
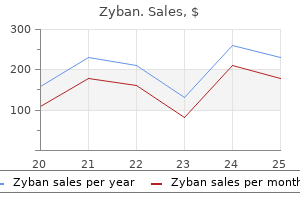
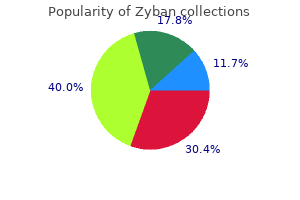
Zyban
| Contato
Página Inicial
Erik D. Maki, PharmD, BCPS
- Associate Professor, College of Pharmacy and Health Sciences, Drake University, Des Moines, Iowa
Newer technology anxiety 2nd trimester cheap zyban 150 mg with mastercard, which uses flow cytometry to accurately identify immature granulocytes anxiety 9 months postpartum zyban 150 mg buy on-line, has been shown to be as effective depression symptoms headache buy 150 mg zyban amex, with faster turnaround time and less operator variability than manual differentials anxiety relief techniques cheap 150 mg zyban amex. C-reactive protein levels increase within 6 to 8 hours after infection and peak after 24 hours depression research buy cheap zyban 150 mg on-line. Serial determinations may be useful for identifying infants who do not have a bacterial infection or in monitoring response to treatment for infected infants. Increased levels can also be seen with noninfectious causes, such as respiratory distress syndrome. Several have been shown to rise early in the course of infection, and in the future cytokine assays may be helpful in diagnosis or in guiding decisions regarding therapy. Empiric use of third-generation cephalosporins is not recommended because of concerns for development of resistance and the increased risk for invasive candidiasis with prolonged administration. Empiric therapy for late-onset sepsis usually consists of vancomycin and an aminoglycoside, providing coverage for coagulase-negative Staphylococci, S. As with early-onset disease, if Gram-negative meningitis is suspected, consider adding a third-generation cephalosporin. Carbapenems may be considered, depending on local resistance patterns or if the patient had previously received therapy with a third-generation cephalosporin. Once a pathogen is identified, therapy should be tailored to the species and antimicrobial susceptibilities. However, there is little evidence from randomized, controlled trials on the appropriate duration of treatment for cultureproven sepsis, especially in preterm and low birth weight infants. In well-appearing infants without clinical or hematologic evidence for infection, standard practice is to discontinue antibiotics if cultures have been negative after 48 hours. Management decisions are much more challenging for those infants in whom sepsis is highly suspected but cultures are negative, which is often the case for preterm infants. Infants whose mothers received antibiotics during labor may have false-negative blood cultures because of antibiotic suppression. Cerebrospinal fluid culture data may be lacking in infants who are not clinically stable enough to tolerate a lumbar puncture. Noninfectious conditions mimicking sepsis can also complicate the clinical picture. Preventive efforts to reduce the risk of late-onset sepsis have focused on infection control in the postnatal environment. Successful measures include hand hygiene, proper management of central venous catheters, appropriate use of antibiotics, and limited use of histamine-2 blockers and proton pump inhibitors. The roles of exclusive maternal milk feeding and probiotic prophylaxis in prevention of lateonset sepsis require further study. Infants with early-onset meningitis present within the first week of life, usually within 72 hours of birth. These infections are vertically transmitted and are associated with the complications of labor and delivery. Late-onset disease occurs after the first week of life and reflects community or nosocomial transmission. Gram-negative enteric bacilli cause 30% to 40% of cases of neonatal meningitis, and E. Other important Gram-negative organisms include Klebsiella, Enterobacter, Citrobacter, and Serratia species. The clinical presentation of neonatal meningitis is largely the same as that of neonatal sepsis without meningitis. The most common finding is temperature instability, which occurs in approximately 60% of infants with meningitis. Most infants present with a full, but not bulging, fontanelle without meningeal signs. For clinically stable infants, the lumbar puncture should be performed before administration of antibiotics. Cerebrospinal fluid protein and glucose values are highly variable in neonates with and without meningitis. Cerebrospinal fluid Gram stain may be helpful in providing an early presumptive etiologic diagnosis, although a negative Gram stain certainly does not exclude the diagnosis. Empiric therapy for early-onset meningitis includes ampicillin and an aminoglycoside. If infection with a Gram-negative organism is suspected, the regimen should be expanded to include cefotaxime in addition to ampicillin and an aminoglycoside. Once a pathogen is identified, therapy should be tailored according to the causative organism. Group B streptococcus meningitis is treated initially with ampicillin (or penicillin) plus an aminoglycoside. Group B streptococcus has thus far been shown to be uniformly susceptible to penicillins. A fourthgeneration cephalosporin (cefepime) or a carbapenem (meropenem) in combination with an aminoglycoside should be considered for infection with members of the Enterobacteriaceae family with inducible beta-lactamase resistance. Recent studies have shown that recommended meningitic doses of meropenem may be toxic at lower gestational ages and may produce seizures. Most of these organisms are resistant to penicillin, and treatment with vancomycin is often required. Although the adjunctive use of corticosteroids for Haemophilus influenzae B meningitis in older children has been demonstrated to decrease neurologic morbidity, there is no evidence that corticosteroids improve the outcome for neonatal bacterial meningitis other than tuberculosis meningitis. Mortality rates were estimated at almost 50% in the 1970s,6 and have decreased to current estimates of 10% to 20%,31,68 with higher mortality rates among preterm infants. Neurologic sequelae include developmental delay, seizures, hydrocephalus, cerebral palsy, blindness, and hearing loss. Studies estimate that among survivors, 21% to 38% will have mild deficits and 24% to 29% will have severe neurologic sequelae. Early-onset pneumonia is usually acquired within the first 3 days of life via vertical transmission, including aspiration of infected amniotic fluid and transplacental transmission. The risk for late-onset pneumonia is highest among infants who require mechanical ventilation. Other risk factors include extreme prematurity, prolonged hospitalization, and previous bloodstream infection. Ureaplasma urealyticum has been potentially linked to the development of chronic lung disease in colonized infants. However, the significance of this association is unknown, and the efficacy of antimicrobial therapy for colonized infants is also uncertain. Chlamydia trachomatis pneumonia and ophthalmia neonatorum are discussed in more detail elsewhere. Definitive culture data are often lacking for cases of late-onset, community acquired neonatal pneumonia. Streptococcus pneumoniae is considered a predominant causative pathogen in this population. Staphylococcus aureus, Streptococci, Klebsiella pneumoniae, Citrobacter, Enterobacter, Serratia, and Pseudomonas have all been shown to have the potential to cause extensive lung injury, including abscess formation, empyema, and pneumatoceles. Receipt of Tdap vaccine during pregnancy allows for maternal pertussis antibody transfer to the neonate. This provides protection for infants from birth to the time of infant pertussis vaccination at 2 months. Other associated signs are apnea, lethargy, poor feeding, temperature instability, abdominal distention, poor perfusion, and metabolic acidosis. In addition, mechanically ventilated infants may require increased oxygen or ventilatory support. The differential diagnosis for neonatal pneumonia includes many noninfectious causes, such as transient tachypnea of the newborn, respiratory distress syndrome, meconium aspiration, pulmonary hemorrhage, pneumothorax, hypoglycemia, and metabolic acidosis. Anatomic abnormalities that can cause respiratory distress include primary pulmonary hypoplasia, tracheoesophageal fistula, choanal atresia, congenital diaphragmatic hernia, and congenital heart disease, among many others. The differential diagnosis is broad, and causative pathogens are rarely identified. Chest radiographs can be helpful in making the clinical diagnosis, although there is significant radiologic overlap between pneumonia and other respiratory disorders of the newborn. In pneumonia, radiographs often reveal bilateral alveolar densities with air bronchograms, or irregular, patchy pulmonary infiltrates. Pleural effusions are seen in up to two thirds of pneumonia cases, and are almost never seen in uncomplicated respiratory distress syndrome. If an infant has been intubated for several days, the endotracheal tube will invariably become colonized and will be of little value in the evaluation for sepsis. Therapy can then be tailored to susceptibility results if a causative organism is identified. Empiric antibiotic therapy for lateonset pneumonia will depend on local bacterial resistance patterns in both the hospital and the community. Vancomycin and an aminoglycoside are commonly used as empiric therapy to provide coverage against coagulasenegative Staphylococci and methicillin-resistant S. If Pseudomonas is suspected, an aminoglycoside plus an anti-pseudomonal beta-lactam, such as ceftazidime or piperacillin-tazobactam, should be given. In developed countries, the morbidity and mortality from neonatal pneumonia depend largely on the gestational age of the patient, severity of disease, and underlying medical conditions, especially chronic lung disease. This is owing to enhanced bacterial adherence to the foreskin and increased bacterial colonization in the urogenital tract. Infection of the urinary tract in neonates is thought to be acquired either through hematogenous spread or by ascending infection, which is often associated with anatomic abnormalities. Adhesins on the bacterial surface allow for increased adhesion to urogenital tract cells, and fimbriae are important in promoting persistence of infection. Other common causative organisms include other Enterobacteriaceae: Klebsiella, Enterobacter, Proteus, Citrobacter, Salmonella, and Serratia. Gram-positive organisms are isolated much less frequently than Gram-negative organisms, although Enterococci, S. The clinical presentation of preterm infants is similar to that of term infants, although preterm infants may also have hypoxia or apnea with bradycardia. Definitive diagnosis must be made by urine culture with specimens obtained by catheterization or suprapubic bladder aspiration. Samples collected into a bag are inappropriate because they are frequently contaminated. Catheterization cultures with greater than 1000 colony-forming units per milliliter are considered meaningful. If the infection is caused by a highly resistant pathogen, or if there is a known anatomical abnormality, a urine culture may need to be repeated 2 to 3 days after start of treatment to confirm sterilization of the urine. If cultures remain positive despite adequate therapy, the infant should be further evaluated for a potential reservoir of infection. Neonates are usually given intravenous antibiotics for the entire course, although older infants are often switched to oral antibiotics after demonstration of clinical improvement. If prenatal ultrasound data are not available, a renal ultrasound should be performed after the infant has clinically stabilized. Ultrasound can detect structural abnormalities, although it cannot detect vesicoureteral reflux or renal scarring. Voiding cystourethrogram is performed to detect vesicoureteral reflux, and this is usually done 3 to 6 weeks after completion of antibiotic treatment. If renal damage is suggested by ultrasound, renal cortical scintigraphy can be performed to better assess for renal scarring. In neonates, the most common route for infection to the bone or joint is by hematogenous spread. There are important differences in the pathophysiology of musculoskeletal infections in neonates compared with older children and adults. In all ages, metaphyses are susceptible to hematogenous seeding of infection because of the reduced rate of blood flow within metaphyseal blood vessels. In infants, secondary ossification centers have not yet formed, and their cartilaginous epiphyses are supplied with blood directly from metaphyseal blood vessels. Therefore, osteomyelitis in infants commonly leads to epiphyseal damage and joint infections. This contiguous infection rarely occurs in older children and adults with osteomyelitis because the epiphyses and metaphyses have separate blood supplies. Similarly, anatomic differences in the blood supply to the spinal column render neonates more susceptible to discitis than to vertebral body osteomyelitis. The signs and symptoms of osteomyelitis and joint infections in neonates are often subtle and similar to signs of sepsis. Some will show positional preference, lack of use of the involved extremity (pseudoparalysis), joint or limb swelling, or pain with passive motion as with diaper changes. If left untreated, septic arthritis of the hip can lead to spontaneous drainage along the internal obturator muscle, resulting in a lower abdominal mass just above the inguinal canal. Imaging studies should be obtained for any patient with suspected osteomyelitis or septic arthritis. Findings can include deep soft tissue swelling, widening of the joint space or joint dislocation, osteoporosis, periosteal new bone formation, and bony destruction. Bony changes, however, are not apparent until 7 to 10 days after onset of infection. For this reason, further imaging is often required for patients in whom there is a high index of suspicion. Ultrasound can detect subperiosteal collections and joint effusions, so it is very useful in cases of suspected septic arthritis.
This increase in the capacity of the pulmonary arteries also indicates that vascular constriction must play a strategic role in maintaining high pulmonary vascular tone during fetal life bipolar depression checklist order zyban overnight delivery. Numerous local growth and transcription factors regulate fetal lung vascular growth anxiety 9 months postpartum 150 mg zyban buy free shipping, many of which are favored by the low-oxygen intrauterine environment depression or bipolar purchase zyban with american express. Endodermal lung buds arise from the ventral aspect of the foregut by the fifth week of gestation depression definition causes generic 150 mg zyban mastercard. The pulmonary trunk anxiety jaw muscle tension proven 150 mg zyban, derived from the truncus arteriosus, divides into the aorta and pulmonary trunks by 8 weeks of gestation by growth of the spiral aortopulmonary septum. In the human lung, the pre-acinar vascular branching pattern is present by the 20th week of fetal life. Vasculogenesis is the de novo organization of blood vessels produced by the migration and differentiation of angioblasts or endothelial progenitor cells. These angioblasts migrate, adhere, and form vascular tubes that become arteries, veins, or lymphatics depending on the local growth factors within the mesenchyme. Because the placenta serves as the organ of gas exchange, most of the fetal right ventricular output bypasses the lung via the foramen ovale and the ductus arteriosus, and is directed to the systemic circulation. Pulmonary pressures are equivalent to systemic pressures because of elevated pulmonary vascular resistance, and only approximately 10% of the combined ventricular output is directed to the pulmonary vascular bed. Multiple mechanisms maintain high pulmonary vascular resistance and low pulmonary blood flow in the fetus, including low oxygen tension, low basal production of vasodilator products. The fetal pulmonary circulation also exhibits a marked "myogenic response" as gestation progresses, meaning that the vasculature responds to vasodilatory stimuli with active vasoconstriction. For example, maternal hyperoxygenation activates endothelial nitric oxide synthase and increases pulmonary blood flow to postnatal levels in fetal lambs. Although it is assumed that vasoconstrictors help maintain high pulmonary vascular tone in utero, surprisingly little is known about their specific roles throughout gestation. Some of the proposed fetal pulmonary vasoconstrictors include endothelin-1 and vasoconstrictor products of arachidonic acid metabolism such as thromboxane and leukotrienes. Hypoxia activates RhoA, which increases Ca2+ sensitivity of the contractile myofilaments in the vascular smooth muscle. A rapid and dramatic decrease in pulmonary vascular resistance allows half of the combined ventricular output to be redirected from the placenta to the lung, leading to an eight- to tenfold increase in pulmonary blood flow. This increase in pulmonary blood flow increases pulmonary venous return and left atrial pressure, promoting functional closure of the one-way valve of the foramen ovale. Systemic vascular resistance also increases at birth, in large part owing to removal of the low-resistance vascular bed of the placenta. As pulmonary vascular resistance drops and oxygen tension rises, blood flow through the patent ductus arteriosus reverses and the ductus arteriosus functionally closes. Mechanical distention of the lungs initiates the process of rapid structural adaptation of the pulmonary vessels. There is an increase in cell length and surface-tovolume ratio as the cells "spread" within the vessel wall to increase lumen diameter and lower resistance. In postmortem arterial-injected specimens, the number of nonmuscular arteries that fill with injection material increases rapidly during the first 24 hours, suggesting that there is a rapid increase in the number of precapillary arteries "recruited" into the pulmonary circulation after birth. This oxygen response emerges at approximately 70% gestation in the fetal lamb and continues to develop as gestation progresses. Cyclooxygenase-1 in particular is upregulated during late gestation, leading to an increase in prostacyclin production in late gestation and early postnatal life. Potential causes of antenatal remodeling of the pulmonary vasculature are strategic environmental exposures or genetic risk factors. In animal studies, newborn rats exposed in utero to fluoxetine developed pulmonary vascular remodeling, abnormal oxygenation, and higher mortality when compared with vehicle-treated controls. An increase in reactive oxygen species such as superoxide and hydrogen peroxide in the smooth muscle and adventitia of pulmonary arteries has been demonstrated in neonatal animal models of pulmonary hypertension. Congenital diaphragmatic hernia includes abnormal diaphragm development, herniation of abdominal viscera into the chest, and a variable degree of lung hypoplasia. Herniation occurs most often in the posterolateral segments of the diaphragm, and 80% of the defects occur on the left side. A similar developmental arrest occurs in pulmonary arterial branching, resulting in reduced cross-sectional area of the pulmonary vascular bed, thickened media and adventitia of small arterioles, and abnormal medial muscular hypertrophy extending distally to the level of the acinar arterioles. Some infants may have exceptionally severe left ventricular dysfunction that leads to dependence on the right ventricle for systemic perfusion; this subset may benefit from clinical strategies that maintain patency of the ductus arteriosus. Risk factors for pulmonary hypertension include extremely low gestational age, small for gestational age, oligohydramnios, duration of mechanical ventilation, and prolonged oxygen therapy. Pulmonary hypertension persisted to discharge in the majority of the infants, and was associated with longer hospitalization times and higher mortality. Alveolar capillary dysplasia remains universally fatal despite treatment with all known modalities, including extracorporeal support. The diagnosis can only be made with certainty based on microscopic examination of the lung. Surfactant protein B deficiency has been reported most commonly, and is characterized by early presentation, radiographic findings of ground-glass opacities, progressive respiratory failure, and early death. Clinical Therapy of Persistent Pulmonary Hypertension of the Newborn Persistent pulmonary hypertension of the newborn presents with labile oxygenation, differential saturation (higher SpO2 in the right upper extremity compared with a lower extremity), or profound hypoxemia despite oxygen and mechanical ventilation. Echocardiography also determines whether left ventricular insufficiency is present, which could trigger pulmonary venous hypertension that would only be aggravated by a pulmonary vasodilator. Systemic blood pressure should be maintained at normal levels for age with volume and cardiotonic therapy, with the primary goal to optimize left and right ventricular function and enhance systemic O2 transport. An "inodilator" such as milrinone may improve left ventricular function and reduce pulmonary venous hypertension, both of which may improve pulmonary blood flow and oxygenation in infants with refractory hypoxemic respiratory failure. However, hyperoxia may also exaggerate oxidative stress, increase pulmonary vascular contractility, and impair the pulmonary dilator response to nitric oxide. Alkalosis induced by hyperventilation or infusion of sodium bicarbonate was frequently employed prior to the approval of inhaled nitric oxide. Prolonged alkalosis may paradoxically worsen pulmonary vascular tone, reactivity, and permeability edema,129 and it may produce cerebral constriction, reduced cerebral blood flow, and worse neurodevelopmental outcomes. The registry maintained by the Extracorporeal Life Support Organization facilitates sharing of data and supports decision making for individual patients (see Chapter 78). Doses greater than 20 ppm provide no benefit and increase the risk of methemoglobinemia and other complications. The use of enteral sildenafil was reported in a small, randomized, controlled trial that showed a dramatic improvement in oxygenation and survival. Postdischarge medical problems for the first year of life include a greater than 25% incidence of reactive airways disease and a 15% to 20% incidence of significant feeding difficulty and/or poor weight gain (<fifth percentile for age). Current investigations are focusing on newer prostacyclin analogues specifically designed for inhalation, such as iloprost or treprostinil. Neurodevelopmental disability rates are similar in infants with moderate versus severe hypoxemic respiratory failure,153 and no therapy to date has been demonstrated to improve developmental outcomes. Serial screening for late sensorineural hearing loss is mandatory, as its prevalence is 6% to 10% and will persist through school age. Lung vascular development: implications for the pathogenesis of bronchopulmonary dysplasia. Intrapulmonary arterial development during fetal life: branching pattern and structure. Prenatal origins of human intrapulmonary arteries: formation and smooth muscle maturation. Control mechanisms of lung alveolar development and their disorders in bronchopulmonary dysplasia. Hypoxia-inducible factor-1alpha in pulmonary artery smooth muscle cells lowers vascular tone by decreasing Myosin light chain phosphorylation. Mild hypoxia impairs alveolarization in the endothelial nitric oxide synthase-deficient mouse. Reactivity of the human fetal pulmonary circulation to maternal hyperoxygenation increases during the second half of pregnancy: a randomized study. Increasing oxygen tension dilates fetal pulmonary circulation via endothelium-derived relaxing factor. Physiologic characterization of endothelin A and B receptor activity in the ovine fetal pulmonary circulation. Pulmonary vascular effects of serotonin and selective serotonin reuptake inhibitors in the late-gestation ovine fetus. Rho kinase activation maintains high pulmonary vascular resistance in the ovine fetal lung. Rho kinase modulates postnatal adaptation of the pulmonary circulation through separate effects on pulmonary artery endothelial and smooth muscle cells. Endothelium-derived nitric oxide plays a larger role in pulmonary veins than in arteries of newborn lambs. Developmental differences in endotheliumdependent responses in isolated ovine pulmonary arteries and veins. Role of venoconstriction in thromboxaneinduced pulmonary hypertension and edema in lambs. Human postnatal pulmonary arterial remodeling: ultrastructural studies of smooth muscle cell and connective tissue maturation. Rac and Rho play opposing roles in the regulation of hypoxia/reoxygenation-induced permeability changes in pulmonary artery endothelial cells. Acute effects of partial compression of ductus arteriosus on fetal pulmonary circulation. Intracellular pH and tyrosine phosphorylation but not calcium determine shear stress-induced nitric oxide production in native endothelial cells. Role of endothelium-derived relaxing factor during transition of pulmonary circulation at birth. Chronic nitric oxide inhibition in utero produces persistent pulmonary hypertension in newborn lambs. Prostacyclin synthesis in ovine pulmonary artery is developmentally regulated by changes in cyclooxygenase-1 gene expression. Effect of indomethacin on pulmonary vascular response to ventilation of fetal goats. Serum salicylate levels and right-to-left ductus shunts in newborn infants with persistent pulmonary hypertension. Analysis of nonsteroidal antiinflammatory drugs in meconium and its relation to persistent pulmonary hypertension of the newborn. Persistent pulmonary hypertension of the newborn and smoking and aspirin and nonsteroidal antiinflammatory drug consumption during pregnancy. Nonsteroidal antiinflammatory drugs in late pregnancy and persistent pulmonary hypertension of the newborn. Maternal use of selective serotonin re-uptake inhibitors and persistent pulmonary hypertension of the newborn. Antidepressant medication use and risk of persistent pulmonary hypertension of the newborn. Congenital heart disease associated with selective serotonin reuptake inhibitor use during pregnancy. Persistent pulmonary hypertension of the newborn is associated with mode of delivery and not with maternal use of selective serotonin reuptake inhibitors. Persistent pulmonary hypertension of the newborn and selective serotonin reuptake inhibitors: lessons from clinical and translational studies. Clinical characteristics and follow up of Down syndrome infants without congenital heart disease who presented with persistent pulmonary hypertension of newborn. Increased incidence of idiopathic persistent pulmonary hypertension in Down syndrome neonates. Prevalence of congenital heart defects and persistent pulmonary hypertension of the neonate with Down syndrome. International experience with trisomy 21 infants placed on extracorporeal membrane oxygenation. Betamethasone attenuates oxidant stress in endothelial cells from fetal lambs with persistent pulmonary hypertension. Chronic intrauterine pulmonary hypertension impairs endothelial nitric oxide synthase in the ovine fetus. Decreased gene expression of endothelial nitric oxide synthase in newborns with persistent pulmonary hypertension. Pulmonary hypertension alters soluble guanylate cyclase activity and expression in pulmonary arteries isolated from fetal lambs. Increased hydrogen peroxide downregulates soluble guanylate cyclase in the lungs of lambs with persistent pulmonary hypertension of the newborn. Superoxide dismutase and inhaled nitric oxide normalize phosphodiesterase 5 expression and activity in neonatal lambs with persistent pulmonary hypertension. Prostacyclin production and mediation of adenylate cyclase activity in the pulmonary artery: alterations after prolonged hypoxia in the rat. Thromboxane inhibition reduces an early stage of chronic hypoxia-induced pulmonary hypertension in piglets. Plasma immunoreactive endothelin-1 concentrations in infants with persistent pulmonary hypertension of the newborn. Elevated immunoreactive endothelin-1 levels in newborn infants with persistent pulmonary hypertension. Role for Endothelin-1nduced superoxide and peroxynitrite production in rebound pulmonary hypertension associated with inhaled nitric oxide therapy. L-Citrulline ameliorates chronic hypoxia-induced pulmonary hypertension in newborn piglets.
Hypocalcemia owing to high-phosphate infant formula has been previously cited as a cause of late-onset seizures anxiety uncertainty management theory cheap zyban 150 mg amex. Rarely depression ribbon 150 mg zyban overnight delivery, congenital hypoparathyroidism in association with other genetic abnormalities such as DiGeorge syndrome anxiety and chest pain buy zyban on line. These infants may have severe congenital heart disease as well as a hypoparathyroid state with hypocalcemia and hypomagnesemia that precipitates seizures depression fallout purchase zyban australia. Hyponatremia and Hypernatremia Hyponatremia is a metabolic disturbance that may result from inappropriate secretion of antidiuretic hormone after severe brain trauma depression after divorce buy discount zyban on line, infection, or asphyxia,107 but is an uncommon isolated cause of neonatal seizures (see Chapter 44). Although intraventricular or periventricular hemorrhage may occur in otherwise asymptomatic infants, the neonate with a catastrophic deterioration of clinical status shows signs of apnea, bulging fontanelle, hypertonia, and seizures. Other sites of intracranial hemorrhage that may cause seizures include within the subarachnoid space, but that is usually associated with a more favorable outcome. Subdural hematoma, whether spontaneous or with craniocerebral trauma, should always be considered, particularly when focal trauma to the face, scalp, or head has occurred; simultaneous occurrences of cerebral contusion and infarction should also be considered. Cerebral infarction has been described in neonates with seizures and can result from events during the antepartum, intrapartum, or neonatal periods (see Chapters 59 and 60). Either preterm or term neonates with infarction may also present without seizure expression. Destructive lesions such as porencephaly require approximately 5 to 7 days before appearing radiographically. Radiographic documentation of brain lesions needs to be obtained before beginning extracorporeal membrane oxygenation because the anticoagulation required for this procedure may convert "bland" or ischemic infarctions to hemorrhagic forms, with greater risk for cerebral edema and herniation. Venous infarction in the deep white matter of the preterm brain also occurs in association with intraventricular hemorrhage. Other congenital infections include those caused by enteroviruses and parvoviruses. Increasing lethargy and obtundation with or without seizures may suggest the subacute presentation of encephalitis during the postnatal period. Serial spinal fluid analyses document progressively increasing protein or pleocytosis. Bacterial infections acquired in utero or postnatally from either gram-negative or gram-positive organisms are also associated with neonatal seizures. Some organisms such as Escherichia coli, group B streptococci, Listeria monocytogenes, and mycoplasmas may produce severe leptomeningeal infiltration, with possible abscess formation and cerebrovascular occlusions. Seizures may result in the newborn with malformations who experiences stress around the time of birth,71 which presumably lowers seizure thresholds. Brain anomalies may occur as a result of either genetic causes from conception or acquired defects during the first half of gestation. Specific dysgenesis syndromes, such as holoprosencephaly and lissencephaly, are often associated with characteristic facial or body anomalies. Unfortunately, infants may also lack physical clues to the presence of a brain malformation. Nine percent of 356 infants presenting with neonatal seizures had brain malformations. Focal or regional brain malformations are rare causes of early-onset epilepsy in neonates and young infants3; functional imaging studies such as positron emission tomography scans18 may identify localized areas of altered brain metabolism, which can assist in a neurosurgical approach to seizure management, even in young children who fail to respond to antiepileptic drug maintenance. Dysplastic or destructive brain lesions, as documented on neuroimaging, may be associated with specific biochemical defects, such as glycine encephalopathy or branched-chain aminoacidopathies. Pregnancy, labor, and delivery histories for these infants are commonly uneventful. The emergence of feeding intolerance as well as increasing lethargy, stupor, coma, and seizures is an early indication of an inborn metabolic disturbance during the first few days of life. The newborn with an inherited metabolic disorder may initially present as a neurologically depressed and hypotonic child with asphyxia and seizures. Some children respond to specific dietary therapies, including vitamin supplementation, depending on the enzymatic defect. Specific urea cycle defects, such as ornithine transcarbamylase or carbamoyl phosphate synthetase deficiency, may present with coma and seizures during the first 2 days of life, with marked elevations in plasma ammonia levels. These infants may respond to aggressive treatment with an exchange transfusion, dialysis, and appropriate dietary adjustments. Prophylactic doses of pyridoxine may be needed to achieve and maintain seizure control. Other rare causes of seizures include disorders of carbohydrate metabolism with coincident hypoglycemia,54 as well as peroxisomal disorders, such as neonatal adrenoleukodystrophy or Zellweger syndrome. A defect in a glucose transporter protein necessary to move glucose across the blood-brain barrier has also been reported, which results in hypoglycorrhachia and seizures. Molybdenum cofactor deficiency and isolated sulfite oxidase deficiencies are other rare metabolic defects that cause neonatal seizures and associated destructive changes on neuroimaging, which may resemble cerebrovascular disease or asphyxial insults. Certain drugs, such as short-acting barbiturates, may be associated with seizures within the first several days of life. Seizures may occur directly after substance withdrawal, or be associated with longer-standing uteroplacental insufficiency promoted by chronic substance use and poor prenatal health maintenance by the mother. Careful review of placental-cord specimens may reveal chronic or acute lesions that contribute to antepartum or intrauterine asphyxia. Inadvertent fetal injection with a local anesthetic agent during delivery may induce intoxication, which is a rare cause of seizures. Patients present during the first 6 to 8 hours of life with apnea, bradycardia, and hypotonia, and are comatose, without brainstem reflexes. Determination of plasma levels of the suspected anesthetic agent establishes the diagnosis. Treatment consists of ventilatory support and removing the drug by therapeutic diuresis, acidification of the urine, or exchange transfusion. Rarely, neonates with idiopathic localization-related or partial seizures without neuroimaging abnormalities present with intractable epilepsy. Neurocutaneous syndromes, such as incontinentia pigmenti and tuberous sclerosis, may also present during the neonatal period with symptomatic epilepsy as one clinical manifestation of these genetic disorders (see Chapter 102). Incontinentia pigmenti is accompanied by a vesicular crusting rash that initially mimics a herpetic infection. Two common fetal presentations of tuberous sclerosis are a cardiac tumor, usually a rhabdomyoma, or rarely a connatal brain tumor, both noted on fetal sonography. Neonatal seizures also may be the presenting feature,60 with documentation of intracranial lesions on postnatal neuroimaging. Exposure to barbiturates, alcohol, heroin, cocaine, or methadone commonly presents with neurologic findings that include tremors and irritability (see Chapter 53). Response to antiepileptic medication is usually good, although some authors describe variable success. Further studies are needed to clarify the relationship between phenotypic and genotypic expressions of this disorder. Seizures in neonates after asphyxia support either acute intrapartum events or antepartum disease processes. The child with seizures may also express clinical and laboratory signs of evolving cerebral edema. The presence of a bulging fontanelle with neuroimaging evidence of increased intracranial pressure and cerebral edema. Hyponatremia and increased urine osmolality suggest the syndrome of inappropriate secretion of antidiuretic hormone accompanying acute or subacute cerebral edema. Alternatively, failure to document evolving cerebral edema during the first 3 days after asphyxia, or documentation of encephalomalacia or cystic brain lesions on neuroimaging shortly after birth. Liquefaction necrosis requires 2 weeks or longer after the presumed in utero asphyxial event to produce a cystic cavity, which is then visible on neuroimaging. Isolated seizures in an otherwise asymptomatic neonate can suggest a disease process occurring during either the postnatal or antepartum periods. Neonates present with seizures as a result of postnatal illnesses from intracranial infection, cardiovascular lesions, drug toxicity, or inherited metabolic diseases. Children with antepartum injury may express isolated seizures after in utero cerebrovascular injury on the basis of thrombolytic or embolic disease of the mother, placenta, or fetus. Fetal injury also may occur after ischemiahypoperfusion events from circulatory disturbances, such as maternal shock, chorioamnionitis, or placental-fetal vasculopathy. Neonatal expression of seizures may reflect recent physiologic stress during parturition, which lowers seizure threshold in susceptible brain regions that have been previously damaged. Spinal fluid analyses include cell count, protein, glucose, lactate, pyruvate, amino acids, and culture studies to consider central nervous system infection, intracranial hemorrhage, and metabolic disease. Metabolic acidosis on serial arterial blood gas determinations may alternatively suggest an inherited metabolic disease, particularly if intrapartum asphyxia was not judged to be severe. Absence of multiorgan dysfunction may alert the clinician to other etiologies for seizures besides intrapartum asphyxia. Signs of chronic in utero stress such as growth restriction, early hypertonicity after neonatal depression, joint contractures, or elevated nucleated red blood cell values all suggest longer-standing antepartum stress to the fetus. Identification of genetic or syndromic conditions can contribute to the expression of neonatal encephalopathies independent of asphyxial injury. Lysosomal enzyme studies are also occasionally considered to diagnose specific enzymatic deficiencies in children with neonatal seizures (see Chapter 99). Treatment Rapid infusion of glucose or other supplemental electrolytes should be initiated before antiepileptic medications are considered. Serum magnesium concentrations should also be measured because hypomagnesemia may accompany hypocalcemia; 0. If the decision to treat neonates with antiepileptic medications is reached, important questions must be addressed with respect to who should be treated, when to begin treatment, which drug to use, and for how long neonates should be treated. Some authors suggest that only neonates with clinical seizures should receive medications; brief electrographic seizures need not be treated. The half-life of phenobarbital ranges from 45 to 173 hours in the neonate; the initial loading dose is recommended at 20 mg/kg, with a maintenance dose of 3 to 4 mg/kg per day. Therapeutic levels are usually suggested to range from 10 to 40 mg/ mL, although there is no consensus with respect to drug maintenance. Therapeutic hypothermia may elevate phenobarbital blood levels and prolong the half-life. One study suggests a half-life of 54 hours in preterm infants to 18 hours in term infants. Diazepam is highly protein bound and displacement of bilirubin from albumin is possible. Deposition into muscle precludes its use as a maintenance antiepileptic medication because profound hypotonia and respiratory depression may result, particularly if barbiturates have also been administered. Although it has no known drug interactions and is excreted by the kidney, the pharmacokinetics and safety profile are unknown; however, the half-life is longer than that of the adult at approximately 18 hours. A starting loading dose is 20 mg/ kg but as much as 60 mg/kg loading dose has been reported before seizures are lessened or controlled. Mechanisms of seizure generation, propagation, and termination are different during early brain development as compared with more mature ages. These strategies have different rationales: (1) provide single or combination therapies focused on the signaling pathways for a specific etiology of brain disorder. Single/Synergistic Treatments for General Neonatal Disease States One class of medications is the N-methyl-D-aspartate antagonists, such as topiramate,43 useful in the treatment of asphyxia and stroke since this drug reduces the excitatory and harmful effects of extracellular glutamate. Combination therapies such as therapeutic hypothermia with topiramate further lessen the severity of brain injury after stroke in a rodent model. Such an approach suggests that treatment of the underlying cause with single or synergistic drugs may indirectly reduce the risk for seizures by reducing brain injury and, therefore, treating the underlying cause for neonatal seizures. A variety of experimental models of asphyxia-induced seizure activity in immature brain animals have indicated a certain degree of efficacy with these drugs. Such models provide data regarding pharmacologic and physiologic characteristics of neuronal responses after an asphyxial stress, which causes excessive release of excitotoxic neurotransmitters38 such as glutamate. The administration of this drug to neonatal rats who sustained global hypoxic injury both acutely suppressed seizures in a dose-dependent manner and also prevented later life apoptosis in the adult animals. Such an experimental drug represents more comprehensive neuroprotective treatment by addressing both antiepileptogenic as well as anticonvulsant actions in the immature brain that sustained injury. Treatments That Alter Neurotransmission Another therapeutic approach considers drugs that alter neurotransmission in the immature neuron to reduce seizure risk. This rearrangement of membrane receptors occurs over the first few months of life. Bumetanide reduces kainicinduced seizures in neonatal, but not adult, rats, and burst firing in hippocampus slices. Some claim that this particular diuretic can be safely used for the neonate, although its long-term safety profile needs to be better studied. It has also been recently suggested that pharmacologic agents that can diminish bursting behavior in neonatal neurons can add an additional level to the control of seizures. This supports the use of this agent as a potential antiepileptic medication in this age group. One needs to also establish that these agents can reach the brain in appropriate concentrations and lack short- as well as long-term adverse effects. A specific etiology may alter seizure threshold by epigenetic modification, changing the specific genetic variability within individuals. This generalization is further complicated by the timing and specific brain region of damage that may have occurred remotely during the antepartum as opposed to the intrapartum or neonatal periods, and selectively affected deep gray matter as well as neocortical structures. Drug binding in neonates with seizures has only recently been reported, and can be altered in a sick neonate with organ dysfunction. Toxic side effects may result from elevated free fractions of a drug, which adversely affect cardiovascular and respiratory function. Discontinuation of drugs before discharge from the neonatal unit is usually recommended so that clinical assessments of arousal, tone, and behavior will not be hampered by medication effect. However, newborns with congenital or destructive brain lesions on neuroimaging, or those with persistently abnormal results on neurologic examinations at the time of discharge, may suggest to the clinician that a slower tapering of medication is required over several weeks or months. Neonatal seizures rarely reoccur during the first 2 years of life, and prophylactic antiepileptic drug administration need not be maintained past 3 months of age, even in the child at risk.
In addition anxiety foods zyban 150 mg purchase on-line, trophic or minimal enteral feedings (10-20 mL/kg per day) should be initiated with expressed human milk as soon as possible after birth mood disorder pathophysiology purchase zyban online. Strategies related to the advancement of enteral feeds and weaning of parenteral nutrition will be discussed subsequently depression levels buy zyban online from canada. When neonatal amino acid solutions became available anxiety disorder nos purchase zyban 150 mg free shipping, many physicians chose to use parenteral nutrition exclusively in sick preterm infants because of concerns about necrotizing enterocolitis depression kidshealth order zyban 150 mg visa. Parenteral nutrition was thought to be a logical continuation of the transplacental nutrition the infants would have received in utero. However, this view discounts any role that swallowed amniotic fluid may play in nutrition and in the development of the gastrointestinal tract. In fact, by the end of the third trimester, amniotic fluid provides the fetus with the same enteral volume intake and approximately 25% of the enteral protein intake of a term breastfed infant. Provision of Nutritional Support the extremely premature neonate is born with glucose stores of only 200 kcal and loses 1% of body protein per day when provided with intravenous glucose alone. A number of observational studies have described the influence of nutritional practices on growth and have found that differences in caloric and protein intake in the first weeks account for the largest difference in growth among premature infants. This section reviews the basis of recommendations for nutritional support of premature infants. Minimal Enteral Feeding Trophic or minimal enteral feedings involve hypocaloric, low-volume (typically 24 mL/kg per day) feeds to promote intestinal maturation and do not contain sufficient calories to sustain somatic growth. Proposed benefits include maturation of the preterm intestine (both structurally and functionally), reduced liver dysfunction, and improved feeding tolerance. In a neonatal piglet model, at least 40% of total nutrient intake supplied enterally is needed to sustain normal gastrointestinal growth. Initiation of enteral nutrition is often delayed in premature infants with intrauterine growth restriction because of the concern that these infants are at an increased risk of necrotizing enterocolitis. However, a recent randomized trial evaluated early versus delayed initiation of enteral feeding for preterm growth-restricted infants and found no evidence of a difference in the incidence of necrotizing enterocolitis between groups. Consequently, the authors concluded that there was no evidence of benefit in delaying the introduction of minimal enteral feeds in preterm infants with intrauterine growth restriction beyond 24 to 48 hours of age. Although a large multicenter trial that more clearly evaluates early feeding may be desirable, such a trial appears unlikely. Standardized Feeding Guidelines Enteral feeding practices vary considerably among different centers. In addition, standardized feeding guidelines, regardless of the content of the guideline, have been shown to reduce the incidence of necrotizing enterocolitis in premature infants. Despite differences in study populations and composition of amino acid solutions, all studies demonstrated positive nitrogen balance in response to parenteral amino acids and improved protein balance with higher amino acid intake. Consequently, the initial goal of limiting catabolism and preserving endogenous protein stores in premature infants can be accomplished with provision of as little as 1. Stable isotope techniques have also been used to evaluate the effect of amino acids on protein metabolism in premature infants. In these studies, stable isotope tracers of one or more essential amino acids are used to reflect whole body protein kinetics. Thureen and colleagues conducted a randomized trial of low (1 g/kg per day) versus high (3 g/kg per day) amino acid intake in infants with extremely low birth weights immediately after birth. Infants in the control group received glucose alone on the first day of life, with a stepwise increase in amino acid intake thereafter (1. Infants who received amino acids on the first day of life were found to have positive nitrogen balance without any major adverse effects, whereas infants in the control Rate of Advancement of Enteral Feeds the rate at which enteral feedings should be advanced in preterm infants has also been the subject of much debate. Similar to the studies discussed previously, the higher amino acid dose resulted in greater improvement in nitrogen balance without evidence of adverse effects. In premature infants, rates of urea production are higher than in term neonates and adults, consistent with high rates of protein turnover and oxidation. Some investigators have even suggested that azotemia might be evidence of the effective utilization of amino acids as an energy supply rather than of protein intolerance, but this contention remains unproven. Although the initial goal of providing intravenous amino acids to premature infants to limit catabolism and preserve endogenous protein stores can be accomplished even if total caloric intake is low, ultimately, both protein and energy must be supplied in quantities sufficient to support optimal growth. This is true regardless of whether parenteral nutrition is used exclusively or as a bridge to full enteral feedings. In a series of studies, Zlotkin and colleagues evaluated the effect of intravenous energy and nitrogen intake on nitrogen retention. However, at low energy intake (~50 kcal/kg per day), increasing nitrogen intake from 494 to 655 mg/kg per day (3 to 4 g/kg of amino acids per day) had no effect on nitrogen retention or weight gain. However, at higher energy intakes (~80 kcal/kg per day), the same increase in nitrogen intake resulted in a significant increase in the rate of both nitrogen retention and weight gain. Many conditions and interventions commonly encountered in extremely premature infants are known to increase protein requirements. Underlying disease states such as sepsis or surgical stress increase catabolism and can negatively impact protein accretion. In addition medications such as systemic steroids, fentanyl, and insulin can also impact protein accretion. Dexamethasone has been shown to increase protein catabolism by increasing protein oxidation and proteolysis, resulting in decreased accretion of protein. Concerns about these first-generation solutions included high concentrations of glycine, glutamate, and aspartate; the presence of unwanted peptides; and high acidity. Reports of hyperammonemia and acidosis in the early 1970s were associated with the use of these first-generation solutions in neonates. Although amino acid solutions have been significantly modified, the perceived risks associated with the protein hydrolysates linger, contributing to the hesitancy by some clinicians to administer early parenteral amino acids. The amino acid pattern of these mixtures reflects that of high-quality dietary proteins with large amounts of glycine and alanine, absence of glutamate and aspartate, and absence or poor solubility of tyrosine and cysteine. The newest solutions include modifications of crystalline amino acids for use in pediatric patients. The currently available solutions include modifications of crystalline amino acids for use in pediatric and neonatal patients (Table 43-4). TrophAmine was originally formulated to match plasma amino acid concentrations of healthy term, breastfed infants; Premasol is identical in composition to TrophAmine. Cysteine is not supplied by most amino acid solutions because it is not stable for long periods of time in solution. However, cysteine hydrochloride can be added during the compounding process just prior to delivery of the solution. It is no surprise that the ideal composition of intravenous amino acid mixtures is unknown. Whether the goal should be to match amino acid concentrations of term, breastfed infants or some other standard is not known. Clearly, the ultimate goal is to achieve plasma amino acid concentrations in response to provision of parenteral nutrition that optimize both growth and neurodevelopment without toxicity. To optimize nutrition and growth, particularly in a premature infant, the requirements for specific amino acids need to be more precisely defined. Cysteine, tyrosine, and arginine are often considered conditionally essential amino acids for premature infants. Tyrosine is not present in appreciable amounts in currently available amino acid solutions because of its low solubility. Snyderman found lower rates of weight gain, nitrogen retention, and plasma concentrations of tyrosine in premature infants given a tyrosine-deficient diet. The activity of this enzyme in premature infants was thought to be inadequate for growth and nitrogen retention without tyrosine supplements. However, stable isotope studies have demonstrated active phenylalanine hydroxylation in very premature (26 weeks) and premature (32 weeks) infants. However, it remains unclear whether enough tyrosine can be endogenously produced from phenylalanine in premature infants to support normal rates of protein accretion. N-acetyl tyrosine, although currently added to TrophAmine, is not highly bioavailable. Nonetheless, several studies provide indirect evidence that N-acetyl tyrosine improves protein accretion in preterm infants. Cysteine may be a conditionally essential amino acid for premature infants, but is not contained in currently available amino acid solutions. Some studies have shown that the fetal liver lacks the enzyme system to convert methionine into cysteine and that infants on a cysteinefree diet demonstrate impaired growth and low plasma cysteine levels. Other studies have demonstrated that there is enough cystathionase in extrahepatic tissues of the fetus and premature infant to synthesize cysteine when an adequate amount of methionine is provided. Studies using stable isotope techniques have demonstrated active endogenous cysteine synthesis in low birth weight infants. However, it is important to note that cysteine hydrochloride supplements can produce metabolic acidosis unless appropriately buffered with acetate. Glutamine is one of the most abundant amino acids in both plasma and human milk, yet it is not supplied by currently available amino acid solutions because glutamine is unstable in aqueous solution. Glutamine is a major energy substrate for small intestinal mucosa, as proved by a high glutamine uptake from the lumen and from arterial blood during the newborn period in rats. Several studies suggest that parenteral glutamine supplementation is of benefit in selected populations of critically ill adults. It is present in large concentrations in the retina and brain of the fetus, reaching a peak concentration at birth. When newborn nonhuman primates are fed taurine-deficient formula, growth is depressed, but this does not occur in human preterm infants, despite declining plasma and urine taurine levels. Nevertheless, there is some limited evidence that taurine supplementation might influence auditory brainstem evoked responses. It is important to note that currently available amino acid solutions have not been modified for more than 20 years and that none were designed specifically to meet the needs of extremely premature infants. Future research efforts should be directed at designing a fourth generation of amino acid solutions to optimize amino acid nutrition provided to the most vulnerable infants. As discussed earlier in this chapter, rates of glucose production and utilization in term infants are approximately 3 to 5 mg/kg per minute, whereas an extremely premature infant has a much greater need, 8 to 9 mg/kg per minute. Infants who weigh 1000 g or more usually tolerate a 10% glucose solution initially, whereas infants weighing less than 1000 g probably need to be started on a 5% glucose solution, given their higher total fluid requirements and predisposition toward hyperglycemia. The definition of hyperglycemia also varies but is generally set at a plasma level above 150 mg/dL (8. Alternatively, a lower concentration of dextrose solution can be used, although solutions less than 2. The appropriate balance of glucose and lipid in parenteral nutrition is critical for achieving maximal nutritional benefit. In fact, nutrient and protein retention is maximal if the nonprotein caloric balance between carbohydrate and lipid is approximately 60: 40. This more closely mimics the fat content of breast milk and minimizes excess energy expenditure, which can occur if a disproportionate amount of nonprotein calories is given as glucose. Even at higher protein intakes, a parenterally fed infant with extremely low birth weight may need 80 to 90 kcal/kg per day for nonprotein energy supplies. The caloric requirements of a parenterally fed neonate are much lower than those fed enterally. It is important to realize that providing excessive calories via parenteral nutrition does not correlate with higher rates of growth. In addition, it should be emphasized that it is not difficult to provide adequate nonprotein energy, and it can be done without using highly concentrated glucose solutions. They are made up of neutral triglycerides, egg yolk phospholipids to emulsify, and glycerol to adjust the tonicity. Emulsions containing fish oil provide a direct source of very long chain omega-3 fatty acids as docosahexaenoic acid and eicosapentaenoic acid. The early administration of intravenous lipids to preterm infants has been the subject of discussion and debate primarily centered on the acute metabolic effects of early intravenous lipids and potentially adverse effects, such as chronic lung disease and bilirubin toxicity as a result of free fatty acids displacing bilirubin from albumin binding sites. A meta-analysis found no increase in chronic lung disease resulting from early lipid administration to premature infants. Triglyceride concentrations are most often used as an indication of lipid tolerance, and maintaining triglyceride concentrations below 200 mg/dL seems prudent. Intravenous lipid emulsions may undergo lipid peroxidation, which may form organic free radicals and potentially initiate tissue injury. Light, especially phototherapy, may play some role in increasing lipid peroxidation in intravenous lipid emulsions. However, multivitamin preparations included in the intravenous solutions are a major contributor to a generation of peroxides, and lipid emulsions may have only a minor additive effect. Based on these studies, some clinicians protect intravenous lipid solutions from light, although the importance or efficacy of this practice is unclear. Lipid particles supplied by intravenous lipid solutions are similar in size to endogenously produced chylomicrons. Like chylomicrons, clearance of these lipid particles also depends on the activity of lipoprotein lipase. Heparin theoretically releases lipoprotein lipase from the endothelium into the circulation, but there is no evidence that this increases lipid utilization in preterm infants. In addition, increased lipoprotein lipase activity may produce high levels of free fatty acids and be in excess of the clearance capacity of the premature infant. Consequently, the routine addition of heparin to lipid emulsions for this purpose (to stimulate lipolysis) is not recommended on the basis of currently available evidence. Carnitine facilitates transport of long chain fatty acids through the myocardial membrane, and as such plays an important role in the oxidation of these long chain fatty acids. Premature infants receiving parenteral nutrition have low carnitine levels, but the clinical significance of this remains uncertain. A Cochrane review found no evidence to support the routine supplementation of parenterally fed neonates with carnitine. Human Milk Fortifiers Human milk does not completely meet the nutritional needs of premature infants; insufficient protein, calcium, phosphorus, sodium, zinc, vitamins, and possibly energy are provided by human milk to optimally support most premature infants. Human milk fortifiers have been developed to address many of these inadequacies (Tables 43-6 and 43-7).
The higher saturation indicates falling pulmonary vascular resistance and increasing pulmonary blood flow mood disorder versus bipolar cheap zyban 150 mg buy line. Lower saturations indicate increasing pulmonary vascular resistance mood disorder group activities purchase generic zyban on line, branch pulmonary artery stenosis depression symptoms noise buy generic zyban 150 mg on line, or pulmonary dysfunction from edema anxiety before work order zyban 150 mg fast delivery. Acidosis can be present in infants with associated truncal stenosis and regurgitation or aortic arch interruption anxiety workbook pdf purchase zyban in india. As the pulmonary vascular resistance drops, the pulmonary blood flow increases, resulting in a murmur and signs and symptoms of pulmonary overcirculation. Truncal valve stenosis and a regurgitation murmur also can be easily identified by a thorough physical examination. The patient may have bounding pulses and increased pulse pressure because decreased diastolic pressure is secondary to runoff into the branch pulmonary arteries. All of these patients should also be screened for the presence of a thymus, and their calcium levels should be measured. This single trunk overrides a large ventricular septal defect that allows for mixing of the systemic venous return and pulmonary venous return. In type I truncus there is a short main pulmonary artery segment arising from the truncus, which then gives rise to branch pulmonary arteries. Both pulmonary and systemic blood flows are determined by the relative systemic vascular resistance and pulmonary vascular resistance. As the pulmonary vascular resistance falls, there tends to be increased pulmonary blood flow, which then results in pulmonary venous overcirculation and increased left atrial and left ventricular size. Laboratory Evaluation An electrocardiogram may show biventricular hypertrophy or may be normal; however, a chest x-ray shows cardiomegaly and pulmonary overcirculation. While performing the echocardiogram, attention must be paid to define the truncal valve, branch pulmonary arteries, aortic arch anatomy, and coronary arteries. Management and Prognosis In patients with truncus arteriosus, increased pulmonary blood flow generally responds to anticongestive measures such as diuretics and digoxin. Supplemental oxygen should be avoided because this decreases the pulmonary vascular resistance, which increases pulmonary blood flow. Those with moderate to severe truncal valve stenosis and regurgitation generally do not respond to medical management and require balloon dilation or surgical repair. In those neonates with DiGeorge syndrome, careful management of calcium levels is required. Associated Defects A number of other intracardiac defects are associated with truncus arteriosus. This repair includes closure of the ventricular septal defect and placement of a right ventricle to pulmonary artery homograft. Associated defects, including truncal valve stenosis, aortic arch interruption, coronary abnormalities, and branch pulmonary artery atresia, increase the risk of the procedure but do not preclude it. The long-term prognosis for this repair is excellent for children with straightforward truncus arteriosus. In this disorder, there must be complete mixing of the systemic and pulmonary venous return to allow for adequate single-ventricle output. The blood from this single ventricle is pumped either to the systemic or pulmonary circulation. The predominant circulation must then support the other through a patent ductus arteriosus. The oxygen saturation in these cases is determined by the relative resistances across the pulmonary and systemic vascular beds. It is important to recognize that many babies have lower pulmonary vascular resistance, resulting in unrestricted pulmonary blood flow. Oxygen acts as a pulmonary vasodilator and therefore increases pulmonary blood flow, thus reducing systemic blood flow, resulting in acidosis and hepatic and renal shutdown. When single-ventricle physiology is determined, the next step is to determine whether the pulmonary or systemic circulation requires support. If the neonate has single-ventricle physiology, then a Norwood surgery is planned with additional variations, including the DamusKaye-Stansel procedure as required. The Norwood procedure is then followed by a bidirectional Glenn procedure (anastomosing the superior vena cava to the branch pulmonary arteries) between 3 and 9 months of age. At this stage, the pulmonary and systemic the most important associated defect is pulmonary and subpulmonary stenosis. Clinical Presentation At presentation, double-outlet right ventricle usually is manifested by neonatal cyanosis and/or murmurs. The relationship of the great arteries to each other and presence of pulmonary stenosis should be easily identified. Mild to moderate aortic valve stenosis is well tolerated in utero, generally resulting in left ventricular hypertrophy. The pulse oximetry differential between the upper extremity and lower extremity may suggest a right-to-left shunt at the level of the duct. Arterial blood gas and electrolyte measurements can be followed to indicate tissue perfusion. Associated Defects Mild aortic stenosis can be accompanied by a large patent ductus arteriosus, which may exaggerate the pressure gradient across the aortic valve because of overcirculated pulmonary blood flow. If it is present, it should raise the possibility of a tunnel from the left ventricle to the aorta. Management and Prognosis Mild aortic stenosis is well tolerated, and no immediate intervention is necessary other than outpatient follow-up. Moderate to severe aortic stenosis can progress in the first few months of life, and careful follow-up is needed. Any indication of congestive heart failure or ventricular dysfunction in an infant with severe aortic stenosis is an indication for balloon or surgical valvotomy. Critical aortic stenosis is a neonatal emergency and continues to result in relatively high morbidity and mortality. Success rates with neonatal balloon valvuloplasty have been good and acceptable when faced with the alternative of surgery, but it does have a significant downfall with residual stenosis, creation of aortic regurgitation, and the need for a redo procedure. The selection of babies with borderline criteria for a two-ventricle approach remains controversial and challenging. Based on cardiac output and severity of the aortic stenosis, there are varying degrees of a systolic ejection murmur radiating to the neck. With critical aortic stenosis, as long as the ductus arteriosus is patent, the physiology is similar to hypoplastic left heart syndrome. When the ductus arteriosus closes, these patients exhibit signs of cardiovascular shock, acidosis, and multiorgan failure. Laboratory Evaluation Because the severity of neonatal aortic stenosis is difficult to assess clinically, careful noninvasive assessment is essential. In type B, the interruption occurs between the left common carotid artery and left subclavian artery. In type C, the interruption occurs between the right and the left common carotid arteries. The presence of an aberrant right subclavian artery (the origin of the right subclavian artery from the descending aorta distal to the left subclavian artery) may occur with both coarctation of the aorta and interruption. Coarctation of the aorta presents an increased afterload to the left ventricle, resulting in left ventricular hypertrophy and hypertension. The ductus arteriosus therefore is critical to survival in these babies because it allows for perfusion of the descending aorta and the lower body from the pulmonary artery. The true severity in these juxtaductal types of coarctation of the aorta is usually best revealed when the ductus arteriosus closes. The neonatal coarctation is also unique in its involvement of the right ventricle because of the afterload and ventricular interaction to which it is subjected. Bicuspid aortic valve and ventricular septal defect are common isolated associated defects. Other associated lesions include aortopulmonary window, truncus arteriosus, or transposition of the great arteries. The ventricular septal defect can be malaligned (posterior deviation of the conal septum) and can cause subaortic obstruction. Partial or complete DiGeorge syndrome or microdeletion of chromosome 22 is found in association with aortic arch interruption and occasionally in association with coarctation of the aorta. Laboratory Evaluation the electrocardiogram and chest radiograph of a neonate with coarctation of the aorta or aortic arch interruption are usually normal. Significant cardiomegaly suggests associated lesions or ventricular dilation or dysfunction after the ductus arteriosus closes. Echocardiography defines the arch with considerable accuracy, although predicting the severity of the coarctation with the ductus arteriosus open can be difficult. Abdominal aortic pulsatility when the ductus arteriosus has closed is a good indicator of the severity of the coarctation. Clinically significant neonatal coarctation also results in moderate to severe right heart dysfunction. Right-to-left shunting at the ductal level is an important sign of significant obstruction. Transverse arch hypoplasia, especially with a long segment between the left carotid and left subclavian arteries, also suggests a significant coarctation of the aorta. Pulse oximetry and arterial blood gas measurements in the upper and lower extremities can confirm ductal shunting and perfusion. Clinical Presentation Symptom-free newborn infants who have diminished leg pulses on routine discharge examination have mild coarctation of the aorta and usually no associated aortic valve stenosis or septal defects. Early signs and symptoms of congestive heart failure should raise concern about the presence of associated defects. Careful palpation of all pulses, including the neck, can provide valuable anatomic data. The pulse discrepancy should be confirmed by blood pressure measurement in both arms and both legs. Precordial hyperactivity, a single second heart sound, a gallop rhythm, and hepatomegaly indicate significant obstruction or associated defects. Holosystolic murmurs suggest either a ventricular septal defect or mitral regurgitation. The typical systolic murmur, well localized to the back, which is heard in older children with coarctation of the aorta, is not usually heard in neonates. Management and Prognosis Uncomplicated coarctation of the aorta can be repaired electively in early childhood. Surgical repair with end-to-end anastomosis remains the primary approach in many centers. Balloon angioplasty of native coarctation of the aorta can also be considered and still remains a topic of debate. Neonates with congestive heart failure or signs of poor perfusion must be treated with prostaglandin E1 to maintain or restore ductal patency. All neonates with aortic arch interruption must have primary surgical repair of both the aortic arch abnormality and associated defects. Similarly, neonates with coarctation of the aorta and a large ventricular septal defect undergo primary repair. Those with significant arch hypoplasia might require mobilization of the descending aorta to provide enough tissue to relieve the obstruction. Balloon angioplasty of native coarctation of the aorta is usually reserved for older children, but might be useful in the treatment of selected neonates, especially as a palliative procedure. Long-term growth of the repair might be an issue in up to 30% of babies, with premature infants having a higher risk. After birth, even when pulmonary vascular resistance falls and pulmonary blood flow increases, right ventricular output is usually adequate to supply both the systemic and the pulmonary circulations. However, closure of the ductus arteriosus dramatically alters this balance and results in profound systemic hypoperfusion with acidosis and multisystem organ failure. Associated Defects the most important associated defects are anomalies of pulmonary venous return96 or of the right aortic arch. Occasional neonates with aortic atresia have a normal mitral valve and normal left ventricular size because of an associated ventricular septal defect. The absence of an atrial septal defect creates severe in utero pulmonary venous hypertension and limits pulmonary blood flow after birth. Babies born with hypoplastic left heart syndrome often have tachypnea and mild cyanosis. There is a moderate right ventricular impulse, a single second heart sound, and often a third heart sound is present. Murmurs, if present, are caused by increased pulmonary flow or tricuspid valve regurgitation. If the ductus arteriosus is patent, the pulses can be nearly normal; however, as the ductus arteriosus closes, it is difficult to palpate the pulses and the perfusion is poor. A restrictive atrial septum will increase the left atrial pressure and pulmonary venous pressure, which will lead to pulmonary edema. The combination of pulmonary edema and restricted pulmonary blood flow produces profound hypoxia. The Norwood operation76 and the application of cardiac transplantation to the neonate14 with hypoplastic left heart syndrome have afforded new hope to the families of newborn infants with this otherwise lethal cardiac defect. The advances in both of these approaches have brought us much closer to the reality of an acceptable quality and duration of life. Pulse oximetry averages 70% to 90%, depending on the pulmonary blood flow and the degree of pulmonary edema. The chest radiograph shows cardiomegaly and increased pulmonary blood flow with some degree of pulmonary venous congestion. Anatomy and Pathophysiology Hypoplastic left heart syndrome includes aortic valve atresia, mitral valve atresia, and severe left ventricular and proximal aortic hypoplasia as well as aortic coarctation. Coronary artery abnormalities have been recognized but have uncertain impact on long-term myocardial function. In hypoplastic left heart syndrome, the entire systemic circulation is supplied by blood through the main pulmonary artery that crosses the ductus arteriosus and enters the aorta.
Order genuine zyban on-line. Is your chest pain a heart attack?.
References
- Edfeldt K, Swedenborg J, Hansson GK, Yan ZQ: Expression of toll-like receptors in human atherosclerotic lesions: A possible pathway for plaque activation. Circulation 2002;105:1158-1161.
- Meric F, Milas M, Hunt KK, et al. Impact of neoadjuvant chemotherapy on postoperative morbidity in soft tissue sarcomas. J Clin Oncol 2000;18(19):3378-3383.
- Padua L, Tonali P, Aprile I, Caliandro P, Bartoccioni E, Evoli A. Seronegative myasthenia gravis: Comparison of neurophysiological picture in MuSK+ and MUSK? patients. Eur J Neurol. 2006;13:273-276.
- Faltas BM, Prandi D, Tagawa ST, et al. Clonal evolution of chemotherapyresistant urothelial carcinoma. Nat Genet 2016;48(12):1490-1499.
- Dufour AB, Casey VA, Golightly YM, Hannan MT. Characteristics associated with hallux valgus in a population- based foot study of older adults. Arthritis Care Res (Hoboken) 2014; 66(12):1880-6.
- Murray DJ, Boulet JR, Kras JF, et al: Acute care skills in anesthesia practice: A simulation-based resident performance assessment, Anesthesiology 101:1084, 2004.
- Schmid TE, Eskenazi B, Baumgartner A, et al: The effects of male age on sperm DNA damage in healthy non-smokers, Hum Reprod 22:180n187, 2007.
- Iwaya T, Maesawa C, Tamura G, et al. Esophageal carcinosarcoma: a genetic analysis. Gastroenterology 1997;113:973.