
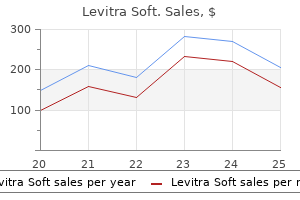
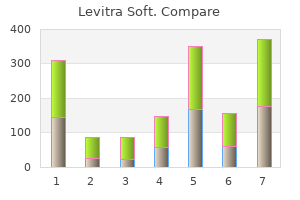
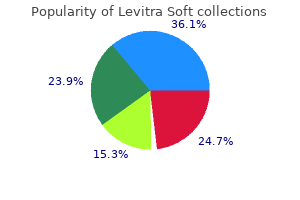
Levitra Soft
| Contato
Página Inicial
Jane M. Prosser, MD
- Fellow, Medical Toxicology
- New York City Poison Center
- New York University Medical Center
Tubular transport maximum (Tm): the maximum rate of transport for a substance (eg impotence after robotic prostatectomy buy levitra soft with visa, TmG denotes the maximum reabsorptive rate of glucose) erectile dysfunction and testosterone injections levitra soft 20 mg low cost. The glomerulus men's health erectile dysfunction pills cheap levitra soft online american express, proximal tubule erectile dysfunction pills buy purchase levitra soft now, descending limb and ascending limb erectile dysfunction treatment delhi levitra soft 20 mg order visa, distal tubule, and collecting duct. Approximately 60% to 70% of the filtered fluid is reabsorbed in the proximal tubule. The primary transport process underlying fluid reabsorption is active sodium reabsorption. Water and many other filtered solutes then are reabsorbed passively as an isosmotic reabsorbate. The Na+ then is extruded actively across the basolateral membrane, giving rise to Na+ reabsorption. Chloride and bicarbonate ion are reabsorbed passively either through the cell or through the tight junctions between the cells (the proximal tubule has "leaky" tight junctions), providing a balance of charge. The tissue is very leaky to water so that as solute is reabsorbed through the cell into the interstitial space, water follows passively by osmotic coupling to the solute, moving through the cells or through the "leaky" tight junctions between the cells. The entry step for Na+ across the luminal cell membrane is normally a coupled process. The two most dominant transport processes are Na+-H+ exchange, which is important for Na+ reabsorption and acidbase balance, and Na+-glucose cotransport, which is important for both Na+ and glucose reabsorption. Both processes are passive steps that are driven by the Na+ gradient into the cell (set up by the Na+ pump). Hence, glucose entry often is referred to as secondary active transport even though the entry step is passive. Once inside the cell, glucose is transported passively across the basolateral membrane by a facilitated diffusion process (passive glucose transporter) into the interstitial space and taken up into the peritubular capillaries. Under normal conditions, all filtered glucose is reabsorbed, except for trace quantities, from the tubular lumen of the proximal tubule, utilizing the Na+glucose cotransport process at the luminal border. However, both Na+ and glucose must bind to specific, but saturable, sites on the Na+-glucose cotransport carrier protein, making glucose reabsorption saturable. Hence, under conditions of elevated plasma glucose levels, such as in diabetes mellitus, or an increased glomerular filtration rate, such as in pregnancy, the filtered glucose load can exceed the capacity for glucose transport; that is, the Na+ glucose cotransporters become saturated, leaving un-reabsorbed glucose behind in the tubular fluid which is swept away into the final urine (glycosuria). In the presence of un-reabsorbed glucose, the "trapped" glucose will act as an osmotic solute, leading to an osmotic diuresis. The associated diuresis can be particularly problematic in patients with diabetes mellitus. The reabsorption of other organic solutes in the proximal tubule also is coupled to Na+ as a Na+-solute cotransporter at the luminal cell membrane, Both sugars, such as galactose, and most amino acids, such as glutamate and glycine, are cotransported with Na+ and display both a tubular transport maximum and a renal plasma threshold (the transport of some amino acids, such as lysine and proline, is not Na+ dependent). Galactose can compete with glucose for binding and transport by the Na+-glucose carrier so that with elevated plasma levels of galactose, such as in pregnancy, galactose can contribute to appearance of glucose in the urine. The proximal tubule is also the site of reabsorption of certain organic acids, with the most dominant normally being lactate anion. Two Na+dependent cotransport process at the luminal membrane appear to underlie organic acid reabsorption: one specific for monocarboxylates such as lactate, pyruvate, acetoacetate, and -hydroxybutyrate and the other for di- and tricarboxylates such as malate, succinate, and citrate. Once inside the cell, the carboxylates exit the cell by means of a variety of exchange processes. Other organic acids, such as urate, an end product of purine catabolism, are both secreted and reabsorbed in the proximal tubule; both processes are Na+-independent, with the reabsorptive mechanisms dominating. Finally, the proximal tubule is the site of secretion of numerous organic anions (paraaminohippurate, oxalate) and cations (choline, guanidine) by separate, saturable transport processes that often involve anion exchange processes that are Na+-independent. Larger peptides and proteins such as myoglobin and albumin bind to the luminal membrane and enter the cell by receptor-mediated endocytic processes and are delivered to lysosomes for degradation. Some filtered inorganic anions, such as sulphate and phosphate, also are reabsorbed in the proximal tubule via a Na+ cotransport process; hence, their transport can be defined by a Tm and renal plasma threshold. The appearance of glucose in the urine is a consequence of which of the following processes in the proximal tubule Upon admission to the emergency room, he is diagnosed with diabetic ketoacidosis, which is accompanied by extreme hypovolemia, supposedly because of the brisk diuresis. His urine is "tea" colored as a result of breakdown of skeletal muscle by the cocaine, so-called rhabdomyolysis. In diabetes mellitus, in which plasma glucose levels are markedly elevated, the high glucose load being filtered (with an elevated concentration) can exceed the capacity of the luminal Na+-glucose cotransporter to reabsorb glucose (ie, the carrier is saturated). The excess glucose that is not reabsorbed is trapped in the tubular fluid because no transport pathways are present in later nephron segments to reabsorb this hexose. In diabetic ketoacidosis, plasma levels of glucose are elevated, leading to an excess filtered load of glucose. The increased rate of filtration of glucose can exceed the capacity of the Na+-glucose cotransporter in the proximal tubule to reabsorb all the glucose. The excess glucose that is not reabsorbed will be retained in the tubular lumen and generate a solute diuresis. Larger peptides and proteins such as myoglobin and albumin bind to the luminal membrane and enter the cell by receptormediated endocytic processes and are delivered to lysosomes for degradation. Myoglobin, if crystallized in the renal tubules, can lead to a toxic effect, sometimes even renal failure. The reabsorption of glucose is coupled to Na+ via a luminal membrane Na+-glucose cotransporter. The favorable downhill electrochemical gradient for Na+ entry can drive influx of glucose up its chemical gradient to elevated levels inside the cell, thereby appearing to be an active influx of glucose (even though it is passive), giving rise to what is termed secondary active transport of glucose. Many amino acids are reabsorbed in the proximal tubule by Na+amino acid cotransport processes, whereas others are reabsorbed by Na+-independent transport processes. Oligopeptides are reabsorbed in the proximal tubule by first being metabolized to their constitutive amino acids by luminal membrane peptidases and then being transported by Na+-amino acid cotransporters and Na+-independent amino acid transporters into the cell. Large peptides and proteins are reabsorbed in the proximal tubule by receptor-mediated endocytosis. His pulmonary edema and peripheral edema improve when furosemide (Lasix), a loop diuretic, is administered. He returns to his primary care physician 3 weeks after the hospitalization and complains of weakness, dizziness, and nausea. An electrolyte panel demonstrates hypokalemia, and he is started on supplemental potassium, with improvement of his symptoms. Loop diuretics: Act on the sodium-potassium-chloride cotransporter in the loop of Henle and decrease the reabsorption of sodium and water. Hypokalemia with loop diuretics: An increased flow rate through the late distal tubule and cortical collecting duct causes dilution of luminal potassium concentration and favors potassium secretion. Patients with congestive heart failure, cirrhosis, and pulmonary edema often are started on these medications. Their site of action is primarily on the sodium-potassium-chloride cotransporter (Na-K-Cl cotransporter) in the loop of Henle, hence the term loop diuretics. This expected side effect results because the increased flow rate through the distal tubule and cortical collecting duct causes a dilution decrease in the luminal potassium concentration and favors potassium secretion. Hypokalemia presents clinically with muscle weakness, nausea, fatigue, dizziness, and intestinal ileus and, if potassium is low enough, may lead to coma and fatal cardiac arrhythmias. Spironolactone is an antagonist of aldosterone, and amiloride acts on the sodium channel; both do not result in increased potassium loss. Know about reabsorption and secretion in the loop of Henle, distal tubule, and collecting duct. Potassium-sparing diuretic: A diuretic that acts by inhibiting sodium reabsorption and potassium secretion in the late distal tubule and cortical collecting duct, thereby inhibiting the loss of potassium. Aldosterone: A mineralocorticoid hormone that stimulates the reabsorption of sodium from and the secretion of potassium into the late distal tubule and cortical collecting duct. The loop of Henle plays a particularly central role in giving the kidneys the ability to both concentrate and dilute urine, providing the foundation for both osmotic balance and volume balance. The loop of Henle consists of the thin descending limb, the thin ascending limb, and the thick ascending limb, which ends at the macula densa (adjacent to its own glomerulus). The segments reabsorb 25% to 30% of the filtered NaCl, primarily in the thick ascending limb, with a smaller fraction of water, thereby rendering the medullary interstitial fluid hypertonic and the fluid leaving the thick ascending limb hypotonic, a condition that is necessary for excreting a urine with a variable osmolality. This occurs by a mechanism referred to as the countercurrent multiplier system that is dependent on the transport properties of the various segments: high water permeability and low NaCl permeability of the thin descending limb, high NaCl permeability and low water permeability of the thin ascending limb, and low water permeability with active reabsorption of Na+, along with Cl-, of the thick ascending limb, the segment that is the driving force for the whole process. Active reabsorption of Na+, along with Cl-, by the thick ascending limb renders the medullary interstitial fluid hypertonic, causing reabsorption of water from the descending limb. However, relatively more NaCl than water is transported into the interstitium, and so the medullary interstitium becomes hypertonic. With the countercurrent flow of fluid down the descending limb and up the ascending limb, a vertical amplification of the interstitial hypertonicity develops, increasing from approximately 290 mOsmol/kg at the corticomedullary junction to as high as 1200 to 1400 mOsmol/kg near the tip of the papilla (see the references at the end of this case for more detail). Conversely, fluid leaving the thick ascending limb is hypotonic (approximately 100 mOsmol/kg). An essential transport process for Na+ and Cl- reabsorption in the thick ascending limb is the entry step at the luminal membrane: Modulating or inhibiting this cotransporter directly regulates net transport of NaCl across the cell, thereby regulating the magnitude of the medullary interstitial hypertonicity. The K+ and Cl- diffusion processes set up a lumen-positive membrane potential, as shown in the figure. Because the paracellular pathway through the tight junctions is more selective for cations, the lumen-positive potential arising from the cellular transport processes will lead to passive reabsorption of Na+ between the cells as part of the process of NaCl reabsorption in this segment. As fluid leaves the loop of Henle, it enters the distal convoluted tubule in the cortex. Here Na+, along with Cl-, is reabsorbed actively, with the entry of Na+ across the luminal membrane being coupled to Cl- by a thiazidesensitive NaCl cotransporter. The water permeability of the segment is relatively low so that little water is reabsorbed by this segment. Fluid passes from the distal convoluted tubule into the late distal tubule (connecting tubule/initial collecting tubule) and on into the cortical collecting duct and medullary collecting duct segments. The same cells also contain a K+ channel at the luminal border, and this provides for K+ secretion across the luminal border into the tubular fluid. K+ enters the cell across the basolateral membrane via the Na+ pump, which maintains high intracellular K+ concentrations, and then exits the cell either via the luminal membrane K+ channel, giving rise to K+ secretion, or via a basolateral membrane K+ channel, recycling back into the interstitium. Aldosterone secretion is stimulated by volume depletion (through the renin-angiotensin-aldosterone system), as is observed in hemorrhage and after the administration of high-ceiling loop diuretics. Aldosterone primarily acts in the connecting tubule and principal cells of the cortical collecting duct to increase the reabsorption of Na+ and Cl- and the secretion of K+. In addition, aldosterone acts by increasing the opening of existing luminal membrane Na+ and K+ channels. These effects require protein synthesis, and so the effects on transport are apparent only after a delay of 1 or 2 hours. Na+ reabsorption in these cells is stimulated by enhanced Na+ entry and Na+ efflux after the increased opening of existing Na+ channels, by synthesis of new Na+ channels, and by synthesis of new Na+ pumps. The stimulation of net Na+ reabsorption causes a hyperpolarization of the tubule, with an increased luminal negativity (basolateral side positivity), and depolarization of the luminal membrane per se. This leads to a more favorable gradient for K+ to diffuse from the cell into the luminal fluid by K+ channels in the luminal cell membrane of the principal cells. Increased K+ diffusion (secretion) into the lumen, coupled with increased K+ uptake into the cell caused by the stimulation of the Na+ pump (increased Na+ efflux, increased K+ uptake) at the basolateral membrane, leads to an enhanced rate of K+ secretion into the tubular lumen. If the tubular flow rate does not change, the tubular fluid K+ concentration will be elevated, ultimately reducing the electrochemical gradient for K+ diffusion across the luminal membrane, limiting the rate of K+ secretion. Conversely, under conditions in which the tubular flow rate to the collecting ducts is elevated, such as after treatment with a loop diuretic, the K+ concentration in the tubular fluid will be lower, providing a more favorable electrochemical gradient for K+ diffusion into the lumen, thereby leading to enhanced K+ secretion and in turn enhanced K+ excretion. This can be ameliorated by treatment with potassium supplements or administration of K+-sparing diuretics such as amiloride and spironolactone. Amiloride acts to block the luminal Na+ channel in the late distal tubule and cortical collecting ducts, thereby markedly reducing Na+ reabsorption and in turn K+ secretion. Spironolactone, in contrast, competes with aldosterone for its receptor and depresses both Na+ reabsorption and K+ secretion in the late distal tubule and collecting duct. Furosemide, a "high-ceiling" diuretic, is a potent agent because it binds to and inhibits which of the following transport processes The Na+-glucose cotransporter in the proximal tubule the Na+-K+ exchange pump in all nephron segments the Na+-K+-Cl- cotransporter in the thick ascending limb the Na+-Cl- cotransporter in the distal convoluted tubule the Na+ channel in the cortical collecting duct One week later, the patient returns to the clinic complaining of dizziness, weakness, and nausea. This is a critical transporter for reabsorption of NaCl from the thick ascending limb into the medullary interstitium. This transport of NaCl is the driving force behind the establishment of the hypertonicity of the medullary interstitium that is essential for the reabsorption of water from the collecting ducts and the generation of a concentrated urine. Inhibition of the thick ascending limb cotransporter will lead to both a greater load of NaCl left behind in the tubular fluid, increasing urinary NaCl levels, and a reduced hypertonicity of the medullary interstitium (less NaCl), decreasing the gradient for water reabsorption from the collecting ducts. This leads to a rapid and sustained increase in urinary volume flow along with significant urinary levels of NaCl. Loop diuretics such as Lasix (furosemide) potently inhibit the Na+-K+-Cl- cotransporter in the thick ascending limb. NaCl reabsorption in the thick ascending limb through this cotransporter is the driving force behind the operation of the countercurrent multiplier and the ability to excrete a concentrated urine (and a diluted urine). Inhibition of this cotransporter leads to a much greater load of Na+ being delivered to the distal tubule and collecting ducts. With the increased delivery of Na+ and fluid to the late distal tubule and cortical collecting ducts, K+ secretion by the late distal tubule and cortical collecting ducts will be enhanced, leading to hypokalemia. Aldosterone-secreting tumors may lead to hypertension, usually causing elevated serum sodium levels and low potassium levels (because of urinary reabsorption of sodium and excretion of potassium). One of the basic tests in the workup of newly diagnosed hypertension is serum electrolytes to assess for this disorder. Loop diuretics are potent diuretics that inhibit the Na+-K+-Cl- cotransporter at the luminal membrane of the thick ascending limb, thereby inhibiting NaCl reabsorption by this segment and water reabsorption by the medullary collecting ducts. Administration of loop diuretics or other "upstream" diuretics can lead to increased tubular fluid flow to the late distal tubule and collecting ducts which, in turn, may stimulate K+ secretion and the development of hypokalemia. Potassium-sparing diuretics such as amiloride and spironolactone inhibit Na+ reabsorption and, in turn, K+ secretion by the late distal tubule and collecting ducts.
Category 2: A well-defined corneal dystrophy that has been mapped to one or more specific chromosomal loci impotence 19 year old cheap 20 mg levitra soft mastercard, but the gene(s) remains to be identified erectile dysfunction pills otc levitra soft 20 mg purchase with mastercard. Category 3: A well-defined corneal dystrophy in which the disorder has not yet been mapped to a chromosomal locus icd 9 code erectile dysfunction neurogenic buy levitra soft us. Category 4: Reserved for a suspected new erectile dysfunction treatment natural way purchase levitra soft in united states online, or previously documented erectile dysfunction miracle cheap 20 mg levitra soft amex, corneal dystrophy, although the evidence for its being a distinct entity is not yet convincing. The category assigned to a corneal dystrophy may change with time as more information about it is obtained. Gray patches, microcysts, and/or fine lines in the corneal epithelium are seen on examination. These are usually best seen with sclerotic scatter, retroillumination, or a broad tangential beam. Fingerprint lines are thin, relucent, hairlike lines; several of them can be arranged in a concentric pattern so they resemble fingerprints. Maps and fingerprints consist of thickened or multilaminar strips of epithelial basement membrane. Symptoms that are related to recurrent epithelial erosions and to transient blurred vision are more common in patients older than 30 years but can be seen at any age. Basement membrane changes in the visual axis can cause irregular astigmatism and blurred vision. Unilateral epithelial basement membrane changes may be related to localized trauma rather than a dystrophy. In some cases, clinical findings may mimic corneal intraepithelial dysplasia, and removed material should be submitted for histology. There are frequent mitoses and a thickened basement membrane with projections into the basal epithelium; the basal epithelial cells have increased glycogen. On confocal microscopy, hyporeflective areas are seen in the basal epithelium ranging from 40 to 150 m in diameter, with potential reflective spots inside. Tiny epithelial vesicles are seen-most easily with retroillumination-extending out to the limbus. Imaging the microstructural abnormalities of Meesmann corneal dystrophy by in vivo confocal microscopy. On immunohistochemistry, there is scattered staining on Ki67 without evidence of increased mitotic activity. In Meesmann dystrophy, such band-shaped, feathery lesions do not exist, and the corneal involvement is more diffuse. Also, the intraepithelial cysts of Meesmann are not as densely crowded as in Lisch dystrophy but are isolated, with clear spaces between the cysts. Lisch corneal dystrophy is genetically distinct from Meesmann corneal dystrophy and maps to xp22. Retroillumination shows sectorial, densely crowded clear microcysts in a feathery shape. Disruption of epithelial tight junctions leads to abnormally high epithelial permeability. Amyloid deposition is noted in the basal epithelial layer on transmission electron microscopy. There is a significant decrease in vision, with photophobia, irritation, and tearing, and a progression of protruding subepithelial lesions. Soft contact lenses are effective in managing the abnormal epithelial permeability to decrease recurrences. A spectrum of clinical manifestations of gelatinous droplike corneal dystrophy in Japan. Epithelial barrier function and ultrastructure of gelatinous drop-like corneal dystrophy. The basal epithelial cell layer shows high reflectivity from small granular material without any shadows. Confluent, irregular, and coarse geographic opacities with varying densities develop at the level of the Bowman layer and superficial stroma, mostly centrally. Symptoms often begin in the first or second decade of life with painful recurrent epithelial erosions. Vision is reduced by both anterior scarring with surface irregularity and anterior stromal edema. The Bowman layer is replaced by fibrocellular material in a pathognomonic wavy, "saw-toothed" pattern. On confocal microscopy, distinct deposits are found in the epithelium and Bowman layer. The deposits in the basal epithelial cell layer show reflectivity, with round edges and dark shadows. Recurrent erosions cause ocular discomfort and pain, with worsening of vision from corneal opacification. Amyloid may also accumulate in the subepithelial area, giving rise to poor epithelialstromal adhesion. Epithelial atrophy and disruption, with degeneration of basal epithelial cells, and focal thinning or absence of the Bowman layer increase progressively with age. An eosinophilic layer between the epithelial basement membrane and Bowman layer develops, with stromal deposition of the amyloid substance distorting the corneal lamellar architecture. Amyloid stains rose to orange-red with Congo red dye and metachromatically with crystal violet dye, and it exhibits dichroism and birefringence. Electron microscopy reveals extracellular masses of fine 810m fibrils that are electrondense and randomly aligned. In vivo confocal microscopy reveals characteristic linear images that should be differentiated from those seen in infection with fungal hyphae. The spectrum of corneal changes is broad, and the classic branching lattice figures may not be present in all cases. Refractile lines, central and subepithelial ovoid white dots, and diffuse anterior stromal haze appear early in life. These lines start centrally and superficially and spread centrifugally and deeper. The stroma can take on a groundglass appearance, but the peripheral cornea remains clear. It is thought that lattice dystrophy recurs more frequently after grafting than does granular or macular dystrophy. One study suggested that granular dystrophy recurred more often than lattice; the study, however, had a 5-year follow-up; the mean time of recurrence for lattice is 9 years (range, 326 years). The mutated gelsolin is seen deposited in the conjunctiva, sclera, and ciliary body, along the choriocapillaris, in the ciliary nerves and vessels, and in the optic nerve. Extraocularly, amyloid is detected in arterial walls, peripheral nerves, and glomeruli. On confocal microscopy, deposits are seen along the basal epithelial cells and stromal nerves. The classic corneal lattice lines are less numerous and more peripheral, and they spread centripetally from the limbus. Histochemically, the deposits are noncollagenous protein that may derive from the corneal epithelium and/ or keratocytes. The dystrophy is slowly progressive, with most patients maintaining good vision and visual acuity only rarely dropping to 20/200 after age 50. Recurrent erosions occur and vision decreases as the opacities become more confluent. Recurrent erosions may be treated with therapeutic contact lenses and superficial keratectomy. Recurrence in the graft (anteriorly and peripherally) may occur after many years as fine subepithelial opacities varying from the original presentation. Rodshaped bodies are seen on electron microscopy, as are randomly aligned fibrils of amyloid. Determination of treatment strategies for granular corneal dystrophy type 2 using Fourier-domain optical coherence tomography. Stellate-shaped opacities with intervening clear spaces can be seen in retroillumination. They accumulate in the endoplasmic reticulum and not in lysosomal vacuoles, as seen in systemic mucopolysaccharidoses. On confocal microscopy, blurred accumulations of light-reflective material are seen in the anterior corneal stroma. Unlike most corneal dystrophies, it has an autosomal recessive inheritance, involves the entire corneal stroma and periphery, and may involve the corneal endothelium. Patients with macular dystrophy show focal, gray-white, superficial stromal opacities that progress to involve full stromal thickness and extend to the corneal periphery. Involvement of the Descemet membrane and endothelium is indicated by the presence of cornea guttae. Epithelial erosions are possible, but symptoms usually involve a decrease in vision, between the ages of 10 and 30. There are 3 variants of macular dystrophy, and they are distinguished based on biochemical differences. Errors occur in the synthesis of keratan sulfate and in the activity of specific sulfotransferases involved in the sulfation of the keratan sulfate lactose aminoglycan side chain. This test can help in the diagnosis of macular dystrophy, even in preclinical forms and carriers. Recurrent erosions are treated like other stromal dystrophies, and photophobia may be reduced with tinted contact lenses. Pathologically, the opacities are accumulations of unesterified and esterified cholesterol and phospholipids. In the normal process of embedding tissue in paraffin, cholesterol and other fatty substances are dissolved; therefore, the pathologist must be made aware of the requirement for special stains. Electron microscopy shows abnormal accumulation of lipid and dissolved cholesterol in the epithelium, in the Bowman layer, and throughout the stroma. Confocal microscopy reveals disruption of the basal epithelial/subepithelial nerve plexus, with highly reflective intracellular and extracellular deposits. However, diagnosis is usually made by the second or third decade, although it may be further delayed in patients who have the acrystalline form of the disease. Central subepithelial crystals are seen in only 50% of patients and do not involve the epithelium. Abnormal serum lipids are managed by diet and/or medication but do not affect the progression of the corneal dystrophy. Most patients have elevated serum cholesterol levels that often respond to dietary therapy or medication. Visual morbidity in thirty-four families with Schnyder crystalline corneal dystrophy (an American Ophthalmological Society thesis). On electron microscopy, the collagen fibril diameter is about half the normal size in all lamellae. Abnormal lamellar layers consisting of thin filaments arranged in an electron-lucent ground substance separate the lamellae of normal appearance. The course is nonprogressive or slowly progressive, with moderate to severe vision loss. Congenital stromal dystrophy of the cornea caused by a mutation in the decorin gene. Transmission electron microscopy shows membrane-based inclusions with delicate granular material. Confocal microscopy shows an accumulation of pathologic material in stromal cells and inclusions in the basal nerves. Fleck dystrophy may be associated with decreased corneal sensation, limbal dermoid, keratoconus, central cloudy dystrophy, punctate cortical lens changes, pseudoxanthoma elasticum, or atopy. On electron microscopy, there is disorganization of the posterior stromal lamellae. On confocal microscopy, there are microfolds and a hyperreflective layer in the posterior stroma. The cornea is flat (<41 D) and thin (as low as 380 m) and there is associated hyperopia. Focal endothelial abnormalities have been observed, as have a prominent Schwalbe line, fine iris processes, pupillary remnant, iridocorneal adhesions, corectopia, pseudopolycoria, and anterior stromal tags. On electron microscopy, there are membrane-bound intracellular vacuoles containing electron-dense material suggestive of secondary lysosomes, and there are inclusions consistent with lipofuscin-like lipoprotein, suggesting a degenerative process. Onset is usually after age 30, but it has been reported in children as young as 3 years. Primary dysfunction of the endothelial cells manifests as increased corneal swelling and deposition of collagen and extracellular matrix in the Descemet membrane, which is thickened. It is not clear whether the reduction in the posterior nonbanded zone and the increase in thickness of the posterior banded zone (posterior collagenous layer) are primary effects of endothelial dysfunction or are secondary to chronic corneal edema. As the endothelium further decompensates, the central corneal thickness may approach 1 mm (0. Epithelial edema develops, leading to microcystic edema; this later progresses to epithelial bullae, which may rupture. Fuchs usually presents in the fifth or sixth decade of life (except for the early-onset variant, which may present in the third decade or earlier). Symptoms are rare before age 50 and are related to the edema, which causes a decrease in vision, as well as pain secondary to ruptured bullae. Symptoms are often worse upon awakening because of decreased surface evaporation during sleep.
A trephine is centered over the pupil and used to incise the previously made flap to a depth slightly below the initial lamellar dissection erectile dysfunction vitamin e buy generic levitra soft from india, ideally leaving a 1-mm flap rim impotence from alcohol cheap 20 mg levitra soft with visa. A blunt spatula is gently introduced at the plane of the lamellar flap erectile dysfunction ultrasound protocol discount levitra soft 20 mg line, and the abnormal tissue is separated and lifted off erectile dysfunction epilepsy medication cheap levitra soft 20 mg buy on-line. The donor tissue is then prepared using an artificial anterior chamber and a microkeratome with the same thickness head as in the initial procedure impotence at 46 buy levitra soft 20 mg mastercard. The donor disk is then transferred to the host bed and, if there is a good match, the donor tissue may adhere spontaneously without sutures, although 10-0 nylon sutures can be used to anchor the graft and ensure proper alignment. In the 2-stage approach, the diameter of the host bed can be matched precisely with the diameter of the donor tissue with nice vertical incisions from trephination. Recently, the femtosecond laser has been used to perform the lamellar dissections of both the host and donor tissue in a single session. Deep anterior lamellar keratoplasty To obtain the best visual outcome, the interface must be smooth and clear, and almost all host stromal tissue must be removed. The Anwar big-bubble technique is the most widely used method of isolating Descemet membrane. If a big bubble cannot be produced, manual dissection is possible, but it risks loss of best-corrected visual acuity due to incomplete removal of the host stromal tissue. Depending on surgeon preference, the anterior lamellae may be dissected and removed, leaving a thin layer of stroma, or left untouched. A tunnel is then fashioned from the deepest point of the trephination incision, extending 23 mm to the paracentral cornea and running parallel to the surface of the cornea to avoid perforation of Descemet membrane. Air is forcefully injected into the stroma and, hopefully, enters the pre-Descemet plane. If this step is successful, an air bubble outlined by a circular white band will suddenly appear. A limbal paracentesis is made to drain aqueous humor from the eye in order to reduce the pressure and help prevent perforation of the cornea while exposing Descemet membrane. The anterior wall of the bubble is then entered with a sharp 15° blade to create a 1-mm opening. Once incised, the bubble collapses; some surgeons then inject viscoelastic material into the collapsed bubble to help with the meticulous dissection. When the spatula is lifted anteriorly, the stroma on the top of the spatula is incised using a sharp blade. Inadvertent entry is not infrequent early in the learning curve, and it happens occasionally among experienced surgeons. The donor tissue is prepared by punching an appropriate-sized button with a trephine. Trypan blue can be used to stain the endothelium to improve visualization in order to facilitate the removal of Descemet membrane and endothelium from the donor tissue. Postoperative Care and Complications Double anterior chamber or Descemet detachment Descemet detachment or pseudodouble anterior chambers can occur because of fluid in the interface from a microperforation or retained viscoelastic material. Injection of air into the anterior chamber can help with resolution of the detachment; however, it may also reduce endothelial cell count and lead to the development of an anterior subcapsular cataract. Opacification and vascularization of the interface Meticulous irrigation and cleaning of the lamellar bed at the time of surgery reduces the likelihood of opacification. Retained interface debris, secondary vascularization, microbial infections, or wrinkles of Descemet membrane can reduce vision or prolong vision rehabilitation. Because the endothelium is not transplanted, endothelial rejection cannot take place. However, epithelial rejection, subepithelial infiltrates, and stromal rejection can occur, but these usually respond to corticosteroid therapy. Inflammatory necrosis of the graft Although inflammatory necrosis of the graft has previously been described as an allograft reaction, no immunohistopathologic evidence has confirmed this, and recent series have not shown this phenomenon. Prognosis following retention of a clear graft is poor despite corticosteroid therapy. Quality of vision and graft thickness in deep anterior lamellar and penetrating corneal allografts. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty: a report by the American Academy of Ophthalmology. Endothelial Keratoplasty Gerrit Melles introduced the technique of posterior endothelial lamellar keratoplasty in 1998. The tissue is marked to outline the microkeratome incision and assure proper centration of the cut to avoid thick edges and the possibility of including peripheral donor epithelium. A trephine is used to create a disk-shaped lamella of donor tissue from 8 to 9 mm in diameter. Several studies using vital dye staining of the endothelium after insertion of the donor corneal tissue have shown that placing tissue through a 3-mm incision causes more damage to the endothelium than using a 5-mm incision, regardless of the technique used to place the tissue. This maneuver can be performed with a variety of instruments, including a hook, a specially designed Descemet stripper, or an irrigation/aspiration handpiece. The stripping can be performed under viscoelastic, air, or irrigation with balanced salt solution. Whether the retention of Descemet membrane in these cases may predispose to dislocation of the graft is controversial. The goal is to minimize trauma to the donor endothelium during the insertion and positioning of the tissue in the anterior chamber. In one technique, the tissue can be placed on a sheet glide or the conjunctiva over a bed of viscoelastic and then pushed or pulled into the anterior chamber using forceps or a bent 27-gauge needle. Another popular technique is to fold the tissue using specially designed forceps to minimize tissue compression. Retrospective series comparing endothelial cell loss with different techniques and devices are now being reported; however, at this time, there is no clear consensus on which technique is best. It is not clear what factors are responsible for tissue adherence, but it is probably due to a combination of physical and physiologic factors. B, Glide insertion of donor tissue (left); Busin glide insertion of donor tissue incisions, and sweeping the surface of the cornea with a (right). The air fill duration and pressure necessary to donor graft to the host stromal bed. Comparison of donor insertion techniques for Descemet stripping automated endothelial keratoplasty. Endothelial keratoplasty: the influence of insertion techniques and incision size on donor endothelial survival. On the first postoperative day, the lenticule should be well centered, without fluid in the interface. Some surgeons discontinue the topical corticosteroids after 1 year to reduce the incidence of steroid-induced ocular hypertension or cataract formation; however, in one recent report, graft rejection increased at 1218 months after cessation of the steroid drops. Other clinicians use the topical corticosteroids indefinitely, particularly in pseudophakic patients. Dislocation of the donor graft occurs primarily within the first 24 hours, but occasionally, inadvertent trauma from eye rubbing or a sudden blow to the eye has caused the donor disk to be displaced at a later time. The dislocation is managed with reinjection of air, which can be performed in the office or in the operating room, scheduled when convenient. Spontaneous reattachment of both partial and fully dislocated lenticules has been reported. In rare cases, epithelial ingrowth may lead to graft failure that is missed on clinical examination but recognized on histologic examination of the tissue after removal. The source of the ingrowth may be host surface epithelial cells implanted within the eye during placement of the donor tissue or donor epithelial cells inadvertently left in place and implanted following eccentric trephination beyond the microkeratome dissection. In most reports, the prognosis with epithelial ingrowth is benign and the condition can simply be observed without further intervention. Epithelial ingrowth after Descemet stripping automated endothelial keratoplasty: description of cases and assessment with anterior segment optical coherence tomography. Interface opacification may occur because of retention of fibers, incomplete removal of Descemet membrane, calcareous deposition, and persistent interface fluid. In most patients, the textural interface opacity improves or disappears completely over time with improvement in visual acuity. The underlying cause is believed to be either retained viscoelastic or shearing of the stromal fibrils due to an irregular lamellar microkeratome cut of the donor tissue. Preexisting basement membrane changes may cause superficial irregularity or subepithelial fibrosis. Another potential factor is light scattering due to preexisting long-standing corneal edema. Another possible cause for decreased vision is alteration of the posterior corneal curvature due to the unevenness and thickness of the donor tissue on the host posterior stroma. Corneal haze determined by confocal microscopy 2 years after Descemet stripping with endothelial keratoplasty for Fuchs corneal dystrophy. Quality of vision in patients with Fuchs endothelial dystrophy and after Descemet stripping endothelial keratoplasty. Phakic Descemet stripping automated endothelial keratoplasty: prevalence and prognostic impact of postoperative cataracts. The primary graft failure rate seen in published reports varies between 3% and 12%; higher rates are associated with surgeons in the early stages of the learning curve, and lower rates are associated with more experienced surgeons. The lower rates probably reflect better surgical technique, which results in less tissue manipulation and a lower rate of graft dislocations and thus less endothelial trauma. The lower incidence may be related to the lack of corneal sutures, which reduces the risk of inflammation due to suture erosion and secondary vascularization. However, the extended learning curve, the increased risk of loss of donor tissue during preparation, the increased difficulty of intraocular manipulation of the thin and friable tissue (increasing endothelial cell loss), and the increased incidence of graft detachment have made it a more challenging technique for the cornea surgeon but one that is increasingly utilized. This finding suggested that endothelial migration across the posterior cornea could lead to restoration of corneal clarity. In this setting, descemetorrhexis with implantation of donor tissue may stimulate migration of host or donor endothelial cells, although whether the donor tissue interacts with the host endothelial cells or serves as the source of the endothelial cells is unknown. This raises the possibility that in patients with an abnormal Descemet membrane (Fuchs and posterior polymorphous dystrophy), replacement of the abnormal Descemet membrane with freefloating donor tissue may stimulate migration of endothelial cells either from the donor tissue or from the peripheral host endothelium. In another report, corneal clearance occurred without placement of a ny tissue after removal of Descemet membrane and endothelium, suggesting that it may not be necessary to use donor tissue at all to stimulate migration of the peripheral host endothelial cells. Adaptive (or acquired) responses are higher-order specific responses directed against unique antigens and will be discussed in detail in Chapter 2. Innate immune responses, or natural immunity, require no prior contact with or "education" about the stimulus against which they are directed. This chapter introduces the crucial cells of the immune system and discusses their functions in innate immunity. Neutrophils feature cytoplasmic granules and lysosomes and are the most abundant granulocytes in the blood. They are efficient phagocytes that readily clear tissues and degrade ingested material and act as important effector cells through the release of granule products and cytokines. Neutrophils dominate the infiltrate in experimental models and clinical examples of active bacterial infections of the conjunctiva, sclera (scleritis), cornea (keratitis), and vitreous (endophthalmitis). Neutrophils constitute the principal cell type in ocular inflammation induced by lipopolysaccharides (discussed later) and after direct injection of most cytokines into ocular tissues. Eosinophils Eosinophils, a second type of polymorphonuclear leukocyte, also contain abundant cytoplasmic granules and lysosomes, but the biochemical nature of eosinophilic granules consists of more basic protein (thus acidic dyes, such as eosin, will bind to these proteins). Eosinophils are abundant in the conjunctiva and tears in many forms of atopic conjunctivitis, especially vernal and allergic conjunctivitis. Basophils and mast cells Basophils are the blood-borne equivalent of the tissue-bound mast cell. Mast cells exist in 2 major subtypes-connective tissue and mucosal-both of which can release preformed granules and synthesize certain mediators de novo that differ from those of neutrophils and eosinophils. In contrast, mucosal mast cells require T-lymphocyte cytokine help for granule formation, and they normally contain low levels of histamine. They perform this function through their expression of high-affinity Fc receptors for immunoglobulin E (IgE). Fc (from "fragment, crystallizable") refers to the constant region of immunoglobulin that binds cell surface receptors (see Chapter 2). Other stimuli, such as complement or certain cytokines, may also trigger degranulation. The uveal tract also contains numerous connective tissuetype mast cells, whereas the cornea has none. Monocytes and macrophages Monocytes, the circulating cells, and macrophages, the tissue-infiltrating equivalents, are important effectors in all forms of immunity and inflammation. Monocytes are relatively large cells (1220 µm in suspension but up to 40 µm in tissues) that normally travel throughout the body. Most tissues have at least 2 identifiable macrophage populations: tissue-resident and blood-derived. Macrophages are extremely important effector cells in adaptive and innate immunity. Only after full activation do macrophages become most efficient at the synthesis and release of inflammatory mediators and the killing and degradation of phagocytosed pathogens. Lymphocytes Lymphocytes are small (1020 µm) cells with large, dense nuclei that are also derived from stem cell precursors within the bone marrow. Unlike other leukocytes, however, lymphocytes require subsequent maturation in peripheral lymphoid organs. Lymphocytes can be subdivided by the expression of specific cell-surface proteins (ie, surface markers). These markers are in turn related to the functional and molecular activity of individual subsets. Three broad categories of lymphocytes have been identified: T lymphocytes; B lymphocytes; and non-T, non-B lymphocytes. The innate immune response requires no prior exposure to the foreign substance and is similar for all encountered triggers. The result is the generation of biochemical mediators and cytokines that recruit innate effector cells, especially macrophages and neutrophils, to remove the offending stimulus through phagocytosis or enzymatic degradation. For example, in endophthalmitis, bacteria-derived toxins or host cell debris stimulates the recruitment of neutrophils and monocytes, leading to the production of inflammatory mediators and phagocytosis of the bacteria.
In the emergency center valium causes erectile dysfunction cheap levitra soft online amex, the patient is lethargic and confused with a low-grade fever and is hyperventilating erectile dysfunction treatment phoenix buy levitra soft amex. Her urine drug screen is negative reasons erectile dysfunction young age levitra soft 20 mg order line, but the arterial blood gases reveal an anion gap metabolic acidosis top erectile dysfunction pills buy 20 mg levitra soft, probably as a result of the aspirin overdose impotence from smoking order generic levitra soft on-line. An increase in the rate of production (eg, lactic acid or ketoacids) or ingestion of noncarbonic acids or substances that increase lactic acid or ketoacid production will cause a decrease in the plasma concentration of bicarbonate. The anion gap helps identify the type of acidosis and estimate the magnitude of the acid load to the system. Chemoreceptors involved in response to an acidbase disturbance: Two groups of chemoreceptors respond to a metabolic acidosis: 1. A thorough history and physical examination often will reveal clues necessary to make the diagnosis. In this case, the history of depression with stressful final examinations coming up and an empty bottle of recently purchased aspirin make one think of the possibility of salicylate poisoning. Salicylate poisoning may cause clinical symptoms of vomiting, sweating, tachycardia, fever, lethargy confusion, coma, seizures, cardiovascular collapse, and possibly pulmonary or cerebral edema. Salicylate ingestion can cause a multitude of effects, depending on the magnitude of the ingestion. Abnormal laboratory findings may include anion gap metabolic acidosis, hypokalemia, hypoglycemia, and a positive urine ferric chloride test. Other agents are also possible, including acetaminophen, alcohol, and illicit drugs. Treatment of salicylate toxicity includes activated charcoal to decontaminate the stomach (possibly gastric lavage), correction of Elevated levels of salicylates increase the sensitivity of the respiratory center in the brain. The metabolic acidosis results in hyperventilation and a compensatory respiratory alkalosis. Definitions Respiratory center: Located in the reticular formation of the medulla it is responsible for maintaining a rhythmical cycle of breathing and integrating neural input from a variety of receptors. Acidbase disturbances are generally identified as being of respiratory or metabolic origin. Respiratory acidbase disorders are a consequence of a respiratory disturbance that results in a change Until the disturbance is corrected, renal function will compensate the disruption. This case involves a metabolic acidosis caused by the ingestion of an acidic substance. Respiration is spontaneously and rhythmically initiated by the respiratory center located in the reticular formation of the medulla. Neural signaling to the inspiratory and expiratory muscle groups maintains the cycle of breathing. Numerous mechanisms are capable of modifying the signal to alter the frequency and depth of breathing in response to voluntary stimuli, reflexes and other neural stimuli, and a variety of chemical or mechanical stimuli. Impulses from the peripheral chemoreceptors are carried by the glossopharyngeal nerve to the respiratory center. Stimulation of the peripheral chemoreceptors causes an increase in ventilatory rate. Central chemoreceptors located on the medulla are separated from the blood by the bloodbrain barrier. This important control mechanism serves to dampen the respiratory response to an acidbase disturbance. In the present case of salicylate intoxication, there also may be a direct stimulation of the respiratory center that will cause a further increase in the respiratory rate with a resultant respiratory alkalosis (hypocapnia) superimposed on the metabolic acidosis. This example emphasizes the importance of the interactions between the central and peripheral chemoreceptors. In disorders in which one or the other chemoreceptor is blocked or nonfunctional, severe aberrations in breathing patterns are observed. In addition to the chemoreceptors outlined above, there are three receptor groups that are located in the lungs. J-receptors (juxtapulmonary capillary receptors) are located in the interstitium near alveoli and blood capillaries. Increasing pressure in the interstitium by edema or capillary engorgement stimulates J-receptors, causing bronchoconstriction and tachypnea. They are located in such a way that they have immediate contact with inhaled air and are stimulated by cigarette smoke, dust, fumes, and cold air. Stimulation of irritant receptors leads to bronchoconstriction, hyperpnea, coughing, and sneezing. Pulmonary stretch receptors are located in airway smooth muscle and are stimulated by distention of the lung and serve to protect the lungs against being overinflated. The cause of the hyperventilation is described by which of the following statements Administration of oxygen by mask Administration of benzodiazepine for possible alcohol withdrawal Leaving the patient on room air Placing the patient on a low opiate infusion to prevent opiate withdrawal [20. Which of the following statements best describes his condition after the elevation climb To the contrary, as soon as the peripheral chemoreceptors sense an increase in the H+, there will be an immediate increase in the rate of ventilation. This is the appropriate compensatory response because the initial perturbation was a decrease in the bicarbonate concentration from the acid insult. The only drive for ventilation is the fall in O2 resulting from the near cessation of breathing. Applying oxygen will remove the remaining drive for ventilation, and breathing will stop. Medications that further suppress respirations, such as sedatives (benzodiazepines, opiates, hypnotics), are contraindicated. At the time of admission, his abdomen had some bruising but no distention or tenderness. His blood pressure is normal but lower than it was when he presented to the hospital, and he has a slightly increased heart rate. The surgeon makes a diagnosis of hypovolemia that probably is caused by intraabdominal hemorrhage and prepares the patient for exploratory surgery. What is the response of the juxtaglomerular cells to decreased extracellular fluid and arterial pressure Often after surgery or trauma, a Foley catheter is placed in the bladder to measure urine output accurately. Decreasing urine output may be because of hypovolemia or injury to the urinary tract system. In this case, the decreased urine output probably was secondary to hypovolemia, because the patient also has hypotension and tachycardia. The blood pressure remained relatively normal initially because of the renin-angiotensin system, which sensed the decreased blood flow to the renal artery, and the sympathetic nervous system, which sensed the decreased blood volume and pressure. Decreased blood volume and pressure will be sensed by volume and pressure receptors, leading to modest vasoconstriction and increased systemic blood pressure. With excessive blood loss (hypovolemic shock), the action of the autonomic (sympathetic) nervous system causes pronounced vasoconstriction of the renal arteries with shunting of blood to vital organs (brain, heart, lungs) and is seen clinically with decreased urine output. Replacement with crystalloid fluids and blood is necessary to maintain kidney perfusion and prevent acute tubular necrosis. In any case, the source of bleeding must be addressed and intravascular volume must be replaced. Autoregulation: the maintenance of normal blood flow to an organ during periods of altered arterial pressure. Typically, under conditions of volume expansion (eg, drinking a liter of water), urine output is increased, whereas under conditions of volume depletion (eg, hemorrhage, profuse sweating) urine output is decreased. In this case, the patient probably has had an intraabdominal hemorrhage during trauma that has led to modest volume depletion. The renal system responds by reducing urine output in an attempt to maintain volume-water balance. As this case demonstrates, several mechanisms come into play to regulate urine output during volume depletion, including the sympathetic nervous system, volume-sensitive hormonal systems, and intrinsic autoregulator mechanisms. Although the mechanism of this response is not fully understood, it appears to be predominantly related to myogenic stretch receptors in the wall of the afferent arteriole, similar to what is observed in precapillary sphincters in muscle capillaries during autoregulation of muscle blood flow. The efferent arteriole does not appear to be involved in the autoregulation mechanisms. The elevated pressure in the afferent arteriole stretches the arteriole, causing the arteriole to respond, inducing constriction. Conversely, under conditions of depressed mean arterial pressure, such as observed The reduced pressure decreases the stretch of the afferent arteriole, causing the arteriole to respond, inducing dilation. These cells are juxtapositioned to their own afferent arteriole and control constriction of the arteriole. Extrinsic factors play a significant role in regulating renal function during both hypo- and hypervolemia and normally overpower the intrinsic autoregulatory mechanisms. In hypovolemic states, the reduction in blood volume results in reduced renal blood flow and reduced hydrostatic pressure along the renal vasculature. The decrease in pressure in the afferent arteriole is sensed by baroreceptors in the afferent arteriole, leading to stimulation of renin release from the juxtaglomerular cells of the afferent arteriole (increased sympathetic activity also increases renin release). Aldosterone, in turn, acts on the renal distal tubule and cortical collecting ducts to enhance sodium (and chloride) reabsorption, leading to salt retention and an associated retention of water with a corresponding decrease in urine output. The sympathetic nervous system also is intimately involved in regulating renal function during alterations in volume balance. Volume depletion will be accompanied by a decrease in blood volume and venous return to the heart that will be sensed by baroreceptors (volume receptors) in the atria and pulmonary veins and pressure receptors in the renal afferent arteriole, leading to increased sympathetic activity. This will result in sympathetically mediated vasoconstriction and partial return of mean arterial pressure toward normal. If blood volume depletion is modest-less than 10% of blood volume-the changes are modest, but will help maintain blood pressure near normal. With more severe cases of hypovolemia (15% to 25% blood loss), there is a more pronounced sympathetic-mediated vasoconstriction. Conversely, during volume expansion, baroreceptors will sense an increase in blood volume and mean arterial pressure, leading to a decrease in sympathetic activity which, in turn, will lead to vasodilation and a return of blood pressure toward normal. Both of these components are filtered at the glomerulus and excreted in the urine. His doctor suspects that the patient may be developing renal insufficiency that is leading to a reduced glomerular filtration and, as a result, hypervolemia and hypertension. The kidneys respond by reducing urinary volume flow, thus limiting the potential extent of hypovolemia. Increases in the plasma levels of which of the following hormones will bring about the most dramatic decrease in urinary volume flow rate Elevated serum sodium Elevated serum osmolarity Elevated urine sodium Elevated urine catecholamines Answers [21. Both the renal afferent and efferent arterioles are innervated with sympathetic nerves that regulate contraction and dilation of the arterioles. Aldosterone regulates the reabsorption of sodium (and chloride) from the distal tubule and the cortical collecting duct, bringing about retention of salt and water and an increase in extracellular fluid volume. A 1-hour glucose challenge test is performed along with her other prenatal laboratories, and they are all normal. Where in the renal glomerulus-tubule structure is glucose reabsorbed actively (secondary active transport) Other actively reabsorbed solutes: Organic acids, amino acids, proteins and peptides, phosphate, and sulfate. The glycosuria acts as an osmotic diuretic and leads to the common symptoms of uncontrolled diabetes: urinary frequency, nocturia, and frequent thirst. The presence of glycosuria is not suggestive of gestational diabetes, and a 1-hour diabetic screen must be performed to rule out that disease. Describe the role of sodium with reabsorption of organic acids, amino acids, and proteins. Definitions Glycosuria: A condition characterized by the appearance of glucose in the urine. Aldosterone induces the synthesis of a myriad of new proteins in the late distal tubule and cortical collecting duct, including the synthesis of new Na+ channels and Na+ pumps. Regulation of sodium balance and extracellular fluid volume, and renal regulation of potassium, calcium, and magnesium. She has undergone computed tomographic imaging of her head, which revealed cerebral swelling but no evidence of hemorrhage or brain herniation. The nurse calls the physician because the patient has developed hypernatremia and has had a significant increase in dilute urine output. The findings are confirmed, and it is determined that the patient has central diabetes insipidus as a result of the head trauma. Signs and symptoms include polyuria and polydipsia along with the production of dilute urine (< 300 mOsmol/kg). Free-water clearance: the volume of water (urine) cleared from the plasma per unit time in excess (positive free-water clearance) or deficit (negative free-water clearance) from the volume estimated if the urine were isosmotic (with plasma) for the given amount of solute excreted in the same time. A quantitative measure of how dilute (hypotonic) or concentrated (hypertonic) the urine is (milliliters of water/time) relative to the isosmotic state. Daily urine output is highly variable, related to water and food intake, with typical urine volumes of 1 or 2 L (osmolalities of 200-500 mOsmol/kg or so). The water permeability of the cortical and medullary collecting ducts is relatively low in the basal state, primarily because of the low water permeability of the luminal (apical) cell membrane of the principal cells. After phosphorylation, the vesicles move to and fuse with the luminal cell membrane, increasing the water permeability of the luminal membrane. In the cortical collecting duct, water then can be reabsorbed passively from the hypotonic luminal fluid (typically near 100 mOsmol/kg as fluid enters the cortical collecting duct) across the luminal border into the cell. The basolateral membrane normally has significant water permeability as a result of constitutive expression of other aquaporins (typically aquaporins 3 and 4). Hence, as water moves across the luminal border by osmosis, modestly reducing the osmolality of the cytoplasm, the water will diffuse from the The osmotic reabsorption of water in the cortical segment of the collecting duct serves to present a smaller volume, but near isosmotic fluid, to the medullary collecting ducts so that water reabsorption in the medullary segment continues without a major reduction in the hypertonicity of the medullary interstitium. Water reabsorption continues, increasing the tubular fluid osmolarity, with the fluid approaching osmotic equilibrium with the medullary interstitium, thereby rendering a small but concentrated urine. A defect in the water channels or in the trafficking of the channel to the luminal membrane will diminish the antidiuretic response, a condition referred to as nephrogenic diabetes insipidus. Hence, the tubular fluid entering the cortical collecting duct (approximately 100 mOsmol/kg) remains hypotonic, leading to excretion of copious but dilute urine (a diuresis). The granules migrate down the axons of the supraopticohypophysial tract into the posterior pituitary and are stored in the nerve terminals, from where they are released into the plasma.
Generic levitra soft 20 mg without prescription. Enhancement Drug - SNL.
References
- Birk DE, Nurminskaya MV, Zycband EI: Collagen fibrillogenesis in situ: fibril segments undergo post-depositional modifications resulting in linear and lateral growth during matrix development, Dev Dyn 202(3):229-243, 1995.
- Tan KK, Grzeszczuk R, Levin DN et al. A frameless stereotactic approach to neurosurgical planning based on retrospective patient image registration. Technical case. J Neurosurg 79: 296-303, 1993.
- Guarda LA, Tran TA. The pathology of breast biopsy site marking devices. Am J Surg Pathol. 2005;29(6):814-819.
- Boyle AJ, Teuteberg JJ, Ascheim DD, et al. LVADs for less acutely ill patients: Do current data justify the strategy? ASAIO 2008;54:A22.
- Steidle CP, Mulcahy JJ: Erosion of penile prosthesis: a complication of urethral catheterization, J Urol 142:736n739, 1989.
- Vera PL, Preston DM, Moldwin RM, et al: Elevated urine levels of macrophage migration inhibitory factor in inflammatory bladder conditions: a potential biomarker for a subgroup of interstitial cystitis/bladder pain syndrome patients, Urology 116:55n62, 2018.