
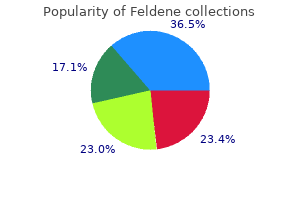
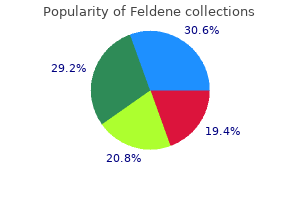
Feldene
| Contato
Página Inicial
Bryan T. Kelly, MD
- Attending Orthopedic Surgeon, Hospital for Special Surgery,
- New York, New York
Small cell carcinoma of the bladder presents as any other bladder tumor diet for arthritis sufferers uk discount 20 mg feldene, most frequently with hematuria rheumatoid arthritis diet supplements discount feldene uk. The tumor usually presents as muscle-invasive disease (94% in 1 series) arthritis knees running trusted 20 mg feldene, and often with metastatic disease (67% in same series) arthritis medication ultram cheap feldene 20 mg with mastercard. Due to the high rate of early dissemination undifferentiated inflammatory arthritis definition order feldene 20 mg fast delivery, chemotherapy is the mainstay of treatment, with radical cystectomy often performed afterward. The significance of bladder trabeculation in the female lower urinary system: An objective evaluation by urodynamic studies. Detection of blastomyces A antigen by immunodiffusion may be helpful in diagnosis. Other serologic testing with enzymeimmnoassay and radioimmunoassay have high sensitivity (85Â88%) and specificity (100%). It is treated by transurethral resection with possible cystectomy, if invasion is suspected. Small cell carcinoma of the urinary bladder: A contemporary review with a special focus on bladder-sparing treatments. Fungal infections of the genitourinary system: Manifestations, diagnosis, and treatment. Pulmonary fibrosis (fibrosing alveolitis) is a potentially lethal toxicity; it can develop 1Â6 mo after treatment and has been reported to occur beyond 6 mo. Bleomycin may also cause hypersensitivity pneumonitis and nodular pulmonary densities. Clinical indications of pulmonary toxicity may include any of the following: Cough (nonproductive), dyspnea, pleuritic chest pain, fever, tachypnea, rales, lung restriction, and hypoxemia. Renal insufficiency is a risk factor for bleomycin toxicity (80% eliminated by the kidney). In prostate, the term blue nevus has been used when melanin is confined to ovoid or elongated melanocytes in the stroma, whereas the term melanosis has been used for those prostatic lesions that have melanin in both the stromal melanocytes and glandular epithelium. Effect of lifestyle changes on erectile dysfunction in obese men: A randomized controlled trial. Other possible urologic sequelae of high-dose chemotherapy exposures include bladder fibrosis, fistula, bladder contracture, chronic urinary tract infections, pyuria, and secondary malignancies. Catheter drainage and continuous bladder irrigation may limit acrolein exposure to bladder urothelium. The base of the flap should be at least 4 cm, while the tip should be at least 3 cm. The tubularized flap is then anchored to the psoas minor tendon, and either direct or tunneled anastomosis with the ureter is then performed. Incidence and prevention of bladder toxicity from cyclophosphamide in the treatment of rheumatic diseases: A data-driven review. Prostate cancer has a predilection to metastasize to bone but bone metastasis from renal cell carcinoma, urothelial carcinoma, and adrenocortical carcinoma is also seen. The diagnosis often involves a radionucleotide bone scan with confirmatory imaging study and possibly a biopsy. Radiation therapy is often highly successful at controlling local bony symptoms and radioisotopes such as strontium-89 are useful for palliation of more extensive bone metastasis. Radium 223 (Xofigo) an -emitter has been approved for bony metastatic prostate cancer and can improve quality of life and extend survival in metastatic castrate resistant prostate cancer. If torsion of the cord can be ruled out by palpation of the unequivocally normal testicle, appendiceal torsion can be observed. As originally described, the test consists of 2 parts: r the patient coughs with a full bladder, and simultaneous urine loss from the urethra is visually confirmed. Bonney cautioned that the fingers must be carefully placed to avoid compressing the urethra in the midline. The contemporary clinical utility of the test has been questioned by many clinicians. Radiographs are taken of centrifuged urine samples, which are obtained immediately after a barium enema. In 1 series of 10 patients, in 7 of the 10, the Bourne test was the only positive evidence of an otherwise occult colovesical fistula later proven at surgery. The system takes into account 3 main factors: r Anatomic location of the lesion (upper motor neuron, lower motor neuron) r Completeness of the lesion (partial vs. Lifestyle factors and duration of androgen deprivation affect bone mineral density of patients with prostate cancer during 1st year of therapy. Due to low specificity, if a lesion is identified, particularly when solitary, further investigation is necessary using confirmatory testing. Bone scans are extensively used in prostate cancer to detect and follow bone metastases. In prostate cancer patients with extensive bony metastasis, the bone scan may have a "super scan" appearance, in which the focal lesions coalesce to produce diffusely increased uptake. An increase in the contrast between bone and background soft tissue and faint or absent renal images are the typical appearances seen on a "super scan. The natural history of the disease is unknown, but the lesions usually follow a benign clinical course, and spontaneous regression is observed. The papules are asymptomatic, discrete, small (averaging 4 mm in diameter), flat, reddish violaceous or brown, often coalescent, and usually have a smooth, velvety surface. Many patients have a history of genital infection with viral warts or herpes simplex. Individual lesions can be adequately treated by excision, cautery, cryoablation, or laser surgery, much as ordinary warts, without the need for wide surgical margins. Classification is based on homogeneity and complexity of cystic fluid, presence or absence of septations, calcifications, or solid components; and the density of cystic fluid as determined by Hounsfield units. Patients may be asymptomatic with occult disease or display neurologic symptoms such as headache, nausea, and vomiting, mental status changes, seizures, or focal signs. Patients presenting with urologic tumors and neurologic signs should be worked up for brain metastases. Due to their high impact on quality of life, these often require prompt treatment usually via radiation therapy or surgical removal. Factors of perceived pressure, alteration of the vertical plane, and time were combined to form a 7-point scale. Traditional assessment tools include the MadsenÂIversen Point System and the Boyarsky Guidelines. The World Health Organization classification is used in most of the rest of the world. A new look at bladder neck obstruction by the Food and Drug Administration regulators: Guidelines for investigation of benign prostatic hypertrophy. The incision site in the lateral posterior surface of the kidney can be accurately identified by injecting indigo carmine in the posterior renal artery branch. Once the capsule is incised, the parenchyma is divided with the blunt end of the knife in the proper plain. Extraovarian and testicular origins have been reported, and they usually present as an ovarian mass. Light microscopy demonstrates distinctive nests of transitional cells indistinguishable from urothelium. Generally asymptomatic and benign, these lesions are often incidentally discovered. Retroperitoneal location is exceedingly rare with only approximately 60 cases reported in the literature. Most retroperitoneal bronchogenic cysts are located near the left adrenal gland or peripancreatic. Anatomopathologic criteria include pseudostratified, ciliated columnar epithelium with cartilage, smooth muscle or seromucous glands. Infection, perforation, hemorrhage, and malignant degeneration are possible and surgical extirpation is recommended. These seeds, when placed into periprostatic tissue, have been noted to migrate, at times entering the prominent periprostatic veins and traveling centrally. Multiple investigations have yielded varying rates of seed displacement and embolization ranging from 0. The most common target organ is the lung, but reports of coronary artery and hepatic emboli exist through a patent foramen ovale. Because of their size, these emboli are often asymptomatic and are diagnosed incidentally on imaging studies. A combined endoscopic needle sling procedure that utilizes a rectus fascial strip placed at the bladder neck through a vaginal incision. The fascial sling is held in place with needles placed through the anterior abdominal wall, similar to the Stamey and Raz suspension needle procedures. Brunn nests represent a further invagination within the lamina propria and are a more progressed form of a Brunn bud. Cystitis cystica is thought to result from a Brunn nest that closes over on itself, forming a cyst. Relevant urologically for its innervation of the bladder outlet and in erectile function and ejaculation. Multicenter prospective randomized 52-week trial of calcium hydroxylapatite versus bovine dermal collagen for treatment of stress urinary incontinence. Brushite stones are particularly dense and are 2nd only to cysteine stones in their resistance to fragmentation. Calcium phosphate is the most common type of stone seen in distal renal tubular acidosis (type 1). On metabolic evaluation, primary calcium phosphate stone formers tend to have higher urine volumes, and higher calcium and lower citrate excretion than do idiopathic calcium oxalate formers. Collagen is no longer available but is included in the table due to its widespread use in the past. Although variable in clinical presentation, a preliminary nonbullous phase is usually characterized by severe pruritus and nonspecific skin changes, followed by formation of confluencing vesicles and marked erythema of the skin. Immunohistochemical evaluation of the skin biopsy shows IgG deposition along the skin basement membrane. Commonly used medications are anti-inflammatory agents (eg, corticosteroids, tetracyclines, dapsone) and immunosuppressants (eg, azathioprine, methotrexate, mycophenolate mofetil, cyclophosphamide). It qualitatively detects highÂmolecular-weight basement membrane complexes, present when tumor cells become invasive and undergo proteolytic degradation. The small size of particles (90% <40 m) allows them to be phagocytosed, which can result in distant migration and granuloma formation. Begins to degrade in 12 wk; completely degraded in 19 mo, but the injected material transforms into living connective tissue. Durasphere is more viscous than collagen, and its injection was more technically demanding. This phase transformation takes place rapidly (within 60s), and this effect creates increased tissue bulk. Textured polydimethylsiloxane macro particles (>100 m) suspended in a bioexcretable carrier hydrogel of polyvinylpyrrolidone (povidone) in which the solid particle content is 33% of the total volume. Viscous gel of dextranomer microspheres (50 mg/mL) in a carrier gel of nonanimal stabilized hyaluronic acid, constituting a biocompatible and biodegradable implant. The hyaluronic acid acts mainly as a carrier, leaving the dextranomer microspheres at the implant site. The reflex is commonly elicited by touching the labium minus lateral to the clitoris or squeezing the glans penis and observing for anal contraction. Treatment of bullous Ò‘ pemphigoid with low-dose oral cyclophosphamide: A case series of 20 patients. However, these calcifications can be a nidus for chronic bacterial infections in some men as many are surrounded by biofilm. Radiation oncologists have explored the use of prostate calcifications as naturally occurring fiducial markers. The relationship between prostate cancer and calcifications has not been confirmed. Extensive calcifications can be seen after some cases of cryotherapy of the prostate and with tuberculous involvement of the prostate. Influence of prostatic calculi on lower urinary tract symptoms in middle-aged men. Transrectal ultrasound anatomy of the prostate and seminal vesicles in healthy men. Elevated blood urea nitrogen as a predictor of mortality in patients admitted for decompensated heart failure. They may represent epidermal cysts that have, over time, lost their normal wall and calcified. Microscopically, broad rete pegs, filled with benign squamous cells and surrounded by a layer of inflammatory cells, are noted. The prostatic stones are usually located between adenoma and the compressed prostatic tissue sometime referred to as the "surgical capsule" of the gland. Many prostatic stones appear to be calcified proteinaceous bodies called corpora amylacea. Corpora amylacea have no clinical significance, and even if dense or clumped, they are usually not palpable. Primary or endogenous calculi are said to be formed in acini from corpora amylacea. The classical clinical picture is a necrotic and progressive skin ulcer (reticular pattern), primarily in the lower legs and susceptible to local infection. It is a product of mural calcification and occlusion of cutaneous and subcutaneous arteries and arterioles. Calciphylaxis is reported to be a lethal complication with an estimated 1-yr survival rate of 45.
No clear causal evidence has been established to link breast cancer to a diet high in fats arthritis in dogs aspirin dose purchase feldene 20 mg on-line, alcohol intake rheumatoid arthritis fatal feldene 20 mg order otc, smoking or abortion rheumatoid arthritis diet soda buy 20 mg feldene otc. If the axillary nodes are considered clinically malignant on examination or imaging arthritis diet management feldene 20 mg buy low price, the patient should have full axillary clearance at the time of surgery arthritis knee naproxen best feldene 20 mg. The importance of micrometastases in long-term survival has not yet been established. Clearance side effects include lymphoedema (10 to 30% is intractable) nerve damage, particularly sensory loss of the intercostobrachial nerve which supplies the upper inner aspect of the arm, wound infection and seroma formation. Prophylactic irradiation of the internal mammary and supraclavicular nodes does not seem to prolong survival. There is no upper age limit for breast-conserving surgery and older women should be offered and treated with the same options as younger women. As lesions are often impalpable, they must be localised prior to surgery by a wire hook placed under image guidance preoperatively or through radiolabelled markers injected into the lesion. Mastectomy removes all breast tissue with some overlying skin, and usually the nipple. The underlying chest wall muscles are left intact, although radical mastectomy involves the removal of the pectoral muscles. Mastectomy complications include seroma formation (common), skin flap necrosis and infection. Immediate breast reconstruction at the time of mastectomy decreases psychological morbidity. Breast reconstruction should be performed by experienced surgeons and the patient appropriately counselled prior to their operation. Options include direct insertion of a textured silicone breast prosthesis in a small-breasted patient with adequate skin flaps or the use of a myocutaneous flap. In late breast reconstruction, an expander placed under the chest wall muscles is gradually inflated over several months before the placement of a permanent prosthesis. Postoperative radiotherapy and chemotherapy can be utilised after immediate breast reconstruction once the wound has healed. While silicone leakage is rare with newer breast prostheses, there is no evidence that the leaked silicone is carcinogenic or associated with connective tissue disorders. Areola and nipple reconstruction, including tattooing, should be delayed at least 6 months to allow the breast to settle. Some women will require surgery to the contralateral breast (reduction mammoplasty or mastopexy) to facilitate symmetry. A systemic review concluded that postoperative radiotherapy would prevent five additional breast cancer deaths for every 100 treated women at 10 years. Jacobs & Finlayson: Breast Cancer-Early Diagnosis and Treatment of Cancer Series. Adjuvant tamoxifen is recommended for 5 years in the premenopausal age group where the breast cancer mortality rate is reduced by 30% (15-year absolute reduction of 9%) in both axillary lymph node negative and positive patients. The survival advantage exists post-chemotherapy, which should be given prior to commencing tamoxifen. Aromatase inhibitors (anastrozole, letrozole) may be used in a neoadjuvant setting for both oestrogen receptor positive and negative tumours to facilitate breast conservation surgery and also to prevent recurrence. Current trials suggest their survival benefit to be greater than that of tamoxifen. They inhibit aromatase, the enzyme responsible for peripheral conversion of androgens to oestrogens. As they do not have agonist properties at the oestrogen receptors, they are not associated with an increased uterine cancer or thromboembolic risk, but sexual dysfunction and particularly musculoskeletal side effects contribute to a discontinuation rate of up to 20%. Luteinising hormone-releasing agonists are newer agents that seem to confer a survival benefit. Trastuzumab shows efficacy as a single agent, usually given for 2 years, but synergy when used with taxane chemotherapeutic agents. Increasing advances have led to lower radiation doses with fewer severe side effects but moist skin desquamation is to be expected. Cardiac deaths still occur in older women who received high-dose radiation for left-sided breast cancer. Radiation pneumonitis continues to affect up to 2% of patients and post-radiotherapy pain remains an issue for some women. A systemic review has confirmed a reduction in the annual mortality rate of 27% for premenopausal women and 11% for postmenopausal women. Anthracyclinebased regimes appear superior; however, taxanes are used if the cancer is resistant to anthracyclines. Neoadjuvant chemotherapy shows no mortality difference but may allow breast conservation surgery by shrinking a larger tumour. Follow-up is mandatory as the risk of developing contralateral breast cancer is approximately 0. Interestingly, the highest rate of recurrence after a mastectomy is in the first 3 years post-surgery, while recurrence after conservative surgery occurs at a fixed rate per year. Prognostic factors associated with an increased risk of locoregional recurrence are: involved margins (3. Note that multiple other biological markers are under investigation using tissue microarray and proteomics for their clinical significance. BreastScreen Australia recommends screening biannually from 50 until 69 years of age, as the highest survival benefit is seen in women in this age bracket. While screening does cause anxiety, follow-up of women with a false-positive result shows they are no more anxious than an age-matched control. It is estimated that only one extra case of breast cancer every 10 years will occur for every 2 million women screened due to the radiation exposure from mammography. It is clear that two mammographic views (oblique and craniocaudal) improve screening sensitivity and that detection is improved further with repeat reading of films. Treatment involves radical mastectomy and modified chemotherapy regimens if a woman is pregnant. Some women will have delivery expedited to facilitate treatment and this complex decision involves multidisciplinary team care. There is no evidence that pregnancy after breast cancer increases the relapse risk for women. Five-year survival is only 50% and patient neglect plays a significant part, as symptoms may have been present for months or years prior to hospital attendance. Primary treatment is adjuvant or neoadjuvant chemotherapy then radiotherapy, as mastectomy has a high local recurrence rate, although successful neoadjuvant therapy sometimes facilitates surgery months later. The average period of survival after metastasis is 18 to 24 months; however, aggressive hormone-negative tumours are associated with much shorter survival times. Metastatic hormone sensitive tumours may be kept indolent by various anti oestrogen regimes. Chemotherapy is recommended for symptomatic patients only, as there is no evidence that treating asymptomatic metastatic disease increases survival. First-line chemotherapy achieves response rates of approximately 50% with symptom palliation and improved quality of life. Sequential single-agent chemotherapy, usually preferred as combination chemotherapy, has higher toxicity and does not show a survival advantage. Marrow infiltration may reduce any of the blood progenitor cell lines and chemotherapy is recommended. Malignant pleural effusions are common and most will re-accumulate if simply aspirated, hence pleurodesis is preferred. The potentially fatal complication of hypercalcaemia is treated with intravenous hydration and bisphosphonates. Central nervous system metastases are common and isolated brain involvement may be treated with high-dose steroids, surgical excision and radiotherapy. It goes without saying that these patients have a significant psychological burden and are best managed by a multidisciplinary team. Assessment of clinical palpation of the axilla as a criterion for performing the sentinel node procedure in breast cancer. Value of breast imaging in women with painful breast: observational follow up study. Breast cancer and hormone replacement therapy: collaborative reanalysis of data form 51 epidemiological studies of 52 705 women with breast cancer and 108 411 women without breast cancer. Predictive factors associated with axillary lymph node metastases in T1a and T1b breast carcinomas: analysis in more than 900 patients. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomized trials. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. Effect of radiotherapy after breastconserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of 22) 23) 24) 25) 26) 27) 28) 29) 30) 31) individual patient data for 10 801 women in 17 randomised trials. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomized trials. Pregnancy after treatment of breast cancer-a population based study on behalf of Danish Breast Cancer Cooperative Group. The value of estrogen and progesterone receptors in the treatment of breast cancer. Vulvar pain in association with an essentially normal-appearing vulva is termed vulvodynia. The most common causes of pruritus vulvae are the dermatoses and fungal infections of the vagina and vulva. The most common causes of chronic vulvar pain are the dermatoses where severe · · · · scratching can cause skin splitting or where the dermatosis is characterised by pain. When there is vulvar pain with no obvious cause evident and the vulva looks essentially normal, this is called vulvodynia and is a common cause of entry dyspareunia and even apareunia. Other dermatoses that occur elsewhere on the body can also occur on the vulva such as psoriasis, herpetiform lesions and fixed-drug eruptions and these are managed along the usual lines. However, up to 20% of women may be asymptomatic and the diagnosis is usually suspected due to the characteristic appearance of the vulva. It occurs in 1 in 80 women and usually affects older women (peri and postmenopausal), although it is important to realise that it can occur at any age, even in children and infants. The condition often extends to include the perianal skin resulting in pruritus ani. With time, the collagen fibres contract resulting in fibrosis and anatomical distortion. This results in fusion of the labia minora to the labia majora with obliteration of the interlabial space (labial resorption), introital stenosis making sexual penetration difficult or even impossible, and burying of the clitoris resulting in reduced sensation. This term is no longer used as the epidermis is not atrophic at all and actually has a high cell turnover. In the early phase of the condition, the patient experiences episodes of pruritus which often resolve spontaneously after 1 to 2 weeks. In young women, it is often mistakenly diagnosed as Candida infection as the pruritic episodes will often resolve when anti-Candida therapy is used, but this is just coincidental. Ignoring the condition in children and young women can lead to significant vulvar scarring and permanent introital stenosis. The condition is lifelong, and in the advanced stages the vulva is distorted with loss of the labia minora and clitoris, and introital stenosis and patchy pigmentation throughout. Management consists of avoidance of local irritants and the application of a high-potency corticosteroid preparation, usually as an ointment. This should be used frequently until the symptoms are brought under control and then used on a prophylactic basis to prevent further flare-ups. With aggressive use of topical corticosteroids to eliminate pruritus, this risk should be reduced. The condition usually responds to the removal of irritant factors (soaps, pads, panty liners, deodorants, etc. Rustcoloured patches are seen both on the vulva and in the vagina, occasionally with ulceration, and these are extremely tender. If the condition is confined to the vagina, the resultant discharge may be helped with the long-term application of hydrocortisone cream per vaginam, although this condition often requires systemic corticosteroids to bring it under control and then high-potency topical corticosteroids to maintain control. It is usually bilateral, although it can be focal and, if so, definitely requires biopsy. On the vulva, the lesions are well demarcated with a distinct border and are usually quite erythematous in colour but often lack the scaliness that is seen in lesions elsewhere. Originally described as often occurring in patients with gonorrhoea, this association is now extremely rare. The preferred management is surgery (under general anaesthetic) and this involves draining the abscess and creating a new permanent opening using the technique of marsupialisation. Herpes genitalis this is the most common cause of recurring painful lesions on the vulva. The lesions usually present with clusters of painful vesicles, always in the same location, and then form superficial ulcers. They are acquired by sexual contact and respond well to a short course of oral antiviral therapy. If they are recurrent, then long-term prophylaxis against further outbreaks is achieved by continuous low-dose oral antiviral therapy. Lichen planus this is a potent cause of vulvar pain and has been discussed in the previous section. This condition is less common than lichen planus but has a very similar clinical presentation. Patients present with painful erythematous lesions scattered throughout the vulva and vagina. It is regarded as an autoimmune disorder and the characteristic histological feature is a heavy infiltration of plasma cells.
This was likely due to a prolonged delivery arthritis pain and stress buy feldene american express, with impaction and/ or cord tightly around neck arthritis pain medication meloxicam buy feldene line. This pustular-erythematous eruption on the face is consistent with the benign rash of erythema toxicum chronische arthritis definition purchase cheapest feldene. Congenital herpes simplex virus infection: two unique cutaneous presentations associated with probable intrauterine transmission rheumatoid arthritis case study buy generic feldene canada. While it may appear benign initially arthritis foundation gout diet order 20 mg feldene, progression to central nervous system disease and/or disseminated (multi-organ) disease can occur. Pustules may be present from birth in the condition of congenital candidal infection, or appear later particularly with Staphylococcus aureus skin infection. The differential diagnosis needs to include the much more common condition, erythema toxicum, which is described earlier. Congenital dermal melanocytosis (Mongolian spot) is the most frequently encountered newborn pigmented lesion. It presents as a large pigmented macule with indefinite borders, often distributed over the lower back. It appears as a red area on the upper eyelids, root of nose, upper lip and/or nape of neck. These lesions are benign, often fade with time but nonetheless may case maternal anxiety. A capillary malformation (port-wine stain or naevus flammeus) is a deep vascular naevus, usually found on the face, often in the distribution of a division of the trigeminal nerve. Although commonly benign, there is a rare but important risk of associated neuroepileptic syndromes. It becomes larger for several months and then regresses spontaneously, usually by 3 years of age. Treatment is necessary if the haemangioma distorts tissue such as the eyelid or airway. Occasionally, very large haemangioma leave redundant skin or scar tissue after regressing. Large haemangiomas (often separately classified) may be associated with platelet destruction and thrombocytopenia (Kasabach Merritt phenomenon). Fat necrosis is an indurated area of skin where pressure has been applied over a protracted period. While not always warranted for the common and benign skin issues, a paediatric or dermatological opinion may assist families to decide on a desired course of action. Following this general examination, the systematic examination moves to the hands, followed by the arms, head, face, neck, thorax, abdomen, hips, legs and feet. This has the advantage that, unlike a systems-oriented approach to examination, there will be little need to backtrack during the examination. It can be accomplished in a relatively short time without undue disturbance to the newborn and it is unlikely that abnormalities will be missed. A caveat to this approach includes auscultation of the heart early in the examination. In this instance, a more settled and quiet neonate will better facilitate cardiac auscultation. Treatment with oral propranolol (utilising the anti-angiogenesis effect of Я-agonists) is increasingly being administered. Often supernumerary digits are found joined to the ulnar side of the hand by a thin pedicle of tissue without bone (post-axial polydactyly). Ligature in the immediate newborn period is associated with complications and no longer recommended. Pre-axial (radial) polydactyl may be associated with syndrome diagnoses and warrants further assessment. The cardiovascular examination, which is undertaken when the thorax is examined, may be initiated by palpation of the brachial artery during examination of the arm. GraspandMororeflexes this is an opportune time to elicit the grasp and Moro reflexes and check head control when pulled from supine. Pulling the newborn from the wrists allows an assessment of head control to be made. In this starting position, the lower back, buttocks and legs remain on the cot surface. This may suggest abnormalities of connective tissue, or be part of a syndromic diagnosis. Acquiredpathology Failure of normal spontaneous movement or failure to move symmetrically may suggest a fracture of the humerus or clavicle after a difficult delivery or the presence of a deep tissue or bone infection. The proportionally shorter legs and arms seen in this infant are consistent with achondroplasia. Abnormalities of the Moro reflex occur symmetrically if there is central nervous system depression or neuromuscular disease, or unilaterally in conditions such as fracture of the clavicle or a brachial plexus injury. Remember, a watchful mother is often nearby and reassurance and explanation is required prior to conducting the Moro assessment. Elicitation of these reflexes, along with a general appraisal of tone, strength, level of activity and alertness, form an appropriate neurological screening examination. The finding of macrocephaly, usually defined as a head circumference > 97th percentile for gestational age, requires that hydrocephalus be ruled out as a possible cause by cranial ultrasound imaging. Shapeandmoulding A newborn cranial vault is made up of distinct separate bones or plates. There may be overlapping of the individual cranial vault bones due to moulding, facilitating movement through the birth canal. The triangle-shaped posterior fontanelle can often be hard to palpate in the immediate postnatal period (due to movement and moulding of the separate cranial vault bones). However, appropriate paediatric follow-up over time may prevent unnecessary cranial radiation. Extra-cranialswellingsorhaematomas Classification of extra-cranial fluid collections or haematomas is important based on the various causes and blood-fluid collections that can occur along certain anatomical planes. Caputs are characterised by tissue oedema and are often associated with cranial vault moulding. They can be due to prolonged engagement in the birth canal or vacuum-assisted delivery. Cephalohaematomas rarely expand after birth; they may completely resolve, or calcify leaving a minor convexity to the cranial vault. A subgaleal haemorrhage occurs due to shearing of blood vessels outside of the periosteum, below the epicranial aponeurosis (galea aponeurotica). They can occur spontaneously, but vacuum-assisted delivery increases the risk significantly. If a cranial swelling is evident, close observation is required, especially after an instrumental delivery. If a subgaleal haemorrhage is suspected, regular cardiovascular monitoring and prompt senior neonatal advice is required. Spina bifida is a much more common type of neural tube defect 608 Chapter 66 Assessment of the Neonate involving failure of fusion of the neural tube, usually the lower spine. Increasing awareness of the role that folate supplementation plays in preventing neural tube defects, including mandatory folate fortification of flour and bread (common in many jurisdictions around the world; commenced in Australia in 2009), has decreased the overall prevalence of neural tube defects. Several syndromes are associated with underdevelopment of the auricle or a low positioning (low-set ears) of the auricle on the head. Low-set is defined as when the top of the ear helix falls below a horizontal line that is imaged through the middle of the eyes and outer canthus. Pre-auricular pits or skin tags may be benign, familial or associated with deficits of auditory acuity. Unilateral tearing suggests a blocked tear duct, which almost always resolves spontaneously. Pupillary reflexes to light should be present and elicited (both directly and consensually) in the term newborn. Bilateral cleft lip and palate may be associated with a more generalised midline defect with abnormalities of the brain and pituitary gland. The roof of the mouth should be inspected to detect a cleft but must also be palpated to exclude a sub-mucosal defect of the palate. Excessive secretions should alert the examiner to the possibility of a problem with deglutition (inability to swallow): oesophageal atresia, central neurological depression or neuromuscular disease. A ranula presents as a mass beneath the tongue and is due to partial blockage of the submandibular duct. Other oral lesions are rare; however, if present they may warrant further expert opinion because they may be derived from the thyroid gland, be tumours or interfere with the patency of the airway. If there is nothing abnormal between the light of the ophthalmoscope and the retina then a bright orange-red view is obtained through the pupil. Provided the remainder of the examination is normal, this common finding is often attributable to a prolonged birth or difficult extraction. The tongue may be large in Beckwith-Wiedemann syndrome, which may be associated with hypertrophy of limbs and organs as well as severe hypoglycaemia. However, the extent in which tongue-tie leads to clinically significant symptoms is not supported by high-quality evidence. This has lead to a diversity of opinion (and hence management practices) between professional groups such as midwives, lactation nurses, paediatricians, speech pathologist and surgeons. When counselling parents, this diversity in opinion, and hence management, should be acknowledged. The most serious is choanal atresia, which is an abnormal membranous cover in the nasopharynx which causes airway obstruction and respiratory distress. Since the neonate prefers to breathe through the nose, severe problems result if the choanal atresia is bilateral. The diagnosis is made if a neonatal airway suction catheter or feeding tube cannot be passed further than 1 to 2 cm through the affected nostril. Sternomastoidtumour A sternomastoid tumour is due to a haematoma of the sternomastoid muscle and usually presents as a tendency for the newborn to favour head rotation towards the side of the tumour. Assessment for the presence or absence of associated palatal defects is important. Physiotherapy by passive and active stretching of the muscle is indicated, although the majority will improve spontaneously. Hepatomegaly the normal liver edge can often be palpated in the newborn period, up to one or two finger-breadths below the right costal margin. Faster rates, which are often associated with sternal recession and use of the accessory muscles of respiration, define respiratory distress, which is discussed in Chapter 70. Stridor should not be present and suggests a laryngeal cause of airway obstruction. Enlargement may be associated with intrauterine infection or a haematological condition causing extramedullary haemopoiesis. Umbilicalcord the umbilical cord should be clean and contain three vessels: two small but thick-walled muscular arteries and one slightly larger but thin-walled vein. The site through which the umbilical vessels entered the abdomen in fetal life can be palpated as a defect in the linea alba. If an umbilical hernia is present, the bowel contents protrude through this defect, especially during crying or straining. Provided antenatal ultrasounds are normal, and a postnatal assessment is otherwise unremarkable, no specific follow-up is required (although opinions differ as to whether or not postnatal renal assessment is warranted). Breasts Small, firm, discrete swellings below the nipples may signal newborn breast enlargement. This hormoneresponsive condition is common in the newborn, particularly initially and in some breastfed infants. Cardiovascularexamination the quality of the pulse should be palpated at the cubital fossa. More commonly, however, a weak or absent pulse in the lower limbs may be associated with coarctation of the aorta. Prompt detection of a critical coarctation prior to closure of the ductus arteriosus can be life-saving. The normal heart rate is usually between 100 and 170 bpm but may be lower if the newborn is in deep sleep or higher if crying. The praecordial impulse is palpated to determine that it is on the left side and of normal character with no thrills. In the male, the spermatic cord is no more than several millimetres in diameter and should be palpable below the external inguinal ring. If a hernia is palpated, an attempt should be made to reduce it through the inguinal canal. Inguinal hernias, unlike umbilical hernias, require prompt operative treatment due to the risk of bowel strangulation. Femaleexternalgenitalia In the female, the labia minora are more prominent than later in life. Enlargement of the clitoris or ambiguous genitalia require close inspection and documentation as well as delicate discussions with the family. Divarication of 612 Chapter 66 Assessment of the Neonate Hymenal skin tags are not uncommon and regress over several months. Maleexternalgenitalia the foreskin is normally adherent to the glans and cannot be retracted until 3 to 6 years of age. Forcible attempts to do this may result in scarring of the tissue at the tip of the foreskin, which may lead to phimosis later in life. Importantly, phimosis is rare and does not often occur in the early childhood years. This has occurred in response to changing cultural and societal norms with emerging contention around circumcision. Many families often decide prenatally whether they wish circumcision to be performed. Reasons for this are based on cultural and religious expectations as well as personal preference and beliefs. Importantly, there are no medical indications for circumcision in the newborn period.
The diagnosis is confirmed by laparoscopic visualization of filmy perihepatic adhesions arthritis treatment glucosamine chondroitin generic feldene 20 mg on-line. The apex of the triangle flap is then brought down to the lower apex of the ureterotomy and a 5-0 chromic stay suture is placed rheumatoid arthritis herpes zoster order generic feldene canada. Flank "bulge" is not a true hernia and is believed to be due to laxity of the transversus and oblique abdominal wall muscles osteoarthritis in fingers discount feldene on line, caused by injury to the intercostal nerves rheumatoid arthritis diet in tamil purchase feldene us, in particular the 11th intercostal arthritis pain aspirin order feldene 20 mg line, and accentuated in part by unopposed contraction of contralateral musculature. Care should be taken to avoid injury to the intercostal nerves during incision and closure. Lesions are multicentric and whitish to yellowish in color with slightly elevated papules and plaques with sizes ranging from 1Â3 mm. Most patients are asymptomatic but some consider receiving treatment for cosmetic reasons since the lesions do not resolve spontaneously. It is thought to result embryologically from an incomplete breakdown of the wall between the ectoderm and the urethra being formed by the urethral folds. It is a common anatomic finding with rare symptoms, including dysuria, gross hematuria, spotting of blood, or hematospermia. Amazonian parasitic catfish (Candiru) and leeches have also been reported to enter the urethra while bathing in a river. Lacuna magna in 6 boys with postvoid bleeding and dysuria: Alternative approach to treatment. The classic patient will present with the inability to void for an entire day and will have a large volume of urine in her bladder. For diagnosis, a retained urine volume of 1 L or more and lack of sensation or urgency is necessary. Systemic therapy (bisphosphonate or denosumab) therapy has also been shown to play a role in the prevention of osteoporosis and reduce fracture risk. The diameter in millimeters of the instrument is determined by dividing the French size by 3 (eg, an 18 Fr catheter has a diameter of 6 mm). The system was introduced by a 19th century French medical instrument manufacturer. Osteoporosis management program decreases incidence of hip fracture in patients with prostate cancer receiving androgen deprivation therapy. Frequency is further categorized as 1 of the storage symptoms (experienced during the bladder filling phase or storage phase of micturition), as opposed to a voiding or postmicturition symptom. It entails ligating the spermatic vessels and hinges on the premise that the testicle will survive from the vasal and cremasteric collaterals. The operation was originally described as a 2-stage procedure in which the vessels are divided, and then 6 mo later the testicle is brought down to the scrotum, after collaterals have become well developed. Both techniques have a fairly high success rate, but 2-stage is reported to have a slightly better success rate (85% for 2-stage vs. Measurement of testis size in mentally retarded males has been suggested as a simple screening test for this condition. Because this term is so nonspecific, it is not a currently accepted meaningful term for diagnosis or treatment planning. In childhood, hypercalciuria was theorized and in adults, fastidial organisms were once thought to be the cause. Long-term outcome of laparoscopic Fowler-Stephens orchiopexy in boys with intra-abdominal testis. Impaired drainage on delayed films or isotope renography must be confirmed before surgery. The frequency and frequency dysuria syndromes of childhood: Hypercalciuria as a possible etiology. Parasitic infections (filariasis, schistosomiasis) can also induce inflammatory changes in the cord (see also Section I: "Spermatic Cord Mass and Tumors. It is caused by a failure of separation of the ureteric bud from the mesonephric duct that leads to persistence of the Gartner duct, often with cystic dilation. The Gartner duct is associated with mullerian duct developmental anomalies and Ð with abnormal ureteric development, such as ureteric ectopia. Abnormal development of the ureter also results in the maldevelopment, ectopic kidney, or absence of the ipsilateral kidney. The usual presentation is an anterior vaginal wall mass with ipsilateral renal dysgenesis with or without urinary incontinence. Differential diagnoses include ectopic ureterocele, urethral diverticulum, urethral tumor, Skene gland cyst or abscess, and vaginal wall cysts or tumors. Treated surgically, depending on anatomic anomalies, including transvaginal or transabdominal excision of the Gartner duct and closure of any associated urinary fistula; reconstruction of bladder neck and urethra; reimplantation of ipsilateral and/or contralateral ureter; or removal of nonfunctioning renal unit and ectopic ureter. During laparoscopy, sperm and eggs are mixed and transferred into 1 of the fallopian tubes, allowing in vivo fertilization. The correlation between size of renal cell carcinoma and its histopathological characteristics: a single center study of 1867 renal cell carcinoma cases. Other organisms can involve the kidney through disseminated infection (eg, Aspergillus sp. Associated predisposing factors include catheters, antibiotics, diabetes mellitus, hospitalization, and immunocompromised states. Urinary colonization is usually asymptomatic, whereas invasive fungal infection of bladder may have irritative voiding symptoms. It is varied in appearance and malignant potential, with prognosis and behavior depending on histology. Physical arousal caused by this syndrome can persist for extended periods of time. Orgasm can sometimes provide temporary relief, but within hours the symptoms return suddenly. Amphotericin B bladder irrigation is recommended only for fluconazole-resistant organisms (eg, C. Adult-type ganglioneuroblastoma in the adrenal gland treated by a laparoscopic resection: Report of a case. It does not metastasize, but can locally recur after resection and be locally aggressive. Histologically, the lesion is composed of ganglion cells with abundant cytoplasm and large nuclei. In males, piercings include the penile glans, shaft, urethra, scrotum, and combinations of these. Chancroid is treated with a single oral dose of azithromycin, or a single intramuscular dose of ceftriaxone, or oral erythromycin for 7 days. Primary syphilis is treated with a single dose of intramuscular penicillin G or a single dose of oral azithromycin in a penicillin allergic patient. Skin loss can less commonly occur as a result of trauma, usually blunt; however, penetrating trauma can also result in skin loss. It can discriminate between women with interstitial cystitis, those with incontinence, and those with none of these diagnoses. In the case of skin loss to due to debridement for infection, the infection should be stable prior to reconstruction being performed. In the case of penile skin loss in an uncircumcised male, a flap using redundant foreskin may be harvested to address a proximal defect. Split-thickness skin grafts can be used to address both penile and scrotal skin defects. Vacuum-assisted closure therapy has been effective in early management with skin grafts (see also Section I: "Scrotum and Testicle, Trauma. Validation of a modified National Institutes of Health chronic prostatitis symptom index to assess genitourinary pain in both men and women. Patients present with infertility, and usually with small to normal testes and azoospermic semen specimens. Histologically, Sertoli cells line the seminiferous tubules with a complete absence of germ cells and normal interstitium. Aplasia may represent the endpoint of various etiologies, resulting in this histologic appearance. Their role in the definitive management of patients with prostate cancer is currently evolving. They are most commonly a manifestation of sexually transmitted infections, including chancroid, genital herpes, lymphogranuloma, and primary syphilis. Assessment of the testicular cytology by fine-needle aspiration and the imprint technique: Are they reliable diagnostic modalities? The clinical assessment of gestational age or duration of pregnancy reflects the "menstrual age. Rapid determination of gestational age in the delivery room includes assessment of soles of the feet, breast nodules, earlobe, hair, and the external genitalia of males. Babies born 36 wk and earlier the testes are usually partially descended, the scrotum is small with very few rugae. Term infants (39 wk and beyond) should have the testes fully descended, the scrotum should appear normal sized with prominent rugae. A Stamey needle is delivered through a stab incision at the upper border of the pubis, then transferred under digital guidance through the anterior vaginal wall at the level of the bladder neck. Using a flank incision, the kidney is exposed and freed at the upper pole, lower pole and posteriorly. The renal pelvis is incised and the incision can be continued to include the calices to allow for removal of more significant calculi. Evaluation of a minimal-incision pubovaginal suspension as an adjunct to other pelvic-floor surgery. Its presence is associated with biochemical recurrence and adverse pathologic features such as seminal vesicle invasion, extraprostatic extension, and positive surgical margins. The unit is rotated 180 to allow anastomosis of the reduced end of the ascending colon to the urethra and the ureters to the terminal ileum. The external and internal obliques and the transversalis muscle are bluntly opened along their fibers. After transecting the transversalis fascia, the peritoneum is swept medially to expose the ureter at its midsection. Should the Gleason grading system for prostate cancer be modified to account for high-grade tertiary components? Tertiary Gleason pattern 5 in Gleason 7 prostate cancer predicts pathological stage and biochemical recurrence. The principle involves advancing the ureters across the trigone to the midline such that both ureteral orifices are juxtaposed. A single incision is made in the trigone mucosa, which will serve to join traction sutures from each ureter that are anchored in the midline. A muscle sparing modified Gibson incision for hand-assisted retroperitoneoscopic nephroureterectomy and bladder cuff excisionÂan approach through a window behind the rectus abdominus muscle. Donald Gleason between 1969 and 1974, in which prostate cancer mortality data were correlated to low-magnification architectural patterns of prostate carcinoma. To account for variations within tumors, 2 grades are recorded: the predominant, or primary, grade and the less extensive, or secondary, grade. The Gleason score is a strong independent predictor of cancer behavior and treatment outcome for prostate cancer patients. Pattern 3 is separated from pattern 4 because this separation usually distinguishes Gleason score 6 from Gleason score 7 tumors, with the latter having a significantly worse prognosis. The glands are fairly large, round or oval, and are approximately equal in size and shape. Well-circumscribed nodule of single, separate glands with the glands more loosely arranged and not as uniform as in pattern 1. Minimal invasion by neoplastic glands into the surrounding benign prostatic tissue. The cells are smoothly rounded or oval with open lumens and are not angular, as seen in pattern 3. These small glands are often called microglands and are usually smaller than Gleason pattern 1 or 2 glands. The small glands of pattern 3, in contrast to small poorly defined glands of pattern 4, are distinct glandular units and 1 should be able to draw an imaginary circle around each of them. Cribriform glands may also be Gleason pattern 3, with these glands being slightly larger than benign glands and having regular outer contours. Cribriform pattern 3 must be separated from cribriform pattern 4, intraductal cribriform proliferations, and prostatic duct adenocarcinoma. They are fused, poorly defined with only occasional lumen formation, or cribriform. Fused glands are chains, nests, or masses of glands that are no longer completely separated by intervening stroma. Fused glands contain rare strands of residual stroma that may give the appearance of partial separation of the glands. Cribriform glands of pattern 4 are either large cribriform glands (cribriform sheets) or small cribriform glands with irregular infiltrating borders. The small cribriform glands with irregular infiltrating borders of pattern 4 must be distinguished from cribriform pattern 3, in which the small cribriform glands have regular borders. Fragments of cribriform carcinoma in needle biopsies of the prostate imply a cribriform cancer and are designated pattern 4. It is controversial whether cribriform glands of cancer that otherwise would be considered Gleason pattern 4 should be considered Gleason pattern 5 if comedonecrosis is present. Separating poorly defined pattern 4 glands from cords and nests of tumor with virtually no glandular differentiation or with only vacuoles is a problem, but usually not critical because any combination of the 2 patterns will lead to a Gleason score of 8Â10, all of which are poorly differentiated (Image). Presents most commonly in childhood with bilateral flank masses, which are large kidneys with many cysts. This change contributes to obliteration of capillary lumina of the glomerular tuft, a feature of glomerulosclerosis.
Buy feldene 20 mg on line. What are some non-surgical treatment options for foot and ankle arthritis?.
References
- Dimitrakov J, Tchitalov J, Zlatanov T, et al: Corticotropin-releasing hormone perturbations in interstitial cystitis patients: evidence for abnormal sympathetic activity, Urology 57(6 Suppl 1):128, 2001.
- Johnson PC. Autoregulation of blood flow. Circ Res. 1986;59: 483-495.
- Watanabe Y, et al. Dopamine selectively induces migration and homing of naive CD8+ T cells via dopamine receptor D3.
- Hald T, Mygind T: Control of life-threatening vesical hemorrhage by unilateral hypogastric artery muscle embolization, J Urol 112:60-63, 1974.
- El-Abbadi M, Giachelli CM: Mechanisms of vascular calcification. Adv Chronic Kidney Dis 2007;14:54-66.