
Duricef
| Contato
Página Inicial
David Morgan, M.D.
- University of Texas
- Southwestern Medical Center
- Parkland Memorial Hospital
- Dallas, TX
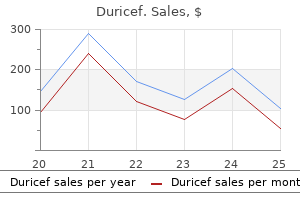
The converse is a stroke syndrome with sudden onset of maximal symptoms that remain stable; this suggests an embolic process such as a cardioembolic stroke due to atrial fibrillation medicine garden discount duricef 250mg mastercard. Intracerebral hemorrhage often presents with abrupt onset of symptoms medications neuropathy duricef 250mg purchase on line, but close questioning may reveal that symptoms actually progressed over 15 to 30 minutes as the hematoma grew and expanded medications on airplanes purchase duricef cheap. Each year stroke affects almost 800 treatment yeast infection women 500mg duricef purchase mastercard,000 people in the United States and about 16 million people throughout the world medications such as seasonale are designed to generic 250 mg duricef with amex. A full understanding of how patients with stroke and cerebrovascular disease come to medical attention, along with a logical approach for defining the mechanism of stroke, are needed for safe and effective implementation of acute therapies and prevention strategies. This chapter will focus on clinical manifestations of all types of cerebrovascular disease and how clinicians can approach diagnostic evaluation. Overview of Clinical Stroke Stroke and cerebrovascular disease are caused by some disturbance of the cerebral vessels in almost all cases. In simple terms, we can divide stroke in to two major types: ischemic and hemorrhagic. Ischemic stroke is the most common variety and is responsible for 80% to 85% of all strokes; hemorrhagic stroke accounts for the remainder. Ischemic stroke occurs when a blood vessel in or around the brain becomes occluded or has a high-grade stenosis that reduces the perfusion of distal cerebral tissue. A variety of mechanisms and processes can lead to such occlusions and will be discussed later in more detail. On rare occasions, venous thrombosis can occlude a cerebral vein and lead to ischemic as well as hemorrhagic strokes (venous infarction). Clinical Manifestations of Stroke and Cerebrovascular Disease Stroke is similar to real estate in that much of its presentation and prognosis depend on size and location. Blood vessels that supply different parts of the brain are affected by different types of cerebrovascular disease and have different mechanisms (pathophysiology) for the stroke. This concept greatly influences and defines the approach a vascular neurologist or neurosurgeon uses when assessing patients with a stroke or cerebrovascular disease. Several scoring systems have been developed (Table 30-3) that may be useful for assessing such risks. Of course, any such assessment tool must be tempered by good clinical judgment and consideration of all clinical factors. One is sudden blindness in one eye, which typically occurs as a "shade coming down" over the eye. Some patients report a graying out of vision in the eye, like looking through a gray haze or cloud. This symptom complex typically resolves in a few minutes, although it can last for several hours. There is sometimes pain in or around the eye, but patients usually do not have any other focal neurological complaints. Some cases of amaurosis are due to emboli to the retinal circulation from an ulcerated plaque in or near the carotid bifurcation in the neck. Other cases can be due to local disease in the ophthalmic artery or in the posterior ciliary artery that supplies the optic nerve. Patients report uncontrollable shaking of a limb that can be precipitated by movement. The sentinel headache present as an acute headache that is unusual in terms of its nature, severity, and onset. Myriad clotting disorders have been associated with strokes in young adults, the most common being lupus anticoagulants, anticardiolipin antibodies, and protein C and protein S deficiency. Clotting disorders related to hematological malignancies can cause both ischemic and hemorrhagic strokes. The "other" category covers a host of conditions, some rare and some common, that cause strokes in young adults. Patients with complex or complicated migraines, prolonged auras, or taking contraceptives have a higher risk of stroke. Our focus here is on specific systemic disorders that lead to specific or unusual types of strokes. There are a number of unique systemic disorders that cause strokes in patients of any age. Autoimmune diseases, such as lupus, can produce strokes through a variety of mechanisms that include advanced or premature atherosclerosis, vasculitis, hypercoagulable states, and cardioembolic events. It is a fallacy to assume that drug abuse only occurs in young patients or those from certain demographic groups. All patients admitted with a stroke should be tested for drug abuse with urine toxicology screens, not excluding those older than 50 years and white-collar professionals. Ischemic Stroke Syndromes There are numerous manifestations of ischemic stroke, and they can be classified based on brain location involved, artery affected, or symptoms produced. Although advanced diagnostic techniques have altered some of the clinical rules of stroke symptoms and etiology, there are still some useful concepts that can guide us in terms of stroke location and mechanism. Tables 30-1 and 30-2 list some classic ischemic stroke syndromes with their major clinical manifestations, vascular territory, and underlying pathophysiology. Typically, clinicians look for unilateral weakness or sensory deficits, unilateral visual field abnormalities, speech disturbance (aphasia or dysarthria), neglect syndromes, unilateral ataxia, ophthalmoplegias, or gaze abnormalities as clues of a stroke. Symptoms such as vague diffuse weakness alone, headaches alone, memory loss, abnormal behavior, or isolated dizziness are rarely caused by an ischemic stroke. The appearance of a lesion in a typical vascular territory (based on brain imaging) is a key feature of almost all stroke syndromes. There are specific syndromes that indicate small-vessel involvement deep in the brain. These so-called lacunar strokes are due to occlusion of small penetrating arteries that arise directly from larger parent vessels. Favored locations include the deep basal ganglia structures, thalamus, and brainstem (pons). These lesions can occur anywhere in the cerebral vasculature, but they tend to have a preference for specific locations such as the bifurcation of the carotid artery in the neck, intracranial carotid siphons, proximal portion of the middle cerebral artery, mid-portion of the basilar artery, and aortic arch. An atherosclerotic plaque forms over many years, then ruptures causing formation of a superimposed thrombus. A variety of conditions such as atrial fibrillation, endocarditis, prior myocardial infarction, valvular disease, and cardiomyopathy often lead to formation of intracardiac thrombi that subsequently embolize to the brain (and other organs). Such cases often entail a special evaluation because of the unique processes and conditions that can produce strokes in this age group. Mechanisms for strokes related to cancer include a hypercoagulable state and nonbacterial thrombotic endocarditis. Oftentimes these strokes are multiple, variable in size, and in different vascular territories. Intracerebral hemorrhage is typically caused by rupture of a blood vessel within the brain parenchyma. Patients typically develop a focal neurological deficit suddenly, but symptoms often evolve over 10 to 30 minutes as the hematoma gradually expands. Headache is commonly present, and the vast majority of patients have markedly elevated blood pressure (often in excess of 200 mmHg systolic) even without a prior history of hypertension. Cerebral amyloid angiopathy is caused by deposition of one or more amyloid proteins within the wall of cerebral small arterioles. This occurs in up to 15% of cases of ischemic stroke and is associated with large strokes, cardioembolic strokes, and the use of anticoagulants and thrombolytic agents. Intracerebral hemorrhage can occur as a consequence of anticoagulation use, administration of thrombolytic therapy (either for a stroke or another systemic condition), other coagulopathies, hematological disorders, endocarditis, infections (fungal, bacterial, viral), drug abuse (cocaine, heroin, amphetamines), brain tumors (typically metastases), and venous thrombosis. However, using modern imaging techniques, we can now image aneurysms that occur more distally in the arterial tree. Depending on the location of the ruptured aneurysm, some patients may have additional focal neurological findings. For example, an aneurysm involving the posterior communicating artery can produce an ipsilateral third nerve palsy that involves the pupil. Rupture of an aneurysm of the anterior communicating artery can produce speech and behavioral changes. Aneurysmal rupture that leads to extensive bleeding around the brain and in to the ventricles can lead to altered mental status, coma, and sometimes early or sudden death due to dramatic increases in intracranial pressure. Many medical conditions can present with stroke-like symptoms and even physical findings, but with a different etiology. This has obvious implications in terms of acute therapy, ongoing care, and secondary prevention. Table 30-7 lists some common stroke mimics and diagnostic tests that may be helpful for making the diagnosis. Factors of key concern include prior medical history with assessment of stroke risk factors (hypertension, diabetes, heart disease, etc. We are particularly concerned about symptoms such as disturbances of speech, language, and mentation; evidence of cranial nerve dysfunction (diplopia, vision loss in one eye or sector, dysarthria, dysphagia, facial weakness); focal motor weakness or coordination problems; gait abnormalities; and sensory symptoms. A particular challenge for stroke patients is that often their ability to sense or report these various symptoms may be affected by the very stroke causing the symptoms. This makes obtaining historical details from family, friends, or caregivers very important. Time of stroke onset is often (and incorrectly) assumed to be when the patient is found with evidence of a stroke. If a patient has been under constant observation, the time of onset will be when the patient was first noticed to have stroke symptoms. But if a patient has been home alone and discovered with stroke symptoms by a family member, the time of onset has to be when the patient was last known to be normal (assuming the patient cannot determine the time of onset). Therefore, in the case of a patient who awakens in the morning unable to speak at 7 am, time of onset is assumed to be when the patient went to bed normal the night before, unless there is clear documentation otherwise. As already noted, this is a key step in determining stroke mechanism and etiology. Besides vital signs and a thorough neurological examination, there are particular aspects of the general medical examination that provide important diagnostic information to the clinician. These include an assessment for cervical bruits, a complete cardiac examination, checking blood pressure and pulses in both arms, a skin examination, and evidence of trauma to the head and neck. Table 30-8 offers an outline of a neurological assessment for patients with known or suspected cerebrovascular disease. Clinicians often use a variety of scales or scoring systems to assess severity of various types of stroke. These scoring systems can provide guidance about treatment options as well as overall prognosis. Brain Imaging Our ability to rapidly and accurately image the brain and cerebral vasculature has been an important step and driver in our capability to determine the type of stroke, its locations, and likely mechanism. On-site personnel or remote radiology reading technologies and services can provide a reading within 30 to 60 minutes. The ability to rapidly perform and interpret brain imaging is a key component of a primary stroke center. Intracerebral hemorrhages appear as white lesions in the brain parenchyma that represent the actual hematoma. Arrow indicates a subacute stroke (darker gray area) in right occipital lobe in a patient with a new visual field deficit present for about 24 hours. White dots (arrows) show areas of acute ischemic or infarction consistent with several acute strokes in a patient with atrial fibrillation. Using this technique, studies have shown that up to 40% of ischemic strokes may have microhemorrhages within the area of ischemia. For example,a patient may present with symptoms pointing to a small-vessel stroke deep in the brain. In the proper setting, this type of stroke might be caused by typical vascular risk factors such as hypertension or diabetes. After a week or more, methemoglobin becomes extracellular and becomes bright on T1 and T2 sequences. Hemosiderin is then formed in the hematoma and produces a dark signal in gradient echo sequences45. A B Imaging Cerebral Vasculature Of equal importance to imaging brain parenchyma is detailed imaging of the cerebral vasculature, both extracranial (aorta, carotid and vertebral arteries) and intracranial vessels. Both techniques can provide information about direction and velocity of blood flow. Carotid ultrasound can be performed serially over the course of months and years to assess changes in the degree of stenosis of a neck artery, and it can determine plaque size and composition. By injecting the various cerebral vessels, an angiogram can determine (in cases of a vessel stenosis or occlusion) exactly where the blood supply is coming from and going to . The angiogram can detect collateral vessels (or lack thereof) that may be supplying a region of brain thought to be poorly perfused due to occlusion of a proximal vessel. We have often seen patients with apparent lack of flow through a severely diseased basilar artery, only to find that abundant collaterals are supplying the brainstem with adequate perfusion. Using computer reconstruction algorithms, images from all the above techniques can be assembled in to three-dimensional (3D) pictures to provide a comprehensive view of the cerebral vessels. These images can be rotated and flipped as needed to aid the clinician in determining the type, location, and severity of the lesion (stenosis, aneurysm, etc. Computed tomographic angiography provides modestly more precise anatomical detail in terms of its ability to detect small aneurysms and small dissection flaps, and accurately determine the degree of arterial stenoses. Carotid duplex ultrasound is a safe and noninvasive method to image selected segments of the large vessels in the neck. Benefits of platelet function testing for improving efficacy and safety of stroke therapy remain experimental; however, such testing may be important for detecting platelet dysfunction in patients with hemorrhagic stroke. Blood cultures may be obtained in patients with multiple embolic strokes to rule out endocarditis. Since the heart can be the cause of up to 25% of all strokes, a thorough cardiac assessment is needed in most cases.
Beckman as a false aneurysm xerogenic medications order duricef amex, results from a disruption of the aortic wall and essentially represents a contained rupture of the aorta medicine 02 buy duricef 250 mg on line. Aortic aneurysms result in significant morbidity and mortality treatment cheap duricef 500 mg with amex, accounting for nearly 13 medications gabapentin generic duricef 250mg visa,000 deaths and 55 medications during pregnancy order duricef online,000 hospital discharges per year in the United States. Timely and appropriate intervention may improve the natural history of the disease process. This chapter reviews the pathophysiology, epidemiology, and prognosis of aortic aneurysms. Pathophysiology of Aortic Aneurysms A wide variety of pathological states are associated with aortic aneurysms (Box 37-1). These include degenerative diseases, inherited disorders, infections, inflammatory conditions. Specific disorders associated with aortic aneurysms are discussed later in this chapter. Important determinants of aortic aneurysm formation include inflammation, proteolysis of the structural components of the aortic wall, and abnormal biomechanical forces3. Understanding the underlying pathophysiology of aneurysm formation is critical not only for prevention of initial aneurysm formation but also for limiting aneurysm growth and expansion. Traditionally, pathological aortic aneurysm formation was ascribed to a process akin to atherogenesis. Although advances in basic and clinical investigation in both lesion types have revealed some common themes, newer studies suggest that aneurysm formation is fundamentally different from atherosclerosis. Preferential weakening of the adventitia and media-rather than an intimal proliferative process, as in atherosclerosis-results in diminished aortic resilience and tensile strength, culminating in aortic wall thinning, dilation, and increased wall stress, all of which may result in rupture. Although atherosclerotic changes may be seen in the wall of aneurysms, these changes may be a consequence of local turbulent flow as opposed to a cause of aneurysm formation. Elastin provides radial and longitudinal support, enabling the aorta to respond to pulsatile flow while maintaining normal arterial dimensions. The importance of elastin in maintaining aortic structure is highlighted by animal models where elastase infusion results in elastin breakdown and experimental aortic aneurysm formation. Loss of collagen, another important structural element, is an additional contributor, and the relative balance of elastin and collagen deposition, among other factors, may be critical for determining aneurysm formation. This is exacerbated by up-regulation of collagenases, resulting in further collagen degradation as described later. In the thorax, the aorta can be subdivided in to three segments: ascending aorta (from the base of the heart to the innominate artery), transverse aorta or aortic arch (including the great vessels and extending to the left subclavian artery), and descending aorta (from the distal edge of the subclavian artery to the level of the diaphragm). Like other arterial structures, the aorta is composed of three layers: tunica intima, tunica media, and adventitia. The presence of elastin fibers in the media defines the aorta as an elastic artery and provides the tensile strength that permits the aorta to withstand pulsatile delivery of blood from the heart. Definition of Aortic Aneurysm In adults, the normal diameter of the aorta is approximately 3 cm at the origin, 2. Mild expansion that does not meet these criteria may be referred to as aortic ectasia. True aneurysms are classified in to two major groups on the basis of morphology: (1) fusiform. Note the different aortic segments: ascending aorta, aortic arch, and descending aorta. Aortic aneurysm specimens reveal increases in leukocyte infiltration, cytokine concentration, and leukocyte adhesion molecules. Both elastin-related and collagenrelated autoantigens have been identified and may participate in initiation of process. Increase in proteolysis is not accompanied by change in inhibitors of process, yielding a degenerative environment. Abdominal aorta is predisposed to aneurysm formation because of adverse blood flow patterns and its relative lack of elastin and vascular smooth muscle compared with thoracic aorta. Pathology of aortic aneurysms varies in different segments of the aorta and in different predisposing diseases. Frequently observed histological features include cystic medial necrosis, mucoid infiltration, and cyst formation in the setting of elastin necrosis and vascular smooth muscle apoptosis. Despite differences in pathophysiology due to location and underlying etiology, formation of all aortic aneurysms involves to some degree the processes described in the following discussions. Proteolytic Degradation Several proteolytic enzymes contribute to degradation of structural components of the arterial wall, ultimately increasing risk of aneurysm formation. Matrix metalloproteinase levels are increased in states of inflammation and oxidant stress, both known to play a role in aneurysm formation. By reducing levels of proteolytic enzymes, several other therapies may potentially be of therapeutic benefit in aneurysmal disease. A meta-analysis of five studies including 697 patients with small aortic aneurysms (<55 mm) treated with or without statins suggested that statin therapy was associated with lower rates of expansion. However, the initial signals that drive inflammatory cell recruitment remain unclear. Animal studies with experimental aneurysm models have confirmed the human studies and demonstrated that increased inflammation promotes aneurysm formation. Indeed, as mentioned previously, some data suggest that statins, known to have beneficial antiinflammatory properties beyond their effect on cholesterol lowering, may limit aneurysm growth and expansion. Variations in biomechanical factors have been noted in the differing regions of the aorta. Relative deficiencies in structural elements combined with adverse blood flow patterns predispose the abdominal aorta to aneurysm formation. Compensatory mechanisms occur after aneurysm formation have developed, but they do not stop the process. Thus, aneurysm expansion is promoted by an imbalance of biomechanical forces and compensatory mechanisms. Several specific structural changes may predispose the abdominal aorta to aneurysm formation. For example, elastin within the aortic wall is organized in to circumferential plates, or lamellae, that respond to the pulsatile load created by the heart. Each lamellar unit consists predominantly of two elastin bundles and vascular smooth muscle. However, deposition of elastin is not uniform along the aorta, with the thoracic aorta incorporating 35 to 56 lamellar units compared to only 28 in the abdominal aorta. In addition, the abdominal aorta has a decreased concentration of nutritive vasa vasorum compared to more proximal aortic segments. In areas of macrophage infiltration, elastin deposition is not organized in to mature effective bundles. Indeed, compared with normal specimens, aneurysm specimens have a ninefold reduction in desmosine, a marker for mature elastin cross-linking. Another factor that may make the abdominal segment of the aorta more prone to aneurysm formation is blood flow patterns specific to that segment. In experimental models, the infrarenal segment of the aorta is subject to much higher levels of oscillating flow and reflected pressure waves compared with the suprarenal segment,102 resulting in higher levels of aortic wall tension. The largest and most recent of these studies screened nearly 10,012 women (mean age, 69. Among 4237 subjects aged 65 to 80 who participated in a screening study among general practitioners in West Sussex, United Kingdom, 2290 women agreed to undergo abdominal ultrasonography. This dramatically lower prevalence in women has been confirmed in subsequent studies. Aneurysms usually affect the elderly, seldom occurring in those younger than 60 years of age, and there is a clear increase in incidence with increasing age, even when limiting the studies to older individuals. However, all these factors should be taken in to consideration when considering risk in any given individual. Risk increases to nearly 10-fold with an affected male sibling and 23-fold when a female sibling is affected. Early studies suggested evidence of both sex-linked and autosomal dominant patterns of inheritance. In a large autopsy study performed over a quarter of a century, one fourth of abdominal aneurysms were ruptured on postmortem examination. In a comparison of patients with aortic aneurysms divided in to two groups at a cutoff point of 6 cm, survival was markedly decreased in the patients with larger aneurysms. At 3 years, nearly 20% of both groups had died, although abdominal aneurysms accounted for only a quarter of the deaths in both groups. Cardiovascular mortality unrelated to the aneurysm accounted for 40% of total mortality, and cancer caused slightly more than 20% of the deaths. After 5 years, there was no significant difference in survival between the groups, each with a near 25% mortality rate. In one study of patients too ill for surgery, aneurysm rupture rates ranged from 9. Degeneration of the media within the arterial wall results in impaired structural integrity of the aorta, leading to eventual aortic dilation, aneurysm formation, and risk of rupture. Finally, some aneurysms develop because of a familial predisposition termed familial thoracic aortic syndrome. Initial aneurysm size at the time of diagnosis is the most important predictor of thoracic aneurysm growth. Prospective studies will be required to determine whether these factors can improve assessment of patients at high risk for aneurysm rupture and can improve selection of patients for aneurysm repair. Because of the high morbidity and mortality and the high rate of aortic dissection, even with aneurysms of less than 5. Abnormalities in fibrillin synthesis may affect multiple tissues in patients with Marfan syndrome, including the cardiovascular, skeletal, and ocular systems. Dilation of the aortic root has been demonstrated early in childhood in patients with Marfan syndrome. The clinical consequences of aortic coarctation are varied, ranging from being life-threatening in infancy to remaining unappreciated until adulthood. Intermediate follow-up studies suggest that percutaneous balloon angioplasty repair results in a 2% to 5% rate of repair-site aortic aneurysm formation. Complications of pregnancy caused the death of 15% of the women who became pregnant. Other Conditions Associated with Aortic Aneurysm Although most aortic aneurysms occur as a result of degenerative processes in the aortic wall as described earlier, certain disease states including vasculitis, infection, and inherited abnormalities of structural proteins predispose patients to aortic aneurysm formation (see Box 37-1). It most commonly occurs in patients older than 55 years of age and is twice as common in women as men. As with other vasculitides, risk of intervention is greatest during the state of active inflammation, and there is an increased risk of rupture, dissection, and/or future aneurysmal dilation at the site of revascularization. These disorders are known to be associated with an increased risk of aortic aneurysm formation. Relapsing polychondritis is a paroxysmal and progressive inflammatory disease of the cartilaginous structures, affecting the ear, nose, and hyaline cartilage of the tracheobronchial tree. Cardiovascular disease, including aortic aneurysms, is found in 25% to 50% of patients. Two large necropsy studies including 22,000 and 20,000 patients, respectively, revealed a combined incidence of 0. In contrast to the typical degenerative or vasculitic fusiform expansion, mycotic aneurysms are more likely to be saccular. The outpouching may range in size from 1 mm to 10 cm and include components of acute and chronic inflammation, hemorrhage, abscess formation, and necrosis. Clinical manifestations of mycotic aneurysm most commonly include pain and fever and, if related to a new aneurysm, should prompt directed investigation. The organisms that most commonly cause mycotic aneurysms include Staphylococcus and Salmonella species, which cause 40% and 20% of mycotic aneurysms, respectively. In a series of more than 22,000 autopsies performed at one urban medical center in the first half of the 20th century, only 1 of 308 aortic aneurysms had tuberculous aneurysms,249 whereas there were no tuberculous aneurysms among 20,000 autopsies performed in a rural setting. It is thought that direct extension from a contiguous source, such as the spine or lung, may cause 75% of tuberculous aneurysms. The patient may be asymptomatic, have a palpable or radiologically visible paraaortic mass, complain of chest or abdominal pain, or present with aortic rupture and hypovolemic shock. Tuberculous aneurysms that are symptomatic or rapidly expanding and pseudoaneurysms typically require surgical repair. Classically, this arises after a latent phase of roughly 10 to 30 years from initial spirochete infection. Destruction of the elastic lamina occurs as a consequence of lymphoplasmacytic infiltrate around the vasa vasorum, owing to direct spirochete infection of the aortic media. This ultimately leads to expansion but also fibrosis and calcification, producing the classic "tree bark" radiographic pattern. Involvement of the coronary ostia may result in coronary stenosis and resultant anginal symptoms. Hoshina K, Sho E, Sho M, et al: Wall shear stress and strain modulate experimental aneurysm cellularity, J Vasc Surg 37(5):10671074, 2003. Kawasaki T, Sasayama S, Yagi S, et al: Non-invasive assessment of the age related changes in stiffness of major branches of the human arteries, Cardiovasc Res 21(9):678687, 1987. Zhang J, Schmidt J, Ryschich E, et al: Increased apoptosis and decreased density of medial smooth muscle cells in human abdominal aortic aneurysms, Chin Med J (Engl) 116(10):15491552, 2003. Visse R, Nagase H: Matrix metalloproteinases and tissue inhibitors of metalloproteinases: structure, function, and biochemistry, Circ Res 92(8):827839, 2003. Involvement of the vasa vasorum in the pathogenesis of aortic aneurysms, Arterioscler Thromb 11(6):16671677, 1991. An elastolytic metalloproteinase expressed by aneurysm-infiltrating macrophages, J Clin Invest 96(1):318326, 1995. Davis V, Persidskaia R, Baca-Regen L, et al: Matrix metalloproteinase-2 production and its binding to the matrix are increased in abdominal aortic aneurysms, Arterioscler Thromb Vasc Biol 18(10):16251633, 1998. Nishimura K, Ikebuchi M, Kanaoka Y, et al: Relationships between matrix metalloproteinases and tissue inhibitor of metalloproteinases in the wall of abdominal aortic aneurysms, Int Angiol 22(3):229238, 2003.
Finally medications you can take while nursing generic duricef 250mg buy line, a 218 synthesis of three studies addressing this question reported odds ratios of 2 symptoms thyroid cancer buy generic duricef 250mg. Interestingly medicine daughter order 250 mg duricef amex, hospital-based studies suggest that anatomical distribution of disease may differ in blacks symptoms after conception 500 mg duricef buy otc, with a higher percentage of distal disease in black subjects medicine 770 purchase duricef 250 mg free shipping, even after adjustment for diabetes and other cardiovascular risk factors. A 1995 meta-analysis of early case-control studies conducted in the late 1980s and early 1990s suggested an odds ratio of 6. This may be related to the quality of the studies included in the meta-analysis, which included primarily small case-control studies. Differences in the relative strength and significance of risk factors in men and women have been examined in several studies. Many of these studies have concluded that risk factors do not differ substantially in men and women. A more meaningful approach may be to look at the percentage of the population achieving some categorically defined measure of change. Results are shown with multivariable adjustment and after exclusion of subjects with baseline cardiovascular disease, where such exclusion was attempted. Aboyans V, Lacroix P, Lebourdon A, et al: the intra- and interobserver variability of ankle-arm blood pressure index according to its mode of calculation, J Clin Epidemiol 56:215, 2003. Kreines K, Johnson E, Albrink M, et al: the course of peripheral vascular disease in noninsulin-dependent diabetes, Diabetes Care 8:235, 1985. Report and recommendations of an international workshop sponsored by the American Heart Association and the American Diabetes Association, 18-20 September 1992, New Orleans, Louisiana, Diabetes Care 16:1199, 1993. McKenna M, Wolfson S, Kuller L: the ratio of ankle and arm arterial pressure as an independent predictor of mortality, Atherosclerosis 87:119, 1991. The Cardiovascular Health Study Group, Arterioscler Thromb Vasc Biol 19:538, 1999. Ankle Brachial Index Collaboration: Ankle brachial index combined with Framingham risk score to predict cardiovascular events and mortality. Bainton D, Sweetnam P, Baker I, et al: Peripheral vascular disease: consequence for survival and association with risk factors in the Speedwell prospective heart disease study, Br Heart J 72:128, 1994. Gallotta G, Iazzetta N, Milan G, et al: Prevalence of peripheral arterial disease in an elderly rural population of southern Italy, Gerontology 43:289, 1997. Jonason T, Bergstrom R: Cessation of smoking in patients with intermittent claudication: effects on the risk of peripheral vascular complications, myocardial infarction and mortality, Acta Med Scand 221:253, 1987. Summary and Conclusions Peripheral artery disease is atherosclerotic obstruction of the arteries of the lower extremities. Peripheral artery disease prevalence is sharply age related, rising to more than 10% among patients in their 60s and 70s. Prevalence appears to be higher among men than women for moderate to severe disease. Peripheral artery disease is cross-sectionally associated with cardiovascular and cerebrovascular disease. Winsor T: Influence of arterial disease on the systolic blood pressure gradients of the extremity, Am J Med Sci 220:117, 1950. Haltmayer M, Mueller T, Horvath W, et al: Impact of atherosclerotic risk factors on the anatomical distribution of peripheral arterial disease, Int Angiol 20:200, 2001. Natarajan S, Glick H, Criqui M, et al: Cholesterol measures to identify and treat individuals at risk for coronary disease, Am J Prev Med 25:50, 2003. Dormandy J, Heeck L, Vig S: Predictors of early disease in the lower limbs, Semin Vasc Surg 12:109, 1999. Jelnes R, Gaardsting O, Hougaard Jensen K, et al: Fate in intermittent claudication: outcome and risk factors, Br Med J (Clin Res Ed) 293:1137, 1986. Reunanen A, Takkunen H, Aromaa A: Prevalence of intermittent claudication and its effect on mortality, Acta Med Scand 211:249, 1982. Kornitzer M, Dramaix M, Sobolski J, et al: Ankle/arm pressure index in asymptomatic middle-aged males: an independent predictor of ten-year coronary heart disease mortality, Angiology 46:211, 1995. Critical limb ischemia is defined by chronic ischemic pain at rest and/or presence of ischemic skin lesions (gangrene or ulcerations). The classic symptom of intermittent claudication is an exercise-induced discomfort in the calf associated with reversible muscle ischemia and relieved by rest. The term claudication is derived from the Latin word claudica to , meaning " to limp," which is typical of the gait pattern of the patient who experiences claudication when walking. Discomfort develops only during exercise, steadily increases during walking activity to a point where the patient has to stop, and then is quickly relieved by rest without change of position. This sequence of exercise-induced progression and complete relief with rest are important clinical differentiators of claudication from other lower-extremity musculoskeletal conditions. Patients with claudication have severe limitations in exercise performance and walking ability. In healthy persons, maximal muscle oxygen consumption is determined primarily by maximal oxygen delivery, rather than mitochondrial metabolic rate. This basic relationship can be expressed as: Blood flow = Pressure ÷ Vascular resistance In healthy persons, exercise is a major stimulus for vasodilation, causing a decrease in peripheral resistance, which when combined with an increase in systemic pressure results in a large increase in arterial flow to skeletal muscle. Normal arteries have the capacity to support large volumetric increases in blood flow without a significant drop in pressure across the large and medium conduit vessels. Major factors that determine the pressure drop across an arterial stenosis include blood flow velocity and the resistance caused by the stenosis,which in turn is defined by the length and internal radius of the stenosis and blood viscosity. Therefore, blood flow and oxygen delivery match muscle metabolic demand at rest and exercise. In contrast, in peripheral artery disease (bottom) arterial stenosis results in turbulent flow. Increased resistance associated with stenosis and loss of kinetic energy results in pressure drop across stenosis. In addition, endothelial function is impaired, resulting in further loss of vascular function. These changes limit blood flow response to exercise, resulting in mismatch of oxygen delivery to muscle metabolic demand. Changes in skeletal muscle metabolism further compromise efficient generation of highenergy phosphates. Oxidant stress-the result of inefficient oxidation-further impairs endothelial function and muscle metabolism. This equation makes clear that the radius or cross-sectional area of the stenosis is the primary factor in determining the drop in pressure and flow across a stenosis; a 50% reduction in crosssectional diameter of the vessel results in a 16-fold increase in resistance. This relationship indicates that as a stenosis worsens, perfusion pressure (and thus the potential pressure that can be dissipated across the stenosis) and the maximal achieved blood flow will decrease dramatically. The dissipation of energy that occurs as blood flow traverses a stenosis is determined in part by the morphology of the stenosis and blood viscosity. Resting blood flow is usually preserved because of the pressure of arterial collaterals in most patients. A patient with mild claudication may have stenosis at only a single site, such as the iliac artery, but a patient with moderate or severe claudication could have occlusive disease at multiple sites, including the iliac, femoral, and popliteal arteries. Based on the Poiseuille equation, the length of an individual stenosis has only mild impact on blood flow and the pressure gradient. Nevertheless, the hemodynamic effect of two equivalent lesions in series is double that of a single lesion. An exercise-induced increase in flow velocity across a 50% stenosis could significantly increase the pressure gradient and reduce distal perfusion pressure. The associated fall in peripheral resistance would be insufficient to compensate for the fall in pressure, and distal blood flow would decrease. Thus the critical arterial stenosis needed to reduce distal blood flow during exercise may be only 50%. However, when flow velocity increases with exercise, the same iliac artery lesion becomes hemodynamically significant, resulting in a loss of pedal pulses due to the decrease in ankle pressure distal to the stenosis. Thus anatomy per se may not provide sufficient evidence of the functional significance of a particular degree of arterial stenosis. This is because resting blood flow is sufficient to meet the relatively low metabolic needs of the tissue, and therefore there is no mismatch between supply and demand to maintain leg oxygen consumption. This plateau reflects dissipation of energy across the stenotic lesions, removing any additional driving force for increase in flow. Despite the plateau in oxygen delivery during exercise, further increases in oxidative work output are supported by increases in muscle oxygen extraction. The resultant mismatch between the demands for bioenergetics and the flow supply also contribute. Critical Artery Stenosis the hemodynamic significance of an arterial stenosis is not only a function of the percent stenosis, but also linear flow velocity across the lesion, as reflected in the Poiseuille equation. The concept integrates the relationship of a stenotic narrowing in an artery with arterial flow velocity and the resultant volumetric flow distal to the stenosis. Importantly, a critical artery stenosis may differ between resting and exercising states because flow velocity in these two conditions is different. Because the pressure gradient across any given stenosis is proportional to the flow velocity, states of higher flow velocity, as occurs with exercise, may result in a decrease in distal perfusion pressure, whereas states of lower velocity, as occurs at rest, may not. For example, resting blood flow velocity in the femoral artery may be only 10 to 20 cm/s, corresponding to a downstream calf blood flow of 1 to 2 mL/100 mL of tissue/min. Distal flow will be maintained, since the mild reduction in perfusion pressure will be compensated by a reduction in downstream peripheral resistance. Once the stenosis becomes greater than 90%, there is a greater pressure gradient and fall in distal perfusion pressure, and changes in peripheral resistance can no longer compensate. In this example, the critical arterial stenosis needed to reduce distal blood flow at rest is 90%. Other Contributors to Altered Blood Flow in Peripheral Artery Disease Although arterial flow limitations are of critical importance in the pathophysiology of claudication, the hemodynamic status of the limb correlates poorly with exercise performance. After exercise-induced claudication, total neutrophil number and the proportion of activated neutrophils are higher in venous blood draining from the affected leg than in arterial blood. Furthermore, activated leukocytes release thromboxane A2 (TxA2), which is a vasoconstrictor and promotes platelet aggregation. Thus the generation of free radicals and oxidative stress can be mediators of tissue injury. Leukocytes may play an important role in ischemic disease via formation of microemboli and induction of oxidative damage. Activated neutrophils may adhere to other leukocytes and blood cells, further narrowing the vessel lumen and, through release of mediators, increasing vessel wall damage. In one study, P-selectin expression was significantly increased in patients with intermittent claudication and critical ischemia compared to controls. Sequelae are increase in expression of mitochondrial enzymes and accumulation of lactate and acylcarnitines. Kreb Cycle Increased Expression Mitochondrial Enzyme Glucose Fatty Acids Lactate Accumulation Acylcarnitine Accumulation. These steps have been previously identified as targets of oxidative injury in myocardial perfusion-reperfusion models. Supplementation with the antioxidant vitamin C improves endothelial function in patients with diabetes. Muscle Structure and Function in Peripheral Artery Disease In healthy humans, exercise requires coordinated recruitment of appropriate muscle fiber types to meet the demands of specific exercise conditions. There is recruitment of type I oxidative slowtwitch fibers that have high mitochondrial content with low-intensity repetitive contractions. Depending on the exercise intensity of these contractions, the fuel is a balance of fat and carbohydrate oxidation. These fibers have fewer mitochondria than type I fibers and have easy fatigability. These changes reflect a complex combination of changes associated with disuse due to exercise limitation and direct injury from ischemia, ischemia-reperfusion, and chronic inflammatory mechanisms. Patients with claudication also demonstrate extensive skeletal muscle denervation by histological criteria. Denervation injury has been confirmed by electrophysiological testing, and these abnormalities are progressive over time. The neurophysiological changes suggest that the underlying pathophysiology is a distal axonopathy affecting nerve fibers of all sizes. Measures of blood flow in the leg correlate with neurological symptom scores, examination scores, and electrophysiological testing. Increased capillarity may be in compensation for the reduction in large-vessel blood flow, and these changes in peripheral diffusion (higher conductance) may have functional relevance. Whether these gait abnormalities are related to muscle denervation and weakness or are adaptations to minimize development of pain is unknown. Muscle mitochondrial content and mitochondrial enzyme activities reflect the functional state of the individual. Skeletal muscle mitochondrial oxidative enzyme activities increase with exercise training and decrease with prolonged bed rest or inactivity. An increased mitochondrial content might improve oxygen extraction under ischemic conditions and could reflect a compensatory mechanism for any intrinsic abnormality in mitochondrial oxidative capacity. During normal metabolic conditions, fuel substrates such as fatty acids, protein, and carbohydrates are converted to acyl-coenzyme A (CoA) intermediates for oxidative metabolism in the Krebs cycle. These coAcoupled intermediates are linked to the cellular carnitine pool through reversible transfer of acyl groups between carnitine and CoA. Thus, during conditions of metabolic stress, incomplete oxidation or utilization of an acyl-CoA will lead to their accumulation. Transfer of the acyl group to carnitine will result in accumulation of the corresponding acylcarnitine. Importantly, acylcarnitine accumulation may have functional significance in that patients with the greatest accumulation have the most reduced treadmill exercise performance. This limitation in the blood flow response to exercise has metabolic consequences. At the onset of exercise, however, there is a marked delay in systemic uptake of oxygen that parallels a slowed response in skeletal muscle uptake of oxygen. Large-vessel obstruction impairs delivery of oxygenated blood to skeletal muscle during exercise, resulting in a supply/demand mismatch.
Buy duricef paypal. What are the early symptoms of Dehydration. By Dr. Kamal (with English captions).
In contrast symptoms esophageal cancer generic duricef 500mg overnight delivery, numerous observational studies reported stabilization or improvement in renal function4 treatment herniated disc discount 250 mg duricef fast delivery,2527 and hypertension control8 treatment ear infection order duricef 250mg on line,28 medicine 3 sixes buy 500mg duricef amex,29 after renal stenting symptoms type 1 diabetes duricef 500mg generic. Finally, the medical literature is filled with ambiguous and inconsistent terminology regarding renovascular syndromes. If renal perfusion is normal, revascularization is not indicated regardless of stenosis severity; such patients should be followed for development of vital organ injury. If renal hypoperfusion is documented, such patients may be considered to have "unilateral" renal injury. This form of renal injury is not mentioned in existing guidelines and has not been studied in randomized controlled trials, but we generally consider such patients candidates for renal revascularization to preserve renal function. Selective renal angiography showed extensive intrarenal arteriolar disease, including pruning of distal vessels, ill-defined renal pyramids, and poor cortical blood flow (B). Medical therapy was adjusted because of advanced parenchymal disease without renal intervention, and blood pressure normalized. Left renal artery stenting was performed because of hypoperfusion of left kidney and absence of parenchymal disease. Interpretation of data is limited by the uncertain clinical relevance of these classification groups. Second, many patients with hypertension have intrarenal parenchymal disease, leading to hypertensive nephropathy and self-perpetuating hypertension. In these patients, hypertension is sustained by intrarenal mechanisms including increased sympathetic nerve activity, renin-angiotensin system activity, and impaired sodium excretion regardless of patency of the proximal renal artery. The survival of medically treated patients with renovascular disease has not been defined, but most late deaths are due to cardiovascular events rather than progressive renal failure. These data also suggest that the outcomes of renal revascularization are better when revascularization is performed before the development of advanced parenchymal disease. Improvement in renal function after stenting occurred in 8% to 22% of patients in a systematic review,18 and 20 of 22 cohort studies reported improvement or stabilization of renal function. Because renal revascularization rarely cures hypertension, these patients should be treated aggressively with antihypertensive medical therapy. Patients with renal hypoperfusion should be treated before the development of advanced renal failure and ischemic nephropathy. The best candidates for revascularization are those with baseline serum Cr less than 2. In the 600 days prior to revascularization, renal function deteriorated progressively. After stenting, the slope of the reciprocal Cr relationship is zero, suggesting stabilization of renal function. Hanzel G, Balon H, Wong O, et al: Prospective evaluation of aggressive medical therapy for atherosclerotic renal artery stenosis, with renal artery stenting reserved for previously injured heart, brain, or kidney, Am J Cardiol 96:13221327, 2005. La Batide-Alanore A, Azizi M, Froissart M, et al: Split renal function outcome after renal angioplasty in patients with unilateral renal artery stenosis, J Am Soc Nephrol 12:1235 1241, 2001. Mangiacappra F, Trana C, Sarno G, et al: Translesional pressure gradients to predict the blood pressure response after renal artery stenting in patients with renovascular hypertension, Circ Cardiovasc Interv 3:537542, 2010. Radermacher J, Chavan A, Bleck J, et al: Use of Doppler ultrasonography to predict the outcome of therapy for renal-artery stenosis, N Engl J Med 344:410417, 2001. Remuzzi G, Bertani T: Pathophysiology of progressive nephropathies, N Engl J Med 339:1448, 1998. Balk E, Raman G, Chung M, et al: Effectiveness of management strategies for renal artery stenosis: a systematic review, Ann Intern Med 145:901912, 2006. Krum H, Sobotka P, Mahfoud F, et al: Device-based antihypertensive therapy: therapeutic modulation of the autonomic nervous system, Circulation 123:209215, 2011. Zeller T, Ulrich F, Muller C, et al: Predictors of improved renal function after percutaneous stent-supported angioplasty of severe atherosclerotic ostial renal artery stenosis, Circulation 108:22442249, 2003. Dorros G, Jaff M, Mathiak L, et al: Four-year follow-up of Palmaz-Schatz stent revascularization as treatment for atherosclerotic renal artery stenosis, Circulation 98:642, 1998. Hansen by color Doppler flow, only 40% of these accessory renal vessels are currently identified by renal duplex ultrasound examination. Aortography and renal angiography may be indicated after a positive duplex ultrasound study in selected patients. Patients with severe hypertension and negative or nondiagnostic duplex ultrasound examinations, especially children and young adults, should also undergo angiography. In planning open operative therapy, imaging includes lateral aortography to evaluate the mesenteric vessels. Optimal methods of operative renal reconstruction vary with the patient, pattern of renal artery disease, and clinical significance of associated aortic lesions. Prevalence, Evaluation, and Diagnosis Prevalence As discussed in Chapter 23, it has long been recognized that anatomical renal artery disease may be clinically silent. Conversely, the disease may account for 3% of hypertension within the general population. Of patients presenting for chronic renal replacement therapy, 10% to 20% have renal artery disease. With this in mind, we recommend evaluation for renovascular disease in all persons with severe hypertension, especially when severe hypertension is found in combination with excretory renal insufficiency. Diagnosis When a unilateral renal artery lesion is confirmed in an adult patient with severe hypertension, its functional significance should be defined. Unfortunately, measurement of renal vein renin does not have great value when severe bilateral disease or disease to a solitary kidney is present. Therefore, the decision for empirical intervention is based on severity of the renal artery lesions, severity of hypertension, and degree of associated renal insufficiency. In the latter instance, issues determining recovery of excretory renal function in patients with ischemic nephropathy remain ill-defined. In these circumstances, correction of a renal artery lesion may be justified to eliminate all possible causes of hypertension and renal dysfunction. Because the probability of blood pressure benefit is lower in such a patient, morbidity from the procedure must also be predictably low. If both renal arteries have only moderately severe disease (65%-80% diameter-reducing stenosis), renal revascularization is undertaken only if hypertension is severe. Evaluation Through continued improvements in software and probe design, renal duplex ultrasonography is an accurate and reliable method to identify hemodynamically significant renal atherosclerotic disease. In addition, preparation is minimal (an overnight fast), and there is no need to alter antihypertensive medications. When evaluating for renovascular renal insufficiency, a negative renal duplex ultrasound examination effectively excludes ischemic nephropathy because the primary consideration is global renal ischemia based on main renal artery disease affecting both kidneys. When screening for renovascular hypertension, however, a negative duplex ultrasound examination does not reliably exclude surgical disease due to stenotic accessory arteries or branch renal artery disease. Because renal insufficiency usually parallels the severity of hypertension, a patient who presents with severe renal insufficiency but only mild to moderate hypertension usually has renal parenchymal disease. Characteristically, renovascular hypertension associated with severe renal insufficiency or dialysis dependence is associated with very severe bilateral stenoses or total renal artery occlusions. Patient age, type of lesion, medical comorbidity, and concomitant aortic disease must be considered in selecting patients for open surgical or endovascular management. In the complete absence of hypertension, renal artery intervention is not recommended by any method. In general, functional studies are used to guide management of unilateral lesions. Empirical renal artery repair is performed without functional studies when hypertension is severe and renal artery disease is bilateral or the patient has ischemic nephropathy. With the exception of disease requiring bilateral ex vivo reconstructions that are staged, all hemodynamically significant renal artery disease is corrected in a single operation. Having observed beneficial blood pressure and renal function response regardless of kidney size or histological pattern on renal biopsy, nephrectomy is reserved for unreconstructible renal artery disease to a nonfunctioning kidney. Patients requiring large doses of multiple medications will often have reduced requirements while hospitalized on bed rest. If continued therapy is required, vasodilators and selective -adrenergic blocking agents are the drugs of choice. Management Options Management of renal artery disease discovered incidentally during evaluation of cardiac, aortoiliac, or infrainguinal disease is controversial. In this setting, the decision must address the need for additional diagnostic tests and the decision whether or not to perform combined intervention. Advocates for combined intervention frequently cite "natural history" data (Table 25-1) that suggest atherosclerotic lesions of the renal artery frequently progress and progression is associated with irretrievable decline in kidney size and function. Renal artery stenosis at baseline was not associated with a decline in kidney size or function. This conclusion is supported by the retrospective experience reported by Williamson et al. In patients with functionally significant renal artery lesions and severe hypertension, contemporary results of operative management argue for a selective approach toward renal artery intervention. These include all patients with severe or difficult-to-control hypertension, especially when associated with renal insufficiency. From a practical standpoint, the three basic operations that have been most frequently used are aortorenal bypass, renal artery thromboendarterectomy, and renal artery reimplantation. Although each method may have its proponents, no single approach provides optimal repair for all types of renal artery disease. Aortorenal bypass, preferably with saphenous vein, is probably the most versatile technique. However, thromboendarterectomy is especially useful for ostial atherosclerosis involving multiple renal arteries. When the artery is sufficiently redundant, reimplantation is probably the simplest technique and one particularly appropriate for combined repairs of aortic and renal pathology. Just prior to renal artery occlusion, a bolus of 100 units of heparin per kilogram body weight is given intravenously, and systemic anticoagulation is verified by activated clotting time. Unless required for hemostasis, protamine is not routinely administered for reversal of heparin at completion of the operation. Aortorenal Bypass the most common method of revascularization is aortorenal bypass. Three types of material are available for conduit: autologous saphenous vein, autologous hypogastric artery, and prosthetic grafts. However, if the vein is small (<4 mm in diameter) or sclerotic, the hypogastric artery or a synthetic prosthetic graft may be preferable. Thromboendarterectomy In cases of bilateral atherosclerosis of the renal artery origins, simultaneous bilateral endarterectomy may be the most appropriate procedure. Although endarterectomy may be performed in a transrenal fashion, the transaortic technique is used in the majority of instances. Transaortic endarterectomy is performed through a longitudinal aortotomy, with sleeve endarterectomy of the aorta and eversion endarterectomies of the renal arteries. When combined aortic replacement is planned, the transaortic endarterectomy is performed through the transected aorta. When using the transaortic technique, it is important to mobilize the renal arteries extensively to allow eversion of the vessel in to the aorta. Renal Artery Reimplantation After the renal artery has been dissected from the surrounding retroperitoneal tissue, the vessel may be somewhat redundant. The renal artery must be spatulated and a portion of the aortic wall removed, as in renal artery bypass. Splanchnorenal Bypass Splanchnorenal bypass and other indirect procedures are also used as alternative methods for renal revascularization. Length of arteriotomy is at least three times diameter of artery to prevent recurrent anastomotic stenosis. For the anastomosis, 6-0 or 7-0 monofilament polypropylene sutures are used in continuous fashion under loupe magnification. If apex sutures are placed too deeply or with excess advancement, stenosis can be created, posing risk of late graft thrombosis. Duodenum is mobilized from the aorta laterally in standard fashion or, for more complete exposure, ascending colon and small bowel are mobilized. B, Plaque is transected proximally and distally, and with eversion of renal arteries, atherosclerotic plaque is removed from each renal ostium. Each major defect prompted immediate operative revision, and in each case a significant defect was discovered. At 12-month follow-up, renal artery patency free of critical stenosis was demonstrated in 97% of normal studies, 100% of minor defects, and 88% of revised major defects, providing an overall patency of 97%. Among the five failures with normal ultrasound studies, three occurred after ex vivo branch renal artery repair. Ex Vivo Reconstruction Operative strategy for renal artery branch vessel repair is determined by the required exposure and anticipated period of renal ischemia. When reconstruction can be accomplished with less than 30 minutes of ischemia, an in situ repair is undertaken without special measures for renal preservation. When longer periods of ischemia are anticipated, one of two techniques for hypothermic preservation of the kidney are considered. These techniques include renal mobilization without renal vein transection and ex vivo repair and anatomical replacement in the renal fossa. Ex vivo management is necessary when extensive exposure will be required for extended periods. Consequently, flawless technical repair plays a dominant role in determining postoperative success. Intraoperative duplex ultrasonography provides a rapid, safe method of verifying technically flawless repair. Once imaged, defects can be viewed in multiple projections during conditions of uninterrupted pulsatile blood flow.
References
- Brandes CB, Smith RW. Characterization of patients with primary peroneus longus tendinopathy: a review of twenty-two cases. Foot Ankle Int. 2000;21(6):462-468.
- Rosen Y, Bloch BN: 3T MR of the prostate: reducing susceptibility gradients by inflating the endorectal coil with a barium sulfate suspension, Magn Reson Med 57(5):898-904, 2007.
- Mandelker D, Zhang LY, Kemel Y, et al. Mutation detection in patients with advanced cancer by universal sequencing of cancer-related genes in tumor and normal DNA vs guideline-based germline testing. JAMA 2017;318(9):825-835.
- Geha AS, Sessler AD, Kirklin JW: Alveolar-arterial oxygen gradients after open intracardiac surgery, J Thorac Cardiovasc Surg 51(5):609-615, 1966.
- Gorczynski RJ: Basic pharmacology of esmolol, Am J Cardiol 56:3F, 1985.
- Krishnan JA, Brower RB. High-Frequency Ventilation for Acute Lung Injury and ARDS CHEST, 2004;126:518-27.