
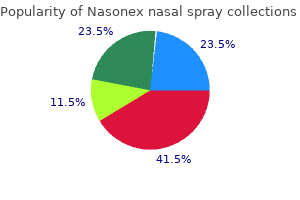
Nasonex nasal spray
| Contato
Página Inicial
Vikram J Anand
- Consultant surgeon
- Kalra Hospital and Sri Ram Cardio-Thoracic
- & Neurosciences Centre,
- New Delhi, India
- Supervisor for postgraduate surgical studies
- The National Board of Examinations,
- New Delhi, India
- Surgical tutor and examiner
- The Royal College of Surgeons of Edinburgh,
- Scotland, UK
- Professor of surgery and former director,
- department of surgery
- Maulana Azad Medical College and
- Associated Hospitals, New Delhi, India
B allergy shots pregnant buy nasonex nasal spray without a prescription, Bilateral inguinal adenopathy allergy medicine erectile dysfunction nasonex nasal spray 18 gm buy mastercard, with developing groove sign as adenopathy expands above and below the inguinal ligament allergy forecast new jersey nasonex nasal spray 18 gm purchase line. Risk factors for infection include young age allergy treatment energy nasonex nasal spray 18 gm buy line, unprotected intercourse allergy treatment for foods order nasonex nasal spray 18 gm with visa, multiple sexual partners, new sexual partners, and sexual activity associated with illicit drug use. It is transmitted through contact with infected secretions, most often sexually, although vertical transmission from mother to infant is well described. Certain gonococcal strains are more likely to cause disseminated gonococcal infections. Symptoms and signs may include fevers, myalgias, arthralgias, asymmetrical polyarthritis, and a characteristic dermatitis consisting of a small number (<30) of skin lesions on the distal extremities that begin as papules and progress to pustules and ulcerations. Vertical transmission to neonates may result in ophthalmia neonatorum, sepsis, arthritis, meningitis, rhinitis, vaginitis, urethritis, and inflammation at the sites of fetal monitoring. Gonococcal infections diagnosed in preadolescent children usually indicate sexual abuse. Culture (usually on ThayerMartin medium) is 95% sensitive in symptomatic men but is less so for asymptomatic men and women (80%90%). Definitive diagnosis of gonorrhea by culture from any genital or extragenital site requires confirmation of isolates by biochemical, enzymatic, serologic, or nucleic acid testing. After the culture is submitted, this type of identification is usually performed by the laboratory without requesting it, and when these methods are used, there should be no pitfalls in interpreting the extragenital culture data. Most commercial laboratories now offer testing of extragenital specimens using nucleic acid amplification. Serologic tests have been used for epidemiologic studies, but they should not be used for diagnosis. Clinical Manifestations Asymptomatic urethral infections occur in at least 30% of men and asymptomatic cervical infections occur in at least 50% of women. More than 50% of rectal and up to 90% of pharyngeal gonorrhea in men and women may be asymptomatic. These numbers highlight the importance of a thorough sexual history in all atrisk patients that focuses on a history of exposure rather than symptoms. Urethral discharge and dysuria are the most frequent signs occurring 2 to 5 days after exposure. Acute epididymitis manifesting as unilateral scrotal pain is the most common local complication. Rarely, cellulitis, lymphangitis, or periurethral abscesses may complicate local infections. Differential diagnosis of urethritis in men includes Chlamydia trachomatis, Mycoplasma genitalium, and Trichomonas vaginalis infections. Among women, the most common manifestation of local gonococcal infection is cervicitis, which tends to occur 5 to 10 days after exposure. When patients are symptomatic, common complaints include a vaginal discharge, dysuria, and genital itching. Concomitant infection of the urethra may occur in up to 90% of women and accounts for some of these symptoms. Among men and women with rectal gonorrhea, those who are symptomatic may complain of rectal discharge, pain, and tenesmus. Most cases of rectal gonorrhea in men result from receptive anal intercourse; some cases in women may result from perineal contamination. Most cases of pharyngeal gonorrhea are asymptomatic; when present, signs and symptoms may include acute pharyngitis, tonsillitis, and cervical lymphadenopathy. Conjunctivitis is rare in adults and usually is a result of self-inoculation from anogenital infections. By the 1980s, widespread resistance to both of these drug classes rendered them all but useless. Subsequently, drug resistance to aminoglycosides, spectinomycin,2 macrolides, trimethoprim-sulfamethoxazole (Bactrim),1 and fluoroquinolones has made the treatment of gonorrhea more challenging. Male condoms, when used correctly and consistently, are highly effective in preventing infection. All sexually active men who have sex with men should be screened annually at all sites of exposure. Up to 20% persons diagnosed with gonorrhea become reinfected in the next few months. Rescreening 3 months after infection is treated is recommended in both men and women. Repeat testing during the third trimester for those at continued risk is recommended. Management of pharyngeal gonorrhea is crucial to prevent the emergence and spread of antibiotic-resistant Neisseria gonorrhoeae. There have been no reports of ceftriaxone-resistant strains in the United States, although strains resistant to oral cephalosporins have been reported. Ceftriaxone (Rocephin), the preferred cephalosporin, is given intramuscularly and is effective for infections at all sites. Cefixime (Suprax) is effective for anogenital infections, but it may have lower efficacy than ceftriaxone for pharyngeal infections. All sexual contacts in the preceding 60 days of index patients should also be treated. For penicillin-allergic patients, treatment of gonorrhea has become more challenging. Spectinomycin has only 80% efficacy in treating pharyngeal gonococcal infections, but spectinomycin is no longer available in the United States. Cases of high-level resistance to azithromycin have been described recently in the United States. Suspected treatment failures should prompt clinicians to obtain cultures and antimicrobial susceptibility testing. Confirmed treatment failures using the preferred ceftriaxone-based regimen should be treated based on antimicrobial susceptibility testing results in consultation with an infectious diseases specialist. To prevent gonococcal ophthalmia neonatorum, 1% silver nitrate aqueous solution, 0. Other potential causes include Mycoplasma genitalium, Trichomonas vaginalis, herpes simplex virus, adenovirus, and urethral trauma. Additionally, although screening commonly occurs in women, empiric treatment without confirmatory testing is routinely extended to sexual partners of those who test positive. Risk Factors Pathophysiology Urethritis is inflammation of the urethra caused by infection or traumatic injury. Immunity to infection is relatively short-lived, contributing to reinfection or persistent infection. The most common complaints are of urethral discharge and/or dysuria, usually appearing 1 to 3 weeks after exposure. Physical examination should include inspection for inguinal lymphadenopathy, ulcers, and/or urethral discharge. Performing the testing on urine avoids invasive sampling of the urethra and may improve patient acceptance. Because most infections in males and females are asymptomatic, screening at-risk individuals is a cornerstone of secondary prevention. The United States Preventive Services Task Force recommends screening all sexually active and pregnant women age 24 or younger; recommends screening women age 25 or older only if they are at increased risk, whether or not they are pregnant; and concludes that there is insufficient evidence to assess benefits and harms of screening in men. The incubation period for gonococcal urethritis is typically shorter and the discharge is more copious and purulent. Recommended first-line agents are azithromycin (Zithromax) 1 g orally in a single dose or doxycycline (Vibramycin) 100 mg orally twice a day for 7 days. Posttraumatic urethritis is 10 times more likely in patients using latex catheters than silicone catheters for intermittent catheterization. Clinical Manifestations Alternative regimens include erythromycin base (Ery-Tab) 500 mg orally four times a day for 7 days; or erythromycin ethylsuccinate (E. Patients with confirmed urethritis in whom test results are not already known or immediately available should also be treated empirically for gonorrhea with ceftriaxone (Rocephin) 250 mg intramuscularly in a single dose. Patients with symptoms of persistent or recurrent infection can be re-treated with the initial regimen if they were not compliant with treatment or have been reexposed to an untreated partner. If the patient was compliant and was not reexposed, he or she should be treated with metronidazole (Flagyl) 2 g orally in a single dose; or tinidazole (Tindamax) 2 g orally in a single dose plus azithromycin (Zithromax) 1 g orally in a single dose. The recent increase in rates has occurred in both men and women, in all regions, in all age groups between 15 and 44 years of age, and in all ethnicities except for Native Hawaiians/Other Pacific Islanders. Increased rates were also seen in men ages 20-29, in the West and South, and in black men. All patients with Chlamydia infection should be screened again 3 to 6 months after treatment. Other risk factors include living in the southern part of the United States or an urban area, young age (20 to 29 years), and being born to a mother infected with syphilis. Reactive arthritis is an uncommon complication in men, as is Reiter syndrome (arthritis, conjunctivitis/uveitis, urethritis, mucocutaneous lesions). Primary infection manifests with signs and symptoms at the site of infection; secondary and tertiary syphilis manifest with systemic signs and symptoms. Syphilis is primarily sexually transmitted but may be transmitted perinatally or through nonsexual cutaneous transmission. Prevention Prevention includes both avoiding initial infection and preventing disease progression through early detection and treatment. Transmission of syphilis can be reduced (although not eliminated) by using condoms. Screening for syphilis in pregnancy combined with treatment of infected women reduces perinatal transmission. The chancre, a painless ulcer with sharp borders, is usually solitary and associated with regional lymphadenopathy. Atypical presentations include extragenital location (most commonly oral or anal) and the presence of pain or multiple lesions. Differential Diagnosis Syphilis, which can affect every organ system, has historically been called the great mimicker. Syphilis is on the differential diagnosis of, most commonly, conditions causing genital ulcers or lesions, conditions causing systemic rashes affecting the palms and soles, conditions causing ocular and otologic manifestations (uveitis, sudden visual changes, hearing loss), and conditions causing dementia, meningitis, or ataxia. Other clinical manifestations include highly infectious flat lesions (condyloma lata), fever, malaise, sore throat, headache, myalgias, alopecia, and, rarely, renal, bone, eye, or liver involvement. Tertiary syphilis is a late manifestation in untreated people and includes neurosyphilis, cardiovascular, and gummatous disease. Cardiovascular syphilis most commonly manifests as aortitis of the ascending aorta. The clinical manifestations of neurosyphilis are numerous and include meningitis with or without vascular involvement, dementia, tabes dorsalis (posterior column involvement with ataxia and bowel and bladder dysfunction), and ocular or otologic involvement. Congenital syphilis has early (birth to 2 years) and late (2 to 20 years) clinical manifestations. Early signs include hepatosplenomegaly, rash, fever, neurosyphilis, pneumonitis, rhinitis, generalized lymphadenopathy, hepatitis, ascites, hematologic disease, renal disease, periostitis, and osteochondritis. Late manifestations (present in 40% of untreated patients) include skeletal deformities, neurologic disease (deafness), dental abnormalities, and ocular abnormalities. Treatment Penicillin G is the preferred treatment for all stages of syphilis; other forms of penicillin (oral penicillin, combinations of benzathine and procaine) are not effective. The stage and extent of clinical disease determine which preparation is used, the dosage, and the length of treatment (Table 1). In penicillin-allergic patients, antibiotic alternatives exist for all types and stages of syphilis except for syphilis in pregnancy and congenital syphilis. Alternative treatment of primary and secondary syphilis and early latent syphilis includes doxycycline (Vibramycin) 100 mg orally twice a day or tetracycline 500 mg orally four times daily for 14 days. Penicillin-allergic patients with late latent syphilis can be treated with doxycycline 100 mg orally twice daily or tetracycline 500 mg orally four times daily for 28 days, recognizing that there is limited data to support this treatment. Treatment of pencillin-allergic patients with tertiary syphilis should be done is consultation with a specialist. The Jarisch-Herxheimer reaction is an acute febrile reaction (with accompanying headache, myalgias, and other symptoms) occurring within 24 hours of treatment of syphilis. Diagnosis Diagnostic evaluation of syphilis depends on the stage and location of suspected infection. Darkfield microscopy or direct fluorescent antibody testing is done on tissue or exudates obtained from an ulcer or chancre (primary infection). Nontreponemal testing may be falsely positive with other medical conditions, but antibody titers correlate with disease activity and therefore can indicate response to treatment. Treponemal tests are specific for syphilitic infection but usually stay reactive regardless of treatment or disease status. Treponemal test antibody titers do not match the level of disease activity and therefore cannot be used to monitor treatment response. Reverse screening has been used in which a treponemal specific test is the initial screening test, followed by a non-treponemal test. Neurosyphilis is diagnosed based on clinical signs and symptoms using laboratory testing to support a clinical diagnosis. Laboratory testing includes reactive 887 Monitoring No definite criteria exist for either cure of syphilis or treatment failure. It is recommended that nontreponemal antibody titers be followed every 6 months, and patients should be periodically reexamined for clinical signs or symptoms of syphilitic infection. Treatment failure is probable in patients with either persistent or recurrent clinical signs or symptoms or a sustained fourfold increase in nontreponemal antibody titer (compared to maximum titer at time of treatment). Treatment failure is possible if nontreponemal antibody titers fail to decline fourfold within 6 months after treatment. Complications Complications of syphilis are primarily related to neurologic involvement, tertiary syphilis, or late manifestations of congenital syphilis. Discordant results from reverse sequence syphilis screeningfive laboratories, United States, 20062010. Reexamining syphilis: An update on epidemiology, clinical manifestations, and management.
A mean sleep latency is then calculated from the average initial sleep latency from each nap allergy news order nasonex nasal spray us. Mean sleep latencies shorter than 8 minutes are considered abnormal and indicative of pathologic excessive daytime sleepiness allergy medicine for kids 18 gm nasonex nasal spray order otc. Patients should be instructed to sleep well for at least 2 weeks preceding the study allergy medicine like singular buy nasonex nasal spray uk, to allow at least 6 to 7 hours per night (and when possible allergy to semen order genuine nasonex nasal spray, extending time in bed to 8-9 hours) allergy medicine safe pregnancy 18 gm nasonex nasal spray fast delivery, and many sleep specialists document the quantity of sleep before the test with actigraphy monitoring or a sleep diary to ensure adherence to this recommendation and exclude the contaminating influence of insufficient sleep quantity. The patient is seated in a dim room in a comfortable, semi-reclined position and asked to remain alert but passive for four 40-minute periods that are 2 hours apart. Diagnostic and Therapeutic Approach to Common Sleep Disorders Insomnia the insomnia disorders all share three basic components: repeated complaints of insomnia, which may involve difficulties falling asleep, staying asleep, poor sleep quality, or waking undesirably early; an adequate time and opportunity for sleep; and a complaint of resultant daytime impairment. Insomnia is the most common of sleep complaints: nearly 45% of people were affected intermittently within the past year in some large studies, and up to 15% suffer chronic insomnia disorders. Risks for insomnia include female sex, older age, and a psychiatric or medical comorbidity. Chronic insomnia should be distinguished from short-term insomnia, which may occur in anyone occasionally. To a lesser extent, these same markers for hyperarousability are seen in other causes of primary insomnia (see Box 1). In the past, insomnia was classified into primary and secondary, with secondary insomnia being far more common. Secondary insomnia was thought to be a result or accompaniment of an underlying illness. For example, it has previously been thought that treatment of secondary insomnia ought to focus on treatment of the underlying disorder. Newer evidence indicates that this approach may be suboptimal for the following reasons: secondary insomnia does not reliably improve when the underlying disorder does; secondary insomnia in general responds to treatment directed at insomnia; and in some cases, the underlying disorder, such as depression, responds better to treatment when the insomnia is addressed directly and concurrently. Furthermore, in several illnesses, such as depression, insomnia may predate the depression by months, and insomnia is a risk factor for future development of many psychiatric illnesses. In addition, primary insomnia was further divided into subtypes of idiopathic insomnia, psychophysiologic (learned) insomnia and paradoxical insomnia (sleep state misperception). Secondary insomnia was also divided into various subtypes such as inadequate sleep hygiene, insomnia due to medical condition, mental disorder, drug or substance. However, it is rare to encounter patients who fit under one of these subtypes exclusively. Most patients with insomnia, primary and secondary, tend to have some diagnostic criteria listed under many of these subtypes. Some individuals do not appear to require precipitating or propagating factors to develop chronic insomnia and have underlying redisposition toward insomnia. These individuals manifest insomnia from infancy and persist despite optimization of sleep hygiene and habit. However, in most cases of insomnia, precipitating and/or propagating influences may be found through careful interview and help establish a secure diagnosis. In these individuals, identifiable precipitating causes that may be traumatic, stressful periods or struggles, medical illness, drugs, or toxins. However, even when the cause is removed, a conditioned response built upon associated and at times maladaptive sleep-related behaviors ensues. Instead of beginning to relax for sleep under permissive circumstances, the affected patient experiences paradoxical arousal as they approach their sleep conditions. The patient under the influence of the precipitating cause may have spent many hours worrying, uncomfortable, clock-watching, or otherwise raising their anxiety levels. Propagating factors include these same behaviors that help maintain sleeplessness once it has begun and may additionally include irregular sleep schedules and the use of drugs. Effective treatment strategies for insomnia focus on removing any residual precipitating influences and mitigating or eliminating propagating influences. The main therapies for insomnia are sleep hygiene, behavioral therapies, cognitive therapies, and pharmacologic therapies. Growing recognition of the adverse effect profile of sedativehypnotic drugs, particularly zolpidem (Ambien), which has been associated with heightened risks of falls and sleep walking, sleep eating, and related amnestic behaviors, has also encouraged a shift toward an earlier application of behavioral approaches to coping with insomnia. Insomnia may occur when parents fail to establish and enforce an appropriate nightly bedtime, so that their child may subsequently stall and refuse to go to bed in a timely fashion. In other cases, insomnia may occur when a child cannot fall asleep until a usual condition is present, such as being held, rocked, or fed. Appropriate advice and treatments include strict limit-setting for bedtime resistance; maintaining regular sleep schedules with avoidance of napping during the daytimes; and curtailing disrupting influences, such as television watching, gaming, and computer use. Selected children benefit from incentives such as a patient-parent contract that offers privileges for slightly later bedtimes on weekends after the child adheres regularly to a specified sleep schedule during school nights. Four considerations for restoring normal sleep hygiene to discuss with all insomnia patients in the office include these three central concepts: · Maintain a regular sleep schedule. After 20 to 30 sleepless minutes spent trying to fall asleep, the patient should be instructed to leave the bedroom to pursue a quietly distracting activity, such as reading mundane material or watching a boring television program, and waiting until he or she feels sleepy enough to return to bed. Patients should explicitly avoid reading in bed, listening to the radio in bed, or watching television in bed if they are having difficulty initiating or maintaining sleep. Patients should be instructed to remove clocks from their bedrooms or hide the clock face so as to make the insomnia period timeless and of uncertain duration. Falling asleep should not be a race against time, and repetitive checking of the time only serves to reinforce anxiety and further activate the mind (see stimulus control, Table 1). For the same reason, when watching television, discourage patients from watching news shows with scrolling tickertape newsflashes with clock time shown. Patients who worry, plan, or think out their problems in bed should be encouraged to schedule a time earlier in the evening, well in advance of their normal bedtime, to attempt to work out these concerns prior to carrying them into bed. This "constructive worry" or "worry time" represents a practical form of cognitive and stimulus control therapy. There are numerous other associated issues and behaviors that may be useful for application in selected patients, such as cutting down overall time in bed (sleep restriction), establishing a regular and relaxing bedtime routine (such as by taking a relaxing bath, listening to soothing music, or having a light snack before bed), avoiding daytime naps, avoiding caffeinated beverages after noontime, and establishing a regular morning exercise routine and avoiding evening exercise. It is important for the physician to avoid overloading the patient with too many considerations and tasks at once, however, as the burden of implementing these suggestions then becomes tantamount to too many obtrusive "swing thoughts" during a golf swing. One or two concepts to start with are sufficient, and once mastered and implemented, the patient can gradually phase in other ideas over time. Relaxation training and cognitive behavioral therapy can be very helpful in selected receptive patients who have failed the above typical self-help measures, and as a last resort, periodic or even scheduled chronic pharmacotherapy can also be implemented. There are now several highly effective and tolerable hypnotic medications available for short-term, intermittent, and chronic use. The class of nonbenzodiazepine receptor agonists (the socalled "Z" drugs, or zolpidem [Ambien], zaleplon [Sonata], and ezopiclone [Lunesta]) are preferred by most sleep specialists but some of them remain costlier than the older generation choices, including the benzodiazepines-which have adverse effects on sleep architecture-as well as diphenhydramine (Benadryl) and trazodone (Desyrel),1 which each have less specific sleeppromoting effects and more adverse effects and potential for drug-drug interactions, especially in elderly patients. The clinical pharmacology of the most commonly prescribed and most useful hypnotic medications are summarized in Table 2. A concern with each of these may be the potential for habituation of efficacy; fall risk; and the potential to cause sleepwalking, sleep eating, or other amnestic behaviors during sleep. If these adverse effects result, the hypnotic drug should be promptly discontinued with a shift toward the use of cognitive behavioral therapy strategies. In women, zolpidem should be used with particular caution given the slower metabolism of the drug, thereby promoting vulnerabilities to carryover sedation and unpleasant "hangover" type feelings or driving safety risks during the morning commute the next morning. Pharmacologic therapy of insomnia may be bolstered in the future by the advent of suvorexant,2 a novel hypocretin antagonist that has a wake-suppressing rather than sleeppromoting mechanism of action. Further clinical experience will likely be necessary to establish the role of this medication as a treatment for insomnia. In wake, the resulting ventilatory pattern is governed by careful integration of classic feedback systems designed to keep blood pH at approximately 7. Hypopneas are significant declines in tidal volume sufficient to result in significant reduction in oxygenation. The likelihood and extent of upper-airway collapse is determined by the neural input into the dilating upper-airway muscles, influence of sleep state, and upper-airway anatomy. Beyond obesity, many but not all patients have a predisposing anatomy of a narrowed oropharynx, such as a low-lying palate or redundant soft palate tissue, a thickened tongue base, or a narrow hypopharynx, although nasal anatomy with septal deviation or chronic congestion may also aggravate the problem. Snoring without other symptoms, signs, or polysomnographic evidence of upper-airway obstructions such as hypersomnia, frequent associated arousals, or significant airflow limitation is termed primary snoring. An otorhinolaryngology consultation may be helpful in determining which surgical approaches may be most beneficial for the individual. Assessment and appropriate counseling for weight loss, cardiovascular risk factors, and driving while untreated (or extreme caution) should be part of a treatment plan. Weight loss may reduce soft tissue in the neck, making the oropharynx less compressible. The improvement in lung volumes accompanied by weight loss also favor enhancement of longitudinal traction on the upper airway, the so-called "tracheal tug. Among the lifestyle or behavioral changes, positional therapy involves employing one or more simple strategies to enforce sleep only in nonsupine body positions, usually on the side. The patient wears a snug-fitting T-shirt with a pocket sewn onto the back between the shoulder blades with two or three tennis or wiffle balls inserted into it to discourage the patient from turning onto the back during sleep. A correctional device for positional sleep apnea is also approved in the European Union. Unfortunately, shoulder or hip pain often limits the application of positional therapy, especially in elderly persons, and long-term adherence or compliance remains poor, with only about one-third of patients able to perpetuate positional therapy strategies in long-term follow-up. Nasal pillows, a type of cannula that provides a tight seal within the nares, are most effective at lower treatment pressures; they may be favored by many patients with claustrophobia but may dislodge at higher pressures or with frequent nocturnal movement. Nasal masks of various types are used in many patients, but if mouth breathing and consequent leak are a problem, a chin strap may be added, or an oronasal face mask may be substituted. They provide a means of advancing the mandible that pull the tongue base forward slightly, opening the oropharyngeal airway to some degree and obviating some apnea and hypopnea events. There is as yet limited experience with the device; however, this may be an option for some patients who are averse to or intolerant of other therapies. In heart failure, the presence of central sleep apnea syndrome or Cheyne-Stokes breathing imparts a poor prognosis. Treatment-Emergent Central Sleep Apnea Syndrome Treatment-emergent central sleep apnea syndrome is a subtype of central sleep apnea wherein patients have significant obstructive/ anatomical problems with ventilation, but also have unstable ventilatory patterns noted in patients with central sleep apnea syndromes. Some patients clearly continue to manifest frequent central sleep apneic events more than five times per hour, leading to the suboptimal outcomes of persisting clinical complaints of hypersomnia and medical risk. Sleep-Related Hypoventilation the causes of hypoventilation during sleep include primary pulmonary parenchymal disorders, neuromuscular conditions affecting bellows musculature, or restrictive physiology of the chest wall accompanying kyphoscoliotic disorders or morbid obesity. Failure to treat significant nocturnal hypoventilation may result in the development of sequelae of hypoxemia such as polycythemia, pulmonary hypertension, and right heart failure, or of hypercapnic respiratory failure. These therapies are best titrated in the context of a supervised overnight laboratory polysomnogram under the direction of a sleep or pulmonary medicine specialist. Central sleep apnea has a heterogeneous pathophysiology and may be idiopathic or due to high-altitude-induced periodic breathing, due to Cheyne-Stokes breathing, or narcotic-induced. Neurologic causes-such as brainstem infarction or neurodegenerative internalmedicinebook. Narcolepsy and Central Disorders of Hypersomnolence Narcolepsy is the prototypical central disorder of hypersomnolence. Cataplexy is a distinctive and highly specific symptom characterized by emotionally provoked muscle atonia intruding into wakefulness that is seen in a minority of patients overall and may precede but more often follows onset of the main symptom of hypersomnia. In addition to sleepiness and cataplexy, the full clinical pentad of narcolepsy also includes symptoms of sleep paralysis (the inability to move the body upon awakening), hypnogogic hallucinations (the intrusion of dream imagery and mentation into conscious awareness following awakening), and sleepmaintenance insomnia (with frequent nocturnal arousals and difficulty maintaining sleep). However, narcolepsy is most frequently monosymptomatic, with the sole symptom being pervasive, enduring sleepiness and decreased vigilance with a tendency toward dozing off inadvertently in permissive settings and the overwhelming desire to nap during the daytime, especially in the afternoons. Naps are most often highly refreshing; scheduled naps can be utilized to therapeutic advantage or indeed, in rare patients, as the sole treatment for those bent on avoiding stimulant pharmacotherapy. Narcolepsy is relatively uncommon, affecting approximately 1:2000 of the general population. While the etiology of narcolepsy remains unknown, most experts continue to favor a long hypothesized autoimmune cause. Within the last few years, epidemic narcolepsy-cataplexy following H1N1 vaccination in Europe and Asia also provided further support for the autoimmune hypothesis of narcolepsy. Unfortunately, these tantalizing discoveries have not yet yielded clear insight into pathogenic mechanisms nor more specific therapies for patients, and the mainstay of treatment for the condition remains the use of older stimulant and wake-promoting medications, or prescribed therapeutic napping, as naps are most often highly refreshing and restorative in narcolepsy patients. Idiopathic hypersomnia is a closely related condition often difficult to distinguish from narcolepsy without cataplexy, although a few nuanced clinical features tend to distinguish it from narcolepsy, chiefly a characteristically reported unrefreshing nocturnal sleep and nap quality. Idiopathic hypersomnia has previously been further subclassified as variants with or without prolonged sleep period, although these phenotypes are overlapping and current diagnostic standards have eliminated this distinction. Hypersomnia is also commonly associated with as many as 50% of those with myotonic dystrophy type 1. The mainstay of treatment for each of these conditions is stimulant and wake-promoting agent therapy, with the goal of improved vigilance and psychomotor functioning. Stimulants and wakepromoting agents range in intensity from lower to higher intensity and efficacy/tolerability options, from modafinil (Provigil) and armodafinil (Nuvigil) on the milder end of the spectrum-although selected narcolepsy patients respond quite well to these drugs-to methylphenidate (Ritalin), and to the amphetamines (Adderall). Relevant clinical pharmacology of the stimulant medications commonly used in clinical practice are summarized in Table 4. Pitolisant (Wakix), a selective H3 subtype histamine inverse agonist/antagonist proven effective as a wake promoting agent for narcolepsy, recently received European Medicines Agency marketing authorization but is currently unavailable in the United States. Patients with uncontrolled hypersomnias should be cautioned against driving, operating dangerous machinery, or engaging in other similarly dangerous activities or hobbies while they are drowsy, as they may be prone to sudden and unpredictable sleep attacks. The most common circadian rhythm disturbances are actually exogenous influences on the patient and his/her circadian axis, which in these cases is functioning normally but is unable to adjust rapidly enough to the required new temporal milieu. Jet lag disorder results when an individual crosses across several transmeridian time zones in a single day. Crossing one or two time zones is usually not too difficult for the traveler to accommodate, but crossing three time zones typically causes symptoms of jet lag. Flying eastward is generally much more difficult than flying westward, as patients more easily accommodate phase delay then phase advancing, or "loss" of time. Also critical is attempting to rapidly adapt to the new time zone, such as by seeking regular sunlight exposure during the daytime and avoiding light exposure in the evening. Shift-work sleep disorder results from workers who must constantly and regularly alter or rotate their work schedules between different shifts (so-called "swing shifts") or workers who must 2 704 Not available in the United States.
Bacteremic patients have a longer length of stay new allergy medicine just approved by fda buy nasonex nasal spray us, and one recent report suggests that this is due to a longer time to resolution of fever allergy forecast johannesburg generic nasonex nasal spray 18 gm. Many experts continue to recommend that blood cultures be obtained as part of the diagnostic evaluation of patients who are ill enough to require hospitalization; blood cultures are not necessary for those who will be managed as outpatients allergy forecast gainesville fl discount nasonex nasal spray 18 gm overnight delivery. Other enterobacteriaceae allergy testing risks cheap nasonex nasal spray 18 gm, including Klebsiella species and Proteus species allergy to yellow 5 symptoms order 18 gm nasonex nasal spray with amex, are also occasionally implicated. Other gram-negative pathogens such as Pseudomonas, Serratia, Enterobacter, and Acinetobacter should be considered in health careassociated infections. Enterococcus is an uncommon pathogen in community-acquired infections, but it must be considered in health careassociated infections, including vancomycin-resistant enterococci. Other gram-positive pathogens include Streptoccocus agalactiae and Staphylococcus species. Although a common cause of acute cystitis in young women, Staphylococcus saprophyticus is a rare cause of pyelonephritis; the finding of Staphylococcus aureus in a urine culture should always prompt a search for an extrarenal source of infection that might have served as a source of hematogenous seeding. It is clear that the prevalence of resistance varies depending on geographic region, and clinicians often do not have access to meaningful local resistance data. Recent reports of increasing fluoroquinolone resistance among uropathogens are of great concern, although overall resistance rates in North America remain low. Hospitalization should be considered for patients who cannot tolerate oral intake or who have severe pain or signs of severe sepsis. A strategy of initial management in the emergency department or an observation unit with an initial dose of parenteral antibiotic therapy, intravenous fluids, and symptomatic treatment of nausea and pain may be used in select patients to avoid hospital admission. Patients who will be treated as outpatients should have a stable social situation and the ability to contact the physician and return promptly if their symptoms worsen. Hospitalization is generally recommended for patients with complicated infections. There are surprisingly few prospective randomized trials of the treatment of pyelonephritis. For patients who require hospitalization, parenteral therapy with an aminoglycoside, a third-generation cephalosporin, or a fluoroquinolone is recommended. At my institution, we discourage fluoroquinolones for this indication because there are other effective alternatives and we wish to minimize the use of these very broad-spectrum agents in the hospital setting. If a gram-positive pathogen is suspected or suggested by the results of urine Gram stain, ampicillin or ampicillin-sulbactam (Unasyn) with or without an aminoglycoside can be used. Patients should receive intravenous therapy until they are clinically improving and able to reliably tolerate oral intake; oral therapy can be chosen based on the results of urine culture and susceptibility data. The narrowest spectrum, least expensive agent to which the isolated pathogen is susceptible should be chosen. Bacteremic patients might take longer to respond but do not require more prolonged parenteral therapy. Longer courses of therapy may be required for select patients with complicated pyelonephritis. For outpatients, initial empiric therapy with a fluoroquinolone is recommended, with adjustment of therapy, if needed, based on the results of urine culture. Although prospective randomized trials are lacking, several retrospective studies as well as several prospective nonrandomized trials suggest that Pyelonephritis which does not achieve adequate levels in the urine. Patients with inflammatory bowel disease or with history of gastric bypass procedures also have an increased risk for stone formation. Pathophysiology Renal calculi are broadly classified into two major categories of calcareous (calcium containing) or noncalcareous stones based on the presence or absence of calcium. Calcareous stones account for approximately 80% of urinary calculi, with the most common stone composition being calcium oxalate (70%), followed by calcium phosphate (5% to 10%). Commonly occurring noncalcareous stones include struvite or infection stones (15% to 20%) uric acid (10%) and less-common cystine stones (1%). The process of stone formation starts when urine within the nephron becomes supersaturated with stone-forming salts that ultimately precipitate out of solution as crystals. This is a complex process, with interplay between the urinary solutes and stone inhibitors. Natural stone inhibitors such as citrate, TammHorsfall glycoprotein, and nephrocalcin attempt to block this process, but once the concentration of stone-forming crystals reaches a certain threshold (concentration product), stone crystals can form. Small crystals are often unstable and can dissolve; however, if the supersaturated state exists along with low levels of citrate, then the stone crystals form by homogenous aggregation. Once formed, the crystal structure continues to grow through a process of heterogeneous aggregation by adsorption of other types of crystals or cellular debris. Hypercalciuria (more than 200 mg per 24 hours) is the most common urinary abnormality associated with the formation of calcium stones. Type I absorptive hypercalciuria occurs in approximately 55% of stone formers and is diagnosed with high urinary calcium (more than 200 mg per 24 hours) in the presence of a low-calcium diet (400 mg/day). Other, lesscommon forms of hypercalciuria include increased calcium leakage from the kidney (renal hypercalciuria) or as a result of increased bone resorption from excess parathyroid hormone (primary hyperparathyroidism). Primary hyperparathyroidism is present in less than 5% of patients with stone disease, but it should be considered in any stone patient with serum calcium greater than 10mg/dL. Hyperoxaluria (more than 45 mg per 24 hours) can also contribute to stone formation. Enteric hyperoxaluria is the most common reason for increased urinary oxalate and is found in patients with chronic diarrhea. Malabsorption of enteric fat leads to saponification of divalent cations (calcium and magnesium), leading to increased oxalate absorption. This is commonly seen in patients with short-bowel syndrome, following bariatric surgery, or resulting from inflammatory bowel disease. Increased dietary consumption of oxalate (nuts, chocolate, tea, rhubarb, broccoli, spinach) can also lead to hyperoxaluria. Primary hyperoxaluria is the result of an autosomal recessive inborn error of metabolism that can lead to early end-stage renal failure (by age 15 years) and death without a combined liver and kidney transplant. Lastly, a low level of the oxalate-degrading bacteria Oxalobacter formigenes has been shown to increase the risk of forming oxalate stones. Hyperuricosuria (more than 600 mg per 24 hours) along with a urinary pH less than 5. High uric acid is often the result of a high-protein diet but it can also occur in patients with end-ileostomies, gout, or myeloproliferative diseases. Follow-up urine cultures to document microbiological response are not recommended in patients who have responded clinically. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: a randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Moreover, up to 50% of these patients will experience a recurrent stone within 5 years of their original episode. Most stone patients have their first stone between the ages of 20 and 60 years of age, with peak incidence in the fourth to sixth decade of life. These ages coincide with the years of peak employment and productivity, which can be affected significantly by kidney stones. An employee with kidney stones files roughly $3500 more in medical claims than a coworker who does not have kidney stones. Risk Factors the risk of developing a stone depends on many factors including sex, fluid intake, diet, geographic location, obesity, and the presence of inflammatory bowel disease or other systemic medical conditions. Ethnic European men are more likely than Hispanic, Asian, or African American men to develop a stone. Patients who live in the southeastern United States have the highest rates of kidney stones when compared to residents of other regions, with the highest incidence of stones peaking 1 to 2 months after the hottest months of the year. Persons with occupations exposing them to continual high temperatures have been found to have an approximately eightfold increased rate of forming a kidney stone compared to other workers. Simply being adequately hydrated by increasing Struvite (infection) stones are composed of magnesium, ammonium, and calcium phosphate and are the leading cause of large stones that occupy the entire renal pelvis (staghorn calculi). These stones are caused by urea-splitting bacteria, which result in alkalization of the urine. The most common organisms associated with struvite stones are Klebsiella pneumoniae, Proteus mirabilis, and Ureaplasma urealyticum. Failure to treat these stones carries an increased risk of renal damage, sepsis, and possibly death. Cystinuria (more than 250 mg per 24 hours) leads to stone formation as a result of an autosomal recessive disorder of dibasic amino acid transport. Homozygous patients usually present with their first stone during childhood, which may be pure cystine or may be mixed with calcium oxalate. Pure cystine stones are radiolucent on plain radiographic imaging and are yellow in appearance. Treatment Once a stone has been discovered, treatment depends on multiple factors including size, location, presence of obstruction, evidence of systemic illness or fevers, and presence of nausea and vomiting. For patients who are clinically stable, outpatient expectant management is generally possible with a combination of oral hydration, pain control, and antiemetics. Medical expulsive therapy with the addition of an a-blocker such as tamsulosin1 (Flomax 0. Ultimately, approximately 98% of stones 5 mm or less pass spontaneously, taking an average time of 12 days to dislodge. Invasive Treatment If the patient has signs of sepsis, intractable pain, or nausea and vomiting, then immediate procedural intervention should be considered. Options include cystoscopy with placement of a ureteral stent to temporarily decompress the obstruction, or placement of a percutaneous nephrostomy tube. Septic patients should be emergently decompressed with a ureteral stent or a nephrostomy tube. The decision to recommend a procedural intervention is often multifactorial, involving factors such as chance for spontaneous passage, absolute indications for intervention, and patient preference and work and family requirements. Ureteral stones larger than 1 cm have a minimal chance of passing and require surgical treatment in most cases. After ureteroscopy a ureteral stent may be left in place, which is generally removed in the office in 1 to 2 weeks. Stents are usually well tolerated, but some patients do experience bothersome urinary symptoms including urgency, frequency, and bladder pain at the end of urination. Percutaneous access is obtained by either interventional radiology or by the urologist, and a 30-F working tract is created. The calculus is then fragmented by ultrasonic or pneumatic lithotripsy devices, and fragments are removed. Clinical Manifestations Patients with renal calculi generally present for evaluation when the stone begins to move down the urinary tract. Acute renal or ureteral colic from an obstructive calculus is described as intermittent crampy pain that is severe and often debilitating. Some patients also experience nausea and vomiting during these episodes and can have varying amounts of blood in the urine. Patients with staghorn calculi can present with signs and symptoms of a systemic infection and are at risk for progression to sepsis. Diagnosis A thorough history should be taken during the initial evaluation, with questions focusing on the nature and location of the pain, radiation of the pain, duration of pain, and presence of nausea, vomiting, dysuria, and hematuria. Questions directly related to stone disease should be asked, such as personal or family history of stone disease, age of first stone, and history of recurrent urinary tract infections. If the patient has had prior stones, it is important to ask how the stone was managed, did it pass spontaneously or was an intervention required The physical examination usually demonstrates significant costovertebral angle or flank tenderness to palpation. Peritoneal signs are not common with renal calculi, and an alternative diagnosis should be pursued if these are found. Patients with fevers, tachycardia, or labile blood pressure and flank pain should be considered to have an obstructing stone and should be treated emergently. Attention should be paid to the urinalysis for presence of crystals, hematuria, signs of infection, and pH. An elevated creatinine could indicate obstruction of the kidney or dehydration from nausea and vomiting. Initial imaging studies usually consist of a plain abdominal radiograph to examine for the presence and location radiopaque stones. These samples should be analyzed for urine volume, pH, calcium, creatinine, sodium, phosphate, oxalate, uric acid, citrate, and cystine levels. General recommendations to prevent recurrent stones include increasing water intake to make at least 2 L of urine per day and adhering to a low-salt, low-meat, moderatecalcium diet. Hypercalciuria is treated by thiazide diuretics (hydrochlorothiazide)1 25 mg daily and/or potassium citrate (Urocit-K) 10 to 20 mEq twice daily. Hyperoxaluria is treated by decreasing dietary intake of oxalate with oral calcium supplementation. Renal Calculi Hyperuricosuria is treated by the addition of potassium citrate to increase the urinary pH plus allopurinol (Zyloprim) to decrease serum uric acid. Patients with cystine stones are best managed by a lowmethionine diet and alkalization of the urine with potassium citrate. If these measures are not sufficient, cystine binders such as tiopronin (Thiola) or D-penicillamine (Cuprimine) can help prevent recurrent cystine stones. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: A 5-year randomized prospective study. Primary hyperparathyroidism with intermittent hypercalcaemia: serial observations and simple diagnosis by means of an oral calcium tolerance test. Two-year experience with ureteral stones: Extracorporeal shockwave lithotripsy v ureteroscopic manipulation. Direct and indirect costs of nephrolithiasis in an employed population: Opportunity for disease management Computed tomography scan demonstrating large right perirenal hematoma and thrombosed posterior segmental artery. The kidney, followed by the bladder and urethra, are the most commonly involved genitourinary organs. Still, early involvement of the urologist is prudent to help plan further interventions. The spectrum of genitourinary injuries is widespread, and management can range from immediate repair to temporization with delayed reconstruction. The goal of a urologist in the trauma setting is to establish urinary drainage in order to optimize kidney function, minimize hemorrhage, and control urinary extravasation to reduce associated complications such as infection or ileus.
Syndromes
- Bleeding
- Personality, mood, or emotional changes
- Hematoma (blood accumulating under the skin)
- Nausea
- Inability to pull the retracted foreskin over the head of the penis
- Tai chi
The initial lesion is typically an erythematous allergy zyrtec side effects nasonex nasal spray 18 gm buy mastercard, tender pustule or abscess with a small area of necrosis allergy testing does it work cheap nasonex nasal spray 18 gm line. The benign appearance of this lesion belies the widespread and aggressive tissue destruction that has occurred beneath it allergy symptoms face numbness purchase 18 gm nasonex nasal spray with visa. Direct inspection through skin incisions reveals extensive gangrene of the superficial tissues and fat that rarely involves the underlying fascia and muscles allergy shots dosage nasonex nasal spray 18 gm buy with visa. These lesions characteristically exude a thin allergy testing jersey ci 18 gm nasonex nasal spray buy with mastercard, brown, malodorous discharge, which manifests mixed flora with abundant polymorphonuclear leukocytes with Cellulitis Cellulitis is an acute infection of the skin and underlying soft tissues. It commonly begins as a hot, red, edematous, sharply defined eruption and may progress to lymphangitis, lymphadenitis, or in severe cases, necrotizing fasciitis and gangrene. Cellulitis usually occurs in local skin trauma caused by insect bites, abrasions, surgical wounds, contusions, or other cutaneous lacerations. Immunosuppressed patients are particularly susceptible to the progression of cellulitis to regional or systemic infections, and Bacterial Diseases of the Skin Folliculitis these patients should be treated aggressively with systemic antibiotics, drainage, and debridement when indicated. Cellulitis is 20´ fold more common in patients with chronic venous stasis or lymphedema. Recurrent cellulitis may occur in patients at the exact site of saphenous donor site surgery. Initial presentation is that of a rapidly expanding, tender, erythematous, indurated area of skin. An ascending lymphangitis may be present, especially in cellulitis involving an extremity often associated with regional lymphadenopathy. Systemic signs and symptoms can eventually evolve and when present, mandate hospitalization and treatment with systemic antibiotics. If fever, septicemia, or other signs of advancement to deeper tissues are present, the patient should be admitted to the hospital for blood and wound cultures, parenteral antibiotics (see Table 1), and observation. If a prompt response is not observed after parenteral antibiotic treatment, surgical exploration of the involved area may be indicated to establish an etiologic diagnosis and rule out the presence of necrotic or gangrenous tissue. Immunosuppressed patients or patients with recurrent cellulitis should be extensively examined to exclude chronic sources of infection, and these patients should be treated with parenteral antibiotics until the cellulitis resolves, followed by 5 to 7 days of oral antibiotics. Crepitus, which is caused by the accumulation of gas in the tissue produced by facultative or obligate anaerobes, can be palpated in 25% of patients, and it mandates immediate surgical attention. Predisposing factors include perirectal abscess and ischiorectal abscess, both of which may track to the deeper structures of the pelvis, leading to abscess formation and subsequent septicemia. This infection can occur after amputation and is usually associated with diabetes mellitus (75% of cases) or peripheral vascular disease (50% of cases). Synergistic necrotizing cellulitis is commonly caused by mixed flora originating in the gastrointestinal tract. Coliforms are the most prevalent aerobes (Escherichia coli, Klebsiella, Proteus), and anaerobic flora include Bacteroides, Peptostreptococcus, Clostridium, and Fusobacterium. The primary treatment modality is aggressive debridement of nonviable skin and subcutaneous tis´ sues. This may involve several operations and dressing changes under general anesthesia, which should be performed until all necrotic tissue is removed. Rotation or free myocutaneous flaps and split-thickness skin grafting may cover areas of tissue loss when necessary. If the perineum is involved, fecal diversion by colostomy may be necessary to facilitate healing. Empiric parenteral antibiotics effective against polymicrobial gram-positive and gram-negative aerobic and anaerobic flora are also a mainstay of therapy. However, antibiotic coverage must be modified as soon as culture and susceptibility testing reveal specific offending organisms (Table 2) to reduce the emergence of resistant organisms. It is often associated with local crepitus and systemic signs of toxemia, which are caused by the anaerobic, gas-forming bacilli of the Clostridium species. This infection most often occurs after abdominal operations on the gastrointestinal tract; penetrating trauma, such as gunshot wounds, and frostbite can also expose muscle, fascia, and subcutaneous tissues to these organisms. Common to all these conditions is an environment containing tissue necrosis, low oxygen tension, and sufficient amounts of amino acids and calcium to allow germination of clostridial spores and production of the lethal toxin. They have also been isolated in the human gastrointestinal tract and skin, most importantly in the perineum and oropharynx. Clostridium perfringens is the most common isolate (in 80% of cases) and is among the fastest growing clostridial species, having a generation time under ideal conditions of approximately 16 minutes. This organism produces collagenases and proteases that cause widespread tissue destruction and produces toxin, which is associated with the high mortality rate of clostridial myonecrosis. The toxin, a phospholipase C, causes platelet-neutrophil complexes, vascular obstruction, and extensive compromised vascular perfusion, leading to necrosis of the muscle and overlying fascia, skin, and subcutaneous tissues. Historically, clostridial myonecrosis was a disease associated with battle injuries, but 60% of current cases occur after trauma: 50% after automobile accidents and the remainder after crush injuries, industrial accidents, and gunshot wounds. Mortality can be the result of a failure to recognize that clostridial infection is underway, which leads to a delay in the debridement of devita´ lized tissues. Patients often complain of a sudden onset of pain at the site of trauma or surgical wound, which increases rapidly in severity and extends beyond the original borders of the wound. The skin initially exhibits tense edema, but its pale appearance progresses to a magenta hue. A Gram stain examination of wound discharge reveals abundant gram-positive rods with a paucity of leukocytes. The diagnosis of gas gangrene is based on the appearance of the muscle on direct visualization by surgical exposure, because many changes are not apparent when inspected through a small traumatic wound. As the disease process continues, the muscle becomes frankly gangrenous, black, and extremely friable. Despite profound hypotension and impending organ failure, these patients may be remarkably alert and extremely sensitive to their surroundings. They feel their impending doom and often panic just before slipping into toxic delirium and eventually into coma. The clinical features should arouse suspicion early in the course, so the disease can be recognized and treated with aggressive surgical debridement. Gas in the wound is a relatively late finding, and ´ by the time crepitation is observed, the patient may be near death. Approximately 15% of blood cultures are positive, but this is also a late finding. Serum creatinine kinase levels, although relatively nonspecific, are always elevated in cases with muscle involvement. It is highest in cases involving the abdominal wall and lowest in those affecting the extremities. Among the signs that prognosticate a poor outcome are leukopenia, thrombocytopenia, hemolysis, and severe renal failure. Myoglobinuria is common and can contribute significantly to worsening renal function. Frank hemorrhage may also be present and indicates disseminated intravascular coagulation. Successful treatment of this life-threatening infection depends on early recognition and debridement of devitalized and infected ´ tissues. Surgical intervention should include wide debridement ´ of all necrotic tissue and amputation if extremities are involved. Hyperbaric oxygen (100% O2 at 3 atm) has been reported to reduce associated tissue loss and mortality; however, core treatment is surgical debridement, and it should never be delayed to ´ arrange for hyperbaric oxygen treatments. In animal studies of gas gangrene, hyperbaric oxygen was not efficacious, whereas clindamycin (Cleocin) treatment had dramatic effects in reducing mortality. Clindamycin is the treatment of choice because of its ability to suppress toxin production. Cardiovascular collapse mandates careful monitoring of intravenous fluid resuscitation, which may require large volumes. Failure to adequately resuscitate these patients compromises therapy by limiting oxygen delivery and antibiotic distribution to the affected tissues and may promote progression to multisystem organ failure. In this process, the bacterial tissue invasion is primarily superficial, extending to the fascial layer without muscle involvement. Spontaneous gas gangrene caused by Clostridium septicum can occur in the absence of trauma in patients with gastrointestinal lesions such as carcinoma of the colon. Necrotizing Fasciitis Necrotizing fasciitis is an aggressive soft tissue infection involving the fascia with extensive undermining and tracking along anatomic planes. This process usually occurs in patients with significant comorbidity, such as diabetes mellitus or peripheral vascular disease, but it is also seen in obese or malnourished patients and intravenous drug abusers. Cellulitis is a frequent occurrence, and progressive necrosis to subcutaneous tissue results from thrombosis of the perforating vessels. Ninety percent of these infections have a polymicrobial cause, and it is common to culture up to five organisms from the fascial planes involved with this infection. Polymicrobial necrotizing fasciitis most commonly evolves from a benign-appearing skin lesion (80% of cases). Minor abrasions, insect bites, injection sites, and perirectal abscesses have been implicated. Surgical procedures, especially bowel resections, and penetrating trauma can be complicated by superficial wound infections that evolve into necrotizing fasciitis. The infection commonly involves the buttocks and perineum, which results from untreated perirectal abscesses or decubitus ulcers; intravenous drug abusers commonly participate in "skin popping," which leads to infections of the upper extremities. Fifty percent of group A streptococcal necrotizing fasciitis patients have a portal of entry such as an insect bite, slivers, surgical procedures, or burns, whereas the other 50% have no portal of entry, and the infection begins at the exact site of nonpenetrating trauma, such as a muscle strain or bruise. This idiopathic form, commonly known as spontaneous necrotizing fasciitis, is particularly dangerous because of the frequent delay in diagnosis. For those with a portal of entry, the initial presentation is a slowly advancing cellulitis that progresses to a firm, tense, woody feel of the subcutaneous tissues. This entity may be distinguished from other aggressive anaerobic soft tissue infections. Often, a broad, erythematous tract along the route of the underlying fascial plane can be discerned through the skin. If an open wound exists, probing the edges with a blunt instrument permits ready dissection of the superficial fascia well beyond the wound margins, and this is the most important diagnostic feature of necrotizing fasciitis. On direct inspection, the fascia is swollen and dully gray in appearance, with stringy areas of fat necrosis. A thin, brown exudate can be expressed from the wound, but frank purulent drainage is rare. These wounds are remarkably insensate when found and mandate immediate debridement. Wide debridement and ´ parenteral antibiotics have a profound effect on survival, and limited or staged debridement has no place in the treatment of this ´ very aggressive, life-threatening infection. Parenteral antibiotics (see Table 2) should be directed against the polymicrobial aerobic and anaerobic microorganisms isolated from these infections. Every effort should be made to quickly identify the offending organisms, and antibiotic therapy should be changed accordingly. In patients with no defined portal of entry, severe pain at the site of previous nonpenetrating trauma is common. These patients usually have a slightly elevated white blood cell count with a left shift and an elevated pulse. Later, erythema, induration, and warmth occur and may rapidly progress to violaceous skin, ecchymosis, and blister formation. A markedly elevated creatine phosphokinase level in a patients with any erythematous rash may suggest a necrotizing process. By the time these late cutaneous findings are present, most patients have evidence of shock and organ failure. Misdiagnosis and delay in diagnosis are common and associated with significant morbidity and mortality. Surgical exploration with debridement of infected and necrotic tissue in ´ addition to systemic antibiotic therapy directed toward the aerobic Streptococcus organism can result in decreased morbidity and mortality (see Table 1). Less commonly, this condition has occurred after urologic manipulation or as a late complication of deep anorectal suppuration. Definitive diagnosis is made by identification of a necrotic black area on the scrotum associated with local and systemic signs of infection. Left untreated, death ensues from uncontrolled, severe systemic sepsis and multiple-organ failure. Prompt recognition and treatment can minimize tissue loss, especially the skin and soft tissues of the scrotum, labia, and perineum, and may prevent complete loss of genitalia. The infection is often polymicrobial, as with necrotizing fasciitis, with several species of aerobic and anaerobic bacteria predominating. Successful treatment is based on early recognition and vigorous surgical debridement, occasionally including diversion ´ of the fecal stream. Empiric treatment is appropriate until results of culture and susceptibility testing are available (see Table 2). The therapeutic benefit of hyperbaric oxygen treatments has not been proved, and it should be used only as an adjunct to surgical debridement. Although sepsis caused by Pseudomonas aeruginosa is often indistinguishable from other types of gram-negative sepsis, a characteristic skin lesion may develop with erythematous macular eruptions that quickly become bullous with central ulceration and necrosis. These lesions may be distinguished from the lesions of pyoderma gangrenosum (a noninfectious dermatosis) by their association with clinical signs of infection. Treatment is primarily administration of antimicrobial therapy effective against the Pseudomonas organism and by debridement ´ of the multiple lesions. This may lessen the bacterial burden, perhaps allowing greater antibiotic efficacy. Bacterial Diseases of the Skin Sea and Freshwater Infections Infections caused by V. Although infections ´ caused by these organisms cannot be differentiated from those caused by mixed infections, a history of exposure to sea water (V.
Generic nasonex nasal spray 18 gm free shipping. Rheumatoid Arthritis and Gluten Intolerance.
References
- Neufeld EB, Wastney M, Patel S, et al. The Niemann-Pick C1 protein resides in a vesicular compartment linked to retrograde transport of multiple lysosomal cargo. J Biol Chem 1999;274:9627.
- Mullner M, Urbanek B, Havel C, et al. Vasopressors for shock. Cochrane Database Syst Rev. 2004;(3):CD003709.
- Spector TD, Conaghan PG, Buckland- Wright JC, et al. Effect of risedronate on joint structure and symptoms of knee osteoarthritis: results of the BRISK randomized, controlled trial [ISRCTN01928173]. Arthritis Res Ther 2005; 7(3):R625-33.
- Wilson WH, Pittaluga S, Nicolae A, et al. A prospective study of mediastinal gray-zone lymphoma. Blood 2014;124(10):1563-1569.
- Crane JM, Scherz HS, Billman GF, et al: Ischemic necrosis: a hypothesis to explain the pathogenesis of spontaneously ruptured enterocystoplasty, J Urol 146:141n144, 1991.
- Crawford MW, Lerman J, Saldivia V, Carmichael FJ. Hemodynamic and organ blood flow responses to halothane and sevoflurane anesthesia during spontaneous ventilation. Anesth Analg 1992;75:1000-1006.
- Chou, D.S., Abdelshehid, C., Clayman, R.V., McDougall, E.M. Comparison of results of virtual-reality simulator and training model for basic ureteroscopy training. J Endourol 2006;20:266-271.