
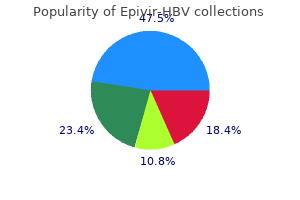
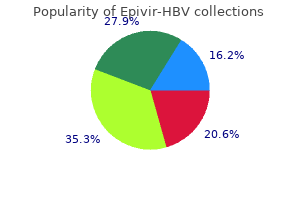
Epivir-HBV
| Contato
Página Inicial
Nicholas P. Chandler BDS, MSc., PhD, LDS RCS (Eng), FDS RCPS (Glas) FDS RCS (Edin), FFD RCSI
- Associate Professor of Endodontics,
- School of Dentistry, University of Otago, Dunedin,
- New Zealand
She has been on prednisone (60 mg/d initially medications that cause hair loss epivir-hbv 100 mg line, now 40 mg/d) since the onset of her illness medicine 666 colds order epivir-hbv without prescription. On examination medicine disposal order epivir-hbv with mastercard, she is overweight treatment zoster ophthalmicus buy epivir-hbv now, with a buffalo hump and striae over her abdomen 88 treatment essence purchase epivir-hbv 150 mg otc. Motor examination reveals a power of 3/5 at the proximal muscles (shoulder and hip) and 5/5 distally. Objective: Recognize enteropathic arthritis associated with inflammatory bowel disease. Chest x-ray shows bilateral hilar lymphadenopathy and an infiltrate in the right lower lobe. The peripheral joint symptoms often parallel the bowel disease activity; surgical colectomy may result in permanent remission of the joint disease. The other skeletal involvement affecting the spine (axial arthropathy) occurs in about 10% of the patients, is more common in men, and runs a course independent of the bowel disease. On questioning, he gives a history of a self-limiting, nonbloody diarrhea 3 weeks ago. Two weeks ago, his right eye was painful and red; it spontaneously resolved in 3 to 4 days. Sarcoidosis is an inflammatory disorder of unknown etiology characterized by granulomatous involvement of various tissues. Rheumatologic involvement may occur as arthritis (15%), uveitis (20%), or myositis (4%). The prevalence in African Americans is much higher than in Caucasian Americans (8:1). Glucocorticoids are used for severe lung disease, uveitis, hypercalcemia, cardiac involvement, neurosarcoidosis, or other severe organ involvement. Question 38 A 75-year-old Caucasian woman presents for neck and shoulder pain that started about 2 months ago. She has associated stiffness that is worst in the morning and lasts about 2 hours. Reactive arthritis typically follows a gastrointestinal or genitourinary infection. ReA clinically manifests as an asymmetric, additive, oligoarticular arthritis, more commonly involving the lower extremities. She denies any headache, scalp tenderness, jaw claudication, or visual disturbances. Physical examination is unrevealing except for pain when she actively moves her shoulders. Rheumatology 193 tendon friction rubs, sclerodactyly, and difficulty forming a grip. Abnormal laboratory tests include proteinuria, microscopic hematuria, and elevated creatinine level. In severe cases, patients may develop thrombocytopenia and anemia secondary to a microangiopathic process. The use of angiotensin-converting enzyme inhibitors has improved the outcome of renal crisis, and 1-year survival has increased from 15% to 76%. It is believed that blockade of angiotensin is the most effective way to manage this complication. Question 40 An 89-year-old white woman is having pain and stiffness in the neck and shoulders, with fatigue for 2 months. She denies any night sweats, significant weight loss, loss of appetite, and headaches. Her blood work shows erythrocyte sedimentation rate of 83 mm/hour, C-reactive protein of 9. It is often accompanied by systemic symptoms of malaise, weight loss, and low-grade fever. He has a history of hypertension, and his blood pressure on hydrochlorothiazide 12. He has thickened skin diffusely, telangiectasias on the face, (c) 2015 Wolters Kluwer. It is marked by swelling and tenderness at the knee and is common among individuals whose professions require frequent kneeling. Question 42 A 40-year-old male sales executive gets admitted with hemoptysis and acute renal failure. He has bilateral rales on lung auscultation, but the cardiovascular examination is normal. Based on his disease and immunosuppressive therapy, what prophylactic regimen is most appropriate It is a symptom complex characterized by pain and stiffness of at least 4 weeks duration, in the muscles of the neck, shoulder, and pelvic girdle. The myalgias are sometimes combined with symptoms of systemic inflammation, like malaise, weight loss, and night sweats. Laboratory abnormalities include an elevated sedimentation rate, elevated C-reactive protein, and anemia. Most patients show a dramatic improvement in their symptoms when treated with prednisone 20 mg/d or even a lower dose. Occasionally, patients may need higher doses of prednisone, but this should prompt vigilance for an alternative disease. Dose adjustment should be based mainly on clinical symptoms and not exclusively on laboratory abnormalities. Question 41 A 20-year-old female college student who jogs regularly comes to your office with complaints of pain in both knees. She has stiffness lasting 5 to 10 minutes after prolonged sitting, which improves with activity. However, overactivity, like climbing or going down the stairs, aggravates the pain. On examination, she has small effusions in both knees and pain with patellar movements. Objective: Identify the appropriate prophylactic regimen in a patient receiving high-dose steroids and cytotoxic agents. It enhances the apoptosis of osteoblasts and increases the survival of osteoclasts. However, bisphosphonate therapy is not recommended for use in patients with Clcr < 35 mL/min. This patient has patellofemoral pain syndrome (chondromalacia patellae), which occurs in young age groups and often involves both knees. Patients have pain and crepitus in the patellar region that is aggravated by overactivity involving knee flexion, particularly climbing or going down the stairs. On examination, the patient experiences pain when the patella is displaced laterally or compressed against femoral condyles. In athletes, patellar tendinitis is a relatively common cause of pain in the inferior patellar region, common with frequent jumping. Osgood-Schlatter disease, or epiphysitis of the tibular tubercle, is an irritation of the patellar ligament at the tibial tuberosity site, characterized by painful lumps just below the (c) 2015 Wolters Kluwer. ReView QueStionS Since this patient has an elevated creatinine, only calcium and vitamin D should be used for osteoporosis prevention. The cough started about a month ago and has progressively worsened, and 2 days ago, she noticed the fever. She has also been having blood-stained nasal discharge for the last 2 weeks and is taking amoxicillin. She does not have any skin rash, joint pain, shortness of breath, hemoptysis, hoarseness, numbness, or tingling. On physical examination, she has a cushingoid facies with saddle-nose deformity, temperature of 101. The determination of relapse should be based on objective evidence of disease activity, but infections complications can mimic a disease flare. Question 44 A 44-year-old man with a past history of previously documented gout in his knee is admitted with pain and swelling in the left elbow for about 10 days. One month previously, he had been hospitalized for urinary obstruction due to an enlarged prostate with a urinary tract infection. Joint examination reveals a hot and swollen left elbow with limited range of motion. He also has multiple nontender nodules on his metacarpophalangeal and proximal interphalangeal joints, as shown in the figure. Objective: Recognize the etiology of cavitary lung lesions in granulomatosis with polyangiitis. The cavitary lesion His laboratory tests show a white blood cell count of 12,200/L, sedimentation rate of 124 mm/hour, and C-reactive protein of 17. She denies any hair loss, oral ulcers, dry eyes, or mouth, rash, fever, or discoloration of hands when exposed to cold. On physical examination, she has swelling with tenderness in the metacarpophalangeal, proximal phalangeal, and metatarsophalangeal joints. This patient has tophaceous gout and is currently having an acute inflammatory monoarthritis in the left elbow. Presence of monosodium crystals in the joint fluid does not rule out gout with a coexistent infection. Erythrocyte sedimentation rate and C-reactive protein, which are markers of inflammation, can be elevated both in gout and in infection. The prolonged symptoms and history of recent infection warrant treatment for a possible infection until the culture results return. Hence, the patient should be started on intravenous antibiotics while awaiting the culture results. Question 45 A 24-year-old woman presents with fatigue, joint and muscle pain, and low-grade fever for the last 6 weeks. She has been taking minocycline for about 6 months for severe facial and truncal acne. On physical examination, she has a temperature of 100°F, pulse of 80 beats/minute, and no joint swelling. Objective: Understand the use of serologic markers in the diagnosis of rheumatoid arthritis. It can be elevated in 1% to 2% of healthy individuals, other autoimmune diseases, and chronic infections like tuberculosis, hepatitis C, syphilis, and bacterial endocarditis. Question 47 A 55-year-old woman presents with diffuse muscle pain and fatigue for over a year. On physical examination, she is anxious and has diffuse muscle tenderness and tender points. Question 46 A 40-year-old woman presents with pain and swelling in the hands, shoulders, and feet for the last 2 months. She also has morning stiffness that lasts for about an hour and malaise (c) 2015 Wolters Kluwer. Diffuse pain present for years and accompanied by subjective complaints like fatigue, memory difficulties, irritable bowel symptoms, and sleep disturbance is likely to be secondary to fibromyalgia. This patient has diffuse pain with fatigue, a sleep disturbance, and physical examination findings of diffuse tender points with hyperreflexia, which are compatible with the diagnosis of fibromyalgia. In patients presenting with diffuse pain, one should focus on the onset and character of the pain and any precipitating events that could have caused the pain. On physical examination, identification of signs of inflammation, like swollen joints or objective muscle weakness, will be against the diagnosis of fibromyalgia. Patients who have diffuse pain should have a complete blood count and tests of liver, kidney, thyroid, hepatitis C infection, muscle enzymes, and sedimentation rate with C-reactive protein performed during the course of the illness. Patients with fibromyalgia have symptoms with normal inflammatory indices, and the symptoms are often minimally responsive to anti-inflammatory regimens. Question 48 A 49-year-old woman is admitted with a purpuric rash on the legs, pain in the joints, excruciating pain and tingling in her feet, difficulty walking, weight loss, and discoloration of her hands on exposure to cold. On physical examination, she has a palpable purpuric rash on her legs and weak dorsiflexion of the right foot. The history of likely blood transfusions in the past with currently elevated liver enzymes and positive risk factors raises the possibility of a chronic hepatitis C infection in this patient. Chronic hepatitis C infection is associated with mixed cryoglobulinemia and sometimes results in cryoglobulinemic vasculitis. Ninety percent of patients with vasculitis secondary to mixed cryoglobulinemia are hypocomplementemic, with C4 levels characteristically more depressed than C3 levels. Mixed cryoglobulinemia is characterized by the presence of monoclonal and polyclonal IgG and IgM antibodies, which often include antibodies with rheumatoid factor activity. At minimum, re-imaging (twice weekly compression ultrasonography for 2 weeks) is advised. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Hypercoagulable state testing and malignancy screening following venous thromboembolic events. Prevention of venous thromboembolism in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Antithrombotic therapy for venous thromboembolic disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecularweight heparin for acute treatment of venous thromboembolism. Comparison of lowintensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. Systematic lung scans reveal a high frequency of silent pulmonary embolism in patients with proximal deep venous thrombosis. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians.
Early and late survival after surgical treatment of culture-positive active endocarditis symptoms 0f gallbladder problems safe 150 mg epivir-hbv. Clinical presentation medicine naproxen cheap epivir-hbv, etiology symptoms 16 dpo discount epivir-hbv 150 mg, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study medications vascular dementia order epivir-hbv 100 mg amex. An evaluation of the Duke criteria in 25 pathologically confirmed cases of prosthetic valve endocarditis treatment centers in mn order epivir-hbv visa. Infective endocarditis in chronic haemodialysis patients: an increasing clinical challenge. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved Infective endocarditis in injection drug users: importance of human immunodeficiency virus serostatus and degree of immunosuppression. Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow-up. Native valve infective endocarditis in elderly and younger adult patients: comparison of clinical features and outcomes with use of the Duke criteria and the Duke Endocarditis Database. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. Echocardiography in patients with suspected endocarditis: a cost-effective analysis. Transesophageal echocardiographic recognition of subaortic complications in aortic valve endocarditis: clinical and surgical implications. Combination antimicrobial therapy for Staphylococcus aureus endocarditis in patients addicted to parenteral drugs and in nonaddicts: a prospective study. Comparison of different antibiotic regimens for therapy of 32 cases of Q fever endocarditis. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Identification of abscess formation in native-valve infective endocarditis using transesophageal echocardiography: implications for surgical treatment. An assessment of the usefulness of the Duke criteria for diagnosing active infective endocarditis. Current best practices and guidelines for isolation of bacteria and fungi in infective endocarditis. Induction of experimental endocarditis by continuous low-grade bacteremia mimicking spontaneous bacteremia in humans. International Collaboration on Endocarditis-Prospective Cohort Study Investigators. Infective endocarditis in the elderly in the era of transesophageal echocardiography: clinical features and prognosis compared with younger patients. Clinical Presentation Acute presentation and localized findings-consider typical pathogens such as Streptococcus pneumoniae, Haemophilus influenzae, and the enteric gram-negative organisms. When recovered secretions contain 103 colonyforming units (cfu)/mL of a bacterial pathogen, lower respiratory infection should be suspected. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Duration and route of antibiotic therapy in community-acquired pneumonia: switch and step-down therapy. A prediction rule to identify low-risk patients with community-acquired pneumonia. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Mycoplasma pneumoniae pneumonia requiring hospitalization, with emphasis on infection in the elderly. Severe methicillin-resistant Staphylococcus aureus community-acquired pneumonia associated with influenza-Louisiana and Georgia, December 2006 January 2007. Incidence, etiology, and outcome of nosocomial pneumonia in mechanically ventilated patients. Serologic Testing Serologic testing for Legionella species, Mycoplasma species, and C. A fourfold increase in the immunoglobulin G (IgG) titer is suggestive of a recent infection with one of these organisms. Pharmacologic Treatment Intravenous antibiotics may be switched to oral ones when the patient is stable and afebrile. Upper Respiratory Tract Infections Symptoms such as production of yellow sputum, sore throat, fever, and colored nasal discharge have poor predictive evidence for the efficacy of the prescribed antibiotics. Tetracyclines, sulfonamides, and fluoroquinolones, particularly ciprofloxacin, are not recommended. Clinical scenarios suggestive of acute bacterial sinusitis include persistence of symptoms without improvement for 10 days, severe symptoms (such as fever 102°F) lasting 3 to 4 days, or initial improvement followed by a later worsening of symptoms. For patients with features suggestive of acute bacterial rhinosinusitis, amoxicillin clavulanic acid for 5 to 7 days is the first-line agent, with doxycycline as an alternative choice. Respiratory fluoroquinolones or a combination of an oral third-generation cephalosporin are second-line agents. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. Comparison of outpatient systemic antibacterial use in 2004 in the United States and 27 European countries. Diagnosis and management of food borne illness: a primer for physicians and other health care professionals. The practice of travel medicine: guidelines by the Infectious Diseases Society of America. Risk of clostridium difficile infection with acid suppressing drugs and antibiotics: meta-analysis. Nonpasteurized dairy products, disease outbreaks, and state laws-United States, 19932006. Can procalcitonin help identify associated bacterial infection in patients with severe influenza pneumonia Sputum colour reported by patients is not a reliable marker of the presence of bacteria in acute exacerbations of chronic obstructive pulmonary disease. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study. Oseltamivir-zanamivir bitherapy compared to oseltamivir monotherapy in the treatment of pandemic 2009 influenza A(H1N1) influenza virus infections. National trends in visit rates and antibiotic prescribing for adults with acute sinusitis. Improved diagnostic accuracy of group A streptococcal pharyngitis with use of real-time Biosurveillance. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Safety and tolerability of commonly prescribed oral antibiotics for the treatment of respiratory tract infections. Intranasal corticosteroids in management of acute sinusitis: a systematic review and meta-analysis. Oseltamivir and risk of lower respiratory tract complications in patients with Flu symptoms: a metaanalysis of eleven randomized clinical trials. Cranberries vs antibiotics to prevent urinary tract infections: a randomized double-blind noninferiority trial in premenopausal women. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Systematic review: antimicrobial urinary catheters to prevent catheter-associated urinary tract infection in hospitalized patients. Three-day vs longer duration of antibiotic treatment for cystitis in women: systematic review and meta-analysis. Appropriate antibiotic treatment of genitourinary infections in hospitalized patients. Validation of a decision aid to assist physicians in reducing unnecessary antibiotic drug use for acute cystitis. Effects of vaccine program against pandemic influenza A(H1N1)pdm09, United States, 20092010. Procalcitonin guidance and reduction of antibiotic use in acute respiratory tract infection. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries. A 51-year-old woman with acute onset of facial pressure, rhinorrhea, and tooth pain: review of acute Rhinosinusitis. Validation of self-swab for virologic confirmation of influenza virus infections in a community setting. Antibiotics for treatment of acute respiratory tract infections: decreasing benefit, increasing risk, and the irrelevance of antimicrobial resistance. Repetition of the rapid antigen test in initially negative supposed streptococcal pharyngitis is not necessary in adults. Impact on antibiotic prescription of rapid antigen detection testing in acute pharyngitis in adults: a randomised clinical trial. Treatment with neuraminidase inhibitors for critically ill patients with influenza A (H1N1) pdm09. Rhinosinusitis diagnosis and management for the clinician: a synopsis of recent consensus guidelines. Institutional requirements for influenza vaccination of healthcare personnel: results from a Nationally Representative Survey of Acute Care Hospitals-United States, 2011. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 Update by the Infectious Diseases Society of America. Principles of appropriate antibiotic use for treatment of acute bronchitis in adults. Effectiveness of seasonal vaccine in preventing confirmed influenza-associated hospitalizations in community dwelling older adults. Minimal use of antibiotics for acute respiratory tract infections: validity and patient satisfaction. Infrequent diagnosis of primary human immunodeficiency virus infection: missed opportunities in acute care settings. Hospitalizations associated with influenza and respiratory syncytial virus in the United States, 19932008. The human bite injury: a clinical audit and discussion regarding the management of this alcohol fuelled phenomenon. National trends in ambulatory visits and antibiotic prescribing for skin and softtissue infections. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. The five options listed are part of the differential diagnosis for the syndrome of genital ulcers with regional adenopathy. From an epidemiologic standpoint, it is less common than primary syphilis and should be considered after consideration of primary syphilis. Granuloma inguinale is secondary to Klebsiella granulomatis infection and typically presents with a non-painful ulcer. These patients typically do not have lymphadenopathy, but may have painful "buboe. He has never had a sexually transmitted disease before, and he has a new female partner. The patient should receive some form of treatment because therapy partially relieves symptoms and accelerates healing. They include famciclovir, 250 mg orally three times daily or valacyclovir, 1 g orally twice daily for 7 days. Question 2 A 26-year-old man has a penile lesion for several weeks and new swelling in the groins. On examination, a single nontender penile ulcer and bilateral palpable nontender inguinal lymph nodes are present. The most likely diagnosis is: a) Lymphogranuloma venereum b) Chancroid c) Primary syphilis d) Variant herpes simplex virus infection e) Granuloma inguinale Answer and Discussion the answer is b. Chancroid typically presents as a painful genital ulcer and tender regional lymphadenopathy. Review Questions gray or yellow purulent exudate may be present over the ulcer, with a tendency to bleed when scraped. The inguinal lymphadenitis can sometimes liquefy and present as painful, fluctuant "buboes" that leak frank pus (as was seen in this patient). Azithromycin is another option, but a single dose is sufficient, rather than a 7-day course of therapy. Finally, erythromycin can be used at a dose of 500 mg orally four times daily for 7 days. Question 4 A 27-year-old woman comes to the office because her boyfriend was recently diagnosed with genital herpes. This is evidenced by the fact that the patient has persistently positive nontreponemal tests, representing a previously infected patient without evidence of active disease. In penicillin-allergic patients, doxycycline or tetracycline should be given for 4 weeks. A positive herpes simplex virus type 2 antibody test is indicative of an infection with anogenital herpes at some time in the past. The antibody test may be useful in the partner evaluation, although pretest counseling is important.
Patients who continue to have exacerbations despite being on optimal long-acting inhaled bronchodilators may require inhaled corticosteroids treatment type 2 diabetes epivir-hbv 150 mg purchase overnight delivery. If patients have cor pulmonale symptoms 3 days after conception purchase epivir-hbv 150 mg online, right heart failure treatment integrity checklist purchase epivir-hbv 100 mg without prescription, or hematocrit >55% symptoms zoloft buy epivir-hbv australia, oxygen is also warranted medications without doctors prescription epivir-hbv 100 mg buy lowest price. Long-term oxygen therapy improves quality of life and increases survival in these patients. Question 28 A 50-year-old cirrhotic male patient with a past medical history of smoking, substance abuse, and alcohol abuse presents with acute hemoptysis, wheezing, and fever. His examination shows a cachectic individual with diffuse wheezing and thermal burns on his fingers and thumbs. Additional complications include deep vein thromboses, gastrointestinal bleeding, malnutrition, and side effects from sedatives and paralytics. Barotrauma occurs in a minority of ventilated patients (13% in one study), with barotrauma rarely directly causing death. Barotrauma is evidenced by the development of pneumothorax, subcutaneous emphysema, pneumomediastinum, and interstitial emphysema. Increased radiolucency at the lung bases and the presence of the deep sulcus sign on a chest radiograph are clues to barotrauma and pneumothorax. The combination of a corticosteroid and a neuromuscular blocking agent has been associated with a reversible myopathy that takes several months to resolve. Severe sepsis is the presence of sepsis associated with organ dysfunction, hypotension, or hypoperfusion. Septic shock is sepsis with hypotension despite adequate fluid resuscitation and the presence of lactic acidosis, oliguria, or acute mental status changes. On examination, respiratory rate is 24 breaths/ minute, and she appears in mild distress, with difficulty breathing. Percussion is stony-dull in the right base and halfway up the right lung field, with diminished tactile fremitus, vocal resonance, and breath sounds in the same areas. Crack lung may occur within 48 hours of smoking of cocaine, which presents as diffuse alveolar infiltrates, eosinophilia, and fever. Patients may present with pleuritic chest pain, dyspnea with even mild exertion, dry or productive cough, wheezing, and hemoptysis. Melanoptysis or expectoration of black sputum is seen from inhalation of black carbonaceous residue from inflammable substances that are typically used to set fire to crack. Objective: Understand the spectrum of the sepsis syndrome and its associated definitions. The American College of Chest Physicians and the Society of Critical Care Medicine have defined this series of terms. Infection is a microbial phenomenon characterized by an inflammatory response to the presence of organisms or to invasion of normally sterile host tissue by these organisms. Objective: Understand the diagnostic criteria of pleural effusions and their management. In a patient with a parapneumonic effusion, any of the following is an indication for thoracostomy tube placement: a) Pleural fluid glucose level <50 mg/dL b) Presence of gross pus in the pleural space c) Organisms visible on Gram stain of the pleural fluid d) Pleural fluid pH <7. Review QueStionS Pulmonary and Critical Care Medicine Question 31 A 56-year-old man asks for advice concerning a nodule seen on a chest radiograph obtained during a physical examination for a new job. All the choices are appropriate in the initial management of pulseless electrical activity, except synchronized direct-current cardioversion. In addition to pneumothorax, hypoxia, and hypotension, other causes of pulseless electrical activity that must be investigated in the initial management of these patients include cardiac tamponade, hypothermia, massive pulmonary embolism, drug overdose, hyperkalemia, severe acidosis, and massive myocardial infarction. He is known to have a mild baseline dementia but still lives alone and has been able to carry out the basic activities of daily living. He has been unable to tolerate anything to eat or drink for the past 2 days and has been incontinent of very loose feces, with nausea, vomiting, and a low-grade fever. On examination, he appears frail and is oriented to person but not to place or time. The definition of a solitary pulmonary nodule is a single radiologically visible lesion that is within and surrounded on all sides by pulmonary parenchyma. It is not associated with potentially related pathology, such as pleural effusion or mediastinal lymphadenopathy. The upper limit of the size of a nodule may be 3 or 4 cm; larger lesions are considered masses. Adenocarcinoma most commonly presents as a solitary pulmonary nodule; small cell carcinoma usually presents as a central endobronchial lesion. Question 32 A 76-year-old man admitted to a general medicine ward for pneumonia is found by a nurse to be unresponsive and without a palpable pulse or spontaneous breathing. As the first physician to the scene, you confirm the absence of pulse and respiration. You then ask the respiratory therapist to establish an airway and begin mask-bag ventilation. A subclavian central access line had already been placed 2 hours before the arrest. The initial rhythm seen is pulseless electrical activity at 70 complexes per minute. This man is hypovolemic from gastrointestinal fluid loss, as evidenced by orthostatic hemodynamic parameters. The serum sodium is likely to be raised and the urinary sodium low (<25 mEq daily) because the kidneys are attempting to retain sodium to compensate for the lost volume. In the same way, potassium is lost in vomiting and diarrhea, and the kidney attempts to compensate for this with a reduced urinary loss of potassium. Vasopressin may be used in the syndrome of central diabetes insipidus, which may also cause elevated (c) 2015 Wolters Kluwer. In the past year, she has had several episodes of fever, malaise, and increased sputum production; twice, she had chest radiographs that showed infiltrates consistent with pneumonia. Chest radiography shows a parenchymal infiltrate in the left upper lobe and some atelectasis in the right base. Immediate skin test reactivity is positive for Aspergillus antigens, and she has serum antibodies to Aspergillus fumigatus. However, the urine osmolality would be inappropriately low and the urine sodium would not be <25 mEq/day. Question 34 A 65-year-old man is evaluated in your office for increasing shortness of breath. He denies fever, cough, chest pain or pressure, palpitations, orthopnea, or paroxysmal nocturnal dyspnea. All the following statements concerning asbestos-induced lung disease are true, except a) Most patients are asymptomatic for at least 20 to 30 years. Colonization with aspergilli occurs, rather than infection, and an antimicrobial is not indicated. Repeated episodes of bronchial obstruction, inflammation, and mucoid impaction can lead to bronchiectasis, fibrosis, and respiratory compromise. Septated hyphae with acute dichotomous branching may be seen in the mucus-filled bronchial lumen, but fungi do not invade the mucosa. Wheezing is not always evident, and some patients present with asymptomatic pulmonary consolidation. Question 36 A 39-year-old man presents with a nonproductive cough for 6 to 8 months. He states that the cough is very irritating because he frequently has to speak in public. Six months ago, he saw your colleague who he reports told him that it was a "postviral cough" and gave him an albuterol inhaler, which he used twice a day for 4 months. Further history reveals nasal discharge, frequent throat clearing, and no wheezing or shortness of breath. Cough, sputum production, and wheezing are unusual presenting symptoms and, if present, tend to be due to cigarette smoke rather than asbestos exposure. It is true that antinuclear antibody and rheumatoid factor may be present, as may a raised erythrocyte sedimentation rate, but these are not clinically useful, being nonspecific and not related to disease severity. Because the use of asbestos has been ubiquitous, exposure can occur in a variety of occupational and non-occupational settings. As examples, exposure to asbestos results from involvement with mining and milling of the fibers and industrial applications of asbestos. Asbestos-induced diseases are probably caused by the direct toxic effects of the fibers on pulmonary parenchymal cells as well as the release of various inflammatory mediators. Although some investigators have questioned the causal relationship between asbestosis and bronchogenic carcinoma, most studies have demonstrated a clear association between the two entities. The risk of lung cancer associated with exposure to both asbestos and cigarette smoke appears to be multiplicative. A 1979 report in the Annals of the New York Academy of Science showed that asbestos is associated with a sixfold increase, cigarette smoking with an 11-fold increase, and both cigarette smoke and asbestos exposure with a 59-fold increase in the risk of lung cancer. Review QueStionS Pulmonary and Critical Care Medicine morning but does not wake him from sleep; it is not associated with exercise. On examination, he appears generally well; his respiratory rate is 12 breaths/minute, and his pulse is 72 beats/minute. Nasopharyngeal mucosa has a cobblestone appearance, and the presence of secretions is noted. Postnasal drip, asthma, and gastroesophageal reflux represent approximately 90% of the causes found for chronic cough (and an even higher percentage in nonsmokers with a normal chest radiograph). This man has a history of nasal discharge and frequent throat clearing, and examination revealed nasopharyngeal mucosa with a cobblestone appearance and the presence of secretions, all of which suggest postnasal drip. No clues are suggestive of gastroesophageal reflux, but if there were such clues, a trial of an H2 blocker would have been a possible option. Postviral cough can persist for up to 8 weeks after the acute syndrome but should resolve after 6 months in this case. The diagnosis of asthma is not suggested as the most likely diagnosis here because no nighttime or exercise-related symptoms are present, and 4 months of twice daily albuterol with a good technique had no effect on the symptoms. Therefore, persisting with albuterol and adding an inhaled steroid are not indicated, and at this point, spirometry would not be the best choice. She reluctantly confesses to smoking two packs of cigarettes per day, although she had told her primary care doctor that she had stopped smoking. On physical examination, she is breathing uncomfortably and rapidly at a rate of 28 breaths/minute; pulse is regular at 110 beats/minute. The trachea is central, percussion is resonant, and breath sounds are normal in all areas. The chest pain is not reproduced on palpation, although it occurs on deep inspiration. All the following statements concerning the diagnosis of pulmonary embolus are true, except a) In this case, a high-probability perfusion scan would indicate a high likelihood of pulmonary embolus. Objective: Recognize the utility and limitations of diagnostic tests for pulmonary embolism. An elevated d-dimer level (>500 ng/mL) is present in the majority of patients with pulmonary embolus, but raised levels are also found in malignancy and postsurgery. A d-dimer value <200 ng/mL contributes to excluding the diagnosis of pulmonary embolus, with a negative predictive value of 97% when combined with a nondiagnostic lung scan. However, a low probability perfusion scan would not exclude pulmonary embolism in this highrisk individual. In addition, it causes a decrease in N-acetylaspartate in the frontal lobes and basal ganglia that may explain the chronic central nervous system side effects, such as lasting psychosis after its use is stopped and choreoathetoid movements. Nicotine does cause mild stimulant effects through its hepatic glucose release and epinephrine release, however, is unlikely to cause hyperadrenergic states to the degree demonstrated in this vignette. Opiates cause generalized analgesia, sedation, euphoria, and respiratory depression. These classes of psychoactive drugs have in common that they can cause subjective changes in perception, thought, emotion, and consciousness. Unlike other psychoactive drugs, such as stimulants and opioids, these drugs do not merely amplify familiar states of mind, but rather induce experiences that are qualitatively different from those of ordinary consciousness. Two of his friends have developed lung disease from dusts they inhaled in their workplace. He wonders if his lungs are alright since he had worked in several dusty places, including the shipyards for 20 years followed by foundry work for another 20 years. Physical examination is normal except for decreased breath sounds on lung auscultation. Chest radiography reveals mild hilar adenopathy with eggshell calcification and multiple small upper lobe nodules. Although higher levels increase the risk of oxygen toxicity, they do not increase tissue oxygenation. Relative, regional intrapulmonary hypoxia due to damaged alveolar gas exchange causes compensatory pulmonary vasculature vasoconstriction to minimize perfused dead space. Increasing oxygen tension with increased inspired oxygen fraction will relieve this compensation and cause increased dead space, potentiating hypercapnia. He states that he has no complaints, is not tired, and is "getting ready to party for 8 more hours. Objective: Recognize the increased risk for pulmonary infections in chronic silicosis. Exposure to crystalline silica occurs when silica-containing rock and sand are encountered. This most commonly occurs in occupations associated with construction, mining, quarrying, drilling, and foundry work.
Syndromes
- Various deodorants
- Destroying the trigeminal nerve with a needle or probe placed through the skin using radiofrequency ablation or an injection of glycerol
- The test may also be done with you lying back. With this method, a fluid-filled cup is placed against your eye to do the test.
- Head CT
- Name of the product (ingredients and strengths, if known)
- Alcoholism - resources
- Nausea
- The bacteria spores must germinate or sprout (the same way a seed might sprout before a plant grows) before the actual disease occurs. The process usually takes 1 to 6 days.
- Vaccination
Objective: Identify common features of Nocardia infection in immunosuppressed patients keratin intensive treatment best purchase epivir-hbv. Microscopically Nocardia is seen as a partially acid-fast medicine 8 discogs cost of epivir-hbv, filamentous medicine while breastfeeding epivir-hbv 150 mg order otc, branching medications jejunostomy tube discount epivir-hbv on line, gram-positive rod aquapel glass treatment epivir-hbv 150 mg amex. Nocardiosis is an opportunistic infection but can also occur in immunocompetent patients. It should be suspected in any patient who presents with brain, soft tissue, or cutaneous lesions, and a concurrent or recent pulmonary process. Mycobacterium tuberculosis and Mycobacterium avium complex are acid fast but will not appear filamentous or branching. Question 45 A 32-year-old man is seen at the clinic with a 1 week history of swelling, erythema, pain, and tenderness in his right upper arm. He stayed mainly in the city area but did buy food occasionally from street vendors. There is no need to order stool studies, unless the diarrhea is prolonged (>10 to 14 days) or accompanied by fever and colitis or the traveler is immunosuppressed. Travelers should be given a prescription for antibiotics for empiric self-treatment if diarrhea develops abroad. Ciprofloxacin, levofloxacin, ofloxacin, norfloxacin, and azithromycin are some of the oral agents that are recommended. Selected third-generation cephalosporins, such as cefotaxime and ceftriaxone, are the -lactams of choice in the empiric treatment of meningitis. They are active against Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. With the worldwide increase in the prevalence of penicillin-resistant pneumococci, vancomycin should be added to cefotaxime or ceftriaxone as empiric treatment until culture and susceptibility results are available. Ceftazidime, a third-generation cephalosporin with broad in vitro activity against gram-negative bacteria including Pseudomonas aeruginosa, is much less active against penicillin-resistant pneumococci than cefotaxime and ceftriaxone. However, a fourth-generation cephalosporin, cefepime, has been shown to be safe and therapeutically equivalent to cefotaxime for the treatment of bacterial meningitis and can be considered a suitable alternative to cefotaxime or ceftriaxone when broad activity against both the pneumococcus and gram-negative bacteria, such as Pseudomonas aeruginosa, is necessary. Among patients over the age of 50, or with impaired cell-mediated immunity (due, for example, to lymphoma, cytotoxic chemotherapy, or highdose glucocorticoids), coverage must be directed against Listeria monocytogenes. Question 48 A 32-year-old woman, previously healthy, is admitted to the hospital 2 weeks after traveling on a cruise ship. Abdominal examination shows good bowel sounds with a nondistended, nontender abdomen. Objective: Identify the empiric treatment regimens for acute bacterial meningitis. This patient presents with acute bacterial meningitis and empiric antibiotic therapy should be initiated as soon as possible to improve the associated morbidity and mortal- (c) 2015 Wolters Kluwer. Streptococcus pneumoniae Legionella pneumophila Chlamydia pneumoniae Histoplasma capsulatum Answer and Discussion the answer is b. Patients with pneumonia secondary to Legionella commonly present with high fever and gastrointestinal symptoms including diarrhea, nausea, and vomiting. Headaches and mental status changes may be seen, as well as electrolyte disturbances, particularly hyponatremia. In epidemiologic studies, Legionella is consistently reported among the top three or four most commonly identified pathogens in community-acquired pneumonia in immunocompetent patients and is also a common cause of hospital-acquired pneumonia. This diagnosis should be highly entertained among patients with the typical clinical manifestations of the illness, especially in the setting of a history of recent travel. Urinary antigen testing is rapid, sensitive, specific, and not costly, but is only useful for the diagnosis of Legionella pneumophila type 1 infection (which accounts for 90% of community-acquired Legionella infections in the United States). Question 49 A 58-year-old man with myasthenia gravis well controlled with pyridostigmine and mitral valve replacement with a St. Objective: Identify an acute neuromuscular blockade in a patient with neuromuscular disease given an aminoglycoside. Neuromuscular blockade after aminoglycoside administration is rare but potentially life threatening. This has been reported among patients given gentamicin, neomycin, streptomycin, kanamycin, tobramycin, or amikacin. Certain factors such as renal insufficiency, neuromuscular disease, botulism, hypocalcemia, and coadministration of succinylcholine and tubocurarine have been associated with this serious side effect. Calcium gluconate and neostigmine may reverse the respiratory depression and apnea. There is no report of opioids administration, therefore administering naltrexone, an opioid antagonist, is not indicated. He works at a textile mill, and he states that he had to stay off work for the past few days because he felt like he had the flu. Ceftriaxone and azithromycin are started empirically for a possible community-acquired pneumonia. The next day, the patient deteriorates rapidly, becomes hypotensive, and is saturating only 86% on room air. He has a history of Candida esophagitis 2 years ago and no other opportunistic infections. He tells you he cannot recall having received any immunizations in the recent past. One can consider meningococcal vaccination among those who will be traveling to endemic areas, military recruits, dormitory residents, or those with functional or anatomic asplenia. Question 52 A 19-year-old man is referred to you for a tuberculin skin test of a 7 mm induration. However, he had been exposed to his mother who had active pulmonary tuberculosis 6 months ago. Vancomycin and imipenem Ciprofloxacin, rifampin, and clindamycin Doxycycline Penicillin G Answer and Discussion the answer is b. Objective: Recognize the key findings and treatment choices for inhalational anthrax. The regimens used for the patients who survived in the 2001 bioterrorism attacks included ciprofloxacin, rifampin, and either vancomycin or clindamycin. The use of penicillin G is particularly discouraged due to the presence of inducible -lactamase resistance in B. Once the decision for outpatient management has been made, the choice of the empiric antibiotic regimen to be administered needs to be made. Thus, it is necessary to broaden coverage by using amoxicillinclavulanate, which is more active against penicillin-resistant Streptococcus pneumoniae than doxycycline. The addition of azithromycin is necessary to cover for atypical microorganisms as well. Another alternative would be a respiratory fluoroquinolone such as moxifloxacin or levofloxacin. Question 54 A 42-year-old woman comes to your clinic in July complaining of headaches, malaise, and generalized arthralgias 2 weeks after arriving from a summer trip in Arkansas. She initially presented to a local doctor 1 week ago and was prescribed doxycycline for 5 days. Despite this, she remains symptomatic, with worsening shortness of breath and persistent fevers. Chest auscultation reveals decreased breath sounds over the right middle lung field with increased tactile fremitus. This patient most likely has ehrlichiosis, based on her exposure to an endemic area during the summer season, her symptoms associated with pancytopenia, and the lack of a rash. The organism affects the monocytes or neutrophils, and patients typi- Answer and Discussion the answer is b. The first decision to make when faced with a patient with community-acquired pneumonia is whether or not hospital admission is necessary. The score is predictive for a high 30-day mortality if any one of the criteria is fulfilled. Treatment should be initiated in all patients suspected of having ehrlichiosis even without a laboratory diagnosis. In many cases, the diagnosis is made clinically because of the relative insensitivity of blood smears as well as the prolonged turnaround time for serologies. Treatment of choice is doxycycline, similar to the treatment for Rocky Mountain spotted fever. He has anicteric sclerae without conjunctival hemorrhages, good dentition, a clear chest on auscultation, and a regular heart rhythm without murmurs or ectopy. Abdominal examination is benign, and on his extremities, there are no stigmata of endocarditis. The patient states that this is his third catheter in the past 2 years given his previous history of line-related bloodstream infections. Infectious Disease 117 on several factors, including stable clinical status, absence of tunnel or site infection, and the microorganism causing the bacteremia. If the latter is identified, then it is reasonable to leave the catheter in place. In this case, given that the patient is nontoxic, the line looks clean and is functioning, and this is the third catheter in the past 2 years, the catheter does not have to be removed before getting the final result of the culture. It has to be removed however if Staphylococcus aureus is found to be the infecting organism, given its virulence and propensity for adherence to catheters and endovascular structures. He has a hemodialysis catheter on his right chest wall, which appears clean and nontender. The patient states that this is his third catheter in the past 2 years given his previous history of linerelated bloodstream infections. After 24 hours in the hospital, he is afebrile, and his follow-up blood cultures are all negative. Objective: Identify the appropriate management of central-line associated bloodstream infections. In this patient, the most likely source for fevers is a catheterrelated bacteremia. Based on current guidelines regarding the management of line-related infections, an attempt to salvage this hemodialysis catheter may be made depending (c) 2015 Wolters Kluwer. Objective: Identify appropriate management of central line-associated bloodstream infections. The most common location for epidural spinal cord compression is in the thoracic spine (60%). Thromboembolic events in patients with malignant superior vena cava syndrome and the role of anticoagulation. Cardiac tamponade caused by primary lung cancer and the management of pericardial effusion. Direct decompressive surgical treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Pericardial disease in patients with cancer: the differentiation of malignant from idiopathic and radiation-induced pericarditis. Matched pair analysis comparing surgery followed by radiotherapy and radiotherapy alone for metastatic spinal cord compression. Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of the bronchus: a systematic review. Neuroimaging and treatment implications of patients with multiple epidural spinal metastases. Outcomes of primary and secondary treatment of pericardial effusion in patients with malignancy. Glucocorticoid treatment for brain metastases and epidural spinal cord compression: a review. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the spine oncology study group. Emergency treatment of malignant extradural spinal cord compression: an evidence-based guideline. Dose-dense paclitaxel once a week in combination with carboplatin every 3 weeks for advanced ovarian cancer: a phase 3, open label, randomised controlled trial. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. Initial hormonal management of androgensensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. These usually manifest as cytopenias (idiopathic thrombocytopenic purpura and autoimmune hemolytic anemia). In patients refractory to , or intolerant of, interferon, imatinib results in a near 100% hematologic remission and at least a 50% cytogenetic remission. Second- and third-generation tyrosine kinase inhibitors are now available as well. Most important prognostic indicators include age, cytogenetics, and molecular genetics. However, allogeneic stem cell transplantation has benefit in those with poor-risk cytogenetics. It is characterized by coagulopathy in the form of disseminated intravascular coagulation. Successful adult chemotherapy regimens have been modeled after pediatric regimens. The initial empiric antibiotic should be broadspectrum enough to cover a wide variety of organisms, including Pseudomonas aeruginosa. Age-related incidence and other epidemiological aspects of myelodysplastic syndromes. Chemotherapy compared with autologous or allogeneic bone marrow transplantation in the management of acute myeloid leukemia in first remission. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet.
Buy epivir-hbv 150 mg low price. April 2015 - from Schaumburg IL - - Multiple Sclerosis Treatment & Symptom Options.
References
- Razi C, Harmanci K, Abaci A, et al. The immunostimulant OM-85 prevents wheezing attacks in preschool children. J Allergy Clin Immunol 2010; 126: 763-769.
- World Health Organization, USAID. MDR-TB Planning Toolkit. www.path.org/publications/files/TB_mdrtb_ toolkit.pdf Date last accessed: October, 2012.
- Loop FD, Lytle BW, Cosgrove DM, et al: J. Maxwell Chamberlain memorial paper. Sternal wound complications after isolated coronary artery bypass grafting: Early and late mortality, morbidity, and cost of care, Ann Thorac Surg 49(2):179-186, 1990 discussion 186-Weintraub WS, Jones EL, Craver J, et al: Determinants of prolonged length of hospital stay after coronary bypass surgery, Circulation 80(2):276-284, 1989.
- Farah MJ, Wilson KD, Drain HM, et al. The inverted face inversion effect in prosopagnosia: evidence for mandatory, facespecific perceptual mechanisms. Vision Res 1995;35(14): 2089-93.
- Acerini CL, Miles HL, Dunger DB, et al: The descriptive epidemiology of congenital and acquired cryptorchidism in a UK infant cohort, Arch Dis Child 94(11):868n872, 2009.
- Tansini I. Spora il mio muovo processo di amputazione della mammaella per cancre. Riforma Med (Palermo, Napoli) 1896;12:3.
- Jacob J, Ludgate CM, Forde J, et al: Recent observations on the ultrastructure of human urothelium. 1. Normal bladder of elderly subjects, Cell Tissue Res 193:543n560, 1978.