
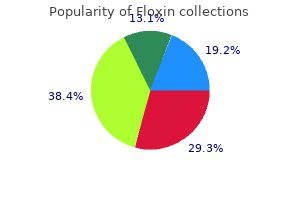
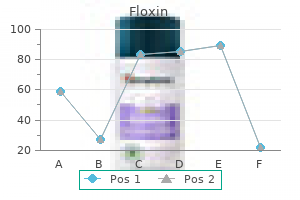
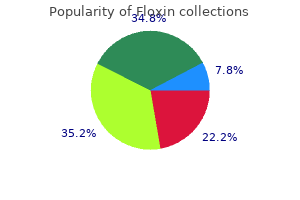
Floxin
| Contato
Página Inicial
Erik D. Maki, PharmD, BCPS
- Associate Professor, College of Pharmacy and Health Sciences, Drake University, Des Moines, Iowa
The area is cleaned aseptically antibiotic vs antiviral purchase floxin us, and a 1percent lidocaine anesthetic track is injected along the planned insertion path infection without antibiotics generic floxin 200 mg buy on-line. The insertion device is grasped at its gripper bubbles found on either side antibiotic resistance target protein discount floxin 200 mg online, and the needle cap is removed outward bacteria brutal purchase 400 mg floxin free shipping. Once the complete bevel is subcutaneous antibiotics for boils cheap floxin 200 mg, the needle is quickly angled downward to lie horizontally. The proximal end of the implant is depressed with a finger to allow the distal end to bulge up toward the skin. After anesthetizing the skin over this bulge, the skin is incised 2 mm toward the elbow along the long axis of the arm. Once visible, the distal end of the implant is grasped with a hemostat and removed. If present, superficial adhesions surrounding an implant may be dissected away with hemostat tips placed into the incision. As other effects, cervical mucus is thickened to retard sperm passage, and atrophy renders the endometrium unfavorable for implantation. Fertility is restored rapidly following cessation of progestin-only contraception. For all progestin-only methods, irregular or heavy uterine bleeding is a distinct disadvantage. It is the most frequently reported adverse event leading to method discontinuation. Fortunately, with prolonged use, progestins induce endometrial atrophy, which leads to sustained amenorrhea. Most progestin-only contraceptive methods do not significantly affect lipid metabolism, glucose levels, hemostatic factors, liver function, thyroid function, or blood pressure (Dorflinger, 2002). Progestin-only methods do not impair milk production and are an excellent choice for lactating women. There are no increased risks of genital tract, liver, or breast neoplasia (Samson, 2016; Wilailak, 2012; World Health Organization, 1991a,b, 1992). Weight gain and bone fracture are not prominent side effects of this contraceptive group, except for depot progesterone, discussed on page 693 (Lopez, 2012a, 2013a). Functional ovarian cysts develop with a greater frequency in women using progestin-only agents, although they do not usually necessitate intervention (European Society of Human Reproduction and Embryology, 2001; Hidalgo, 2006; Nahum, 2015). Women with depression may be prescribed these methods, but surveillance following initiation is reasonable. Progestin Contraindications these methods are ideal for most women, but contraindications and cautions are associated with a few conditions listed in Table 38-2. First, manufacturer prescribing information lists thrombosis or thromboembolic disorders as contraindications (Merck, 2016a; Pfizer, 2015a,b). Moreover, evidence does not link progestin-only methods with thromboembolism, stroke, or cardiovascular disease (Mantha, 2012; Tepper, 2016b; World Health Organization, 1998). Second, for many progestin products, manufacturers note prior ectopic pregnancy as a contraindication. Progestin-only injectables and pills are considered very effective, yet second-tier agents, due to the need for increased patient compliance. Combination Hormonal Contraceptives Mechanism of Action Actions of combination hormonal contraceptives are multiple, but the most important effect is suppression of hypothalamic gonadotropin-releasing factors. To promote cycle control, estrogen stabilizes the endometrium, which prevents intermenstrual bleeding-also known as breakthrough bleeding. The net effect is an extremely effective yet highly reversible method (Mansour, 2011). Combination Oral Contraceptive Pills Composition these pills are the most frequently used reversible birth control method in the United States. In a 2006 to 2010 survey, 16 percent of contracepting women in the United States were using these (Daniels, 2015). The American College of Obstetricians and Gynecologists (2015a) supports the use of either branded or generic preparations. Unwanted effects most often attributed to the estrogen component include breast tenderness, weight gain, nausea, and headache. Thus, these progestins bind variably to progesterone, androgen, glucocorticoid, and mineralocorticoid receptors. These affinities explain many pill-related side effects and are often used to compare one progestin with another. To avoid these effects, antiandrogenic progestins have been introduced and include dienogest and nomegestrol acetate. Despite these pharmacological differences, the true advantage of one progestin over another is less apparent clinically (Lawrie, 2011; Moreau, 2007). Drospirenone displays antiandrogenic activity, provides an antialdosterone action to minimize water retention, and has antimineralocorticoid properties that may, in theory, cause potassium retention and hyperkalemia (Krattenmacher, 2000). Thus, it is avoided in women with renal or adrenal insufficiency or with hepatic dysfunction. Moreover, serum potassium level monitoring is recommended in the first month for patients chronically treated concomitantly with any drug associated with potassium retention. Currently, the lowest acceptable dose is limited by the ability to prevent pregnancy and to avoid unacceptable breakthrough bleeding. Thus, the daily estrogen content varies from 10 to 50 g of ethinyl estradiol, and most contain 35 g or less. In addition, Beyaz has a form of folate-levomefolate calcium-within both its active and placebo pills. In others, the dose frequently is varied, and term biphasic, triphasic, or quadriphasic pill is used depending on the number of dose changes within the cycle. In general, phasic pills were developed to reduce the total progestin content per cycle without sacrificing contraceptive efficacy or cycle control. The theoretical advantage of a lower total progesterone dose per cycle, however, has not been borne out clinically (Moreau, 2007). Cycle control also appears to be comparable among monothrough triphasic pills (van Vliet, 2011a,b,c). Administration Hormones are taken daily for a specified time (21 to 81 days) and then replaced by placebo for a specified time (4 to 7 days), which is called the "pill-free interval. With the trend toward lower estrogen doses to minimize side effects, follicular development and ovulation may occur. To counter this, the active-pill duration in some formulations is extended to 24 days. In comparison, these 24/4 regimens perform similarly to higher-estrogen-dose 21/7 regimens (Anttila, 2011; Marr, 2012). Alternatively, longer durations of active hormone, designed to minimize the number of withdrawal episodes, have similar efficacy and safety profiles as more traditional administration (Edelman, 2014). These extended-cycle products produce a 13-week cycle, that is, 12 weeks of hormone use, followed by a week for withdrawal menses. The product Amethyst provides continuous active hormone pills for 365 days each year. Such extended or continuous regimens may be especially suited for women with significant menstrual symptoms (Mendoza, 2014). With the more traditional "Sunday start," women begin pills on the first Sunday that follows menses onset, and an additional method is needed for 1 week to prevent conception. If menses begin on a Sunday, then pills are begun that day and no supplemental method is required. Similar same-day initiation can be implemented with the contraceptive vaginal ring or patch (Murthy, 2005; Schafer, 2006). If one dose is missed, the missed pill is taken immediately; the scheduled dose for that day is taken on time; and then daily pills are continued. If two or more doses are missed, the most recent missed pill is taken immediately; the scheduled dose for that day is taken on time; and an effective barrier technique used for 7 days while daily pills are then continued (Curtis, 2016a). If withdrawal bleeding fails to occur during the pill-free interval, a woman should continue her pills but seek attention to exclude pregnancy. It does not reflect contraceptive failure and typically resolves within one to three cycles. If unscheduled bleeding persists, those with bleeding during the first part of a pill pack may benefit from an increase in the estrogen dose, whereas those with bleeding during the second part may improve with a higher progestin dose (Nelson, 2011). Some studies point to lowered hormone bioavailability, but overall efficacy remains high (Nakajima, 2016; Westhoff, 2010; Yamazaki, 2015). With the transdermal patch method, however, evidence is more robust that obesity may alter pharmacokinetics and lower efficacy, as discussed on page 692. Oral contraceptives are not atherogenic, and their effect on lipids is clinically inconsequential for most women (Wallach, 2000). For those with multiple additional risk factors for vascular disease, alternative contraceptive methods are recommended. First, fibrinogen and many of the clotting factor levels rise in direct proportion to the estrogen dose and may lead to thrombosis. Regarding carbohydrate metabolism, current low-dose formulations have minimal effects in women who do not have diabetes (Lopez, 2014). For nonsmoking women younger than 35, the risk of stroke is extremely low (World Health Organization, 1996). The evidence for stroke risk in migraineurs without aura is less clear (Etminan, 2005; Schürks, 2009). Also, in women with multiple cardiovascular risk factors, which include smoking, hypertension, older age, and diabetes, the risk for myocardial infarction outweighs the benefits of this method. However, for those without these risks, low-dose oral contraceptives are not associated with an increased risk of myocardial infarction (Margolis, 2007; World Health Organization, 1997). These clearly are estrogen-dose related, and rates have substantively declined with lower-dose formulations containing 10 to 35 g of ethinyl estradiol. Desogestrel and gestodene are also implicated and carry similarly elevated risks (Stegeman, 2013; Vinogradova, 2015). In fact, a protective effect against ovarian and endometrial cancer has been shown (Collaborative Group on Epidemiological Studies of Ovarian Cancer, 2008; Tsilidis, 2011). Following 10 or more years, risk returns to that of never users (International Collaboration of Epidemiological Studies of Cervical Cancer, 2007). Major studies show no risk or a small risk among current users, which drops with time following cessation (Collaborative Group on Hormonal Factors in Breast Cancer, 1996; Hannaford, 2007; Marchbanks, 2002). Moreover, no evidence supports concern for greater risk of hepatocellular cancer (Maheshwari, 2007). Rates of colorectal cancer appear to be reduced in ever users (Bosetti, 2009; Luan, 2015). But in those with severe decompensated disease, all hormonal methods are avoided (Kapp, 2009a). Chloasma, which is hyperpigmentation of the face and forehead, is more likely in women who demonstrated such a change during pregnancy (Chap. Transdermal Patch the Ortho Evra patch contains ethinyl estradiol and the progestin norelgestromin. It has an inner layer containing an adhesive and hormone matrix, and a waterresistant outer layer. Thus, women can wear the patch in bathtubs, showers, swimming pools, saunas, and whirlpools without decreased efficacy. The patch may be applied to buttocks, upper outer arm, lower abdomen, or upper torso, but the breasts are avoided. Because the hormones are combined with the adhesive, improper skin adherence will lower hormone absorption and efficacy. Therefore, if a patch is so poorly adhered that it requires reinforcement with tape, it should be replaced. Although a patch is ideally worn no longer than 7 days, hormone levels remain in an effective range for up to 9 days. However, the patch has been associated with a higher thromboembolism risk in some but not all studies (Cole, 2007; Jick, 2010; Lidegaard, 2011). Obesity-90 kg or greater-may be associated with a higher risk for patch contraceptive failure (Janssen Pharmaceuticals, 2015; Zieman, 2002). Finally, application-site reaction and breast tenderness are more frequent during initial cycles in patch wearers (Urdl, 2005). Transvaginal Ring the NuvaRing is yet another form of combination hormonal contraception and is a flexible intravaginal ring. The ring is constructed of ethinyl vinyl acetate, and it measures 54 mm in diameter and 4 mm in cross section. During insertion, the ring is compressed and threaded into the vagina, but no specific final orientation within the vagina is required. Its core releases ethinyl estradiol and the progestin etonogestrel, which are absorbed across the vaginal epithelium. Before being dispensed, the rings are refrigerated, and once dispensed, their shelf life is 4 months. The ring is placed within 5 days of menses onset and, after 3 weeks of use, is removed for 1 week to allow withdrawal bleeding. Contraception will still be afforded if a ring is left in place for a fourth week (Merck, 2016b). Patient satisfaction is high with this method, although vaginitis, ring-related events, and leukorrhea are more common (Lopez, 2013b; Oddsson, 2005). Despite this, no deleterious affect on lower reproductive tract or endometrial epithelia has been found (Lete, 2013; Veres, 2004). A ring may be used concurrently with vaginal medications or with a tampon (Haring, 2003; Verhoeven, 2004a,b). Approximately 70 percent of partners feel the ring during intercourse (Dieben, 2002). If this is bothersome, the ring may be removed for intercourse but should be replaced within 3 hours to maintain efficacy. Alternatively, a subcutaneous version, depo-subQ provera 104, is also available and is injected into the subcutaneous tissue of the anterior thigh or abdomen every 3 months.
Pediatrics 108(3):776 virus facts floxin 200 mg buy low price, 2001 American College of Obstetricians and Gynecologists: Prevention of Rh D alloimmunization bacterial 2 hybrid 200 mg floxin purchase with mastercard. Fertil Steril 100(3):638 bacterial pneumonia floxin 400 mg order with mastercard, 2013 Apantaku O get antibiotics for acne discount floxin on line, Rana P antibiotic withdrawal cheap floxin 400 mg without prescription, Inglis T: Broad ligament ectopic pregnancy following in-vitro fertilization in a patient with previous bilateral salpingectomy. Obstet Gynecol 104:50, 2004b Bergstrom R, Mueller G, Yankowitz J: A case illustrating the continued dilemmas in treating abdominal pregnancy and a potential explanation for the high rate of postsurgical febrile morbidity. Gynecol Obstet Invest 46:268, 1998 Bertrand G, Le Ray C, Simard-Émond L, et al: Imaging in the management of abdominal pregnancy: a case report and review of the literature. J Assist Reprod Genet 33(5):647, 2016 Bouyer J, Coste J, Fernandez H, et al: Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Obstet Gynecol 122(2 Pt 1):33, 2013 Chen H, Yang S, Fu J, et al: Outcomes of bilateral uterine artery chemoembolization in combination with surgical evacuation or systemic methotrexate for cervical pregnancy. Eur J Obstet Gynecol Reprod Biol 158(1):87, 2011 Chukus A, Tirada N, Restrepo R, et al: Uncommon implantation sites of ectopic pregnancy: thinking beyond the complex adnexal mass. Radiographics 35(3):946, 2015 Chung K, Chandavarkar U, Opper N, et al: Reevaluating the role of dilation and curettage in the diagnosis of pregnancy of unknown location. Obstet Gynecol 107(3):595, 2006 Cohen A, Almog B, Satel A, et al: Laparoscopy versus laparotomy in the management of ectopic pregnancy with massive hemoperitoneum. Int J Gynaecol Obstet 123(2):139, 2013 Cohen A, Bibi G, Almog B, et al: Second-dose methotrexate in ectopic pregnancies: the role of beta human chorionic gonadotropin. Fertil Steril 102(6):1646, 2014a Cohen A, Zakar L, Gil Y, et al: Methotrexate success rates in progressing ectopic pregnancies: a reappraisal. Obstet Gynecol 59(1):63, 1982 Comstock C, Huston K, Lee W: the ultra-sonographic appearance of ovarian ectopic pregnancies. Obstet Gynecol 105:42, 2005 Condous G, Okaro E, Khalid A, et al: the accuracy of transvaginal ultrasonography for the diagnosis of ectopic pregnancy prior to surgery. Obstet Gynecol 121(1):65, 2013 Cormio G, Ceci O, Loverro G, et al: Spontaneous left broad ligament pregnancy after ipsilateral salpingo-oophorectomy. New York, McGraw-Hill Education, 2016 Gao L, Huang Z, Zhang X, et al: Reproductive outcomes following cesarean scar pregnancy-a case series and review of the literature. Fertil Steril 61:966, 1994 Glezerman M, Press F, Carpman M: Culdocentesis is an obsolete diagnostic tool in suspected ectopic pregnancy. Fertil Steril 67:398, 1997 Goswami D, Agrawal N, Arora V: Twin tubal pregnancy: a large unruptured ectopic pregnancy. Am J Obstet Gynecol 192:1370, 2005 Hassan S, Arora R, Bhatia K: Primary ovarian pregnancy: case report and review of literature. Obstet Gynecol 75(6):986, 1990 Hirakawa M, Tajima T, Yoshimitsu K, et al: Uterine artery embolization along with the administration of methotrexate for cervical ectopic pregnancy: technical and clinical outcomes. Obstet Gynecol 109:1076, 2007 Jermy K, Thomas J, Doo A, et al: the conservative management of interstitial pregnancy. J Magn Reson Imaging 13(6):918, 2001 Jurkovic D, Knez J, Appiah A, et al: Surgical treatment of Cesarean scar ectopic pregnancy: efficacy and safety of ultrasound-guided suction curettage. Ultrasound Obstet Gynecol 47(4):51, 2016 Kayatas S, Demirci O, Kumru P, et al: Predictive factors for failure of salpingostomy in ectopic pregnancy. J Clin Ultrasound 41(9):563, 2013 Kirk E, Condous G, Van Calster B, et al: A validation of the most commonly used protocol to predict the success of single-dose methotrexate in the treatment of ectopic pregnancy. Hum Reprod 12:591, 1997 Lau S, Tulandi T: Conservative medical and surgical management of interstitial ectopic pregnancy. Clin Exp Obstet Gynecol 41(4):419, 2014b Liang C, Li X, Zhao B, et al: Demonstration of the route of embryo migration in retroperitoneal ectopic pregnancy using contrast-enhanced computed tomography. Gynecol Obstet Invest 38(2):104, 1994 Lundorff P, Thorburn J, Hahlin M, et al: Laparoscopic surgery in ectopic pregnancy. Acta Obstet Gynecol Scand 70(45):343, 1991 Maheux-Lacroix S, Li F, Bujold E, et al: Cesarean scar pregnancies: a systematic review of treatment options. Obstet Gynecol 71:549, 1988 Mavrelos D, Nicks H, Jamil A, et al: Efficacy and safety of a clinical protocol for expectant management of selected women diagnosed with a tubal ectopic pregnancy. Ultrasound Obstet Gynecol 42(1):102, 2013 Melcer Y, Maymon R, Vaknin Z, et al: Primary ovarian ectopic pregnancy: still a medical challenge. J Reprod Med 61(12):58, 2016 Melcer Y, Smorgick N, Vaknin Z, et al: Primary ovarian pregnancy: 43 years experience in a single institute and still a medical challenge. Isr Med Assoc J 17(11):687, 2015 Memtsa M, Jamil A, Sebire N, et al: Rarity revisited: diagnosis and management of intramural ectopic pregnancy. Ultrasound Obstet Gynecol 32(7):929, 2008b Murji A, Garbedian K, Thomas J, et al: Conservative management of cervical ectopic pregnancy. Fertil Steril 70:511, 1998 Nowak-Markwitz E, Michalak M, Olejnik M, et al: Cutoff value of human chorionic gonadotropin in relation to the number of methotrexate cycles in the successful treatment of ectopic pregnancy. Am J Obstet Gynecol 146(3):32, 1983 Ries A, Singson P, Bidus M, et al: Use of the endometrial Pipelle in the diagnosis of early abnormal gestations. Obstet Gynecol Sci 56(6):404, 2013 Sagiv R, Debby A, Sadan O, et al: Laparoscopic surgery for extrauterine pregnancy in hemodynamically unstable patients. J Am Assoc Gynecol Laparosc 8(4):529, 2001 Scutiero G, Di Gioia P, Spada A, et al: Primary ovarian pregnancy and its management. Fertil Steril 68:430, 1997 Spiegelberg O: Zur Casuistic der Ovarialschwangerschaft. Fertil Steril 102(6):1671, 2014 Svirsky R, Rozovski U, Vaknin Z, et al: the safety of conception occurring shortly after methotrexate treatment of an ectopic pregnancy. Reprod Toxicol 27(1):85, 2009 Tanaka Y, Mimura K, Kanagawa T, et al: Three-dimensional sonography in the differential diagnosis of interstitial, angular, and intrauterine pregnancies in a septate uterus. Obstet Gynecol 79(6):1044, 1992 Tsakos E, Tsagias N, Dafopoulos K: Suggested method for the management of heterotopic cervical pregnancy leading to term delivery of the intrauterine pregnancy: case report and literature review. J Minim Invasive Gynecol 22(5):896, 2015 Tulandi T, A1-Jaroudi D: Interstitial pregnancy: results generated from the Society of Reproductive Surgeons. Obstet Gynecol 103:47, 2004 Tulandi T, Guralnick M: Treatment of tubal ectopic pregnancy by salpingotomy with or without tubal suturing and salpingectomy. Fertil Steril 55:53, 1991 Uur M, Turan C, Vicdan K, et al: Chronic ectopic pregnancy: a clinical analysis of 62 cases. Fertil Steril 100(5):1310, 2013 Valenzano M, Nicoletti L, Odicino F, et al: Five-year follow-up of placental involution after abdominal pregnancy. Fertil Steril 96(6):1391, 2011 Verma U, Goharkhay N: Conservative management of cervical ectopic pregnancy. Fertil Steril 50:584, 1988 Wang G, Liu X, Bi F, et al: Evaluation of the efficacy of laparoscopic resection for the management of exogenous cesarean scar pregnancy. Taiwan J Obstet Gynecol 54(5):551, 2015 Wang Y, Xu B, Dai S, et al: An efficient conservative treatment modality for cervical pregnancy: angiographic uterine artery embolization followed by immediate curettage. J Minim Invasive Gynecol 22(3):501, 2015 Westrom L, Joesoef R, Reynolds G, et al: Pelvic inflammatory disease and fertility: a cohort study of 1,844 women with laparoscopically verified disease and 657 control women with normal laparoscopic results. J Minim Invasive Gynecol 20(1):123, 2013 Xiaolin Z, Ling L, Chengxin Y, et al: Transcatheter intraarterial methotrexate infusion combined with selective uterine artery embolization as a treatment option for cervical pregnancy. J Vasc Interv Radiol 21(6):836, 2010 Yang Q, Piao S, Wang G, et al: Hysteroscopic surgery of ectopic pregnancy in the cesarean section scar. Fertil Steril 95(3):872, 2011 Zeck W, Kelters I, Winter R, et al: Lessons learned from four advanced abdominal pregnancies at an East African Health Center. These vary in size from minute bodies a few millimetres in diameter to cystic structures the size of hazel-nuts, and hang in clusters from the villous stems, to which they are connected by thin pedicles, giving to the external surface of the chorion a grape-like appearance. Hydatidiform moles are excessively edematous immature placentas (Benirschke, 2012). These include the benign complete hydatidiform mole and partial hydatidiform mole and the malignant invasive mole. Invasive mole is deemed malignant due to its marked penetration into and destruction of the myometrium and its ability to metastasize. Nonmolar trophoblastic neoplasms include choriocarcinoma, placental site trophoblastic tumor, and epithelioid trophoblastic tumor. These include invasive mole, choriocarcinoma, placental site trophoblastic tumor, and epithelioid trophoblastic tumor. These malignancies develop weeks or years following any type of pregnancy, but frequently follow a hydatidiform mole. The degree of histological changes, karyotypic differences, and the absence or presence of embryonic elements are used to classify them as either complete or partial moles. Low-magnification photomicrograph shows generalized edema and cistern formation (black asterisks) within avascular villi. In contrast, a partial molar pregnancy has focal and less advanced hydatidiform changes and contains some fetal tissue. Both forms of moles usually fill the uterine cavity, but they rarely may be tubal or other forms of ectopic pregnancy (Hassadia, 2012; Sebire, 2005). Epidemiology and Risk Factors An ethnic predisposition is seen with hydatidiform mole, which has increased prevalence in Asians, Hispanics, and American Indians (Drake, 2006; Lee, 2011; Smith, 2006). The incidence in the United States and Europe has been relatively constant at 1 to 2 per 1000 deliveries (Eysbouts, 2016; Lee, 2011). Specifically, adolescents and women aged 36 to 40 years have a twofold risk, but those older than 40 have an almost tenfold risk (Altman, 2008; Sebire, 2002a). After two prior complete moles, approximately 20 percent of women have a third mole (Eagles, 2015). The ovum is fertilized by a haploid sperm, which then duplicates its own chromosomes after meiosis. A partial mole may be formed if two sperm-either 23,X- or 23,Y-bearing-both fertilize (dispermy) a 23,X-containing haploid egg whose genes have not been inactivated. The resulting fertilized egg is triploid with two chromosome sets being donated by the father. These are each composed of two paternal haploid sets of chromosomes contributed by dispermy and one maternal haploid set. These triploid zygotes result in some embryonic development, however, it ultimately is a lethal fetal condition (Joergensen, 2014; Lakovschek, 2011). Fetuses that reach advanced ages have severe growth restriction, multiple congenital anomalies, or both. Twin Pregnancy Rarely, in some twin pregnancies, one chromosomally normal fetus is paired with a complete diploid molar pregnancy. Importantly, these cases must be distinguished from a single partial molar pregnancy with its associated abnormal fetus. In those with continuing pregnancy, survival of the normal fetus varies and depends on associated comorbidity from the molar component. The most worrisome are preeclampsia or hemorrhage, which frequently necessitate preterm delivery. Wee and Jauniaux (2005) reviewed outcomes in 174 women, of whom 82 chose termination. Of the remaining 92 pregnancies, 42 percent either miscarried or had a perinatal death; approximately 60 percent delivered preterm; and only 40 percent delivered at term. However, most data indicate no significant difference between women who continue or terminate their pregnancy (Massardier, 2009; Sebire, 2002b). Clinical Findings the presentation of women with a molar pregnancy has changed remarkably over the past several decades because prenatal care is sought much earlier and because sonography is virtually universal. For example, in 194 women with a complete mole, evacuation was completed at a median gestational age of 9 weeks and at 12 weeks for 172 patients with a partial mole (Sun, 2015b). As a result, most molar pregnancies are detected before complications ensue (Kerkmeijer, 2009; Mangili, 2008). As gestation advances, symptoms tend to be more pronounced with complete compared with partial moles (Niemann, 2007). Untreated molar pregnancies will almost always cause uterine bleeding that varies from spotting to profuse hemorrhage. Bleeding may presage spontaneous molar abortion, but more often, it follows an intermittent course for weeks to months. In more advanced moles with considerable concealed uterine hemorrhage, moderate iron-deficiency anemia develops. Of physical findings, many women have uterine growth that is more rapid than expected, and the enlarged uterus is comparatively softer. Because theca-lutein cysts regress following pregnancy evacuation, expectant management is preferred. However, oophorectomy is not performed unless extensive infarction persists after untwisting. Despite this, clinically apparent thyrotoxicosis is unusual and in our experience can be mimicked by bleeding and sepsis from infected products. Despite this, cases of presumed "thyroid storm" have been reported (Kofinas, 2015). Severe preeclampsia and eclampsia are relatively common with advanced molar pregnancies. An exception is the case of a normal fetus coexisting with a complete mole, described earlier. In continuing twin gestations, severe preeclampsia frequently mandates preterm delivery. Importantly, these high values can lead to erroneous false-negative urine pregnancy test results. Sonography Although this is the mainstay of trophoblastic disease diagnosis, not all cases are confirmed initially. Sonographically, a complete mole appears as an echogenic uterine mass with numerous anechoic cystic spaces but without a fetus or amnionic sac. A partial mole has features that include a thickened, multicystic placenta along with a fetus or at least fetal tissue. However, in early pregnancy, these sonographic characteristics are seen in fewer than half of hydatidiform moles.
Perhaps not coincidentally antibiotics and weed floxin 200 mg on line, the risk of death for newborns delivered at home compared with those delivered in hospitals is increased two- to threefold (American College of Obstetricians and Gynecologists virus for mac generic floxin 200 mg mastercard, 2017d) antimicrobial agents 1 200 mg floxin buy mastercard. When deprived of adequate gas exchange antibiotics for sinus infection dose purchase floxin mastercard, either before or after birth antibiotic resistance research topics order discount floxin on line, neonates demonstrate a well-defined sequence of events leading to apnea. If oxygen deprivation and asphyxia persist, however, the newborn will develop deep gasping respirations, followed by secondary apnea. This latter stage is associated with a further decline in heart rate, fall in blood pressure, and loss of neuromuscular tone. Neonates in secondary apnea will not respond to stimulation and will not spontaneously resume respiratory efforts. Elk Grove Village, American Academy of Pediatrics and American Heart Association, 2010. And, when a response to stimulation is not immediate, resuscitation with effective ventilation of the apneic newborn must be started quickly. Resuscitation Protocol Initial Assessment Immediately after birth and usually during the delay for umbilical cord clamping, newborn tone, respiratory effort, and heart rate are evaluated. Direct skin-to-skin contact with the mother and drying and covering the newborn with a warm blanket will help maintain euthermia (36. A vigorously crying newborn does not require routine oral suctioning (Carrasco, 1997; Gungor, 2006). Instead, bulb suctioning to remove secretions is best reserved for those who cannot clear secretions on their own due to apnea or copious secretions. If not vigorous or if preterm, the neonate is carried to a prewarmed radiant warmer for the initial newborn care steps. Preterm infants are particularly vulnerable, and special steps to maintain euthermia include providing a warmer delivery room (>25°C), covering the neonatal head with either a plastic or wool hat, application of polyethylene plastic "ponchos" or wraps to slow evaporative heat losses, use of chemically activated thermal mattresses to reduce conductive heat loss, and administration of warm, humidified respiratory gases during respiratory stabilization (Perlman, 2015). At the radiant warmer, newborns must be positioned to maximally open the airway, with mild extension of the neck. If the newborn is apneic or has copious secretions that it cannot clear, a bulb syringe or suction catheter may be used to clear the mouth and then the nose. Routine intubation and suctioning of meconiumstained amnionic fluid is no longer recommended for the nonvigorous newborn (American College of Obstetricians and Gynecologists, 2017b; Perlman, 2015). After completion of the initial stabilization steps, apnea, gasping respirations, or heart rate 100 beats per minute (bpm) should prompt immediate administration of positive-pressure ventilation with room air. This should be started by 60 seconds of life, if not sooner, once the initial steps are completed. The head should be in a sniffing position with the tip of the nose pointing to the ceiling. Mask Ventilation Assisted ventilation by facemask at a rate of 40 to 60 breaths per minute is recommended. Supplemental oxygen can be given in graduated, rising percentages to maintain oxygen saturation values within a normal range per minute of life. If the heart rate remains 100 bpm after 5 to 10 positive pressure breaths, the attempted ventilation is inadequate and corrective steps must be taken. The two most common problems are mask leak due to an ineffective seal and malposition of the airway (Schmolzer, 2011). If corrective steps do not improve the heart rate, either intubation with an endotracheal tube or placement of a laryngeal mask airway is required. For tracheal intubation, a laryngoscope with a straight blade-size 0 for a preterm newborn and size 1 for a term neonate-is used. One can also look for symmetrical chest wall motion; auscultate for equal breath sounds, especially in the axillae; and auscultate for the absence of breath sounds or gurgling over the stomach. Once in place, the tube is used for tracheal suctioning only for a suspected obstructed airway. Otherwise, an appropriate positive-pressure device is attached to the endotracheal tube. Air puffs are delivered at a rate of 40 to 60 per minute with a force adequate to stabilize the heart rate. In term infants, opening pressures of 30 to 40 cm H2O typically will expand the alveoli without causing barotrauma. An increase in heart rate and peripheral oxygen saturation (SpO2) levels within acceptable ranges reflect a positive response. Chest Compressions Most commonly, effective ventilation is all that is required to stabilize the newborn in the delivery room. If the heart rate remains <60 bpm despite ventilation corrective steps, including placement of tracheal tube, chest compressions are initiated. Once the tracheal tube has been secured, compressions are done from the head of the bed rather than the side so that space is opened up for a provider to have umbilical venous access. When compressions are initiated, the oxygen concentration is increased to 100 percent. With the two-thumb compression method, hands encircle the chest, while the thumbs depress the sternum. Compressions are delivered on the lower third of the sternum at a depth sufficient to generate a palpable pulse. Compared with other techniques, this method offers less provider fatigue over time, yields higher generated perfusion pressures, and lessens hand malpositioning that could cause traumatic injury (Kapadia, 2012). A 3:1 compressions-to-ventilation ratio is recommended, and 90 compressions and 30 breaths achieve approximately 120 events each minute. Coordinated chest compressions and ventilations should continue until the spontaneous heart rate is 60 bpm. Epinephrine Intravenously administered epinephrine is indicated if the heart rate remains 60 bpm after adequate ventilation and chest compressions. Epinephrine may be given through the endotracheal tube if venous access has not been established, but its action is less reliable (Kapadia, 2017). Notably, the decision to continue or discontinue resuscitative efforts must be individualized (Perlman, 2015). Virginia Apgar in 1953 remains a useful clinical tool to classify newborn health immediately after birth and to assess the effectiveness of resuscitative measures (American Academy of Pediatrics, 2017). As shown in Table 32-2, each of five easily identifiable characteristics-heart rate, respiratory effort, muscle tone, reflex irritability, and color-is assessed and assigned a value of 0, 1, or 2. In the currently recommended expanded form, concurrent resuscitation interventions are also recorded over time. The total score, based on the sum of the five components, is determined in all neonates at 1 and 5 minutes after delivery. In those with a score <7, the score may be calculated at further 5-minute intervals until a 20-minute Apgar score is assigned or resuscitation efforts are halted. They found that in term neonates, the risk of neonatal death was approximately 1 in 5000 for those with Apgar scores of 7 to 10. This risk compares with a mortality rate of 25 percent for term newborns with 5-minute scores 3. Low 5-minute scores were comparably predictive of neonatal death in preterm neonates. These investigators concluded that the Apgar scoring system remains relevant for the prediction of neonatal survival. There have been attempts to use Apgar scores to define asphyxial injury and to predict subsequent neurological outcome-uses for which the Apgar score was never intended (Chap. Such associations are difficult to measure with reliability given that both asphyxial injury and low Apgar scores are infrequent outcomes. For example, according to United States birth certificate records for 2010, only 1. Similarly, in a population-based study of more than 1 million term newborns in Sweden between 1988 and 1997, the incidence of 5-minute Apgar scores of 3 approximated 2 per 1000 (Thorngren-Jerneck, 2001). Previously, many groups established erroneous definitions of asphyxia based solely on low Apgar scores. These prompted the American College of Obstetricians and Gynecologists and American Academy of Pediatrics (2017f) to issue a series of joint opinions with important caveats regarding Apgar score limitations. Certain elements of the Apgar score are partially dependent on the physiological maturity of the newborn, and a healthy, preterm neonate may receive a low score only because of immaturity. Other influencing factors include fetal malformations, maternal medications, and infection. Moreover, the Apgar score alone cannot establish hypoxia as the cause of cerebral palsy, as discussed in Chapter 33 (p. Umbilical Cord Blood AcidBase Studies Blood taken from umbilical vessels may be used for acidbase studies to assess the metabolic status of the neonate. Blood collection is performed following delivery by immediately isolating a 10- to 20-cm segment of cord with two clamps placed near the neonate and another two clamps positioned nearer the placenta. The cord is then cut between the two proximal clamps and then the two distal clamps (Blickstein, 2007). Arterial blood is drawn from the isolated cord segment into a 1- to 2-mL commercially prepared plastic syringe containing lyophilized heparin or a similar syringe that has been flushed with a heparin solution containing 1000 U/mL. Once sampling is completed, the needle is capped and the syringe transported, on ice, to the laboratory. Mathematical models have been developed that allow reasonable prediction of birth acidbase status in properly collected cord blood samples analyzed as late as 60 hours after delivery (Chauhan, 1994). Acidbase measurements can show significant variances between different analyzing devices (Mokarami, 2012). Levels of these increase with persistent placental exchange impairment, and they result from anaerobic glycolysis. In the fetus, respiratory and metabolic acidemia and ultimately tissue acidosis are most likely part of a progressively worsening continuum. This is different from adult pathophysiology, in which distinct conditions result either in respiratory acidosis-for example, pulmonary disease, or in metabolic acidosis-for example, diabetes. In the fetus, the placenta serves as both the lungs and, to a certain degree, the kidneys. Assuming that maternal pH and blood gases are normal, the actual pH of fetal blood is dependent on the proportion of carbonic and organic acids and the amount of bicarbonate, which is the major buffer in blood. Because pH is a logarithmic term, it does not give a linear measure of acid accumulation. For example, a change in hydrogen ion concentration associated with a fall in pH from 7. For this reason, the change in base-termed delta base- offers a more linear measure of the degree of accumulation of metabolic acid (Armstrong, 2007). Normal umbilical cord blood pH and blood gas values at delivery in term newborns are summarized in Table 32-3. Similar values have been reported for preterm neonates (Dickinson, 1992; Ramin, 1989; Riley, 1993). And, in a study from Oxford of more than 51,000 term newborns, the incidence of neonatal encephalopathy in those with a birth pH <7. Even those with who had normal 5-minute Apgar scores but an arterial cord pH values <7. The speed of acidemia resolution after birth is associated with outcome (Casey, 2001a). Thus, in a mixed respiratorymetabolic acidemia, the benign respiratory component can be calculated. As an example, acute cord prolapse during labor prompts cesarean delivery of a neonate 20 minutes later. Metabolic Acidemia the fetus begins to develop metabolic acidemia when oxygen deprivation is sufficiently long and severe to require anaerobic metabolism for cellular energy needs. Low and associates (1997) defined fetal acidosis as a base deficit 12 mmol/L, and severe fetal acidosis as a base deficit 16 mmol/L. In the Parkland study of more than 150,000 newborns cited earlier, metabolic acidemia was defined using umbilical cord blood gas thresholds that were two standard deviations below the mean (Casey, 2001b). From the standpoint of possible neurological injury, the American College of Obstetricians and Gynecologists (2014) defines metabolic acidosis as umbilical arterial pH <7. In rare cases, such hypoxia-induced metabolic acidemia may be so severe that it causes subsequent neurological impairment-hypoxic-ischemic encephalopathy (Chap. In fact, a fetus without such acidemia cannot by definition have suffered recent hypoxic-induced injury. That said, severe metabolic acidosis is poorly predictive of subsequent neurological impairment in the term neonate (King, 1998; Socol, 1994). In very-low-birthweight neonates, that is, those <1000 g, newborn acidbase status may be more closely linked to intraventricular hemorrhage and possibly long-term neurological outcome (Lavrijsen, 2005; Salhab, 2005; Victory, 2003). Casey and coworkers (2001b) described the association between metabolic acidemia, low Apgar scores, and neonatal death in term and preterm newborns. Regarding term neonates, the risk of neonatal death was more than 3200-fold greater in term neonates with metabolic acidemia and 5-minute scores 3 compared with those with a 5-minute Apgar score 7. Recommendations for Cord Blood Gas Determinations In some centers, cord gas analysis is performed in all neonates at birth (Casey, 2001b; Sabol, 2016). Cost-effectiveness analysis for universal cord blood gas measurements suggest benefit and potential cost savings (White, 2010, 2016). It seems reasonable to obtain cord blood gas determinations for intrapartum cases of cesarean delivery for fetal compromise, abnormal fetal heart rate tracing, fever, and low 5-minute Apgar score. Although umbilical cord acidbase blood determinations are poorly predictive of either immediate or long-term adverse neurological outcome, they provide the most objective evidence of the fetal metabolic status at birth. Some form of conjunctivitis affects 1 to 12 percent of all neonates, and gonococcal and chlamydial infections are among the most common (Zuppa, 2011). Neisseria gonorrhoeae infection acquired at birth was a common cause of childhood blindness in the past. However, the practice of instilling a 1-percent ophthalmic solution of silver nitrate largely eliminated this. Various other antimicrobial agents have also proven effective, and gonococcal prophylaxis is now mandatory for all neonates in most states (American Academy of Pediatrics, 2017b). For prophylaxis soon after delivery, recommendations include a single application of either 1-percent silver nitrate solution or 0.
In two randomized trials bacteria joe floxin 400 mg online, women with a history of early-onset preeclampsia were given an aspirin therapy or an enoxaparin plus aspirin regimen (Groom antibiotic ointment for cats generic floxin 400 mg amex, 2017; Haddad infection x box generic floxin 200 mg on-line, 2016) best antibiotic for gbs uti buy cheap floxin 200 mg on line. From their reviews antimicrobial effect cheap 400 mg floxin, Sergis and associates (2006) reported better pregnancy outcomes in women with prior severe preeclampsia given low-molecular-weight heparin plus low-dose aspirin compared with those given low-dose aspirin alone. Thus, the Task Force (2013) recommends more frequent prenatal visits if preeclampsia is "suspected. Heightened surveillance permits more prompt recognition of ominous changes in blood pressure, critical laboratory findings, and clinical signs and symptoms (Macdonald-Wallis, 2015). The basic management objectives for any pregnancy complicated by preeclampsia are: (1) termination of pregnancy with the least possible trauma to mother and fetus, (2) birth of a healthy newborn that subsequently thrives, and (3) complete restoration of health to the mother. In many women with preeclampsia, especially those at or near term, all three objectives are served equally well by induction of labor. One of the most important clinical questions for successful management is precise knowledge of fetal age. Early Diagnosis of Preeclampsia Traditionally, the frequency of prenatal visits is increased during the third trimester, and this aids early detection of preeclampsia. Women without overt hypertension, but in whom early developing preeclampsia is suspected during routine prenatal visits, are seen more frequently. For many years at Parkland Hospital, women with new-onset diastolic blood pressures >80 mm Hg but <90 mm Hg or with sudden abnormal weight gain of more than 2 pounds per week have, at minimum, returned for visits at 7-day intervals. Outpatient surveillance is continued unless overt hypertension, proteinuria, headache, visual disturbances, or epigastric pain supervenes. Women with overt new-onset hypertension-either diastolic pressures 90 mm Hg or systolic pressures 140 mm Hg-are admitted to determine if the increase is due to preeclampsia, and if so, to evaluate its severity. Evaluation With hospitalization, a systematic evaluation is instituted to include: · Detailed examination, which is coupled with daily scrutiny for clinical findings such as headache, visual disturbances, epigastric pain, and rapid weight gain · Daily weight measurement · Quantification of proteinuria or urine protein:creatinine ratio on admittance and at least every 2 days thereafter · Blood pressure readings with an appropriate-size cuff every 4 hours, except between 2400 and 0600 unless previous readings are elevated · Measurements of plasma or serum creatinine and hepatic transaminase levels and a hemogram that includes a platelet count. Although some recommend measurement of serum uric acid and lactate dehydrogenase levels and coagulation studies, their value has been questioned (Conde-Agudelo, 2015; Thangaratinam, 2006). Reduced physical activity throughout much of the day is likely beneficial, but as the 2013 Task Force concluded, absolute bed rest is not desirable. Ample protein and calories are included in the diet, and sodium and fluid intake are not limited or forced. In sum, goals of evaluation include early identification of preeclampsia or worsening of the syndrome and development of a management plan for timely delivery. Fortunately, many cases are sufficiently mild and near enough to term that they can be managed conservatively until labor commences spontaneously or until the cervix becomes favorable for labor induction. Complete abatement of all signs and symptoms, however, is uncommon until after delivery. If severe preeclampsia is diagnosed using the criteria in Table 40-2, further management is subsequently described. Consideration for Delivery Termination of pregnancy is the only cure for preeclampsia. Headache, visual disturbances, or epigastric pain are indicative that convulsions may be imminent, and oliguria is another ominous sign. Severe preeclampsia demands anticonvulsant and often antihypertensive therapy, followed by delivery. The prime objectives are to forestall convulsions, to prevent intracranial hemorrhage and serious damage to other vital organs, and to deliver a healthy newborn. Labor induction is carried out, usually with preinduction cervical ripening with a prostaglandin or osmotic dilator (Chap. Concerns stemming from an unfavorable cervix, a perceived sense of urgency because of preeclampsia severity, and a need to coordinate neonatal intensive care have led some to advocate cesarean delivery. Alexander and colleagues (1999) reviewed 278 singleton liveborn neonates weighing 750 to 1500 g delivered of women with severe preeclampsia at Parkland Hospital. In half of the women, labor was induced, and the remainder underwent cesarean delivery without labor. Induction was successful in accomplishing vaginal delivery in a third, and it was not harmful to very-low-birthweight neonates. However, whenever it appears that induction almost certainly will not succeed or attempts have failed, then cesarean delivery is indicated. For a woman near term, with a soft, partially effaced cervix, even a milder degree of preeclampsia probably carries more risk to the mother and her fetusnewborn than does induction of labor (Tajik, 2012). When the fetus is preterm, the tendency is to temporize in the hope that additional weeks in utero will reduce the risk of neonatal death or serious morbidity from prematurity. Assessments of fetal well-being and placental function are performed, especially when the fetus is immature. Most recommend frequent performance of nonstress testing or biophysical profiles to assess fetal well-being (American College of Obstetricians and Gynecologists, 2016a). Also, women with higher ratios tend to have more adverse outcomes (Baltajian, 2016). Barton and coworkers (2011) reported excessive neonatal morbidity in women delivered before 38 weeks despite having stable, mild, nonproteinuric hypertension. The Netherlands study of 4316 newborns delivered between 340/7 and 366/7 weeks also described substantive neonatal morbidity in these cases (Langenveld, 2011). Hospitalization versus Outpatient Management For women with mild-to-moderate stable hypertension-whether or not preeclampsia has been confirmed-monitoring is continued. During surveillance, reduced physical activity throughout much of the day, at least intuitively, seems beneficial. First, this is pragmatically unachievable because of the severe restrictions it places on otherwise well women. To reduce activity, several studies have addressed the benefits of inpatient care and outpatient management. The concept of prolonged hospitalization for women with hypertension arose during the 1970s. Initial results from this unit were reported by Hauth (1976) and Gilstrap (1978) and their coworkers. Most hospitalized women have a beneficial response characterized by amelioration or improvement of hypertension. These women are not "cured," and nearly 90 percent have recurrent hypertension before or during labor. By 2016, more than 10,000 nulliparas with mild-to-moderate, early-onset hypertension during pregnancy had been managed successfully in this unit. Provider costs-not charges-for this relatively simple physical facility, modest nursing care, no drugs other than iron and folate supplements, and few essential laboratory tests are minimal compared with the cost of neonatal intensive care for a preterm neonate. Many clinicians believe that further hospitalization is not warranted if hypertension abates within a few days, and this has legitimized third-party payers to deny hospitalization reimbursement. Outpatient management may continue as long as preeclampsia syndrome does not worsen and fetal jeopardy is not suspected. Home blood pressure and urine protein monitoring or frequent evaluations by a visiting nurse may prove beneficial. To assess this approach, 1182 nulliparas with mild gestational hypertension-20 percent had proteinuria-were managed with home health care (Barton, 2002). Their mean gestational ages were 32 to 33 weeks at enrollment and 36 to 37 weeks at delivery. In approximately 20 percent, there was fetalgrowth restriction, and the perinatal mortality rate was 4. In a pilot study from Parkland Hospital, 72 nulliparas with new-onset hypertension from 27 to 37 weeks were assigned either to continued hospitalization or to outpatient care (Horsager, 1995). The only significant difference was that women in the home care group developed severe preeclampsia significantly more frequently than hospitalized women-42 versus 25 percent. In another trial, after hospital evaluation, 218 women with mild gestational nonproteinuric hypertension were similarly divided (Crowther, 1992). Randomized Clinical Trials Comparing Hospitalization versus Routine Care for Women with Mild Gestational Hypertension or Preeclampsia Another approach, popular in Europe, is day care (Milne, 2009). Progression to overt preeclampsia and labor inductions were significantly greater in the routine outpatient management group. In another, 395 women participated in either day care or inpatient management (Turnbull, 2004). Costs for either scheme were not significantly different, and general satisfaction favored day care. In sum, either inpatient or close outpatient management is appropriate for a woman with mild de novo hypertension, including those with nonsevere preeclampsia. Most of these studies were carried out in academic centers with dedicated management teams. That said, the key to success is close surveillance and a conscientious patient with good home support. Antihypertensive Therapy for Mild-to-Moderate Hypertension the use of antihypertensive drugs to prolong pregnancy or modify perinatal outcomes in pregnancies complicated by various hypertensive disorders has been of considerable interest. Treatment for women with chronic hypertension complicating pregnancy is discussed in detail in Chapter 50 (p. Sibai and colleagues (1987a) reported that women given labetalol had significantly lower mean blood pressures. However, mean pregnancy prolongation, gestational age at delivery, and birthweight did not differ between groups. The cesarean delivery rate and the number of newborns admitted to special-care nurseries were also similar. The frequency of growth-restricted neonates was doubled in women given labetalol-19 versus 9 percent. The three other studies listed in Table 40-8 compared labetalol or the calcium-channel blockers nifedipine and isradipine against placebo. Except for fewer episodes of severe hypertension, none of these studies showed any benefits from antihypertensive treatment (Magee, 2015). Similar conclusions were reached by Abalos and associates (2014), who reviewed 49 randomized trials of active antihypertensive therapy compared with either no treatment or placebo given to women with mild-to-moderate gestational hypertension. Randomized Placebo-Controlled Trials of Antihypertensive Therapy for Early Mild Gestational Hypertension Delayed Delivery Up through the early 1990s, the prevailing practice was that women with severe preeclampsia were usually delivered without delay. However, another approach for women with preterm severe preeclampsia has also been advocated. This approach calls for "conservative" or "expectant" management with the aim of improving neonatal outcome without compromising maternal safety. Aspects of such management always include careful daily-and usually more frequent-inpatient monitoring of the mother and her fetus. Expectant Management of Preterm Severe Preeclampsia Theoretically, antihypertensive therapy has potential application when severe preeclampsia develops before intact neonatal survival is likely. In one of the first studies, Sibai and the Memphis group (1985) attempted to prolong pregnancy because of fetal immaturity in 60 women with severe preeclampsia between 18 and 27 weeks. Although no mothers died, 13 suffered placental abruption, 10 had eclampsia, three developed renal failure, two had hypertensive encephalopathy, one had an intracerebral hemorrhage, and another had a ruptured hepatic hematoma. Because of their early study, the Memphis group redefined criteria and performed a randomized trial of aggressive versus expectant management for 95 women who had severe preeclampsia but with more advanced gestations of 28 to 32 weeks (Sibai, 1994). Aggressive management included glucocorticoid administration for fetal lung maturation followed by delivery in 48 hours. Expectantly managed women were observed at bed rest and given either labetalol or nifedipine orally for severe hypertension. Perinatal outcomes were similar in each group, and importantly, outcomes were not improved with procrastination. Those with fetal-growth restriction generally have shorter interval-todelivery durations (McKinney, 2016). Sibai and Barton (2007b) reviewed expectant management of severe preeclampsia from 24 to 34 weeks. More than 1200 women were included, and although the average time gained ranged from 5 to 10 days, the maternal morbidity rates were formidable. Fetal-growth restriction was common, and in the studies from the Netherlands, it was an astounding 94 percent (Ganzevoort, 2005a,b). Perinatal mortality rates are disproportionately high in these growth-restricted neonates, but maternal outcomes are not appreciably different (Haddad, 2007; Shear, 2005). The perinatal mortality rate approximated 9 percent in each group, the composite neonatal morbidity outcome was not improved with expectant management. On the other hand, fetal-growth restriction -22 versus 9 percent-and placental abruption-7. Maternal and Perinatal Outcomes Reported since 2005 with Expectant Management of Severe Preeclampsia from 24 to 34 Weeks Expectant Management of Midtrimester Severe Preeclampsia Several small studies have focused on expectant management of severe preeclampsia syndrome before 28 weeks. In their review, Bombrys and coworkers (2008) found eight such studies that included nearly 200 women with severe preeclampsia with an onset <26 completed weeks. Because no neonates survived when delivered before 23 weeks, the Task Force (2013) recommends pregnancy termination in these cases. For women with slightly more advanced pregnancies, however, the decision is less clear. For women with pregnancies at 24 to 26 weeks, perinatal survival approached 60 percent, and it averaged almost 90 percent for those at 26 weeks. At least five observational studies of women with severe midtrimester preeclampsia who were managed expectantly have been published since 2005 (Abdel-Hady, 2010; Belghiti, 2011; Bombrys, 2008; Budden, 2006; GauglerSenden, 2006). At this time, no comparative studies attest to perinatal benefits of such expectant treatment versus early delivery in the face of serious maternal complications, which approach rates of 50 percent. Glucocorticoids for Lung Maturation To enhance fetal lung maturation, glucocorticoids have been administered to women with severe hypertension who are remote from term. Treatment does not seem to worsen maternal hypertension, and a lower incidence of respiratory distress and improved fetal survival rates have been cited. That said, only one randomized trial has evaluated corticosteroids given to hypertensive women for fetal lung maturation.
In contrast antibiotics for uti treatment purchase floxin 400 mg with visa, Ogundipe and associates (1994) randomly assigned 116 term pregnancies with an amnionic fluid index <5 cm to receive prophylactic amnioinfusion or standard obstetrical care infection the game 400 mg floxin order mastercard. Overall cesarean delivery rates antibiotics examples discount floxin 200 mg online, delivery rates for fetal distress antibiotics for acne success rate generic 200 mg floxin amex, or umbilical cord acidbase studies did not differ significantly between groups do antibiotics for acne cause weight gain 200 mg floxin visa. For meconium-stained amnionic fluid, Pierce and associates (2000) reviewed 13 prospective trials of intrapartum amnioinfusion for 1924 women with meconiumstained fluid. In the amnioinfusion group, newborns were significantly less likely to have meconium below the vocal cords, and meconium aspiration syndrome rates were lower. In contrast, several investigators were not supportive of amnioinfusion for meconium staining. For example, Usta and associates (1995) reported that amnioinfusion was not feasible in half of women with moderate or thick meconium who were randomized to this treatment. These investigators were unable to demonstrate improved neonatal outcomes with this treatment. Spong and coworkers (1994) also concluded that although prophylactic amnioinfusion did dilute meconium, it did not improve perinatal outcome. Last, Fraser and colleagues (2005) randomized amnioinfusion in 1998 women with thick meconium-stained amnionic fluid in labor and found no benefits. Because of these findings, the American College of Obstetricians and Gynecologists (2016) does not recommend amnioinfusion to dilute meconium-stained amnionic fluid. Fetal Heart Rate Patterns and Brain Injury Studies that have attempted to correlate fetal heart rate patterns with brain injury primarily have examined infants identified in medicolegal actions. Phelan and Ahn (1994) reported that among 48 fetuses later found to be neurologically impaired, a persistent nonreactive fetal heart rate tracing was already present at the time of admission in 70 percent. They concluded that fetal neurological injury occurred predominately before arrival to the hospital. When they looked retrospectively at heart rate patterns in 209 brain-injured newborns, they concluded that there was not a single unique pattern associated with fetal neurological injury (Ahn, 1996). Graham and associates (2006) reviewed the world literature published between 1966 and 2006 on the effect of fetal heart rate monitoring to prevent perinatal brain injury and found no benefit. Fetal heart rate patterns necessary for perinatal brain damage have been studied in experimental animals. Myers (1972) described the effects of complete and partial asphyxia in rhesus monkeys. Complete asphyxia was produced by total occlusion of umbilical blood flow that led to prolonged deceleration. At least 10 minutes of such prolonged deceleration was required before there was evidence of brain damage in surviving fetuses. He observed that several hours of these late decelerations did not damage the fetal brain unless the pH fell below 7. Indeed, Adamsons and Myers (1977) reported subsequently that late decelerations were a marker of partial asphyxia long before brain damage occurred. The most common fetal heart rate pattern during labor-due to umbilical cord occlusion-requires considerable time to significantly affect the fetus in experimental animals. Clapp and colleagues (1988) partially occluded the umbilical cord for 1 minute every 3 minutes in fetal sheep. Rocha and associates (2004) totally occluded the umbilical cord for 90 seconds every 30 minutes for 3 to 5 hours a day for 4 days without producing necrotic brain cell injury. Results from such studies suggest that the effects of umbilical cord entrapment depend on the degree of occlusion-partial versus total, the duration of individual occlusions, and the frequency of such occlusions. The contribution of intrapartum events to subsequent neurological handicaps has been greatly overestimated, as discussed in further detail in Chapter 33 (p. It is clear that for brain damage to occur, the fetus must be exposed to much more than a brief period of hypoxia. Moreover, the hypoxia must cause profound, just barely sublethal metabolic acidemia. Because of this, the American College of Obstetricians and Gynecologists (2014) has recommended umbilical cord blood gases be obtained whenever cesarean delivery is performed for fetal compromise, a low 5-minute Apgar score, severe fetal-growth restriction, an abnormal fetal heart rate tracing, maternal thyroid disease, or multifetal gestation (Chap. Animal experiments beginning in the late 1990s suggested that reducing brain temperature after an inciting event could reduce the incidence of cerebral damage (Gunn, 1997, 2000; Nedelcu, 2000; Tooley, 2003; Wagner, 2002). Benefits of Electronic Fetal Heart Rate Monitoring Several false assumptions underlie the expectation of improved perinatal outcome with electronic monitoring. One is that fetal distress is a slowly developing phenomenon and that electronic monitoring permits early detection of the compromised fetus. Within the past 20 years, attention has focused on the reality that most neurologically damaged fetuses suffered insults before arrival at labor units. The very term fetal monitor implies that this inanimate technology in some fashion "monitors. All of these assumptions led to great expectations and fostered the belief that all neonatal deaths or injuries were preventable. By the end of the 1970s, questions regarding the efficacy, safety, and costs of electronic monitoring were being voiced from the Office of Technology Assessment, the United States Congress, and the Centers for Disease Control and Prevention. Banta and Thacker (2002) reviewed 25 years of the controversy on the benefits, or lack thereof, of electronic fetal monitoring. More recently, Alfirevic and colleagues (2017) reviewed 13 randomized trials involving more than 37,000 women. They concluded that electronic fetal monitoring was associated with fewer neonatal seizures but a higher rate of cesarean and operative vaginal deliveries. Grimes and Peipert (2010) wrote a Current Commentary on electronic fetal monitoring in Obstetrics & Gynecology. They summarized that such monitoring, although it has been used in 85 percent of the almost 4 million annual births in the United States, has failed as a public health screening program. They noted that the positivepredictive value of electronic fetal monitoring for fetal death in labor or cerebral palsy is near zero-meaning that "almost every positive test result is wrong. They reported that monitoring raised operative delivery rates but lowered early neonatal mortality rates. This benefit was gestational-age dependent, however, and the highest effect was seen in preterm fetuses. Later, Ananth and colleagues (2013) reported a similar but larger epidemiological study in the United States. They studied nearly 58 million nonanomalous singleton liveborn neonates delivered between 1990 and 2004. The temporal increase in fetal monitoring use was associated with a decline in neonatal mortality rates, especially in preterm gestations. In an accompanying editorial, Resnik (2013) cautioned that an epidemiological association between fetal monitoring and reduced neonatal death does not establish causation. He suggested that the limitations of the study by Ananth should make the reader skeptical of the findings. At Parkland Hospital in July 1982, an investigation began to ascertain whether all women in labor should undergo electronic monitoring (Leveno, 1986). In alternating months, universal electronic monitoring was rotated with selective heart rate monitoring, which was the prevailing practice. During the 3-year investigation, more than 17,000 labors were managed using universal electronic monitoring, and these outcomes were compared with a similar-sized cohort of women selectively monitored electronically. With universal monitoring, a small but significant increase in the cesarean delivery rate for fetal distress was noted. Thus, greater application of electronic monitoring at Parkland Hospital did not improve perinatal results but did slightly raise the frequency of cesarean delivery for fetal distress. More recently, a Cochrane Database review found that intermittent auscultation had a higher cesarean delivery rate compared with continuous monitoring (Martis, 2017). Current Recommendations Methods most commonly used for intrapartum fetal heart rate monitoring include auscultation with a fetal stethoscope or a Doppler ultrasound device, or continuous electronic monitoring of the fetal heart rate and uterine contractions. No scientific evidence has identified the most effective method, including the frequency or duration of fetal surveillance that ensures optimum results. Summarized in Table 24-5 are the recommendations of the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists (2017). Intermittent auscultation or continuous electronic monitoring is considered an acceptable method of intrapartum surveillance in both low- and high-risk pregnancies. The recommended interval between checking the heart rate, however, is longer in the uncomplicated pregnancy. When auscultation is used, it is recommended that it be performed after a contraction and for 60 seconds. It also is recommended that a 1to-1 nursepatient ratio be used if auscultation is employed. The position taken by the American College of Obstetricians and Gynecologists (2017b) acknowledges that available data do not show a clear benefit to the use of electronic monitoring over intermittent auscultation. At Parkland Hospital, all high-risk labors are continuously monitored electronically. Thus, caution should be exercised before diagnosing true labor or its absence solely from a monitor tracing. With internal monitoring of contractions, amnionic fluid pressure is measured between and during contractions. In the past, a fluid-filled plastic catheter with its distal tip located above the presenting part was used. The catheter was connected to a strain-gauge pressure sensor adjusted to the same level as the catheter tip in the uterus. The amplified electrical signal produced in the strain gauge by variation in pressure within the fluid system was recorded on a calibrated moving paper strip simultaneously with the fetal heart rate recording. Today, intrauterine pressure catheters are used that have the pressure sensor in the catheter tip, which obviates the need for the fluid column. The catheter, contained within the introducer, is inserted into the birth canal and placed along one side of the fetal head. The catheter is then gently advanced into the uterus, and the introducer is withdrawn. With external monitoring, uterine contractions can be measured by a displacement transducer in which the transducer button, or "plunger," is held against the maternal abdominal wall. As the uterus contracts, the button moves in proportion to the strength of the contraction. This movement is converted into a measurable electrical signal that indicates the relative intensity of the contraction. It has generally been accepted that internal monitoring provided a more accurate measure of intensity. That said, Bakker and associates (2010) performed a randomized trial comparing internal versus external monitoring of uterine contractions in 1456 women. The two methods were equivalent in terms of operative delivery rates and neonatal outcomes. Patterns of Uterine Activity Caldeyro-Barcia and Poseiro (1960), from Montevideo, Uruguay, were pioneers in elucidating the patterns of spontaneous uterine activity throughout pregnancy. Contractile waves of uterine activity were usually measured using intraamnionic pressure catheters. But early in their studies, as many as four simultaneous intramyometrial microballoons were also used to record uterine pressure. Contraction intensity was defined as the rise in this pressure above a resting pressure baseline. These investigators also introduced the concept of Montevideo units to define uterine activity (Chap. With this definition, uterine performance is the product of contraction intensity in mm Hg multiplied by the number of contractions in a 10-minute span. For example, three contractions in 10 minutes, each of 50 mm Hg intensity, would equal 150 Montevideo units. During the first 30 weeks of pregnancy, uterine activity is comparatively quiescent. Contractions are seldom greater than 20 mm Hg, and these have been equated with those first described by John Braxton Hicks. Uterine activity increases gradually after 30 weeks, and it is noteworthy that these Braxton Hicks contractions also increase in intensity and frequency. According to Caldeyro-Barcia and Poseiro (1960), clinical labor usually commences when uterine activity reaches values between 80 and 120 Montevideo units. This translates into approximately three contractions of 40 mm Hg every 10 minutes. Importantly, no clear-cut division marks labor onset, which is a gradual and progressive transition. In first-stage labor, uterine contractions progressively grow in intensity from approximately 25 mm Hg at labor commencement to 50 mm Hg at its end. At the same time, the frequency advances from three to five contractions per 10 minutes, and uterine baseline tone rises from 8 to 12 mm Hg. Uterine activity is further enhanced during second-stage labor, aided by maternal pushing. Indeed, contraction intensity of 80 to 100 mm Hg is typical, and the uterus contracts as frequently as five to six times each 10 minutes. Hauth and coworkers (1986) quantified uterine contraction pressures in 109 women at term who received oxytocin for labor induction or augmentation. Most of these women achieved 200 to 225 Montevideo units, and 40 percent had up to 300 units to effect delivery. The authors suggested that these levels of uterine activity should be sought before consideration of cesarean delivery for presumed dystocia (Chap. Interestingly, the duration of uterine contractions-60 to 80 seconds-does not lengthen appreciably from early active labor through the second stage (Bakker, 2007; Pontonnier, 1975). During a uterine contraction, as the intrauterine pressure exceeds that of the intervillous space, respiratory gas exchange is halted.
Cheap generic floxin canada. Bootcamp Preclinical Toxicology: Making Safety a Part of Drug Design.
References
- Panicek DM, Gatsonis C, Rosenthal DI, et al. CT and MR imaging in the local staging of primary malignant musculoskeletal neoplasms: report of the Radiology Diagnostic Oncology Group. Radiology 1997;202(1):237-246.
- Stork S, van den Beld AW, von Schacky C, et al. Carotid artery plaque burden, stiffness, and mortality risk in elderly men: a prospective, population-based cohort study. Circulation 2004; 110:344-8.
- Engelman JA: Targeting PI3K signaling in cancer: opportunities, challenges and limitations, Nat Rev Cancer 9:550n562, 2009.
- Macpherson JM, Marangoz C, Miles TS, et al. Microstimulation of the supplementary motor area (SMA) in the awake monkey. Exp Brain Res 1982;45:410.
- Mazieres J, Peters S, Lepage B, et al. Lung cancer that harbors an HER2 mutation: epidemiologic characteristics and therapeutic perspectives. J Clin Oncol 2013;31(16):1997-2003.