
Pristiq
| Contato
Página Inicial
Susan Faye Dent, MD
- Instructor in the Department of Medicine
- Member of the Duke Cancer Institute
https://medicine.duke.edu/faculty/susan-faye-dent-md
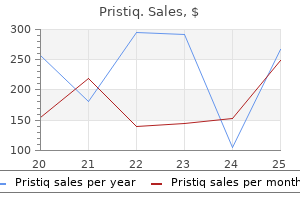
A target range of 4 to 14 g/mL has been suggested by some investigators for patients with epilepsy [69] medications 5 rights 50 mg pristiq for sale,[70] medications made from animals 100 mg pristiq buy visa. Use of serum concentration data may aid in the interpretation of drug interactions and adherence issues symptoms xanax overdose buy cheap pristiq 50 mg on-line. Given ongoing concerns regarding the interchangeability of various generic formulations of this drug [71] medications side effects prescription drugs buy on line pristiq,[72] symptoms 6 days after iui purchase generic pristiq canada, additional monitoring of serum concentrations both before and following generic substitution would also seem prudent. While the effect of adding an enzyme inducer to a regimen containing lamotrigine is well recognized, an important clinical question involves deinduction, following the removal of a concomitant inducer such as phenytoin or carbamazepine. In a recent pharmacokinetic analysis of lamotrigine serum concentration data derived from the pivotal conversion-to-monotherapy trial [75], Anderson et al. Importantly, these data suggested that lamotrigine concentrations did not significantly change (increase) until the concomitant enzyme-inducing drug was completely removed, and concentrations of either phenytoin or carbamazepine approached zero [76]. Modest reductions (approximately 30%) in lamotrigine serum concentrations have been noted in patients receiving concomitant oxcarbazepine [77], [78], [79], [80] and eslicarbazepine (approximately 14%) [81]. Comedication with ezogabine (retigabine) also seems to result in a modest 20% reduction in lamotrigine serum concentrations, although given that this medication is no longer available, this particular interaction would not seem relevant [82]. Valproate can markedly reduce lamotrigine clearance and prolong elimination half-life by about 60 hours [83]. Pharmacokinetic studies in adult volunteers have suggested that the maximal theoretical inhibition of lamotrigine clearance by valproate is approximately 65%, with 50% of maximal inhibition occurring at valproate plasma concentrations of approximately 5 to 6 g/mL. Maximal theoretical inhibition appears to occur at valproate concentrations of approximately 50 g/mL. These data suggest that valproate-mediated inhibition of lamotrigine begins at very low valproate doses. Data suggest that this interaction is slowly reversible, beginning within 3 days of valproate discontinuation and is largely gone within 2 weeks [85]. While earlier studies suggested that concurrent treatment with lamotrigine may result in modestly decreased valproate serum concentrations, this is unlikely to be of clinical significance [86],[87]. Effect of Lamotrigine upon Other Drugs Lamotrigine does not induce or inhibit any cytochrome P450 isozymes. These properties would predict lamotrigine to have a low incidence of causing pharmacokinetic interactions. Addition of lamotrigine does not alter serum concentrations of phenytoin, phenobarbital, primidone, carbamazepine, or carbamazepine epoxide [52],[60],[88],[89]. Occasional use of acetaminophen would not be expected to alter lamotrigine pharmacokinetics [91]. One anecdotal report has suggested a potential interaction between the serotonin-selective reuptake inhibitor sertraline and lamotrigine, with lamotrigine serum concentrations increasing following the addition of the antidepressant [92]; however, changes in lamotrigine concentrations are likely to be modest and are unlikely to be relevant in most patients [93]. The study with the highest dose (500 mg) [98] demonstrated a mean reduction in seizure frequency of 36% compared to baseline. These studies supported the initial approval for the indication of lamotrigine as adjunctive therapy for partial seizures in persons 16 years and older. In this study, the percentage of patients with at least a 50% reduction in seizure frequency was significantly greater than placebo (42% vs. Monotherapy for Partial Seizures Efficacy as monotherapy in partial seizures has been shown by several trials, including a multicenter, double-blind randomized trial comparing 500 mg of lamotrigine to an active control of 1000 mg of valproate [75] and a conversion-to-monotherapy study using an historical control group [101]. The primary end point for the active control study was proportion of patients exiting the trial according to a criterion of doubling of greatest 2-day or 1-month seizure rates observed in the baseline period. With this primary end point, 56% of patients taking lamotrigine completed the trial compared to 20% receiving low-dose valproate. In the historical control study, exit rates for participants were less than the aggregated exit rates for pseudoplacebo groups in eight completed conversion-to-monotherapy trials. Lamotrigine has been shown to have equivalent efficacy to immediate-release carbamazepine [102] and phenytoin [103] in double-blind, randomized clinical studies of recent-onset epilepsy in adults. Similarly, lamotrigine was shown to have comparable effectiveness when compared to controlled-release carbamazepine in newly diagnosed elderly patients with epilepsy [104]. Patients treated with lamotrigine were found to have a significantly longer time to treatment failure than either gabapentin or topiramate. A subsequent Cochrane review of a comparison 1258 between lamotrigine and carbamazepine included 9 trails and concluded that moderate quality evidence indicates lamotrigine superiority for treatment failure due to any reason or due to adverse effects, but carbamazepine superiority for efficacy as measured by time to first seizure [106]. Monotherapy dosing of lamotrigine has been examined in a retrospective cohort of 188 patients [107]. Of the 146 patients who were successfully treated, 68 (47%) were treated with 200 mg/d or less. Doses of 250 mg/d or more were more common for those patients who were older or had epilepsy for longer than 5 years. LennoxGastaut Syndrome in Children A large (n = 169) multicenter, double-blind, randomized add-on trial of lamotrigine demonstrated efficacy of lamotrigine for the treatment of major motor seizures in children and young adults with LennoxGastaut syndrome [108]. The target dose of lamotrigine was 15 mg/kg for patients not taking valproate and 5 mg/kg for those taking valproate. Major motor seizures, defined as atonic, tonic, major myoclonic, and tonicclinic, were reduced by 32% compared to baseline. Other studies have supported the efficacy of lamotrigine in LennoxGastaut syndrome [109], [110], [111]. A small case series suggested that myoclonus may worsen with lamotrigine treatment in some patients with generalized epilepsy [119]. Importantly, no serious adverse events, nor aggravation of other seizure types, were noted. Similarly, long-term seizure freedom in patients with juvenile myoclonic epilepsy has been reported to be comparable in patients randomized to receive lamotrigine or valproate [123]. While these data are certainly useful, the decision as to which agent should be considered drug of the first choice will likely still depend on patient-specific characteristics, such as gender, pregnancy, weight gain, etc. Safety and Tolerability Listen Similar to efficacy, the safety profile of lamotrigine has been defined by numerous clinical studies. Of the adverse effects reported with lamotrigine, rash has received the most attention [124],[125]. The incidence of serious rash associated with hospitalization and discontinuation of lamotrigine in the pediatric population was assessed in a prospectively followed cohort of pediatric patients (2 to 16 years of age) with epilepsy receiving adjunctive therapy. Interestingly, the clinical trials of lamotrigine for adults with bipolar disorder identified a rash rate of 0. When compared to either carbamazepine or phenytoin as monotherapy for new-onset epilepsy, lamotrigine monotherapy for new-onset epilepsy had an equivalent rash rate [102],[103]. In general, the risk for serious rash appears to be increased either when lamotrigine is initiated at a high starting dose or when the dosage is rapidly escalated [125]. There is also evidence that the combination of valproate and lamotrigine may increase the risk of serious rash in both pediatric and adult patients. This has included lymphadenopathy, eosinophilia, aseptic meningitis, and hemophagocytic lymphohistiocytosis [130],[131] (Lamictal Prescribing Information, 7/2018). These adverse reactions are apparently more likely during the initial titration of treatment but may occur after exposures lasting years. Improvement typically follows discontinuation of treatment and recurrence can follow reexposure. The diagnosis of a lamotrigine-related adverse immunologic reaction should, of course, follow exclusion of other possible causes, including infectious etiologies. The most common central nervous system and systemic adverse effects reported with lamotrigine conversion and monotherapy. Some adverse events are related to pharmacodynamic interactions, which occur most commonly with carbamazepine. However, a randomized, double-blind comparison study of lamotrigine and carbamazepine for new-onset epilepsy in the elderly (aged 65 to 90 years old) found no significant difference in most quality of life and adverse effects measures [133]. The one significant difference was a decrease in dysphoria for those taking lamotrigine. When compared to levetiracetam, lamotrigine did not have a significant difference in efficacy or tolerability in a prospective, randomized, open-label monotherapy study of patients with newly diagnosed focal or generalized epilepsy [134]. Other studies have also suggested that lamotrigine has a favorable psychotropic profile and may improve mood in some patients [135], [136], [137]. Data derived from rodents as well as human ex vivo placental perfusion studies suggest that lamotrigine easily and rapidly crosses the placenta [44]. Comparison of lamotrigine serum concentration in maternal and umbilical cord blood has identified a median infant-to-mother concentration ratio of 0. A direct comparison of the effect of lamotrigine on the fetus has been found to be lower than valproate and similar to carbamazepine with an odds ratio of 1. Molecular determinants of voltage-dependent gating and binding of poreStefani A, Spadoni F, Siniscalchi A, et al. Inhibition by lamotrigine of the generation of nitric oxide in rat forebrain slices. The effect of lamotrigine upon development of cortical kindled seizures in the rat. Effects of lamotrigine and conventional antiepileptic drugs on amygdala- and 1997;12(suppl 1):S2S9. Steady-state pharmacokinetics and bioavailability of immediate-release and extended-release formulations of lamotrigine in elderly epilepsy patients: use of stable isotope methodology. Transplacental passage of lamotrigine in a human placental perfusion Dickens D, Owen A, Alfirec A, et al. Evaluation of transport of common antiepileptic drugs by human multidrug and immediate-release formulations by pharmacokinetic simulation. In vitro N-glucuronidation of a novel antiepileptic drug, lamotrigine, by human liver microsomes. N+-glucuronidation, a common pathway in human metabolism of drugs with a tertiary amine group. Lamotrigine: single-dose pharmacokinetics and initial 1 week experience in Provinciali L, Bartolini M, Mari F, et al. The effect of age and comedication on lamotrigine clearance, tolerability, and Hussein Z, Posner J. Concentrationeffect and concentrationtoxicity relations with lamotrigine: a Toxicol. Lamotrigine and therapeutic drug monitoring: retrospective survey following the Froscher W, Keller F, Vogt H, et al. Compulsory generic switching of antiepileptic drugs: high switchback rates to Battino D, Croci D, Granata T, et al. Lamotrigine plasma concentrations in children and adults: influence of age and Vauzelle-Kervroedan F, Rey E, Cieuta C, et al. Influence of oxcarbazepine and methsuximide on lamotrigine concentrations in introduction of a routine service. The interaction potential of retigabine (ezogabine) with other antiepileptic drugs. Effect of lamotrigine on carbamazepine epoxide/carbamazepine serum lamotrigine in healthy subjects. Single dose pharmacokinetics of carbamazepine-10,11-epoxide in patients on Sidhu J, Job S, Singh S, et al. Lack of interaction between sertraline and lamotrigine in psychiatric Sabers A, Ohman I, Christensen J, et al. Report of the therapeutics and technology assessment subcommittee and quality standards subcommittee of the American Academy of Neurology and the American Epilepsy Society. Double-blind comparison of lamotrigine and carbamazepine in newly diagnosed partial seizures. Lamotrigine monotherapy in newly diagnosed untreated epilepsy: a Saetre E, Perucca E, Isojarvi J, et al. An international multicenter randomized double-blind double-blind comparison with phenytoin. Lamotrigine versus carbamazepine monotherapy for epilepsy: an individual Warshavsky A, Eilam A, Gilad R. Lamotrigine as monotherapy in clinical practice: efficacy of various dosages in participant at a review. Lamotrigine adjunctive therapy in childhood epileptic encephalopathy (the Schlumberger E, Chavez F, Palacios L, et al. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy: Crespel A, Genton P, Berramdane M, et al. Double-blind, placebo-controlled study of lamotrigine in primary generalized Biton V, Di Memmo J, Shukla R, et al. Efficacy and tolerability of lamotrigine in juvenile myoclonic epilepsy in Dooley J, Camfield P, Gordon K, et al. Lamotrigine-associated rash: risk/benefit considerations in adults and Deng Y, Li S, Zhang L, et al. Cognitive and behavioral effects of lamotrigine and carbamazepine monotherapy in Saetre E, Abdelnoor M, Perucca E, et al. Antiepileptic drugs and quality of life in the elderly: results from a randomized 2008;71:15271534. The LaLiMo trial: lamotrigine compared with levetiracetam in the initial 26 weeks of monotherapy for focal and generalized epilepsy-an open-label, prospective, randomized controlled multicenter study. The neurobiology of antiepileptic drugs for the treatment of nonepileptic conditions. Practice parameter update: management issues for women with epilepsy- Epilepsy Behav. Both agents have a favorable pharmacokinetic and safety profile, making them attractive as therapy for seizure management. The drug is a white to off-white crystalline powder with a faint odor and bitter taste.
A first seizure often is the first identifiable sign of epilepsy symptoms exhaustion generic pristiq 100 mg with amex, and in some cases treatment brown recluse spider bite pristiq 50 mg for sale, it is possible to recognize the specific underlying disorder (form of epilepsy) at its earliest presentation [60] medications blood donation pristiq 50 mg buy without prescription. In the case of Dravet syndrome medications you cannot eat grapefruit with proven 50 mg pristiq, the first definitive sign may be a febrile seizure-typically hemiclonic and prolonged-and treatment atrial fibrillation pristiq 100 mg purchase, with a genetic test, the epilepsy may be diagnosed before "unprovoked" seizures emerge [74]. Such situations are rare and difficult to accommodate in many epidemiologic studies because of the relatively crude diagnostic information used. For the field of epilepsy, however, they are increasingly important and should not be ignored. Etiology Terminology for referring to etiology has evolved considerably in recent years. The old, traditional terms, idiopathic, cryptogenic, and symptomatic, have been replaced by clearer, more descriptive language. Note, these are categories for causes, not the form (syndrome) of epilepsy per se. Each was carefully defined: genetic refers to causes for which, to our best understanding, the seizures are a direct result of the genetic error and seizures are the core symptom of the disorder. This differs from the older term idiopathic (meaning "presumed genetic") as a basis for the genetic inference is stated, and, unlike idiopathic, genetic includes disorders that do not necessarily have a "benign" outcome. The unwieldy term "structuralmetabolic" is intended to identify people with known underlying brain disorders that are primary contributors to their epilepsy. As most metabolic and many structural disorders have a genetic basis, the distinction between geneticstructural metabolic may seem fuzzy. The distinction focuses on the mechanism by which the genetic defect influences epilepsy as well as the constellation of symptoms presented by the patient, primarily seizures or seizures secondary to some other medical condition. The role of autoimmunity, an extremely important contributor to some epilepsies, is not adequately evoked by the term structural metabolic either [75]. As the mechanisms linking the precipitating cause to the development of epilepsy become better understood, it becomes more difficult to pigeonhole some causes. For example, some forms of cortical malformations that cause epilepsy are themselves due to viral infections in utero [76]. Finally, for referring to situations in which the cause is simply unknown, the term "unknown" is suggested. This is meant to be considered as a true statement of uncertainty or ignorance, without assumptions. The ability to identify the likely causes of epilepsy has changed dramatically over time with the introduction and increasing sophistication of neuroimaging and genetic testing. These changes are not uniformly implemented across countries or even across subpopulations within a country. Consequently, the unevenness of precision raises problems for cross population (including across time period) comparisons. For epidemiologic purposes, especially on the global level, a very pragmatic distinction could be made between what might be called complicated and uncomplicated epilepsy. Complicated epilepsy would include any epilepsy associated with a factor that is presumed to cause epilepsy (stroke, trauma, tuberous sclerosis, etc. Implicitly, uncomplicated would refer to epilepsy in which there is no clear insult or condition to which the occurrence of the epilepsy can be attributed and the individual is neurotypical (normal exams and cognition). Febrile seizures are a well-described and recognized seizure disorder, which, for historical reasons, has been distinguished (both clinically and in research) from epilepsy. For those involved in detailed genetic investigations, this may be an inappropriate distinction. For the epidemiologist, however, who may not always have the necessary clinical and particularly the genetic detail, the distinction is of value. It also has important clinical implications for the treatment of most of these children with such seizures. Epilepsy Syndromes Epilepsy syndromes have been alluded to above and are presented in greater detail in subsequent chapters of this book. Epilepsy, like cancer, is not a single disorder, and the efforts to identify specific forms of epilepsy reflect the importance of the diversity within the epilepsies. The epilepsy syndromes represent forms of epilepsy that have different causes, different manifestations, different implications for short- and long-term management and treatment, anticipatory guidance, genetic counseling, and longterm outcomes. Many epidemiologic studies do not attempt to identify specific forms of epilepsy; however, in large-scale population- and community-based studies, it is possible to do so, provided the investigators have access to the necessary information and the expertise needed to diagnose these syndromes [59], [60], [61]. As the questions in epileptology become increasingly sophisticated, including precise characterization of specific causes, types of seizures, and types of epilepsy, the gap between what typical epidemiologic studies can do versus the types of information needed from them has been widening. Seizure Types Perhaps the greatest and most relevant distinction for broad-scaled epidemiologic investigations is between convulsive and nonconvulsive seizures as a very crude marker of severity. Convulsive seizures include seizures with tonic, clonic, or combined tonic and clonic components. Nonconvulsive seizures are generally myoclonic, atonic, and spasms, as well as isolated focal motor phenomena. Nonconvulsive seizures also include nonmotor seizures, primarily absence, atypical absence, focal impaired awareness (formally complex partial or focal dyscognitive), and autonomic seizures. Correct identification for epidemiologic 58 studies depends on the source of information. In practice, the old lay distinction of big and little seizures may be all that is captured. Epidemiologic Challenges Listen Epidemiologic studies have provided valuable insights into the frequency of seizures within the population and have provided the initial impetus for some of the distinctions outlined above. Epidemiologists need, however, to be vigilant to potential sources of bias that threaten the validity of their findings. The ability of diagnosticians to appropriately identify cases and the capabilities of epidemiologists to identify those cases within the population are fundamental issues within the field of epidemiology. As the clinical and scientific field of epilepsy has grown more sophisticated, epidemiologists must work to keep up with important diagnostic and lexical distinctions. Diagnostic Issues and Considerations in Ascertaining Cases Seizures and epilepsy present a complex situation because the diagnosis is not based on a single source or type of information. To have a valid diagnosis, one must also be able to rule out many other conditions that mimic seizures. Ideally, a diagnosis of epilepsy should be undertaken by medical practitioners with expertise in epilepsy [83]. Unfortunately, access to neurologists and epilepsy specialists is often lacking in developing countries and often poor in developed countries as well. Consequently, diagnoses may be made by those with only minimal expertise in the field [84],[85]. Estimates of misdiagnosis rates suggest that over one-fifth of persons with a diagnosis of epilepsy may be misdiagnosed [86],[87]. Reevaluation of initial diagnosis of epilepsy in epidemiologic studies reports rates of 23% [88],[89] with diagnostic doubt among patients diagnosed by neurologists and nonspecialists reported at 5. The report estimates that 74,000 people in England are misdiagnosed with epilepsy and are therefore receiving inappropriate treatment. The financial cost of unnecessary or incorrect treatment combined with lost employment was estimated in 2007 at 134 million per annum [91]. Epidemiologic studies that rely on medical registers for case ascertainment provide valuable insights into levels of misdiagnoses. Primary care registers, a common source of case ascertainment in epidemiologic research, have also been found to include persons incorrectly diagnosed with epilepsy. Following the epileptologic evaluation, 30% of established and suspected cases were identified as not fulfilling the diagnostic criteria for epilepsy. These high levels of misdiagnosis have resulted in calls for a gold standard diagnostic criterion to distinguish epilepsy from other conditions with similar clinical features [86]. The implementation of these guidelines for children is monitored on a longitudinal basis by Epilepsy12, which conducts nationwide audits aiming to ensure a standardized level of provision across the United Kingdom [95]. In addition to the determination of whether or not someone has epilepsy, adequate information is needed to identify the specific form of epilepsy and its underlying cause. While this level of detail is frequently absent from traditional epidemiologic studies, it 59 must be incorporated in the future if epidemiologic studies are to continue to inform scientific and clinical endeavors relevant to epilepsy as it is understood and treated today. Without a meaningful diagnostic evaluation, epidemiologic studies can do little more than provide an approximate head count, which previous work has shown to be rather error prone. The lumping together of highly diverse disorders that share the diagnostic label "epilepsy" also limits the ability of epidemiologic studies to provide meaningful prognostic information. The case ascertainment options described above, based on medical registers, may not be suitable for all epidemiologic studies. Where these registers are unavailable, or considered unrepresentative, other more population-based methods may be used to identify people with epilepsy, albeit these methods also have their own unique challenges. Screening questionnaires, for example, are a common tool used in epidemiologic studies. In the second phase, these positive cases are evaluated clinically to confirm the presence of epilepsy. The screening tool reported sensitivity and specificity at 96% and 98%, respectively. More recently, a three-stage survey methodology has been proposed that comprised a two-item first survey, a more extensive second survey, and a third-stage clinical validation. This methodology reported a sensitivity of 49% and specificity of 100% and was found to be 37% less expensive than the more traditional two-stage process [97]. Screening tools are advocated by the World Health Organization, whose "Global Campaign Against Epilepsy" supports those undertaking epidemiologic research in resource-poor countries [98]. Demonstration projects managed under this program, in addition to assessments of local knowledge, attitude, and health service provision, undertake epidemiologic door-to-door studies to determine prevalence estimates. Other case ascertainment sources used in epidemiologic studies include prescription databases recording antiseizure medication usage. By definition, these studies estimate "treated epilepsy" and are more common in developed countries where the treatment gap is minimal. Prescription databases have been found to offer a suitable means by which the prevalence of epilepsy can be determined in community samples [99]. A potential source of bias in identifying persons with epilepsy from prescription databases is that cases cannot be clinically validated [100],[102]. This bias is magnified in situations where diagnosis is not recorded on the database and where "estimates" of drug use among people with epilepsy are applied [103],[104]. While antiseizure medications have been previously identified as "tracers" of epilepsy due to their chronic and highly specific usage [104], the growing use of antiseizure medication for indications other than epilepsy, such as pain, migraine, bipolar disorders, agitation, hormonal imbalance, and weight reduction, makes the identification of epilepsy through drug prescriptions of dubious validity. A methodology for case ascertainment that is becoming more frequently used in North American studies is the self-report survey. These studies typically include epilepsy-specific items in large population-based health surveys [105], [106], [107], [108]. The Canadian Health Survey, for example, was completed by over 130,000 persons, all of whom were questioned as to their health status, health care utilization, and determinants of health [105]. The California Health Interview Survey provided similar data on over 41,000 persons [108]. The Behavioral Risk Factor Surveillance System [109] provides an example of the typical type of epilepsy-specific items that can be included in these surveys: "Have you ever been told by a doctor that you have a seizure disorder or epilepsy More recently, the 2008 Health Styles Survey in the United States was used to examine life satisfaction among a representative sample of community-dwelling adults with self-reported epilepsy [110]. Where these items are common to both those with and without a self-report of epilepsy, important disparities can be identified. A selection bias may exist however whereby, despite the broad community-dwelling population from which samples are drawn, those who agree to participate in surveys may differ in some fundamental way from those who decline. This method also faces the challenge previously observed among studies examining prescription databases whereby cases are not clinically validated. Whether those who self-disclose epilepsy do in fact have the condition cannot be determined, no more so than those who have epilepsy but chose not to disclose it. Despite these challenges, population-based surveys that are conducted on an ongoing basis as part of a health surveillance system have recently been strongly endorsed by a cross-party report published by the U. This has led some researchers to propose that the most valid method to identify cases of epilepsy is to access multiple sources of case ascertainment [16]. Data linkage studies, for example, provide opportunities to simultaneously examine both population-based and hospital-based registers [112],[113]. These multicase ascertainment studies make it possible "not only to estimate the number of cases missed by each source but also to indirectly estimate the number of cases missed by the combined dataset" [114, p. Choice of case ascertainment, however, may not always be at the discretion of the epidemiologist. Resources of appropriately trained personnel, funding, and sophistication of health care services are some of the many factors that influence how the same study might be conducted differently in different jurisdictions. Variations in methodology have traditionally been identified as producing highly varying estimates of epilepsy [51],[115]. Recent research suggests that the influence of methodology on variation may have been somewhat overstated [2]. Irrespective, the lack of harmonized definitions employed across studies is a cause for concern. While the use of large-scale studies and attempts to harmonize definitions should ideally result in comparability across studies, all endeavors in clinical epilepsy research must face the challenges of epilepsy diagnosis. Repeated studies from tertiary centers find that a substantial proportion of adults referred for refractory epilepsy do not have epilepsy but have nonepileptic seizures [118]. This raises further concerns regarding the epidemiologic studies that repeatedly find a relationship between other psychiatric disorders (depression, anxiety, schizophrenia, and even suicidal ideation and suicide) and epilepsy. If the epilepsy is actually a nonepileptic psychiatric disorder and not epilepsy, that could explain a substantial proportion of this literature. Replication of findings, if based on the same diagnostic error, should not be taken as evidence that the association is necessarily real. No obvious solution to this problem is evident at this time; however, it is a strong reminder that population-based studies may contain considerable diagnostic error, and their findings should be interpreted cautiously. Summary Listen Epidemiology has been key in demonstrating the relatively high frequency of seizures in the population and in challenging longheld beliefs about the uniformly poor seizure outcomes associated with seizures.
Development can be delayed from the infancy or after a regression beginning between 3 months and 2 years of age treatment neuropathy order pristiq with amex. In other creatine synthesis disorders treatment 4 sore throat pristiq 100 mg purchase, seizures may present in the first months of life treatment 001 purchase 50 mg pristiq overnight delivery. Generalized tonicclonic medications migraine headaches order pristiq with american express, astatic medicine 666 colds pristiq 100 mg, absence, myoclonic, or focal seizures have all been described. Other clinical features may include dystonia, dyskinesias, microcephaly, and autistic behaviors [63]. A mild form presenting with severe speech delay, mild autism, and infrequent seizures has also been identified [64]. Testing is typically initiated by quantifying urine, plasma, and/or spinal fluid guanidinoacetate and creatine. Those diagnosed and treated in infancy may have normal or almost normal development [67]. Creatine transporter deficiency is less amenable to treatment though clinical improvement has been reported in some when treated with a combination of oral creatine, -arginine, and glycine. Early-Onset Multiple Carboxylase De ciency (Holocarboxylase Synthetase De ciency) 643 Early-onset multiple carboxylase deficiency presents in the first week of life with lethargy, respiratory abnormalities, irritability, poor feeding, and emesis. Generalized tonic seizures, focal motor seizures, and multifocal myoclonic jerks develop in 25% to 50% of cases. As this enzyme links biotin to four carboxylases in the mitochondria and one in the cytosol, an inactivity of all carboxylases results. Although rare, this condition is very important to recognize because prompt treatment with biotin may result in dramatic improvement. Laboratory findings demonstrate ketoacidosis and a characteristic pattern on organic acid analysis. Electrographically, a burst suppression pattern or multifocal spikes are observed. When not diagnosed and treated early, seizures are a prominent feature occurring in 50% to 75% of affected children. In fact, seizures are the presenting feature in 38% of patients and may be generalized tonicclonic, focal, myoclonic, or epileptic spasms. As the disease progresses, ataxia, optic atrophy, and sensorineural hearing loss develop. Diagnosis is typically made via abnormalities in urine organic acid and plasma acylcarnitine analysis. Biotinidase enzyme activity can be measured in leukocytes and cultured fibroblasts. When this condition is considered as a differential diagnosis, a therapeutic trial with high-dose oral biotin should be started while awaiting test results. Menkes Disease (Kinky Hair Disease) An X-linked disorder of copper absorption, Menkes disease, was first described by Menkes and colleagues in 1962. A characteristic twisting of the hair shaft, resulting in "kinky hair" of the head and eyebrows, is noted on microscopic examination of the poorly pigmented hairs. Affected boys may be premature and may have neonatal hyperbilirubinemia or hypothermia. Progressive neurologic deterioration with spasticity is present by 3 months of age. Seizures typically develop by 2 to 3 months of age and coincide with a neurologic regression [75]. Neuroimaging may show brain atrophy, focal areas of necrosis, and subdural collections. Daily copper injections may be beneficial if administered early in the course of the disease. It is now known that both Menkes and occipital horn syndrome conditions are allelic due to mutations in the same gene [77]. Disorders of Carbohydrate Metabolism Glut-1 Transporter De ciency Syndrome (De Vivo Disease) the Glut-1 transporter deficiency syndrome was first described in 1991 by De Vivo et al. Clinical features in the early-onset form of the disease include infantile seizures, developmental delay, spasticity, ataxia, hypotonia, and acquired microcephaly. Additional confirmation of impaired glucose transport can be performed through uptake assays in erythrocytes [80] and clinical genetic testing is available. Neonatal seizures are often the first identified feature of this syndrome in its classical form though patients with later onset and mild epilepsy have been described. Typical seizure types include absence, myoclonic, astatic, focal, and generalized seizures. Paroxysmal eyehead movements that appear as aberrant gaze saccades may be an early symptom in many patients and strongly suggest the diagnosis [82]. Affected individuals without a neonatal onset of epilepsy have been identified and a screening for lumbar puncture should be considered in anyone with refractory epilepsy when a genetic diagnosis has not yet been established [83]. Early initiation of the ketogenic diet is effective in the treatment of seizures as well as overall disease progression, as it provides an alternative cerebral energy source [84]. A >90% reduction in seizures has been reported in over eighty percent of a cohort of patients on the ketogenic diet [85]. Some patients have attempted a modified Atkins diet with reports of partial or complete efficacy when compared to the ketogenic diet though further study is needed [87],[88]. Most patients develop a dyskinetic phenotype in later childhood manifested by isolated movement disorders including episodic dyskinesias and ataxia [91]. Other Disorders Fructose 1,6-bisphosphatase deficiency, a rare, potentially life-threatening disorder of gluconeogenesis, presents within the first few days of life with respiratory abnormalities, hypotonia, lethargy, hepatomegaly, irritability, and seizures. Laboratory findings reveal lactic acidosis, ketosis, hypoglycemia, elevated plasma concentrations of alanine, and the presence of abnormal urinary organic acids with glycerol and glycerol-3phosphate [95]. Hereditary fructose intolerance (fructose 1,6-bisphosphate aldolase deficiency) may be seen in the neonatal period in infants who are formula fed and given fructose or sucrose early in life. Symptoms include profound hypoglycemia, emesis, and acute symptomatic seizures that are secondary to the hypoglycemia. If the disease is readily diagnosed, fructose and sucrose can be eliminated from the diet before significant cerebral injury occurs [95]. Mitochondrial Disorders Disorders of energy metabolism may present with early- or later-onset epilepsy. When not functioning properly, organs most dependent on cellular energy show symptoms-especially the brain. While multiorgan involvement and lactic acidosis were initially described as sine qua non of the disease, these findings are not reliably present and the vast majority of patients do not present with the classically described syndromes. We now know that almost any unexplained neurologic symptom can be due to mitochondrial dysfunction, especially refractory epilepsy. The epilepsy may occur in isolation, or with other neurologic problems including optic nerve disease, retinal pigmentary changes, hearing loss, developmental delays, neuropathy, and myopathy. Myoclonic epilepsy has been associated with mitochondrial disease, but patients with almost any seizure type, including generalized epilepsy and epileptic spasms, are seen [97]. These conditions typically occur due to genetic abnormalities leading to aberrant mitochondrial function. Diagnostic testing initially involves looking for a combination of biochemical abnormalities in plasma amino acids, acylcarnitines, lactate, pyruvate, and urine organic acids, though they lack sensitivity [98]. For many patients, diagnosis is now routinely made using genetic testing, circumventing the need for invasive studies. Treatment varies and includes preventing worsening during metabolic or physiologic stresses, avoiding mitochondrial toxins and poisons, use of select cofactors and supplements, and providing comprehensive preventative and symptomatic care. The E1 enzyme is itself a complex structure, a heterotetramer of two - and two -subunits. Structural abnormalities, such as Leigh syndrome like changes in the basal ganglia or deep gray matter lesions, white matter disease, and agenesis of the corpus callosum, are at times present on neuroimaging [103]. The ketogenic diet may benefit these patients with varying degrees of efficacy and clinical improvement noted [105]. Pyruvate Carboxylase De ciency Pyruvate carboxylase is a biotin-responsive enzyme that converts pyruvate to oxaloacetate in the citric acid cycle. Two predominant clinical presentations occur with pyruvate carboxylase deficiency, an autosomal recessive disorder. The neonatal type (type B) manifests with severe lactic acidemia and death in the first few months of life. The infantile and juvenile type (type A) begins in the first 6 months of life with episodes of lactic acidemia precipitated by an infection. Developmental delay, failure to thrive, hypotonia, and seizures, including epileptic spasms with hypsarrhythmia, may be seen [106]. A benign form (type C) also has been described with recurrent metabolic acidosis and normal neurologic development [107]. Seizures are related to the energy dysfunction that occurs secondary to citric acid cycle dysfunction. Treatment with the ketogenic diet or corticotropins may markedly exacerbate the disorder and should be avoided [108],[109]. Anaplerotic therapy with triheptanoin (C7 oil) has been proposed as an alternative treatment [110]. Diagnosis is made via analysis of amino and organic acids followed by genetic testing. Deficiency of pyruvate carboxylase enzyme activity can be measured in fibroblasts [111]. Biochemical defects in both nuclear and mitochondrially encoded genes have been identified with this condition. It is genetically heterogeneous, and depending on the etiology, may be autosomal recessive or dominant, X linked, or maternally inherited [112]. The clinical presentation is often acute to subacute, involving regression, cranial nerve and bulbar dysfunction, progressive hypotonia, lactic acidosis, and failure to thrive. Neuroimaging shows bilateral, fairly symmetric, basal ganglia, thalamic, and/or midbrain lesions that can fluctuate in severity. Varying degrees of white matter lesions may also be present along with cortical and cerebellar atrophy [113]. Aside from mitochondrial disease, other disorders that lead to deep gray matter lesions need to be excluded, including biotin and thiamineresponsive basal ganglia disease, vigabatrin toxicity, select genetic and metabolic leukoencephalopathies, toxin exposures, and select organic acidurias including glutaric aciduria. As Leigh syndrome is not due to one specific entity, a variety of different focal and generalized seizures have been described [114]. Disorders of Amino and Organic Acids Metabolism Amino and organic acids predominantly form from the catabolism of proteins and carbohydrates. Any enzymatic defect in these metabolic pathways leads to an accumulation of potentially acidic compounds, and partial inhibition of the citric acid and urea cycles. Acidosis and hyperammonemia ensue leading to encephalopathy and at times, seizures. These disorders, when most severe (a severe enzyme deficiency), typically present in the newborn period, especially after an infant is exposed to a protein or carbohydrate challenge in the diet. For some, this means after feeding in the first week of life, while for others, it is after the introduction of solid foods. Regardless of the type of amino or organic acid disorder, the acute presentation is often similar. Milder enzyme deficiencies may present with a later sudden-onset epileptic encephalopathy (later infancy, childhood, or in the adult years) in the midst of a physiologic stressor (illness, surgery, fasting) that leads to accelerated catabolism. Thus, many of these metabolic disorders should be considered in a patient with an acute to subacute epileptic encephalopathy of later onset as well when an etiology for the problem remains unknown. As genetic knowledge of these conditions has evolved, we have moved from making an analyte-based diagnosis from blood and urine testing to confirmatory molecular genetic diagnostic studies. As a consequence of the metabolic defect, toxic levels of the essential amino acid phenylalanine accumulate. If untreated, severe intellectual disability, autistic behavioral disturbances, psychosis, and acquired microcephaly can result. Primary treatment is a phenylalanine-free diet and addition of large neutral and essential amino acids. With early detection and institution of this diet, the neurologic sequelae of hyperphenylalaninemia can be prevented or significantly minimized [129]. The enzyme defect leads to accumulation of the branched-chain amino acids-valine, leucine, isoleucine- and their keto acids in body tissues and fluids. If left untreated, these signs may progress to stupor, apnea, opisthotonos, myoclonic jerks, and focal and generalized seizures. A characteristic odor can be detected in the urine and cerumen, but this may not be detectable until several weeks after birth. Laboratory testing reveals a metabolic acidosis and elevated blood and urine ketones. Ferric chloride testing of the urine causes a graygreen reaction, and the 2,4-dinitrophenylhydrazine test is positive. Definitive testing can be performed by enzyme assay and molecular genetic studies [132]. Tharp described resolution of this pattern in an affected infant when dietary therapy was initiated [134]. Pathologic studies reveal diffuse myelin loss and increased total brain lipid content. Disordered neuronal migration may occur with heterotopias and disrupted cortical lamination. Acute treatment is aimed at counteracting the effects of hypoglycemia, acidosis, and ending catabolism.
If the unit is to be shipped to another facility for transfusion treatment of hyperkalemia buy discount pristiq 100 mg on-line, it must be tested for transmissible diseases medicine doctor purchase line pristiq, similar to allogeneic blood treatment jaundice buy pristiq with paypal. If any of the transmissible disease tests are positive treatment 1st line generic pristiq 50 mg on-line, the unit must be labeled with a biohazard label medicine grace potter order pristiq 100 mg on line. However, directed donors do not have a lower incidence of transmissible disease markers14 and thus do not support a realistic rationale for these donations. Examples are past use of donor-specific transfusions before kidney transplantation, maternal platelets for a fetus projected to have neonatal alloimmune thrombocytopenic purpura, or family members of a patient with a rare blood type. An exception is donation of maternal platelets for a neonate with neonatal alloimmune thrombocytopenic purpura. As the genetic basis of hemochromatosis has become better understood, blood removed from these patients appears to be safe and red cells from patients with hemochromatosis are normal during blood bank storage,15 and although a blood collection program can operate successfully, this has not gained general acceptance. Red cells, platelets, granulocytes, blood stem cells, mononuclear cells, or plasma can be obtained by apheresis. The process results in a platelet concentrate with a volume of approximately 250 mL and containing approximately 3. Currently, blood cell separators produce a platelet concentrate that contains less than 5 × 106 leukocytes and thus can be considered leukocyte reduced. Cohn Jeffrey McCullough Xiangrong He Chronic shortages of group O red cells stimulated interest in the use of apheresis for collecting the equivalent of two units of red cells from some ©2021 McGraw Hill. Terms of Use · Privacy Policy · Notice · Accessibility donors, especially group O. The process results in a platelet Countway Medical Library concentrate with a volume of approximately 250 mL and containing approximately 3. The red cells usually have a very high hematocrit (Hct) count as they are removed from the instrument, but an additive solution is incorporated, and the red cells can be stored for the usual 42 days. Red cells obtained by apheresis have the same characteristics as those produced from whole blood. Because two units of red cells are removed, donors may donate only every 4 months. Because the efficiency of granulocyte extraction from whole blood is less than for platelets, the leukapheresis procedure involves processing 6500 to 8000 mL of donor blood for approximately 3 hours. To increase the separation of granulocytes from other blood components, hydroxyethyl starch is added to the blood-cellseparator flow system. In addition, glucocorticoids and granulocyte colony-stimulating factor have been administered to granulocyte donors to increase the granulocyte count and the granulocyte yield. Plasmapheresis usually can be performed in approximately 30 minutes and produces up to 750 mL of plasma. Because few red cells are removed, the procedure can be repeated up to two times per week, so theoretically a donor could provide a large amount of plasma. Because of the nature and possible frequency of plasma donation, special donor criteria apply. Because a plateletpheresis concentrate would be the sole source of platelets for a transfusion, the donor must not have taken aspirin for at least 3 days. Not more than 200 mL of red cells per 2 months or approximately 1500 mL of plasma per week can be removed. The laboratory testing of donors and apheresis components for transmissible diseases is the same as for whole-blood donation. Thus, the likelihood of disease transmission from apheresis components is the same as from whole blood. This type of reaction is managed by slowing the blood flow rate through the instrument, which slows the rate of citrate infusion. When granulocyte colony-stimulating factor and glucocorticoids are used in leukapheresis to obtain a granulocyte concentrate, approximately 60% of donors experience side effects-usually myalgia, arthralgia, headache, or flulike symptoms. During the last few years, testing for West Nile virus, Trypanosoma cruzi, Babesia,19 and, more recently, Zika have been added. Cohn Jeffrey McCullough Xiangrong He Laboratory Tests for Transmissible Agents of Donated Blood ©2021 McGraw Hill. Each step in the overall process of donor evaluation and testing adds to blood safety in important ways, and the donor Page 10 / 34, Claudia S. Terms of Use · Privacy Policy · Notice · Accessibility Tests for transmissible diseases further reduce the proportion of infectious donors. Currently, the risk of acquiring a transfusion-transmitted disease is Of use for immunodeficient recipients. Currently, the risk of acquiring a transfusion-transmitted disease is very low (Table 1384). The most problematic infections transmitted currently are caused by bacteria from infected platelet concentrates that are stored at room temperature. Oxygen delivery equals the product of cardiac output and the arterial oxygen content, which is mainly found bound to Hb. Oxygen delivery in most anemic patients can generally be compensated by increasing cardiac output. However, in patients with underlying comorbidities such as cardiovascular diseases, oxygen delivery becomes more dependent on arterial oxygen content and Hb level. Therefore, red cell transfusions are indicated to increase oxygen-carrying capacity in anemic patients, particularly in critically ill patients with cardiovascular comorbidities. It had been common practice to maintain critically ill patients at a Hb of 100 g/L; however, data in favor of this target level are lacking. Instead, multicenter randomized controlled trials indicate that compared with a target Hb of 100 g/L, target hemoglobin values of 70 to 80 g/L are associated with equivalent or better outcomes in most patient populations. The exclusion criteria included age younger than 16 years, active blood loss at the time of enrollment, admission after a routine ©2021 McGraw Hill. Terms of Use · Privacy Policy · Notice · Accessibility cardiac procedure, chronic anemia, imminent death, and others. Secondary outcomes included 60-day mortality, death during hospitalization, and multiple-organ dysfunction. The exclusion criteria included age younger than 16 years, active blood loss at the time of enrollment, admission after a routine cardiac procedure, chronic anemia, imminent death, and others. These findings also have been confirmed in subsequent metaanalysis of trials examining transfusion threshold. They were randomized to either the restrictive arm of Hb lower than 70 g/L versus 90 g/L for the liberal arm. Cohn Jeffrey McCullough Xiangrong He groups had similar characteristics, including equivalent numbers and grades of cirrhosis. The results of this study also favored a restrictive transfusion ©2021 McGraw Hill. Overall adverse events were lower in the restrictive transfusion group as well (P =. Mortality within the first 45 days was the primary outcome, and the rate of further bleeding and in-hospital complications were used as secondary outcomes. The two patient groups had similar characteristics, including equivalent numbers and grades of cirrhosis. The probability of survival at six weeks was higher in the restrictive strategy group (P =. In the restrictive transfusion arm, 51% of patients did not receive any transfusion, compared with 15% of patients in the liberal arm (P <. Generally, a transfusion threshold of 80 g/L is supported by subgroup analysis of three randomized transfusion trials that included patients with coronary artery disease. However, the rate of patients with acute pulmonary edema was significantly higher in the liberal transfusion arm. The primary outcome was death or an inability to walk across a room without human assistance on 60-day followup. Secondary outcomes included inhospital myocardial infarction, unstable angina, or death for any reason. The study found that a restrictive transfusion strategy of 80 g/L was not associated with worse outcomes, with the exception of an increase in myocardial infarction that was marginally statistically significant. Taken together, the evidence points to a Hb threshold of 80 g/L as the safe level to maintain for most asymptomatic patients with a history of cardiovascular disease. Patients with acute coronary syndrome continue to be an important exception for which current data are insufficient to support any guideline. The primary outcome measures the composite of all-cause mortality or recurrent nonfatal myocardial infarction within 30 days after randomization. One prospective study found a significant association between anemia and a decreased ability to walk independently after recovering from surgical procedures. Cohn Jeffrey McCullough Xiangrong He versus liberal (100 g/L) transfusion strategy. Terms of Use · Privacy Policy · Notice · Accessibility the authors concluded that a liberal transfusion strategy does not increase ambulation scores. The authors concluded that a liberal transfusion strategy does not increase ambulation scores. Although the transfusion threshold of 80 g/L may not be generalizable to the lower-risk orthopedic patient populations, until adequately powered studies are conducted, maintaining Hb lower than 80 g/L is generally considered the right approach for orthopedic patients. In addition, quality-of-life studies do indicate that a higher Hb level allows for faster recovery. It compared 2 Hb transfusion thresholds (70 and 100 g/L) on neurologic recovery after traumatic brain injury. A total of 200 patients with closed head trauma were enrolled within six hours of injury. The Glasgow Outcome Scale score was dichotomized as favorable (good recovery and moderate disability) or unfavorable (severe disability, vegetative, or dead) at 6 months post injury. The authors found, in this patient population, that maintaining Hb concentration of greater than 100 g/L did not result in improved neurologic outcome at 6 months. On the contrary, the transfusion threshold of 100 g/L was associated with a higher incidence of thromboembolic events. Although some studies reported a shorter hospital stay in the restrictive transfusion groups, the systematic review found insufficient evidence to recommend a restrictive strategy for neurologically impaired patients. In contrast to most of the other studies as of this writing, the evidence developed in this pilot trial suggests potential harm from using a lower threshold in this population. The primary outcome was mean Hb for 15 days after surgery, which demonstrated a statistically significant hemoglobin separation of the two groups (94. Regarding secondary outcomes, the evidence showed greater cerebral desaturation in the low trigger group, but no difference in muscular desaturation using near-infrared spectroscopy. Vascular complications were increased in the low-trigger group (18 vs 8 in the high-trigger group; P =. Because this is a small pilot trial, the optimal transfusion threshold for vascular surgery patients is unknown at this time. Basically, clinical trials of transfusion triggers for pediatric patients fall into two categories: general studies of critically ill pediatric patients and studies focused on high-risk neonates (see Table 1386). The restrictive arm used a Hb threshold of 70 g/L, versus a liberal threshold of 95 g/L. Terms of Use · Privacy Policy · Notice · Accessibility days old to 14 years of age) g/L dysfunction syndrome Page 14 / 34 In stable, critically ill children, a Hb threshold of 70 g/L can decrease transfusions without increasing adverse outcomes to 14 years of age. The restrictive Countway Medical Library arm used a Hb threshold of 70 g/L, versus a liberal threshold of 95 g/L. Thus, the authors concluded that for critically ill children, a Hb threshold of 70 g/L could decrease transfusion requirements without increasing the incidence of adverse outcomes. However, all three subanalyses were limited by small sample size, so no definitive conclusions could be drawn because of insufficient power. Trials in the neonate population have focused on premature babies and infants of very low birth weight. Unlike the clinical trials in adults, where most studies found that a restrictive transfusion approach was as good as, or possibly superior to , a liberal transfusion strategy, the results from clinical trials in premature infants were mixed. The Iowa Trial was a single-center randomized clinical trial to test whether using lower Hct thresholds for red cell transfusion would reduce the number of transfusions received by preterm infants with birth weights of 500 to 1300 g. The transfusion thresholds varied with the level of respiratory support needed and age. They found infants in the restrictive transfusion group were more likely to develop parenchymal brain hemorrhage or periventricular leukomalacia; they also had more frequent episodes of apnea. The Iowa Trial also found a reduction in the number of transfusions but not the number of donor exposures in the restrictive transfusion arm. However, the lack of difference in donor exposure most likely resulted from the use of a single-donor transfusion program. The authors suggested a more liberal transfusion practice in the neonatal population, especially in preterm infants. A total of 451 infants were randomized into restrictive (Hb 68115 g/L) or liberal (Hb 77135 g/L) transfusion arms. Using the same strategy as the Iowa Trial, the actual transfusion threshold was determined by a combination of age and level of respiratory support. The study found the mean number of transfusions triggered by a Hb threshold was significantly lower in the restrictive group. However, this difference was offset by a small but statistically significant difference in transfusions given for clinical reasons, many of which were for bleeding or surgery. The authors concluded that in extremely-low-birthweight infants, maintaining a higher Hb level results in more infants receiving transfusions but confers little evidence of benefit. A 2011 metaanalysis based on four trials with 614 premature infants found that the restrictive transfusion group received fewer transfusion and donor exposures, but they were more likely to be transfused at a later age.
When degrading crosslinked fibrin treatment quinsy discount 100 mg pristiq mastercard, plasmin initially cleaves the C-terminal region of the -chains and -chains within the D domain medications for rheumatoid arthritis order pristiq 50 mg fast delivery. Subsequently medicine descriptions purchase pristiq without prescription, some of the connecting regions between the D and E domains are severed treatment 5th toe fracture pristiq 50 mg order mastercard. Fibrin is ultimately solubilized upon hydrolysis of additional peptide bonds within the central portions of the coiled-coil connectors medications an 627 order pristiq no prescription, giving rise to fibrin degradation products such as D-dimer. Assay of crosslinked D-dimer fragments is employed clinically to identify disseminated intravascular coagulation-like states associated with excessive plasmin-mediated fibrinolysis. Several biologic activities, including inhibition of platelet function,226 potentiation of the hypotensive effects of bradykinin,227 chemotaxis,228 and immune modulation,229 are ascribed to fibrin breakdown products. When plasmin forms on the fibrin surface, both its lysine binding sites and its active site are occupied. This is the basis for its specificity as a lytic agent in the treatment of thrombosis. This may reflect neutralization by fibrin of components in plasma that impair plasminogen75 also reflect a conformational change in plasminogen upon binding to fibrin. Basement membrane proteins such as thrombospondin,235 laminin,236 fibronectin,237 and fibrinogen,238 are readily degraded by plasmin in vitro, suggesting possible roles in inflammation,239 tumor cell invasion,240 embryogenesis,241 ovulation,242 neurodevelopment,243,244 and prohormone activation. Impaired wound healing is observed in the plasminogen "knockout,"248 and is reversed upon simultaneous deletion of fibrinogen. In the lung, the fibrinolytic system mediates lung matrix remodeling, through mechanisms that appear to be independent of fibrin degradation. Hajjar Jia Ruan the role of the fibrinolytic system in vascular remodeling during atherosclerosis appears to be complex. Terms of Use · Privacy Policy · Notice · Accessibility 264 As the injury resolves, fibrin endothelial cell lining of blood vessels, deposition of intravascular fibrin and organization of a thrombus occurs. The role of the fibrinolytic system in vascular remodeling during atherosclerosis appears to be complex. Among 93 patients with type I plasminogen deficiency, the prevalence of thrombosis was 24%, or 9% when the propositi were excluded. Hajjar Jia Ruan plasminogen deficiency may occur in liver disease, sepsis, and Argentine hemorrhagic fever resulting from decreased synthesis and/or increased ©2021 McGraw Hill. Terms of Use · Privacy Policy · Notice · Accessibility catabolism,299 but associated thrombosis may be a result of abnormalities in other hemostatic factors in these very ill patients. Bleeding resolves upon initiation of all-trans-retinoic acid therapy, which eliminates expression of promyelocyte annexin A2, probably through a transcriptional mechanism. These phenotypes complicate the use of antifibrinolytic therapy in trauma and argue for the early use of tranexamic acid in the setting of severe trauma with hemorrhage. Hajjar Jia Ruan line placement, Kawasaki disease, and Henoch-Schönlein purpura in this age group. Because arterial thrombosis immediately renders distal tissue ischemic with rapid onset of dysfunction and necrosis, a critical problem is minimizing time to restoration of flow. Thrombolytic therapy should be viewed as one part of an overall antithrombotic plan that frequently includes anticoagulants, antiplatelet agents, and mechanical approaches (such as mechanical thrombectomy in stroke), all designed to rapidly restore flow, prevent reocclusion, and promote healing. Here, we review thrombolytic approaches to stroke and peripheral vascular disease. Thrombolytic therapy for deep vein thrombosis, pulmonary embolism, and myocardial infarction are discussed elsewhere (Chap. However, if large amounts of plasminogen activator overwhelm the natural regulatory systems, plasmin may be formed in the blood, resulting in degradation of susceptible proteins, the "lytic state. Several therapeutic agents, from both recombinant and natural sources, are available and approved for thrombolytic use (Table 1353). The degree of "fibrin specificity," is critical in determining the intensity of action at the site of a thrombus. Regarding site of delivery, systemic therapy via peripheral vein is simpler and does not require specialized facilities, but results in greater systemic complications. Anticoagulant therapy is routinely continued after completion of fibrinolytic therapy to prevent reocclusion. Regarding site of delivery, systemic therapy via peripheral vein is Access Provided by: simpler and does not require specialized facilities, but results in greater systemic complications. Regional delivery with a catheter placed close to the proximal end of the thrombus can provide a high local concentration with a smaller total dose, thereby increasing the local effect and limiting systemic exposure. Fibrinolytic therapy is often administered in combination with an anticoagulant to block fibrin formation and with an antiplatelet agent to limit continued platelet deposition. In addition, mechanical approaches such as percutaneous coronary intervention often play a vital role in removing the underlying cause of thrombosis. The activation of plasmin has effects beyond the thrombus, including a reduction in fibrinogen, increase in fibrinogen degradation products, and depletion of plasminogen and 2-plasmin inhibitor. Screening coagulation tests, including the activated partial thromboplastin time, prothrombin time, and thrombin clotting time, will be prolonged depending on the intensity of the lytic state. Tests reflecting plasminogen activation such as the euglobulin clot lysis time will be abnormal. Platelet membrane proteins also may be degraded, resulting in abnormal platelet function. High doses of a nonspecific activator, such as streptokinase, will cause a more marked lytic state, compared to that seen with a fibrin-specific agent such as reteplase. Patient selection for fibrinolytic therapy depends on careful consideration of risks and benefits (Table 1354). For patients with acute myocardial infarction or stroke there is a higher tolerance of bleeding complications, because lytic therapy can be lifesaving and limit disability. Timing of treatment is also critical, with greater benefit achieved with earlier administration. Selection of Patients for Thrombolytic Therapy Treat those most likely to respond and benefit Acute myocardial infarction: Within 12 hours of onset; consider percutaneous intervention Stroke: Ischemic stroke within 4. Hajjar Jia Ruan Massive or submassive embolism, especially with hemodynamic compromise ©2021 McGraw Hill. Terms of Use · Privacy Policy · Notice · Accessibility Avoid bleeding complications Major contraindications Page 18 / 57 Patient selection for fibrinolytic therapy depends on careful consideration of risks and benefits (Table 1354). For patients with acute myocardial Countway Medical Library infarction or stroke there is a higher tolerance of bleeding complications, because lytic therapy can be lifesaving and limit disability. Timing of Access Provided by: treatment is also critical, with greater benefit achieved with earlier administration. Whereas fibrinolytic therapy for acute pulmonary embolism may be lifesaving, the potential benefits for venous disease are less clear and more likely to be associated with bleeding problems. Although aspirin and anticoagulants may be useful in prevention, thrombolytic therapy is the only available intervention during the acute stage. The appropriate use of thrombolytic therapy for stroke is based on an understanding of its pathogenesis. Ischemic stroke is most commonly caused by rupture of an atherosclerotic plaque within a large-sized or medium-sized artery in the neck or cranium. In addition, transient ischemic attacks and strokes involving small arteries can result from embolization of plateletfibrin thrombi that form on atherosclerotic vessels in the neck and ascending aorta, or from embolization of thrombi that form in the heart in association with atrial fibrillation, valve dysfunction, artificial valves, or endocardial thrombi. Current approaches to thrombolytic therapy for stroke are based on imaging to define the etiology, results of clinical trials, and the experience with thrombolysis for acute myocardial infarction. Additionally, arteriography can identify obstructed vessels and follow the course of recanalization during thrombolytic therapy. Hajjar Jia Ruan pathologic role of the occluded vessel, the importance of early recanalization in preserving myocardium, and the impressive decrease in morbidity/ and ©2021 McGraw Hill. Terms of Use · Privacy Policy · Notice · Accessibility mortality resulting from early reperfusion. The experience with thrombolytic treatment for stroke also highlights important differences from myocardial infarction. The arterial anatomy of the aorta, or from embolization of thrombi that form in the heart in association with atrial fibrillation, valve dysfunction, artificial valves, or endocardial thrombi. Countway Medical Library Access Provided by: Current approaches to thrombolytic therapy for stroke are based on imaging to define the etiology, results of clinical trials, and the experience with thrombolysis for acute myocardial infarction. Modern computed tomography and magnetic resonance imaging can identify ischemic areas and localize areas of hemorrhage quite early. Clinical studies have generally followed the successful designs used for myocardial infarction that demonstrated the critical pathologic role of the occluded vessel, the importance of early recanalization in preserving myocardium, and the impressive decrease in morbidity and mortality resulting from early reperfusion. The arterial anatomy of the brain is more complex, the time from onset of ischemia to irreversible necrosis is shorter, the risk and consequences of bleeding are greater, and there is more variability in the thrombo(embolic) occluding lesion. Furthermore, the occlusive plateletfibrin thrombus that precipitates a myocardial infarction is quite small, whereas the occlusive lesion causing ischemic stroke may be a large in situ thrombus, small plateletfibrin embolus, or large embolus of varying age and composition originating from the left atrium. Thrombolysis has had a smaller impact for stroke than it has for myocardial infarction, based largely on these differences. Major Fibrinolytic Therapy Trials in Stroke Countway Medical Library Access Provided by: Study No. The combined results showed a 30% improvement in clinical outcomes at 3 months and the benefit persisted at 12 months, despite a 10fold increase in early symptomatic intracranial hemorrhage. Furthermore, the metaanalysis alluded to the potential benefit of extending the treatment window to 4. The primary outcome of functional status at 90 days did not differ between groups, while fewer patients in the intensive group had any intracranial hemorrhage (odds ratio: 0. The number of patients with any serious adverse event did not differ significantly between the intensive group and the guideline group. The dose effect of alteplase was evaluated in a group of predominantly Asian patients with acute ischemic stroke who were eligible for thrombolysis reperfusion therapy. Streptokinase Therapy Countway Medical Library the dose effect of alteplase was evaluated in a group of predominantly Asian patients with acute ischemic stroke who were eligible for thrombolysis reperfusion therapy. Fewer patients treated with low-dose alteplase than with standard-dose alteplase (1% vs 2%) had the secondary outcome of symptomatic intracerebral hemorrhage. Streptokinase Therapy Streptokinase has been evaluated in three large stroke trials. In a phase 2B study, there were no significant differences in intracranial bleeding or other serious adverse events in patients receiving alteplase versus tenecteplase. Intraarterial Thrombolysis Intraarterial administration allows delivery of a high concentration of a plasminogen activator in proximity to the thrombus, more accurate anatomic diagnosis, the ability to observe the course of recanalization, and lower total doses of drug that might reduce intracranial hemorrhage. On the other hand, this approach requires specialized facilities and experienced personnel to perform arteriography and selective catheterization, which may delay treatment. The proportion of patients with an excellent functional outcome was significantly better in the intraarterial urokinase group (42% vs 23%, p = 0. Intracerebral hemorrhage within 24 hours of treatment occurred in 9% and 2%, respectively (p=0. This study suggested that intraarterial fibrinolysis has the potential to increase the likelihood of excellent functional outcome in appropriate clinical settings. Overall, these studies show that treatment of acute stroke with thrombolytic therapy can lead to recanalization of the occluded artery and improvement in clinical outcomes. Terms of Use · Privacy Policy · Notice · Accessibility In summary, current recommendations limit thrombolytic therapy for stroke to patients presenting within 3 hours of symptom onset. The best results are obtained in patients who meet strict eligibility requirements (Table 1356). Patients should be closely monitored for bleeding complications, especially intracranial hemorrhage, and careful attention should be paid to blood pressure and other comorbidities. Anticoagulation is useful to prevent thrombus extension, while thrombolytic therapy or surgery can restore perfusion. Early approaches to acute peripheral arterial occlusion involved streptokinase, and small studies demonstrated reperfusion in approximately 40% of patients, with greater success in treating occlusions of recent onset, and bleeding complications in up to one-third of patients. Advantages include delivery of a high concentration of drug directly to the site of thrombosis, the ability to follow the course of treatment using the treatment catheter, and identification of local vascular lesions requiring endovascular or surgical treatment after recanalization. Treatment involves arterial access from a remote site followed by fluoroscopic guidance of the catheter to administer drug directly into the thrombus. Terms of Use · Privacy Policy · Notice · Accessibility 410 Ouriel and colleagues411 reported that thrombolytic therapy resulted in a 70% recanalization reperfusion occurs in approximately 75% of cases. There was, however, a survival advantage in patients receiving in 1974 by Dotter and colleagues409 of successful thrombolysis in peripheral arterial occlusion using locally administered thrombolysis, practice moved Countway Medical Library progressively to the nearly exclusive use of local intraarterially administered treatment. Advantages include delivery of a high concentration of drug Access Provided by: directly to the site of thrombosis, the ability to follow the course of treatment using the treatment catheter, and identification of local vascular lesions requiring endovascular or surgical treatment after recanalization. Therapy is delivered by continuous infusion over hours to days and requires close monitoring and a large dose of thrombolytic agent. There was, however, a survival advantage in patients receiving primary thrombolytic therapy, largely as a result of the decrease in the occurrence of in-hospital complications. There was a significant reduction in the frequency and magnitude of surgical interventions eventually required in patients randomized to initial thrombolysis. Major hemorrhagic complications were significantly more frequent with urokinase (13%) than with surgery (6%; p = 0. Key points include early, accurate angiographic diagnosis, appropriate intrathrombic catheter positioning, and, in some cases, definitive endovascular or surgical procedures. Reports document successful treatment of intraabdominal thrombosis including Budd-Chiari syndrome,431 portal vein thrombosis,432434 and mesenteric vein thrombosis. The most serious complication, intracranial hemorrhage, occurs in approximately 1% of patients and is associated with a high mortality and serious disability in survivors. Risk factors for intracranial hemorrhage, including prior stroke, serious head trauma, intracranial surgery, tumor, and vascular disease, such as aneurysms, atrioventricular malformations, and uncontrolled hypertension, are strong contraindications to fibrinolytic therapy. Treatment of bleeding involves local measures as well as correction of the systemic hypocoagulable state resulting from proteolysis of plasma proteins and platelets (Table 1357). For serious bleeding, an antifibrinolytic agent, such as -aminocaproic acid, can be administered, but will be effective only if the fibrinolytic agent remains in the blood. Countway Medical Library Treatment of bleeding involves local measures as well as correction of the systemic hypocoagulable state resulting from proteolysis of plasma proteins Access Provided by: and platelets (Table 1357).
Buy pristiq cheap online. I'm A Stranger || Restless Modern Lyrics.
References
- Tauber MG. Brain edema, intracranial pressure and cerebral blood flow in bacterial meningitis. Pediatr Infect Dis J. 1989;8(12):915-917.
- Hashimoto S, Fujii W, Takahashi T, et al. Pulmonary hyalinizing granuloma with hydronephrosis. Intern Med 2002;41:463-6.
- Jenkins C, Chan J, Hanekom L, et al: Accuracy and feasibility of online 3-dimensional echocardiography for measurement of left ventricular parameters, J Am Soc Echocardiogr 19:1119-1128, 2006.
- Coleridge-Smith P, Labropoulos N, Partsch H, et al: Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs-UIP consensus document. Part I. Basic principles, Eur J Vasc Endovasc Surg 31(1):83-92, 2006.
- Moazami N, Diodato MD, Moon MR, et al: Does functional mitral regurgitation improve with isolated aortic valve replacement? J Card Surg 19:444, 2004.
- Morselli PG. Fixation for forehead endoscopic lifting: a simple, easy, no-cost procedure. Plast Reconstr Surg 1996;97:1309.
- Sheu JJ, Tsai TH, Lee FY, et al. Early extracorporeal membrane oxygenator-assisted primary percutaneous coronary intervention improved 30-day clinical outcomes in patients with ST-segment elevation myocardial infarction complicated with profound cardiogenic shock. Crit Care Med. 2010;38(9):1810-1817.