
Lamisil
| Contato
Página Inicial
J. David Frank, MBBS, FRCS
- Former Consultant Paediatric Urologist,
- Bristol Urological Institute, Southmead Hospital
- Bristol, United Kingdom
Finally fungus gnats natural insecticide lamisil 250 mg buy on line, as prognostic and predictive biomarkers become validated in clinical practice antifungal for nails lamisil 250 mg purchase online, the management of oropharyngeal cancers will hopefully become more individualized fungus underarm order 250 mg lamisil mastercard. Posterior and lateral boundaries are formed by the muscular pharyngeal wall (superior and middle constrictors) fungus species order generic lamisil online. The superior extent is the level of the soft palate (some define this as the level of the hard palate) antifungal oral rinse 250 mg lamisil purchase overnight delivery. The oropharynx is further subdivided into five areas, which include the lateral pharyngeal walls, tonsillar regions, posterior wall, base of the tongue, and soft palate. Additionally, the pharynx consists of six major muscles, the superior pharyngeal constrictor, middle pharyngeal constrictor, inferior pharyngeal constrictor, stylopharyngeus, salpingopharyngeus, and palatopharyngeus. Cancer arising in the oropharynx can extend laterally or posteriorly to involve the parapharyngeal or retropharyngeal spaces, respectively. The posterior pharyngeal wall begins at the Passavant ridge of the superior constrictor. The layers of the posterior pharyngeal wall are critical to the understanding of the spread of cancer in this area and include mucosa, submucosa, superior constrictor, pharyngobasilar fascia, and prevertebral fascia. The pharyngobasilar fascia is a natural barrier to the spread of cancer and is separated from the prevertebral fascia by areolar tissue. Posterior extension of cancer through the muscles and into the pharyngobasilar fascia, but not the prevertebral fascia, can still allow a complete surgical resection with clear margins. The base of the tongue extends from the circumvallate papillae to the vallecula at the base of the epiglottis and encompasses the glossoepiglottic and pharyngoepiglottic folds. Superiorly and laterally, the base of the tongue extends to the glossopalatine sulcus and the glossopharyngeal folds inferiorly and laterally. The pharyngeal branch arises prior to the glossopharyngeal nerve traveling intimately with the stylopharyngeus muscle. The pharyngeal branch then merges with the pharyngeal branch of the vagus nerve (cranial nerve X), which then proceeds to the pharyngeal plexus located within the external fascia of the pharynx. Although the pharyngeal branch provides most of the sensory innervation, the tonsillar branch of the glossopharyngeal nerve directly supplies the oropharyngeal isthmus as it communicates with the lesser palatine nerve (from cranial nerve V2). The soft palate receives its innervation from the lesser palatine branch of the maxillary nerve. The six major muscles of the pharynx all derive motor input from pharyngeal and superior laryngeal branches of the vagus nerve (cranial nerve X) through the pharyngeal plexus, except the stylopharyngeus. The superior aspect of the pharynx receives blood from the pharyngeal branch of the ascending pharyngeal artery and descending branches of the lesser palatine arteries. The inferior aspect of the pharynx receives blood supply from the inferior thyroid artery and superior thyroid artery. The rest of the pharynx receives blood from the ascending palatine and tonsillar branches of the facial artery as well as from the maxillary artery. The internal carotid artery, which is an essential surgical landmark, lies deep to the superior constrictor muscles and medial to the medial pterygoid muscle. Lymphatics the lymphatic drainage of the oropharynx varies greatly across the different subsites, but the two lymph node basins most frequently involved are the internal jugular nodes and the retropharyngeal nodes. The base of the tongue has both superficial and deep lymphatic networks that are bilateral in up to 30% of patients. The soft palate has three distinct drainage systems, anterior, middle, and posterior. The anterior system drains primarily the hard palate and the anterior aspect of soft palate and involves the level I lymph nodes. The posterior system can also drain bilaterally to the retropharyngeal nodes via penetration of the lymphatics through the superior constrictor muscles. Furthermore, in order to maintain a malignant phenotype, a transcriptionally active viral genome appears to be necessary. Disruption of the viral genome also dissociates viral early (E) gene transcription from the viral early polyadenylation signal, leading to use of host poly(A) signals and transcription of virushost fusion transcripts with a longer half-life. These events lead to increased levels of E6 and E7 proteins, which, together with loss of additional inhibitory effects of E2, result in cellular immortalization, deregulated proliferation, and increased genomic instability. More rarely, concatemeric integrants are observed, where viral copies (including intact E2) are arranged in a head-to-tail fashion with partially deleted copies at the 5 and 3 ends. Integration of high-risk human papillomavirus: a key event in cervical carcinogenesis Viral integration is a consequence of an overall destabilization process of the chromosomal integrity in replicating epithelial cells that express the viral E6 and E7 genes. B: Projected annual number of patients with oropharyngeal, oral cavity, laryngeal, and other pharynx cancers through the year 2030. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer-systematic review and meta-analysis of trends by time and region. The recommendation was updated in 2011 that boys aged 11 or 12 years should also be vaccinated with three shots. The posterior pharyngeal wall, which begins at Passavant ridge, transitions from ciliated respiratory epithelium of the nasopharynx to nonkeratinizing stratified squamous epithelium of the oropharynx. The lymphoepithelium of Waldeyer ring is formed by the fusion of the overlying stratified squamous epithelium that extends into the deep tonsillar crypts within the underlying lymphoid tissue. Tumors of this histology tend to arise in older patients with a history of tobacco and alcohol abuse. The presence of intracellular and extracellular keratin is common, and the cells are large and have the characteristic intracellular bridges. This cancer has a propensity for submucosal spread with central ulceration and is composed of tightly packed moderately pleomorphic cells that form cords and nests. Patients typically present with late-stage disease including regional and distant metastases. These cancers will stain for both epithelial markers including keratin and mesenchymal markers including vimentin. Cancer cells are typically surrounded by lymphocytes and have large vesicled nuclei that are positive for cytokeratin. The unique histologic features include lesions that arise from the tonsillar crypts without associated dysplasia of the epithelial surface. Additionally, these cancers exhibit lobular growth and are infiltrated with lymphocytes. Finally, the cells lack significant keratinization and demonstrate a prominent "basaloid" morphology. First, these cancers are frequently described as poorly differentiated based on immature appearance of the cells, when in fact these cells closely resemble the reticulated epithelium of the tonsillar crypts and are actually highly differentiated. There are conflicting data as to which neoplasm is actually the most frequent, but a recent series that focused on minor salivary gland malignancies of the oropharynx identified mucoepidermoid carcinomas as the most frequent, followed by adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and carcinoma ex-pleomorphic adenoma. Physical Examination A complete examination of the head and neck should be performed on all patients. In addition to inspection of the mucosal surfaces, the tonsils and base of the tongue must be palpated to assess the extent of the tumor and for any submucosal spread. Moreover, the extent of the lesion into the deep tissues of the base of the tongue, vallecula, and glossopharyngeal sulcus is often only evident upon palpation. Assessment of the mandible range of motion and a thorough examination of the cranial nerves also must be performed, with an emphasis on sensation of the lower face and tongue, along with mobility of the tongue and palate. Cranial nerve deficits or the presence of trismus implies local invasion into the mandible or masticator spaces. All levels of the neck must be evaluated bilaterally, given the rich lymphatic network that drains the oropharynx and the high incidence of metastasis to the cervical lymph nodes. Examination of the oropharynx through direct transoral visualization (A) or flexible nasopharyngoscopy (BD). They are primarily indicated in the assessment of advanced-stage cancers where there is concern for involvement of the mandible, parapharyngeal space, prevertebral fascia, cervical nodes, or retropharyngeal nodes. Chest radiograph is useful as a screening for metastasis to the lungs, second primary cancers, and chronic changes associated with the use of tobacco. The optimum timing after chemotherapy and radiation therapy is not known, but an interval of 12 weeks has generally been recommended to allow for a reduction in the radiation-induced inflammation and therefore improve the accuracy of the test. Staging Endoscopy and Biopsy Patients with primary epithelial cancers of the upper aerodigestive tract should undergo examination under anesthesia independent of the presenting T stage. Direct visualization and palpation of the tumor improve the assessment of submucosal spread and invasion of surrounding structures, especially in patients presenting with trismus. A thorough examination using direct laryngoscopy for a synchronous second primary cancer is essential, as these lesions can occur in 8% to 12% of patients with history of tobacco use. Approximately 2% to 9% of patients who have cancer of the oropharynx will initially present with cervical lymphadenopathy with an unknown primary. Bilateral tonsillectomy is merited in these cases because of a 10% rate of contralateral spread from occult tonsil lesions. Disruption of this pathway leads to an upregulation of p16 expression that can be detected by immunohistochemistry. Therefore, the goal of treatment is to not only achieve an oncologic cure but also preserve the multimodal function of the oropharynx. Traditional surgical approaches to the oropharynx are associated with significant morbidity, which prompted a shift toward nonsurgical modalities in the 1990s, specifically using radiation or chemoradiation, which have been the mainstay therapeutic approaches for the past 15 to 20 years. Although the oncologic results for radiation-based therapies have been shown to be equivalent to traditional surgical approaches, the short-term and long-term sequelae can significantly impact quality of life. These transoral approaches potentially allow for the adjuvant therapy to be modified based on the pathological findings of the resection specimen. This novel paradigm can reduce the radiation doses and may theoretically decrease the long-term side effects. The lateral pharyngotomy, originally described by Trotter in 1920, requires resection of the mandible, hypoglossal nerve, and lingual artery in order to achieve adequate visualization of the resection margins. Since that time, the technique has been modified in an effort to preserve these vital structures. The tendon of the digastric muscle is then divided exposing the stylohyoid and mylohyoid muscles, which are subsequently released from the hyoid at their insertion. The hypoglossal nerve and lingual artery, the two most important structures, are then isolated. At this point, the extent of parapharyngeal space involvement can be accurately assessed, and the ascending pharyngeal artery can be identified and ligated to allow the posterior belly of the digastric muscle, the stylohyoid muscle, and external carotid artery system to be retracted and rotated. The point of entry into the pharynx is determined by the location of the tumor and most frequently is at the level of the vallecula. Alternatively, the pharyngotomy can be performed more superiorly in the oropharynx at the level of the tonsillar region, but this requires transection of the styloglossus muscle. If the tumor extends to the vallecula, a third entry point is at the ipsilateral piriform sinus. Once the pharyngotomy is performed, the incised mucosa is retracted superiorly to allow adequate visualization of the lesion and circumferential margins, and the cancer is resected en bloc. For smaller defects, mobilization of the posterior wall of the pharynx from the prevertebral fascia can facilitate primary closure. In the cases of larger defects, a microvascular free tissue transfer is the preferred method for anatomic restoration for optimal speech and swallowing outcomes. Additionally, extensive involvement of the parapharyngeal space, invasion of the nasopharynx, or involvement of more than half of the base of the tongue are considered contraindications. Once the neck dissection is completed, the suprahyoid muscles are transected 5 mm above the hyoid bone. The hypoglossal nerves are identified near the greater cornu of the hyoid bilaterally and preserved along with the superior laryngeal nerves and the lingual arteries. The preepiglottic space is then identified, and dissection is carried down to the vallecula. The pharyngotomy is facilitated by placing a retractor through the mouth into the vallecula, and the pharynx is entered at this level through the vallecula. The mucosal edge is retracted superiorly to allow visualization of the base of the tongue and the cancer. In most cases, the wound can be closed primarily by suturing the mucosa of the base of the tongue to the vallecula. The remaining wound is closed in layers by reapproximating the musculature of the base of the tongue to the periosteum of the hyoid and the suprahyoid musculature to the cuff of muscle left on the hyoid. Ideal lesions for this approach are those that are confined to the base of the tongue, although cancers that extend laterally can be addressed with combination of suprahyoid and lateral pharyngotomy approaches. Contraindications to this approach include extension of the cancer to the circumvallate papillae, as the defect would be difficult to close primarily and the exposure is poor, and involvement of the epiglottis or larynx, as laryngeal resection would also be required. Mandibulotomy with paralingual extension into the floor of mouth provides excellent exposure to the tonsillar fossa, soft palate, and the base of the tongue. The mandibulotomy can be performed either in the midline or paramedially, between the lateral incisor and canine tooth. Lateral mandibulotomy is not recommended because the dynamic forces on the mandible are not symmetric, and intermaxillary fixation may be necessary to maintain appropriate occlusion. Additionally, the lateral mandibulotomy site is routinely within the radiation fields, which may lead to problems with wound healing and potentially osteoradionecrosis. A paramedian mandibulotomy offers the advantages of a median mandibulotomy and avoids the transection of the genioglossus muscles. The skin incision is made from the lower lip to the hyoid bone, and a curvilinear extension can be used to include a neck dissection. The skin, subcutaneous tissue, and lip musculature are incised until the mandible is exposed. The paramedian mandibulotomy is performed through the socket of the extracted lateral incisor juxtaposed to the canine, after the mandible is preplated. Following transection of the mandible, the two segments are retracted laterally, and the mucosal incisions are made in the floor of mouth. In order to facilitate closure, a 6- to 8-mm cuff of mucosa should be left attached to the lingual gingiva. The mucosal incision can be extended to the retromolar trigone or into the vallecula if exposure to the base of the tongue is necessary.
Unfortunately fungus gnats coffee grounds discount lamisil 250 mg on line, what constitutes an adequate margin to insure the removal of microscopic extension remains controversial antifungal nail cream buy discount lamisil line. Detailed studies comparing the adequacy of various margin sizes during excision of cancer of the lip have not been performed anti fungal anti bacterial shampoo discount lamisil 250 mg buy on-line. Even when such margins are maintained definition of fungus purchase discount lamisil on-line, studies show that up to a 13% risk remains and that the final surgical specimen will display positive margins fungus plague inc safe lamisil 250 mg. Intraoperative frozen sections of the mental or infraorbital nerve may also be necessary. If cancer cells are present at the infraorbital foramen, segmental resection of the maxillary bone may be indicated. The revised distal nerve stump is then biopsied to determine if further resection and/or other treatments are needed. Treatment of cancer, which encroaches on the alveolar process or the outer cortex of the mandible, should include a marginal mandibulectomy. Management of the Neck the management of regional lymph nodes in patients with cancer of the lip currently remains controversial. The management of regional lymph nodes in patients with lip carcinoma, therefore, requires a thorough understanding of the patterns of lymphatic drainage system for comprehensive tumor assessment and effective treatment planning. Cervical metastasis from both the upper and lower lips occurs in a predictive orderly fashion. Cancers occurring in the upper lip metastasize first to the preauricular or infraparotid lymph nodes, followed by the submandibular nodes. Cancers of the lower lip tend to spread to the submental and submandibular nodes first, followed by the upper deep cervical nodes. Due to embryologic fusion planes, contralateral or bilateral metastases may develop in patients with lower lip cancers. In patients with clinically palpable metastatic lymph nodes, cervical lymphadenectomy is appropriate. When metastasis is present in the parotid lymph nodes, a parotidectomy, with preservation of the facial nerve, should be done in conjunction with neck dissection. Ipsilateral neck dissection is sufficient if postoperative radiation is planned, to include the contralateral N0 neck. Such a strategy preserves the contralateral facial artery, which in turn will improve blood supply to local reconstructive flaps. Generally accepted medical practice at this time dictates that neck dissection should be undertaken in oral cancers carrying a significant risk for occult cervical metastasis. On the other hand, T1 lesions carry a metastases rate of only 5%,11 and therefore, neck dissection might not be mandated in the absence of other features. The presence of such aggressive features such as recurrence, perineural invasion, and poorly differentiated histology requires evaluation and consideration before a decision not to perform a neck decision is made. Bilateral supraomohyoid dissection should be considered when highrisk tumors involve the central portion of the lower lip. The functional and cosmetic consequences of supraomohyoid dissection can be kept to a minimum. If bilateral metastases are found, full bilateral neck dissection is indicated, normally with an attempt to preserve the internal jugular vein on at least one side. With cancer of the upper lip, an ipsilateral dissection of the superficial or lateral lobe of the parotid gland may also be indicated. Adjuvant radiotherapy has been used for elective treatment of the neck in selected high-risk patients. It should not, however, be considered a replacement for neck dissection because 54% of patients treated prophylactically with neck radiotherapy will go on to develop neck metastases within 2 years of treatment. Patients with large or poorly differentiated lip cancers are most likely the ones to benefit from this technique. Recurrence at distant sites is extremely rare once the primary has been locally and regionally controlled. Local recurrence of cancer of the lip following initial treatment with surgery or radiation ranges from ~5% to 25% overall and is the most common form of treatment failure. As would be expected, the rate of local recurrence tends to increase proportionately with the size of the original cancer. The specific involved subsite has been associated with varied chances for local recurrence. The highest incidence has been noted with cancer of the commissure, and the lowest with cancer of the lower lip. Recurrence of cancer of the lip is best managed with aggressive surgical resection, incorporating the use of intraoperative margin assessment to assure complete clearance of the tumor. Because up to one-fourth of patients presenting with cancer of the lip will present with subsequent cervical lymph node metastases, strong consideration to elective neck dissection should be considered. Except in cases of bone involvement, local recurrences of cancer of the lip should not be expected in 60% to 85% of cases where appropriate surgical management techniques have been employed. Regardless, the goals of reconstruction remain to restore oral competence, maintain oral opening, and achieve an aesthetic result that approaches normal appearance. For adequate function of the lip, it is best if continuity of the orbicularis muscle sphincter can be restored in some fashion, particularly in the lower lip. Aesthetically, it is best if all incisions can be placed along the peripheral borders of the lip unit (mental and melolabial creases) or parallel with the lines of relaxed skin tension of the lips. When approaching reconstruction of the lip, one should first assess the lesion and attempt to determine the amount of mucosa, muscle, and skin that will be required. Accurate assessment of three-dimensional tissue loss and required volume for reconstruction is paramount to the success of reconstruction of the lip. The effect of lip defects upon facial appearance will be exaggerated as a result of the displacement of wound edges by the lateral pull of the facial muscles. These defects can be divided into vermilion-only defects, defects that involve less than one-third of the total lip length, defects that involve between one- and two-thirds of the total length of the lip, and finally total lip defects. Defects isolated to the vermilion may be approached with healing by secondary intention, direct primary wound closure, and mucosal advancement flaps. Healing by secondary intention is appropriate for small superficial defects confined to the vermilion. Small defects, which do not distort the remaining vermilion or lip contour, are amenable to primary closure, although this technique may lead to unsightly bunching of the remaining vermilion. More commonly, the resulting defect is large enough to require an advancement flap of the labial mucosa. Dissection for this flap is done in the submucosal plane toward the gingival buccal sulcus. Two back cuts at each commissure toward the gingival buccal may be required to facilitate advancement. Neural and vascular connections can be preserved and stretched forward with the advancing flap, optimizing sensory function for the restored vermilion. Occasionally, the mucosal flap is of insufficient bulk to accomplish a desired result. In such cases, a pedicled orbicularis oris can be rotated into the base of the defect to improve cosmesis. Generally, defects involving less than one-third of the horizontal length of the lip can be closed primarily. The lip lends itself well to primary closure due to its remarkable tolerance for stretching. The long axis of either closure should be oriented parallel with relaxed skin tension lines leading to a more obliquely oriented flap in the lateral portions of the lip. M-plasty is often helpful to allow avoidance of crossing subunit borders and prevent alar or vermilion distortion. For fullthickness defects, the mucosa is reapproximated first, followed by the muscle layer, and finally the skin, with an emphasis on precise reapproximation of the vermillion. Reestablishment of the vermilion border is essential because even minute misalignment is easily recognizable. Defects involving less than one-third of the horizontal length can be closed primarily. The cheeks and, less commonly, the chin are the natural sites to obtain additional tissue for lip reconstruction. A large variety of techniques have been described that transfer tissue from these areas into the lip. The most commonly chosen method involves transposition of skin and subcutaneous tissue from the melolabial fold, using a pedicle that is either superiorly or inferiorly based. The melolabial flap is designed so that the donor site, as it is closed, is well hidden within the melolabial crease. The use of a superiorly based pedicle tends to cause greater cosmetic detraction because it disrupts the medial portion of the melolabial crease-a situation that can be improved later by placing an incision across the pedicle in a fashion that restores the full line of the crease. It is not capable of truly restoring the orbicularis muscle but rather relies on a certain degree of tightness. Surfacing for the underside of these flaps may be done either with a second flap, including the skin or oral mucosa, or with application of a graft of skin or mucosa. A skin graft can be buried beneath the cheek flap in a "delayed" fashion for 2 to 3 weeks, allowing the combined tissues to be later transferred as a composite. Defects greater than one-third, but less than two-thirds of the horizontal lip, are ideally reconstructed with pedicled or tissue flap rotated from the opposing lip. The majority of the reconstructions of this size are achieved with the aid of an Abbe cross-lip flap, an Estlander cross-lip flap, or a Karapandzic flap. Both Abbe and Estlander flaps use full-thickness tissue transferred from opposing lips pedicled on the labial artery. They differ in that the Abbe flap is used for defects medial to the oral commissure. This technique typically results in blunting of the commissure angle and may require a commissuroplasty at a later date. B: Full-thickness incisions performed while maintaining a small pedicle, which contains the labial artery; C: Donor flap rotated to the upper lip. B: Defect involving the lateral third of the lip is shown with designed Estlander flap. C: Tissue from the upper lip rotated inferiorly while maintaining small pedicle containing the labial artery. Traditionally, both flaps are designed with the same height as the defect and half the width. This results in a decrease in length of the donating lip, proportional to the increase of the received lip. It is particularly important to ensure that the full vertical height of the defect is replaced with the transposed tissue. Asymmetry of the horizontal length is easily overlooked, but even minor elevations in vertical height draws attention. Although originally described with a wedge shape, cross-lip flaps may be also designed in a rectangular or M shape when desired. Both Abbe and Estlander flaps also lend well to combinations with other forms of reconstruction, and multiple cross-lip flaps may be used simultaneously. The biggest drawback to the use of cross-lip flaps is the total denervation that occurs as they are transferred; however, some motor and sensory function will generally redevelop over the course of several months to a year. The Karapandzic flap is a circumoral advancement technique that preserves the vascularity, sensation, and the function of the remaining orbicularis oris muscle. As the incisions approach the vicinity of the oral commissure, however, the Karapandzic flap should be extended out to the surrounding cheek because the melolabial crease closely approximates the commissure. The integrity of the neurovascular supply and muscle fibers of the orbicularis oris muscle is thereby preserved, which results in good functional and aesthetic outcomes. However, the degree of resulting microstomia created can be limiting, especially in patients who wear dentures. B: Full-thickness defect following resection of the tumor with planned circumoral rotation. Preservation of muscle fibers and neurovascular supply while performing Karapandzic flap. In the mid-19th century, Bernard and von Burow separately described a method for reconstruction of full-thickness defects, which are larger than two-third of the lip. It involves direct medial advancement of tissue from the cheeks, which is facilitated by removal of strategically placed triangles of skin that allow for a more even redistribution of the facial tissues. Overall functional and cosmetic results with this reconstruction are typically only fair because satisfactory restoration of the orbicularis sphincter is often difficult to achieve. Several modifications of the Bernard cheiloplasty have been described in attempt to produce more favorable scars and better muscle function. The excised triangles are partial thickness only, thereby preserving the neurovascular supply to the orbicularis oris and buccinators muscles. This technique can be used to restore near-total loss of the lip and may be adapted for reconstruction of either the upper or the lower lip. This flap uses incisions placed within the alar crease and includes the removal of crescent-shaped areas of cheek tissue adjacent to the alae. This prevents deformity of the alar base, lip, and oral commissure by preserving the alar crease. The perialar crescentic advancement flap works well for defects of the upper cutaneous lip, especially those located immediately inferior to the nasal sill. Lesions involving greater than two-thirds of the lower lip benefit from reconstructions using modifications of the Bernard cheiloplasty. The perialar crescentic advancement flap is best suited for defects of the upper cutaneous lip. B: Central-thickness incisions and subcutaneous flaps elevated to preserve neurovascular supply. Not only do the internal and external lining have to be replaced, but oral competence needs to be restored. In such cases, the rotation of large amounts of local tissues may lead to further facial disfigurement, and microstomia.
Prolactin stimulates integrin-mediated adhesion of circulating mononuclear cells to endothelial cells fungus won't go away 250 mg lamisil purchase visa. From Reproductive Neuroendocrinology and Lactation to Vasoinhibins 261 Moreno-Carranza anti fungal wall paint purchase discount lamisil on line, B fungus gnats houseplants get rid cheap 250 mg lamisil visa. Expression of prolactin gene and secretion of prolactin by rat retinal capillary endothelial cells fungal nail salon buy discount lamisil 250 mg on line. Changes in the expression of neurohypophyseal prolactins during the estrus cycle and after estrogen treatment antifungal yeast effective lamisil 250 mg. A 14 kDa prolactin-like fragment is secreted from the hypothalamo-neurohypophyseal system of the rat. Prolactin promotes oxytocin and vasopressin release by activating neuronal nitric oxide synthase in the supraoptic and paraventricular nuclei. Thus, there is an imperative to attend to the causes and treatment of this disease. Although there are therapies that inhibit progression of the disease, they fail to eradicate it. Relapse after controlling the progression can occur, accompanied by more aggressive cell growth that is often fatal. The innervation of the prostate may also play a significant role in the control of the prostate. We also address evidence of morphological changes in the major pelvic ganglion in males related to sexual experience, and how this may affect the prostate. In the rat, the prostate is mainly divided into two ventral lobes the same size as the empty bladder, two lateral lobes, and one dorsal lobe. In the rat, the prostate is also located caudal to the bladder, but in the rat, prostatic ducts only converge on the urethra (Ahmed et al. Neuroendocrine and Molecular Aspects of the Prostate 265 of such gland in females was first reported by Reiner de Graaf in 1672, but not named until 1880 by Alexander J. This female prostate comprises clusters of alveoli and ducts embedded in a fibromuscular stroma, although compared to the male prostate, it is poorly developed. Simple epithelial cells constitute the prostate alveoli and they produce the glandular fluid. A second type of epithelium forms the prostatic ducts, which contain smooth muscle, the contraction of which expels the prostatic fluid into the prostatic urethra. A feature of the epithelial cells comprising the alveoli is their internal organization: they show a polarity in the cytoplasm, in which the nucleus is typically located in the basal region close to the prostatic stroma, while the endoplasmic reticulum and Golgi apparatus are situated close to the lumina (Maslova et al. This organization enables components of the prostatic fluid to be evacuated into the alveolar luminae. The prostatic fluid contains carnitine, phospholipids, citric acid, calcium ions, sodium, zinc, high levels of glucose (Kuosa et al. The latter two promote the release of sperm from the coagulated ejaculate, which enables fertilization (Golan et al. In the female, the epithelium of the alveolus contains distinct basal proliferating, intermediate, and secretory cells. More detailed studies report that the secretory glands of the female prostate have merocrine secretion (secretory vacuoles and granules) and apocrine secretion (apical "buds" that enter the lumen) (Zaviacic et al. The composition of this secretion is similar to that found in the male prostate; for that reason, it is speculated that it promotes egg fertilization (Biancardi et al. Also reported are an abundant stroma, and high levels of collagen and elastin fibers associated with smooth muscle cells and fibroblasts. Despite being a small organ, physiologically, the female prostate seems to be active because the secretory products are discharged into the ducts in response to sexual events (Zaviacic et al. Perhaps the prostate gland is rudimentary in females as a result of the absence of testosterone during embryonic and neonatal periods (Biancardi et al. Under these conditions, a developed female prostate is observed 266 Behavioral Neuroendocrinology having two ventral lobes similar of the ventral lobes of the male prostate, and histologically, it contains columnar epithelial cells, which are more active in the presence of testosterone (Biancardi et al. This metabolite is 5 to 10 times more active than testosterone itself because it forms a more stable complex with the androgen receptor (Ekman 2000). When the hormone is given to castrated animals, the parameters return to levels similar to those observed in normal tissue (Wright et al. Clearly, the prostate gland is dependent on the presence of androgens to maintain its weight and adequate functioning, but with the inherent risk of hormonal dysfunction, which can lead to prostate disease. However, as they have a high level of expression they are used as markers of activity of the different lobes of the prostate (Reiter et al. The two types of receptors differ in the signaling pathways triggered and the regulatory mechanisms involved. This process provides a higher production rate and semen quality that promotes both the survival of sperm and egg fertilization (Sofikitis and Miyagawa 1993; Soto-Cid et al. The main nerves known to regulate the prostate are the Pelvic nerve (PvN) and the Hypogastric Nerve (HgN), which emerge from the thoracic, lumbar, and sacral segments of the spinal cord. The PvN originates from the L6-S1 segments forming a trunk; the HgN fibers originate from the T12 and L6 segments, converging in the mesenteric ganglion and emerging as the HgN. Both nerves converge in the major pelvic ganglion, and then distribute to the pelvic area including the prostate gland (Wang et al. There are also structural changes in the pelvic ganglion that are related to sexual experience (White et al. The ganglion from male rats that experienced sexual activity is more highly organized and has a greater number of satellite cells that surround, or are near, the ganglion cells, than the ganglion of sexually inactive males, that despite being in the presence of a receptive female showed low, or no, interest in courtship or copulation. Perhaps these effects are due to low testosterone production, the decline in androgen receptor expression in the ganglion or low synthesis of the survival neurotrophic factor, neurturin (Yan and Keast 2008; Yan et al. The organization and development of the ganglion depends on the presence of androgens (Melvin and Hamill 1989; Keast 1999), and the HgN and PvN are involved in the secretory functions of the prostatic fluid by inducing the contraction of the smooth muscle that surrounds epithelial cells and ducts that converge in the prostatic urethra (Bruschini et al. It is important to recognize that neurotransmitters and neuromodulators are also related to other functions, such as cell proliferation, repair of nerve tissue, neural network "training" with neurotrophic factors, and regulation of synaptic transmission; all of these impact the functioning of the pelvic ganglion and thereby the prostate gland (Calenda et al. A possible basis for this difference is the lack of control in the medial preoptic area where this behavior pattern is regulated. As this pathology progresses, it becomes difficult to identify individual epithelial cells, leading to a phase of metaplasia, and over time, these changes develop into prostatic dysplasia (Herrera-Covarrubias et al. Histologically, metaplasia corresponds to a mature epithelium that resembles the normal tissue but with a characteristic mitotically active area, and can be considered as the origin for the generation of dysplastic cells with the potential of malignancy. This is the early stage of development that can be transformed, over time, into neoplasia. For this reason, dysplasia is considered a preneoplastic or precancerous stage (HerreraCovarrubias et al. While the neoplasia remains in situ, it is considered benign, but when it spreads outside the limits of the tissue, it is considered malignant (Van Cleef et al. While the roles of each of the signaling pathways and the significance of trimethylation of the p53 gene are not well understood, they all converge on two processes-increased cell proliferation and decreased apoptosis. Thus, pathologies of the prostate are at least the result of the participation of several signaling pathways in response to hormonal activation. The female prostate is also susceptible to disease, for example, ductal infections and abscesses that are prevalent in childhood and puberty (Nickles et al. Prostatic disease is also associated with age in women and female rodents (Pongtippan et al. Because few studies have been conducted with the female prostate, at present, the etiology and possible role of hormones in female prostatic disease is not known. While these findings are suggestive of a correlation between hormonal levels and female prostatic pathology, further research is required. Evidently, both neural and hormonal mechanisms respond to sexual activity and can affect the prostate, even to the extent of inducing prostate pathology. It is possible that alteration of behavioral events, and the hormonal and autonomic concomitants, or axotomy, can produce prostatic pathology, for example, hyperplasia, metaplasia, or dysplasia via their effects on the structure of the pelvic ganglion and/or prostatic hormone receptors. Further research is required to ascertain the relative contributions of specific neural and endocrine factors to the healthy physiology and pathology of the prostate in females as well as in males. Carlos Beyer, his wisdom in the use of simple methodologies to answer complicated scientific questions had a major impact on us as students and now as researchers. Phosphorylation of the alpha(1) subunit of L-type, voltage-dependent calcium channels. Influencia de la prolactina y las hormonas sexuales esteroideas sobre la morfología e histología prostática en la rata. Investigación, Instituto de Neuroetología, Universidad Veracruzana, Xalapa, Veracruz, México. Subsequently, we reported that natural mating behavior in female rats produces analgesia during intromissions, and especially ejaculation, that is more potent than a supra-analgesic dose of morphine (Gomora, Beyer, Gonzalez-Mariscal, and Komisaruk, 1994). We tested his hypothesis by administering the glycine receptor antagonist strychnine directly to the spinal cord via intrathecal. Response to mild, innocuous stimulation as if it were noxious is termed "allodynia. When this tonic glycine-induced inhibition is blocked by strychnine administered to the spinal cord, normally innocuous tactile stimuli become aversive. These findings have been confirmed and extended by multiple other investigators based on behavioral and/or neurophysiological evidence (Baba et al. Comparable effects are produced by administration of the glycine precursor Milacemide. Milacemide is converted to glycinamide, which in turn is converted to glycine in the brain (Christophe et al. Milacemide administration counteracts the allodynic effect of strychnine (Khandwala and Loomis, 1998). Recently, we reported that glycinamide, administered to otherwise untreated rats, increased vocalization thresholds to tail shock (Beyer et al. The rats were maintained in a dark-light cycle (14 h light: 10 h dark: lights off at 12:00). Four rats were housed per cage; they were fed with Purina rat pellets and water ad libitum. Rats were ovariectomized (ovx) under ether anesthesia and injected after surgery with i. After one week of ovariectomy, animals were anesthetized for surgery with Ketamine (Bristol laboratories, 25 mg. From Sexual Behavior to Analgesia to an Antinociceptive Agent 281 One week after implantation of the intrathecal catheter and before intrathecal injection, rats were observed in a Plexiglas cylindrical arena (50 cm diameter) for 5 min. Rats having motor problems as a result of the catheter implantation were discarded. After control observations, rats were injected with one of the following solutions: glycinamide (50, 200, or 800 mg/kg body weight) dissolved in saline solution (1 ml/kg body weight) and injected i. Rostrocaudal diffusion following intrathecal injection at this volume is usually limited to the spinal cord within the first 30 min after injection (Yaksh and Rudy, 1976). Rats were replaced in the cylindrical Plexiglas cage and their behavior was recorded and registered. Additionally, the response to cutaneous stimulation with a von Frey fiber was determined at 5, 10, 15, 20, and 25 min after injection, as described above. Other types of motor or aversive reactions were recorded with video equipment (Sony Co. Ovx rats were placed inside the cylindrical Plexiglas arena and allowed to adapt for 5 min. The vocalization threshold to tail shock was ascertained at 30, 45, 60, and 90 min after i. In the control, zero glycinamide group, the vocalizations ranged from 80% at 5 and 10 min, decreasing steadily to 40% at 25 min. Glycinamide at all 3 dose levels significantly reduced this high proportion of vocalization at points during the first 15 min after strychnine injection. It is noteworthy that the strongest inhibition of vocalization (down to about 10% or less) was obtained with the lowest dose level of glycinamide at each of the test periods up to 15 min. It is curious that the lowest dose level of glycinamide actually tended to produce a decrease in vocalization threshold, reaching significance at 90 min. Thus, glycinamide 800 mg/kg potentiated scratching and seizures, and glycinamide 50 mg/kg potentiated hopping (data not shown). Allodynia is characterized by a painful response to otherwise innocuous or low-threshold tactile stimulation (Silvilotti and Woolf, 1994). The present findings are consistent with, and extend, previous findings that glycine, per se, can antagonize the allodynia-producing effect of strychnine (Beyer et al. In addition to glycine, other glycine receptor agonists, specifically, beta-alanine, taurine, betaine, and serine, also were reported to counteract strychnine-induced allodynia (Beyer et al. At some doses, glycinamide paradoxically produced motor activity indicative of hyperalgesia. This observation is consistent with the report that glycine administered intrathecally at certain doses also produced hyperalgesia (Beyer et al. The present findings of the ability of glycinamide administered intraperitoneally to rapidly. Prior research in this laboratory found that administration of glycine directly to the spinal cord. In the present study, we analyzed the effect of graded doses of glycinamide on strychnineinduced allodynia and vocalization threshold to tail shock. Ovariectomized rats were used to assess the effect of glycinamide (0, 50, 200, or 800 mg/kg) i. We recorded behavioral responses to air puff on the fur and gentle von Frey fiber stimulation. The allodynic responses to strychnine were significantly reduced by all doses of glycinamide. Glycinamide (800 mg/kg) significantly elevated the vocalization threshold to tail shock against the vocalization threshold-lowering effect of strychnine.
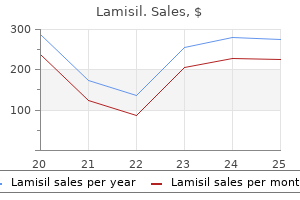
Pathologic Staging All information used in clinical staging and in histologic study of the surgically resected specimen is also used for pathologic staging (Table 15 antifungal killer buy cheap lamisil. The pathologic description of any neck dissection should describe the size fungus vulva order 250 mg lamisil mastercard, number fungus dog vomit buy generic lamisil 250 mg, and level of involved lymph nodes antifungal dog shampoo order lamisil 250 mg, as well as whether extracapsular spread is present antifungal pills side effects discount lamisil 250 mg without prescription. Specimens should also be examined for the presence of lymphovascular and/or perineural invasion in the primary cancer resection. In a trial to assess for tumor biomarkers predictive of outcome in laryngeal carcinoma, Bradford et al. Expression of Bcl-xL, a member of the antiapoptotic Bcl-2 family of proteins, was increased in patients with recurrent/persistent tumors. The results of these studies suggest that a peripheral blood draw could someday be used to identify patients with advanced-stage cancer that may be more likely to respond to an organ preservation protocol that uses induction chemotherapy (Table 15. Occult cervical lymph node metastases are often associated with cancer of the supraglottic larynx. In this group, based on the preoperative staging of the cancer, 14% of cases had occult metastases involving lymph nodes in T1 cancer, 21% in T2 cancer, 35% in T3 cancer, and 75% in T4 cancer. The incidence of occult metastases was higher for the less differentiated cancer and for primary cancer with a higher T stage. In a subset of patients with lateralized supraglottic primary tumors, contralateral occult regional spread occurs in 37% of patients. The authors stressed the importance of bilateral regional nodal treatment with supraglottic tumors even in the N0 setting. In a study from Washington University of 2,550 patients with cancer of the larynx and hypopharynx, the overall incidence of delayed regional metastases was 12. Delayed regional metastases and distant metastases were related to advanced primary cancer (T4 stage), lymph node metastases (node positive [N+]), the cancer arising in the hypopharynx as the primary site, and locoregional cancer recurrence (p = 0. Advanced regional metastases at initial diagnosis (N2 and N3 disease) increased the incidence of delayed and distant metastases threefold (p = 0. Incidences of delayed regional metastases by anatomic location of the primary cancer were glottic, 4. Delayed regional metastases to the ipsilateral-treated neck had a significantly worse survival prognosis than did delayed metastases to the contralateral untreated neck. Among patients with cancers of the head and neck region, ~8% eventually develop distant metastases. A supraglottic primary cancer is the most common subsite associated with the development of distant metastases. The overall 5-year disease-specific survival after patients developed distant metastases was 6. Distant metastases were related to advanced local cancer (T3 + T4), lymph node metastases at presentation (N+), and locoregional cancer recurrence (p = 0. A meta-analysis of variables that predispose to a higher incidence of distant metastasis identified tumor location (hypopharynx > larynx), advanced primary disease (T3 + T4), regional metastasis (N+), locoregional cancer recurrence, and advanced regional metastasis (N2 + N3). Cancer of the lung was the most common second primary and two-thirds of patients who developed a second primary cancer died of disease. With a median follow-up of 68 months, 68 patients (28%) have developed 72 additional cancers. Microscopically, keratotic lesions are characterized by increased thickness of the normally present keratin layer of the epithelium. Hyperkeratosis is defined as the presence of a keratin layer in a normally nonkeratinized epithelium and may represent an early response to mucosal trauma. Moderate-Changes are limited to the lower two-thirds of the epithelial thickness. Severe-Changes involve more than the lower two-thirds of the epithelial thickness. The standard criterion for diagnosis is the presence of atypical changes throughout the epithelium without evidence of surface maturation or invasion through the basement membrane. The actual rate of malignant progression for untreated cases of laryngeal is unknown; however, some estimates have been reported to be as high as 40%. They are graded into well-, moderately, and poorly differentiated cancers based on the degree of differentiation, cellular pleomorphism, and mitotic activity. Immunoreactivity for keratin is universally present and cells also express epidermal growth factor receptors. The majority of basaloid carcinomas of the larynx present as supraglottic primaries (64. Because it produces few early symptoms, patients often present with a bulky cancer. Histologically, this cancer is composed of elongated papillary fronds of welldifferentiated squamous epithelium with extensive keratinization. The margins of the cancer have "pushing" rather than infiltrative growth that is usually accompanied by an exuberant host response of inflammatory cells. Regional lymph nodes may be enlarged and raise suspicion for occult malignancy, but this cancer does not metastasize, and nodal enlargement is invariably part of the host inflammatory response. The combination of the gross appearance of the cancer and the suggestive histologic findings is usually sufficient to establish the diagnosis. Within the larynx, a majority of these cancers arise from the glottis with the remainder diagnosed in the supraglottis. The typical patient is a male in his fifties or sixties who have been hoarse for at least a year before presentation. Overall prognosis is excellent with proper treatment, even among patients with locally advanced cancer. In the series, there were no reported episodes of posttreatment anaplastic transformation. Disease-specific survival was also noted to be comparable to those from series reporting on surgical management; however, local control (66% at 5 years) was noted to be inferior in comparison to surgery. Individuals who experienced a local recurrence (21/62) were capable of undergoing successful salvage resection of persistent cancer. Increased mean levels of expression of survivin, a member of the inhibitor of apoptosis protein family, in regions of parakeratosis have been shown to have the capacity to differentiate verrucous carcinoma from laryngeal papillary hyperplasia. Among these, salivary gland tumors, cartilaginous neoplasms, sarcomas, and neuroendocrine carcinomas have been the types most commonly reported. Adenocarcinoma Adenocarcinomas of the larynx follow the distribution of the laryngeal mucous glands and are primarily supraglottic and subglottic in origin. Clinically, the cancers appear as submucosal, nonulcerated masses and symptoms are the same as for carcinomas of the larynx. Most adenocarcinomas of the larynx present with advanced primary cancer and cervical lymph node metastases. Distant metastases to the liver and lung account for the dismal 5-year survival under 20%. Postoperative radiotherapy is usually advocated, although the numbers of reported cases are too small to know if this confers a survival benefit. Adenosquamous carcinoma is an uncommon but aggressive variant of head and neck squamous cell carcinoma with a propensity for regional and distant metastases with ~50% of cases presenting with a laryngeal primary. Very little has been reported concerning the risk factors or etiology of this variant. The most common site of origin is the subglottis, followed by supraglottic primaries. These cancers produce only vague symptoms while they spread in a perineural and infiltrative growth pattern. When the primary originates from the subglottis, patients typically present with involvement of the laryngeal framework, trachea, thyroid gland, and esophagus. Adenoid cystic carcinoma of the larynx can be difficult to treat because of the predilection for perineural spread and pulmonary metastases. The mainstay of treatment, dependent upon stage and presentation, has typically been surgery (open vs. Locoregional control with functional laryngeal preservation was obtained with a follow-up of at least 5 years in two patients. The authors suggested that this regimen represented an alternative for selected patients with this diagnosis when laryngeal preservation is desired and salvage laryngectomy would be used for nonresponders. Low-grade cancers rarely spread beyond the confines of the larynx and conservation surgical approaches without neck dissection may be curative. The extent of surgery is dictated by the extent of the cancer and elective neck dissection is recommended, even for smaller cancers, because of the risk of occult neck metastases. Its incidence is difficult to know because the low-grade form of this tumor is often confused with a benign chondroma. It predominantly affects men (3:1 male-to-female ratio) between the ages of 50 and 70 years and arises from the hyaline cartilages of the larynx. Chondrosarcoma arising from the cricoid cartilage tends to grow into the airway and cause progressive obstruction, whereas chondrosarcoma arising from the thyroid cartilage typically protrudes laterally and presents as a firm mass in the neck. Endoscopically, the tumor appears as a firm, submucosal mass that is difficult to biopsy because it is so dense. On imaging, these lesions are typically hypodense, wellcircumscribed masses containing mottled calcifications with smooth walls centered within the cartilage. Partial laryngectomy with voice preservation and reoperation if the tumor recurs is an option in selected patients. Challenges arise with tumors arising in the cricoid, and a variety of techniques have been described to reconstruct the larynx following partial resection with reconstruction of the cricoid, using hyoid bone, rib, and strap muscle. High-grade chondrosarcomas usually require a total laryngectomy, with neck dissection reserved for clinical or radiographic evidence of metastasis. Five-year survival rates are not useful data for chondrosarcomas of the larynx, especially with low-grade tumors, because recurrences and subsequent mortality may occur well beyond this time point. Laryngeal carcinoid tumors can be mistaken as being an indolent pathology yet has reported rate of regional and distant metastasis of 33%. Conservative surgical resection with therapeutic neck dissection (in N+ patients) has been advocated. Elective neck dissection is considered unnecessary because of the low rate of associated occult spread. Atypical carcinoid tumors are aggressive lesions with regional and distant metastatic rates ranging from 43% to 67%. Surgical resection is considered the treatment standard with bilateral elective neck dissection being advocated for supraglottic presentations. Small cell neuroendocrine carcinoma has a poor associated prognosis with 90% of patients experiencing regional and/or distant metastasis. Nonsurgical treatment is advocated for this diagnosis and frequently requires a multidrug chemoradiation regimen. The tumors tend to be low grade and are rarely associated with regional or distant spread. The four most commonly described histologic variants are pleomorphic, round cell, myxoid, and well-differentiated liposarcoma. Well-differentiated liposarcoma represents ~65% of cases and can be easily confused with a basic lipoma both macroscopically and microscopically. Wide surgical excision is advocated for this tumor with little evidence of a role for radiation in this setting. Although controversy exists regarding the relative merits of either treatment modality, the rates of cancer control are similar, and patients should be made aware of the options available. Surgical options include endoscopic laser resection, open partial laryngectomy, and total laryngectomy. In contrast, advanced-stage cancers of the larynx typically require combined multimodality therapy to treat the primary site and regional lymphatics. Primary surgical management and adjuvant radiation therapy (with or without chemotherapy) versus chemoradiation with surgery reserved for salvage are typically the options employed in this setting. The procedure may be effectively employed in combination with neck dissection and postoperative radiotherapy when necessary, particularly for moderately advanced supraglottic carcinomas. Invasion of the cricoid cartilage is the most significant limitation of this procedure. All three surgical approaches have been employed for radiation failure but with increased failure and complication rates compared with primary surgical treatment. A decision to treat a cancer of the larynx initially with radiation may complicate the potential for a satisfactory result with salvage partial laryngectomy. The treatment of cancer of the larynx should be individualized with various treatment modalities and surgical procedures according to the size and extent of the cancer, the age and physical condition of the patient, and the skill and experience of the treating physicians. He survived the operation but died several weeks later from pneumonia; after his death, the procedure was condemned. In 1873, Billroth of Vienna performed what is considered to be the first successful laryngectomy. Since then, surgery for cancer of the larynx has seen significant advances that have made the surgery both safe and reliable. These operations are classified according to the surgical approach used and the degree of resection. Path of potential lateral deep invasion for a primary cancer of the glottis that may affect the extent of endoscopic resection. Tumor recurrence was statistically related to the margin status at original resection (p = 0. This open conservation laryngeal technique is reserved for T1 glottic cancers involving the mid true vocal cord and results in cure rates of >90% in selected patients. An endoscopy is performed before the laryngofissure is undertaken, and the cancer is mapped for the suitability of laryngofissure and cordectomy, following which a tracheostomy is performed.
Cheap lamisil 250 mg visa. Curette is King [Callus Tuesday] (2019).
References
- Myers JL, Katzenstein AA. Microangiitis in lupus-induced pulmonary hemorrhage. Am J Clin Pathol 1986;85(5):552-6.
- Ji RR, Zhang Q, Law PY, Low HH, Elde R, Hokfelt T. Expression of m, d, and k-opioid receptor-like immunoreactivities in rat dorsal root ganglia ater carrageenan-induced inlammation. J Neurosci 1995;15:8156-8166.
- Kim BJ, Sohn H, Sun BJ, et al. Imaging Characteristics of Ischemic Strokes Related to Patent Foramen Ovale. Stroke 2013;44(12): 3350-56.
- Varma N, Varma S, Marwaha RK, Malhotra P, Bansal D, Malik K, Kaur S, Garewal G. Multiple constitutional aetiological factors in bone marrow failure syndrome (BMFS) patients from north India. Indian J Med Res 2006;124(1): 51-56.
- Slaughter TF, Sreeram G, Sharma AD, et al: Reversible shear-mediated platelet dysfunction during cardiac surgery as assessed by the PFA-100 platelet function analyzer, Blood Coagul Fibrinolysis 12:85, 2001.
- Kuehn B. State, federal efforts underway to identify children with ?Bubble Boy Syndrome'. J Am Med Assoc 2010;304:16.