
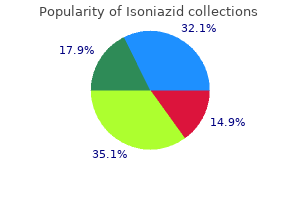
Isoniazid
| Contato
Página Inicial
Thomas M. Bashore, MD
- Professor of Medicine
- Division of Cardiovascular Medicine
- Director, Fellowship Training Program
- and Adult Congenital and Valvular Disease Program
- Duke University Medical Center
- Durham, North Carolina
Muscle weakness medicine pouch best purchase for isoniazid, pain 5ht3 medications cheapest isoniazid, rhabdomyolysis symptoms dizziness nausea order genuine isoniazid online, hyperglycemia symptoms schizophrenia cheap isoniazid 300 mg online, hyperlipidemia medicine jar paul mccartney generic isoniazid 300 mg buy line, and acute renal failure may also occur. Consequently, they develop a hyponatremic syndrome indistinguishable from inappropriate antidiuresis. Differential Diagnosis Hypodipsic hypernatremia usually can be distinguished from other causes of inadequate fluid intake. Previous episodes and/or denial of thirst and failure to drink spontaneously when the patient is conscious, unrestrained, and hypernatremic are virtually diagnostic. The hypernatremia caused by excessive retention or intake of sodium can be distinguished by the presence of thirst as well as the physical and laboratory signs of hypervolemia rather than hypovolemia. All three forms are associated with a failure to fully dilute the urine and mount a water diuresis in the face of hypotonic hyponatremia. However, the disorders with which they are associated and the types of salt and water imbalance that result differ. The hypervolemic form typically occurs in disorders like severe congestive heart failure or cirrhosis in which water is retained in excessive of sodium. The hypovolemic form typically occurs in disorders such as severe diarrhea, diuretic abuse, or mineralocorticoid deficiency in which sodium is lost in excess of water. Euvolemic hyponatremia, however, is due mainly to expansion of total body water caused by excessive intake in the face of a failure to dilute the urine in response to excessive water intake. One is a nonhemodynamic stimulus such as nausea or a cortisol deficiency, which can be corrected quickly by treatment with antiemetics or cortisol. The other is a primary defect in osmoregulation caused by another disorder such as malignancy, stroke, or pneumonia that cannot be easily or quickly corrected. This amount plus an allowance for continuing insensible and urinary losses should be given over a 24- to 48-h period. If hyperglycemia and/or hypokalemia are present, insulin and/or potassium supplements should be given with the expectation that both can be discontinued soon after rehydration is complete. Plasma urea/creatinine should be monitored closely for signs of acute renal failure caused by rhabdomyolysis, hypovolemia, and hypotension. A long-term management plan to prevent or minimize recurrence of the fluid and electrolyte imbalance also should be developed. This should include a practical method to regulate fluid intake in accordance with variations in water balance as indicated by changes in body weight or serum sodium determined by home monitoring analyzers. Prescribing a constant fluid intake is ineffective and potentially dangerous because it does not take into account the large, uncontrolled variations in insensible loss that inevitably result from changes in ambient temperature and physical activity. Clinical Characteristics Antidiuresis of any cause decreases the volume and increases the concentration of urine. If not accompanied by a commensurate reduction in fluid intake or an increase in insensible loss, the reduction in urine output results in excess water retention which expands and dilutes body fluids. If the hyponatremia develops gradually or has been present for more than a few days, it may be largely asymptomatic. However, if it develops acutely, it is usually accompanied by symptoms and signs of water intoxication that may include mild headache, confusion, anorexia, nausea, vomiting, coma, and convulsions. Other clinical signs and symptoms vary greatly, depending on the type of hyponatremia. The hypervolemic form is characterized by generalized edema and other signs of marked volume expansion. The eutopic forms occur most often in patients with acute infections or strokes but have also been associated with many other neurologic diseases and injuries. In some of them, all young boys, the inappropriate antidiuresis has been traced to a constitutively activating mutation of the V2 receptor gene. The inappropriate antidiuresis in these patients appears to be permanent, although the hyponatremia is variable owing presumably to individual differences in fluid intake. Thus, the rate of urinary sodium excretion is low (unless sodium reabsorption is impaired by a diuretic), and the hyponatremia is usually accompanied by edema, hypokalemia, azotemia, and hyperuricemia. If hyperglycemia is present, its contribution to the reduction in plasma sodium can be estimated either by measuring plasma osmolarity for a more accurate estimate of the true "effective" tonicity of body fluids or by correcting the measured plasma sodium for the reduction caused by the hyperglycemia using the simplified formula corrected Pna = measured Pna + (Pglu 90)/36 where Pna = plasma sodium in meq/L and Pglu = plasma glucose in mg/dL. If the plasma osmolarity and/or corrected plasma sodium are below normal limits, hypotonic hyponatremia is present and further evaluation to determine the type should be undertaken in order to administer safe and effective treatment. This differentiation is usually possible by evaluating standard clinical indicators of the extracellular fluid volume (Table 374-3). If these findings are ambiguous or contradictory, measuring plasma renin activity or the rate of urinary sodium excretion may be helpful provided that the hyponatremia is not in the recovery phase or is due to a primary defect in renal conservation of sodium, diuretic abuse, or hyporeninemic hypoaldosteronism. Thus, an increase in body water of 10% (~4 L in a 70-kg adult) reduces plasma osmolarity and sodium by ~10% (~28 mosmol/L or 14 meq/L). An increase in body water of this magnitude is rarely detectable on physical examination but will be reflected in a weight gain of about 4 kg. It also increases glomerular filtration and atrial natriuretic hormone and suppresses plasma renin activity, thereby increasing urinary sodium excretion. The resultant reduction in total body sodium decreases the expansion of extracellular volume but aggravates the hyponatremia and further expands intracellular volume. The latter increases brain swelling and intracranial pressure, which probably produces most of the symptoms of acute water intoxication. Within a few days, this swelling may be counteracted by inactivation or elimination of intracellular solutes, resulting in the remission of symptoms even though the hyponatremia persists. The resultant antidiuresis is enhanced by decreased distal delivery of glomerular filtrate that results from increased reabsorption of sodium in proximal nephron. If the reduction in urine output is not associated with a commensurate reduction in water intake or an increase in insensible loss, body fluids are expanded and diluted, resulting in hyponatremia despite an increase in body sodium. This treatment often produces a solute diuresis that serves to remove some of the excess water. Another vaptan (Tolvaptan) can be given orally starting at a dose of 15 mg po and increasing to 30 mg or 60 mg at 24 h intervals depending on the effect. With either approach, fluid intake should be restricted to less than urine output. In a hyponatremic adult, an excretion rate >25 meq/d (or 25 eq/mg of creatinine) could be considered high. Regulating fluid intake so that it under replaces urine output by 5mL/kg body weight/h will raise serum sodium at a rate of about 1% an hour. In any event, serum sodium should be checked every 24 h to ensure it is not raised faster than 1mEq/L per hour or above the lower limit of normal. The periods of vaptan (V) therapy are indicated by the green shaded boxes at the top. Note that sodium increased progressively when vaptan increased urine output to levels that clearly exceeded fluid intake. This can be achieved by restricting total fluid intake to less than the sum of urinary and insensible losses. Because the water derived from food (300700 mL/d) usually approximates basal insensible losses in adults, the aim should be to reduce total discretionary intake (all liquids) to ~500 mL less than urinary output. Adherence to this regimen is often problematic and, even if achieved, usually reduces body water and increases serum sodium by only about 12% per day. Therefore, it is often necessary to add a treatment that increases urinary water excretion. Some restriction of fluid intake may also be necessary to achieve satisfactory control of the hyponatremia. Its mechanism of action is unclear but probably involves increased retention of sodium. It also increases urinary potassium excretion, which may require replacement through dietary adjustments or supplements and may induce hypertension, occasionally necessitating discontinuation of the treatment. As with other treatments, care must be taken to ensure that serum sodium does not rise too quickly or too far. In that condition, use of an osmotic diuretic such as urea is reported to be effective in preventing or correcting hyponatremia. However, some vaptans may be effective in patients with a different type of activating mutation so the response to this therapy may be neither predictable nor diagnostic. In hypervolemic hyponatremia, fluid restriction is also appropriate and somewhat effective if it can be maintained. The infusion of hypertonic saline is contraindicated because it further increases total body sodium and edema and may precipitate cardiovascular decompensation. Tolvaptan is approved by the Food and Drug Administration for this indication with the caveat that treatment should be initiated or reinitiated in hospital. Its use should also be limited to 30 days at a time because of reports that longer periods may be associated with abnormal liver chemistries. As with the treatment of other forms of hyponatremia, care must be taken to ensure that plasma sodium does not increase too rapidly or too far. Hyponatremia, for example, appears to be more common and is more likely to be due to infectious diseases such as cholera, shigellosis, and other diarrheal disorders. Acting through thyroid hormone receptors and, these hormones play a critical role in cell differentiation and organogenesis during development and help maintain thermogenic and metabolic homeostasis in the adult. Autoimmune disorders of the thyroid gland can stimulate overproduction of thyroid hormones (thyrotoxicosis) or cause glandular destruction and hormone deficiency (hypothyroidism). Benign nodules and various forms of thyroid cancer are relatively common and amenable to detection by physical examination or various imaging techniques. The thyroid (Greek thyreos, shield, plus eidos, form) consists of two lobes connected by an isthmus. It is located anterior to the trachea between the cricoid cartilage and the suprasternal notch. The recurrent laryngeal nerves traverse the lateral borders of the thyroid gland and must be identified during thyroid surgery to avoid injury and vocal cord paralysis. The thyroid gland develops from the floor of the primitive pharynx during the third week of gestation. The developing gland migrates along the thyroglossal duct to reach its final location in the neck. This feature accounts for the rare ectopic location of thyroid tissue at the base of the tongue (lingual thyroid) as well as the occurrence of thyroglossal duct cysts along this developmental tract. Neural crest derivatives from the ultimobranchial body give rise to thyroid medullary C cells that produce calcitonin, a calcium-lowering hormone. The C cells are interspersed throughout the thyroid gland, although their density is greatest in the juncture of the upper one-third and lower two-thirds of the gland. Calcitonin plays a minimal role in calcium homeostasis in humans but the C-cells are important because of their involvement in medullary thyroid cancer. Thyroid gland development is orchestrated by the coordinated expression of several developmental transcription factors. Mutations in these developmental transcription factors or their downstream target genes are rare causes of thyroid agenesis or dyshormonogenesis, although the causes of most forms of congenital hypothyroidism remain unknown (see Chap. Because congenital hypothyroidism occurs in ~1 in 4000 newborns, neonatal screening is now performed in most industrialized countries. Transplacental passage of maternal thyroid hormone occurs before the fetal thyroid gland begins to function and provides significant hormone support to a fetus with congenital hypothyroidism. Early thyroid hormone replacement in newborns with congenital hypothyroidism prevents potentially severe developmental abnormalities. The thyroid follicular cells are polarized-the basolateral surface is apposed to the bloodstream and an apical surface faces the follicular lumen. This binding leads to Tg reabsorption from the follicular lumen and proteolysis within the cytoplasm, yielding thyroid hormones for secretion into the bloodstream. Deiodination leads to production of the potent hormone triiodothyronine (T3) or the inactive hormone reverse T3. After secretion into the thyroid follicle, Tg is iodinated on tyrosine residues that are subsequently coupled via an ether linkage. Reuptake of Tg into the thyroid follicular cell allows proteolysis and the release of newly synthesized T4 and T3. Thyroid follicles are formed by thyroid epithelial cells surrounding proteinaceous colloid, which contains thyroglobulin. Follicular cells, which are polarized, synthesize thyroglobulin and carry out thyroid hormone biosynthesis (see text for details). The thyroid gland extracts iodine from the circulation in a highly efficient manner. The iodide transport mechanism is highly regulated, allowing adaptation to variations in dietary supply. Another iodine transporter, pendrin, is located on the apical surface of thyroid cells and mediates iodine efflux into the lumen. Mutation of the pendrin gene causes Pendred syndrome, a disorder characterized by defective organification of iodine, goiter, and sensorineural deafness. Europe remains mildly iodine-deficient, and health surveys indicate that iodine intake has been falling in the United States and Australia. In areas of relative iodine deficiency, there is an increased prevalence of goiter and, when deficiency is severe, hypothyroidism and cretinism. Cretinism is characterized by mental and growth retardation and occurs when children who live in iodine-deficient regions are not treated with iodine or thyroid hormone to restore normal thyroid hormone levels during early life. These children are often born to mothers with iodine deficiency, and it is likely that maternal thyroid hormone deficiency worsens the condition. Concomitant selenium deficiency may also contribute to the neurologic manifestations of cretinism. Iodine supplementation of salt, bread, and other food substances has markedly reduced the prevalence of cretinism. Unfortunately, however, iodine deficiency remains the most common cause of preventable mental deficiency, often because of societal resistance to food additives or the cost of supplementation.
The patients should wash their hands after gel application and keep the area of gel application covered with clothing to minimize the risk of gel transfer to another person medicine in ancient egypt isoniazid 300 mg for sale. One or two 4-mg nongenital testosterone patches are applied daily over the skin of the back medications used for depression order isoniazid 300 mg online, thigh symptoms 4 days post ovulation isoniazid 300 mg on line, or upper arm away from pressure areas medications vitamins buy isoniazid 300 mg low price. Bioadhesive buccal testosterone tablets at a dose of 30 mg are applied twice daily on the buccal mucosa symptoms 8 weeks pregnant cheap isoniazid 300 mg visa. Intranasal testosterone is administered as a spray in each nostril 3 times a day (33 mg/day). Establishing Efficacy of Testosterone Replacement Therapy Because a clinically useful marker of androgen action is not available, correction of symptoms, induction and maintenance of secondary sex characteristics, and restoration of testosterone levels into the mid-normal range remain the goal of therapy. Testosterone should be measured 3 months after initiating therapy to assess adequacy of therapy. There is substantial inter-individual variability in serum testosterone levels, especially with transdermal gels, presumably due to genetic differences in testosterone clearance and substantial variation in transdermal absorption. In patients who are treated with testosterone enanthate or cypionate, testosterone levels should be 350600 ng/dL 1 week after the injection. If testosterone levels are outside this range, adjustments should be made either in the dose or in the interval between injections. In men on transdermal patch, gel, or buccal testosterone therapy, testosterone levels should be in the midnormal range (400750 ng/dL) 412 h after application. Multiple dose adjustments are often necessary to achieve testosterone levels in the desired therapeutic range. Restoration of sexual function, induction and maintenance of secondary sex characteristics, well-being, and maintenance of muscle and bone health are important objectives of testosterone replacement therapy. The patient should be asked about sexual desire and activity, the presence of early morning erections, and the ability to achieve and maintain erections adequate for sexual intercourse. The hair growth in response to androgen replacement is variable and depends on ethnicity. Hypogonadal men with prepubertal onset of androgen deficiency who begin testosterone therapy in their late twenties or thirties may find it difficult to adjust to their newly found sexuality and may benefit from counseling. If the patient has a sexual partner, the partner should be included in counseling because of the dramatic physical and sexual changes that occur with androgen treatment. Contraindications for Androgen Administration Testosterone administration is contraindicated in men with prostate or breast cancer (Table 384-4). Testosterone therapy should not be administered without further urologic evaluation to men with a palpable prostate nodule or induration, or prostate-specific antigen >3 ng/mL, or with severe lower urinary tract symptoms (American Urological Association lower urinary tract symptom score >19). Testosterone replacement should not be administered to men with baseline hematocrit 50%, severe untreated obstructive sleep apnea, uncontrolled or poorly controlled congestive heart failure, or to men with myocardial infarction, stroke, or acute coronary syndrome in the preceding 3 months. Source: Reproduced from the Endocrine Society Guideline for Testosterone Therapy of Androgen Deficiency Syndromes in Men (Bhasin S et al: J Clin Endocrinol Metab 95:2536, 2010). Potential adverse effects include acne, oiliness of skin, erythrocytosis, breast tenderness and enlargement, leg edema, and increased risk of detection of prostate events. In addition, there may be formulation-specific adverse effects such as skin irritation with transdermal patch; risk of gel transfer to a sexual partner with testosterone gels; buccal ulceration and gum problems with buccal testosterone; pain and mood fluctuation with injectable testosterone esters; cough and injection site pain with long-acting testosterone undecanoate; and, nasal irritation, epistaxis, and nasal scab with intranasal formulation. Hemoglobin Levels Administration of testosterone to androgendeficient men is typically associated with a ~3% increase in hemoglobin levels, due to increased erythropoiesis, stimulation of erythropoietin, suppression of hepcidin, and increased iron availability for erythropoiesis. The magnitude of hemoglobin increase during testosterone therapy is greater in older men than younger men, and in men who have sleep apnea, a significant smoking history, or chronic obstructive lung disease, or who live at high altitude. The frequency of erythrocytosis is higher in hypogonadal men treated with injectable testosterone esters than in those treated with transdermal formulations, presumably due to the higher testosterone dose delivered by the typical regimens of testosterone esters. Erythrocytosis is the most frequent adverse event reported in testosterone trials in middle-aged and older men and is also the most frequent cause of treatment discontinuation in these trials. If hematocrit rises above 54%, testosterone therapy should be stopped until hematocrit has fallen to <50%. After evaluation of the patient for hypoxia and sleep apnea, testosterone therapy may be reinitiated at a lower dose. However, androgen administration can exacerbate preexisting metastatic prostate cancer. It is not known whether long-term testosterone administration will induce these microscopic foci to grow into clinically significant cancers. Evaluate the patient 36 months after treatment initiation and then annually to assess whether symptoms have responded to treatment and whether the patient is suffering from any adverse effects. Adjust the number of pellets and/or the dosing interval to achieve serum testosterone levels in the normal range. If hematocrit is >54%, stop therapy until hematocrit decreases to a safe level; evaluate the patient for hypoxia and sleep apnea; reinitiate therapy with a reduced dose. Measure bone mineral density of lumbar spine and/or femoral neck after 12 yr of testosterone therapy in hypogonadal men with osteoporosis or low trauma fracture, consistent with regional standard of care. Evaluate formulation-specific adverse effects at each visit: uccaltestosteronetablets*: Inquire about alterations in taste and B examine the gums and oral mucosa for irritation. Serum testosterone levels are maintained when the application site is washed 46 h after application of the testosterone gel. Source: Reproduced with permission from the Endocrine Society Guideline for Testosterone Therapy of Androgen Deficiency Syndromes in Adult Men (Bhasin S et al: J Clin Endocrinol Metab 95:2536, 2010). Cardiovascular Risk As discussed above, there is insufficient evidence to determine whether testosterone replacement therapy increases the risk of major adverse cardiovascular events in hypogonadal men. A large prospective randomized trial is being planned to determine the effects of testosterone replacement therapy on major adverse cardiovascular events in middle-aged and older men with low testosterone levels and symptoms of androgen deficiency. The causes of death among power lifters included suicides, myocardial infarction, and hepatic coma. Orally administered androgens also have been associated with insulin resistance and diabetes. However, if needed, accredited laboratories use gas chromatography-mass spectrometry or liquid chromatography-mass spectrometry to detect anabolic steroid abuse. In recent years, the availability of high-resolution mass spectrometry and tandem mass spectrometry has further improved the sensitivity of detecting androgen abuse. Ratios above 4 suggest exogenous testosterone use but can also reflect genetic variation. Synthetic testosterone has a lower 13C:12C ratio than endogenously produced testosterone and these differences in 13C:12C ratio can be detected by isotope ratio combustion mass spectrometry, which is used to confirm exogenous testosterone use in individuals with a high testosterone to epitestosterone ratio. Basaria S et al: Effects of testosterone administration for 3 years on subclinical atherosclerosis progression in older men with low or low-normal testosterone levels: A randomized clinical trial. Bhasin S et al: Testosterone therapy in men with androgen deficiency syndromes: An endocrine society clinical practice guideline. Bhasin S et al: Effect of testosterone supplementation with and without a dual 5-reductase inhibitor on fat-free mass in men with suppressed testosterone production: a randomized controlled trial. Hall the female reproductive system regulates the hormonal changes responsible for puberty and adult reproductive function. Normal reproductive function in women requires the dynamic integration of hormonal signals from the hypothalamus, pituitary, and ovary, resulting in repetitive cycles of follicle development, ovulation, and preparation of the endometrial lining of the uterus for implantation should conception occur. It is critical to understand pubertal development in normal girls (and boys) as a yardstick for identifying precocious and delayed puberty. To achieve these functions in repeated monthly cycles, the ovary undergoes some of the most dynamic changes of any organ in the body. Primordial germ cells can be identified by the third week of gestation, and their migration to the genital ridge is complete by 6 weeks of gestation. Germ cells persist within the genital ridge, are then referred to as oogonia, and are essential for induction of ovarian development. In patients with 45,X Turner syndrome, primordial germ cells proliferate and migrate to the genital ridge, but do not persist as their survival requires the presence of pregranulosa cells that are dependent on the presence of both X chromosomes. The germ cell population expands, and starting at ~8 weeks of gestation, oogonia begin to enter prophase of the first meiotic division and become primary oocytes. Granulosa cells are derived from mesonephric cells that invade the ovary early in its development, pushing the germ cells to the periphery. Although there is evidence that both oocyte-like cells and follicle-like structures can form from embryonic stem cells in culture, there is, as yet, no clear evidence that this occurs in vivo and thus, the ovary appears to contain a nonrenewable pool of germ cells. Through the combined processes of mitosis, meiosis, and atresia, the population of oogonia reaches its maximum of 67 million by 20 weeks of gestation, after which there is a progressive loss of both oogonia and primordial follicles through the process of atresia. It appears that entry into meiosis provides some degree of protection from programmed cell death. The oocyte persists in prophase of the first meiotic division until just before ovulation, when meiosis resumes. The quiescent primordial follicles are recruited to further growth and differentiation through a highly regulated process that limits the size of the developing cohort to ensure that folliculogenesis can continue throughout the reproductive life span. The theca interna cells that surround the developing follicle begin to form as the primary follicle grows. Acquisition of a zona pellucida by the oocyte and the presence of several layers of surrounding cuboidal granulosa cells mark the development of secondary follicles. Bidirectional signaling between the germ cells and the somatic cells in the ovary is a necessary component underlying the maturation of the oocyte and the capacity for hormone secretion. The early stages of follicle growth are primarily driven by intraovarian factors; after initial recruitment, development to the secondary follicle stage may take close to a year. They migrate along the scaffold of the olfactory neurons across the cribiform plate to the hypothalamus where they separate from the olfactory neurons. Thus, like the ovary, the hypothalamic and pituitary components of the reproductive system are present before birth. However, the high levels of estradiol and progesterone produced by the placenta suppress hypothalamic-pituitary stimulation of ovarian hormonal secretion in the fetus. Recruitment to the small antral stage generally occurs over several cycles with further growth to follicle sizes of >47 mm in several waves during a single cycle. A single dominant follicle emerges from the growing follicle pool within the first 57 days after the onset of menses while the majority of follicles fall off their growth trajectory and become atretic. The dominant follicle undergoes rapid expansion during the 56 days prior to ovulation, reflecting granulosa cell proliferation and accumulation of follicular fluid. Ovulation requires production of extracellular matrix leading to expansion of the cumulus cell population that surrounds the oocyte and the controlled expulsion of the egg and follicular fluid. Both progesterone and prostaglandins (induced by the ovulatory stimulus) are essential for this process as are members of the matrix metalloproteinase family. Gonadotropin levels are cyclic during the reproductive years and increase dramatically with the loss of negative feedback that accompanies menopause. Metabolic signals, including adipocyte-derived leptin, play a permissive role in reproductive function (Chap. The sequence of steps and the enzymes involved in the synthesis of steroid hormones are similar in the ovary, adrenal, and testis. However, the enzymes required to catalyze specific steps are compartmentalized and may not be abundant or even present in all cell types. These steroid precursors cross the basal lamina to the granulosa cells, which receive no direct blood supply. Theca cellproduced androstenedione and, to a lesser extent, testosterone are also secreted into peripheral blood, where they can be converted to dihydrotestosterone in skin and to estrogens in adipose tissue. The hilar interstitial cells of the ovary are functionally similar to Leydig cells and are also capable of secreting androgens. However, high levels of androgens may be produced by luteinized theca cells in women with hyperthecosis. As in the follicle, both cell types are required for steroidogenesis in the corpus luteum. The luteinized granulosa cells are the main source of progesterone production, whereas the smaller theca lutein cells produce 17-hydroxyprogesterone and androgenic substrates for aromatization to estradiol by the luteinized granulosa cells. Production of estrogen metabolites by the corpus luteum plays a significant role in maintenance of the vascularization required for its function. Steroid Hormone Actions Both estrogen and progesterone play critical roles in the expression of secondary sexual characteristics in women (Chap. Estrogen promotes development of the ductule system in the breast, whereas progesterone is responsible for glandular development. In the reproductive tract, estrogens create a receptive environment for fertilization and support pregnancy and parturition through carefully coordinated changes in the endometrium, thickening of the vaginal mucosa, thinning of the cervical mucus, and uterine growth and contractions. Progesterone induces secretory activity in the estrogen-primed endometrium, increases the viscosity of cervical mucus, and inhibits uterine contractions. Both gonadal steroids play critical roles in negative and positive feedback of gonadotropin secretion. Progesterone also increases basal body temperature and has therefore been used clinically as a marker of ovulation. The vast majority of circulating estrogens and androgens are carried in the blood bound to carrier proteins, which restrain their free diffusion into cells and prolong their clearance, serving as a reservoir. Inhibin A is present in both granulosa and theca cells and is secreted by the dominant follicle. Inhibin A is also present in luteinized granulosa cells and is a major secretory product of the corpus luteum. Inhibins function as potent antagonists of activins through sequestration of the activin receptors. For the majority of the cycle, the reproductive system functions in a classic endocrine negative feedback mode. The resultant granulosa cell proliferation is responsible for increasing early follicular phase levels of inhibin B. Increasing levels of estradiol are responsible for proliferative changes in the endometrium. Luteal phase length is relatively constant between 12 and 14 days in normal cycles; thus, the major variability in cycle length is due to variations in follicular phase length.
Even if new neurons are able to integrate into spinal cord circuits and become properly innervated treatment 02 buy isoniazid 300 mg fast delivery, they would have to grow long axons that would take many months to years to project to appropriate targets and attract myelinating Schwann cells medications for osteoporosis isoniazid 300 mg fast delivery. Furthermore medications causing gout buy isoniazid 300 mg on line, cells would need to be grafted at multiple spinal cord and brainstem levels medicine cards buy isoniazid 300 mg without prescription, and the upper motor neuron deficit would need to be treated by replacing projecting neurons in the motor cortex medicine evolution order generic isoniazid canada. An additional complication is the recent finding that spinal motor neurons have unique segmental identity, and replacement cells might need to be generated with a range of molecular identities in order to integrate at multiple spinal levels. A more tractable near-term solution would be to graft support cells that could rescue or protect endogenous motor neurons from damage. The cells dispersed and were able to rescue motor neurons, a very promising result, but disappointingly, the animals became weak and died at the same rate as untreated control animals. In the hope that patients will respond differently than mice, a clinical trial based on this approach has been approved by the U. While these stem cell banks were still being produced, the first Japanese study to use stem cells was approved in August, 2013, and involved patients who were to receive customized therapy using cells derived from their own skin fibroblasts. A challenge is to coax the replacement cells to recreate an epithelium in the subretinal space. This outcome serves as a caution for the challenges involved in bringing a customized cell therapy to the clinic. This lax regulation has spawned a veritable industry of stem cell clinics making unsubstantiated claims of success in treating nervous system diseases. Patients have died from treatments in unregulated clinics operating in countries around the world and three patients became blind in a well-publicized incident following stem cell treatments delivered by a Florida clinic. These activities represent the dark side of the stem cell revolution perpetrated by practitioners who exploit the desperation of patients and their families. Legitimate and effective stem cell therapies will emerge over time, but given the prevalence and abundance of misleading information available on the internet and elsewhere, a trusted and well-informed physician can play a key role in helping patients navigate the current cell therapy minefield. Hong S et al: Complement and microglia mediate early synapse loss in Alzheimer mouse models. Lowenstein A seizure (from the Latin sacire, "to take possession of") is a transient occurrence of signs or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. Depending on the distribution of discharges, this abnormal brain activity can have various manifestations, ranging from dramatic convulsive activity to experiential phenomena not readily discernible by an observer. Although a variety of factors influence the incidence and prevalence of seizures, ~510% of the population will have at least one seizure, with the highest incidence occurring in early childhood and late adulthood. The meaning of the term seizure needs to be carefully distinguished from that of epilepsy. Epilepsy describes a condition in which a person has a risk of recurrent seizures due to a chronic, underlying process. This definition implies that a person with a single seizure, or recurrent seizures due to correctable or avoidable circumstances, does not necessarily have epilepsy (although a single seizure associated with particular clinical or electroencephalographic features may establish the diagnosis of epilepsy). Epilepsy refers to a clinical phenomenon rather than a single disease entity, because there are many forms and causes of epilepsy. However, among the many causes of epilepsy there are various epilepsy syndromes in which the clinical and pathologic characteristics are distinctive and suggest a specific underlying etiology. Using the definition of epilepsy as two or more unprovoked seizures, the incidence of epilepsy is ~0. Determining the type of seizure that has occurred is essential for focusing the diagnostic approach on particular etiologies, selecting the appropriate therapy, and providing potentially vital information regarding prognosis. This system is based on the clinical features of seizures and associated electroencephalographic findings. Other potentially distinctive features such as etiology or cellular substrate are not considered in this classification system, although this will undoubtedly change in the future as more is learned about the pathophysiologic mechanisms that underlie specific seizure types. Focal seizures originate within networks limited to one brain region (note that the term partial seizures is no longer used). Focal Onset (Can be further described as having intact or impaired awareness, motor or nonmotor onset, or evolve from focal to bilateral tonic clonic) 2. Focal seizures arising from the tem- 3051 poral or frontal cortex may also cause alterations in hearing, olfaction, or emotional state. Some patients describe odd, internal feelings such as fear, a sense of impending change, detachment, depersonalization, déjá vu, or illusions that objects are growing smaller (micropsia) or larger (macropsia). These subjective, "internal" events that are not directly observable by someone else are referred to as auras. In contrast, generalized seizures may result from cellular, biochemical, or structural abnormalities that have a more widespread distribution. Focal seizures arise from a neuronal network either discretely localized within one brain region or more broadly distributed but still within a cerebral hemisphere. With the new classification system, the subcategories of "simple focal seizures" and "complex focal seizures" have been eliminated. Instead, the classification emphasizes the effect on awareness (intact or impaired) and nature of the onset (motor or nonmotor). In the past this was referred to as focal seizures with secondary generalization, but the new system relies on descriptions of the type of generalized seizures that evolve from the focal seizure. Because focal seizures can arise from the medial temporal lobe or inferior frontal lobe. However, the region of seizure onset may be detected using surgically placed intracranial electrodes. The patient is unable to respond appropriately to visual or verbal commands during the seizure and has impaired recollection or awareness of the ictal phase. The start of the ictal phase is often a motionless stare, which marks the onset of the period of impaired awareness. The impaired awareness is usually accompanied by automatisms, which are involuntary, automatic behaviors that have a wide range of manifestations. Automatisms may consist of very basic behaviors such as chewing, lip smacking, swallowing, or "picking" movements of the hands, or more elaborate behaviors such as a display of emotion or running. The patient is typically confused following the seizure, and the transition to full recovery of consciousness may range from seconds up to an hour or longer. Examination immediately following the seizure may show an anterograde amnesia or transient neurological deficits (such as aphasia, hemi-neglect, or visual loss) caused by postictal inhibition of the cortical regions most involved in the seizure itself. The range of potential clinical behaviors linked to focal seizures is so broad that extreme caution is advised before concluding that stereotypic episodes of bizarre or atypical behavior are not due to seizure activity. For example, a patient having a focal motor seizure arising from the right primary motor cortex near the area controlling hand movement will note the onset of involuntary movements of the contralateral, left hand. Since the cortical region controlling hand movement is immediately adjacent to the region for facial expression, the seizure may also cause abnormal movements of the face synchronous with the movements of the hand. First, in some patients, the abnormal motor movements may begin in a very restricted region such as the fingers and gradually progress (over seconds to minutes) to include a larger portion of the extremity. This phenomenon, described by Hughlings Jackson and known as a "Jacksonian march," represents the spread of seizure activity over a progressively larger region of motor cortex. This condition, termed epilepsia partialis continua, is often refractory to medical therapy. This evolution is observed frequently following focal seizures arising from a region in the frontal lobe, but may also be associated with focal seizures occurring elsewhere in the brain. A focal seizure that evolves into a generalized seizure is often difficult to distinguish from a primary generalized onset tonic-clonic seizure, because bystanders tend to emphasize the more dramatic, generalized convulsive phase of the seizure and overlook the more subtle, focal symptoms present at onset. In some cases, the focal onset of the seizure becomes apparent only when a careful history identifies a preceding aura. Nonetheless, distinguishing between these two entities is extremely important, because there may be substantial differences in the evaluation and treatment of epilepsies characterized by focal versus generalized onset seizures. Several types of generalized seizures have features that place them in distinctive categories and facilitate clinical diagnosis. Typical Absence Seizures Typical absence seizures are charac- terized by sudden, brief lapses of consciousness without loss of postural control. The seizure usually lasts for only seconds, consciousness returns as suddenly as it was lost, and there is no postictal confusion. Although the brief loss of consciousness may be clinically inapparent or the sole manifestation of the seizure discharge, absence seizures are usually accompanied by subtle, bilateral motor signs such as rapid blinking of the eyelids, chewing movements, or small-amplitude, clonic movements of the hands. The seizures can occur hundreds of times per day, but the child may be unaware of or unable to convey their existence. Because the clinical signs of the seizures are subtle, especially to parents who may not have had previous experience with seizures, it is not surprising that the first clue to absence epilepsy is often unexplained "daydreaming" and a decline in school performance recognized by a teacher. There are a number of variants of generalized motor seizures, including pure tonic and pure clonic seizures. Brief tonic seizures lasting only a few seconds are especially noteworthy since they are usually associated with specific epilepsy syndromes having mixed seizure phenotypes, such as the Lennox-Gastaut syndrome (discussed below). Atonic Seizures Atonic seizures are characterized by sudden loss of postural muscle tone lasting 12 s. A very brief seizure may cause only a quick head drop or nodding movement, whereas a longer seizure will cause the patient to collapse. This can be extremely dangerous, because there is a substantial risk of direct head injury with the fall. Similar to pure tonic seizures, atonic seizures are usually seen in association with known epilepsy syndromes. Myoclonic Seizures Myoclonus is a sudden and brief muscle contraction that may involve one part of the body or the entire body. A normal, common physiologic form of myoclonus is the sudden jerking movement observed while falling asleep. Although the distinction from other forms of myoclonus is imprecise, myoclonic seizures are considered to be true epileptic events because they are caused by cortical (versus subcortical or spinal) dysfunction. Epileptic Spasms Epileptic spasms are characterized by a briefly sustained flexion or extension of predominantly proximal muscles, including truncal muscles. For example, the lapse of consciousness is usually of longer duration and less abrupt in onset and cessation, and the seizure is accompanied by more obvious motor signs that may include focal or lateralizing features. Atypical absence seizures are usually associated with diffuse or multifocal structural abnormalities of the brain and therefore may accompany other signs of neurologic dysfunction such as mental retardation. Furthermore, the seizures are less responsive to anticonvulsants compared to typical absence seizures. They are also the most common seizure type resulting from metabolic derangements and are therefore frequently encountered in many different clinical settings. The seizure usually begins abruptly without warning, although some patients describe vague premonitory symptoms in the hours leading up to the seizure. This prodrome is distinct from the stereotypic auras associated with focal seizures that generalize. The initial phase of the seizure is usually tonic contraction of muscles throughout the body, accounting for a number of the classic features of the event. Tonic contraction of the muscles of expiration and the larynx at the onset will produce a loud moan or "ictal cry. A marked enhancement of sympathetic tone leads to increases in heart rate, blood pressure, and pupillary size. After 1020 s, the tonic phase of the seizure typically evolves into the clonic phase, produced by the superimposition of periods of muscle relaxation on the tonic muscle contraction. The periods of relaxation progressively increase until the end of the ictal phase, which usually lasts no more than 1 min. The postictal phase is characterized by unresponsiveness, muscular flaccidity, and excessive salivation that can cause stridorous breathing and partial airway obstruction. Patients gradually regain consciousness over minutes to hours, and during this transition, there is typically a period of postictal confusion. Patients subsequently complain of headache, fatigue, and muscle ache that can last for many hours. The duration of impaired consciousness in the postictal phase can be extremely long. In the clonic phase, the high-amplitude activity is typically interrupted by slow waves to create a spike-and-slow-wave pattern. Three important epilepsy syndromes are listed below; additional examples with a known genetic basis are shown in Table 418-2. The myoclonic seizures are most frequent in the morning after awakening and can be provoked by sleep deprivation. Many patients also experience generalized tonic-clonic seizures, and up to one-third have absence seizures. Although complete remission is relatively uncommon, the seizures usually respond well to appropriate anticonvulsant medication. There is often a family history of epilepsy, and genetic linkage studies suggest a polygenic cause. The last three syndromes are examples of the numerous Mendelian disorders in which seizures are one part of the phenotype. The multifactorial nature of this syndrome suggests that it is a nonspecific response of the brain to diffuse neuronal dysfunction. Recognition of this syndrome is especially important because it tends to be refractory to treatment with anticonvulsants but responds well to surgical intervention. Given the numerous properties that control neuronal excitability, it is not surprising that there are many different ways to perturb this normal balance, and therefore many different causes of both seizures and epilepsy. Three clinical observations emphasize how a variety of factors determine why certain conditions may cause seizures or epilepsy in a given patient. The normal brain is capable of having a seizure under the appropriate circumstances, and there are differences between individuals in the susceptibility or threshold for seizures. For example, seizures may be induced by high fevers in children who are otherwise normal and who never develop other neurologic problems, including epilepsy. However, febrile seizures occur only in a relatively small proportion of children.
Syndromes
- In men: on the penis, scrotum, around the anus, on the thighs or buttocks
- Avoid standing for long periods. If you must stand for your work, place a stool by your feet. Alternate resting each foot on the stool.
- Congenital adrenal hyperplasia
- Vision problems
- Discoloration of the skin, especially bruising
- ECG
Immediately after birth treatment kidney failure isoniazid 300 mg purchase on-line, the neonatal liver must assume responsibility for bilirubin clearance and excretion medicine symbol order isoniazid online from canada. Since the intestinal flora that convert bilirubin to urobilinogen are also undeveloped treatment pancreatitis 300 mg isoniazid otc, an enterohepatic circulation of unconjugated bilirubin ensues symptoms liver disease buy isoniazid master card. As a consequence treatment effect definition generic 300 mg isoniazid overnight delivery, most neonates develop mild unconjugated hyperbilirubinemia between days 2 and 5 after birth. Peak levels are typically <85170 mol/L (510 mg/dL) and decline to normal adult concentrations within 2 weeks, as mechanisms required for bilirubin disposition mature. Prematurity, often associated with more profound immaturity of hepatic function and hemolysis, can result in higher levels of unconjugated hyperbilirubinemia. A rapidly rising unconjugated bilirubin concentration, or absolute levels >340 mol/L (20 mg/dL), puts the infant at risk for bilirubin encephalopathy, or kernicterus. Under these circumstances, bilirubin crosses an immature blood-brain barrier and precipitates in the basal ganglia and other areas of the brain. Treatment options include phototherapy, which converts bilirubin into water-soluble photoisomers that are excreted directly into bile, and exchange transfusion. These processes normally account for a small proportion of bilirubin that is produced. In various disorders, including thalassemia major, megaloblastic anemias due to folate or vitamin B12 deficiency, congenital erythropoietic porphyria, lead poisoning, and various congenital and acquired dyserythropoietic anemias, the fraction of total bilirubin production derived from ineffective erythropoiesis is increased, reaching as much as 70% of the total. This may be sufficient to produce modest degrees of unconjugated hyperbilirubinemia. Miscellaneous Degradation of the hemoglobin of extravascular collections of erythrocytes, such as those seen in massive tissue infarctions or large hematomas, may lead transiently to unconjugated hyperbilirubinemia. A modest reduction in bilirubin conjugating capacity may be observed in advanced hepatitis or cirrhosis. However, in this setting, conjugation is better preserved than other aspects of bilirubin disposition, such as canalicular excretion. Bilirubin conjugation may be inhibited by certain fatty acids that are present in breast milk, but not serum of mothers whose infants have excessive neonatal hyperbilirubinemia (breast milk jaundice). Alternatively, there may be increased enterohepatic circulation of bilirubin in these infants. Other conventional hepatic biochemical tests such as serum aminotransferases and alkaline phosphatase are normal, and there is no evidence of hemolysis. Hepatic histology is also essentially normal except for the occasional presence of bile plugs within canaliculi. Unconjugated bilirubin accumulates in plasma, from which it is eliminated very slowly by alternative pathways that include direct passage into the bile and small intestine, possibly via bilirubin photoisomers. Many patients are from geographically or socially isolated communities in which consanguinity is common, and pedigree analyses show an autosomal recessive pattern of inheritance. A few lived as long as early adult life without overt neurologic damage, although more subtle testing usually indicated mild but progressive brain damage. In the absence of liver transplantation, death eventually supervened from late-onset bilirubin encephalopathy, which often followed a nonspecific febrile illness. Bilirubin concentrations during phenobarbital administration do not return to normal but are typically in the range of 5186 mol/L (35 mg/dL). For this reason, phenobarbital therapy is widely recommended, a single bedtime dose often sufficing to maintain clinically safe serum bilirubin concentrations. The spectrum of residual enzyme activity explains the spectrum of phenotypic severity of the resulting hyperbilirubinemia. Serum bilirubin concentrations are most often <51 mol/L (<3 mg/dL), although both higher and lower values are frequent. Bilirubin concentrations may fluctuate substantially in any given individual, and at least 25% of patients will exhibit temporarily normal values during prolonged follow-up. More elevated values are associated with stress, fatigue, alcohol use, reduced caloric intake, and intercurrent illness, while increased caloric intake or administration of enzyme-inducing agents produces lower bilirubin levels. Studies of radiobilirubin kinetics indicate that hepatic bilirubin clearance is reduced to an average of one-third of normal. The metabolism and transport of bile acids that do not utilize the bilirubin uptake mechanism are normal. Moreover, on theoretical grounds, the results of such studies should provide no more information than simple measurements of the baseline serum bilirubin concentration. While normal by standard criteria, these individuals had somewhat higher bilirubin concentrations than the rest of the controls studied. It was suggested that additional variables, such as mild hemolysis or a defect in bilirubin uptake, might be among the factors enhancing phenotypic expression of the defect. Another Japanese patient with mild unconjugated hyperbilirubinemia was homozygous for a missense mutation in exon 5. Although biliary tract obstruction or hepatocellular cholestatic injury may present on occasion with a predominantly conjugated hyperbilirubinemia, it is generally not possible to differentiate intrahepatic from extrahepatic causes of jaundice based on the serum levels or relative proportions of unconjugated and conjugated bilirubin. The major reason for determining the amounts of conjugated and unconjugated bilirubin in the serum is for the initial differentiation of hepatic parenchymal and obstructive disorders (mixed conjugated and unconjugated hyperbilirubinemia) from the inheritable and hemolytic disorders discussed above that are associated with unconjugated hyperbilirubinemia. Total bilirubin concentrations are typically between 34 and 85 mol/L (2 and 5 mg/dL) but on occasion can be in the normal range or as high as 340430 mol/L (2025 mg/dL) and can fluctuate widely in any given patient. The degree of hyperbilirubinemia may be increased by intercurrent illness, oral contraceptive use, and pregnancy. Because the hyperbilirubinemia is due to a predominant rise in conjugated bilirubin, bilirubinuria is characteristically present. Aside from elevated serum bilirubin levels, other routine laboratory tests are normal. Physical examination is usually normal except for jaundice, although an occasional patient may have hepatosplenomegaly. These latter patients have usually undergone extensive and often unnecessary diagnostic examinations for unexplained jaundice and have high levels of anxiety. In women, the condition may be subclinical until the patient becomes pregnant or receives oral contraceptives, at which time chemical hyperbilirubinemia becomes frank jaundice. Even in these situations, other routine liver function tests, including serum alkaline phosphatase and transaminase activities, are normal. This pigment is thought to be derived from epinephrine metabolites that are not excreted normally. The pigment may disappear during bouts of viral hepatitis, only to reaccumulate slowly after recovery. These patients have normal serum and biliary bile acid concentrations and do not have pruritus. The pattern in Rotor syndrome resembles that of many acquired disorders of hepatobiliary function, in which coproporphyrin I, the major coproporphyrin isomer in bile, refluxes from the hepatocyte back into the circulation and is excreted in urine. A major phenotypic difference is that the liver in patients with Rotor syndrome has no increased pigmentation and appears totally normal. The only abnormality in routine laboratory tests is an elevation rare disorder is characterized by recurrent attacks of pruritus and jaundice. The typical episode begins with mild malaise and elevations in serum aminotransferase levels, followed rapidly by rises in alkaline phosphatase and conjugated bilirubin and onset of jaundice and itching. The cholestatic episodes, which may begin in childhood or adulthood, can vary in duration from several weeks to months, followed by a complete clinical and biochemical resolution. Between episodes, physical examination is normal, as are serum levels of bile acids, bilirubin, transaminases, and alkaline phosphatase. However, the episodes of jaundice and pruritus can be prolonged and debilitating, and some patients have undergone liver transplantation to relieve the intractable and disabling symptoms. Treatment during the cholestatic episodes is symptomatic; there is no specific treatment to prevent or shorten the occurrence of episodes. Curiously, this gene is expressed strongly in the small intestine but only weakly in the liver. Although these agents can be distinguished by their molecular and antigenic properties, all types of viral hepatitis produce clinically similar illnesses. Inactivation of viral activity can be achieved by boiling for 1 min, by contact with formaldehyde and chlorine, or by ultraviolet irradiation. Its replication is limited to the liver, but the virus is present in the liver, bile, stools, and blood during the late incubation period and acute preicteric/presymptomatic phase of illness. Despite slightly longer persistence of virus in the liver, fecal shedding, viremia, and infectivity diminish rapidly once jaundice becomes apparent. This early antibody response is predominantly of the IgM class and persists for several (~3) months, rarely for 612 months. Left: Hepatitis B isolates fall into one of at least 27-nm hepatitis A virus particles purified from stool of a patient with acute hepatitis A and aggregated by antibody to hepatitis A virus. Right: Concentrated serum from a patient with hepatitis B, demonstrating the 42-nm virions, 8 subtypes and 10 genotypes (AJ). Clinical course and outcome are independent of subtype, but has been identified in contemporary fish. Such transfected cells support in vitro replication of the intact virus and its component proteins. Pre-S1 and pre-S2, upstream of S, combine with S to code for two larger proteins, "middle" protein, the product of pre-S2 + S, and "large" protein, the product of pre-S1 + pre-S2 + S. When packaging within viral proteins is complete, synthesis of the incomplete plus strand stops; this accounts for the single-strand gap and for differences in the size of the gap. Pre-S1 and pre-S2 proteins are also expressed during periods of peak replication, but assays for these gene products are not routinely available. In many cases, this seroconversion coincides with a transient, usually mild, acute hepatitis-like elevation in aminotransferase activity, believed to reflect cell-mediated immune clearance of virus-infected hepatocytes. For example, variants have been described that lack nucleocapsid proteins (commonly), envelope proteins (very rarely), or both. In addition, clusters of fulminant hepatitis B in Israel and Japan were attributed to commonsource infection with a precore mutant. Although such mutants have not been recognized frequently, their existence raises a concern that may complicate vaccination strategies and serologic diagnosis. The clinical spectrum of hepatitis D is common to all eight genotypes identified, the predominant of which is genotype 1. The 5 untranslated region and core gene are highly conserved among genotypes, but the envelope proteins are coded for by the hypervariable region, which varies from isolate to isolate and may allow the virus to evade host immunologic containment directed at accessible virus-envelope proteins. The 5 untranslated region and the C region are highly virions per day; its half-life is 2. The conserved among isolates, whereas the envelope domain E2 contains the hypervariable region. Genotypes differ from one another in sequence homology by 30%, and subtypes differ by ~20%. In addition, differences exist among genotypes in responsiveness to antiviral therapy but not in pathogenicity or clinical progression (except for genotype 3, in which hepatic steatosis and clinical progression are more likely). Among the viral hepatitides, the immunopathogenesis of hepatitis B and C has been studied most extensively. Contributing to the perpetuation of this virus are animal reservoirs, most notably in swine but also in camels, deer, rats, and rabbits, among others. The virus has been detected in stool, bile, and liver, and is excreted in the stool during the late incubation period. The model that has the most experimental support involves cytolytic T cells sensitized specifically to recognize host and hepatitis B viral antigens on the liver cell surface. Similarly, in patients who undergo liver transplantation for end-stage chronic hepatitis B, occasionally, rapidly progressive liver injury appears in the new liver. This, in turn, may explain why, when infection occurs so early in life, immunologic clearance does not occur, and protracted, lifelong infection ensues. After adulthood-acquired infection, chronicity is uncommon, and the risk of hepatocellular carcinoma is very low. This somewhat simplistic formulation does not apply at all to the typical adult in the West with self-limited acute hepatitis B, in whom no period of immunologic tolerance occurs. Persons infected as neonates tend to have a relatively higher level of immunologic tolerance (high replication, low necroinflammatory activity) during the early decades of life and a relatively lower level (but only rarely a loss) of tolerance (and necroinflammatory activity reflecting the level of virus replication) in the later decades of life. Immune complexmediated tissue damage appears to play a pathogenetic role in the extrahepatic manifestations of acute hepatitis B. In patients with chronic hepatitis B, other types of immune-complex disease may be seen. The disorder is characterized clinically by arthritis, cutaneous vasculitis (palpable purpura), and, occasionally, glomerulonephritis and serologically by the presence of circulating cryoprecipitable immune complexes of more than one immunoglobulin class (Chaps. Immune-complex glomerulonephritis is another recognized extrahepatic manifestation of chronic hepatitis C. Immune-complex disorders have been linked, albeit rarely, with both hepatitis A and E. Hepatic cell regeneration is present, as evidenced by numerous mitotic figures, multinucleated cells, and "rosette" or "pseudoacinar" formation. The mononuclear infiltration consists primarily of small lymphocytes, although plasma cells and eosinophils occasionally are present. Liver cell damage consists of hepatic cell degeneration and necrosis, cell dropout, ballooning of cells, and acidophilic degeneration of hepatocytes (forming so-called Councilman or apoptotic bodies). In hepatitis C, the histologic lesion is often remarkable for a relative paucity of inflammation, a marked increase in activation of sinusoidal lining cells, lymphoid aggregates, the presence of fat (more frequent in genotype 3 and linked to increased fibrosis), and, occasionally, bile duct lesions in which biliary epithelial cells appear to be piled up without interruption of the basement membrane. A cholestatic variant of slowly resolving acute hepatitis A also has been described. A more severe histologic lesion, bridging hepatic necrosis, also termed subacute or confluent necrosis or interface hepatitis, is observed occasionally in acute hepatitis. Characteristically, the bridge consists of condensed reticulum, inflammatory debris, and degenerating liver cells that span adjacent portal areas, portal to central veins, or central vein to central vein. This lesion had been thought to have prognostic significance; in many of the originally described patients with this lesion, a subacute course terminated in death within several weeks to months, or severe chronic hepatitis and cirrhosis developed; however, the association between bridging necrosis and a poor prognosis in patients with acute hepatitis has not been upheld. Therefore, although demonstration of this lesion in patients with chronic hepatitis has prognostic significance (Chap.
Order isoniazid 300 mg with mastercard. Carbon Monoxide Test using a Propane Heater in a Tent - 16 Hour Test. (Mr. Heater).
References
- White RI Jr, Mitchell SE, Barth KH, et al. Angio architecture of pulmonary arteriovenous malformations: an important consideration before embolotherapy. AJR Am J Roentgenol. 1983;140:681-86.
- Fletcher R, Veintemilla F: Changes in the arterial to end-tidal PCO2 differences during coronary artery bypass grafting, Acta Anaesthesiol Scand 33:656-659, 1989.
- Monclair T, Brodeur GM, Ambros PF, et al: The international neuroblastoma risk group (INRG) staging system: an INRG Task Force Report, J Clin Oncol 27:298n303, 2009.
- D ayton P, Goldman FD, Barton E: Compartment pressure in the foot. Analysis of normal values and measurement technique. J Am Podiatr Med Assoc 80:521, 1990.
- Ernst ME, Moser M. Use of diuretics in patients with hypertension. N Engl J Med 2009;361(22):2153-2164.
- Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006;144:165-71.
- Lagana S, Taub R, Borczuk A. Utility of Glucose Transporter 1 in the differentiation of peritoneal and pleural mesothelioma from nonmalignant mesothelium. Mod Pathol 2010;23 suppl:406A. 1003.
- Ferreri AJ, Reni M, Foppoli M, et al. High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: a randomised phase 2 trial. Lancet 2009; 374(9700):1512- 1520.