
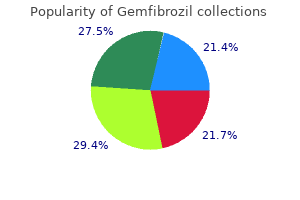
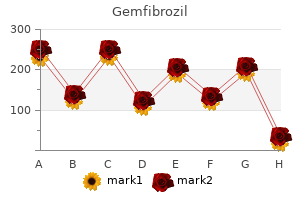
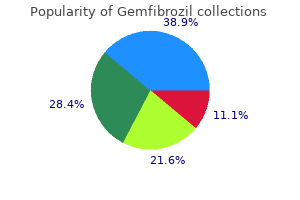
Gemfibrozil
| Contato
Página Inicial
Duncan G. de Souza, MD, FRCPC
- Assistant Professor
- Anesthesiology
- University of Virginia
- Charlottesville, Virginia
When it is located more proximally cholesterol ratio is 3.4 buy discount gemfibrozil 300 mg online, the transected main pulmonary artery may not be long enough to reach the aortic arch cholesterol phospholipid ratio trusted gemfibrozil 300 mg. A rectangular or oval piece of pulmonary homograft is then used to augment the posterior aspect of the opening in the arch and descending aorta cholesterol lowering foods list mayo clinic gemfibrozil 300 mg order online. The pulmonary base can then be sewn to the pulmonary homograft patch posteriorly and directly to the aortic arch anteriorly average cholesterol during pregnancy best purchase for gemfibrozil. Inadequate Aortopulmonary Window A direct anastomosis of a short pulmonary base to the arch may result in narrowing of the aortopulmonary window by pulling the arch inferiorly and the neoaortic root posteriorly cholesterol prescription medication gemfibrozil 300 mg buy. This can result in compression of the left pulmonary artery or left bronchus with serious consequences. Extension of Ductal Tissue In some patients, the ductal tissue extends into the aortic arch between the left carotid and left subclavian arteries. Others have a long ductus, which results in a short descending aorta after the ductal tissue is excised. Incision on Descending Aorta Some surgeons advocate making a 5- to 10-mm opening on the medial aspect of the transected descending aorta P. The pulmonary base is then anastomosed to the opening in the descending aorta and aortic arch. If the ascending aorta has been transected, it is now trimmed to a length of 10 to 15 mm and the open end is beveled. The anastomosis is performed in an end-to-side manner using a 7-0 or 8-0 Prolene suture. Note the probe introduced through the open arch anastomosis to prevent purse-stringing of the ascending aortic suture line. Too Long an Ascending Aorta If the diminutive aorta is left too long, it may kink, thereby causing coronary ischemia. Purse-Stringing the Anastomosis When the ascending aorta is 2 mm or less in diameter, the suture line of the main pulmonary artery to aortic arch may be left untied. More recently, many centers have adopted a right ventricle-to-pulmonary artery graft to provide pulmonary blood flow. The potential advantages of this shunt include a higher diastolic blood pressure in these patients, leading to improved coronary perfusion, and a decreased risk of shunt thrombosis perioperatively. Some questions remain regarding the optimal shunt size and material, the effect on pulmonary artery growth, and the impact of the right ventriculotomy on ventricular function. After transecting the main pulmonary artery just below the bifurcation, an appropriate site for the right ventriculotomy is marked on the right ventricular outflow tract. The confluence patch with the attached Gore-Tex tube is anastomosed to the opening at the pulmonary artery bifurcation. Right Ventricle-Pulmonary Artery Shunt During rewarming, a right ventriculotomy is made at the previously marked site. The proximal end of the tube graft is cut obliquely at the appropriate length and anastomosed to the ventriculotomy. Marking the position with the pulmonary root open is the best way to avoid injuring this valve. Size of Ventriculotomy Dynamic narrowing of the inflow to these shunts has been observed. An adequate core of muscle must be removed along with a slice of underlying endocardium. The ventriculotomy should be no larger than required for unobstructed shunt inflow. Some use a coronary arotic punch to remove the right ventricular muscle underlying the incision. If the "dunk" technique (See below) is utilized, a skin punch of appropriate size is used. To facilitate the second-stage procedure, some surgeons place the conduit from the right ventricle to the right pulmonary artery on the right side of the neoaorta. This may make removal of the prosthetic material easier, and simplify the reconstruction of any anastomotic narrowing. The standard left-sided shunt can also be encircled with a strip of Gore-Tex tape or Silastic that is left long and positioned in front of the neoaorta. This allows the conduit to be more easily found and dissected free at the second-stage procedure. Although many centers have adopted this technique, the long-term implications of this procedure are unknown. However, this source of pulmonary blood flow may be particularly applicable in low-birth-weight patients in whom a 3. Proximal Connection Some have advocated several options to reduce proximal conduit stenosis. The first is the so-called "dunk" technique in which 2 to 3 rings of the ringed Gore-Tex tube graft are inserted into the ventricular cavity and the graft secured with four tacking sutures and two purse-string sutures. Others have advocated for creating a hood on the proximal graft of homograft so as to reduce the angulation required in a direct connection. Gore-Tex Graft on Innominate Artery If a right ventricle-pulmonary artery shunt is constructed, the tube graft sewn to the innominate artery is occluded with a large metal clip near the anastomosis, cut short, and the end oversewn. Systemic-Pulmonary Shunt When selective cerebral perfusion has been performed, and a modified Blalock-Taussig shunt is desired, a new neoaortic cannula is placed and pump outflow transitioned to the new cannula. The shunt is then clamped with a bulldog vascular clamp for the remainder of the rewarming period. Shunt Placement on Pulmonary Artery the distal end of the shunt should be placed as centrally as possible, close to the oversewn ductus on the proximal pulmonary artery. In addition, it may allow the bidirectional Glenn procedure to be performed without cardiopulmonary bypass (see Chapter 31). After rewarming is completed, the shunt is opened and the patient is weaned off cardiopulmonary bypass. Pulmonary vascular resistance is often high for the first 15 to 30 minutes after weaning off bypass. If adequate ventricular function appears to be maintained, these low saturations should be tolerated. Persistent Low Oxygen Saturation If very low oxygen saturations persist, the cause must be determined. One cause of low systemic oxygen saturation is low cardiac output with very low mixed venous saturations. Direct visualization of the heart or, preferably, transesophageal assessment of ventricular function is useful. If decreased function is noted, an increase in inotropic support may improve the situation. If the myocardial contractility remains poor, extracorporeal membrane oxygenator support may be indicated. If a systemic-pulmonary shunt has been used, and shunt flow is thought to be inadequate, the patient should be placed back on cardiopulmonary bypass and the shunt revised. Persistent High Oxygen Saturations High oxygen saturations greater than 85% usually indicate excessive pulmonary blood flow. This may respond to modest hypoventilation and maintaining an inspired oxygen concentration of 21%. If it becomes clear that the problem is excessive shunt size, the shunt should be replaced with a 0. Alternatively, a metal clip may be carefully placed longitudinally on the shunt tubing to decrease its diameter. Residual Arch Obstruction Stenosis of the reconstructed aortic arch may lead to high systemic oxygen saturations because more blood will be directed to the innominate artery and through the shunt. Lower and upper body blood pressures should be checked if this possibility is considered. If a pressure difference greater than 10 mm is present, the patient should be placed back on cardiopulmonary bypass, and recooled so that the arch anastomosis can be revised. An oval patch of Silastic is sutured to the skin edges over the mediastinal chest tube. Povidone iodine (Betadine) ointment is applied to the suture line, and the entire chest is covered with a Betadine-impregnated Vi-Drape. Dysrhythmias After weaning off cardiopulmonary bypass, dysrhythmias often indicate inadequate coronary perfusion. If discoloration of the ventricle is observed or inadequate coronary arterial filling is noted, cardiopulmonary bypass should be recommenced. The anastomosis between the ascending aorta and proximal main pulmonary artery may need to be revised. Banding the pulmonary artery in such patients may encourage the development of a subaortic obstruction and should be avoided. In these cases, two outlets for systemic perfusion are created by anastomosing the pulmonary artery to the ascending aorta, often referred to as the Damus-Kaye-Stansel procedure. Controlled pulmonary blood flow is then established by interposing a Gore-Tex graft from the innominate artery to the right pulmonary artery. The thymus is excised, and a patch of autologous pericardium is harvested and prepared in 0. Cannulation the distal ascending aorta and right atrium are cannulated, and the ductus arteriosus is dissected free from surrounding structures. Procedure Cardiopulmonary bypass is commenced with systemic cooling, and the ductus arteriosus is occluded with a medium-sized metal clip. After a period of cooling, the aortic cross-clamp is applied and cardioplegic solution is infused into the aortic root. The distal opening is closed with an oval pericardial or pulmonary homograft patch with a continuous 6-0 Prolene suture. A generous longitudinal incision is made on the left side of the ascending aorta, adjacent to the pulmonary artery. The proximal pulmonary artery is then opened longitudinally adjacent to the incision in the aorta. The proximal portion of the anastomosis is started at the inferior extent of the incisions on the aorta and pulmonary artery with a running 6-0 or 7-0 Prolene suture. To prevent distortion of the pulmonary root, the distal aspect of the anastomosis is completed by using a hemicone-shaped patch of pericardium or pulmonary homograft to augment the pulmonary artery to aorta confluence with a continuous 6-0 or 7-0 Prolene suture. Tension on the Valvular Apparatus Care must be taken not to distort either the pulmonary or aortic valves when performing this anastomosis. Injury to the Valve When opening the ascending aorta, it is important to keep the incision above the commissures of the valve to avoid valvular insufficiency. Bleeding While performing the posterior aspect of the aorta to pulmonary artery anastomosis and patch augmentation, it is important to ensure complete hemostasis. Bleeding in this area after cessation of cardiopulmonary bypass is difficult to control. Cardiopulmonary bypass must be recommenced if additional adventitial sutures are to be placed in this situation. Alternative Technique Both the pulmonary artery and ascending aorta can be transected just above the sinotubular ridge. The adjacent edges of the two vessels are sewn together for approximately one-third to one-half of their circumferences. Then the distal ascending aorta is anastomosed to the posterior aspect of the double-barrel root with a 5-0 or 6-0 Prolene suture. The medial aspect of the aorta is opened and a corresponding opening is made in the proximal pulmonary artery. Inset: Fashioning the hemicone-shaped patch to complete the pulmonary artery-aortic anastomosis. A: the two roots are anastomosed together along adjacent sides and then attached to the ascending aorta. Completion of the Operation this is also the preferred method if any augmentation is required of the transverse aortic arch. After removal of the aortic cross-clamp, a modified Blalock-Taussig shunt using a 3. The shunt should be clamped until cardiopulmonary bypass is discontinued, at which point the shunt is opened. Vigorous hyperventilation may be required in the early postbypass period because pulmonary vascular resistance is often elevated during this time. The ultimate goal is to achieve a circulation in which the systemic venous return is delivered directly to the pulmonary arteries, and the single ventricle is used for systemic blood flow. The original Fontan operation utilized an atriopulmonary connection for patients with tricuspid atresia. Since then, the procedure and its indications have evolved, allowing for a Fontan circulation in many single-ventricle patients. Obstruction to systemic flow may lead to inadequate systemic perfusion and a low cardiac output state. The flow of blood through a patent ductus arteriosus bypasses the obstruction in either the pulmonary or systemic circulation, maintaining a clinically stable state. In a small group of patients, there is no or minimal obstruction to systemic or pulmonary blood flow. Initially, these patients may demonstrate well-balanced pulmonary and systemic circulations. However, as the pulmonary vascular resistance diminishes over the first several weeks of life, pulmonary blood flow increases and congestive heart failure develops. If pulmonary venous obstruction is present, the patient may be cyanotic owing to increased pulmonary vascular resistance.
Disturbances of this balance can be arrhythmogenic if they are sustained is there bad cholesterol in shrimp purchase gemfibrozil 300 mg mastercard, because even small wall-motion abnormalities in patients are associated with increased dispersion of repolarization cholesterol score of 8 buy discount gemfibrozil line. If cholesterol levels for 60 year old woman best 300 mg gemfibrozil, for example cholesterol medication dry mouth gemfibrozil 300 mg, an individual myocyte in situ was "less contractile" than its neighbors cholesterol medication comparison purchase generic gemfibrozil pills, then it would be stretched (or prevented from shortening) during systole. If this contributed to a gain of additional (or preservation of available) intracellular calcium, then it could enable affected cells to adapt their contractility to external demand on a beat-by-beat basis. Such matching of local contractility to dynamically varying external loads has been shown experimentally in mechanically Acknowledgments the author thanks Dr. Biotechnology and Biological Sciences Research Council, the European Commission, and the Magdi Yacoub Institute. Brines L, Such-Miquel L, Gallego D, et al: Modifications of mechanoelectric feedback induce1d by 2,3-butanedione monoxime and blebbistatin in Langendorff-perfused rabbit hearts. Guharay F, Sachs F: Stretch-activated single ion channel currents in tissue-cultured embryonic chick skeletal muscle. Garny A, Kohl P: Mechanical induction of arrhythmias during ventricular repolarisation: modelling cellular mechanisms and their interaction in 2D. Li W, Kohl P, Trayanova N: Induction of ventricular arrhythmias following a mechanical impact: a 12. Yoshida K, Ulfarsson M, Oral H, et al: Left atrial pressure and dominant frequency of atrial fibrillation in humans. Ambrosi P, Habib G, Kreitmann B, et al: Valsalva manoeuvre for supraventricular tachycardia in transplanted heart recipient. In Kohl P, Sachs F, Franz M, editors: Cardiac Mechano-Electric Coupling and Arrhythmias, Oxford, 2011, Oxford University Press, pp 361368. Befeler B: Mechanical stimulation of the heart: its therapeutic value in tachyarrhythmias. Klumbies A, Paliege R, Volkmann H: Mechanische Notfallstimulation bei Asystolie und extremer Bradykardie. Haman L, Parizek P, Vojacek J: Precordial thump efficacy in termination of induced ventricular arrhythmias. Pellis T, Kette F, Lovisa D, et al: Utility of precordial thump for treatment of out of hospital cardiac arrest: a prospective study. Chan L, Reid C, Taylor B: Effect of three emergency pacing modalities on cardiac output in cardiac arrest due to ventricular asystole. Kaufmann R, Theophile U: Automatie-fördernde Dehnungseffekte an Purkinje-Fäden, Papillarmuskeln und Vorhoftrabekeln von Rhesus-Affen. Casadei B, Moon J, Johnston J, et al: Is respiratory sinus arrhythmia a good index of cardiac vagal tone in exercise Bernardi L, Salvucci F, Suardi R, et al: Evidence for an intrinsic mechanism regulating heart rate variability in the transplanted and the intact heart during submaximal dynamic exercise Craelius W, Chen V, El-Sherif N: Stretch activated ion channels in ventricular myocytes. Kohl P, Bollensdorff C, Garny A: Effects of mechano-sensitive ion channels on ventricular electrophysiology: experimental and theoretical models. Dyachenko V, Christ A, Gubanov R, et al: Misalignment of sarcomeres by mechanical stimuli: an input signal for integrin dependent modulation of ion channels Tamargo J, Caballero R, Gomez R, et al: Pharmacology of cardiac potassium channels. Itano N, Okamoto S, Zhang D, et al: Cell spreading controls endoplasmic and nuclear calcium: a physical gene regulation pathway from the cell surface to the nucleus. Kaasik A, Kuum M, Joubert F, et al: Mitochondria as a source of mechanical signals in cardiomyocytes. Solovyova O, Katsnelson L, Konovalov P, et al: Activation sequence as a key factor in spatiotemporal optimization of myocardial function. Opthof T, Sutton P, Coronel R, et al: the association of abnormal ventricular wall motion and increased dispersion of repolarization in humans is independent of the presence of myocardial infarction. Dyachenko V, Rueckschloss U, Isenberg G: Modulation of cardiac mechanosensitive ion channels involves superoxide, nitric oxide and peroxynitrite. M1 and M2 are connected by an extracellular loop E1, whereas M2 and M3 are connected by a cytoplasmic loop. This general model is true for all the cardiac connexins and the other human connexins. Individual gap junction channels within the atrial and ventricular myocardium are found in abundance at the intercalated discs in the form of membrane complexes or plaques containing a large number of channels, ranging from hundreds to thousands. These plaques can also form along the lateral surfaces of myocytes in normal myocardium and can become even larger structures in stressed or diseased myocardium. The first analysis was performed on a noncardiac connexin, Cx26, and more recently has been revisited, revealing structural detail to a resolution of approximately 0. The structural analysis has not been sufficiently detailed to demonstrate clearly which membrane-spanning domains are forming the channel wall. This step is followed by a demonstration that the substitution does not affect normal channel activity. To establish whether the substituted group is part of the pore wall, a thiol reactive agent such as maleimide or a derivative is then perfused into the preparation while monitoring channel activity. One possible outcome is altered unitary conductance consistent, with the substituted group being a component of the pore wall. One of the roles of gap junction channels is to permit the passage of currents from cell to cell that are essential for action potential propagation throughout the working myocardium. When considering action potential propagation gap junctions can be best understood as components of the longitudinal resistance within the functional syncytium of the myocardium. The intercellular resistance of gap junctions is in series with the intracellular resistance of the cytoplasm, and together they represent longitudinal resistance. Both resistances can affect conduction velocity within the heart, but it is the gap junction channels composed of connexins that dominates longitudinal resistance. Dual whole-cell patch clamp studies of cardiac myocytes have been used to quantify gap junction membrane resistance or junctional conductance in vitro. The estimates of junctional resistance for ventricular myocyte cell pairs reveal that it is often an order of magnitude less than the input resistance of an isolated myocyte, somewhere in the range of 2 to 10 M or 1000 to 100 nS. To better understand how gap junction channels contribute to the normal functions of the heart and how they participate in cardiac arrhythmias and ischemia, it is necessary to first describe their structure and biophysical properties. Site-directed mutagenesis has also been used for Cx43 and Cx37 with various substitution strategies. For Cx37, site-directed mutations in M3 resulted in altered conductive states, which is consistent with M3 participation in forming the pore wall, but does not exclusively demonstrate that either. Cardiac Gap Junctions: Homomeric, Heterotypic, and Heteromeric Forms Hemichannels composed of six connexins from two closed aligned cells form a linkage via the extracellular domains E1 and E2 to create a complete gap junction channel. Instead, a select number of connexins are expressed within the human heart; they are Cx43, Cx40, Cx45, Cx46, and Cx37. As implied in Table 15-1, myocytes within the different regions of the heart are able to coexpress connexins. The expression of a single connexin within myocytes has the potential to generate functional gap junction channels composed of two identical hemichannels, both composed of the same connexin referred to as homomeric. Another type of gap junction channel is also possible, where each hemichannel of two opposing cells is homomeric but each cell expresses a different connexin. Biophysical Properties of Cardiac Gap Junction Channels the biophysical properties of gap junction channels are best illustrated using a dual whole-cell patch clamp on isolated cell pairs. All the cardiac gap junction channels have been studied in connexin-deficient cells that are then transfected with specific cardiac connexins to better understand how homotypic gap channel forms of Cx43, Cx40, Cx45, Cx46, and Cx37 behave. In all cases, each can be shown to gate closed with the application of increased transjunctional voltage (Vj). Ij,inst is the junctional current recorded at the onset of a voltage step, and Ij,ss is the steady state current. Multichannel and single-channel data have allowed the determination of unitary conductance (j,main) for the cardiac connexins, which are listed in Table 15-2. The ability to monitor unitary events has also allowed a better understanding of voltage-dependent gating in connexins, which has been shown to have at least two distinct mechanisms: fast gating and slow gating. This parameter represents the half inactivation voltage or that 15 Ij,inst Ij,ss Rj Rm,1 Rm,2 Ij 2s 100 pA A B 1. MultichannelandSingle-ChannelDataofDifferentTypes ofGapjunctionChannels Channel Type Homotypic Cx43 Cx40 Cx45 Cx46 Cx37 Heterotypic Cx40-Cx43 Cx40-Cx45 Cx43-Cx45 Cx37-Cx43 Co-expressed Cx40/Cx43 Cx37/Cx43 ±70 ±30/>100 31-130 35-280 46,54 53 -80/>100 n. Note that for one voltage polarity, a voltage-dependent deactivation or decline in junctional current is present, much like the homotypic forms. For the other polarity there is, in effect, little or no voltage-dependent closure. In the case of Cx40-Cx45 and to a lesser degree Cx43-Cx45, there is an increase in junctional current, which is best illustrated by the plots of gj versus Vj. This observation suggests that heterotypic gap junction channels have altered voltage sensing and gating relative to their homotypic parents and that Po for these forms might be significantly less than unity, or the asymmetric unitary conductance observed in heterotypic channels is itself voltage dependent. Thus, accurate measurement of total junctional conductance and knowing the unitary conductance for a particular connexin allows an estimate of the total number of functioning channels operating between a cell pair. To determine whether all of channels within a plaque are functional first requires a determination of the number of channels within any one plaque; second, it requires the determination of the number of functional channels within that particular plaque. An analysis of experiments using this dual approach of imaging and electrophysiologic assessment of junctional conductance has revealed that approximately 10% of the channels are functioning within junctional membrane plaques16; furthermore, it appears that Cx43 channels displayed non-independent behaviors associated with phenomena such as transitioning between an active patent state and a silent state on the order of many seconds to minutes, which represents an example of mode shifting. Are there conditions or circumstances in which the silent channels can be activated rapidly via phosphorylation, for example Or are the silent channels already designated or identified for internalization as connexosomes (internalized gap junction membranes) to be trafficked to lysosomes The instantaneous junctional conductance remains relatively constant regardless of the voltage, implying that many if not all the gap junctions are patent when Vj is zero. The application of Vj greater than 50 mV reduces the mean open time, whereas mean closed time remains relatively constant, which translates into reduced open probability (Po) with increased Vj amplitude. Nonstationary analyses of Cx43 and Cx37 have also revealed similar results with open probabilities less than 0. The values of Vj,o for homotypic channels vary from 20 mV for Cx45 to 60 mV for Cx43. Also listed are all the Vj,o values for heterotypic forms that have thus far been determined. Unitary conductance for the cardiac connexins varies greatly, as seen in Table 15-2. For heterotypic forms, the observed unitary conductance can be polarity dependent. Estimates of the number of K+ flowing through a single gap junction channel per second in response to a voltage step of approximately 23. For a number of the exogenous probes and select messengers, it has been possible to determine their flux relative to K+ for specific homotypic connexins, namely Cx43 and Cx40. As solute diameter increases, differences in permeability for the same solute begin to appear between Cx43 and Cx40. The permeability of two synthetic oligonucleotides are also plotted; they are long, rod-shaped molecules (morpholinos) whose minor diameters are 1. The notion of sympathetic and parasympathetic innervation density being less than one-to-one for nerve to myocyte, while never having been quantitatively assessed is consistent with observations describing low innervation density in the ventricular myocardium. With increased size and charge, Cx40 and Cx45 appear to be less permissive or more selective than Cx43. Action Potential Propagation in the Myocardium: the Role of Connexins Two questions arise when considering the role of gap junction channels in the propagation of the cardiac action potential. First, what is the relationship between gap junction number and conduction velocity The first question has been best addressed using a combination of experimental data and computational analysis. In vitro studies of cell pairs and isolated tissues have shown that a pharmacologically induced reduction in gap junctional conductance slows conduction and ultimately can block conduction, whereas increased expression enhances conduction. Results from animal model systems where connexin knockouts of Cx40 have been constructed are consistent with this notion. The second question as to whether gap junction voltage dependence can have a role in conduction velocity requires defining current flow longitudinally within myocytes in response to a propagating action potential. This definition then allows the determination of the transjunctional voltage experienced at the intercalated disc. It is assumed that a myocyte is approximately 100 µm long (L) and has a diameter of approximately 15 µm and that myoplasmic resistance is approximately 400 -cm. Assuming that conduction velocity () is 50 cm/s and that the maximum rate of rise for the action potential is 100 V/s, the longitudinal voltage drop along the long axis of the cell can be determined by Vcell = ([V / s] /) × L, or 20 mV. The former assumes a channel population of homotypic Cx43 channels each with a unitary conductance of approximately 55 pS (19). For 20,000 channels the value is approximately 10 mV per channel, and for 2000 channels it is approximately 100 mV per channel. Homotypic Cx43 unitary conductances of 55 pS are observed when using K+aspartate pipette solutions (see Table 15-2) that best mimic the myoplasmic electrolytes. It is possible for a transjunctional voltage of 10 to 20 mV or larger, as might occur with only a 1000 channels or fewer to result in voltage-dependent channel closure. To assess this possibility, it is necessary to determine how long a transjunctional voltage will persist during the passage of an action potential. What is the duration of the transjunctional voltage for an action potential conducting at 50 cm/s The time course of voltage-dependent closure varies from connexin to connexin, but for the cardiac connexins a 2-ms duration would result in a small reduction in junctional conductance. There are no easily demonstrable intercalated discs, rather the myocytes form smaller junctional plaques. NonVoltage-Dependent Regulators of Channel Patency There are two intrinsic intracellular elements that are able to affect junctional conductance: intracellular pH and intracellular calcium. Lowered intracellular pH, as occurs in ischemia,30 is known to affect many cardiac membrane channels and transporters and can effectively reduce gap junction conductance. The majority of the connexins are similarly affected by acidification, responding to elevated intracellular H+ with reduced junctional conductance that is presumed to be the result of increased closed times and reduced open times. The mechanism of pH-induced alteration of Cx43 gap junction channel open probability has been shown to be manifest by a ball-and-chain configuration between the C-terminus and the cytoplasmic loop between membranespanning domains M2 and M3. In contrast, Cx40 is also pH sensitive, but the mechanism of channel closure is not mediated by a ball-and-chainlike mechanism. The mechanism by which H+ affects Cx40 channel patency has not been elucidated, but the pKa for Cx40 is essentially the same as that for Cx43 (6.
When cornea is affected cholesterol lowering foods herbs order cheapest gemfibrozil and gemfibrozil, it should be treated with atropine cholesterol used in a sentence gemfibrozil 300 mg buy lowest price, steroids cholesterol uses order gemfibrozil with paypal, antibiotics and lubricants amount of good cholesterol in eggs order gemfibrozil american express. These may cause (i) photo- (12 gm orally/day) improves wound healing and promotes synthesis of the mature collagen by corneal fibroblasts cholesterol polyps buy 300 mg gemfibrozil mastercard. Treatment of complications, as below: · Secondary glaucoma should be treated by topical 0. The common ocular lesions include: · Radiation keratoconjunctivitis, · Radiation dermatitis of lids, · Radiation cataract, and · Radiation retinopathy. This is the simplest and most convenient method of topical application, especially for daytime use. Application in the form of eyedrops makes the drug available for immediate action but it is quickly diluted by tears within about a minute. However, the drug is not available for immediate use and ointments blur the vision. These have prolonged contact time like ointments and do not cause much blurring of vision. Pilocarpine ocuserts have been found very useful in patients with primary open-angle glaucoma; by efficiently controlling intraocular pressure with comparatively fewer side-effects. A pre-soaked soft contact lens in 1% pilocarpine has been found as effective as 4% pilocarpine eyedrops in patients with acute angleclosure glaucoma. Intraocular penetration of topically instilled drugs Topically instilled medications largely penetrate intraocularly through the cornea. The main barrier through cornea is its epithelium, which is lipophilic, and crossed readily by nonpolar drugs. Stroma being hydrophilic allows rapid passage of the drug through endothelium into the anterior chamber. Benzalkonium chloride used as preservative also acts as a wetting agent and thus increases the drug absorption. Nowadays, these are sparingly used to deliver drugs for optic neuritis, papillitis, posterior uveitis and also for administering retrobulbar block anaesthesia. Peribulbar anaesthesia has almost replaced the retrobulbar and facial block anaesthesia. Out of the borderline molecular weight drugs, those with high lipid solubility can pass easily. Anti-infective agents · Antibacterial agents · Antiviral drugs · Antifungal agents 2. Anti-inflammatory and immunosuppressive agents · Corticosteroid · Nonsteroidal anti-inflammatory drugs · Immunosuppressive and antimitotic drugs 5. Intraocular injections include: · Intracameral injection (into the anterior chamber), and · Intravitreal injection (into the vitreous cavity). Intravitreal drug implants are inserted in the vitreous cavity through pars plana for sustained and slow release. As there are a wide range of microorganisms, there are also specific antibiotics for almost each organism. Incidence of diarrhoea is less with it than with ampicillin and is thus better tolerated orally. All the cephalosporins have a bactericidal action against a wide range of organisms. In deep-seated inflammations of the orbit or lids, penicillin is given parenterally. In superficial inflammations of the conjunctiva and cornea it is administered locally as drops or ointments. These penicillins are not affected by penicillinase and are, therefore, used for staphylococcal infections which are resistant to other penicillins. Its spectrum is similar to ampicillin except that it is less effective against Shigella and H. Its oral absorption is better than ampicillin and thus higher and more sustained these are very active against Gram-positive cocci and thus have useful antistaphylococcal activity. These have anti-staphylococcal activity and are also effective against certain Gramnegative organisms. These are mainly effective against Gram-negative organisms but not against Staphylococci. Cephalosporins have a low frequency of adverse effects in comparison to antimicrobials in general. Aminoglycosides these are bactericidal and act primarily against Gram-negative bacilli. These are not absorbed orally, distributed mainly extracellularly and are excreted unchanged in the urine. Certain aminoglycosides are too toxic for systemic use and hence used only topically. It has a broader spectrum of action and is effective against Pseudomonas aeruginosa. It is 24 times more active against Pseudomonas aeruginosa and Proteus as compared to gentamicin. It is recommended as a reserve drug for hospital-acquired infections with Gram-negative bacilli, where gentamicin resistance is increasing. It is a widespectrum aminoglycoside, active against most Gram-negative bacilli and some Gram-positive cocci. Tetracyclines these are broad-spectrum bacteriostatic agents with a considerable action against both Gram-positive and Gram-negative organisms as well as some fungi, Rickettsiae and Chlamydiae. Antiviral drugs used in ophthalmology can be grouped as below: For herpes simplex virus infection · Idoxuridine · Vidarabine · Trifluridine · Acyclovir · Famiciclovir For herpes zoster virus infection · Acyclovir · Famiciclovir · Valaciclovir · Vidarabine · Sorvudine Table 19. Polypeptides these are powerful bactericidal agents, but rarely used systemically due to toxicity. Clinically used polypeptides are polymyxin B, bacitracin, colistin and tyrothricin. It is an effective broad-spectrum antimicrobial but suffers the disadvantage of a high incidence (68%) of sensitivity due to neomycin. Side-effects include follicular conjunctivitis, lacrimal punctal stenosis and irritation with photophobia. It is known to inhibit corneal stromal healing, hence its use is not advisable during first few weeks after keratoplasty. It has antiviral activity against herpes simplex, cytomegalo, vaccinia and zoster viruses. Dose: It is used 5 times a day till epithelialization occurs and then reduced to once or twice daily for 45 days to prevent recurrences. Side-effects are superficial punctate keratitis and irritation on prolonged application. Mechanism of action: It blocks nucleic acid synthesis by preventing conversion of cytosine ribose to cytosine deoxyribose. It causes profound corneal epithelial toxicity with superficial punctate keratitis and iritis. If no improvement occurs in 14 days, it is better to change to some other antiviral drug. It is available as 3% ophthalmic ointment and also as tablet for oral use and injection for intravenous use. Indications and doses: (a) Topical 3% ointment is used 5 times a day for epithelial as well as stromal herpes simplex keratitis. Side-effects: A few cases show slight punctate epithelial keratopathy which ceases once the drug is stopped. It is used for treatment of herpes zoster ophthalmicus in a dose of 500700 mg tds for 7 days. It is as effective as acyclovir in acute disease and is more effective in reducing late neuralgia. These are nontoxic, species-specific proteins possessing broad-spectrum antiviral activity. Topical application of 5% pimaricin suspension produces effective concentrations within the corneal stroma but not in intraocular fluid. It adheres well to the surface of the ulcer, making the contact time of the antifungal agent with the eye greater. Dose: 5 mg/kg body weight every 12 hours for 23 weeks, followed by a permanent maintenance dose of 5 mg/ kg once daily for 5 out of 7 days. These are isolated from various species of Streptomyces and consist of a large, conjugated, double-bond system in a lactose ring linked to an amino acid sugar. They work by binding to the sterol groups in fungal cell membranes, rendering them permeable. Polyenes do not penetrate well into the cornea and are not beneficial in deep stromal keratitis. This antibiotic may act as fungistatic or fungicidal depending upon the concentration of the drug and sensitivity of the fungus. Topically, it is effective in superficial infections of the eye in the concentration of 0. Subconjunctival injections are quite painful and more than 300 mg is poorly tolerated. Amphotericin B may be given intravitreally or/and intravenously for treatment of intraocular infections Various imidazole derivatives available for use in ocular fungal infections include: miconazole, clotrimazole, ketoconazole, econazole and itraconazole. Topical (1%) and subconjunctival (10 mg) application of miconazole produces high levels of drug in the cornea which is more dramatic in the presence of epithelial defect. Its 1% suspension is effective topically and is the treatment of choice in Aspergillus infections of the eye. It also has broadspectrum antifungal activity and is used topically as 1% econazole nitrate ointment. Because of its poor intraocular penetration, it is effective only in superficial infections of the eye. It is effective after oral administration and possesses activity against common fungi. It is given as single oral dose of 200400 mg daily up to at least one week after the symptoms have disappeared. It is prescribed for treatment of fungal infections caused primarily by Aspergillus, Histoplasmosis, Blastomycosis. It Chapter 19 Ocular Pharmacology mechanism of action 449 is available for oral and topical use. In primary open-angle glaucoma the miotics reduce this group includes flucystosine, which is a fluorinated salt of pyrimidine. This is achieved by changes in the trabecular meshwork produced by a pull exerted on the scleral spur by contraction of the longitudinal fibres of ciliary muscle. Combination of silver with sulfonamides and with other anti-microbial compounds significantly increases the activity against bacterial and fungal infections. Indications: (i) Primary open-angle glaucoma; (ii) Acute angleclosure glaucoma; (iii) Chronic synechial angleclosure glaucoma. Available preparations and dosage are: (a) Eye drops are available in 1%, 2% and 4% strengths. Except in very darkly pigmented irides maximum effect is obtained with a 4 percent solution. The onset of action occurs in 20 minutes, peak in 2 hours and duration of effect is 46 hours. This direct-acting sympathomimetic drug stimulates both alpha and beta-adrenergic receptors. Indications: It is a very good alternative to pilocarpine in resistant or intolerant cases. Decreased aqueous humour production occurs due to stimulation of alpha receptors in the ciliary body. Local side-effects are burning sensation, reactive hyperaemia of conjunctiva, conjunctival c. Chapter 19 mechanism of action Ocular Pharmacology 451 Timolol and levobunolol are nonselective beta-1 (cardiac) and beta-2 (smooth muscle, pulmonary) receptor blocking agents. The exact mechanism of action of betaxolol (cardioselective beta-blocker) is unknown. Betaxolol is the beta blocker, of choice in patients at risk for pulmonary diseases. It is a cardioselective beta-blocker and thus can be used safely in patients prone to attack of bronchial asthma; an advantage over timolol. It is available as 1% and 2% solution and is almost similar to timolol except that it induces comparatively less bradycardia. These include depression, anxiety, confusion, drowsiness, disorientation, hallucinations, emotional lability, dysarthria and so on. Paresthesias of the fingers, toes, hands, feet and around the mouth are experienced by most of the 452 Section iV Ocular Therapeutics 6. Urinary frequency may also be complained by most of patients due to the diuretic effect. These may be in the form of (i) Bicarbonate depletion leading to metabolic acidosis. Potassium supplement is indicated only when significant hypokalemia is documented. It is not related to the malaise symptom complex caused by biochemical changes in the serum.
Syndromes
- Stop walking and start again a few seconds later
- Radiation to the belly area
- Brief, shrill, high-pitched cry
- Shortness of breath with activity or after lying down (or being asleep for a while)
- Systematic desensitization or exposure therapy may be used to treat phobias. You are asked to relax, then imagine the things that cause the anxiety, working from the least fearful to the most fearful. Gradual exposure to the real-life situation has also been used with success to help people overcome their fears.
- For the main entree, use less meat or have meatless meals a few times a week. Use smaller amounts of meat to reduce the total fat content of the meal.
- Carcinoid syndrome
- Eat less organ meat (such as liver) and shellfish (such as shrimp and lobster)
- Amount swallowed
- Radiant warmer to maintain body temperature
If the anomalous coronary is not intramural cholesterol levels protein shakes safe 300 mg gemfibrozil, it can be excised with a button of aortic wall cholesterol test diet purchase gemfibrozil 300 mg fast delivery. The proximal course of the vessel is mobilized with the electrocautery on a low setting cholesterol level in quail eggs buy gemfibrozil uk, and it is reimplanted in the correct aortic sinus usually slightly higher than normal to prevent kinking average cholesterol daily 300 mg gemfibrozil order otc. The opening in the aorta is patched with a piece of glutaraldehyde-fixed pericardium or Gore-Tex cholesterol msds gemfibrozil 300 mg buy with amex. Good filling of the treated coronary artery branches should be noted before cardiopulmonary bypass is weaned. Aortic Valve Insufficiency Whether the anomalous coronary is unroofed or reimplanted, the commissure between the left and right aortic sinuses may needs to be partially dissected away from P. It must be subsequently resuspended to the aortic wall or patch to prevent aortic valve dysfunction. C: When the unroofing is complete, if the commissure requires resuspension this can be completed. Cardioplegia During the procedure, additional doses of cardioplegic solution are delivered directly into the coronary ostia with an olive-tipped cannula. Difficult Anatomy If inspection of the anomalous coronary anatomy suggests a technically difficult transfer or disruption of the intercoronary commissure by an unroofing procedure, the aorta should be closed and coronary bypass graft considered (the left or both internal thoracic arteries to the left system or the right internal thoracic artery to the right coronary). A stroke is a sudden onset of neurological impairment that is caused by a disruption of the blood supply to the brain (see Box 1. Ischaemic stroke is caused by obstruction of a blood vessel supplying the brain, either due to in-situ thrombus or embolus from a distant site (most commonly the carotid arteries or the heart). Subarachnoid haemorrhage, which usually occurs as a result of rupturing of an aneurysm, may also lead to stroke, but the clinical features and management are very different from stroke and are not covered in this book. Inpatient costs (£911 million per year) are dwarfed by the outpatient and community care costs. There have been considerable advances in our knowledge and understanding of stroke and how to manage it in recent years, particularly with regard to prevention (see Chapters 2, 3 and 11), acute treatment (Chapters 4 and 5) and rehabilitation (Chapters 69). Less progress has been achieved in the management of the longer-term issues facing stroke patients and their families (Chapter 12), including psychosocial problems (Chapter 10). These latter topics must form a focus for future service development and research initiatives. Pathology About 8090% of strokes are ischaemic in origin, and 1020% haemorrhagic. Haemorrhagic strokes tend to be more severe and are associated with higher early mortality. May cause a cranial nerve palsy and a motor and/or sensory deficit on one side of the body. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Another important association of haemorrhagic stroke is antithrombotic treatment with both anticoagulants and antiplatelet agents and thrombolysis (used in the acute treatment of ischaemic stroke and myocardial infarction). Several possible underlying pathologies, of which the commonest is aged-related hyaline arteriosclerosis of the small vessels supplying the brain. Over half of ischaemic strokes are caused by embolus, either from the heart or from atheromatous plaques. About a quarter are due to small vessel occlusion (lacunar stroke), and 15% to large vessel athero-thrombosis. In these terms, hypertension, smoking and atrial fibrillation can be regarded as the most important risk factors for stroke the first two because of their high prevalence and the latter both because of its high prevalence in the elderly (see Chapter 2) and its very strong association with stroke (Table 1. There is considerable overlap between the risk factors for stroke and the risk factors for ischaemic heart disease. The two most striking of these are: · · 3544 4554 5564 6574 7584 85+ Age group the stronger association between blood pressure and stroke risk than blood pressure and ischaemic heart disease; the apparent non-association between serum cholesterol level and risk of stroke in contrast to its strong association with risk of ischaemic heart disease. This reflects both the fall in incidence and improvement in survival following stroke. The downward trend goes back to the early part of the twentieth century, and is likely to reflect a combination of improvements in population health through better living conditions, changes in diet. Sociodemographic Although for a given age men are at a higher risk of stroke than women, overall women account for more strokes than men because of their longer life expectancy and the close association of stroke risk with age. The association of socio-economic status with stroke risk is due to a combination of individual lifestyle factors. The association between alcohol and stroke is complex, in that low levels of alcohol consumption are associated with a lower risk of stroke than complete abstinence. The extent to which this demonstrates a genuine protective effect of alcohol or reflects confounding by other factors. Raised blood pressure: doubling in risk of death from stroke for every 10 mmHg increase in diastolic blood pressure or 20 mmHg increase in systolic blood pressure · Hypercholesterolaemia · Hyperhomocysteinaemia · · Lifestyle Smoking: 50% increase in risk Excessive alcohol consumption: 50100% increase in risk · Physical inactivity: 2. It can be difficult to disentangle the extent to which family history as a risk factor reflects shared exposure to environmental risk factors or genetic predisposition. Recent genome-wide association studies have, however, found strong associations with a couple of gene loci, suggesting that genetic factors do play a part. Observational studies have demonstrated links between upper respiratory tract infections and risk of stroke, and between influenza vaccination and decreased risk of stroke. The explanation for this link remains unclear, though it is plausible that such infections might result in short-term increases in risk. However, such aggregated rates are of little meaning for an individual, given that survival is dependent on a host of factors, such as: · · · Other factors Oral contraception: doubling of risk Hormone replacement therapy: doubling of risk · Major life events · Influenza and other intercurrent infections blood pressures (at least down to a systolic blood pressure of 115 mmHg) are associated with a lower risk of stroke (and ischaemic heart disease). Although epidemiological studies have not demonstrated significant associations between cholesterol and stroke risk, the strong evidence from randomised controlled trials that cholesterol lowering with statins lowers stroke risk suggests that there is a causal association. Conversely, although epidemiological studies have shown a link between raised serum homocysteine levels and risk of stroke, randomised controlled trials have not unequivocally demonstrated that lowering homocysteine (through folate supplementation) leads to reduced stroke risk. Introduction to Stroke 5 · · · Ethnicity better prognosis in the African Caribbean population compared to the white population Atrial fibrillation associated with more severe strokes Co-morbidity such as prior stroke or diabetes, associated with worse survival. Health Care Needs Assessment: the Epidemiologically Based Needs Assessment Reviews, First series, 2nd edn, pp 141244. Physical recovery as measured by ability to perform the activities of daily living is usually maximal by six months after stroke, although more complex aspects of physical recovery such as speech and language abilities may improve over years. Two activities specific to stroke prevention are the use of antithrombotic therapy for atrial fibrillation and surgery for carotid artery stenosis. There are two complementary approaches to stroke prevention: population-based approaches, where the aim is to lower the level of a risk factor in the whole population; and individual-based approaches, where the aim is to identify and treat risk factors in people at high risk of disease. There is a deeper philosophical question about the extent to which health is determined by individual choice or by broader socio-economic and environmental factors that are better influenced by government. The potential role of this approach is being explored in a number of studies worldwide. Identification of people at high risk of stroke There are many potential risk factors for stroke (see Chapter 1). Several of these factors have been combined into risk scores based on analysis of cohort studies. These scores enable the future risk of a cardiovascular event to be calculated (see Table 2. Currently, a cut-off of greater than 20% risk over 10 years is used to identify those who should be offered drug therapy. The Framingham risk score has been in use for over 20 years, but has limitations in that it does not take into account factors such as social deprivation, family history and ethnicity. The core risk factors for cardiovascular disease blood pressure; cholesterol; smoking and diabetes are common to all the scores. Lowering blood pressure leads to important reductions in the risk of both stroke and heart disease. In the randomised trials of blood pressure-lowering therapy, lowering systolic blood pressure by 10 mmHg (or diastolic blood pressure by 5 mmHg) was associated with a 41% reduction in stroke risk and a 22% reduction in coronary heart disease risk. Cholesterol lowering People with raised cardiovascular risk should be offered treatment with a statin. Differences in lifestyle are associated with substantial differences in cardiovascular risk. For example: · · · · Someone eating five or more portions of fruit and vegetable per day has a 26% lower risk of stroke than someone who eats fewer than three A smoker has a 1. This suggests that statins do slow (or possibly even reverse) the development of atherosclerosis. This entails commencing simvastatin 40 mg, and not subsequently monitoring serum lipid levels or increasing the dose or using a higher-intensity statin. The results of a meta-analysis of randomised controlled trials of statins underline the significant benefits of treatment with this class of drug (Table 2. Long-term follow-up of one of these trials, the West of Scotland Coronary Prevention Study, found that the benefits of statin therapy were sustained for 10 years after the trial ended, even though after the trial finished similar proportions of the intervention and control groups were being treated with statins. The controversy revolves around the extent to which it is appropriate or not to extrapolate from randomised controlled trials in secondary prevention or to rely on indirect evidence from epidemiological analyses. The evidence that higher doses of lipid-modifying therapy lead to better outcome is in people with existing coronary heart disease. There is no direct evidence for intensification of lipid-lowering therapy in primary prevention. Again, there have been no trials of different target levels in primary prevention. A justification for targets can be made on the observational epidemiological evidence that lower total cholesterol (down to at least 4 mmol/L) is associated with lower risk of cardiovascular events. It is not clear which strategy would provide best value for money for primary prevention. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Aspirin reduces the risk of serious vascular events, with a relative risk of a vascular event of 0. In randomised controlled trials of primary prevention, this equates to annual risks of 0. The potential for harm needs to be set against this small reduction in the risk of vascular events. Aspirin increases the risk of major gastrointestinal and extra-cranial bleeds, with a relative risk of 1. Thus, on the face of it, aspirin would appear to prevent two major vascular events per major haemorrhage caused. However, risks of stroke and other vascular events have declined since these trials were performed (see Chapter 1), in part because of the emergence of statins. Conversely, it is unlikely that there has been any secular change in the risk of haemorrhage. If the risk of a cardiovascular event has halved because of the use of other drugs, then the ratio of harm to benefit reduces to about one to one, which is not a clear justification for aspirin therapy for primary prevention. While it might be tempting to consider using a cardiovascular risk threshold to determine which people might be offered aspirin therapy, in practice a major determinant of risk of a cardiovascular event is age, which is also a major determinant of risk of haemorrhage. Thus, older people potentially have more to gain from aspirin therapy, but also have more to lose. Aspirin in the primary and secondary prevention of vascular disease: Collaborative meta-analysis of individual participant data from randomised trials. Lipid Modification: Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. Antiplatelet therapy the pendulum has recently swung away from the use of antiplatelet agents for the primary prevention of stroke. Given the emergence of statins as an effective agent for primary prevention and improvements in blood pressure control in recent years, the additional benefit of aspirin has declined in absolute terms, such that it is not clear that the benefit of prevention of cardiovascular events is not neutralised by the increased risk of bleeding (see Box 2. Ongoing trials will clarify whether aspirin is still indicated for primary prevention in specific high-risk groups such as people with diabetes. It is becoming more common as a result of improved survival of people with ischaemic heart disease, which is its major cause. The scores are often grouped into three categories, with anticoagulation the preferred treatment for high risk, antiplatelet therapy for low risk, and either treatment for people at moderate risk. In practice, clinical decision making is a little more complex, as risk of bleeding (the major side effect of warfarin) needs to be taken into account. Validation of clinical classification schemes for predicting stroke: Results from the national registry of atrial fibrillation. Opportunistic: practice staff were encouraged to take the pulse of people aged over 64 when they attended the practice for any reason. Newer anticoagulants that do not require regular blood tests are being developed to mitigate the inconvenience of warfarin therapy. Screening versus routine practice in detection of atrial fibrillation in patients aged 65 or over: Cluster randomised controlled trial. Carotid artery stenosis Carotid artery stenosis that is, narrowing of the carotid artery caused by atherosclerosis increases the risk of stroke. Description of studies Three trials involving 5223 patients followed up for an average of 3. For example, in the Medical Research Council Trial published in 2004, 32 operations would be required to prevent one stroke over a 3. Furthermore, this benefit is likely to be still lower in people treated with current optimal medical therapy (antiplatelet agents, statins and antihypertensives). A less invasive treatment of carotid artery stenosis, carotid artery stenting (insertion of a tube under x-ray control to open up the narrowed artery) has been developed. However, results from randomised controlled trials suggest that this will only have a limited role to play, in that it is associated with a higher risk of perioperative stroke than endarterectomy (though lower risk of perioperative myocardial infarction). This operation has a clear role in people who have had a previous stroke or transient ischaemic attack (see Chapters 3 and 11), but its place in the management of people found to have carotid artery stenosis who have not had a stroke or transient ischaemic attack is less clear cut. This distinction is arbitrary some patients with symptoms lasting less than 24 hours have evidence of infarction on brain imaging, and others with more protracted symptoms have no such evidence. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: Implications for public education and organisation of services.
Discount gemfibrozil 300 mg buy. What is cholesterol?.
References
- Oca P, Zaka R, Dion AS, Freeman TA, Williams CJ. Phosphate and calcium are required for TGFbeta- mediated stimulation of ANK expression and function during chondrogenesis. J Cell Physiol 2010; 224(2):540-8.
- Guzman RP, Zierler RE, Isaacson JA, Bergelin RO, Strandness DE Jr. Renal atrophy and arterial stenosis: a prospective study with duplex ultrasound. Hypertension 1994;23: 346-350.
- Hussain M, Tangen CM, Berry DL, et al: Intermittent versus continuous androgen deprivation in prostate cancer, N Engl J Med 368(14):1314n1325, 2013.
- Gorlin R, Cohen MJ, Levin L. Syndromes of the head and neck. 4th ed. New York (NY): Oxford University Press; 2003.
- Ickeringill M, Shehabi Y, Adamson H, et al. Dexmedetomidine infusion with loading dose in surgical patients requiring mechanical ventilation: hemodynamic effects and efficacy. Anaesth Intensive Care. 2004;32:741-745.
- Lee PY, Fletcher WS, Sullivan ES, et al. Colorectal cancer in young patients: characteristics and outcome. Am Surg 1994;60(8):607-612.
- Rosa P, Hirsch DL, Dierks EJ. Congenital neck masses. Oral Maxillofac Surg Clin North Am 2008;20:339-359.
- Kummerling S, Schubert J: Peyronieis disease. Investigation of staging, erectile failure and operative management, Int Urol Nephrol 27(5):629n637, 1995.