
Hoodia
| Contato
Página Inicial
Lindsay A Borden, M.S., Ph.D.
- Assistant Professor of Psychiatry and Behavioral Sciences
https://www.hopkinsmedicine.org/profiles/results/directory/profile/10003757/lindsay-borden
Prophylaxis throughout pregnancy may be needed and higher doses may be required as pregnancy progresses earthworm herbals buy hoodia 400 mg amex. Respiratory: Pleural effusion (23%) 1% to 10%: Cardiovascular: Bradycardia (5%) herbs menopause buy generic hoodia 400 mg line, peripheral edema (5%) herbs landscaping order 400 mg hoodia fast delivery, thromboembolism (3%) herbals side effects purchase 400 mg hoodia otc, deep vein thrombosis (1%) Dermatologic: Pruritus (1%) Immunologic: Graft complications (skin graft failure in burn patients: 3%) Infection: Localized infection (grafts: 5%) Miscellaneous: Postoperative complication (bile leakage after hepatic surgery; 7%) ayur xaqti herbals cost of hoodia, fever (6% to 7%), procedural complications (seroma; 4%) Frequency not defined: Hematologic & oncologic: Decreased hemoglobin, hematoma Infection: Abscess (abdomen), staphylococcal infection Local: Incision site hemorrhage <1%, postmarketing, and/or case reports: Abdominal distension, anaphylactic shock, anaphylactoid reaction, anaphylaxis, angioedema, ascites, bile leakage (postprocedural), bronchospasm, catheter complication, cerebral embolism, cerebral infarction, chest discomfort, chills, dyspnea, edema, eosinophilia, erythema, flushing, gastrointestinal hemorrhage, granuloma, hemorrhage (internal, postprocedural), hemothorax, hepatitis C, hypersensitivity reaction, hypotension, inflammation, ischemic bowel disease, laryngeal edema, local hemorrhage (spleen), multiorgan failure, mydriasis, nerve compression, paralysis, parathyroid disease, paresthesia, procedural complications (thoracic cavity drainage), pulmonary embolism, renal artery thrombosis, renal failure, respiratory distress, tachycardia, thrombosis, urticaria, wheezing Mechanism of Action Formation of a biodegradable adhesive is done by duplicating the last step of the coagulation cascade, the formation of fibrin from fibrinogen. The solution also contains thrombin, which transforms fibrinogen from the sealer protein solution into fibrin, and fibrinolysis inhibitor (aprotinin), which prevents the premature degradation of fibrin. When mixed as directed, a viscous solution forms that sets into an elastic coagulum. Patches contain fibrinogen and thrombin that, in contact with bleeding surfaces, hydrate, form active fibrin, then produce a fibrin clot. Skin graft adhesion (Artiss only): To adhere autologous skin grafts to surgically prepared wound beds resulting from burns in adults and pediatric patients 1 year Pharmacodynamics/Kinetics Onset of Action Artiss: Full adherence achieved: ~2 hours Time to hemostasis: Evarrest: 4 minutes; Evicel: 4 to 10 minutes; Raplixa: 5 minutes; TachoSil: 3 to 6 minutes; Tisseel: 5 minutes Pregnancy Risk Factor C (manufacturer dependent) Pregnancy Considerations Animal reproduction studies have not been conducted. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions Frequency may vary by product and patient age. Peripheral blood progenitor cell collection and therapy (filgrastim and filgrastim biosimilars): Mobilization of autologous hematopoietic progenitor cells into the peripheral blood for apheresis collection Severe chronic neutropenia (filgrastim and filgrastim biosimilars): Long-term administration to reduce the incidence and duration of neutropenic complications (eg, fever, infections, oropharyngeal ulcers) in symptomatic patients with congenital, cyclic, or idiopathic neutropenia Note: Filgrastim-aafi (Nivestym) and filgrastim-sndz (Zarxio) are approved as biosimilars to filgrastim (Neupogen). Available data do not suggest an association between the use of filgrastim during pregnancy and an increased risk of miscarriage, preterm labor, or adverse fetal outcomes (birth weight or infection) following maternal use for severe chronic neutropenia. An international consensus panel has published guidelines for hematologic malignancies during pregnancy that suggest that although data are limited, administration of granulocyte growth factors during pregnancy may be acceptable (Lishner 2016). One review suggests when utilizing for hematopoietic stem cell mobilization (in healthy donors; not a labeled use) avoiding use during the first trimester until additional outcome information is available (Pessach 2013). Limitations of use: Efficacy in bitemporal recession has not been established; not indicated for use in women. Abnormalities of external male genitalia were reported in animal reproduction studies. Fingolimod causes immune suppression; medical consult needed prior to dental surgery. Effects on Bleeding No information available to require special precautions Adverse Reactions As reported in adults, unless otherwise noted. Elimination of fingolimod takes approximately 2 months; to avoid potential fetal harm, women of childbearing potential should use effective contraception to avoid pregnancy during and for 2 months after discontinuing treatment. Data collection to monitor pregnancy and infant outcomes following exposure to fingolimod is ongoing. Ventricular arrhythmias (prevention): Prevention of documented life-threatening ventricular tachyarrhythmias (eg, sustained ventricular tachycardia) in patients without structural heart disease. Because of the proarrhythmic effects of flecainide, its use should be reserved for patients in whom the benefits of treatment outweigh the risks. No evidence from controlled trials have demonstrated favorable effects of flecainide on survival or the incidence of sudden death. Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions >10%: Central nervous system: Dizziness (19% to 30%) Ocular: Visual disturbances (16%) Respiratory: Dyspnea (~10%) 1% to 10%: Cardiovascular: Palpitation (6%), chest pain (5%), edema (3. Dental professionals should be aware that recommendations differ between dental and general medical surgery. Pregnancy Risk Factor D Pregnancy Considerations Teratogenic effects have been observed in animal reproduction studies. Pharmacodynamics/Kinetics Duration of Action 6 to 8 hours Half-life Elimination Initial phase (distribution): 1 hour; second phase (elimination): 8 hours Time to Peak Plasma: Floctafenic acid: 1 to 2 hours Pregnancy Considerations Floctafenic acid, the active metabolite of floctafenine crosses the placenta. Effects on Dental Treatment Key adverse event(s) related to dental treatment: Abnormal taste. A maximum dose has not been established, but based on a small number of patients, doses up to 1,600 mg/day appear to be well tolerated (Anaissie 1995). Course may include 2 weeks of initial treatment with a lipid formulation of amphotericin B or an echinocandin. Note: Some experts do not routinely use prophylaxis in this setting (Kauffman 2018a). Pneumonia, symptomatic chronic cavitary and/or cavitary disease in immunocompromised patients: Oral: 400 mg once daily for 12 months. Alternate recommendations: Doses of 200 to 400 mg every 48 to 72 hours or 100 to 200 mg every 24 hours have been recommended. Use with caution in patients with renal and hepatic dysfunction or previous hepatotoxicity from other azole derivatives. Patients who develop abnormal liver function tests during fluconazole therapy should be monitored closely and discontinued if symptoms consistent with liver disease develop. Rare exfoliative skin disorders have been observed; fatal outcomes have been reported in patients with serious concomitant diseases. Monitor patients with deep seated fungal infections closely for rash development and discontinue if lesions progress. In patients with superficial fungal infections who develop a rash attributable to fluconazole, treatment should also be discontinued. Anaphylaxis has been reported rarely; use with caution in patients with hypersensitivity to other azoles. May occasionally cause dizziness or seizures; use caution driving or operating machines. Powder for oral suspension contains sucrose; use caution with fructose intolerance, sucrose-isomaltase deficiency, or glucose-galactose malabsorption. Treatment of breastfeeding women with nipple or breast candidiasis with oral fluconazole is common, especially in persistent or recurring infections (Brent 2001). Untreated candida nipple or breast infections may be painful for the mother and can contribute to premature weaning (Brent 2001). The amount of fluconazole contained in the breast milk is not sufficient to treat mucocutaneous candidiasis in the infant (Force 1995; Schilling 1993); concurrent treatment of both the breastfeeding infant and mother may be required (Chetwynd 2002). Decreased Effect Fluconazole may decrease the levels/effects of: Amphotericin B; Clopidogrel; Codeine; Ifosfamide; Losartan; Saccharomyces boulardii the levels/effects of Fluconazole may be decreased by: Didanosine; Etravirine; Rifamycin Derivatives Pharmacodynamics/Kinetics Half-life Elimination Normal renal function: ~30 hours (range: 20 to 50 hours); Elderly: 46. Abnormalities reported include brachycephaly, abnormal facies, abnormal calvarial development, cleft palate, femoral bowing, thin ribs and long bones, arthrogryposis, and congenital heart disease. Use of lower doses (150 mg as a single dose) suggest increased risks to the fetus, however, additional study is needed. The manufacturer recommends females of childbearing potential taking higher doses (400 mg/day) use effective contraception during therapy and for ~1 week after the final fluconazole dose. This milk concentration was obtained following maternal administration of oral fluconazole 200 mg daily for 18 days; the apparent elimination half-life of fluconazole in breast milk was 26. Flucytosine is metabolized to fluorouracil which may cause adverse events if administered during pregnancy; refer to the Fluorouracil (Systemic) monograph for additional information. Effects on Bleeding Thrombocytopenia (nadir: 16 days) and anemia reported in the majority of patients. Based on the mechanism of action, fludarabine may cause fetal harm if administered during pregnancy. Effective contraception should be used to avoid pregnancy during and after treatment for women and men with female partners of reproductive potential. Congenital adrenal hyperplasia, classic (salt-losing adrenogenital syndrome): Oral: 0. Oral: Maintenance therapy: Infants, Children, and Adolescents (actively growing): Usual range: 0. Mechanism of Action Very potent mineralocorticoid with high glucocorticoid activity; used primarily for its mineralocorticoid effects. Promotes increased reabsorption of sodium and loss of potassium from renal distal tubules. Dosing Adult & Geriatric Adrenal insufficiency, primary (Addison disease): Oral: Initial: 0. Prolonged use may increase risk of infection, mask acute infection (including fungal infections), prolong or exacerbate viral infections, or limit response to killed or inactivated vaccines. Amebiasis should be ruled out in any patient with recent travel to tropic climates or unexplained diarrhea prior to initiation of corticosteroids. Prolonged treatment with corticosteroids has been associated with the development of Kaposi sarcoma (case reports); if noted, discontinuation of therapy should be considered (Goedert 2002). Corticosteroid use may cause psychiatric disturbances, including euphoria, insomnia, mood swings, personality changes, severe depression to psychotic manifestation. Patients may require higher doses when subject to stress (ie, trauma, surgery, severe illness). With fludrocortisone, a decrease in dietary sodium is often not required as the increased retention of sodium is usually the desired therapeutic effect. When systemic corticosteroids are needed in pregnancy, it is generally recommended to use the lowest 602 Warnings: Additional Pediatric Considerations May cause osteoporosis (at any age) or inhibition of bone growth in pediatric patients. Fludrocortisone may be used to treat women during pregnancy who require therapy for congenital adrenal hyperplasia or primary adrenal insufficiency (Endocrine Society [Bornstein 2016; Speiser 2018]). Breastfeeding Considerations It is not known if fludrocortisone is excreted in breast milk; corticosteroids are excreted in breast milk. The manufacturer recommends that caution be exercised when administering fludrocortisone to nursing women. In the event of resedation: Repeat doses may be given at 20-minute intervals as needed at 0. Patients with a partial response at 3 mg may require (rare) additional titration up to a total dose of 5 mg (although doses >3 mg do not reliably produce additional effects). In the event of resedation, repeat doses may be given at 20minute intervals if needed, at 0. No differences in safety or efficacy have been reported; however, increased sensitivity may occur in some elderly patients. Dose should be individualized and practitioners should be prepared to manage seizures. Seizures may also develop in patients with concurrent major sedativehypnotic drug withdrawal, recent therapy with repeated doses of parenteral benzodiazepines, myoclonic jerking or seizure activity prior to flumazenil administration. Flumazenil is not a substitute for evaluation of oxygenation; establishing an airway and assisting ventilation, as necessary, is always the initial step in overdose management. Resedation occurs more frequently in patients where a large single dose or cumulative dose of a benzodiazepine is administered along with a neuromuscular-blocking agent and multiple anesthetic agents. Flumazenil should be used with caution in the intensive care unit because of increased risk of unrecognized benzodiazepine dependence in such settings. Flumazenil does not consistently reverse amnesia; patient may not recall verbal instructions after procedure. Use with caution in patients with a history of panic disorder; may provoke panic attacks. Use caution in drug and ethanol-dependent patients; these patients may also be dependent on benzodiazepines. Use with caution in patients with a head injury; may alter cerebral blood flow or precipitate convulsions in patients receiving benzodiazepines. Use caution in patients with mixed drug overdoses; toxic effects of other drugs taken may emerge once benzodiazepine effects are reversed. Use caution in hepatic 604 dysfunction; repeated doses of the drug should be reduced in frequency or amount. Warnings: Additional Pediatric Considerations Pediatric patients (especially 1 to 5 years of age) may experience resedation; these patients may require repeat bolus doses or continuous infusion. Dietary Considerations Avoid alcohol for the first 24 hours after administration or as long as the effects of benzodiazepines exist. Pharmacodynamics/Kinetics Onset of Action 1-2 minutes; 80% response within 3 minutes; Peak effect: 6-10 minutes Duration of Action Resedation occurs after ~1 hour (range: 19-50 minutes); duration related to dose given and benzodiazepine plasma concentrations; reversal effects of flumazenil may wear off before effects of benzodiazepine Half-life Elimination Children: Terminal: 20-75 minutes (mean: 40 minutes) Adults: Alpha: 4-11 minutes; Terminal: 40-80 minutes Moderate hepatic dysfunction: 1. Breastfeeding Considerations It is not known if flumazenil is excreted in breast milk. Flumazenil should only be used in an emergency situation and not as a means of hastening recovery from conscious sedation. Flumazenil should be used with caution in patients routinely taking benzodiazepines for other therapeutic uses, withdrawal symptoms will be induced. Pregnancy Risk Factor C Pregnancy Considerations Adverse effects were observed in some animal reproduction studies. Central nervous system: Drowsiness (20%), anxiety, depression, dizziness, extrapyramidal reaction, fatigue, insomnia, motor dysfunction, sedation, sleep disorder, vertigo Dermatologic: Skin rash Endocrine & metabolic: Weight gain (15%), galactorrhea, increased serum prolactin, menstrual disease Gastrointestinal: Heartburn, increased appetite, nausea, stomach pain, vomiting, xerostomia Neuromuscular & skeletal: Myalgia, weakness Mechanism of Action Flunarizine is a selective calcium channel blocker that prevents cellular calcium overload by reducing excessive transmembrane calcium influx; also has antihistamine properties. Has greater effect on decreasing the frequency of migraine attacks than on decreasing the severity or duration of attacks. Inhibits inflammatory cell migration and reverses increased capillary permeability to decrease access of inflammatory cells to the site of inflammation; does not depress hypothalamus. Use Body oil: Treatment of moderate to severe atopic dermatitis in pediatric patients 3 months; treatment of atopic dermatitis in adults Cream, ointment, topical solution: Relief of inflammatory and pruritic manifestations of corticosteroidresponsive dermatoses Scalp oil: Treatment of psoriasis of the scalp in adults Shampoo: Treatment of seborrheic dermatitis of the scalp Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions Frequency not defined. Atopic dermatitis: Topical: Body oil: Apply thin film to affected area 3 times daily Corticosteroid-responsive dermatoses: Topical: Cream, ointment, solution: Apply a thin layer to affected area 2 to 4 times daily; may use occlusive dressings to manage psoriasis or recalcitrant conditions Scalp psoriasis: Topical: Scalp oil: Massage thoroughly into wet or dampened hair/scalp; cover with shower cap. Seborrheic dermatitis of the scalp: Topical: Shampoo: Apply no more than 1 ounce to scalp once daily; work into lather and allow to remain on scalp for ~5 minutes. Pregnant females adequately controlled on flunisolide for asthma may continue therapy; if initiating treatment during pregnancy, use of an agent with more data in pregnant females may be preferred (Namazy 2016). May depress the formation, release, and activity of endogenous chemical mediators of inflammation (kinins, histamine, liposomal enzymes, prostaglandins) through the induction of phospholipase A2 inhibitory proteins (lipocortins) and sequential inhibition of the release of arachidonic acid. Not for oral, ophthalmic, or intravaginal use; do not apply to the face, axillae, groin, or diaper area unless directed by health care provider. Use the least amount needed to cover the affected area; discontinue when control is achieved. Shampoo: Has not been proven to be effective in corticosteroid responsive dermatoses other than seborrheic dermatitis of the scalp. Warnings: Additional Pediatric Considerations Topical corticosteroids may be absorbed percutaneously.
Total plasma concentrations of phenytoin are decreased in the mother during pregnancy; unbound plasma (free) concentrations are also decreased and plasma clearance is increased neem himalaya herbals 60 kapsuliu order generic hoodia. Due to pregnancyinduced physiologic changes herbs to help sleep hoodia 400 mg purchase otc, women who are pregnant may require dose adjustments of phenytoin in order to maintain clinical response; monitoring during pregnancy should be considered (Harden and Pennell 2009) herbals that reduce inflammation order hoodia now. Monitoring can then be continued once each trimester during pregnancy and postpartum; more frequent monitoring may be needed in some patients konark herbals discount hoodia 400 mg otc. In women taking phenytoin who are trying to avoid pregnancy herbals in hindi cheap hoodia 400 mg without prescription, potentially significant interactions may exist with hormone-containing contraceptives; consult drug interactions database for more detailed information. Pharmacodynamics/Kinetics Onset of Action Within 3 to 8 minutes Duration of Action 45 to 60 minutes Half-life Elimination 1 to 2 hours Pregnancy Considerations In general, medications used as antidotes should take into consideration the health and prognosis of the mother; antidotes should be administered to pregnant women if there is a clear indication for use and should not be withheld because of fears of teratogenicity (Bailey, 2003). Consultation with a clinical toxicologist or poison control center is recommended in patients who may require physostigmine administration. When indicated and used properly by a clinical toxicologist, physostigmine is safe and effective (Watkins 2015). Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Abnormal taste. Effects on Bleeding Phytonadione is a synthetic form of vitamin K and has been used as an antidote to reverse warfarin-induced bleeding complications or endogenous vitamin K deficiencies. Menadiol is a water soluble form of vitamin K; phytonadione has a more rapid and prolonged effect than menadione; menadiol sodium diphosphate (K4) is half as potent as menadione (K3). Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Salivation. In general, medications used as antidotes should take into consideration the health and prognosis of the mother; antidotes should be administered to pregnant women if there is a clear indication for use and should not be withheld because of fears of teratogenicity (Bailey 2003). Use of preservative free solutions are preferred when the injection is needed during pregnancy. Adverse Reactions >10%: Cardiovascular: Flushing (8% to 13%) Central nervous system: Chills (3% to 15%), dizziness (5% to 12%), headache (11%) Gastrointestinal: Nausea (6% to 15%) Genitourinary: Urinary frequency (9% to 12%) Neuromuscular & skeletal: Weakness (2% to 12%) Respiratory: Rhinitis (5% to 14%) Miscellaneous: Diaphoresis (29% to 68%) 1% to 10%: Cardiovascular: Edema (<1% to 5%), facial edema, hypertension (3%), palpitation, tachycardia Central nervous system: Pain (4%), fever, somnolence Dermatologic: Pruritus, rash Gastrointestinal: Diarrhea (4% to 7%), dyspepsia (7%), vomiting (3% to 4%), constipation, flatulence, glossitis, salivation increased, stomatitis, taste perversion Genitourinary: Vaginitis, urinary incontinence Neuromuscular & skeletal: Myalgias, tremor 1081 Hepatic Impairment: Adult Mild impairment (Child-Pugh score 5 to 6): No dosage adjustment necessary. Moderate impairment (Child-Pugh score 7 to 9): Initial: 5 mg twice daily; adjust dose based on response and tolerability. Use with caution in patients with cholelithiasis, biliary tract disease, and nephrolithiasis; may induce smooth muscle spasms, precipitating renal colic or ureteral reflux in patients with nephrolithiasis. Use with caution in patients with moderate hepatic impairment; dosage adjustment recommended; use is not recommended in patients with severe hepatic impairment. Effects on Dental Treatment Key adverse event(s) related to dental treatment: May cause orthostatic hypotension; monitor patient rising from dental chair for signs of dizziness. Effects on Bleeding No information available to require special precautions Drug Interactions Metabolism/Transport Effects None known. Increased Effect/Toxicity the levels/effects of Pilocarpine (Systemic) may be increased by: Acetylcholinesterase Inhibitors; BetaBlockers Decreased Effect Pilocarpine (Systemic) may decrease the levels/ effects of: Cimetropium; Sincalide Food Interactions Fat decreases the rate of absorption, maximum concentration and increases the time it takes to reach maximum concentration. Pharmacodynamics/Kinetics Onset of Action 20 minutes; Maximum effect: 1 hour Duration of Action 3 to 5 hours Half-life Elimination 0. Breastfeeding Considerations It is not known if pilocarpine is excreted in breast milk. Due to the potential for serious adverse reactions in the nursing infant, the manufacturer recommends a decision be made to discontinue nursing or to discontinue the drug, taking into account the importance of treatment to the mother. A dose of 5 mg daily produced a significant overall increase in both whole unstimulated salivary flow and parotid stimulated salivary flow. Time to Peak 6 hours (median: 4 to 24 hours) Pregnancy Considerations Adverse events were observed in some animal reproduction studies. Prevents release of inflammatory cytokines and mediators from mast cells in vitro after stimulation by antigen/IgE. Pharmacodynamics/Kinetics Onset of Action Time to significant improvement: 8 days (Wellington 2001) Half-life Elimination Terminal: Oral: 30 to 40 hours Time to Peak Serum: Topical: 2 to 6 hours Pregnancy Risk Factor C Pregnancy Considerations Adverse events were not observed in animal reproduction studies following topical application. Augmentive action of antidepressants thought to be mediated via a serotonin 1A autoreceptor antagonism. Dental Health Professional Considerations See Local Anesthetic/Vasoconstrictor Precautions Pharmacodynamics/Kinetics Half-life Elimination 3 to 4 hours; prolonged in the elderly (average 7 hours; up to 15 hours reported), and cirrhosis (range: 2. Pindolol crosses the placenta and is measurable in the cord blood and amniotic fluid (Gonçalves 2007). The clearance and volume of distribution of pindolol are increased during pregnancy (Gonçalves 2002). Time to Peak ~2 hours; delayed with food Pregnancy Considerations Information related to the use of pioglitazone in pregnant women is limited (Glueck 2003; Ortega-Gonzalez 2005; Ota 2008). Thiazolidinediones may cause ovulation in anovulatory premenopausal women, increasing the risk of unintended pregnancy. Effects on Bleeding No information available to require special precautions Adverse Reactions Adverse reactions and incidences reported are associated with monotherapy unless otherwise stated. It has a mechanism of action that is dependent on the presence of insulin for activity. Glimepiride: A sulfonylurea that stimulates insulin release from the pancreatic beta cells; reduces glucose output from the liver; insulin sensitivity is increased at peripheral target sites. Pregnancy Considerations Use pioglitazone with caution in premenopausal, anovulatory women; may result in a resumption of ovulation, increasing the risk of pregnancy. Pelvic infections: Treatment of postpartum endometriosis or pelvic inflammatory disease caused by betalactamase-producing strains of E. Pneumonia, hospital-acquired (nosocomial): Treatment of moderate to severe hospital-acquired (nosocomial) pneumonia caused by beta-lactamaseproducing strains of Staphylococcus aureus and by piperacillin/tazobactam-susceptible Acinetobacter baumannii, H. Skin and skin structure infections: Treatment of skin and skin structure infections, including cellulitis, cutaneous abscesses, and ischemic/diabetic foot infections caused by beta-lactamase-producing strains of S. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Pioglitazone-dependent patients with diabetes (noninsulin dependent, type 2) or metformin-dependent patients with diabetes (noninsulin dependent, type 2) should be appointed for dental treatment in morning in order to minimize chance of stress-induced hypoglycemia. Effects on Bleeding No information available to require special precautions Adverse Reactions Percentages of adverse effects as reported with the combination product. The clinical significance may be greater with those penicillins that are combined with a betalactamase inhibitor and/or with agents that have greater activity against specific enteric bacterial species. Metformin decreases hepatic glucose production, decreasing intestinal absorption of glucose, and improves insulin sensitivity (increases peripheral glucose uptake and utilization). Tazobactam inhibits many beta-lactamases, including staphylococcal penicillinase and Richmond-Sykes types 2, 3, 4, and 5, including extended spectrum enzymes; it has only limited activity against class 1 beta-lactamases other than class 1C types. Normal platelet function should occur in ~5 elimination half-lives or in <10 hours after discontinuation of piroxicam. Due to pregnancy-induced physiologic changes, some pharmacokinetic properties of piperacillin/tazobactam may be altered (Bourget 1998). Piperacillin/tazobactam is approved for the treatment of postpartum gynecologic infections, including endometritis or pelvic inflammatory disease, caused by susceptible organisms. Effects on Dental Treatment Key adverse event(s) related to dental treatment: Assess unusual presentations of muscle weakness or myopathy resulting from lipid therapy such as patient having a difficult time brushing teeth or weakness with chewing. Pharmacodynamics/Kinetics Onset of Action Analgesia: Oral: Within 1 hour; Maximum effect: 3 to 5 hours Half-life Elimination Children and Adolescents 7 to 16 years: 32. Pharmacodynamics/Kinetics Half-life Elimination ~12 hours Time to Peak ~1 hour Pregnancy Considerations Pitavastatin is contraindicated in pregnant females or those who may become pregnant. Pitavastatin should be discontinued immediately if an unplanned pregnancy occurs during treatment. Adverse Reactions 1% to 10%: Cardiovascular: Hypertension (2%), hypotension (1%) Central nervous system: Headache (1%) Gastrointestinal: Diarrhea (2%), nausea (1%), vomiting (1%) Genitourinary: Nephrotoxicity (4%) Otic: Ototoxicity (2%) Renal: Increased serum creatinine (4%; CrCl: 30 to 90 mL/minute: 10%), acute renal failure (4%), decreased creatinine clearance (4%), renal disease (4%), renal failure syndrome (4%), renal insufficiency (4%) Frequency not defined: Central nervous system: Dizziness Endocrine & metabolic: Hypokalemia Gastrointestinal: Constipation, gastritis Genitourinary: Hematuria Hepatic: Increased serum alanine aminotransferase Respiratory: Dyspnea <1%, postmarketing, and/or case reports: Hypoacusis (reversible), tinnitus (irreversible), vertigo Mechanism of Action Interferes with bacterial protein synthesis by binding to 30S ribosomal subunit resulting in a defective bacterial cell membrane. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Oral mucosal ulcers have been reported; prolonged use may result in oral opportunistic fungal infections Effects on Bleeding No information available to require special precautions Adverse Reactions 1% to 10%: Gastrointestinal: Diarrhea, nausea Genitourinary: Vulvovaginal candidiasis <1%, postmarketing, and/or case reports: Abdominal pain, abnormal hepatic function tests, acute porphyria, anaphylaxis, Clostridioides (formerly Clostridium) difficile colitis, decreased plasma carnitine concentrations, dizziness, dyspepsia, erythematous rash, esophageal ulcer, esophagitis, fatigue, headache, hypersensitivity reaction, macular eruption, maculopapular rash, oral mucosa ulcer, pruritus, skin rash, thrombocytopenia, urticaria, vertigo, vomiting Mechanism of Action Pivmecillinam is a 6-aminopenicillanic acid derivative that is metabolized to the active form of the drug, mecillinam. There are several reports of total irreversible bilateral congenital deafness in children whose mothers received another aminoglycoside (streptomycin) during pregnancy. Although serious side effects to the fetus/ infant have not been reported following maternal use of all aminoglycosides, a potential for harm exists. Information related to the use of pivmecillinam in pregnancy is available (Guinto 2010; Kier 1986; Larsen 2001; Nørgaard 2008; Vinther Skriver 2004). The manufacturer notes pivmecillinam may be used in pregnancy when clinically needed. Product Availability Selexid: Health Canada approved July 2016; anticipated availability is unknown. Pregnancy Considerations Plecanatide and its metabolite are not measurable in plasma when used at recommended doses. Women of reproductive potential should use effective contraceptive measures to avoid becoming pregnant during treatment. Effects on Bleeding No information available to require special precautions Adverse Reactions Adverse reactions reported with filgrastim combination therapy. Limited data related to systemic use in pregnancy are available (Heinonen 1977; Kazy 2005). Based on the relative toxicity compared to other antibiotics, systemic use in pregnancy is not recommended (Knothe 1985). Due to poor tissue diffusion, topical use would be expected to have only minimal risk to the mother or fetus (Leachman 2006). Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding Chemotherapy may result in significant myelosuppression, neutropenia (50% to 52%; grades 3/4: 43% to 47%), anemia (38%; grades 3/4: 22%), thrombocytopenia (25%; grades 3/4: 22%), leukopenia (11%; grades 3/4: 6%). Pomalidomide is an analogue of thalidomide (a known human teratogen) and may cause severe birth defects or embryo-fetal death if taken during pregnancy. In females of reproductive potential, obtain 2 negative pregnancy tests prior to initiation of treatment; females of reproductive potential must avoid pregnancy and use 2 forms of contraception (or continuously abstain from heterosexual sex) beginning at least 4 weeks prior to , during, and for at least 4 weeks after stopping pomalidomide treatment (and during treatment interruptions). Studies in animals have shown evidence of fetal abnormalities and use is contraindicated in women who are or may become pregnant. Pregnancy tests should be performed 10 to 14 days and 24 hours prior to beginning therapy; weekly for the first 4 weeks and then every 4 weeks (every 2 weeks if menstrual cycle irregular) thereafter and during therapy interruptions for at least 4 weeks after discontinuation. Pomalidomide must be immediately discontinued for a missed period, abnormal pregnancy test or abnormal menstrual bleeding; refer patient to a reproductive toxicity specialist if pregnancy occurs during treatment. Males (including those vasectomized) should use a latex or synthetic condom during any sexual contact with women of childbearing age during treatment, during treatment interruptions, and for 28 days after discontinuation. Prescribing and Access Restrictions In Canada, pomalidomide is only available through a restricted distribution program called RevAid. Only physicians and pharmacists registered with the program are authorized to prescribe or dispense pomalidomide. Two negative pregnancy tests with a sensitivity of at least 25 milliunits/mL are required prior to initiating therapy in women of childbearing potential. Local Anesthetic/Vasoconstrictor Precautions Ponatinib may cause hypertension; monitor blood pressure prior to vasoconstrictor use Effects on Dental Treatment Key adverse event(s) related to dental treatment: Oral mucositis Effects on Bleeding Chemotherapy may result in significant myelosuppression, potentially including significant reduction in platelet counts (thrombocytopenia grades 3/4: 36% to 57%) and altered hemostasis. Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions All reported adverse reactions occurred in premature neonates as safety and efficacy has not been established in full term neonates and older pediatric patients with respiratory failure. Cardiovascular: Patent ductus arteriosus (60%), bradycardia, hypotension Hematologic & oncologic: Oxygen desaturation Miscellaneous: Obstruction of endotracheal tube <1%, postmarketing, and/or case reports: Pulmonary hemorrhage Mechanism of Action Endogenous pulmonary surfactant reduces surface tension at the air-liquid interface of the alveoli during ventilation and stabilizes the alveoli against collapse at resting transpulmonary pressures. A deficiency of pulmonary surfactant in preterm infants results in respiratory distress syndrome characterized by poor lung expansion, inadequate gas exchange, and atelectasis. Pharmacodynamics/Kinetics Half-life Elimination ~24 hours (range: 12 to 66 hours) Time to Peak 6 hours Pregnancy Considerations Based on animal data and its mechanism of action, ponatinib is expected to cause fetal harm if used during pregnancy. Women of childbearing potential should use effective contraception during treatment and for 3 weeks after the last dose. Exposure of the drug to laser light at wavelengths >630 nm results in the production of oxygen freeradicals. Release of thromboxane A2, leading to vascular occlusion and ischemic necrosis, may also occur. Oropharyngeal candidiasis: Suspension (13 years and older): Treatment of oropharyngeal candidiasis (including patients refractory to itraconazole and/or fluconazole) Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Xerostomia (normal salivary flow resumes upon discontinuation), abnormal taste, mucositis. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions Adverse reactions occurred with potassium chloride injection unless otherwise specified. Frequency not defined: Cardiovascular: Asystole (with rapid administration or hyperkalemia), bradycardia, chest pain, thrombosis (infusion site), ventricular fibrillation (with rapid administration or hyperkalemia) Dermatologic: Skin rash (oral and injection) Endocrine & metabolic: Hyperkalemia (oral and injection) Gastrointestinal: Abdominal cramps (oral), abdominal distress (oral), abdominal pain (oral), diarrhea (oral), flatulence (oral), gastrointestinal hemorrhage (oral), gastrointestinal irritation (oral), gastrointestinal obstruction (oral), gastrointestinal perforation (oral), gastrointestinal ulcer (oral), nausea (oral), vomiting (oral) Hypersensitivity: Angioedema, hypersensitivity reaction Local: Burning sensation at injection site, erythema at injection site, injection site phlebitis, irritation at injection site, swelling at injection site Respiratory: Dyspnea Mechanism of Action Potassium is the major cation of intracellular fluid and is essential for the conduction of nerve impulses in heart, brain, and skeletal muscle; contraction of cardiac, skeletal and smooth muscles; maintenance of normal renal function, acid-base balance, carbohydrate metabolism, and gastric secretion Pregnancy Considerations Potassium requirements are the same in pregnant and nonpregnant women. Adverse events have not been observed following use of potassium supplements in healthy women with normal pregnancies. Potassium supplementation (that does not cause maternal hyperkalemia) would not be expected to cause adverse fetal events. Pharmacodynamics/Kinetics Half-life Elimination Suspension: 35 hours (range: 20 to 66 hours); Tablets: 26 to 31 hours; Injection: ~27 hours Time to Peak Plasma: Suspension: ~3 to 5 hours; Tablets: ~4 to 5 hours Pregnancy Considerations Adverse events have been observed in animal reproduction studies. The repolarization process within the myocardial cell is due to the efflux of intracellular potassium. The channels associated with this current can be blocked by many drugs and predispose the electrical propagation cycle to torsade de pointes. Local: Edema, irritation, pruritus, rash Mechanism of Action Povidone-iodine is known to be a powerful broad spectrum germicidal agent effective against a wide range of bacteria, viruses, fungi, protozoa, and spores. Povidine-iodine is absorbed systemically as iodine following topical administration to the vaginal mucosa (Velasco 2009; Vorherr 1980). Following vaginal administration as a douche, iodine concentrations are increased in the maternal urine, amniotic fluid, cord blood and fetal thyroid (Bachrach 1984; Mahillon 1989). Transient hypothyroidism in the newborn has been reported following topical use prior to delivery (Danziger 1984). Pharmacodynamics/Kinetics Half-life Elimination 12 to 18 hours Pregnancy Risk Factor D Pregnancy Considerations Adverse effects were observed in animal reproduction studies. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Mucositis and stomatitis Effects on Bleeding No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: Xerostomia (normal salivary flow resumes upon discontinuation) and dysphagia. Effects on Bleeding No information available to require special precautions Adverse Reactions Actual frequency may be dependent on dose, formulation, and/or concomitant levodopa. By binding to these receptors, it is thought that pramipexole can stimulate dopamine activity on the nerves of the striatum and substantia nigra. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions >10%: Central nervous system: Headache (5% to 13%) Endocrine & metabolic: Severe hypoglycemia (type 1 diabetes 17%) Gastrointestinal: Nausea (28% to 48%), anorexia (17%), vomiting (7% to 11%) Miscellaneous: Accidental injury (8% to 14%) 1% to 10%: Central nervous system: Fatigue (3% to 7%), dizziness (2% to 6%) Endocrine & metabolic: Severe hypoglycemia (type 2 diabetes 8%) Gastrointestinal: Abdominal pain (2% to 8%) Hypersensitivity: Hypersensitivity reaction (6%) Neuromuscular & skeletal: Arthralgia (2% to 7%) Respiratory: Cough (2% to 6%), pharyngitis (3% to 5%) Postmarketing and/or case reports: Injection site reaction, pancreatitis Mechanism of Action Synthetic analog of human amylin cosecreted with insulin by pancreatic beta cells; reduces postprandial glucose increases via the following mechanisms: 1) prolongation of gastric emptying time, 2) reduction of postprandial glucagon secretion, and 3) reduction of caloric intake through centrallymediated appetite suppression Pharmacodynamics/Kinetics Duration of Action ~3 hours Half-life Elimination ~48 minutes Time to Peak 20 minutes Pregnancy Risk Factor C Pregnancy Considerations Adverse events have been observed in animal reproduction studies. Effects on Bleeding Prasugrel blocks platelet aggregation and may prolong bleeding time.
Hypersensitivity and anaphylactic reactions have been reported with acetaminophen use; discontinue immediately if symptoms of allergic or hypersensitivity reactions occur herbalshopcom buy generic hoodia 400 mg online. Symptoms of opioid withdrawal may include excessive crying herbals shoppe hedgehog products 400 mg hoodia mastercard, diarrhea himalaya herbals products hoodia 400 mg low cost, fever shahnaz herbals 400 mg hoodia order amex, hyper-reflexia herbals inc hoodia 400 mg order with amex, irritability, tremors, or vomiting or failure to gain weight. Opioid withdrawal syndrome in the neonate may be life-threatening and should be promptly treated. Avoid Concomitant Use Avoid concomitant use of Hydrocodone and Acetaminophen with any of the following: Alcohol (Ethyl); Azelastine (Nasal); Bromperidol; Conivaptan; Eluxadoline; Fusidic Acid (Systemic); Idelalisib; Opioids (Mixed Agonist / Antagonist); Orphenadrine; Oxomemazine; Paraldehyde; Thalidomide Breastfeeding Considerations Acetaminophen and hydrocodone are present in breast milk. Because of addiction liability of opioid analgesics, the use of hydrocodone should be limited to 2-3 days postoperatively for treatment of dental pain. Nausea elicited by opioid analgesics is centrally mediated and the presence or absence of food will not affect the degree nor incidence of nausea. Acetaminophen may increase the levels and enhance the anticoagulant effects of vitamin K antagonists acenocoumarol and warfarin (Coumadin). Limitations of use: Do not use hydrocodone/ibuprofen for the treatment of conditions such as osteoarthritis or rheumatoid arthritis. Reserve hydrocodone/ibuprofen for use in patients for whom alternative treatment options (eg, nonopioid analgesics) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain. Discontinuation of therapy: Decrease dose by 25% to 50% every 2 to 4 days; monitor carefully for signs/ symptoms of withdrawal. If patient displays withdrawal symptoms, increase dose to the previous level and then reduce dose more slowly by increasing interval between dose reductions, decreasing amount of daily dose reduction, or both. Other factors associated with increased risk include younger age, concomitant depression (major), and psychotropic medication use. Even in patients without prior exposure anaphylactoid reactions may occur; patients with "aspirin triad" (bronchial asthma, aspirin intolerance, rhinitis) may be at increased risk. Blurred/diminished vision, scotomata, and changes in color vision have been reported with ibuprofen. Use with caution in patients with hypersensitivity reactions to other phenanthrene derivative opioid agonists (codeine, hydromorphone, levorphanol, oxycodone, oxymorphone). Use with caution in cachectic or debilitated patients and in the elderly; consider the use of alternative nonopioid analgesics in these patients. Onset, duration, and severity depend on the drug used, duration of use, maternal dose, and rate of drug elimination by the newborn. Withhold for at least 4 to 6 half-lives prior to surgical or dental procedures (Douketis 2008). Concurrent use of agonist/antagonist analgesics may precipitate withdrawal symptoms and/or reduced analgesic efficacy in patients following prolonged therapy with mu opioid agonists. Breastfeeding Considerations Hydrocodone and ibuprofen are excreted in breast milk. Dermatologic diseases: Atopic dermatitis; bullous dermatitis herpetiformis; contact dermatitis; exfoliative dermatitis; exfoliative erythroderma; pemphigus; severe erythema multiforme (Stevens-Johnson syndrome); severe psoriasis; severe seborrheic dermatitis; mycosis fungoides. Edematous states: To induce diuresis or remission of proteinuria in the nephrotic syndrome, without uremia, of the idiopathic type or that due to lupus erythematosus. Endocrine disorders: Acute adrenocortical insufficiency; congenital adrenal hyperplasia; hypercalcemia associated with cancer; nonsuppurative thyroiditis; primary or secondary adrenocortical insufficiency; preoperatively and in the event of serious trauma or illness, in patients with known adrenal insufficiency or when adrenocortical reserve is doubtful; shock unresponsive to conventional therapy if adrenocortical insufficiency exists or is suspected. Neoplastic diseases: Palliative management of leukemias and lymphomas (adults); acute leukemia of childhood. Nervous system: Acute exacerbations of multiple sclerosis; cerebral edema associated with primary or metastatic brain tumor, or craniotomy. May potentiate the antitussive effects of hydrocodone; sedative effects are also seen. Pregnancy Considerations Prolonged use of opioids during pregnancy can cause neonatal withdrawal syndrome, which may be life-threatening if not recognized and treated according to protocols developed by neonatology experts. Respiratory diseases: Aspiration pneumonitis; bronchial asthma; berylliosis; fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antituberculous chemotherapy; idiopathic eosinophilic pneumonias; Loeffler syndrome (not manageable by other means); symptomatic sarcoidosis. Rheumatic disorders: As adjunctive therapy for shortterm administration in acute and subacute bursitis, acute gouty arthritis, acute nonspecific tenosynovitis, ankylosing spondylitis, epicondylitis, posttraumatic osteoarthritis, psoriatic arthritis, rheumatoid arthritis, including juvenile rheumatoid arthritis, synovitis of osteoarthritis; during an exacerbation or as maintenance therapy in acute rheumatic carditis, dermatomyositis (polymyositis), temporal arteritis, and systemic lupus erythematosus. Adrenal insufficiency, acute (adrenal crisis): Note: Appropriate fluid resuscitation is also required (Endocrine Society [Bornstein 2016]; Gardner 2011). After the initial 24 hours, may gradually taper the dose; once patient is stable, may resume oral maintenance dosing (Allolio 2015; Endocrine Society [Bornstein 2016]; Endocrine Society [Speiser 2018]; Gardner 2011). Adrenal insufficiency, chronic (eg, primary, secondary, classic congenital adrenal hyperplasia): Oral: 15 to 25 mg/day in 2 to 3 divided doses. Administer the largest dose in the morning upon awakening, followed by next dose 2 hours after lunch (2-dose regimen) or next dose at lunch, followed by smallest dose in the afternoon no later than 4 to 6 hours before bedtime (3-dose regimen) (Endocrine Society [Bornstein 2016]; Endocrine Society [Fleseriu 2016]; Endocrine Society [Speiser 2018]). Stress dosing in patients known to be adrenallysuppressed (ie, prevention of adrenal crisis in glucocorticoid-treated patients) (off-label dose): Sickness: Illness with fever: Oral: Double the routine oral hydrocortisone dose until recovery for fever >38°C [100. May consider a slow taper over several days when vasopressors are no longer required to avoid possible hemodynamic deterioration which may occur with abrupt withdrawal (Keh 2003; Rhodes 2017). Note: Low-dose hydrocortisone in septic shock patients may cause a significant increase in hyperglycemia and hypernatremia. A small study demonstrated that repetitive bolus doses of hydrocortisone caused significant hyperglycemia that was not seen during continuous infusion (Weber-Carstens 2007); practice guidelines recommend strategies for avoidance and/or detection of 680 these side effects, such as dosing by continuous infusion (Rhodes 2017). In life-threatening situations, parenteral doses larger than the oral dose may be needed. Tablets may result in more reliable serum concentrations than oral liquid formulation; use of oral suspension is not recommended. Typically, supplementation for emotional or minimal physiological stress conditions or prior to exercise is not necessary (Elder 2010; Endocrine Society [Speiser 2010]; Shulman 2007). Dosing is generally 2 to 3 times physiologic replacement level (Elder 2010; Shulman 2007). Pheochromocytoma crisis has been reported with corticosteroids (may be fatal); consider the risk in patients with suspected pheochromocytoma. Patients receiving >20 mg per day of prednisone (or equivalent) may be most susceptible. Corticosteroid use may cause psychiatric disturbances, including euphoria, insomnia, mood swings, personality changes, severe depression, or psychotic manifestations. Prolonged use of corticosteroids may increase the incidence of secondary infection, mask acute infection (including fungal infections), prolong or exacerbate viral infections, or limit response to killed or inactivated vaccines. Latent or active amebiasis should be ruled out in any patient with recent travel to tropical climates or unexplained diarrhea prior to corticosteroid initiation. Potentially significant drug-drug interactions may exist, requiring dose or frequency adjustment, additional monitoring, and/or selection of alternative therapy. Warnings: Additional Pediatric Considerations May cause osteoporosis (at any age) or inhibition of bone growth in pediatric patients. Hypoadrenalism may occur in newborns following maternal use of corticosteroids in pregnancy; monitor. When treating women with adrenal insufficiency (primary or central or congenital adrenal hyperplasia) during pregnancy, hydrocortisone is the preferred corticosteroid. Doses may need to be adjusted as pregnancy progresses, and stress doses may be required during active labor. The manufacturer notes that when used systemically, maternal use of corticosteroids have the potential to cause adverse events in a breastfed infant (eg, growth suppression, interfere with endogenous corticosteroid production). Dermatoses: Relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses (eg, eczema; psoriasis; poison ivy, oak, or sumac; insect bites; minor skin irritation; atopic dermatitis [mild to moderate]; seborrheic dermatitis). Ulcerative colitis (adjunctive therapy): Adjunctive treatment of ulcerative colitis, especially distal forms including ulcerative proctitis, ulcerative proctosigmoiditis, left-sided ulcerative colitis, and in some cases involving the transverse and ascending colons. Adverse events similar to those observed with systemic absorption are also observed, especially following rectal use. Dosing Adult & Geriatric Anal and genital itching, external: Topical: Hydrocortisone acetate (1% cream): Apply to affected area 2 to 4 times daily. Hydrocortisone base (cream, 1% gel, 1% lotion, 1% ointment): Apply to affected area 2 to 4 times daily. Atopic dermatitis: Topical: Hydrocortisone butyrate (lotion): Apply thin film to affected area twice daily. Corticosteroid-responsive dermatosis: Topical: Hydrocortisone acetate (cream, lotion): Apply thin film to affected area 2 to 4 times daily. Hydrocortisone base (cream, gel, lotion, ointment, solution): Apply thin film to affected area 2 to 4 times daily. Hydrocortisone butyrate (cream, lipid cream, ointment, solution): Apply thin film to affected area 2 to 3 times daily. Hydrocortisone probutate (cream): Apply thin film to affected area 1 to 2 times daily. Hydrocortisone valerate (cream, ointment): Apply thin film to affected area 2 to 3 times daily. For severe cases of proctitis, 1 suppository 3 times daily or 2 suppositories twice daily may be needed. Ulcerative colitis: Rectal: Foam: One applicatorful (90 mg) 1 to 2 times daily for 2 to 3 weeks, and then every other day thereafter; use lowest dose to maintain clinical response; taper dose to discontinue long-term therapy Suspension: One enema (100 mg) every night for 21 days or until remission (clinical improvement may precede improvement of mucosal integrity); 2 to 3 months of therapy may be required; to discontinue long-term therapy, gradually reduce administration to every other night for 2 or 3 weeks. Contraindications Hypersensitivity to hydrocortisone or any component of the formulation; systemic fungal infections and ileocolostomy during the immediate or early postoperative period (rectal suspension); obstruction, abscess, perforation, peritonitis, fresh intestinal anastomoses, extensive fistulas, and sinus tracts (rectal foam). Children may absorb proportionally larger amounts after topical application and may be more prone to systemic effects. May require higher doses when subject to stress (ie, trauma, surgery, severe infection). Prolonged use of corticosteroids may increase the incidence of secondary infection, mask acute infection (including fungal infections), prolong or exacerbate viral 684 Pediatric Atopic dermatitis: Infants 3 months, Children, and Adolescents: Hydrocortisone butyrate (Locoid Lipocream, Locoid lotion): Topical: Apply a thin film to affected area twice daily; if no improvement within 2 weeks, reassess diagnosis. Close observation is required in patients with latent tuberculosis and/or tuberculosis reactivity; restrict use in active tuberculosis (only fulminating or disseminated tuberculosis in conjunction with antituberculosis treatment). Amebiasis should be ruled out in any patient with recent travel to tropical climates or unexplained diarrhea prior to initiation of corticosteroids. Prolonged treatment with corticosteroids has been also associated with the development of Kaposi sarcoma (case reports); if noted, discontinuation of therapy should be considered. Acute myopathy has been reported with high-dose corticosteroids, usually in patients with neuromuscular transmission disorders; may involve ocular and/or respiratory muscles; monitor creatine kinase; recovery may be delayed. Corticosteroid use may cause psychiatric disturbances, including depression, euphoria, insomnia, mood swings, and personality changes. Allergic contact dermatitis can occur and is usually diagnosed by failure to heal rather than clinical exacerbation; discontinue use if irritation occurs and treat appropriately. In patients with severe ulcerative colitis, it may be hazardous to delay surgery while waiting for response to treatment. Use with caution following acute myocardial infarction; corticosteroids have been associated with myocardial rupture. Use with caution in patients with cataracts and/or glaucoma; increased intraocular pressure, glaucoma, and cataracts have occurred with prolonged use. Absorption is increased by the use of occlusive dressings, application to denuded skin, prolonged use, or application to large surface areas. Avoid use of topical preparations with occlusive dressings or on weeping or exudative lesions. Because of the risk of adverse effects associated with systemic absorption, topical corticosteroids should be used cautiously in elderly patients in the smallest possible effective dose for the shortest duration. Rectal enema: Damage to the rectal wall may occur from improper or careless insertion of the enema tip. Use with caution when there is a probability of impending perforation, abscess, or other pyogenic infection; obstruction; or extensive fistulas and sinus tracts. Rectal foam: Do not insert any part of the aerosol container directly into the anus. Contents are under pressure; do not burn or puncture the container; do not store at temperatures above 48. If there is not evidence of clinical or proctologic improvement within 2 or 3 weeks after initiation of therapy, or if the condition worsens, discontinue use. Contraindicated in obstruction, abscess, perforation, peritonitis, fresh intestinal anastomoses, extensive fistulas, and sinus tracts. Warnings: Additional Pediatric Considerations the extent of percutaneous absorption is dependent on several factors, including epidermal integrity (intact vs abraded skin), formulation, age of the patient, prolonged duration of use, and the use of occlusive dressings. Percutaneous absorption of topical steroids is increased in neonates (especially preterm neonates), infants, and young children. Systemic bioavailability of topical corticosteroids is variable (integrity of skin, use of occlusion, etc. When a topical steroid is needed, low to moderate potency corticosteroids are preferred initially. High potency topical steroids should be used only when clearly needed and after the first trimester (Bae 2012). Breastfeeding Considerations It is not known if systemic absorption following topical administration of hydrocortisone results in detectable quantities in human milk. Extended release: Management of pain in opioid-tolerant patients severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate. Limitations of use: Reserve for use in patients for whom alternative treatment options (eg, nonopioid analgesics, opioid combination products) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain. Moderate to severe pain: Suppository: Relief of moderate to severe pain such as that caused by biliary colic, burns, cancer, myocardial infarction, renal colic, surgery, and trauma (soft tissue and bone). Mothers who are physically dependent on opioids may give birth to Infants who are also physically dependent. Cyanocobalamin acts as a coenzyme for various metabolic functions, including fat and carbohydrate metabolism and protein synthesis, used in cell replication and hematopoiesis.
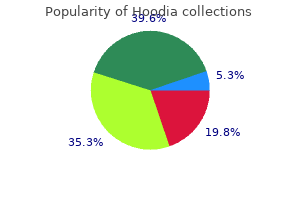
It seems prudent to avoid regular himalaya herbals acne-n-pimple cream purchase hoodia mastercard, frequent use of ibuprofen in patients receiving aspirin for its cardioprotective effects herbals for hair growth purchase hoodia 400 mg on-line. Alternative analgesics (eg herbals companies discount hoodia 400 mg without prescription, acetaminophen) or prescription diclofenac in place of prescription ibuprofen may be a safer choice jeevan herbals cheap hoodia 400 mg visa. Dental Health Professional Considerations See Local Anesthetic/Vasoconstrictor Precautions Use Atrial fibrillation/flutter: Rapid conversion of atrial fibrillation or atrial flutter of recent onset to sinus rhythm (effectiveness has not been determined in patients with arrhythmias >90 days in duration) herbals 2 buy hoodia 400 mg. The presence of bradykinin may cause symptoms of localized swelling, inflammation, and pain. Icatibant inhibits bradykinin from binding at the B2 receptor, thereby treating the symptoms associated with acute attack. Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding Chemotherapy may result in significant myelosuppression, potentially including significant reduction in platelet counts and altered hemostasis. Pharmacodynamics/Kinetics Onset of Action Uncontrolled bleeding: Effects observed within minutes and hemostasis is restored at a median of 11. Verify pregnancy status in females of reproductive potential prior to initiating treatment with idelalisib. Females of reproductive potential should use effective contraception during therapy and for at least 1 month after the final idelalisib dose. The addition of serotonin antagonism to dopamine antagonism (classic neuroleptic mechanism) is thought to improve negative symptoms of psychoses and reduce the incidence of extrapyramidal side effects (Huttunen 1995). Until more information is obtained, it is suggested that the clinician consult with the physician prior to the use of a vasoconstrictor in suspected patients, and that the vasoconstrictor (epinephrine, mepivacaine and levonordefrin [Carbocaine 2% with Neo-Cobefrin]) be used with caution. Effects on Dental Treatment Key adverse event(s) related to dental treatment: Xerostomia and changes in salivation (normal salivary flow resumes upon discontinuation); Patients may experience orthostatic hypotension as they stand up after treatment; especially if lying in dental chair for extended periods of time. Effects on Bleeding No information available to require special precautions Adverse Reactions >10%: Cardiovascular: Tachycardia (3% to 12%; doserelated) Central nervous system: Dizziness (10% to 20%; dose-related), drowsiness (9% to 15%) Endocrine & metabolic: Increased serum prolactin (26%), weight gain (9% to 18%; dose-related) 1% to 10%: Cardiovascular: Orthostatic hypotension (3% to 5%), hypotension (3%; dose-related), palpitations (1%) Central nervous system: Fatigue (4% to 6%), extrapyramidal reaction (4% to 5%), lethargy (3%), aggressive behavior (1%), delusions (1%), restlessness (1%), dystonia (1%) Dermatologic: Skin rash (3%) Endocrine & metabolic: Increased serum triglycerides (10%), increased serum cholesterol (4%), weight loss (1%) Gastrointestinal: Nausea (10%), xerostomia (8% to 10%), diarrhea (5% to 7%), abdominal distress (3%; dose-related) Genitourinary: Ejaculation failure (2%), erectile dysfunction (1%), urinary incontinence (1%) Hematologic & oncologic: Decreased hematocrit (1%) 704 Pharmacodynamics/Kinetics Half-life Elimination Extensive metabolizers: Iloperidone: 18 hours; P88: 26 hours; P95: 23 hours Poor metabolizers: Iloperidone: 33 hours; P88: 37 hours; P95: 31 hours Time to Peak Plasma: 2 to 4 hours Pregnancy Considerations Adverse events have been observed in animal reproduction studies. Iloperidone may cause hyperprolactinemia, which may decrease reproductive function in both males and females. Cytopenias including thrombocytopenia (grade 4 severe: <33%) and anemia (25% to 80%; grade 4: <11%) have been reported. Pharmacodynamics/Kinetics Half-life Elimination Adults: Parent drug: ~18 hours; N-desmethyl metabolite: ~40 hours; Children: Parent drug: ~15 hours Time to Peak 2 to 4 hours Pregnancy Considerations Imatinib crosses the placenta (Burwick 2017). Pregnancy testing should be conducted in females of reproductive potential prior to therapy; women of reproductive potential should use highly effective contraception during imatinib treatment and for 2 weeks after the last imatinib dose. Lower respiratory tract infections: Treatment of lower respiratory tract infections caused by S. Skin and skin structure infections: Treatment of skin and skin structure infections caused by E. Urinary tract infections (complicated and uncomplicated): Treatment of uncomplicated and complicated urinary tract infections caused by E. Cilastatin prevents renal metabolism of imipenem by competitive inhibition of dehydropeptidase along the brush border of the renal tubules. Imipenem is not one of the preferred antibiotics for the management of cystic fibrosis in pregnant females; however, it may be used when a safer alternative is not available (Panchaud 2016). Current research is investigating the use of the salivary stimulant pilocarpine to overcome the xerostomia from imipramine. Effects on Bleeding No information available to require special precautions Adverse Reactions Reported for tricyclic antidepressants in general. Half-life Elimination 8 to 21 hours (Salle 1990); Mean: Children: 11 hours; Adults: 16 to 17 hours; Desipramine (active metabolite): 22 to 28 hours Time to Peak Serum: 2 to 6 hours (Sallee 1990) Pregnancy Considerations Animal reproduction studies are inconclusive. Congenital abnormalities have been reported in humans; however, a causal relationship has not been established. Due to pregnancy-induced physiologic changes, women who are pregnant may require dose adjustments late in pregnancy to achieve euthymia (Altshuler 1996). Topical application to the skin is associated with increases in markers for cytokines and immune cells. Superficial basal cell carcinoma (Aldara 5% cream): Topical treatment of biopsy-confirmed, primary superficial basal cell carcinoma in immunocompetent adults with a maximum tumor diameter of 2 cm located on the trunk (excluding anogenital skin), neck, or extremities (excluding hands and feet), only when surgical methods are medically less appropriate and patient follow-up can be reasonably assured. Imiquimod should be used with caution in patients with preexisting autoimmune conditions. Imiquimod has been evaluated in pediatrics ages 2 to 12 with molluscum, contagiosum, however, studies failed to demonstrate efficacy. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding No information available to require special precautions Adverse Reactions Note: Frequency of reactions vary and are related to the degree of inflammation associated with the treated disease, number of weekly applications, product formulation, and individual sensitivity. Dental Health Professional Considerations Imiquimod cream 5% has been used for actinic cheilitis or keratosis. Imiquimod use in the treatment of oral papilloma virus remains inadequately studied. Although prophylaxis may be given to any nonimmune person, priority should be given to those at greatest risk for measles complications and also to persons exposed in settings with intense, prolonged, close contact (eg, households, daycare centers, classrooms). Some clinical trials were extremely small and skewed the incidence upward ( indicates this trend). HyQvia: Data collection to monitor pregnancy and infant outcomes following exposure to HyQvia is ongoing. Patients may enroll themselves in the HyQvia pregnancy registry by calling (866) 424-6724. Respiratory: Nasopharyngitis (upper limb spasticity: 2%), upper respiratory tract infection (upper limb spasticity: 2%) Blepharospasm and glabellar lines: >10%: Gastrointestinal: Xerostomia (blepharospasm: 16%) Ophthalmic: Blepharoptosis (blepharospasm: 19%; reduction of glabellar lines: <1%), dry eye syndrome (blepharospasm: 16%), visual disturbance (blepharospasm: 12%) 1% to 10%: Central nervous system: Headache (blepharospasm: 7%; reduction of glabellar lines: 5%) Gastrointestinal: Diarrhea (blepharospasm: 8%) Respiratory: Dyspnea (blepharospasm: 5%), nasopharyngitis (blepharospasm: 5%), respiratory tract infection (blepharospasm: 5%) <1%, postmarketing and/or case reports: Any indication: Abdominal distention, abnormal dreams, allergic dermatitis, alopecia, anaphylaxis, antibody development, asthma, blepharospasm, blurred vision, cardiac insufficiency, circulatory shock, corneal perforation, cough, diplopia, dysarthria, edema, erythema, eye disease, eyelid edema, facial pain, facial paresis, fatigue, fixed drug eruption, flu-like symptoms, hematoma at injection site, herpes zoster, hypersensitivity reaction, inflammation at injection site, injection site reaction, lymphadenopathy, madarosis, muscle spasm, myalgia, nausea, pruritus, reduced blinking (leading to corneal ulceration), serum sickness, skin rash, swelling of eye, trismus, urinary incontinence, urticaria, vascular insufficiency, voice disorder, weakness Mechanism of Action IncobotulinumtoxinA is a neurotoxin produced from Clostridium botulinum that inhibits acetylcholine release from peripheral cholinergic nerve endings. Inhibition of acetylcholine release at the neuromuscular junction produces a state of denervation. Cervical dystonia: Treatment of adults with cervical dystonia in both botulinum toxin-naïve and previously treated patients. Glabellar lines: Temporary improvement in the appearance of moderate to severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients. Canadian labeling: Xeomin: Cervical dystonia: Treatment of cervical dystonia (spasmodic torticollis) in adults. Hypertonicity disorders: Treatment of hypertonicity disorders of the seventh nerve (eg, blepharospasm, hemifacial spasm) in adults. Upper limb spasticity: Treatment of poststroke spasticity of upper limb(s) in adults. Xeomin Cosmetic: Glabellar lines: Temporary improvement in the appearance of moderate to severe glabellar lines in adults. Effects on Bleeding No information available to require special precautions Pharmacodynamics/Kinetics Onset of Action Improvement: ~4 to 7 days Duration of Action ~3 to 4 months Pregnancy Risk Factor C Pregnancy Considerations Adverse events were observed in some animal reproduction studies. Canadian labeling does not recommend use for temporary improvement in appearance of moderate to severe glabellar lines during pregnancy. Pharmacodynamics/Kinetics Onset of Action 5 minutes; Peak effect: 1-4 hours Duration of Action 24 hours Half-life Elimination 40-56 hours Time to Peak Serum: ~15 minutes Pregnancy Risk Factor C Pregnancy Considerations Adverse events were not observed in animal reproduction studies. Beta-agonists may interfere with uterine contractility if administered during labor. No increased risk of overall birth defects has been observed according to data collected by the antiretroviral pregnancy registry. Hyperbilirubinemia may occur in neonates following in utero exposure to indinavir. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment No significant effects or complications reported Effects on Bleeding Has been associated with thrombocytopenia, anemia, and hemolytic anemia, but incidence may vary with indication. Adverse Reactions As reported in adults with rheumatoid arthritis, unless otherwise noted. Infliximab crosses the placenta and can be detected in the serum of infants for up to 6 months following in utero exposure. If a biologic agent such as infliximab is needed to treat inflammatory bowel disease during pregnancy, it is recommended to hold therapy after 30 weeks gestation (Habal 2012). Health care providers are also encouraged to enroll women exposed to infliximab during pregnancy in the MotherToBaby Autoimmune Diseases Study by 715 Mechanism of Action the GlaxoSmithKline product is an adjuvanted monovalent split virus (inactivated) preparation of the type A, subtype H5N1 avian strain of influenza virus (A/ Indonesia/05/2005) the Sanofi Pasteur product is a monovalent, split virus (inactivated) preparation of the type A, subtype H5N1 avian strain of influenza virus (A/Vietnam/1203/2004) Both promote active immunity to influenza A H5N1 (avian). Pregnancy Risk Factor C (Sanofi Pasteur product) Pregnancy Considerations Adverse events were not observed in animal reproduction studies using the H5N1 vaccine GlaxoSmithKline adjuvanted product; animal reproduction studies have not been conducted with the Sanofi Pasteur product. Adverse reactions in adults 65 years of age may be greater using the high-dose vaccine, but are typically mild and transient. Women exposed to FluLaval Quadrivalent or Fluarix Quadrivalent vaccine during pregnancy or their health care provider may contact the GlaxoSmithKline registry at 888-452-9622. Women exposed to Afluria Quadrivalent or Flucelvax Quadrivalent vaccine during pregnancy may contact the Seqirus registry at 855-358-8966 or via email at us. Health care providers may enroll women exposed to Fluzone Quadrivalent during pregnancy in the Sanofi Pasteur vaccination registry at 800-822-2463. Canadian labeling: Active immunization of individuals 2 to 59 years of age against influenza disease caused by influenza virus subtypes A and type B contained in the vaccine. Promotes immunity to seasonal influenza virus by inducing specific antibody production. This vaccine is not systemically absorbed following maternal nasal administration and is not expected to result in exposure to the fetus. Pregnant and postpartum women are also at an increased risk of complications from influenza infection. Women exposed to this vaccine during pregnancy may contact the Flublok pregnancy registry at 800-822-2463. Effects on Bleeding Exposure to antisense oligonucleotides may result in significant myelosuppression including reduction in platelet counts (thrombocytopenia) and altered hemostasis. Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: In general, morning appointments are advisable in patients with diabetes since endogenous cortisol levels are typically higher at this time; because cortisol increases blood sugar levels, the risk of hypoglycemia is less. Although patients with diabetes usually recognize signs and symptoms of hypoglycemia and self-intervene before changes in or loss of consciousness occurs, they may not. Inotersen decreases serum vitamin A levels; appropriate concentrations of vitamin A are required for fetal development. Females of reproductive potential and males with female partners of reproductive potential were required to use effective contraception during clinical trials of inotersen (Benson 2018). Within adipose tissue, insulin stimulates the processing of circulating lipoproteins to provide free fatty acids, facilitating triglyceride synthesis and storage by adipocytes; it also directly inhibits the hydrolysis of triglycerides. Effects on Bleeding No information available to require special precautions Pharmacodynamics/Kinetics Onset of Action ~0. Insulin aspart may be 721 Adverse Reactions >10%: Endocrine & metabolic: Hypoglycemia (47% to 75%), severe hypoglycemia (4% to 16%) Frequency not defined: Cardiovascular: Peripheral edema Endocrine & metabolic: Hypokalemia, weight gain Hypersensitivity: Anaphylaxis, hypersensitivity reaction Immunologic: Antibody development Local: Hypersensitivity at injection site (including edema, erythema, or pruritus), lipoatrophy at injection site, lipotrophy at injection site Mechanism of Action Insulin acts via specific membrane-bound receptors on target tissues to regulate metabolism of carbohydrate, protein, and fats. Insulin aspart differs from human insulin by containing aspartic acid at position B28 in comparison to the proline found in human insulin. Use Diabetes mellitus: To improve glycemic control in patients 1 year of age and older with type 1 or type 2 diabetes mellitus Local Anesthetic/Vasoconstrictor Precautions No information available to require special precautions Effects on Dental Treatment Key adverse event(s) related to dental treatment: In general, morning appointments are advisable in patients with diabetes since endogenous cortisol levels are typically higher at this time; because cortisol increases blood sugar levels, the risk of hypoglycemia is less. It is important to confirm that the patient has eaten normally prior to the appointment and has taken all scheduled medications. Effects on Bleeding No information available to require special precautions Pharmacodynamics/Kinetics Onset of Action 10 to 20 minutes; Peak effect: 1 to 4 hours Duration of Action Novolog Mix 50/50: ~13 hours; Novolog Mix 70/30: 18 to 24 hours Half-life Elimination Novolog Mix 50/50: 5. Most available information for use of insulin aspart in pregnancy is from studies using the rapid action solution. Adverse Reactions 10%: Central nervous system: Headache (9% to 12%) Endocrine & metabolic: Severe hypoglycemia (type 1 diabetics on combination insulin therapy: 10% to 18%; type 2 diabetics on combination therapy: 5%) Immunologic: Antibody development Respiratory: Nasopharyngitis (13% to 24%), upper respiratory tract infection (8% to 12%) 1% to 10%: Cardiovascular: Peripheral edema (type 2 diabetes: 3%; type 1 diabetes: <1%) Gastrointestinal: Diarrhea (type 2 diabetes: 6%), gastroenteritis (type 1 diabetes: 5%) Local: Injection site reaction (4%; including discoloration, erythema, hematoma, hemorrhage, mass, nodules, pain, pruritus) Respiratory: Sinusitis (type 1 diabetes: 5%) Frequency not defined: Endocrine & metabolic: Hypokalemia, weight gain <1%, postmarketing and/or case reports: Hypersensitivity reaction, hypertrophy at injection site (lipohypertrophy), lipoatrophy at injection site, urticaria Mechanism of Action Insulin acts via specific membrane-bound receptors on target tissues to regulate metabolism of carbohydrate, protein, and fats. Insulin degludec differs from human insulin by the omission of the amino acid threonine in position B-30 of the B-chain, and the subsequent addition of a side chain composed of glutamic acid and a C16 fatty acid. Staff should be trained to recognize the signs (eg, unusual behavior or profuse sweating in patients who have diabetes) and treat patients who have hypoglycemia; a glucometer should be used to test patient blood glucose levels. Effects on Bleeding No information available to require special precautions Adverse Reactions >10%: Endocrine & metabolic: Hypoglycemia (type 1 diabetes patients using combination insulin regimen: 93% to 95%; type 2 diabetes patients on a combination regimen: 50% to 74%), severe hypoglycemia (type 1 diabetes patients using combination insulin regimen: 6% to 13%; type 2 diabetes patients on a combination regimen: 3%) Immunologic: Antibody development Respiratory: Nasopharyngitis (type 1 diabetes: 25%; type 2 diabetes: 11%) 1% to 10%: Cardiovascular: Peripheral edema (2%) Central nervous system: Headache (6% to 10%) Infection: Influenza (type 1 diabetes: 7%) Local: Injection site reaction (2%; including erythema at injection site, hematoma at injection site, hemorrhage, injection site nodule, injection site pruritus, mass, pain at injection site, skin discoloration at injection site, swelling at injection site, and warmth) Respiratory: Upper respiratory tract infection (6% to 9%) <1%, postmarketing and/or case reports: Hypersensitivity reaction, hypertrophy at injection site, lipotrophy at injection site, urticaria Pharmacodynamics/Kinetics Onset of Action ~1 hour Half-life Elimination ~25 hours (independent of dose) Time to Peak 9 hours Pregnancy Considerations Adverse events were observed in animal reproduction studies secondary to maternal hypoglycemia. Information specific to insulin degludec use in pregnant women is limited (Milluzzo 2017). Mechanism of Action Insulin acts via specific membrane-bound receptors on target tissues to regulate metabolism of carbohydrate, protein, and fats. Insulin promotes hepatic synthesis of fatty acids, which are released into the circulation as lipoproteins. Endocrine & metabolic: Hypoglycemia Local: Hypertrophy at injection site, lipoatrophy at injection site <1%, postmarketing, and/or case reports: Abdominal distension, abdominal pain, allergic skin reaction, anaphylaxis, constipation, decreased appetite, dyspepsia, eructation, flatulence, gastritis, gastroesophageal reflux disease, hypersensitivity reaction, severe hypoglycemia, urticaria, vomiting Mechanism of Action Refer to individual agents. Pharmacodynamics/Kinetics Onset of Action Insulin aspart: 14 minutes Duration of Action Insulin degludec: >24 hours Half-life Elimination Insulin degludec: ~25 hours Time to Peak Insulin aspart: 72 minutes Pregnancy Considerations Refer to individual monographs. Every dental office should have a protocol for managing hypoglycemia in conscious and unconscious patients. Insulin detemir differs from human insulin by the omission of threonine in position B30 and the addition of a C14 fatty acid chain to the amino acid located at position B29. Women who are stable on insulin detemir prior to conception may continue it during pregnancy. Having snack foods or oral glucose tablets or gels available, especially in practices where a large number of surgical procedures are performed, is also prudent (American Diabetes Association 2017). Effects on Bleeding No information available to require special precautions 725 Pharmacodynamics/Kinetics Onset of Action 3 to 4 hours; Peak effect: 3 to 9 hours (Plank 2005) Duration of Action Dose dependent: 6 to 23 hours; Note: At lower dosages (0. Half-life Elimination 5 to 7 hours (dose-dependent) Time to Peak Plasma: 6 to 8 hours Pregnancy Risk Factor B Pregnancy Considerations Insulin detemir has been detected in cord blood. Skeletal muscle effects of insulin include increased protein synthesis and increased glycogen synthesis. Insulin glargine differs from human insulin by adding two arginines to the C-terminus of the B-chain in addition to containing glycine at position A21 in comparison to the asparagine found in human insulin. Insulins are categorized based on the onset, peak, and duration of effect (eg, rapid-, short-, intermediate-, and 726 long-acting insulin). Pharmacodynamics/Kinetics Onset of Action Basaglar: Peak effect: No pronounced peak Lantus: 3 to 4 hours; Peak effect: No pronounced peak Toujeo: 6 hours; Peak effect: Maximum glucose lowering effect may take up to 5 days with repeat dosing; at steady state, the 24-hour glucose lowering effect is ~27% lower than that of Lantus at equivalent doses. Duration of Action Lantus, Basaglar: Generally 24 hours or longer; reported range (Lantus): 10. Women who are stable on insulin glargine prior to conception may continue it during pregnancy. Theoretical concerns of insulin glargine should be discussed prior to conception (Blumer 2013).
Generic 400 mg hoodia with amex. Improve Your Fertility | 5 Herbs To Manage Stress.
References
- Takahashi S, Goto K, Fukasawa H, et al. Computed tomography of cerebral infarction along the distribution of the basal perforating arteries. Part II: Thalamic arterial group. Radiology 1985; 155:119-30.
- Larson EW, Edwards WD: Risk factors for aortic dissection: A necropsy study of 161 cases, Am J Cardiol 53:849, 1984.
- Borlak J, Reamon-Buettner SM. N-acetyltransferase 2 (NAT2) gene polymorphisms in colon and lung cancer patients. BMC Med Genet 2006;7:58.
- Casey JT, Hagerty JA, Maizels M, et al: Early administration of oxybutynin improves bladder function and clinical outcomes in newborns with posterior urethral valves, J Urol 188(4 Suppl):1516n1520, 2012.
- Meng MV, Elkin EP, Latini DM, et al: Treatment of patients with high-risk localized prostate cancer: results from cancer of the prostate strategic urological research endeavor (CaPSURE), J Urol 173(5):1557n1561, 2005.
- Boysen W, Belleville L, Ahkavan A, et al: MP55-11 multi-institutional review of outcomes and complications of robotic-assisted laparoscopic extravesical ureteral reimplantation (RALUR-EV) for treatment of primary vesicoureteral reflux (VUR) in children, J Urol 195(4):e739-e740, 2016.
- Hearse DJ, Bolli R: Reperfusion-induced injury: Manifestations, mechanisms, and clinical relevance, Cardiovasc Res 26:101, 1992.
- Roldan Urgoiti GB, Gustafson K, Klimowicz AC, et al. The prognostic value of HPV status and p16 expression in patients with carcinoma of the anal canal. PLoS One 2014;9(10):e108790.