
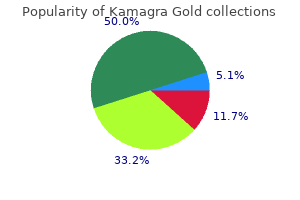
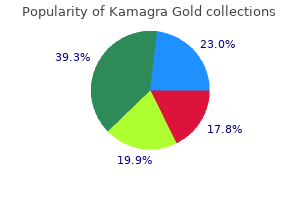
Kamagra Gold
| Contato
Página Inicial
Andrea DiPrincipe Coviello, MD
- Associate Professor of Medicine
https://medicine.duke.edu/faculty/andrea-diprincipe-coviello-md
Others observed an association between silica and lung cancer but it fell short of implicating this mineral in the induction of carcinoma of the lung erectile dysfunction due to zoloft discount kamagra gold 100 mg with amex. There was a decline in the overall age-adjusted mortality rates per million from 2 erectile dysfunction treatment dallas texas 100 mg kamagra gold overnight delivery. Such data indicate efforts to limit workplace exposures have been successful erectile dysfunction in young age discount 100 mg kamagra gold with amex, and should be continued to eradicate this preventable disease erectile dysfunction doctor in delhi kamagra gold 100 mg buy amex. The role of the more numerous silicate particles in the fibrotic process is unclear erectile dysfunction miracle buy discount kamagra gold 100 mg line. Diagnosis of mixed-dust pneumoconiosis requires a detailed occupational history and the finding of irregular opacities on chest radiographs. By definition the mixed dust fibrotic lesions should outnumber the silicotic nodules, otherwise silicosis is the preferred diagnosis. Examples include siderosilicosis in hematite miners, in which diffuse interstitial deposits of iron oxides may be seen in combination with typical silicotic nodules. Another example is asbestosilicosis, in which peribronchiolar interstitial fibrosis and asbestos bodies may be seen along with typical silicotic nodules. This is a fairly common finding in shipyard workers, where sandblasting, boiler-scaling and insulating activities occur simultaneously in a confined space. An extreme case of mixed pneumoconiosis featuring silicosis, asbestosis, talcosis and berylliosis was reported. The development of pulmonary disease depends on factors including the quantity and quality of inhaled dust, occupation within the mine, duration of exposure, interval since last exposure, and other considerations, such as cigarette smoking. In the United States, coal production and the number of coal miners is on the increase: 122 000 individuals in over 2000 mines in 26 states engaged in the production of more than one billion tons of coal in 2007. Coal is ranked to reflect its amount of fixed carbon, volatiles and heating value. Higher ranks (hard coal, anthracite) feature low moisture contents and higher amounts of fixed carbon than the lower-ranked soft coals (lignite, bituminous). Coal dust consists mainly of amorphous non-crystalline carbon together with varying amounts of crystalline silica (quartz), kaolin, mica and other silicates. The quartz content of coal dust is an important determinant of the pathological response. Anthracite usually contains a higher percentage of quartz than bituminous or lignite coal. The intensity of quartz exposure also varies for different jobs, within any particular coal mine. Roof bolters drilling into the ceiling of a shaft or constructing communicating shafts between adjacent coal seams are exposed to higher levels of crystalline silica than individuals working at the coalface, or loading coal for transport. Intratracheal instillation of amorphous carbon in experimental animals results in a substantial influx of macrophages into alveolar spaces, but no appreciable fibrosis. Calcification may be observed in 10:20% of such cases, but in a finely nodular pattern that helps distinguish it from the "eggshell pattern" typical of calcification in silicosis. Magnetic resonance scanning has been reported to be of use in such instances, prior to a biopsy diagnosis. Chronic inhalation of coal dust results in increased numbers of pulmonary inflammatory effector cells, including neutrophils and macrophages. These non-palpable lesions appear as 1:4 mm in diameter black areas distributed diffusely throughout the lung. An upper lobe preponderance is noted, owing to the relative reduction in density of lymphovasculature and particulate clearance in these areas. Together with a diffuse increase in background pigmentation, lesions impart a black appearance to the lung tissue. Macular lesions are typically more numerous in the upper lobes, and blackening also occurs along lymphatics within the secondary lobular septa and beneath the visceral pleura. These cells often extend into and fill adjacent alveolar spaces, as well as involving the peribronchiolar interstitium. The macrophages may form a mantle around respiratory bronchioles and accompanying small pulmonary arteries. Pigmented macrophages are found in the center of the nodules, as well as in the stellate mantle surrounding the lesion. The similar histology of these nodules to silicotic nodules demonstrates the presence of silica in coal dust. Emphysematous changes often occur in the zones adjacent to the coal dust macule, so-called focal emphysema. It closely resembles centrilobular emphysema in its gross and histological features, differing only in its limited extent and invariable association with the dust macule. This process was shown by Heppleston to involve all three orders of respiratory bronchioles, whereas centrilobular emphysema only involves the distal respiratory bronchiole, with a proximal bronchiolitis (see Chapter 17). This process is probably mediated by antiproteases secreted by coal-dust-activated macrophages. The spherical nodules are similar in appearance and distribution to those observed in silicosis, except they are more darkly pigmented. Note presence of birefringent silicate particles adjacent to haphazard array of collagen bundles. Variable amounts of necrosis with cholesterol clefts may be associated with black lipid debris. However, the typical histological picture of tuberculosis may be lacking, even in cases where mycobacteria are demonstrable. Those who develop clinically significant chronic obstructive lung disease are almost invariably miners who smoke. Some anthracotic pigmentation can be found in the lungs of nearly all adults in an industrialized society. Although pigment accumulation is related both to age and amount of cigarette smoking, there is considerable individual variation with regard to efficiency of particle clearance. Carbon electrode makers are exposed to a dust containing crushed coke and anthracite. The forms of commercial importance with the most potential for clinical relevance are typically non-fibrous sheet silicates, such as talc, kaolin and mica. As common airborne dusts in both urban and rural settings, profuse quantities of silicates may be identified in human lung tissue at autopsy, with hundreds of millions of such particles detected using analytic techniques. It is formed by two sheets of silica tetrahedral, separated by a magnesium hydroxide layer. Quartz and the non-commercial varieties of amphibole asbestos, such as tremolite, and anthophyllite are important contaminants. Exposure to talc, which is used in a number of manufacturing processes due to its lubricant properties, occurs in a variety of ways. Other occupations associated with exposure to talc include the leather, rubber, paper and textile industries; manufacture of ceramics, cosmetics, paints, pharmaceuticals, soaps, toiletries, and refractory and roofing materials; plate casting in which molds are dusted with talc before pouring; and dusting of life rafts with talc. Experimental animal studies demonstrated the amphibole contaminants of talc, tremolite and anthophyllite are markedly Diffuse interstitial fibrosis Diffuse interstitial fibrosis has also been described as a pathological response to inhaled coal dust, with severe cases demonstrating classic honeycomb changes, in addition to black pigmentation of lung tissue. This has led to a potential role for silica, silicates and coal dust in the development of diffuse interstitial fibrosis. Cough and wheezing, due to chronic bronchitis, have also been reported,210 the latter possibly resulting in part from airway irritation and mucosal desiccation. Parietal pleural plaques were first described in talc miners, and probably result from contaminating tremolite and anthophyllite asbestos. Macroscopically the lung may contain tiny discrete palpable nodules or show diffuse interstitial fibrosis. Mild lesions consist of dust-laden macrophages and connective tissue in the peribronchiolar and perivascular interstitium. Birefringent particles are observed with polarized light microscopy within giant cells, within macrophages, or free in the interstitium. Talc has also been used as filler for oral medicine preparations, and is one of several types of particles that may embolize to the lung, when oral medications are crushed and injected intravenously (see Chapter 16). Intravascular and interstitial granulomas may be associated with variable degrees of fibrosis. The latter are more numerous and larger than the occasional small birefringent calcific particles observed in giant cells in sarcoidosis (see Chapter 13). No increased lung cancer mortality has been described in a review of talc miners and millers heavily exposed to talc not containing asbestiform minerals, except when there was an association with other known carcinogens. Kaolinite is the major component of kaolin (china clay), and is mined in the state of Georgia in the United States, as well as in Europe, Egypt, Japan and China. The most intense exposures, causing pneumoconiosis, have been reported in kaolin miners and processing plant workers. The hilar lymph nodes are often enlarged, secondary to accumulation of masses of dust-laden macrophages. They show intra- and extracellular deposits of fine golden-brown particulates, located primarily in a peribronchiolar distribution. The nodular masses consist largely of dust deposits, traversed by scattered randomly distributed bands of collagen. Whorled, dense collagenous deposits have been described in some cases, but such lesions should be attributed to contaminating quartz, rather than kaolinite. The transparent forms have been used historically in the doors of lanterns and stoves (isinglass). Mica exposure is often sustained in the setting of exposure to other minerals, such as quartz and feldspar; however, it is apparent that exposure to mica alone may result in pneumoconiosis. Zeolites Zeolites are a complex group of hydrated aluminum silicates that include some 40 distinct mineral species used in the petrochemical industry, waste water treatment, water filtration, cement production and in animal litter. The mineral finds utility as loose-fill thermal insulation and fire production, aggregate in cement, wallboards and plasters, as well as a soil additive and bulking agent in animal feeds. Contamination with tremolite, actinolite or anthophyllite asbestos fibers raised concerns regarding the potential health effects of vermiculite exposure. Vermiculite miners have an increased risk of pleural mesothelioma and carcinoma of the lung. Analysis of lung tissue samples revealed large numbers of high-aspect-ratio tremolite asbestos fibers. In addition, nearly 7% of Libby community residents, without occupational or predominantly fibrous species. Erionite is found naturally in volcanic tuff in some areas of Turkey, where it is used as a construction material and is ubiquitous (see Chapter 36). The carcinogenic and fibrogenic effects of fibrous erionite are similar to , if not actually greater than, those of asbestos. Interest in the pathological effects of zeolites can be largely attributed to the discovery of an epidemic of malignant pleural mesothelioma in two small villages in the Anatolian region of Turkey. Surveys of the villages indicate a high prevalence of pleural calcification, diffuse pleural fibrosis and plaque formation, as well as diffuse interstitial fibrosis. The mineral has been identified in lung tissue from villagers suffering from mesothelioma, as well as in 539 Chapter 14: Occupational lung disease para-occupational exposure, had radiographic evidence of asbestos-related disease. Some animal studies show no tumorigenic potential for vermiculite, following intrapleural injection. As the second lightest known metal, beryllium is more rigid than steel, and an excellent conductor of heat and electricity. Modern usage of beryllium has shifted to the hightechnology and aerospace industries, where it is used in structural materials, guidance systems, optical devices, rocket motor parts and heat shields. It is also used in the electronics industry in ceramic parts, in the manufacture of thermal couplings and crucibles, in nuclear reactors, as well as in dental prosthetics and even in some bicycle frames and golf clubs. The manufacturing of these products results in exposure not only to beryllium silicate but also to beryllium oxide, hydroxide, fluoride, chloride and sulfate. The first ambient air quality standard ever established was that set in 1949 for beryllium, which preceded all others by some 25 years. There is also the potential for bystander exposure in individuals who work in facilities that use beryllium but do not handle the metal itself. In addition exposure can occur in those who live in the vicinity of such facilities, or who handle the clothing of beryllium workers. This is the mechanism for the beryllium lymphocyte proliferation test, used clinically as a biomarker. It may be performed using lymphocytes from the peripheral blood, or those obtained using bronchoalveolar lavage. Machinists appear to have the highest incidence of sensitization and chronic beryllium disease. In some series 10% of the sensitized workers will develop chronic beryllium disease annually. Some population-based studies show chronic disease will eventually develop in 2:16% of such cases. Acute berylliosis is a form of acute pneumonitis resulting from short-term exposure to high levels of soluble salts of beryllium (> 25 µg/m3), with symptoms beginning a few hours to several days after exposure. This has been reported in those engaged in the primary production of beryllium metal, or those exposed to beryllium-containing compounds in the fluorescent light industry. Acute beryllium pneumonitis shares the clinical features of other acute inhalational injuries, with nasopharyngeal irritation, as well as dyspnea, cough and other symptoms of lower airway irritation. In fatal cases of acute berylliosis, the lungs are wet, heavy and congested with the nonspecific histological findings of diffuse alveolar damage, including edema, alveolar epithelial injury and scattered inflammatory cells within the interstitium and alveolar spaces. Chronic beryllium disease was described in fluorescent lamp workers, as well as other beryllium workers and their household contacts. It is also seen in individuals living in areas that surround sites manufacturing beryllium-containing products.
A review and restatement of some problems in histological interpretation of the infant lung johns hopkins erectile dysfunction treatment discount kamagra gold 100 mg online. Longitudinal quantitiation of growth and changes in primary tracheobronchomalacia sites in children erectile dysfunction pump images discount kamagra gold 100 mg buy on-line. The epidemiology of tracheo-oesophageal fistula and oesophageal atresia in Europe erectile dysfunction over 75 buy cheap kamagra gold 100 mg on-line. The absence of clinically significant tracheomalacia in patients having esophageal atresia without tracheoesophageal fistula erectile dysfunction doctor kolkata generic kamagra gold 100 mg buy on line. Prognostic classification for esophageal atresia and tracheoesophageal fistula: Waterston versus Montreal erectile dysfunction treatment patanjali discount 100 mg kamagra gold overnight delivery. Long-term analysis of children with esophageal atresia and tracheoesophageal fistula. Congenital tracheobronchomegaly (Mounier-Kuhn syndrome): a report of 10 cases and review of the literature. Tracheobronchomegaly: report of five cases and demonstration of familial occurrence. Mounier-Kuhn syndrome: report of 8 cases of tracheobronchomegaly with associated complications. Morikawa N, Kuroda T, Honna T, Kitano Y, Fuchimotoa Y, Terawakia K, Kawasakib K, Koinumab G, Matsuokac K, Saekia M. Bronchial atresia: the hidden pathology within a spectrum of prenatally diagnosed lung masses. Tracheobronchial malacia 128 Chapter 3: Congenital abnormalities and pediatric lung diseases, including neoplasms and stenosis in children in intensive care: bronchograms help to predict outcome. Bronchial compression by posteriorly displaced ascending aorta in patients with congenital heart disease. Probable familial congenital bronchiectasis due to cartilage deficiency (Williams-Campbell Syndrome). Cryptorchidism, chest deformities and other congenital anomalies in three brothers. Bronchomalacia occurring in monozygotic twins: further information about its inheritance. Noninvasive treatment of bronchomalacia, successful ventilation of a severely ill infant. A decade of using intraluminal tracheal/bronchial stents in the management of tracheomalacia and/or bronchomalacia: is it better than aortopexy Heterotaxy syndrome: asplenia and polysplenia as indicators of visceral malposition and complex congenital heart disease. Five syndromes (malformation complexes) of pulmonary symmetry, congenital heart disease, and multiple spleens. Ein Hand-und Lehrbuch für Morphologen, Physiologen, Praktische Ärtze und Studierende. Agenesis of the lung: presentation of eight new cases and review of the literature. Agenesis of the lung: report of a case with a review of all previously reported cases. Bilateral agenesis/ aplasia of the lungs: report of a second case in the offspring of one woman. Variation in major pulmonary fissures: incidence in fetal postmortem examinations and a review of significant extrapulmonary structural abnormalities in sixty cases. Horseshoe lung: a case report with unusual bronchial and pleural anomalies and a proposed new classification. Horseshoe lung in association with other foregut anomalies: what is the significance Pulmonary sequestration and related congenital bronchopulmonary-vascular malformations: nomenclature and classification based on anatomical and embryological considerations. Congenital bronchopulmonary vascular malformations: clinical application of a simple anatomical approach in 25 cases. Bronchial atresia is common to extralobar sequestration, intralobar sequestration, congenital cystic adenomatoid malformation and lobar emphysema. Fetal congenital cystic ademomatoid malformations of the lung: a clinical pathologic study of eleven cases. Pulmonary and mediastinal bronchogenic cysts: a clinicopathologic study of 33 cases. Coexistence of bronchial atresia and bronchogenic cyst: diagnostic criteria and embryologic considerations. Subdiaphragmatic bronchogenic cyst with communication to the stomach: a case report. Cutaneous bronchogenic cyst of the back: a case report and review of the literature. Perinatal management of congenital cystic lung lesions in the age of minimally invasive surgery. Congenital cystic adenomatoid malformation: accuracy of prenatal diagnosis, prevalence and outcome in a general population Prenat Diagn 2003;23:997:1002. Cystic adenomatoid malformation of the lung: review of genetics, prenatal diagnosis, and in utero treatment. Outcome of the prenatally diagnosed congenital cystic adenomatoid lung malformation: a Canadian experience. Rhabdomyosarcoma of the lung arising in a congenital adenomatoid malformation Cancer 1977;40:383:8. Bronchioloalveolar carcinoma of the lung and congenital cystic adenomatoid malformation. Bronchioloalveolar carcinoma arising from a congenital cystic adenomatoid malformation in an adolescent: the first case report from the orient. Bronchioloalveolar carcinoma in congenital cystic adenomatoid malformation of lung. Pulmonary congenital cystic adenomatoid malformation as mucinous bronchioloalveolar carcinoma precursors. Congenital pulmonary airway malformation (congenital cystic adenomatoid malformation) with multiple extrapulmonary anomalies: autopsy report of a fetus at 19 weeks of gestation. Prognostic factors associated with congenital cystic adenomatoid malformation of the lung. Successful prenatal management of hydrops, caused by congenital cystic adenomatoid malformation, using serial aspirations. Antenatally suspected congenital cystic adenomatoid malformation of the lung: postnatal investigation and timing of surgery. Congenital cystic adenomatoid malformations may not require surgical intervention. Lower accessory pulmonary artery with intralobular sequestration of lung: a report of seven cases. Congenital bronchopulmonary foregut malformation: pulmonary sequestration communicating with the gastrointestinal tract. Extralobar sequestration with frequently associated congenital cystic adenomatoid malformation, type 2: report of 50 cases. Lobar emphysema, cystic adenomatoid malformation, pulmonary sequestration, and bronchogenic cyst in infancy and childhood: a clinical group. Cystic lung lesions with systemic arterial blod supply: a hybrid of congential cystic adenomatoid malformation and bronchopulmonary sequestration. Congenital lung lesions: classification and concordance of radiological appearance and surgical pathology. Therapeutic embolization of a systemic arterialization of lung without sequestration. Prenatal thoracoabdominal tumor mimicking pulmonary sequestration: a diagnosis dilemma. Systemic arterial supply to the normal basal segments of the left lower lobe treated by coil embolization, with long term follow up. Communicating bronchopulmonary foregut malformations: classification and embryogenesis. Arrest of foregut development in a congenital bronchopulmonary foregut malformation Pediatr Surg Int 1994;9:401:2. Congenital lobar emphysema: the disappearing chest mass: antenatal ultrasound appearance. Congenital lobar emphysema: a case with bronchial atresia and abnormal bronchial cartilage Br J Dis Chest 1982;76:177:84. Congenital lobar emphysema resulting from bronchial sling around a normal right main pulmonary artery. Asynchronous pulmonary hyperplasia associated with tracheal atresia: pathologic and prenatal sonographic findings. Laryngeal atresia or stenosis presenting as second trimester fetal ascites: diagnosis and pathology in three independent cases. Fraser syndrome and cryptopthalmos: review of the diagnostic criteria and evidence for phenotypic mdules in complex malformation syndromes. A case of congenital high airway obstruction syndrome managed by ex utero intrapartum treatment: case report and review of the literature. Congenital pulmonary lymphangiectasis: report of 11 examples with special reference to cardiovascular findings. Autosomal recessive intestinal lymphangiectasis and lymphedema, with facial anomallies and mental retardation. Congenital pulmonary lymphangiectasia presenting as non-immune fetal hydrops and severe respiratory distress at birth: not uniformly fatal. Thoracoscopic stapled resection of multiple esophageal duplication cysts with different pathological findings. Incidence of alveolar capillary dysplasia in severe idiopathic persistent pulmonary hypertension of the newborn. Congenital alveolar dysplasia: an unusual cause of respiratory distress in the newborn. Congenital alveolar capillary dysplasia: a developmental vascular anomaly causing persistent pulmonary hypertension of the newborn. Misalignment of lung vessels: a syndrome causing persistent neonatal pulmonary hypertension. Alveolar capillary dysplasia presenting a pneumothorax: a case report and review of the literature. A rare case of aortic coarctation and ventricular septal defect combined with alveolar capillary dysplasia. Congenital alveolar capillary dysplasia and associated gastrointestinal anomalies. A neonate with coexisting congenital cystic adenomatoid malformation of the lung and alveolar capillary dysplasia: a case report with review of literature. Intralobar sequestration with congenital cystic adenomatous malformation and rhabdomyomatous dysplasia. Rhabdomyomatous dysplasia of the lung: a case report with review of the literature. Rhabdomyomatous dysplasia of the newborn lung associated with multiple congenital malformations of the heart and great vessels. Heterotopic pancreatic tissue presenting as a solid and cystic lung lesion: a very unusual bronchopulmonary foregut malformation. Central nervous system heterotopia in the lung of a fetus with cranial malformation. Embolism of brain tissue in intrapartum and early neonatal deaths: report of 9 cases. The radial alveolar count method of Emery and Mithal: a reappraisal 1: postnatal lung growth. Hypoplasia of medullary arcuate nucleus in unexpected late fetal death (stillborn infants): a pathologic study. Association between pulmonary hypoplasia and hypoplasia of arcuate nucleus in stillbirth. Low amniotic pressure in oligohydramnios: is this the cause of pulmonary hypoplasia A mechanism leading to reduced lung 134 Chapter 3: Congenital abnormalities and pediatric lung diseases, including neoplasms expansion and lung hypoplasia in fetal sheep during oligohydramnios. Fetal breathing and pressures in the trachea and amniotic sac during oligohydramnios in sheep. Fetoscopic temporary tracheal occlusion by means of detachable balloon for congenital diaphragmatic hernia. Pulmonary hypoplasia: lung weight and radial alveolar count as criteria of diagnosis Arch Dis Child 1979;54:614:18. The number of alveoli in the terminal respiratory unit of man during late intrauterine life and childhood. Fetal lung hypoplasia: biochemical and structural variations and their possible significance. Ultrastructural evaluation of type 2 pneumocytes in the hypoplastic lung of rabbit fetuses induced by oligohydramnios. Neonatal pulmonary hypoplasia and perinatal mortality in patients with midtrimester rupture of amniotic membranes: a critical analysis. Becmeur F, Talon I, Schaarschmidt K, Philippe P, Moog R, Kauffmann I, Schultz A, Grandadam S, Toledano D. Outcomes of congenital diaphragmatic hernia: a population based study in Western Australia. Late presentation of Bochdalek-type congenital diaphragmatic hernia in children: a 23 year experience at a single center. The long term follow-up of patients with a congenital diaphragmatic hernia: a broad spectrum of morbidity. Primary ciliary dyskinesia in the paediatric population: range and severity of radiological findings in a cohort of patients receiving tertiary care. Nasal nitric oxide for early diagnosis of primary ciliary dyskinesia: practical issues in children. Non-invasive sampling of nasal cilia for measurement of beat frequency and study of ultrastructure. Functional analysis of cilia and ciliated epithelial ultrastructure in healthy children and young adults.
While 90% of untreated patients die within 2 years impotence foods order 100 mg kamagra gold with mastercard, approximately 80% 8-year survival is noted in cyclophosphamidetreated individuals erectile dysfunction doctors in coimbatore discount kamagra gold 100 mg buy on-line. While age and organ failure are adverse factors zantac causes erectile dysfunction order kamagra gold now, relapses do not affect mortality impotence blood pressure medication buy kamagra gold 100 mg on-line. From 86 to 89% of patients suffer either irreversible vasculitis or therapy-related problems erectile dysfunction doctor lexington ky cheap 100 mg kamagra gold fast delivery. Diffuse pulmonary hemorrhage syndromes in addition to rheumatoid nodules and bronchocentric granulomatosis should also be considered. Lymphomatoid granulomatosis is an Epstein-Barr virusdriven T-cell rich, B-cell lymphoma that often produces necrotic lung nodules and affects the upper respiratory tract, kidney and skin. While it may be angiocentric and angiodestructive, the polymorphous lymphoid infiltrate features malignant cells scattered among reactive lymphocytes (see Chapter 34). Most patients present acutely but symptoms may precede the diagnosis for more than 1 year. In those with pulmonary disease the most frequent systemic findings include fever, myalgia and arthralgia, and weight loss. Fibrin clusters accompany some of the neutrophils and in areas the alveolar wall is obliterated. Depending on the duration of the process, scattered intra-alveolar hemosiderin-laden macrophages can mix with blood. Older lesions often feature polypoid fibroconnective tissue plugs originating in the alveolar walls. In addition, interstitial fibrosis and airway fibrosis with emphysema have been reported. A variety of rare small vessel vasculitides should also be considered in the differential diagnosis. An up to 70% 5-year survival rate is predicated on aggressive steroid, cyclophosphamide and plasmapheresis treatment. Renal biopsies demonstrate necrotizing glomerulonephritis and skin biopsies often feature leukocytoclastic vasculitis. Cytology Bronchoalveolar lavage samples are either macroscopically bloody or contain significant numbers of hemosiderin-laden macrophages. Allergic granulomatosis and angiitis was first described in 1951 by Churg and Strauss and featured patients with severe asthma, blood and tissue eosinophilia, necrotizing vasculitis and extravascular granulomas. In fact, the characteristic "allergic granuloma" is only seen in 10% to 20% of patients. For example, they may be seen in parasitic infections and drug reactions (see Chapters 8 and 16). In fact, one group suggested that a diagnosis could be made on clinical grounds alone in patients with a history of asthma, eosinophilia greater than 1500 cells/ mm3 and clinical/histological vasculitis involving two or more extrapulmonary sites (see Table 8). Microcytic or normocytic anemia may be striking, while serum creatinine levels are elevated. Furthermore, its frequency correlates with vasculitic symptoms rather than those secondary to eosinophilic tissue infiltration. It is satisfying for pathologists to note that the European League Against Rheumatism recommends that histology should be obtained in all cases to assist in diagnosis. However, not all patients have clear-cut stepwise progression as up 732 Chapter 19: Pulmonary vasculitis and pulmonary hemorrhage syndromes Table 10 Churg-Strauss syndrome: main clinical features Asthma Eosinophilia > 10% Sinusitis Lung involvement Peripheral neuropathy Skin involvement Heart involvement Gastrointestinal tract involvement Renal involvement Central nervous system involvement to 20% may have overlapping manifestations from the different phases. Patients are usually in their 30s and the phase can last from 3 to 30 years, although most patients progress within 8 to 10 years. The upper and lower respiratory tracts, heart and gastrointestinal tract are favored sites. Such infiltrates may manifest as Löffler syndrome or chronic eosinophilic pneumonia, eosinophilic gastroenteritis or myocarditis. The third and final phase heralds the appearance of a life-threatening small and medium-sized vasculitis. This phase also features signs and symptoms from the prodromal and eosinophilic phases. The most frequently involved organs are the lungs, peripheral nerves, skin, gastrointestinal tract and heart. Rhinorrhea and nasal polyps are the most common upper respiratory tract manifestations. Mononeuritis multiplex and asymmetric or symmetric sensory or sensorimotor polyneuropathies are more frequent than Guillain-Barré-like syndromes. The common peroneal nerve is most frequently involved, and those with mononeuritis multiplex suffer with motor palsy and sensory deficit including painful hyperesthesia and muscular atrophy. Eosinophilic enteritis involves the small intestine more often than the stomach or colon. Axial chest computed tomogram demonstrates bilateral mainly peripheral ground glass opacities. Myocarditis, coronary artery vasculitis, valvular abnormalities, congestive heart failure and pericarditis are reported. Obstructive uropathy secondary to ureter or prostate involvement are also rare occurrences. Axial chest computed tomogram features multiple lung nodules with ground glass halos (arrows). Parenchymal abnormalities in treated patients resolve more completely than the airway manifestations. Macroscopic pathology Pulmonary hemorrhage or nodules are noted in a small percentage of samples. The arterial media is filled with eosinophils while the intima is starting to collapse. Diagnostic cases feature necrotizing eosinophilic vasculitis, tissue infiltration with eosinophils, and extravascular granulomas. Eosinophils along with lymphocytes, neutrophils, histocytes and even multinucleated giant cells infiltrate small vessel walls. While the entire pulmonary lobule may be involved, vasculitis can be confined to a single compartment, such as the interlobular septa or bronchovascular bundle. Tissue infiltration with eosinophils includes typical airway findings seen in asthma, and/or eosinophilic pneumonia. Bronchial walls are thickened with prominent basement membranes, hypertrophy of submucosal glands and smooth muscle, edema and eosinophils. Extravascular granulomas, also referred to as "allergic granulomas", are distinctive parenchymal lesions. Non-pulmonary organ involvement usually manifests with vasculitis and/or eosinophilic infiltrates. Eosinophilic infiltrates in the upper respiratory tract are seen more often than vasculitis. Parenchymal infiltration with eosinophils, epithelioid histiocytes and multinucleated giant cells (arrow) may lead to hyaline membrane formation. Cytology Bronchoalveolar lavage samples contain many eosinophils, occasional Charcot-Leyden crystals, and perhaps blood. Allergic granulomas, not unlike Wegener granulomatosis, feature geographic necrosis. Serum eosinophil levels fluctuate during the disease and disappear with corticosteroid therapy. While an eosinophil count exceeding 1500/mm3 is one of the diagnostic criteria for disease, mean values range from 4400 to almost 8200. IgE is also elevated at diagnosis in 75% of patients but is nonspecific and usually not seen in those taking steroids for asthma. Interestingly, positive rheumatoid factor is reported in more than half of studied pateints. Parasitic infections, most notably Strongyloides stercoralis and Toxocara canis, present with asthma and systemic illness. Stool and sputum samples should be examined and one should be aware that finding organisms in tissue sections is exceedingly rare. Carbamazine and estrogen may lead to necrotizing granulomatous vasculitis (see Chapter 16). Patient ages range from 10 years to the elderly, with a bimodal distribution featuring incidence peaks at 20 to 30 years and 60 to 70 years. Patients are assessed for cardiac involvement, gastrointestinal disease, renal insufficiency, proteinuria and central nervous system involvement. The reported 5-year mortality rate for patients with none of the factors is 12%, 26% when one factor is present and 46% when three or more are present. Thus, maintenance therapy, corticosteroid-sparing therapies and eosinophil monitoring are very important. Genetics Disease rates are notably higher in siblings, cousins and identical twins. However, since 30% of the nonaffected population have this allele, other factors must exist. Between 60% and 80% of patients have clinical manifestations of both pulmonary and renal disease, between 20% and 40% have only renal disease and less than 10% have disease limited to the lungs. This presentation leads to rapid respiratory failure and is the most common cause of death. Axial chest computed tomogram demonstrates diffuse centrilobular ground-glass nodules secondary to pulmonary hemorrhage. This is secondary to the binding of inhaled carbon dioxide to intraalveolar hemoglobin. Histologically, diffuse alveolar hemorrhage with hemosiderin-laden macrophages is usually accompanied by slight septal widening and occasional neutrophils. Microscopic foci of organizing pneumonia or even hyaline membranes may be noted but convincing vasculitis or phlebitis in areas without hemorrhage should not be seen. Less common manifestations include unilateral or focal opacity and centrilobular nodules. Hemorrhage clears within 10:14 days but with repeated episodes chronic changes of mild fibrosis may occur. Cytology Bronchoalveolar lavage samples may demonstrate blood and numerous hemosiderin-laden macrophages. Capillary walls often contain fibromyxoid connective tissue indicative of prior injury, but neutrophilic capillaritis may not be seen. Tissue injury is caused by antibody binding to reactive epitopes in basement membranes. At these sites the chains are integrated into the membrane in such a way that the lining epitopes are more accessible to circulating antibodies. In addition the subclass distribution is different, with IgG1 present in sera of patients with disease compared to IgG2 in normal sera, suggesting the importance of complement. Since pulmonary hemorrhage is a nonspecific morphological finding, one needs to correlate pathology with clinical and laboratory tests to arrive at the correct diagnosis (see below). Early diagnosis is an important determinant of response to therapy and long-term prognosis. Maintenance immunosuppression is required, which may include rituximab and/or mycophenolate mofetil. This autopsy lung from a patient with systemic lupus erythematosus is overexpanded with blood. Diffuse pulmonary hemorrhage syndromes and capillaritis Diffuse pulmonary hemorrhage is not always associated with vasculitis syndromes. However, those associated with vasculitides almost always feature capillaritis (see above). Capillaritis in the lung has been a controversial phenomenon and is still not accepted by all pathologists. Recognition of capillaritis in other organs is facilitated by the leaking blood and nuclear fragments of neutrophils, which are retained around the blood vessel by encircling collagen. Since pulmonary capillaries lie in interalveolar septa that contain only isolated fibers of collagen, erythrocytes and nuclear dust quickly transit the interstitial space and come to lie principally in the alveolar airspaces. Fibrinoid necrosis of pulmonary capillaries is not usually detectable in light microscopic sections. If larger blood vessels are not also necrotic, the blood might be incorrectly assumed secondary to a bleeding diathesis, or the neutrophils might be incorrectly assumed to be due to an infectious process. Pulmonary capillaritis is a potentially fatal process requiring rapid diagnosis and proper treatment. Bronchoalveolar lavage demonstrates increasingly hemorrhagic samples with serial lavages. If the process is at least 3 days old, hemosiderin-laden macrophages are also noted. Lavage samples must be sent for culture as hemorrhage may be seen in a variety of infections. Although capillaritis can be diagnosed on a transbronchial biopsy, a surgical lung biopsy is the diagnostic gold standard. Periodic acid Schiff stain is often more useful than stains for elastic tissue, reticulin or immunopathological markers for endothelial cells. In cases with impressive hemosiderosis, iron encrustation of arteriolar and venular walls with giant cells may be mistaken for granulomatous vasculitis (see Chapter 2). Many causes are recognized, and correct diagnosis requires a thorough history including drug use and pathology work-up (Table 11). Neutrophilic capillaritis along with intra-alveolar fibrin and scattered histiocytes are noted. The alveolar wall including the capillary is destroyed (arrow) (elastic van Gieson stain). Fibrin balls with hemosiderin are likely to be incorporated into the alveolar wall.
Syndromes
- In Caucasians, lactose intolerance often develops in children older than age 5. In African Americans, the problem can occur as early as age 2.
- Amount swallowed
- If the medication was prescribed for the person
- Unexplained weakness that does not go away
- If the medication was prescribed for the patient
- Social workers
- Endoscopy
From this point onwards mycobacteria have mechanisms that subvert the normal host response how does the erectile dysfunction pump work kamagra gold 100 mg purchase on-line, which leads to bacterial multiplication erectile dysfunction newsletter order kamagra gold 100 mg free shipping. Once ingested erectile dysfunction treatment edmonton discount kamagra gold 100 mg line, the bacteria-containing phagosome is immunologically activated by interferon-g non prescription erectile dysfunction drugs order kamagra gold mastercard, leading to fusion with a lysosome erectile dysfunction information 100 mg kamagra gold otc. Such exposes the organism to a low pH and antibacterial substances (principally reactive oxygen and nitrogen molecules). It is also able to detoxify these host-produced reactive oxygen and nitrogen molecules and to repair the damage caused by these molecules. Frontal chest radiograph of a young adult revealing a massive enlargement of the upper mediastinum and right hilum due to lymphadenopathy. No obvious abnormality other than the hilar lymphadenopathy was noted in the lung parenchyma. Perhaps most importantly, the ability of the mycobacterium to evade the host immune response and to persist within the macrophage. Ingestion of bacteria into macrophages should be the key step to the death and elimination of these bacteria. A very large number of different mechanisms have been identified whereby the mycobacterium might do this. Modulation of antigen processing is one factor in the arrest of phagosome development. The inflammatory lesion within the lung is a dynamic environment containing a variety of protective and regulatory cells. Effector T lymphocytes (purple) mediate control of bacterial growth and the mononuclear composition of the granuloma. Regulatory T lymphocytes (orange) also accumulate in the lesion and limit the ability of the acquired response to stop bacterial growth. Infected phagocytes elaborate cytokines and effector molecules that limit the activity of the lymphocyte response. B cells (blue) accumulate within the lesion in the form of nascent lymphoid follicles; these cells can affect bacterial control and the immunopathologic consequences of infection. Resistance to reactive nitrogen intermediates may be mediated via KatG, a catalase-peroxidase, which can inactivate reactive oxygen, but other genes such as ahpC, glbN and msrA have also been implicated in mycobacterial resistance to such reactive molecules. In addition the mycobacterial proteosome may be able to repair proteins damaged by reactive oxygen and nitrogen molecules. Also, mycobacterial heat shock proteins modify nuclear transcription factors within the macrophage. Ultimately reactive nitrogen intermediates, as well as reactive oxygen intermediates, lysosomal enzymes and toxic peptides are responsible for mycobacterial killing. If the mycobacteria survive, they will multiply until the macrophage bursts and the released organisms are ingested by other macrophages. Activated T cells then return to the site of infection in the lung via the bloodstream. These delayed-type hypersensitivity and cell-mediated immune responses usually contain the mycobacteria within granulomas. Within both the macrophages and the solid caseous centers, organisms are either inactive or replicate very slowly. The granuloma is a well-organized structure, which effectively seals off the mycobacteria from the rest of the host. Liquefaction of the central caseous necrosis creates an inviting extracellular environment for M. The pathogenesis of environmental mycobacterial infection has been little studied. An isolated tuberculoma can be seen in surgical specimens as part of investigation of a single solid lesion. Frequently cavitated lesions are seen in upper zones and vary in size from 1:2 cm to as large as 10 cm. In late-stage disease, most of the inflammation has resolved and has been replaced by fibrosis. These organism-harboring histiocytes are surrounded by varying numbers of lymphocytes, ranging from scattered to a dense lymphocytic "belt". The centers of these granulomas feature striking parenchymal necrosis but granulomas may remain non-necrotizing. This reaction should not be confused with Wegener granulomatosis, where neutrophils are present in the necrotic foci (see below). The cellular response in immunosuppressed/immunocompromised individuals may be decreased and a full granulomatous response may not occur. Vasculitic process in a pulmonary artery branch in a patient with tuberculous consolidation. Well-demarcated non-necrotizing granulomas in a mediastinal lymph node resemble sarcoidosis. Thin, bright red bacilli in an area of caseous necrosis demonstrated with Ziehl-Neelsen stain. After the primary inhalation, a brief acute inflammatory response occurs, followed by a delayed cell-mediated hypersensitivity reaction which leads to the granuloma formation. The Ghon focus is usually subpleural or around fissures and can occur in either lung. Mycobacteria also drain to hilar lymph nodes, which may become enlarged by rapidly established caseous and granulomatous lymphadenitis. The primary pulmonary lesion associated with the regional hilar lymph node granuloma is known as the primary or Ghon complex. In infants, who may not mount a mature immune response, a rapid spread of a primary complex can lead to tuberculous bronchopneumonia, due to erosion of the granulomatous lesion into a bronchus, atelectasis and air trapping. If erosion occurs into a blood vessel, miliary disease, including meningitis, may develop. In extreme cases, tuberculous lymphadenopathy may lead to erosion or perforation of the esophagus by a tracheoesophageal fistula. The average age for tuberculous pleurisy varies among case series but young adults and the elderly appear to be the most affected age groups. This lesion, while not calcified, is longstanding given the focally prominent fibrous capsule. On rare occasions, granulomatous nodules on the pleural surface without parenchymal or nodal association have been described. Secondary pulmonary tuberculosis the usual pathway to secondary pulmonary tuberculosis follows further inhalation of M. Also note the presence of bronchiectasis in the lower segments (bottom left and right). The infectious process has eroded into an airway and involves an adjacent intraparenchymal lymph node. This is an attempt to neutralize and isolate the necrosis from the surrounding lung. A fibrous coat is formed around the area, acting as a physical barrier between the necrosis and adjacent lung tissue. Persistent discharge of caseous debris containing tubercle bacilli can be expectorated in the sputum. The foci of tuberculous pneumonia can vary from small focal lesions to widespread consolidation occupying an entire lobe. Aspirated infectious material can reach terminal bronchioles, resulting in granulomas followed by fibrosis. Thrombosis and infarction are complications of extensive granulomatous vasculitis. If focal lymphatic permeation occurs, a few small tuberculous granulomas may form close to the main lesion. In most cases, there is a slow healing process, and the whole lesion is replaced by fibrosis and eventually calcifies. Especially in endemic areas, this can be complicated further by a chest wall abscess, which in half the cases can involve the ribs. The pleura is thickened, fibrotic and contains characteristic granulomas, often associated with a dense lymphocytic infiltrate. The diagnostic yield of needle biopsy may increase with the guidance of imaging techniques. In some undiagnosed cases, thoracoscopic pleural biopsy may be necessary to obtain diagnostic tissue. The first case reported described post-mortem findings of a renal and pancreatic transplant patient with ill-defined pulmonary spindle cell nodules. This peculiar condition is characterized by tuberculous lymphadenopathy causing bronchial obstruction and atelectasis. While a number of mycobacterial species can present as a typical tuberculous-type granuloma, M. This predominantly spindle cell proliferation from a kidney transplant patient lacks discrete granulomas. This is often associated with disorganized histiocytes, organizing pneumonia or fibrosis. Basal pleurisy is not often evident and only a few cases of environmental mycobacterial pleuritis with effusion have been reported. Association of mycobacterial pseudotumor in mediastinal lymph nodes and simultaneous Kaposi sarcoma has been reported. The predominant species of environmental mycobacteriosis causing the infection, however, varies widely from country to country. It is characterized by non-necrotizing centrilobular and bronchiolocentric granulomas and organizing pneumonia. Clinicopathological correlation the clinical features of tuberculosis are usually due to a combination of systemic features together with local effects at the site of disease. This transbronchial biopsy demonstrates peribronchiolar and interstitial granulomas along with florid mononuclear cell infiltrates and scattered foci of organizing pneumonia. In pulmonary disease cough, sputum production and hemoptysis are caused by the inflammatory response to bacteria in the alveoli and the presence of foreign material within the airways. Breathlessness is not usually a feature unless a very large proportion of the total alveolar space is occupied by inflammatory material. This is the case only in very advanced pulmonary disease, or in the presence of pleural disease with a large pleural effusion causing lung compression. Breathlessness may occur with lesser degrees of alveolar inflammation in those where lung function is already compromised by unrelated chronic lung disease, such as chronic obstructive pulmonary disease. Occasionally breathlessness with wheezing may occur due to bronchial compression by tuberculous involvement of mediastinal lymph nodes and rarely such nodes may rupture into a bronchus, causing cough, expectoration and hemoptysis. Examples of distant hypersensitivity-mediated features are erythema nodosum and uveitis. Fungal infection Several fungal organisms cause necrotizing or non-necrotizing granulomas. Fungi causing pulmonary granulomas include Pneumocystis jiroveci, histoplasma, cryptococcus, blastomyces, coccidioidomyces, South American blastomyces, adiospiromyces and sporothrix (see Chapter 7). Other infections/infestations Rarely bacteria such as Bartonella can cause necrotizing granulomatous inflammation. Cases of extranodal involvement by cat scratch disease tend to occur in immunocompromised patients; however, several cases of pulmonary involvement have been reported in immunocompetent individuals. Cases of congenital pulmonary syphilis usually show numerous spirochetes and the differential diagnosis may not be a problem. Multiple lesions may fuse to form a large solitary lesion with many plasma cells and only a few multinucleated cells. In the absence of bacilli, a number of differential diagnoses should also be considered. Wegener granulomatosis the hallmarks of Wegener granulomatosis are necrotizing pneumonitis, vasculitis and giant cells (see Chapter 19). Elastic-van Gieson and Martius Scarlet Blue stains are often informative in these cases. Serological studies may also aid in the differential diagnosis, especially when renal disease is absent. Ziehl-Neelsen and fungal stains, such as methenamine silver, are advisable in every case of suspected sarcoid. Histologically, sarcoid granulomas are usually non-necrotizing but might feature necrosis and tend to track along the lymphatics in the pleura, interlobular septa and bronchovascular bundles. They can include multinucleated giant cells and these may contain nonspecific inclusion bodies, such as asteroid or Schaumann bodies (see Chapters 2 and 13). In typical sarcoid granulomas, vasculitis may be present involving the adventitia and media but vascular necrosis is not a common feature. Necrotizing sarcoid granulomatosis, as the name suggests, may contain large areas of necrosis along with nonnecrotizing granulomas. The granulomatous process involves bronchioles, as well as blood vessels, and the vasculitic component may sometimes be prominent. Churg-Strauss syndrome Churg-Strauss syndrome is a rare systemic condition seen in asthmatics and may affect the lung (see Chapter 19). Microscopic features can be variable but include necrotizing, granulomatous inflammation with palisading histiocytes and vasculitis. Differential diagnosis can sometimes be difficult due to overlapping features, which also include the eosinophilic infiltrate. Bronchocentric granulomatosis this disease is usually associated with allergic bronchopulmonary fungal disease in asthmatics (see Chapter 15). Infectious 221 Chapter 6: Pulmonary mycobacterial infections processes of other etiologies, including tuberculosis, may present with bronchocentric granulomas. Rheumatoid nodule Pulmonary rheumatoid nodules are identical to those in the subcutaneous tissue and are composed of palisading histiocytes arranged around central areas of necrosis with or without vasculitis (see Chapters 14 and 21). Foreign-body-type cells from aspiration Organic or non-organic aspirated material triggers an inflammatory reaction, which may vary substantially in intensity but is usually associated with a foreign-body-type multinucleated giant cell reaction. Identification of the foreign-body material is also helpful in the differential diagnosis (see Chapter 17).
Discount 100 mg kamagra gold with visa. Mechanisms of Vascular Dysfunction in Diabetes (Joshua A. Beckman MD) Feb 23 2017.
References
- Goldblatt H, Lynch J, Hanzal RF, et al: Studies on experimental hypertension: I. The production of persistent elevation of systolic blood pressure by means of renal ischemia, J Exp Med 59:347n379, 1934.
- Yau P, Watson D, Ascott N, et al: Efficacy of a 90 degree anterior fundoplication vs a total fundoplication in an experimental model. Surg Endosc 14:830, 2000.
- Mannucci PM: Hemophilia and related bleeding disorders: A story of dismay and success. (Lectures), Hematology 1, 2002.
- Jensen A, Sharif H, Olsen J, et al. Risk of breast cancer and gynecologic cancers in a large population of nearly 50,000 infertile Danish women. Am J Epidemiol 2009; 168:49-57.