
Levitra Oral Jelly
| Contato
Página Inicial
Michael Craig, MD
- Assistant Professor Division of Cardiology
- Medical University of South Carolina
- Charleston, South Carolina
The inferior wall is demarcated from the lateral wall of the orbit by the inferior orbital fissure erectile dysfunction and zantac levitra oral jelly 20mg purchase without prescription, a gap between the orbital surfaces of the maxilla and the sphenoid erectile dysfunction jokes discount levitra oral jelly 20mg online. Its posterior part separates the orbit from the temporal and middle cranial fossae erectile dysfunction treatment following radical prostatectomy levitra oral jelly 20mg visa. The lateral walls of the contralateral orbits are nearly perpendicular to each other impotence from prostate surgery buy levitra oral jelly once a day. The bones forming the orbit are lined with periorbita erectile dysfunction age factor cheap 20 mg levitra oral jelly with visa, the periosteum of the orbit. The conjunctival sac is the space bound by the palpebral and bulbar conjunctivae; it is a closed space when the eyelids are closed, but opens via an anterior aperture, the palpebral fissure (L. The inferior eyelid has been everted to show the reflection of conjunctiva from the anterior surface of the eyeball to the inner surface of the eyelid. The semilunar fold is a vertical fold of conjunctiva near the medial angle, at the lacrimal caruncle. Their ciliary margins are free, but they are attached peripherally to the orbital septum (palpebral fascia in the eyelid). In this dissection of the orbit, the eyelids, orbital septum, levator palpebrae superioris, and some fat have been removed. Structures receiving lacrimal drainage from the conjunctival sac are seen medially. The junctions of the superior and inferior eyelids make up the medial and lateral palpebral commissures, defining the medial and lateral angles of the eye (G. The septum constitutes in large part the posterior fascia of the orbicularis oculi muscle. Accessory lacrimal glands may also be present, sometimes in the middle part of the eyelid, or along the superior or inferior fornices of the conjunctival sac. The eyelids come together in a lateral to medial sequence pushing a film of fluid medially over the cornea, somewhat like windshield wipers. From this sac, the fluid passes to the inferior nasal meatus of the nasal cavity through the nasolacrimal duct. It drains posteriorly across the floor of the nasal cavity to the nasopharynx and is eventually swallowed. In addition to cleansing particles and irritants from the conjunctival sac, lacrimal fluid provides the cornea with nutrients and oxygen. The presynaptic parasympathetic secretomotor fibers are conveyed from the facial nerve by the greater petrosal nerve and then by the nerve of the pterygoid canal to the pterygopalatine ganglion, where they synapse with the cell body of the postsynaptic fiber. Vasoconstrictive, postsynaptic sympathetic fibers, brought from the superior cervical ganglion by the internal carotid plexus and deep petrosal nerve, join the parasympathetic fibers to form the nerve of the pterygoid canal and traverse the pterygopalatine ganglion. It occupies most of the anterior portion of the orbit, suspended by six extrinsic muscles that control its movement, and a fascial suspensory apparatus. The maxillary, infra-orbital, zygomatic, and lacrimal nerves convey the postsynaptic fibers to the gland. The connective tissue layer is composed posteriorly of the fascial sheath of the eyeball (bulbar fascia or Tenon capsule), which forms the actual socket for the eyeball, and anteriorly of bulbar conjunctiva. A very loose connective tissue layer, the episcleral space (a potential space) lies between the fascial sheath and the outer layer of the eyeball, facilitating movements of the eyeball within the fascial sheath. Inner layer (inner coat), consisting of the retina, which has both optic and non-visual parts. Within this pigmented and dense vascular bed, larger vessels are located externally (near the sclera). The central artery courses through the optic nerve and divides at the optic disc into superior and inferior branches. The branches of the central artery are end arteries that do not anastomose with each other or any other vessel. Venous blood from this region and the aqueous humor in the anterior chamber drain into the scleral venous sinus. Two involuntary muscles control the size of the pupil: the parasympathetically stimulated, circularly arranged sphincter pupillae decreases its diameter (constrict or contracts the pupil, pupillary miosis), and the sympathetically stimulated, radially arranged dilator pupillae increases its diameter (dilates the pupil). Abnormal sustained pupillary dilation (mydriasis) may occur in certain diseases or as a result of trauma or the use of certain drugs. The contraction and relaxation of the circularly arranged smooth muscle of the ciliary body controls the thickness, and therefore the focus, of the lens. Aqueous humor fills the anterior segment of the eyeball, the interior of the eyeball anterior to the lens, suspensory ligament, and ciliary body. The iris separates the anterior and posterior chambers of the anterior segment of the eyeball as it bounds the pupil. Ciliary ganglion In bright light: (constricted pupil) (B) Anterior view Postsynaptic parasympathetic nerve fiber Sphincter pupillae Chapter 7 · Head 897 the retina consists of two functional parts with distinct locations: an optic part and a non-visual retina. The non-visual retina is an anterior continuation of the pigmented layer and a layer of supporting cells. Clinically, the internal aspect of the posterior part of the eyeball, where light entering the eyeball is focused, is referred to as the fundus of the eyeball (ocular fundus). The macula is a small oval area of the retina with special photoreceptor cones that is specialized for acuity of vision. Except for the cones and rods of the neural layer, the retina is supplied by the central artery of the retina, a branch of the ophthalmic artery. It has the finest vessels of the inner surface of the choroid, against which the retina is pressed. The cornea is the primary refractory medium of the eyeball-that is, it bends light to the greatest degree, focusing an inverted image on the lightsensitive retina of the fundus of the eyeball. The anterior chamber of the eye is the space between the cornea anteriorly and the iris/pupil posteriorly. Aqueous humor is produced in the posterior chamber by the ciliary processes of the ciliary body. The highly elastic capsule of the lens is anchored by zonular fibers (collectively constituting the suspensory ligament of the lens) to the encircling ciliary processes. In other words, in the absence of external attachment and stretching, it becomes nearly round. In the absence of nerve stimulation, the diameter of the relaxed muscular ring is larger. The lens suspended within the ring is under tension as its periphery is stretched, causing it to be thinner (less convex). The active process of changing the shape of the lens for near vision is called accommodation. In addition to transmitting light, the vitreous humor holds the retina in place and supports the lens. Absence of these movements resulting from nerve lesions contributes to double vision. Movements may occur around the three axes simultaneously, requiring three terms to describe the direction of movement from the primarily position. The four recti muscles are named for their individual positions relative to the eyeball. Thus, the inserting tendons of the oblique muscles lie in the same oblique vertical plane. Similarly, no single muscle can act to depress the pupil directly from the primary position. The muscle sheaths of the levator and superior rectus muscles are fused; thus, when the gaze is directed superiorly, the superior eyelid is further elevated out of the line of vision. Triangular expansions from the sheaths of the medial and lateral rectus (continued on p. In fact, muscles rarely act independently and almost always work together in synergistic and antagonistic groups. To understand the actions produced by muscles starting from the primary position, it is necessary to observe the placement and line of pull of the muscle relative to the axes about which the movements occur. For movements in any of the six cardinal directions (large arrows) the indicated muscle is the prime mover. Structures (minus membranous fascia and fat) after enucleation (excision) of the eyeball. Adduction Depression Nose (E) Actions of muscles of orbit as tested clinically (Right Eye) Chapter 7 · Head 903 muscles, called the medial and lateral check ligaments, are attached to the lacrimal and zygomatic bones, respectively. A blending of the check ligaments with the fascia of the inferior rectus and inferior oblique muscles forms a hammocklike sling, the suspensory ligament of the eyeball. Collectively, the check ligaments act with the oblique muscles and the retrobulbar fat to resist the posterior pull on the eyeball produced by the rectus muscles. In diseases or starvation that reduce the retrobulbar fat, the eyeball is retracted into the orbit (inophthalmos). The trochlear and abducent nerves pass directly to the single muscle supplied by each nerve. It is located between the optic nerve and the lateral rectus toward the posterior limit of the orbit. On the left side, the levator palpebrae superioris and superior rectus have been cut and reflected and the orbital fat removed to demonstrate the nerves that traverse the intraconal fat. The short ciliary nerves consist of postsynaptic parasympathetic fibers originating in the ciliary ganglion, afferent fibers from the nasociliary nerve that pass through the ganglion, and postsynaptic sympathetic fibers that also pass through it. The posterior and anterior ethmoidal nerves, branches of the nasociliary nerve arising in the orbit, exit via openings in the medial wall of the orbit to supply the mucous membrane of the sphenoidal and ethmoidal sinuses and the nasal cavities, as well as the dura of the anterior cranial fossa. The external aspect of the retina is also supplied by the capillary lamina of the choroid (choriocapillaris). The choroid is arranged so that the supplying vessels and larger choroidal vessels are externally placed, and the smallest vessels (the capillary lamina) are most internal, adjacent to the non-vascular layer of the retina. The scleral venous sinus returns the aqueous humor, secreted into the anterior chamber by the ciliary processes, to the venous circulation. The scleral venous sinus is a vascular structure encircling the anterior chamber of the eyeball through which the aqueous humor is returned to the blood circulation. For a description of the surface anatomy of the eyelids, see "Surface Anatomy of Face" (p. When irritated, the vessels may enlarge noticeably, and the bulbar conjunctiva may take on a distinctly pink appearance when inflamed ("red" eyes). The normal tough, opaque sclera often appears slightly blue in infants and children and commonly has a yellow hue in many older people. The dark circular opening through which light enters the eyeball, the pupil, is surrounded by the iris (plural = irides), a circular pigmented diaphragm. The relative size of the pupil and iris varies with the brightness of the entering light; however, the size of the contralateral pupils and irides should be uniform. Even slight variations in the position of the eyeballs are noticeable, causing a change in facial expression to a surprised look when the superior eyelid is elevated (as occurs in exophthalmos, or protrusion of the eyeballs, caused by hyperthyroidism), or a sleepy appearance (as occurs when the superior eyelid droops, ptosis, owing to an absence of sympathetic innervation in Horner syndrome). The bulbar conjunctiva is reflected from the sclera onto the deep surface of the eyelid. Under close examination, the openings of these glands (approximately 20 per eyelid) can be seen on the margins of the eyelids, posterior to the two to three rows of emerging cilia or eyelashes. In the medial angle of the eye, a reddish shallow reservoir of tears, the lacrimal lake, can be observed. Lateral to the caruncle is a semilunar conjunctival fold, which slightly overlaps the eyeball. When the edges of the eyelids are everted, a small pit, the lacrimal punctum, is visible at its medial end on the summit of a small elevation, the lacrimal papilla. Fractures of the medial wall may involve the ethmoidal and sphenoidal sinuses, whereas fractures of the inferior wall (orbital floor) may involve the maxillary sinus. Orbital Tumors Because of the closeness of the optic nerve to the sphenoidal and posterior ethmoidal sinuses, a malignant tumor in these sinuses may erode the thin bony walls of the orbit and compress the optic nerve and orbital contents. The easiest entrance to the orbital cavity for a tumor in the middle cranial fossa is through the superior orbital fissure; tumors in the temporal or infratemporal fossa gain access to this cavity through the inferior orbital fissure. Injury to Nerves Supplying Eyelids Because it supplies the levator palpebrae superioris, a lesion of the oculomotor nerve causes paralysis of the muscle, and the superior eyelid droops (ptosis). The loss of tonus of the muscle in the inferior eyelid causes the lid to fall away (evert) from the surface of the eyeball, leading to drying of the cornea. Excessive lacrimal fluid also forms when the lacrimal drainage apparatus is obstructed, thereby preventing the fluid from reaching the inferior part of the eyeball. People often dab their eyes constantly to wipe the tears, resulting in further irritation. Hyperemia of Conjunctiva the conjunctiva is colorless, except when its vessels are dilated and congested ("bloodshot eyes"). An inflamed conjunctiva, conjunctivitis ("pinkeye"), is a common contagious infection of the eye. Choroid fissure Choroid Inner layer of optic cup Sclera Conjunctival sac Eyelid Anterior chamber Iridopupillary membrane Cornea Ectoderm Iris Subconjunctival Hemorrhages Subconjunctival hemorrhages are common and are manifested by bright or dark red patches deep to and within the bulbar conjunctiva. Although the pigment cell layer becomes firmly fixed to the choroid, its attachment to the neural layer is not firm. Persons with a retinal detachment may complain of flashes of light or specks floating in front of the eye. Chapter 7 · Head 911 Pupillary Light Reflex the pupillary light reflex is tested using a penlight during a neurological examination. When light enters one eye, both pupils constrict because each retina sends fibers into the optic tracts of both sides. The first sign of compression of the oculomotor nerve is ipsilateral slowness of the pupillary response to light. The edema is viewed during ophthalmoscopy as swelling of the optic disc, a condition called papilledema. These changes gradually reduce the focusing power of the lenses, a condition known as presbyopia (G.
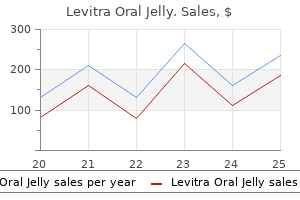
The great vessels expand as cardiac output increases erectile dysfunction guilt in an affair discount generic levitra oral jelly uk, exacerbating the angulation of the ostium to the point where a flaplike closure at the aberrant vessel origin is created erectile dysfunction drugs buy buy discount levitra oral jelly 20mg on-line. Clinical symptoms largely depend on the area supplied by the aberrant artery erectile dysfunction treatment calgary cheap generic levitra oral jelly uk, that is erectile dysfunction drugs nhs order levitra oral jelly 20mg with amex, its dominance erectile dysfunction in cyclists purchase discount levitra oral jelly on line. Between 80% and 90% of these patients die in the first year of life without surgical correction. Neonates experience a sudden drop in pulmonary vascular resistance, pressure, and oxygen content. Catheter-based angiography had previously been the imaging method of choice for the diagnosis of aberrant coronary arteries, but given its invasive nature and two-dimensional fluoroscopic display of three-dimensional anatomy, it may result in incorrect categorizations of coronary anomalies. Patients with Bland-Garland-White syndrome typically present in infancy with heart failure. Clinical, angiographic and hemodynamic findings in patients with anomalous origin of the coronary arteries. Clinical presentation is that of myocardial ischemia, arrhythmias, heart failure, or sudden cardiac death. Anomalous left coronary artery origin from the pulmonary artery: an unusual late presentation of BlandGarlandWhite syndrome. Congenital anomalies of the coronary arteries: imaging with contrast-enhanced, multidetector computed tomography. These measurements are predictive of the presence and degree of coronary artery atherosclerotic plaque burden when compared to measurements on histology, angiography, and intracoronary ultrasound on a per vessel or segment basis. Incidence is virtually 100% by the eighth decade of life, but it is in the low single digits in the second decade. Incidence in women mirrors that of men a decade their junior before the age of 65 to 70, presumably because of the protective effects of estrogen. The investigators also found a slightly lower prevalence in the Chinese population when compared to Caucasians. However, it does occur sparingly in the second and third decade of life in developing lesions. It is thought that ruptured atherosclerotic plaques are followed by calcification as a means of stabilizing the unstable plaque. Pathological specimens confirm that patients with calcified plaque are more likely to have co-occurring, noncalcified ("soft") plaque that is prone to rupture. It should be noted that only approximately 20% of the total plaque volume is calcified. The Agatston score prevails because of the availability of the database for these scores that enables risk stratification. One of the limitations of the Agatston and other scoring methods is that calcium scoring is conventionally performed at 2. Calcium scoring may underestimate the amount of macroscopically visible plaque and fail to detect such plaque in some cases, which may have implications for risk stratification. This method is thought to have resolved the issue of slice thickness, although portability of this method is affected in a manner similar to that of the Agatston method. This is partly explained by the fact that the Callister method does not compute a volume independent of calcium content. For example, if two lesions of equal area differ in calcium content, more area above the nominal threshold will be detected in the higher content lesion. Additionally, linear interpolation will spread the signal of the higher content lesion contained within one slice to other slices, thereby increasing the volume artificially. Mass measurements are computed on the basis of the sum of the integrals of all pixels above a given threshold, multiplied by the voxel volume in mm3, and factored to an appropriate scale. The computed value expresses the total mineral content independent of slice thickness and spatial resolution, but only in the absence of noise. Threshold settings that maximize positive predictive value (minimize false-positive pixels) alter the measurement itself. Nevertheless, this method most closely approaches portability when the threshold setting is appropriately low and the scaling factor is known. In addition, screening with calcium scores is not recommended in low-risk asymptomatic or high-risk patients. The Agatston method has stratified this patient as belonging to the 98th percentile within his age group. Is coronary artery calcium the key to assessment of cardiovascular risk in asymptomatic adults Lesion- and vessel-specific coronary artery calcium scores are superior to whole-heart Agatston and volume scores in the diagnosis of obstructive coronary artery disease. A rosetta stone for coronary calcium risk stratification: Agatston, volume, and mass scores in 11,490 individuals. Numerous cardiac risk factors have been identified in epidemiological studies, such as hypertension, diabetes, smoking, hypercholesterolemia, obesity, sedentary lifestyle, and family history. The remaining one-third of individuals prove to have no or minimal identifiable risk factors. However, thrombosis superimposed on a ruptured atherosclerotic plaque can trigger an acute coronary event that may be potentially fatal (Table 44. Factors that promote plaque vulnerability and rupture include a thin fibrous cap overlying lipid pools and a necrotic core, increased macrophage activity, intraplaque hemorrhage, and plaque progression. This preserves a near normal cross-sectional lumen area until the lesion occupies approximately 40% of the internal elastic lamina area. Negative remodeling is defined as a compensatory decrease in the size of external elastic lamina. According to one study, patients with clinically unstable coronary lesions had more positive remodeling, whereas patients with stable lesions had more negative remodeling. Complex lesion Fibrous cap may be ruptured and possibly ulcerated Fibromuscular tissue deposition may be seen with repair efforts following repeated plaque rupture May slowly grow in size and produce significant arterial narrowing macrophages and metalloproteinases that are responsible for arterial remodeling. Negative remodeling is thought to be associated with fibrotic changes of the arterial wall, which stabilize the plaque, making it less prone to rupture. Calcium deposition can be detected by noninvasive methods in both vulnerable and complex plaques, but classification of the histological type of the detected plaque has yet to be fully elucidated. Moreover, it should be noted that extensively calcified plaques ("hard plaques") are less likely to be associated with acute coronary syndromes. Mineral deposition renders these plaques more stable by uniformly adding stress resistance. Conversely, mild to moderate amounts of calcification destabilize plaques via a nonuniform stiffening effect, making them more susceptible to shear stress. Cone-down view of a frontal chest radiograph demonstrates a heavily calcified left main coronary artery (arrows). High sensitivity and specificity, positive predictive value, and negative predictive value of this modality in the detection of coronary stenoses in comparison to invasive angiography have been reported in several studies. In addition, the increased coverage of 320-slice scanners eliminates oversampling and stair-step artifact on volumetric reconstruction by enabling acquisition of the entire heart in a single heartbeat/gantry rotation without heart-rate restrictions. Of particular clinical interest, noninvasive identification of potentially vulnerable plaques is sometimes possible through the quantification of lesion attenuation values. However, characterization of plaque morphology and composition is imprecise, and its clinical value is unknown. Although it is an invasive procedure, it has been verified to be safe, accurate, and reproducible. A small ultrasound transducer mounted to a coronary angioplasty catheter is advanced by an endovascular route beyond the distal plaque segment of interest. A series of 360-degree cross-sectional images are obtained as the catheter is drawn proximally. Noninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomography. Evaluation of coronary artery calcification by multi-detector row computed tomography for the detection of coronary artery stenosis in Japanese patients. Role of electron-beam computed tomography and nuclear stress testing in cardiovascular risk assessment. Arterial remodeling and coronary artery disease: the concept of "dilated" versus "obstructive" coronary atherosclerosis. However, stenosis greater than 70% results in 41% survival over the same time span. The distal portion of the artery (the area of bifurcation into the left anterior descending and the left circumflex) is most commonly involved in atherosclerosis development because of low shear stress in that region. Left main equivalent disease is defined as a greater than 70% narrowing of both the left anterior descending and the left circumflex coronary arteries. These atherosclerotic lesions are usually complex plaques, with characteristic internal surface ruptures, fissures, and hemorrhages. More advanced scanners may have dual-source technology and wide z-coverage and allow for prospective triggering and iterative reconstruction, thereby reducing radiation exposure. Small vessel caliber and cardiac motion can lead to suboptimal image quality and diagnostic accuracy in the assessment of luminal stenosis as compared with that with conventional angiography. Comparison can be made by acquiring images at rest and under adenosine-induced stress. Proximal and distal reference sites must be located within 5 mm of suspected stenoses in the vessel to determine its normal diameter. During catheterization, pressure change in the affected area can be seen, with ostial lesions lacking contrast reflux into the aortic sinus. Limitations of conventional angiography include underestimation of coronary stenosis and limited ability to evaluate plaque burden and plaque vulnerability in the vessel wall. Patient age, stenosis severity, coronary artery dominance, presence of congestive heart failure, left ventricular function, presence of inflammatory mediators, and hypertension are all survival predictive factors. In addition to the outlined treatment options, patients are encouraged to minimize their risk of adverse coronary events by ceasing smoking and maintaining proper glycemic control, lipid levels, and blood pressure. Prevalence of narrowing 50% of the left main coronary artery among 17,300 patients having coronary angiography. Left main coronary artery stenosis no longer a risk factor for early and late death after coronary artery bypass surgery-an experience covering three decades. Comparison between coronary angioplasty and coronary bypass surgery for the treatment of unprotected left main coronary artery stenosis (the Bologna Registry). Percutaneous coronary intervention with stent implantation versus coronary artery bypass surgery for treatment of left main coronary artery disease: is it time to change guidelines Hemodynamically significant narrowing equal to or greater than 70% the lumen diameter is considered severe. It gives rise to ventricular branches that supply the lateral and posterior aspects of the left ventricle, as well as the superolateral papillary muscle of the mitral valve. Atherosclerotic lesions large enough to result in an acute coronary syndrome are usually complex plaques. Presumably, vessel tortuosity and branching create local variations in shear stress. Because proximal large-caliber epicardial coronary arteries supply such a large myocardial territory, thromboses within these locations leading to acute coronary events portend high morbidity and mortality. These data suggest that while a single culprit lesion can cause an acute coronary event, simultaneous ruptures are frequently located in all three main coronary trunks. It should be noted that nonculprit lesions exhibit positive remodeling to the same degree as culprit lesions, but are distinct in that they are less stenosing, less calcified, and therefore possibly younger lesions. To accurately evaluate the extent of disease, vessel tracking should be used, and each vessel should be examined in its long and short axis. Lumen stenosis can be quantified by measuring the affected area with an electronic caliper on cross-sectional or longitudinal projections. Axial images, multiplanar reconstructions, and tracked curved multiplanar reconstructions can be used to display the course of each vessel individually. Note also the presence of calcification at the takeoff of the first diagonal branch (arrowhead). The proximal and distal vessel calibers to the area of stenosis are used to evaluate the restriction in lumen surface area; in this case, there is greater than 70% stenosis, which is indicative of severe disease. Sensitivity and specificity results for proximal coronary segments were 93% and 95%, respectively, with similar results for mid-segments; distal segments showed a sensitivity of 80% and a specificity of 97%. Conventional coronary angiography is the gold standard for evaluation of coronary artery stenosis. However, it is limited in its ability to visualize calcified plaques and small noncalcified plaques, which renders it inadequate in the evaluation of coronary artery disease in low- and intermediate-risk patients. Differential Diagnosis (for Symptoms of Chest Pain) Coronary artery spasm Mitral valve prolapse Aortic stenosis Acute myocarditis Aortic dissection Pulmonary embolism Gastroesophageal reflux disease Peptic ulcer disease Musculoskeletal disease of the chest wall Clinical Issues Treatment of coronary artery disease is classified into medical therapy and revascularization. Most patients with coronary artery stenosis of greater than 70% derive more benefit from revascularization than from medical therapy. In addition, patients are encouraged to reduce their risk factors for acute coronary events by initiating exercise, ceasing smoking, and maintaining blood pressure, glycemic, and lipid control. Frequency and distribution of thin-cap fibroatheroma and ruptured plaques in human coronary arteries. Noninvasive assessment of coronary artery disease anatomy, physiology, and clinical outcome. Orellana Definition A coronary artery aneurysm (also known as ectasia) is defined as a segment of greater than 1. There are several complications that result from aneurysm formation, such as thrombosis, embolism, vessel rupture, arteriovenous fistula formation, and spasm. Thrombosis is a sequela of slow blood flow and can result in myocardial ischemia or embolization. Rupture of the vessel remains a rare complication due to early detection, but can result in cardiac tamponade. Clinical Features Aneurysms are a common incidental finding on coronary angiography. Patients with coronary artery aneurysms can be asymptomatic or present with angina, congestive heart failure, myocardial infarction, or sudden death.
Affected patients most often become symptomatic in the first few months to years of life erectile dysfunction blue pill levitra oral jelly 20 mg purchase mastercard. Approximately half of pediatric patients with primary pulmonary vein stenosis have an associated cardiac defect what is an erectile dysfunction pump levitra oral jelly 20mg order, and the most are septal defects erectile dysfunction 27 purchase cheap levitra oral jelly. Primary pulmonary vein stenosis has also been associated with bronchopulmonary dysplasia young healthy erectile dysfunction generic 20 mg levitra oral jelly otc. Pediatric patients with pulmonary vein stenosis usually present in the first months to years of life with a history of respiratory symptoms-tachypnea and recurrent pneumonias impotence causes and symptoms levitra oral jelly 20 mg purchase. The most common cause of pulmonary vein stenosis in adults is radiofrequency ablation procedures for treatment of atrial fibrillation. The incidence of pulmonary vein stenosis after radiofrequency pulmonary vein ablation is approximately 13%, and the incidence of complete pulmonary vein occlusion is 0. The mechanism is thought to be periadventitial inflammation and collagen deposition. Symptoms of pulmonary vein stenosis after radiofrequency ablation may develop weeks to months after the ablation procedure. Patients most often present with shortness of breath, chest pain, and sometimes hemoptysis. Other causes of pulmonary vein stenosis in the adult population are very rare and include complications of fibrosing mediastinitis, radiation treatment, malignant infiltration, pericarditis, histoplasmosis, or scarring after surgical intervention. Symptoms may include chest pain, dyspnea, cough, hemoptysis, recurrent pneumonia, pulmonary edema, and pulmonary hypertension. Late diagnosis is common and likely related to the nonspecific nature of the symptoms. Pulmonary vein stenosis may commonly be misdiagnosed as pulmonary embolism, bronchitis, pneumonia, asthma, or lung cancer. Many patients with undiagnosed pulmonary vein stenosis receive multiple unnecessary interventions, including bronchoscopy, thoracentesis, or antibiotic treatment for pneumonia. Approximately 80% of patients have four separate pulmonary vein ostia, 16% have five pulmonary vein ostia, and 4% have three pulmonary vein ostia. The most common nonanomalous pulmonary venous variant is early confluence of superior and inferior pulmonary veins proximal to the left atrium, resulting in a "common" or "conjoined" vein, with only one venoatrial junction on the involved side. Supernumerary or accessory pulmonary veins are extra veins with individual venoatrial junctions separate from the superior and inferior pulmonary veins. Accessory pulmonary veins occur more frequently on the right side, usually the right middle lobe or superior segment of the right lower lobe. Pulmonary vein stenosis causes increased back pressure peripheral to the stenosis, decreasing ipsilateral pulmonary artery flow and increasing contralateral pulmonary artery flow. Over time, the ipsilateral pulmonary artery becomes hypoplastic because of the long-standing decreased blood flow. Therefore, these patients are more sensitive to pulmonary stresses such as infection, interstitial lung disease, and pulmonary emboli. Imaging from a 4-month-old girl with congenital stenosis of the left lower lobe pulmonary vein treated with stenting who presented with heart failure. The left superior pulmonary vein (arrow), as it enters the hilum, is markedly narrow. Underlying molecular mechanisms for pulmonary vein stenosis as a complication of cardiac surgery, in which the atria and pulmonary veins are directly manipulated, remain poorly defined. One likely mechanism is periadventitial inflammation or collagen deposition, which may compromise or even occlude the lumen. How to Approach the Image Accurate and complete diagnosis of primary pulmonary vein stenosis remains challenging. It is imperative that all pulmonary veins be thoroughly investigated in any patient newly diagnosed with any type of congenital heart disease. Most symptomatic patients with pulmonary vein stenosis present with a radiographic appearance of a localized opacity or localized edema. Echocardiography can be used to visualize all pulmonary veins in children with a good acoustic windows. The finding of turbulent flow on color Doppler imaging is suspicious for pulmonary vein stenosis. However, in adults, transesophageal echocardiography is limited by its inability to image deeply into all four pulmonary veins and is less useful in establishing the extent and location of pulmonary vein stenosis. A functional test that detects reduced perfusion to a segment of the lung is likely to add information to that provided by an anatomic image alone. Asymmetrical pulmonary venous stenosis results in redistribution of flow throughout the lungs. Pulmonary vein stenosis results in decreased perfusion in the affected lobe when the resting pulmonary veinleft atrial pressure gradient is at least 5 mmHg or when there is 80% luminal stenosis. Primary pulmonary vein stenosis is characterized by focal narrowing of the junction between one or more pulmonary veins and the left atrium. Length, stenosis morphology and severity can vary from short weblike lesions to long diffusely diseased segments. All postoperative patients in which the left atrium was manipulated should routinely have their pulmonary veins evaluated, because pulmonary vein stenosis can develop long after the surgical procedure. Ostial ablation is associated with an approximate 8% reduction in ostial diameter. Focal narrowing is most prevalent in the left inferior pulmonary vein, likely due to more medial location within the cardiac silhouette, leading to less precise localization of the pulmonary ostium and energy delivery within the pulmonary vein rather than in the preferred ostial location. Findings of pulmonary vein stenosis after radiofrequency ablation include extensive fibrosis in the perihilar tissues. Stenoses usually begin approximately 1 to 2 mm lateral to the ostium and extend peripherally for variable lengths of up to 35 mm. Imaging from a 25-year-old man with refractory paroxysmal atrial fibrillation treated with radiofrequency ablation. Differential Diagnosis Pulmonary vein "pseudo-stenosis" variant is a rare radiological finding of the left inferior pulmonary vein, with a waistlike narrowing involving the venous ostium. Clinical Issues Patients with the pediatric form of pulmonary vein stenosis, either primary or secondary, have a very poor prognosis without treatment. Most of these patients suffer from pulmonary hypertensive crisis, recurrent pulmonary infection, or hemoptysis. Various treatment options are balloon dilatation, stenting, and/or lung transplantation. In adults, clinical success rates of up to 80% have been documented for atrial fibrillation ablation procedures. However, ostial ablation of the pulmonary veins is associated with increased risk of pulmonary vein stenosis, which occurs in 1 to 3% of patients. Other associated severe complications include endocardial charring, pulmonary vein dissection, stroke, hemopericardium, hemothorax, pulmonary vein thrombosis, and atrial or pulmonary vein perforation. Pulmonary vein thrombosis and hemodynamically significant pulmonary vein stenosis can lead to pulmonary venous infarction, fibrosing mediastinitis, pulmonary veno-occlusive disease, and pulmonary arterial hypertension. Less severe complications include small pleural or pericardial effusions and transient small atrial septal defects. Post-radiofrequency ablation pulmonary vein stenosis is mostly treated by endovascular techniques. Risk factors for restenosis include small reference vessel diameter and longer time from pulmonary vein ablation to intervention for pulmonary vein stenosis. Key Points Noninvasive tests are generally sufficient to diagnose pulmonary vein stenosis. Approximately one-half of patients with primary pulmonary vein stenosis have associated cardiac defects. Evaluation for stenotic pulmonary veins is indicated in any young patient with severe pulmonary hypertension. Symptomatic patients after radiofrequency ablation procedures should have a thorough evaluation for possible pulmonary vein stenosis. Pulmonary vein stenosis is a rare cause of pulmonary hypertension and is associated with significant morbidity and mortality. It is imperative that radiologists be familiar with left atrium and pulmonary vein variant anatomy. Multimodality imaging assessment of anatomic and functional pulmonary vein stenosis. Symptoms and signs of significant left-to-right shunt include congestive heart failure, tachypnea, cardiomegaly with enlargement of right heart, and tachycardia. Signs of congestive heart failure, including cardiomegaly and pulmonary vascular prominence, may be seen with significant left-to-right shunting, although these findings are not specific. Limitations include the requirement for intravenous contrast and exposure to ionizing radiation. Axial (b) and coronal (c) views show the anomalous vessel (arrowhead) draining into the left brachiocephalic vein (arrow). Patients may present with tachypnea, cardiomegaly with enlargement of right heart, and tachycardia. For children with scimitar syndrome, however, there is a high incidence of postoperative pulmonary venous obstruction and decreased right lung perfusion. Note the enlarged pulmonary artery suggestive of a significant left-to-right shunt and right-sided heart strain. Outcomes after surgical treatment of children with partial anomalous pulmonary venous connection. The anomalous right pulmonary vein gently curves down in a vertical course in the right mid-lung, traversing the right medial cardiophrenic angle, and resembles a Turkish sword (scimitar), hence the name. The syndrome is also referred to as hypogenetic lung syndrome and congenital pulmonary venolobar syndrome. However, Scimitar syndrome specifically is exceedingly rare, with an incidence of just 2 per 100,000 births. With the return of oxygenated blood to the right atrium, an extracardiac left-to-right shunt is produced. The shunt is often hemodynamically insignificant but when significant can produce right heart volume overload and pulmonary hypertension, depending on the size of the shunt. Scimitar syndrome is also associated with cardiac anomalies 25% of the time, and other anomalies such as diaphragmatic and spinal anomalies can also be seen. Adult: asymptomatic and detected incidentally on chest radiograph Prognosis for those with Scimitar syndrome without associated cardiac anomalies is quite good, as these individuals have a normal or near-normal lifespan. Prognosis is moderate to poor, however, for those who present in the neonatal period, as irreversible pulmonary hypertension can result. Clinical Features Scimitar syndrome is clinically silent in approximately 50% of patients who maintain subclinical left-to-right shunts. Patients may also present with paradoxical embolization if a septal defect is present. The most common signs and symptoms depend on age at presentation and size of left-to-right shunt: Newborn: right heart volume overload, congestive heart failure, pulmonary hypertension Older child: recurrent infections in right lung base Anatomy, Physiology, and Pathophysiology Unilateral pulmonary hypoplasia during embryogenesis is the primary abnormality in Scimitar syndrome, and the anomalous pulmonary venous return develops secondarily. The degree or severity of pulmonary hypoplasia ranges from mild to marked, and it most commonly affects the upper and/or middle lobes. The right pulmonary artery and mainstem bronchus display a similar degree of hypoplasia as the right lung. The right lung additionally often has morphological features of the left lung, including a hyparterial bronchus and absence of the minor fissure. Also, there is sometimes systemic arterialization of the right lung base; however, this entity is distinguished from pulmonary sequestration by having normal lung parenchyma in the affected right lower lobe. The right lung hypoplasia results in volume loss that produces a rightward shift of the mediastinum and dextroposition of the heart. This does not represent true dextrocardia, as the heart maintains normal orientation with the apex directed left. The anomalous pulmonary venous return delivers oxygenated blood to the right atrium, which creates a left-toright shunt with increased blood flow to the pulmonary vessels. If the shunt is significant enough, the right heart may become volume overloaded and enlarged. Finally, if the shunt is right to left 2:1 or greater, pulmonary hypertension may develop, producing Eisenmenger physiology if irreversible. Angiography can be used to visualize filling of the scimitar vein during the venous phase of pulmonary artery angiogram. Angiography is useful, however, for treatment purposes, with embolization of anomalous venous supply undertaken to reduce the size of the shunt. Also, anomalous arterial supply to the right lower lobe may be embolized before planned surgical intervention in order to reduce bleeding complications. Clinical Issues In half of affected patients, Scimitar syndrome produces a very small shunt and is asymptomatic. For those with more significant shunts presenting in the neonatal period, the prognosis is moderate or poor, as irreversible pulmonary hypertension may develop. For the subset of patients with left-to-right shunts greater than 2:1, endovascular or open surgical intervention is recommended to ligate or coil embolize anomalous venous drainage or restore pulmonary venous flow to the left atrium. Finally, when there is a systemic arterial supply, it is often embolized before any operative intervention in order to minimize bleeding complications. Note that the caliber of the anomalous vein does not taper as the vein progresses distally, unlike a normal pulmonary vein. It is a spectrum disorder with clinical signs, symptoms, and prognosis dependent on the severity of left-to-right shunt and age of presentation. Surgical and/or endovascular intervention is required if there are cardiac anomalies or left-to-right shunt is greater than 2:1 to ligate or embolize the anomalous pulmonary vein and/or arterial supply. Suggested Reading Berrocal T, Madrid C, Novo S, Gutierrez J, Arjonilla A, Gomez-Leon N. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology.
Discount 20mg levitra oral jelly overnight delivery. Blink Health - Amazingly Inexpensive E.D. Meds - Meet Jim.
References
- Bailey KM, Castle VP, Hummel JM, et al. Thalidomide therapy for aggressive histiocytic lesions in the pediatric population. J Pediatr Hematol Oncol 2012; 34(6):480-483.
- Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med 2003;139(2):137-47.
- Fang X, Tie J, Xie Y, et al. Detection of gastric carcinoma-associated antigen MG7-Ag in human sera using surface plasmon resonance sensor. Cancer Epidemiol 2010;34: 648-51.
- Kikuchi T, Kamiya Y, Ohtsuka T, et al: Randomized prospective study comparing the laryngeal tube suction II with the ProSeal laryngeal mask airway in anesthetized and paralyzed patients. Anesthesiology 109:54, 2008.