to occur as a presenting symptom in approximately 40% of patients with primary brain tumors and 20% of those with brain metastases. Only 18% of patients had higher seizure frequency (>4/month) or status epilepticus (12%); such frequent seizures are more frequently associated with lowgrade gliomas. Most patients who have seizures associated with their diagnosis of seizures are treated with a single anticonvulsant (>60%), with levetiracetam being the most commonly used anticonvulsant (60%). However, assessment of the role of anticonvulsants in these studies did not fully take into account tumor grade and type, location and size, and extent of resection. Nocturnal or early-morning headaches have been attributed to brain tumors, particularly in relation to increased intracranial pressure, but this feature is inconsistent. Headaches due to brain tumors can occur at any time during the day; conversely, earlymorning headaches can result from other other causes6; hence this is generally a nonspecific and unreliable symptom for diagnosis of brain tumors. Headaches associated with brain tumors can result from mechanical or physiologic causes. Other factors that are postulated to drive seizures associated with brain tumors include changes in ion channels, especially extracellular potassium levels; peritumoral alterations in pH, which increase membrane excitability; elevated levels of connexin 32 and connexin 43, leading to synchronization of potentials in peritumoral neuronal networks; and alterations in blood-brain barrier that can disrupt local homeostasis of electrochemical factors leading to greater propensity to epileptogenesis. This symptom can also occur more prominently owing to the secondary effects of the tumor, such as increased intracranial pressure, seizures, hydrocephalus, depression, or language disturbances, which may mask the underlying, more subtle direct cognitive dysfunction from these tumors; this is also made more challenging by the fact that cognitive function is not routinely assessed at the time of initial diagnosis. However, formal studies that have assessed baseline cognitive function in patients with brain tumors have indicated that more than 90% of these patients manifest some degree of cognitive dysfunction before surgery or other treatments, suggesting that this is a fundamental symptom associated with brain tumors. Cognitive dysfunction has also served as a predictive and prognostic factor associated with outcome. In addition to the direct effects of tumor on cognition, therapeutic interventions against cancer can also affect cognitive function; systemic therapy can cause cognitive impairment in the absence of brain involvement (the so-called chemo-fog). Although such effects can occur in patients of all ages, they are especially seen in long-term survivors of cancer and in elderly patients with malignancies. However, tumors can also induce more subtle effects on the brain that can affect cognitive function. For instance, hippocampal avoidance using carefully planned fields has been used to prevent radiationinduced effects on short-term memory and did not appear to compromise tumor control. Patients typically present with progressive inability to use the contralateral limbs, which, in turn, may affect limb strength, gait, and balance and thus activities of daily living. The tempo of this weakness (progressive over weeks to months) is the main discriminator from other causes of focal weakness such as cerebrovascular disease. Otherwise, clinical findings on examination are identical to upper motor neuron signs of weakness associated with increased tone, extensor plantar responses, and Hoffman signs on the contralateral side. Distal weakness can also occur predominantly in the extremities owing to sensorimotor dysfunction associated with treatment-related or diseaserelated neuropathies. Steroid myopathy can manifest as proximal weakness that can also be confounding given that it may present as gait disturbance or falls. Aggressive physical and occupational therapy to maintain range of motion and muscle bulk and tone are important to allow recovery of strength when there is no direct damage to the major corticospinal pathways. VisionChanges Lesions that impair the function of the eye (retro-orbital or skull base tumors), optic nerve (meningioma, optic glioma, pituitary tumors, ophthalmic tract tumors, lymphoma), or occipital lobe (glioma, metastases, lymphoma) can result in altered vision. Optic nerve lesions produce unilateral visual loss; pituitary tumors that affect the chiasm can cause a bitemporal hemianopsia, whereas occipital lesions result in homonymous hemianopia. Quadrantanopsias can result from temporal lobe (which can cause a contralateral upper quadrantanopsia) or parietal lobe tumors (resulting in an inferior quadrantanopsia). Pupillary abnormalities and oculomotor abnormalities may be caused by tumors growing in the base of the brain and involving the third cranial nerve, fourth nerve, or sixth nerve. Psychological, Behavioral, and Psychiatric Symptoms Patients with brain tumors frequently have comorbid psychological and psychiatric symptoms that are often not recognized or addressed. Adjustment disorder and acute stress disorder were the most common psychiatric diagnoses in patients with brain tumors, with most patients experiencing high psychosocial distress. Accurate identification of these disorders would obviously be critical to the proper choice of interventions. Of note, in a study comparing distress and psychiatric disorders in patients with brain metastases versus those with systemic cancer without brain metastases, it was found that there were no significant differences in the course of the symptoms in these two groups,48 suggesting that unlike patients with newly diagnosed primary brain tumors, those with existing cancer who develop new brain metastases have a different neuropsychological response to the diagnosis. Steroids, which constitute a mainstay in the management of edema in patients with brain tumors, are also associated with psychiatric side effects, including depression, euphoria, paranoid ideation, and anxiety. Overall the cumulative effects of neurobehavioral and psychiatric effects of disease and treatments contribute significantly to the impact on global quality of life of patients with brain tumors. A variety of cerebellopontine angle tumors can particularly involve the facial and vestibulocochlear nerves and cause hearing impairment along with facial weakness and vertigo. Cerebellar tumors could manifest with dysarthria owing to difficulty in articulation. Focal Symptoms of Brain Tumors and Treatment Effects Focal clinical manifestations of brain tumors are dependent on the location of the tumors within the brain and the degree to which they distort or disrupt the structural components of the nervous system (see Table 120-2). GaitDisturbance Hemiparesis resulting from a tumor can cause a circumduction gait owing to increased tone and weakness on the side contralateral to the tumor, usually located in the frontal lobe. Parietal tumors can cause loss of proprioception, astereognosis, and sensory ataxia due to inability to recognize limb position that can result in gait impairment and falls. Patient-Reported Symptoms as End Points for Clinical Trials the improvement in patient symptoms and overall quality of life is arguably the most important end point other than improved survival of any treatment of cancer, including brain tumors. Neurooncology researchers and scientists have recognized that the focus on responses and survival misses the "other benefit" of treatments, including quality-of-life improvement. It included measures to assess patient-oriented outcomes, including cognition, symptoms, and quality of life in a prospective way. Importantly, it was demonstrated that this approach is feasible, with baseline data being collected on more than 80% of patients. However, it is likely that autoimmunity to cancer with central and peripheral nervous system involvement is more common and is not recognized because the symptoms are very mild or ascribed to other causes. Additionally, since these original incidence estimates were made, increased awareness, better definition of these conditions, and improvement in antibody detection techniques would probably make for a much higher frequency of paraneoplasia in cancer patients. The importance of recognizing a paraneoplastic disorder lies mostly in the early detection of an occult cancer but also in the specific treatment of the syndrome to reduce the associated symptoms and disability. The most effective treatment for paraneoplastic neurological disorders is treatment of the underlying cancer. However, additional immunomodulatory treatment is sometimes necessary in severe or refractory cases. In 2004, Graus and colleagues published diagnostic criteria for neurological paraneoplastic syndromes. A possible paraneoplastic syndrome, on the other hand, had three possible scenarios according to the panel: (1) a classical syndrome, no onconeural antibodies, no cancer but at high risk for having an underlying tumor; (2) a neurological syndrome (classical or not) with partially characterized onconeural antibodies and no cancer; and (3) a nonclassical syndrome, no onconeural antibodies, and cancer present within 2 years of diagnosis. The authors further describe the classical syndromes and onconeural antibodies reported to date. The typical initial symptom is dizziness, including vertigo; but unchecked, the condition will result in severe cerebellar dysfunction with dysarthria, double vision, and often profound truncal and appendicular ataxia. Neurological examination is usually remarkable for limb incoordination and nystagmus. Significant disability is very common, with up to two thirds of patients losing the ability to walk by the time treatment halts further progression. Immunomodulatory therapies and chemotherapy, including corticosteroids, immunoglobulin G, cyclophosphamide, tacrolimus, mycophenolate mofetil, and plasma exchange, have been tried. Although there is clearly a rationale for such therapies in the peripheral nervous system, establishing any benefit is extremely difficult, as has been recently reviewed. There is a subacute onset of sensory symptoms, often followed by rapid progression. More commonly there is an associated encephalomyelitis, designated as paraneoplastic encephalomyelitis with sensory neuronopathy. Both clinical and laboratory outcomes showed improvement with a reduction in lower motor severity score, rage score, and nighttime awakenings; there was a notable reduction in the number of children with opsoclonus, action myoclonus, drooling, ataxia, and rage. Normal channel function results in acetylcholine vesicle release from the presynaptic membrane into the synaptic cleft; the process is hampered by autoimmune attack on the channels. Symptoms may improve after plasmapheresis or immunosuppression, supporting the notion that the illness is humoraly mediated. Treatments that increase transmitter release may also improve the weakness; 3,4-diaminopyridine appears to be particularly effective. Although improvements in radiologic tumor response, progression-free survival, and overall survival have long been considered important goals of therapy, it is only recently that the significance of patient experience in terms of physical and psychological systems in the course of the disease has been recognized. Emerging evidence shows that early and comprehensive attempts to identify such symptoms using well-validated and appropriate tools and to institute appropriate interventions along with the direct treatment approaches against the tumor will affect patient outcome. This also necessitates educating medical care providers about the importance of identifying and addressing symptoms early to ensure the best quality of life for the patient and family during the course of the disease. Marie and colleagues reviewed the medical literature over a 44-year period (1966 to 2010) and found 115 cases of inflammatory myopathy associated with leukemias and lymphomas; additionally they reported 32 patients from their series in what is probably the largest series to date looking at this association. The serum creatine kinase is elevated up to 10 times the normal value, and the electromyogram demonstrates findings of myopathy. The rash of dermatomyositis is most commonly diffusely erythematous over the chest and shoulders in a V-shaped distribution. A minority of patients also have a red-violet heliotrope rash over the upper eyelids. Incidental findings on brain magnetic resonance imaging: systematic review and meta-analysis. The international classification of headache disorders, 3rd edition (beta version). Headache secondary to mass responsive to sumatriptan: a brief report from primary care. Frequency of seizures in patients with newly diagnosed brain tumors: a retrospective review. Practice parameter: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Epilepsy in patients with brain tumours: epidemiology, mechanisms, and management. Electrocorticographic discharge patterns in glioneuronal tumors and focal cortical dysplasia. Compromised glutamate transport in human glioma cells: reduction-mislocalization of sodium-dependent glutamate transporters and enhanced activity of cystine-glutamate exchange. In vivo assessment of highgrade glioma biochemistry using microdialysis: a study of energyrelated molecules, growth factors and cytokines. Neurobehavioral status and health-related quality of life in newly diagnosed high-grade glioma patients. Cognitive improvement in meningioma patients after surgery: clinical relevance of computerized testing. A global analysis of multitrial data investigating quality of life and symptoms as prognostic factors for survival in different tumor sites. Cognitive predictors of understanding treatment decisions in patients with newly diagnosed brain metastasis. Cognitive effects of cancer systemic therapy: implications for the care of older patients and survivors. Reduced efficiency of functional brain network underlying intellectual decline in patients with low-grade glioma. Evaluation of resting state networks in patients with gliomas: connectivity changes in the unaffected side and its relation to cognitive function. Disruption of prefrontal brain activation top-down control of working memory capacity as possible mechanism for chemo-fog/brain (chemotherapy-associated cognitive impairment). Interventions for preventing and ameliorating cognitive deficits in adults treated with cranial irradiation. Hippocampal dysfunctions caused by cranial irradiation: a review of the experimental evidence. Comorbid mental disorders and psychosocial distress in patients with brain tumours and their spouses in the early treatment phase. Neurobehavioural changes in patients following brain tumour: patients and relatives perspective. Distress, anxiety and depression in patients with brain metastases before and after radiotherapy. The level of patientreported outcome reporting in randomised controlled trials of brain tumour patients: a systematic review. Paraneoplastic cerebellar degeneration associated with antineuronal antibodies: analysis of 50 patients.
Expression of the brachyury gene has been identified as a definitive diagnostic marker that is common and specific to all chordomas erectile dysfunction medications injection cialis super active 20 mg buy online. Recent advances in radiation therapy provide more avenues for clinicians to consider minimizing neurological dysfunction erectile dysfunction natural treatment options discount cialis super active online visa, even at the price of residual tumor other uses for erectile dysfunction drugs cialis super active 20 mg order free shipping, with primary or adjuvant radiation therapy erectile dysfunction treatment by injection discount cialis super active 20 mg buy online. Ongoing investigations in radiation therapy include the optimization of species of hadron-based therapy erectile dysfunction photos 20 mg cialis super active purchase overnight delivery, and the efficacy of positron emission tomography to affect delivery of intensity-modulated proton therapy (and the ability to detect relative tumor hypoxia) in an attempt to overcome radiation resistance. Conventional chemotherapy is of limited utility; molecular targets offer the best hope for improved effectiveness. Several cultured human chordoma cell lines have been successfully generated in preclinical studies. Certain tyrosine kinases and transcriptional regulators are also overexpressed in chordoma. En bloc resection of primary sacral tumors: Classification of surgical approaches and outcome. Anthracycline, cisplatin, alkylating agents, and camptothecin analogues have been anectodally reported to affect chordomas, with greater sensitivity of dedifferentiated chordoma. A clinical benefit rate (complete response plus partial response and stable disease for longer than 6 months) of 73% was reported. Endonasal endoscopic approach for the resection of chondroid chordoma with skull base involvement. Incidence and relative survival of chordomas: the standardized mortality ratio and the impact of chordomas on a population. En bloc excisions of chordomas in the cervical spine: review of five consecutive cases with more than 4-year follow-up. Benign notochordal cell tumors: a comparative histological study of benign notochordal cell tumors, classic chordomas, and notochordal vestiges of fetal intervertebral discs. Intraosseous benign notochordal cell tumours: overlooked precursors of classic chordomas Clinical outcome for patients with dedifferentiated chondrosarcoma: A report of 9 cases at a single institute. First histologically confirmed case of a classic chordoma arising in a precursor benign notochordal lesion: Differential diagnosis of benign and malignant notochordal lesions. Brachyury: A diagnostic marker for the differential diagnosis of chordoma and hemangioblastoma versus neoplastic histological mimickers. An assessment of the reliability of the Enneking and Weinstein-Boriani-Biagini classifications for staging of primary spinal tumors by the spine oncology study group. Endoscopic endonasal minimal access approach to the clivus: case series and technical nuances. Beyond the nasoseptal flap: Outcomes and pearls with secondary flaps in endoscopic endonasal skull base reconstruction. En bloc resection of primary sacral tumors: classification of surgical approaches and outcome. Long-term clinical outcomes following en bloc resections for sacral chordomas and chondrosarcomas: A series of twenty consecutive patients. Prognostic factors and outcome of pelvic, sacral, and spinal chondrosarcomas: a centerbased study of 69 cases. Proton radiation therapy for head and neck cancer: a review of the clinical experience to date. Dosimetric accuracy of proton therapy for chordoma patients with titanium implants. Current comprehensive management of cranial base chordomas: 10-year meta-analysis of observational studies. Radiation therapy for chordoma and chondrosarcoma of the skull base and the cervical spine: prognostic factors and patterns of failure. Stereotactic radiosurgery of intracranial chordomas, chondrosarcomas, and glomus tumors. Radiosurgery with photons or protons for benign and malignant tumours of the skull base: a review. Long-term control of clival chordoma with initial aggressive surgical resection and gamma knife radiosurgery for recurrence. Residual postoperative tumour volume predicts outcome after high-dose radiotherapy for chordoma and chondrosarcoma of the skull base and spine. Glomus tumors have long been known to consist of nests of cells closely associated with blood vessels and nerves, but their origin has only been clarified relatively recently. Specifically, the paraganglia of the head and neck are closely associated with the parasympathetic nervous system. However, this vascular theory was proved false, and for this reason the name "glomus," denoting also the nest-like morphology, is a misnomer, although it is still widely used. For example, the term chemodectoma, which has mainly been used to refer to carotid body tumors, accurately describes the oxygen-sensing properties of some such tumors, although it is not applicable to all. Hence the term paraganglioma, prefaced by the anatomic site of origin, is currently preferred. From here, they may grow upward to the skull base, through the jugular foramen, or posterior to the mastoid tip. In 1743, von Haller described the carotid body, but not its chemosensory nature, mistaking it for a sympathetic ganglion (which he termed the "ganglion minutum"). In 1903, the histologist Kohn deduced that a series of cell aggregates of the adrenal medulla, carotid body, and other tissues forming ganglion-like bodies represented a homogenous population that he called the "paraganglionic system. According to Glenner and Grimely, such tumors are extra-adrenal paragangliomas, distinct from the adrenal medulla paragangliomas, which are more accurately referred to as pheochromocytomas. This was mainly due to the particular anatomic site and great vascularization of these tumors, not to mention the lack of high-definition imaging techniques. Semmes, in 1951, was the first to surgically remove a glomus jugulare tumor by a suboccipital approach, publishing its description 2 years later. He managed to remove all of the tumor invading the posterior fossa, but not the parts affecting the mastoid or middle ear. He performed a postauricular hypotympanotomy, opening the auditory canal through a retroauricular skin incision and raising a tympanomeatal flap to expose the lower part of the middle ear. In this technique, the external auditory canal skin is temporarily removed to perform a wide-open hypotympanotomy. However, this approach only enabled the complete resection of small glomus jugulare tumors with medial extension, and it was not effective for tumors involving the anterior and medial surfaces of the carotid artery. In the same year, McCabe and Fletcher proposed a new classification system based on their observations of the symptomatology of 45 cases of glomus jugulare tumors, taking into account their extent on radiologic examination (x-ray, retrograde jugulography, and carotid arteriogram) and surgery. Kempe and colleagues, for example, reported in 1971 the combined use of suboccipital craniectomy and standard mastoidectomy to remove a tumor invading the temporal bone and posterior fossa. This forward extension of the translabyrinthine approach, which they had reintroduced in the early 1960s,39,53-55 involves posterior transposition of the entire facial nerve, including the labyrinthine and the intracanicular segments. It also permits wide exposure of the anterior cerebellopontine angle and clivus and partial control of the vertical portion of the internal carotid artery,57 at the expense, however, of the blood supply to the facial nerve. The facial nerve is mobilized along its entire mastoid and tympanic course up to the geniculate ganglion, and the external auditory canal, tympanic membrane, and ossicular chain are removed. These include those proposed by Kempe (1982),68,69 Spector and colleagues (1976),70 and de la Cruz (1994),71 who correlated the anatomic classification with the appropriate surgical approach as follows: tympanic transcanal approach, hypotympanic mastoid-extended facial recess, jugular bulb mastoid-neck (fallopian bridge technique or partial facial nerve rerouting), carotid artery infratemporal fossa, transdural infratemporal fossa or intracranial. These classifications also include those proposed by Sanna and associates (2010),72,73 who modified the Fisch system on the basis of clinical findings, dividing class A into two subgroups and class B into three; Rockley and Hawke (1990)74; Green and colleagues (1994)75; Lawton and coworkers (1998)76; and Borba and associates (2010),58 whose classification system was based on tumor extent and vascularization, and preservation of the facial nerve and middle ear structures. This last classification yielded four types of tumor associated with four corresponding surgical approaches, namely, infralabyrinthine retrofacial (type A); infralabyrinthine prefacial and retrofacial, without (type B) and with (type C) occlusion of the external acoustic meatus; and infralabyrinthine with transposition of the facial nerve (type D). Since the end of 1980s, the potential of the surgical option, in terms of radicality, has been greatly improved by the use of combined approaches as well as the availability of computerized intraoperative support tools. Similarly, in 1989, Bordi and associates described a single-stage posterolateral combined otoneurosurgical approach,83 and in 1994, Patel and coworkers used subtemporal-infratemporal, retrosigmoid, and/or extreme lateral transcondylar approaches in combination with the usual transtemporal-infratemporal approaches. In 2002, Al-Mefty and Teixeira described a combined approach to expose both the extracranial and intracranial extensions of the lesion as the key to their successful resections of "complex glomus jugulare tumors" (in which one or more of the following criteria had to be met: giant size, multiple paragangliomas, malignancy, catecholamine secretion, association with other lesions, previous treatment with adverse outcome). Radical resection of paragangliomas situated around the jugular foramen, the lower clivus, and the high cervical region from an anterolateral direction was proposed in 2006 by Liu and coworkers. This technique grants total exposure of the jugular foramen with multidirectional angles of attack as well as exposure of the infratemporal carotid artery without the need to transect the external ear canal, permanently reroute the facial nerve (which is fully skeletonized from the genu to the stylomastoid foramen but not anteriorly transposed), or translocate the mandible. The need to avoid anterior transposition of the facial nerve was also noted by Borba and colleagues,39,58,77 who also stated that this could be achieved even in radical removal of Fisch class C and D tumors. That being said, preserving the function of the facial and lower cranial nerves has always been a major challenge in temporal paraganglioma surgery. The results were so dismal that Martin, in his 1957 textbook of head and neck tumors, recommended that large cervical tumors that encase the carotid vessels not be resected. In 1971 Shamblin and colleagues developed their classification system designed to help assess the resectability of these tumors. This comprised three main stages, depending on the position of the tumor relative to the jugular foramen, the third stage being subdivided to reflect the degree of carotid canal involvement and intracranial extension. First described by Dawbarn in 1904,121 embolization was described as a kind of "starvation plan" for treating facial carcinomas and sarcomas, and was to have great repercussions on paraganglioma surgery. After surgical exposure, Dawbarn cannulized the external carotid artery and injected liquid paraffin into its branches to deprive the tumor of its blood supply. Although he documented many cases of tumor regression brought about by this approach, the technique was roundly criticized by his colleagues. Cerebral angiography had been introduced by Moniz in 1926, who injected contrast material into the surgically exposed cervical carotid arteries. The first embolization of a glomus jugulare tumor was described by Hekster and colleagues in 1973. In 1994, Casasco and associates documented the first direct intralesional embolization of two paraganglioma types, carotid and jugular, which they achieved using percutaneous puncture and two-dimensional fluoroscopy to check the position of the needle. In the same year, Cohen and coworkers also reported the implant of a covered stent, this time within the intracranial portion of an internal carotid artery encased by a temporal paraganglioma. Initially, many were skeptical about the outcomes that could be achieved and concerned about the radioresistance of such tumors. The initial energy source was later replaced by cobalt-60 and fueled the invention of the Gamma Knife, first prototyped in 1968. This tool used gamma rays in a very similar way to a scalpel and remains a valid neurosurgical implement to this day. This technique was proposed by Wilson in 1946, and the first treatments were performed in 1954. Despite its apparent effectiveness, this technique is limited by relatively high cost, and there are currently very few centers that offer it as a radiosurgery option. In turn, the extra-adrenal paraganglia can be classified into two types: sympathetic, that is, localized in the paravertebral and para-aortic regions; and parasympathetic, that is, situated almost exclusively in the head and neck. Ten to 15% of tumors of the adult paraganglion system are extra-adrenal, and 3% of these occur in the head and neck. Typically, they do not hypersecrete catecholamines, and they often remain undetected until they provoke mass effects. About 35% of the cases described are familial,163 which feature a significantly lower age of onset. In maternal genomic imprinting, for example, the maternal allele is silenced and the paternal allele expressed. In this case, therefore, only mutations inherited from the father are pathogenic and may lead to tumor development (an affected father will transmit the disease to 50% of his progeny), but the offspring who inherit the mutation through maternal transmission will be carriers. Likewise, these mutations also display incomplete penetrance and variable expression. Oxidative stress and apoptosis resistance, potentially interlinked with mitochondrial dysfunction and activation of the hypoxic pathway, have also been proposed as potential mechanisms underlying the tumorigenesis. In the oxidative stress hypothesis, it has been suggested that a pathogenic mutation in succinate dehydrogenase impairs mitochondrial function, thereby depriving the body of the main source of pro-oxidants generated during oxidative phosphorylation. This would lead to severe oxidative stress, creating a significant imbalance between the levels of pro-oxidants and antioxidants. Histopathology the histologic appearance of paragangliomas is similar to the normal histology of the paraganglia. Paraganglia contain two types of cells, both housed in a dense network of capillaries. Chief cells are positive for neuron-specific enolase, chromogranin B, and synaptophysin. The sustentacular cells, on the other hand, are usually found at the periphery of these nests. Indeed, necrosis, nuclear pleomorphism, mitotic activity, and vascular perineural invasion can also be seen in benign tumors. Thompson, for example, introduced a scoring system for pheochromocytoma that takes into account cellular and nuclear features, growth patterns, and the presence of necrosis. Pathogenesis the oncogenic mechanisms behind paragangliomas have not yet been defined. The observations that such tumors are more common at high altitudes, are implicated in oxygen sensing, are highly vascular, and arise from genetic mutations that stimulate the hypoxic response pathway seem to suggest that they may be linked to a critical component of the oxygen sensing or signaling pathways. In clinically significant cases with biochemical evidence of catecholamine excess, the tumor is described as a functional or catecholamine-secreting paraganglioma. This hypertension can be either paroxysmal or sustained and is triggered by various causes, including anesthesia and several medications. Plasma and urine catecholamine metabolites (metanephrine, normetanephrine, vanillylmandelic acid, and free 3-methoxythyramine, a metabolite of dopamine) and catecholamines will all be altered, but plasma free metanephrine and 24-hour urine fractionated metanephrine (and free 3-methoxytyramine) tests are more sensitive. This dysfunction can manifest as pain, vocal hoarseness, and eventually tongue paresis, dysphonia, and dysphagia. Neoplastic invasion of the external auditory canal can lead to tympanic membrane perforation and, rarely, bleeding from the ear. The paralysis of the vagus nerve leads to vocal cord paralysis with hoarseness, inadequate closure of the glottis with aspiration of fluid, and bilateral paralysis of the soft palate with liquid regurgitation through the nose during swallowing. Intracranial extension occurs in roughly 22% of cases159 and is the main cause of death.
Syndromes
- Restlessness
- Mold
- Notice any problems with the muscles in your face
- Toxic injury of the kidney
- Crunching sensation when touching the skin, if there are rib fractures and puncture of the lung
- Diving injuries
- Before the test starts, you will be given a mild sedative to help you relax.
- High risk of bone loss (osteoporosis)
- Always let your doctor know about any cold, flu, fever, herpes breakout, or other illness you may have before your surgery.
An approach exposing the dural sleeve around the maxillary division can be performed with a frontoorbito-zygomatic craniotomy or simply a temporal craniotomy erectile dysfunction milkshake 20 mg cialis super active buy visa. Zygomatic osteotomies are used to obtain a more inferior view of the angle and decrease the need for brain retraction erectile dysfunction caused by high cholesterol order cialis super active with a visa. Trigeminal schwannomas located solely in the posterior fossa do not pose any special surgical problems and can easily be resected via a conventional paramedian suboccipital approach with the same technique as used for vestibular schwannomas impotence home remedies cialis super active 20 mg order without prescription. Surgically erectile dysfunction protocol download free discount 20 mg cialis super active amex, a subtemporal transtentorial route was advocated by Bordi and colleagues18 and McCormick and associates14; however erectile dysfunction caused by spinal stenosis buy cialis super active now, this approach has important drawbacks, as indicated earlier. Cranio-orbito-zygomatic, petrosal, and combined-petrosal approaches have been reported to result in satisfactory surgical results. Because of the soft consistency of the tumor, total surgical removal of a large, multicompartment tumor may be achieved with a single surgical approach. Posterior fossa component of a trigeminal schwannoma can be resected through the expanded trigeminal pore. Type D tumors may extend into the ortbit, pterygopalatine fossa, and maxilla and to the infratemporal fossa. Extracranial trigeminal schwannomas are usually larger than their intracranial counterparts at the time of diagnosis. Transmaxilllary, transmandibulary, and transcervical alternatives have also been described. Radiosurgery is considered an important adjuvant for residual or recurrent tumors smaller than 3 cm in diameter and in patients with symptoms in whom surgery carries a high risk for mortality and morbidity. The aim of radiosurgery is to achieve control of tumor growth without causing additional cranial nerve deficits. Radiosurgery treatment results in more than 500 patients had been reported as of 2015 (see Table 159-2). Reported tumor control rates ranged from 84% to 100% at 5 years (see Table 159-2). Similarly high tumor control rates were reported for linear acceleratorbased radiosurgery. Wallner and colleagues101 reported the results in eight patients treated with 45 to 54 Gy in 1. After follow-up periods ranging from 2 to 15 years, the tumor control rate was 50%, and the time to tumor recurrence ranged from 1. Zabel and associates102 reported the results in 13 patients who received a mean of 57. In their review of 39 patients reported before 1956, Schisano and Olivecrona15 found a 1-year mortality rate of 41%. The advent of microsurgery significantly decreased the mortality rate, and the same authors reported mortality in 1 (5. Surgical results have improved even more since the popularization of skull base approaches. Very high total resection rates, ranging from 75% to 100%, have been reported in the modern literature. Analysis of seven large studies that included 129 patients indicated that resection rates for Jefferson types A, B, and C trigeminal schwannomas were 88%, 71%, and 81%, respectively. A high incidence of symptomatic tumor recurrence has been reported in some studies, whereas long remission periods have been reported in others. In early literature, recurrence rates as high as 60% were reported, even after total resection. In more recent reports about the use of skull base techniques, the recurrence rate was approximately 10%. Preoperative facial pain and diplopia usually respond well to the surgical intervention. Operative complications include cerebrospinal fluid leakage, infection, aseptic meningitis, hemorrhage in the tumor bed, vasospasm, hydrocephalus, and permanent cranial nerve injury. Surgical approaches are directed to the intracranial compartment harboring the tumor. Radiosurgery can be used as adjuvant therapy in recurrent, residual, or inoperable cases and can produce excellent results. Primary radiosurgery can also be considered for selected small trigeminal schwannomas. Trigeminal schwannomas: removal of dumbbell-shaped tumors through the expanded Meckel cave and outcomes of cranial nerve function. Trigeminal schwannomas: removal of dumbbellshaped tumors through the expanded Meckel cave and outcomes of cranial nerve function. Less common neurinomas: orbital, oculomotor, trigeminal, facial, glossopharyngeal, accessory and hypoglossal. With the report of two cases of extracranial carcinoma infiltrating the ganglion by direct extension through the maxillary division. Tumors of the gasserian ganglion; tumor of the left gasserian ganglion associated with enlargement of the mandibular nerve; a review of the literature and case report. Comparison of conventional and skull base surgical approaches for the excision of trigeminal neurinomas. Long-term outcome of trigeminal neurinomas with modified classification focusing on petrous erosion. Surgical treatment of intracavernous trigeminal schwannomas via a fronto-temporal epidural approach. Surgical treatment of dumbbell-shaped neurinomas: report of an experience with 57 cases in a single hospital. Trigeminal schwannomas: a report of 42 cases and review of the relevant surgical approaches. Nonvestibular schwannomas: an evaluation of functional outcome after radiosurgical and microsurgical management. Trigeminal neurinomas with extracranial extension: analysis of 28 surgically treated cases. Trigeminal schwannomas: skull base approaches and operative results in 105 patients. Operative management of trigeminal neuromas: an analysis of a surgical experience with 55 cases. Primary malignant nerve sheath tumor of the gasserian ganglion: a report of two cases. The trigeminal neurinomas with some remarks on malignant invasion of the gasserian ganglion. Malignant trigeminal schwannoma associated with xeroderma pigmentosum-case report. Recognizing schwannomatosis and distinguishing it from neurofibromatosis type 1 or 2. Microanatomy of the central myelin-peripheral myelin transition zone of the trigeminal nerve. Trigeminal neurinoma presenting with intratumoral hemorrhage: report of two cases. Neurinoma of the trigeminal root and atypical trigeminal neuralgia: their commonality. Surgical management of giant trigeminal schwannomas extending into the parapharyngeal space. Removal of infratemporal fossa schwannoma via a transmandibular transpterygoid approach. Osteoplastic maxillotomy approach for infraorbital nerve schwannoma, a case report. Endoscopic approaches to the trigeminal nerve and clinical consideration for trigeminal schwannomas: a cadaveric study. Surgical management of trigeminal schwannomas: defining the role for endoscopic endonasal approaches. Endoscopic endonasal approaches to infratemporal fossa tumors: a classification system and case series. Stereotactic radiosurgery for trigeminal schwannoma: a clinical retrospective study in 52 cases. Clinical experience with Leksell Gamma Knife in the treatment of trigeminal schwannomas. Gamma Knife surgery and trigeminal schwannoma: is it possible to preserve cranial nerve function Stereotactic radiosurgery for trigeminal schwannoma: tumor control and functional preservation. Gamma Knife surgery for nonvestibular schwannomas: radiological and clinical outcomes. Evaluation of tumor expansion after stereotactic radiosurgery in patients harboring vestibular schwannomas. Management of benign cranial nonacoustic schwannomas by fractionated stereotactic radiotherapy. The most common presenting symptoms are nasal obstruction and epistaxis; however, additional symptoms relating to compression or destruction of skull base structures have been reported (Table 160-1). These vascular channels lack the surrounding smooth muscle and innervation of normal blood vessels and therefore tend to bleed profusely when manipulated. As the artery regresses throughout development, it forms a vascular plexus with remnants at the superior margin of the sphenopalatine foramen. Because this site is the most commonly proposed origin for these tumors and they are associated with development, these plexus remnants may influence the vascularity of the tumor. Accelerated tumor growth was described with testosterone treatment, leading to studies of neoadjuvant flutamide (antiandrogen) treatment. Osteology of the infratemporal fossa and lateral aspect of pterygomaxillary fissure and pterygoid plates with the zygomatic arch removed. Studies using the direction of bony displacement to describe different patterns of growth generally trace the locus of origin to the sphenopalatine foramen, where the posterior part of the middle turbinate attaches. Furthermore the orbit provides an additional route to intracranial extension through the superior orbital fissure. Unilateral nasal obstruction and epistaxis are common early symptoms but often do not prompt diagnosis. Anterior growth invades the posterior aspect of the maxillary sinus and, more superiorly, the ethmoid air cells. With lateral growth the pterygoid plates are eroded, and the tumor extends into the pterygomaxillary fissure. From here it invades the infratemporal fossa and gains access to the inferior orbital fissure, with erosion of the greater wing of sphenoid. The orbit is frequently involved through the inferior orbital fissure as well as through the lamina papyracea from the ethmoid tumor component. When the orbit is involved additional symptoms of diplopia, visual loss, and proptosis may develop. A, Photomicrograph (×50) showing the typical, variably thin-walled blood vessels with variable shapes within a background of fibrocollagenous connective tissue stroma. This is from a deeper region of the lesion, which frequently shows greater stromal cell density than do more superficial regions of nasal angiofibromas. In addition, blood and vessels are more obvious in this particular area because the vessels are congested in this focus. B, Photomicrograph (×200) showing a prominent (at high power) feature typical of nearly all nasal angiofibromas: a generally sparse but rather diffuse inflammatory cell infiltrate composed most prominently (or nearly entirely) of scattered mast cells. Mast cells have a so-called fried-egg appearance, with central round to ovoid nuclei and abundant finely granular basophilic cytoplasm. Axial noncontrast computed tomography scan demonstrating orbital involvement through direct extension with proptosis of the globe. Coronal noncontrast computed tomography scan demonstrating extensive skull base erosion with both intracranial extension and lateral extension to the infratemporal fossa. Coronal T2-weighted magnetic resonance image demonstrating direct extension of the juvenile nasal angiofibroma into the middle cranial fossa, the parasellar region involving the internal carotid artery. Coronal contrast-enhanced T1-weighted magnetic resonance image demonstrating extension of a juvenile nasal angiofibroma into the planum sphenoidale. In published data from India, the rate of intracranial involvement is as high as 90%. First, the tumor may cause direct erosion of the foramen rotundum, ovale, and lacerum. Second, from the infratemporal fossa, tumor can invade directly into the middle cranial fossa. Finally, a particularly vexing intracranial extension occurs through the roof of the sphenoid sinus into the sella and medial to the cavernous sinus. Parasagittal contrast-enhanced T1-weighted magnetic resonance image of juvenile nasal angiofibroma with extension into the orbit and middle cranial fossa. Angiography of internal carotid artery demonstrating tumor blush (arrow) and blood supply from the internal carotid artery branches. Angiograph of extensive juvenile nasal angiofibroma with intracranial component obtained after ophthalmic artery superselective embolization, demonstrating postembolization tumor blush (arrow). Biopsy can be dangerous owing to the vascularity of the tumor and is often not necessary because radiographic studies are fairly specific. Tumors tend to appear isointense to hyperintense on T1- and T2-weighted images and to exhibit avid contrast enhancement. Residual tumor blush after angiographic embolization indicates incomplete vessel occlusion or contralateral vascular supply and may necessitate further angiographic procedures for control. Although embolization is associated with a low rate of complications, anastomoses between the internal maxillary artery and ophthalmic artery can result in loss of vision. However, no randomized controlled trials have been performed to compare surgery with other treatments.
Discount cialis super active online mastercard. up b.ed previous year question paper in hindi 2019/entrance exam solved paper 2 math+sci+reasoning.
References
- Bhambhani A, Somnath HS. Percutaneous treatment of Lutembacher syndrome in a case with difficult mitral value crossing. J Invasive cardiol. 2012;24:E54-6.
- Critchley J, Capewell S. Smoking cessation for the secondary prevention of coronary heart disease. Cochrane Database Syst Rev. 2004(1):CD003041.
- Sakimoto K. The cause of the eosinophilia-myalgia syndrome associated with tryptophan use. N Engl J Med. 1990;323:992.
- Chung JH, Park MS, Shin DH, et al. Pulmonary involvement in Erdheim- Chester disease. Respirology 2005;10:389-92.