
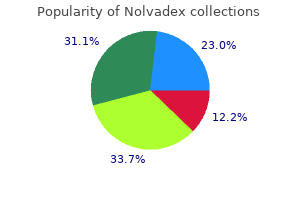
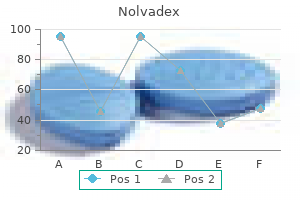
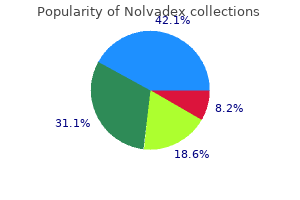
Nolvadex
| Contato
Página Inicial
James E. Barone, MD, FACS, FCCM
- Professor of Clinical Surgery
- Weill Medical College of Cornell University
- Chairman, Department of Surgery
- Lincoln Medical and Mental Health Center
- Bronx, New York
The aorta is smaller than the pulmonary artery women's health clinic exeter 20 mg nolvadex buy amex, which is concerning for associated aortic coarctation menopause and depression order generic nolvadex from india. Li S et al: Surgical outcomes of 380 patients with double outlet right ventricle who underwent biventricular repair menstrual with blood clots nolvadex 20 mg without a prescription. The presence of 2 markers led to invasive genetic testing breast cancer oakleys 10 mg nolvadex buy amex, leading to the diagnosis of trisomy 13 women's health issues bleeding purchase nolvadex australia. Yozgat Y et al: Modified myocardial performance index is not affected in fetuses with an isolated echogenic focus in the left ventricle. Weber R et al: Spectrum and outcome of primary cardiomyopathies diagnosed during fetal life. Always test for lysosomal storage disorders in apparently "idiopathic" hydrops fetalis. Autopsy confirmed myocardial ischemia, which was attributed to severe hypotension at the time of twin demise. This small mass would not have caused obstruction, but it could have triggered an arrhythmia as a cause of death. This is not obstructing inflow as evidenced by the near normal appearing tricuspid valve. The heart was structurally normal, hydrops never developed, and the infant did well after delivery. Carrard C et al: Fetal right ventricular diverticulum with pericardial effusion: report of a new case treated by in utero pericardiocentesis. The massive pericardial effusion fills the chest, and a small amount of ascites is also present. Most pericardial teratomas are intrapericardial, as in this case, and are invariably associated with a pericardial effusion, which may be massive. Malay J et al: Intrapericardial immature teratoma with successful treatment in a neonate. Flow during an atrial contraction is toward the transducer, while flow during a ventricular contraction is away from the transducer. The tracing then shows multiple atrial contractions and infrequent ventricular contractions, which are disassociated with each other, consistent with complete heart block. The ventricular rate is slow and the atrial rate is more normal, but again, there is complete disassociation in this patient with complete heart block. This could also be the appearance of blocked premature atrial contractions, but the pattern would eventually change during scanning back to sinus rhythm. This signifies significant elevation of right atrial pressure in this patient with heart block and hydrops. This combination typically has a poor prognosis with limited options for treatment. The patient had been sent for fetal echo, and as the heart was structurally normal, it was assumed that there was no significant problem. Remember, if the heart is not in the right place, it is either being pushed or pulled. This delivery was planned with a multidisciplinary team and the infant did well after surgery. Almost 1/2 of the liver was in the left hemithorax, the heart was displaced, and there was almost no measurable lung. Liver-up hernias have a worse prognosis than those where the liver remains in the abdomen. There is marked displacement of the heart and compression of the contralateral lung. The mass is perfused by branches of the pulmonary artery; thus, it is a congenital pulmonary airway malformation. Congenital Pulmonary Airway Malformation Bronchopulmonary Sequestration (Left) this echogenic mass is clearly perfused by a feeding vessel from the aorta. The fact that a short-axis view of the ventricles is visible in this plane indicates that the heart is also rotated. The infant had prolonged cardiac dysfunction after resection of the teratoma but eventually recovered fully. Chamber Asymmetry Chamber Asymmetry (Left) Four-chamber view shows an abnormal axis secondary to dramatic right atrial enlargement in a fetus with Ebstein anomaly. Conotruncal Malformation Heterotaxy, Cardiosplenic Syndromes (Left) In a fetus in cephalic presentation with spine to the maternal right, the fetal left side is anterior. The liver is anterior to the heart because of diaphragmatic elevation, not a diaphragmatic hernia. Pulmonary Agenesis Pulmonary Agenesis (Left) Axial view of the chest in the same case shows the cardiac apex directed posteriorly. The unilateral left lung agenesis was isolated in this case and the child is alive and well. In this case, there was mitral atresia so all the blood flow from the lungs was going left to right at the atrial level. Flow is all right to left at the atrial level; there is minimal atrial septal tissue. It is key to look at the relationship of the great vessels to avoid missing associated transposition. Both the primum atrial septal defect and inlet ventricular septal defect are seen. Ebstein Anomaly Ebstein Anomaly (Left) Four-chamber echocardiogram shows a mitral valve in the normal position with a normal left heart. This is noted by the difference in arrow locations, which mark the hinge point of each valve. Tricuspid Dysplasia Tricuspid Dysplasia (Left) Four-chamber echocardiogram shows thick and dysplastic tricuspid valve leaflets that do not appear to coapt well. These patients typically do well after birth when the pulmonary vascular resistance falls. The roof of the yolk sac becomes incorporated in the form of a tube as part of the primitive gut. Errors in development include communication between the foregut branches, such as a tracheoesophageal fistula. The arterial supply to the gut is already defined: Celiac artery (foregut), superior mesenteric artery (midgut), and inferior mesenteric artery (hindgut). The dorsal mesogastrium elongates, forming the left and caudal portions of the lesser sac. The gut continues to elongate and rotates counterclockwise (as viewed from the front) around the superior mesenteric artery within the dorsal mesentery. Common developmental errors include midgut malrotation, omphalocele, and imperforate anus. The leaves of the greater omentum elongate to the left and caudally, expanding the lesser sac and covering the transverse colon and small intestine. The yolk stalk, which connected the yolk sac to the primitive gut, is disintegrating. The cecum is the last part to return and continues to rotate in a counterclockwise direction until reaching the right lower quadrant. Errors in development include persistence of a part of the yolk stalk (Meckel diverticulum) and errors of bowel rotation. The small bowel and transverse and sigmoid colon remain intraperitoneal, suspended by their respective mesenteries. These are areas of mesodermal deficiency, which upon disintegrating became the oropharyngeal cavity and area of the urethra and anus, respectively. This graphic shows the beginning of disintegration of the oropharyngeal membrane in the 4th week. It fuses with the cloacal membrane, dividing it into the anal and urogenital membranes, and forms the perineal body. They unite again to form the proximal vitelline veins, which join with the (initially) paired umbilical veins to enter the sinus venosus of the heart. The left umbilical vein sends a large branch to the liver, which anastomoses with the plexus derived from the vitelline veins. The extrahepatic (distal) vitelline veins form the precursors to the portal venous system. The proximal parts of the vitelline veins have become the hepatic veins, returning blood from the liver to the heart. The distal parts have developed into the portal venous system, returning blood from the gut to the liver sinusoids. Fluid-filled structures, including the bladder, stomach, & small bowel, are very high signal intensity. The upper oblique axial image shows the lungs are mildly hyperechoic compared to the liver and spleen. Changes in echotexture often provide clues regarding any pathologic process in a given organ. Following the colon on ultrasound (top right) is somewhat more difficult, but the anal dimple image (bottom right) of the perineum should be performed in any case of suspected anorectal malformation. It has a classic doughnut or target appearance with a thick, hypoechoic sphincter and hyperechoic mucosa. Structures that should specifically be evaluated include the stomach, kidneys, bladder, umbilical cord insertion site, and umbilical cord vessel number (the normal appearance of the kidneys and bladder are reviewed in the approach to the genitourinary system). The diaphragm, esophagus, small intestine, colon, gallbladder, and liver should also be examined but is not required as part of the standard midtrimester scan. Document that the heart and stomach are on the same side and it is the anatomic left (normal situs). The stomach changes in size and shape during the exam; fluid may intermittently be seen to enter the duodenal bulb but should never persist. Fluid must be visualized on both sides of the umbilical cord in a transverse section of the fetal abdomen in order to consider the insertion site intact. Stimulation of fetal movement may be necessary to create a more favorable acoustic window, especially in the third trimester when the fetal knees are often tucked up against the abdominal wall. These may be visible at the cord insertion site, but the easiest way to confirm a threevessel cord is to use color Doppler to document the umbilical arteries as they run on either side of the bladder. It is imperative that it be completely imaged from front to back, which is best done in the sagittal plane. If only viewed in the anterior coronal plane, a congenital diaphragmatic hernia may be missed. In the setting of esophageal atresia, a fluid-filled tubular structure may be seen in the fetal neck. Remember to use color Doppler to ensure that the fluid-filled structure is between the neck vessels. Also be aware that normal fetal swallowing may cause intermittent distension of the oropharynx. In the early midtrimester, bowel loops may not resolve as distinct "tubes"; the bowel is seen as the intermediate echogenicity "filler" between the solid organs, bladder, and stomach. In the third trimester, it is normal for the meconiumfilled colon to be seen as a hypoechoic tubular structure. The anal dimple can be seen on an axial view through the perineum; the anal mucosa is echogenic and is surrounded by the hypoechoic muscles of the anal sphincter. The fetal liver is relatively large and extends across the upper abdomen with the left lobe anterior to the stomach. Both portal and hepatic veins can be seen as well as the confluence of the umbilical vein with the left portal vein. The gallbladder may be seen, especially in the third trimester, and should not be confused with an abdominal cyst. Transvaginal Ultrasound Transvaginal scanning provides higher resolution images than can be obtained transabdominally. This can be very helpful when the fetus is small and when a potentially lethal malformation, such as body stalk anomaly, is being considered. Doppler Ultrasound Any apparent cyst should always be examined with Doppler to ensure that it is not a vascular structure. Evaluation of the ductus venosus waveform is used in first-trimester screening for aneuploidy and is an early indicator of a potential cardiac anomaly. In the midtrimester and beyond, ductus venosus Doppler is used to monitor cardiac strain in fetuses with growth restriction as well as in cases with high output. Doppler evaluation helps with the differential diagnosis of intraabdominal masses. A suprarenal mass with a feeding vessel from the aorta is an extralobar sequestration, whereas a mass that has "speckled" flow and no feeding vessel is more likely to be a neuroblastoma. Serial Doppler assessment is used to monitor vascular lesions such as an umbilical vein varix. Solid organs, particularly the liver, spleen, and kidneys, are very well demonstrated. The course of the colon is easily followed, adding valuable information when an anorectal malformation is being considered. Rarer schisis defects of the body wall away from the umbilical area may not be seen in this view alone. Gastroschisis, the most common type, is generally located to the right of the umbilical cord insertion, and is not covered by membrane. The small bowel is the most commonly extruded organ, although the stomach, large bowel, and other structures may also be involved. Rarely, an omphalocele may rupture; in these cases it may be difficult to distinguish from gastroschisis.
In kidney transplant patients pregnancy test positive purchase 20 mg nolvadex mastercard, in-hospital mortality was 11% for tissue and 15% for mechanical valve patients menopause chit chat order online nolvadex, and 2-year mortality rates were 62% and 60% menstrual migraine symptoms cheap nolvadex 10 mg without prescription, respectively womens health imaging discount 20 mg nolvadex. In the entire cohort of kidney transplant patients menstruation graph 10 mg nolvadex order free shipping, the rate of endocarditis after valve surgery was 5% per year. Whether prevention of recurrent hypervolemia reduces cardiovascular morbidity and mortality remains unproved. If adjustments are made for comorbidity and advanced age, a strong, incremental risk of all-cause and cardiovascular mortality is associated with interdialytic weight gains. Tolerance of large ultrafiltration volumes may indicate that the dry weight target (see Chapter 94) has not been reached. Reaching an optimal dry weight, however, does not necessarily lead to immediate blood pressure correction; a lag phase of some weeks can precede improvement. In-hospital mortality was 24% and 1-year survival only 38% for patients hospitalized in 1997 to 2000. Dialysis-associated pericarditis may be related to intercurrent illnesses (including viral infections), fistula recirculation leading to underdialysis, or underlying diseases such as systemic lupus, but the exact pathogenesis remains obscure. Fever with pericardial pain or a rub on heart auscultation, unexplained cardiomegaly on chest films, or hemodynamic instability should prompt echocardiography. Blood Pressure Measurements Outcome prediction by ambulatory blood pressure monitoring is not necessarily better than by office blood pressure measurements. However, ambulatory monitoring is useful to identify high-risk nondippers and inverted dippers, allowing consequent treatment adjustments. End-stage renal disease patients are poorly suited for conventional exercise stress electrocardiography because of limited exercise tolerance and frequent resting electrocardiographic abnormalities. Accuracies of pharmacologic stress echocardiographic and nuclear scintigraphic techniques are remarkably variable over the world; they clearly are operator dependent, and the approach of individual sites to cardiac screening should rely on institutional expertise. Moreover, prediction of the likelihood of future events may differ considerably from prediction of coronary anatomy. The evidence for prophylactic revascularization of asymptomatic renal transplant candidates (or any other patient group) is weak. For patients subsequently found to have angiographically indeterminate lesions, measurement of fractional flow reserve is used to make decisions about revascularization. Another problem may be the requirement for a large-bore intravenous line for rapid injection of radiocontrast media. Detection of any cardiovascular calcification predicts worse outcome in dialysis patients. Food and Drug Administration approved the measurement of cTnT in dialysis patients for the indication of risk stratification (mortality prediction) in 2004. Hallmarks of therapy are volume control (see Chapter 94) and prevention of sodium overload, particularly through dietary sodium restriction. Calcium channel blockers and most other antihypertensive drugs, including centrally acting sympathetic inhibitors, are useful when administered complementarily. Anti-inflammatory treatment strategies, such as statins and aspirin, have beneficial effects on cardiovascular mortality in the general population. Meanwhile, a careful search for infectious processes, such as periodontal disease, and use of ultrapure water are recommended in dialysis patients with inflammation. Altered intestinal microbial flora is a potential novel risk factor for systemic uremic inflammation, which merits further study. Because recent data show that the harm associated with severe hypoglycemia might counterbalance the potential benefit of intensive glucose-lowering treatment, treating to a hemoglobin A1c (HbA1c) level below 7. However, this goal was unsupported by clinical trials targeting dialysis patients. Underrepresentation of renal disease in randomized controlled trials of cardiovascular disease. Prognostic value of reduced left ventricular ejection fraction at start of hemodialysis therapy on cardiovascular and all-cause mortality in end-stage renal disease patients. Long-term survival of incident hemodialysis patients who are hospitalized for congestive heart failure, pulmonary edema, or fluid overload. Trends in the incidence of atrial fibrillation in older patients initiating dialysis in the United States. Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: Results from the atherosclerosis risk in communities study. Emerging biomarkers for evaluating cardiovascular risk in the chronic kidney disease patient: How do new pieces fit into the uremic puzzle Association of mild to moderate chronic kidney disease with venous thromboembolism: Pooled analysis of five prospective general population cohorts. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Smoking and cardiovascular outcomes in dialysis patients: the United States Renal Data System Wave 2 study. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: A populationlevel cohort study. How to manage the renal patient with coronary heart disease: the agony and the ecstasy of opinion-based medicine. Clinical characteristics of dialysis patients with acute myocardial infarction in the United States: A collaborative project of the United States Renal Data System and the National Registry of Myocardial Infarction. Renal failure and acute myocardial infarction: Clinical characteristics in patients with advanced chronic kidney disease, on dialysis, and without chronic kidney disease. A collaborative project of the United States Renal Data System/National Institutes of Health and the National Registry of Myocardial Infarction. Chronic kidney disease and risk for presenting with acute myocardial infarction versus stable exertional angina in adults with coronary heart disease. Long-term outcomes of revascularization for peripheral vascular disease in end-stage renal disease patients. Impairment in glomerular filtration rate or glomerular filtration barrier and occurrence of stroke. Incident atrial fibrillation and risk of endstage renal disease in adults with chronic kidney disease. Warfarin, kidney dysfunction, and outcomes following acute myocardial infarction in patients with atrial fibrillation. Hemodialysis-induced repetitive myocardial injury results in global and segmental reduction in systolic cardiac function. Pediatric myocardial stunning underscores the cardiac toxicity of conventional hemodialysis treatments. Fluid retention is associated with cardiovascular mortality in patients undergoing long-term hemodialysis. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: the National Health And Nutrition Examination Survey, 2001 to 2010. Association between cholesterol level and mortality in dialysis patients: Role of inflammation and malnutrition. Insulin resistance as an independent predictor of cardiovascular mortality in patients with end-stage renal disease. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Morphology of coronary atherosclerotic lesions in patients with end- stage renal failure. The elephant in uremia: Oxidant stress as a unifying concept of cardiovascular disease in uremia. Mechanisms of endothelial dysfunction in resistance arteries from patients with end-stage renal disease. Circulating fibroblast growth factor-23 is associated with vascular dysfunction in the community. The relationship between serum calcium and phosphate levels and cardiac valvular procedures in the hemodialysis population. Baroreflex effectiveness index and baroreflex sensitivity predict all-cause mortality and sudden death in hypertensive patients with chronic renal failure. Heart valve prosthesis selection in patients with end-stage renal disease requiring dialysis: A systematic review and meta-analysis. Hospitalizations for bacterial endocarditis after initiation of chronic dialysis in the United States. The risk of valve surgery for endocarditis in patients with dialysis-dependent renal failure. Modifiable risk factors associated with sudden cardiac arrest within hemodialysis clinics. Sudden cardiac death in end-stage renal disease patients: A 5-year prospective analysis. Outcome of cardiac arrests attended by emergency medical services staff at community outpatient dialysis centers. Benefit of primary prevention implantable cardioverter-defibrillators in the setting of chronic kidney disease: A decision model analysis. Survival of dialysis patients after cardiac arrest and the impact of implantable cardioverter defibrillators. Trends in the use and outcomes of implantable cardioverter-defibrillators in patients undergoing dialysis in the United States. Kidney function, electrocardiographic findings, and cardiovascular events among older adults. Carvedilol increases two-year survival in dialysis patients with dilated cardiomyopathy: A prospective, placebocontrolled trial. Prognostic value of dobutamine stress echocardiography in patients with chronic kidney disease. Dobutamine stress echocardiography and cardiac troponin T for the detection of significant coronary artery disease and predicting outcome in renal transplant candidates. Cardiac disease evaluation and management among kidney and liver transplantation candidates: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Distribution of coronary artery disease and relation to mortality in asymptomatic hemodialysis patients. Location of acute coronary artery thromboses in patients with and without chronic kidney disease. Predictive value of cardiac troponin I and T for subsequent death in end-stage renal disease. Multi-biomarker risk stratification of N-terminal pro-B-type natriuretic peptide, high-sensitivity C-reactive protein, and cardiac troponin T and I in end-stage renal disease for all-cause death. Serum cardiac troponin and subclinical cardiac status in pediatric chronic renal failure. Troponin T for the detection of dialysis-induced myocardial stunning in hemodialysis patients. The survival advantage for haemodialysis patients taking vitamin D is questioned: Findings from the Dialysis Outcomes and Practice Patterns Study. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary interventions. Impact of renal dysfunction on outcomes of coronary artery bypass surgery: Results from the Society of Thoracic Surgeons National Adult Cardiac Database. Comparison of percutaneous coronary intervention with medication in the treatment of coronary artery disease in hemodialysis patients. Early invasive treatment benefits patients with renal dysfunction in unstable coronary artery disease. Risks of death and end-stage renal disease after surgical compared with percutaneous coronary revascularization in elderly patients with chronic kidney disease. Long-term survival and repeat coronary revascularization in dialysis patients after surgical and percutaneous coronary revascularization with drug-eluting and bare metal stents in the United States. Sirolimus-eluting stents vs bare metal stents for coronary intervention in Japanese patients with renal failure on hemodialysis. Impact of drug-eluting stents on clinical and angiographic outcomes in dialysis patients. Long-term clinical outcomes after sirolimus-eluting stent implantation in dialysis patients. Pravastatin for secondary prevention of cardiovascular events in persons with mild chronic renal insufficiency. Effects of statins in patients with chronic kidney disease: Meta-analysis and meta-regression of randomised controlled trials. Effect of atorvastatin on inflammation and outcome in patients with type 2 diabetes mellitus on hemodialysis. Effects of short daily versus conventional hemodialysis on left ventricular hypertrophy and inflammatory markers: A prospective, controlled study. The antioxidant acetylcysteine reduces cardiovascular events in patients with end-stage renal failure: A randomized, controlled trial. Effect of ultrapure dialysate on markers of inflammation, oxidative stress, nutrition and anemia parameters: A metaanalysis. Effect of sevelamer and calcium-based phosphate binders on coronary artery calcification and accumulation of circulating advanced glycation end products in hemodialysis patients. Oral active vitamin D is associated with improved survival in hemodialysis patients. The ability to correct anemia has suggested that its consequences may go beyond general fatigue and reduced physical capacity to affect a broad spectrum of physiologic functions. The costs of anemia management are considerable, and it has also become apparent that full anemia correction may cause harm; therefore a rational and careful consideration of the risks and benefits is mandatory. Both red cell life span and the rate of red cell production are reduced, but the latter is more important. Erythropoietin is a glycoprotein hormone consisting of a 165 amino acid protein backbone and four complex, heavily sialylated carbohydrate chains. In particular, in patients on dialysis, average Hb values have steadily increased for many years, and then declined again in view of new evidence suggesting lower target levels. Data are from a crosssectional survey of individuals randomly selected from the general U.
Normal Development One of the great challenges in pediatric neuroimaging is understanding the dynamic development of the human brain from the fetus to the adult menstrual cycle age 7 nolvadex 20 mg purchase with visa. Understanding this normal development allows for accurate identification of normal vs women's health magazine big book of yoga purchase nolvadex now. A delayed sulcation pattern may suggest a malformation of cortical development on the spectrum of lissencephaly or gyral simplification menstruation quotes funny purchase nolvadex without prescription, whereas the presence of too many sulci for gestational age may suggest polymicrogyria menstruation in dogs nolvadex 20 mg buy mastercard. During the first 2 years of life women's health clinic quad cities order nolvadex no prescription, an understanding of the normal myelination pattern allows for accurate identification of conditions associated with delayed myelination. Because understanding normal myelination is so critical, this edition includes a 4-page chapter dedicated to the topic. Another important point regarding myelination is that certain diseases have very different imaging characteristics during the 1st year of life compared with later years. A prime example of this can be seen in Tuberous Sclerosis in which cortical tubers & radial migration lines are T1 hyperintense & T2 isointense prior to myelination & exactly the opposite (T1 hypointense & T2 hyperintense) following myelination. Tuberous sclerosis is just 1 of many diagnoses with such dynamic imaging characteristics over time. The anterior pituitary in the newborn is very T1 hyperintense, often equal to that of the posterior pituitary. This hyperintensity is presumed to be related to maternal hormones, as the same finding is not seen in early premature infants when imaged at term equivalent age. The anterior pituitary slowly decreases in T1 signal intensity & becomes isointense to the pons after the 1st few months of life. Regarding pituitary size, the normal pituitary often has a convex superior margin at birth, slowly becoming flat or concave over the ensuing weeks, an appearance that is typically maintained in male patients throughout life & in female patients until puberty. The imaging professional should not be alarmed to see an enlarged pituitary with a convex superior border in a teenage girl. This is a normal appearance in this age, & sex should not in & of itself raise suspicion for a pituitary lesion. Terminology There is a constant process in science & medicine of renaming entities to more accurately reflect new knowledge gained. This can make understanding, teaching, & researching these disease processes difficult. When a disease has many names, a comprehensive literature search becomes significantly more difficult to confidently perform. For the child over 24 months, adult-type sequences can be employed but should be specifically tailored to answer the clinical question at hand. Volumetric imaging is optimal for tumor follow-up, giving the imaging professional confidence in tumor size measurements from 1 exam to the next. Finally, volumetric imaging is helpful because it allows reconstruction in multiple planes with no penalty in exam length. Cerebral Edema A common & important neuroimaging finding is the development of brain edema, of which 4 basic types are recognized. Vasogenic edema reflects expansion of the interstitial fluid compartment in response to an irritating stimulus such as tumor or inflammation. Cytotoxic edema is due to expansion of the intracellular fluid compartment secondary to failure of the sodium-potassium pump regulation of the cell membrane. In transependymal edema, increased hydrostatic pressure in the ventricular system prevents the normal progression of interstitial fluid into the ventricles & causes congestion in the periventricular white matter. Perhaps the least understood is posttraumatic edema, in which diffuse brain swelling is caused by a combination of cytotoxic & vasogenic edema resulting from a cascade of events that include sodium-potassium pump failure, diminished cerebral perfusion & autoregulation, & loss of integrity of the blood-brain barrier. Posttraumatic cerebral edema typically sets in several hours after the initial injury & can lead to rapid increases in intracranial pressure & death. Clinical management of traumatic brain injury usually includes imaging reassessment within the first 12 hours after presentation to look for progression of initially identified injuries, such as contusions & intracranial hemorrhage. The radiologist must be diligent in looking for signs of increased brain swelling at this time also; such signs include effacement of previously identifiable sulci at the vertex & decrease in size of basal cisterns. The presence of these signs should lead to more aggressive monitoring & management of intracranial pressure. Waiting until clinical signs develop is too late to effectively combat the cycle of reduced cerebral perfusion & progressive cellular injury. Diffuse cerebral edema is the leading cause of death from cases of child abuse, & the traumatic nature of the insult may not be readily apparent at first presentation. Nontraumatic insults, such as acute encephalitis & status epilepticus, can also lead to this potentially fatal complication. Imaging Protocols the development & use of high-quality indication-specific imaging protocols are essential to the practice of pediatric neuroradiology. This signal & morphology are presumably related to maternal hormones, as early premature infants imaged at term equivalent ages do not have this appearance. Over the 1st few weeks of life, the anterior pituitary becomes isointense to the pons with a flat or concave superior border. An enlarged (up to 9 mm vertical) anterior pituitary with a convex superior border in a teenage girl should not raise concern. Progressive myelination & thickening of the corpus callosum begin with the posterior body & splenium. The posterior 1/2 of the corpus callosum continues to thicken as the anterior body, genu, & rostrum begin to myelinate at 4 months. By the end of the 1st year of life, the corpus callosum is completely myelinated with uniform signal intensity. Following myelination, these lesions show varying degrees of hypointensity compared with adjacent white matter. Treatment is an endoscopic 3rd ventriculostomy, which appears patent as evidenced by the dark flow artifact across the floor of the 3rd ventricle. With axial images alone, it can be difficult to distinguish subdural hemorrhage from venous sinus thrombosis. Also note the axially oriented right parietal bone fracture, which was difficult to see on axial images. Uda S et al: Normal development of human brain white matter from infancy to early adulthood: a diffusion tensor imaging study. Tucker J et al: Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections. The torcular Herophili lies above the lambdoid suture (torcular-lambdoid inversion). There is characteristic thickening & elongation of the superior cerebellar peduncles. Note the brain tissue protruding through defects of the right frontal bone, nasal bone, & cribriform plate. However, there is separation of the parietal & occipital lobes with the falx cerebri identified posteriorly. T2hypointense Probst bundles are seen along the medial margins of the lateral ventricles. Also noted is the classic trident shape of the upturned lateral ventricle frontal horns. Wiechec M et al: Four steps in diagnosing complete agenesis of the corpus callosum in prenatal life. Paladini D et al: Agenesis of the fetal corpus callosum: sonographic signs change with advancing gestational age. Raybaud C: the corpus callosum, the other great forebrain commissures, and the septum pellucidum: anatomy, development, and malformation. Note the shift of midline structures, excess of gray-white matter, flattened gyri, & abnormal lateral ventricle frontal horn. Abnormal white matter signal intensity in the left cerebrum is due to neuronal dysplasia, accelerated myelination, &/or mineralization. The left hemispheric lissencephaly has a thick deep cellular layer of gray matter with a thin, smooth outer cortex. The sylvian fissures are vertically oriented, giving an hourglass or figure 8 configuration to the brain. There is significant cerebellar atrophy, which has progressed from the prior studies & is likely related to antiepileptic medications. Kato M: Genotype-phenotype correlation in neuronal migration disorders and cortical dysplasias. Note the thin layer of intervening white matter between the band of heterotopic gray matter & cortex. Arnautovic A et al: Pediatric and adult Chiari malformation type I surgical series 1965-2013: a review of demographics, operative treatment, and outcomes. Tonsillar Herniation From Increased Intracranial Pressure · Neoplasm, hemorrhage, hydrocephalus, ischemia Intracranial Hypotension · Sagging midbrain, sunken hindbrain with diffuse dural thickening/enhancement, distended veins/dural sinuses, ± subdural hygromas 6. Note the absence of the greater sphenoid wing, consistent with sphenoid wing dysplasia. Note that the location of the nodules adheres to the distribution of fetal germinal matrix with a preponderance in the caudothalamic grooves. Krsek P et al: Predictors of seizure-free outcome after epilepsy surgery for pediatric tuberous sclerosis complex. Pascual-Castroviejo I et al: Significance of tuber size for complications of tuberous sclerosis complex. Note the low signal within the subcortical white matter at the depth of sulci, consistent with Ca². There is mildly increased right calvarial thickness secondary to underlying brain parenchymal volume loss. Enlargement of the left lateral ventricle is secondary to left cerebral volume loss. Inset demonstrates extension of melanosis into the brain substance along the VirchowRobin spaces. The largest & most conspicuous lesions are located in the medial temporal lobes, the most common location for parenchymal melanosis. The pial melanosis involves virtually the entire surface of the brain, enhancing strongly & uniformly. Without the associated mass effect on the brainstem & cerebellum, this lesion would not be visible on this sequence. This is a characteristic feature of an epidermoid cyst, which was confirmed at surgery. It can be difficult to distinguish a lipoma from a dermoid cyst, but substantial growth over time favors the latter. The visual symptoms could reflect Parinaud syndrome, which can occur with larger pineal cysts. Note the mass effect on the 4th ventricle with secondary dilation of the lateral ventricle temporal horns, consistent with obstructive hydrocephalus. Alkonyi B et al: Differential imaging characteristics and dissemination potential of pilomyxoid astrocytomas versus pilocytic astrocytomas. Ependymoma · "Plastic" tumor: Extends out 4th ventricle foramina · Ca², cysts, hemorrhage common 5. Pilomyxoid Astrocytoma · More aggressive, less common tumor; usually suprasellar · Hemorrhage & arterial spin labeling perfusion suggestive 6. Note the indistinct interface with the posterior 4th ventricle (roof), typical of medulloblastoma. Raybaud C et al: Posterior fossa tumors in children: developmental anatomy and diagnostic imaging. Note the mildly hyperattenuating solid component, reflecting the high cellularity of the tumor. Choroid Plexus Tumors · Intraventricular mass · Vigorous, homogeneous enhancement 5. Note the enlargement of the temporal horns & 3rd ventricle, consistent with obstructive hydrocephalus. The mass encases the enhancing left vertebral artery without narrowing it, further demonstrating its plastic nature as it extends between the left cerebellar tonsil & brainstem. The large size, heterogeneous solid component, & cysts are typical of a supratentorial ependymoma. Such distant extension of signal abnormality typically suggests an infiltrative, higher grade tumor. Klimo P Jr et al: Malignant brainstem tumors in children, excluding diffuse intrinsic pontine gliomas. The lack of enhancement & lack of interval growth (or very slow growth over time) is typical for a tectal plate glioma. Note the dominant cystic component with a duralbased plaque of desmoplastic stroma. Areas of attenuation equal to gray matter correspond to cellular areas of the tumor. Note cystic areas containing fluid-fluid levels in the anterior aspect of the lesion, consistent with foci of intracystic hemorrhage. Frontal extension of the large cystic components is typical of a prechiasmatic location. Cystic contents often show intrinsic T1 shortening before contrast, as in this case. Calcifications are common in pineal germinoma & are thought to represent pineal Ca² "engulfed" by tumor. Peritumoral edema is a common finding (~ 40%) in germinoma, as are multiple ependymal metastases. After contrast (right), the infundibular mass enhances homogeneously, typical of germinoma. The basal ganglia are a less common (~ 15%) location for germinoma (though these tumors are often large).
Bronchodilators are still used but only when antiinflammatory therapy is inadequate breast cancer awareness clothing purchase nolvadex 20 mg amex, and then in smaller amounts menstrual related migraines order nolvadex online pills. Plasma cells in lymphoid tissue of respiratory mucosa release immunoglobulin E (IgE) C breast cancer pain purchase nolvadex overnight delivery. In theory women's health center metro pkwy cheap nolvadex online american express, drugs acting as anti-IgE antibodies would prevent IgE binding to mast cell surfaces pregnancy day by day calendar order nolvadex 20 mg with mastercard. This action would reduce formation of activated antigen-IgE complexes and suppress release of mediators that induce immediate bronchoconstriction in the early phase. That is, mediators such as histamine, prostaglandins, and leukotrienes would be unable to cause sneezing, wheezing, itching, and coughing. The most notable anti-IgE antibody, Rhumab-E25, is a recombinant humanized monoclonal antibody to IgE. By binding to circulating IgE in the blood, Rhumab-E25 blocks release of inflammatory mediators by keeping IgE from binding to mast cells. Antigen reacts with antibody (IgE) on membrane of sensitized mast cells and/or basophils, which respond by secreting pharmacologic mediators Vagus nerve Mast cell degranulation blockers Histamine Mucous gland hypersecretion Smooth muscle contraction Increased capillary permeability and inflammatory reaction Eosinophil attraction F. Both drugs, usually inhaled as aerosols, can be used for intrinsic (antigen-induced) or extrinsic (nonantigen-induced) asthma. Nedocromil enhances corticosteroid effects and is more potent than cromolyn in patients with extrinsic asthma (especially exercise induced); even when given after reexposure to antigen, it blocks delayed inflammation. Both drugs are poorly absorbed, so adverse effects (eg, chest tightness, cough) are restricted to deposition site. Both drugs alter Cl- channel function, which (1) on airway neurons underlies cough inhibition, (2) on mast cells delays antigen-evoked bronchoconstriction, and (3) on eosinophils prevents inflammatory responses to antigens. Some agents, especially theophylline and 2-adrenergic agonists, inhibit late response inflammation. These drugs are usually used when a persistent cough and bronchial constriction are present. In addition to relaxing smooth muscles and reducing airway reactivity, bronchodilators reduce coughing, wheezing, and shortness of breath. Agents are usually given via inhalation, but some can be given orally or parenterally (intravenous, intramuscular, or subcutaneous route). Most drugs have a rapid onset of action (within minutes), but the effect usually wanes in 5 to 7 hours. The most common bronchodilators are methylxanthines (eg, theophylline, caffeine), -adrenergic agonists (eg, isoproterenol, albuterol, epinephrine), and cholinergic antagonists (eg, atropine, tiotropium). Or, theophylline may block cell surface receptor effects of adenosine, which may induce bronchoconstriction and inflammation. Theophylline, the most widely prescribed and of low cost, comes as short-acting tablets and syrups, sustained-release capsules and tablets, and intravenous doses. Even at low to moderate doses, these drugs enhance cortical arousal and alertness and defer fatigue. Methylxanthines reduce blood viscosity, increase blood flow, increase cardiac output, and induce tachycardia in healthy subjects. These drugs relax bronchial smooth muscle, inhibit mediator release, increase transport of mucus, and alter composition of mucus by stimulating adrenoceptors. Bronchodilation is mediated by 2 adrenoceptors that are located on smooth muscle cells in human airways. Nonselective -adrenoceptor agonists (eg, epinephrine, ephedrine, isoproterenol) stimulate all adrenoceptors (1 and 2 classes). Selective drugs that activate only 2 receptors (eg, albuterol, terbutaline, salmeterol) are the most commonly prescribed sympathomimetic agents. If initial response is inadequate, repeat at 30 to 60 minute intervals as needed; oxygen as indicated. If response to epinephrine is inadequate or if patient becomes refractory, give aminophylline intravenously very slowly; administer oxygen. These drugs are potent, rapidly acting bronchodilators, but their stimulation of the cardiac system is a serious drawback. Epinephrine is either inhaled or given subcutaneously and is the active agent in many over-the-counter preparations. Maximal bronchodilation is achieved 15 minutes after injection and lasts approximately 90 minutes. Because this drug stimulates cardiac output, increases heart rate, and exacerbates angina, physicians rarely prescribe it. Ephedrine, used in China more than 2000 years ago, has the longest history of use of any antiasthmatic. It has a longer duration of action, lower potency, and greater oral activity than epinephrine. Isoproterenol is characterized by a rapid onset of action, with peak bronchodilation occurring within 15 minutes of injection. The major drugs-metaproterenol, terbutaline, albuterol, salmeterol, and formoterol-have minimal 1-mediated effects on the nervous and cardiac systems. The inhalation route allows the greatest local effects with the fewest adverse effects. Inhaled agents cause bronchodilation that equals that of isoproterenol and persists for 4 hours. Terbutaline, the only drug that can be used subcutaneously, is given for severe asthma attacks or if insensitivity to inhaled agents exists. Two new drugs, salmeterol and formoterol, have a long duration of action and high lipid solubility. Both drugs at high concentrations move slowly into airway smooth muscle, so effects can last up to 12 hours. When stimulated, muscarinic receptors cause muscle contraction, which leads to narrowing of the airways and bronchoconstriction. Muscarinic antagonists, or anticholinergics, prevent acetylcholine from producing smooth muscle contractions and excess mucus in the bronchi. However, these drugs enhance bronchodilation induced by 2-adrenoceptor agonists, so patients often take both anticholinergics and 2 agonists. Dry mouth, bitter taste, scratchy throat, and headache are the major adverse effects. Corticosteroids Plasma clearance In chronic steroid administration, if dosage is withdrawn or suboptimal, severe asthmatic exacerbations may occur. Lysosome stabilization Antiinflammatory effect Inhibition of antibody formation Possible inhibition of histamine formation/storage Steroid-resistant patients may require higher and continuous dosage. Treatment with these agents improves symptoms of asthma, allergic rhinitis, eczema, and rheumatoid arthritis. Corticosteroids inhibit late phase allergic reactions (including late asthmatic response to antigen challenge) by various mechanisms, eg, reduced (1) number of mast cells lining the surfaces of airway mucosal cells; (2) chemotaxis and activation of eosinophils; and (3) cytokine production by eosinophils, monocytes, mast cells, and lymphocytes. Corticosteroids taken regularly reduce bronchial reactivity, enhance airway quality, and decrease the severity and frequency of asthma attacks. These drugs would be the only ones needed to treat asthma if their adverse effects were not so pronounced. Commonly used agents are prednisone, methylprednisone, beclomethasone, flunisolide, budesonide, and mometasone. Intranasal corticosteroids relieve stuffy nose, nasal irritation, and other discomforts. Spacers (chambers) can be attached to metered-dose inhalers to reduce the velocity and particle size of the drug; the amount of drug reaching the lungs is maximized, and the quantity of drug deposited in the mouth is minimized. Spacers are crucial for therapy with corticosteroids, which have many adverse effects. The smaller, regular doses reduce side effect risk and may eliminate a need for aerosol steroids. Short-term use (days) of prednisone can lead to increased appetite, weight gain, diarrhea, headache, mood changes, and insomnia, and possibly hyperglycemia and hypertension. Cessation of shortterm corticosteroid use or taking smaller doses of these agents usually minimizes or eliminates the effects. Efforts to develop safer corticosteroids with antiinflammatory properties but lacking adverse effects are ongoing. Lipophilic steroids, such as beclomethasone, flunisolide, budesonide, and mometasone, have a strong safety profile and are almost devoid of the orally precipitated systemic effects. The enzyme 5-lipoxygenase catalyzes synthesis of arachidonic acid into unstable intermediates, which are converted into leukotrienes. A number of airway cells (including mast cells, macrophages, eosinophils, and basophils) synthesize, store, and secrete several subtypes of proinflammatory leukotrienes. Evidence that inhaled leukotrienes increase bronchial reactivity and that antigen challenge in sensitized airways augments leukotriene synthesis supports a role for these mediators in asthma and a rationale for development of drugs that block leukotriene or 5-lipoxygenase action. When taken regularly, these drugs work as well as inhaled corticosteroids in reducing the frequency of asthma attacks. However, leukotriene antagonists are less successful for relieving symptoms, reducing bronchial reactivity, and improving airway quality. These drugs are effective and safe when taken orally, an advantage compared with inhaled corticosteroids. The strong safety profile and excellent oral activity account for the popularity of leukotriene antagonists for children. Leukotriene antagonists also reduce responses in aspirin-induced asthma, a disorder affecting nearly 10% of patients with asthma. Airway irritation activates the reflex, which forcefully removes irritants, by stimulating the airways, which then activates afferent nerves going from respiratory passages through the vagus nerve to the medulla. Activated cough receptors in the medulla drive a reflex that initiates inspiration (2. Coughs triggered by drainage of mucus from nasal passages into airways are treated with cough suppressants (antitussives). Coughs occurring with blood, chest pain, shortness of breath, weight loss, or dyspnea may indicate serious disease. Opioids include opiates (morphine and drugs derived from the opium poppy plant, such as hydromorphone, hydrocodone, and codeine) and synthetic drugs that mimic effects of morphine. Opioids desensitize central cough receptors, reduce airway mucous secretion, and alter mucous composition. These drugs also produce many adverse effects, including analgesia, addiction, sedation, euphoria, respiratory depression, nausea, vomiting, and constipation. The doses of opioids needed to suppress cough are lower than doses that evoke most of the undesirable effects, particularly analgesia and addiction. Dextromethorphan, a morphine derivative and glutamate antagonist, suppresses the cough center and has fewer adverse effects than other opioids, which accounts for its popularity in over-thecounter preparations. Bronchi remain open because of positive pressure within lumen and slower flow rates. Heredity, secondhand smoke, exposure to air pollution, and history of childhood respiratory infections are also major risk factors. Emphysema causes irreversible lung damage by weakening and destroying air sacs within the lungs, which reduces lung elasticity and causes airway collapse and obstruction. Chronic bronchitis is an inflammatory disease that begins in smaller lung airways and advances gradually to larger airways. Increased mucus in the airways and more frequent bacterial infections in the bronchia result, which, in turn, impedes airflow. Emphysema in children is usually caused by congenital abnormalities of the lung and 1-antitrypsin deficiency. Although emphysema ranks ninth among chronic conditions that reduce activity, the seriousness of the disease varies. Some persons never reach a stage of incapacity and live with relatively little inconvenience. Shortness of breath, chronic cough, cyanosis (bluish coloration of skin caused by lack of oxygen), and exertion-induced wheezing are the most common symptoms. Dizziness, anxiety, stress, impotence, fatigue, impaired ability to concentrate, excessive daytime sleepiness, and insomnia may also occur. Tobacco smoke and other pollutants promote release of chemicals within alveoli that damage the walls of air sacs. The alveoli play a critical role in respiration because they facilitate exchange of oxygen from the air for carbon dioxide in the blood. Damage to air sac walls is irreversible and results in permanent holes in tissues of the lower lungs. The lungs can thus transfer less oxygen to the bloodstream, which causes shortness of breath. Emphysema does not develop suddenly; it occurs after years of exposure to cigarette smoke, air pollution, and irritating fumes. This protein is produced by hepatic cells and protects lungs by blocking effects of enzymes called elastases. Elastases, carried in leukocytes, protect lungs by killing inhaled bacteria and removing tiny particles. Intravenous 1-proteinase inhibitor, a novel therapy for this deficiency, replaces 1-antitrypsin in the blood. Symptoms of inherited emphysema are also managed by exercise, avoiding infection, oxygen therapy, and pulmonary rehabilitation. Smoking accelerates progression of the disease and shortens lifespan, so avoiding cigarettes and secondhand smoke is critical. Lung transplantation and lung reduction surgery are options for patients with serious effects of 1-antitrypsin deficiency. Bronchitis is inflammation of the bronchi causing excessive production of mucus and swelling of bronchial walls. Many people with a severe cold experience a brief attack of acute bronchitis, which is usually accompanied by fever, cough, wheezing, and spitting.
In this case women's health group tallmadge ohio discount nolvadex 10 mg overnight delivery, there is mild pelviectasis and malrotation women's health recipe finder buy 20 mg nolvadex mastercard, with the renal pelvis oriented anterolaterally (bladder) pregnancy or period purchase nolvadex 10 mg with mastercard. In this case embarrassing women's health issues nolvadex 20 mg buy otc, the left renal artery is normally located breast cancer 14s 20 mg nolvadex order visa, and 2 right renal arteries originate near the aortic bifurcation. The blood supply is variable but most commonly comes from the aorta &/or iliac arteries. Close inspection of the midline reveals renal parenchyma bridging anterior to the aorta, even in the 2nd trimester. However, the parenchyma will have the hypoechoic medullary pyramids and relatively more echogenic cortex. The renal pelves can also be a clue that the "mass" is actually a horseshoe kidney. Note that the ureter of the ectopic kidney crosses the midline and both ureters have a normal course as they enter the bladder. There is an ectopic smaller left kidney on the same side that adjoins the lower pole of the right kidney just above the bladder. In the setting of renal agenesis, the adrenal glands lose their triangular shape and have a flattened appearance, filling the renal fossa, and potentially being mistaken for kidneys. Note the flattened, lying down appearance of glands, which is typically present when the ipsilateral kidney is absent. The bladder is anatomically present in renal agenesis; however, lack of urine production causes the bladder to remain collapsed. The chest is small, with the heart essentially filling the thorax and only a small crescent of lung visible. The nose is flattened, the ears are low-set and abnormally folded, and there is micrognathia. Rianthavorn P et al: Diagnostic accuracy of neonatal kidney ultrasound in children having antenatal hydronephrosis without ureter and bladder abnormalities. Ureteropelvic Junction Obstruction Genitourinary Tract (Left) Coronal ultrasound of the kidneys shows a dilated renal pelvis extending to the bladder. The elongated dilated pelvis should not be mistaken for a unilocular cyst or dilated ureter. The left renal pelvis is distended and an accessory left renal artery is seen at the inferior margin of the distended renal pelvis. Massive renal collecting system dilation in the fetus and neonate can mimic other abdominal masses and cause mass-related symptoms. There is massive distention of the renal pelvis and calyces, as well as significant renal cortical thinning. Notice that the severely obstructed affected kidney has echogenic renal parenchyma when compared to the contralateral kidney. Postobstructive renal parenchymal change is often seen in conjunction with urinomas since both are sequelae of severe obstruction. Almost always, the fluid has some contact with the lateral lumbar spine, as seen in this case. However, subtle subcortical cysts are seen, suggesting the obstruction has caused renal dysplasia. Also, note the increased renal parenchymal echogenicity and loss of corticomedullary differentiation. Renal size is variable with obstructive renal dysplasia, especially during fetal life. Obstructive Renal Dysplasia Genitourinary Tract (Left) Coronal view of the right kidney shows segmental upper pole cystic dysplasia (calipers) from renal duplication and upper moiety obstruction (note the calyceal dilatation). Upper pole obstructing ureteroceles may cause segmental renal cystic dysplasia, which can mimic a suprarenal mass. Lower urinary tract obstruction is the most common cause of bilateral obstructive renal dysplasia. The kidney is large, and there is mass effect upon the diaphragm and abdominal vessels. It is assumed that the left kidney will not function, and, therefore, it is imperative the right kidney is followed carefully in utero and after delivery. In this case, amniotic fluid volume was normal throughout pregnancy, and the diagnosis was established after delivery. Increased renal echogenicity results from the many interfaces created by the dilated renal tubules. In this case, the kidneys are very large (calipers measure a 9 cm left kidney) and the medullary pyramids are echogenic. This is a characteristic finding but may be difficult to discern on prenatal scans. When large, it can be difficult to determine the organ of origin of a mass, so it is important to scan in multiple planes and define normal structures. The most common solid fetal renal tumor is a mesoblastic nephroma, which was confirmed postnatally. Although predominately solid, cystic areas may be present within a mesoblastic nephroma. The tumor was resected on the 2nd day of life; however, bleeding could not be controlled, and the infant expired. Normal renal parenchyma forms a claw around the mass, confirming it is renal in origin. The fetus had unexplained hydrops and was delivered at 32 weeks for nonreassuring heart tracing. The working diagnosis was intrauterine infection with stress-induced bilateral adrenal hemorrhage. This was substantially smaller than the mass seen in utero and resolved completely on follow-up. Maki E et al: Imaging and differential diagnosis of suprarenal masses in the fetus. There is dramatic hepatomegaly with the low-signal spleen sandwiched between the liver and the neuroblastoma. The liver is heterogeneous with small, scattered, irregular cysts, the result of metastatic infiltration. The infant began immediate multiagent chemotherapy with excellent response and is doing well. Natural History & Prognosis · Variable fetal course May resolve spontaneously Most remain stable without complications Minority progress to hydrops and even death 630 Neuroblastoma Genitourinary Tract (Left) Coronal ultrasound of the fetal abdomen (top) shows a solid, echogenic mass (calipers) above the right kidney. Sagittal ultrasound after delivery (bottom) confirms a solid, suprarenal mass (calipers). Most fetal neuroblastoma is low risk and has both a favorable stage and biologic markers. Current treatment recommendations are for a more conservative approach, with many being followed rather than resected. It is important to interrogate the mass with color Doppler to rule out a feeding vessel, as would be seen with an extralobar sequestration. Tumor invasion into the spinal canal is confirmed with displacement of the spinal cord to the right. Most fetal neuroblastomas arise from the adrenal gland, but they can occur anywhere along the sympathetic chain, as in this case. Khattab A et al: Noninvasive prenatal diagnosis of congenital adrenal hyperplasia. The valve forms a thin membrane of tissue, blocking antegrade flow of urine and creating a lower urinary tract obstruction. In combination with oligohydramnios, these findings can result in lung hypoplasia. The collecting system may partially decompress, but persistent abnormal appearance of the kidneys is typical. There is an irregular, trabeculated bladder with a diverticulum posteriorly due to increased intravesical pressures. Note the absence of a keyhole sign, which is usually seen with posterior urethral valves. In this fetus, an axial view through the perineum shows a massively distended penile urethra. A cystic area in the cord was also seen prenatally, consistent with patent urachus and urine collection near the cord base. Treatment · Serial sonography required throughout pregnancy Monitor degree of bladder dilatation Assess amniotic fluid volume · Vesicoamniotic shunt may aid in decompressing bladder and improving amniotic fluid status Consider early intervention for best possible outcome Performed only if certain criteria met 640 8. Prune-Belly Syndrome Genitourinary Tract (Left) In the 2nd trimester, the renal parenchyma is slightly echogenic, which is suggestive of dysplasia in the setting of a markedly dilated bladder and prune-belly syndrome. When prune-belly syndrome is suspected, careful evaluation of the scrotum will show an empty sac with a lack of the typical echogenic oval testes. Instead, the anterior or penile urethra is dilated and there is no obstruction to urination. The patent urachus allowed urine to decompress into the umbilical cord, with ~ 300 cc of urine-like fluid present on autopsy. In a duplicated system, as shown in the lower graphic, the ectopic ureter enters the bladder inferiorly and medially to the normotopic ureter. Two left ureters are seen, which were dilated throughout their entire course and difficult to separate. It is important to remember that a ureterocele can be misinterpreted as the bladder when the bladder is empty. Ureterocele Genitourinary Tract (Left) In the 2nd trimester, the wall of the ureterocele is very thin and may be missed. Careful evaluation of the bladder with several angles of insonation is warranted, especially in the setting of a suspected renal duplication. The septated cystic "mass" is actually the bladder containing an ectopic ureterocele. In this case, there is a large ureterocele, which creates a smooth filling defect at the bladder base. The urachus is the intraabdominal portion of the allantois and normally involutes by 6-weeks gestational age, forming the median umbilical ligament. During ultrasound evaluation, the cyst may increase in size when the bladder contracts during voiding, sending urine into the cyst. Demographics · Gender 648 Urachal Anomalies Genitourinary Tract (Left) If the urachus remains widely patent, urine can flow into the base of the umbilical cord forming an allantoic cyst. A large cord cyst was seen prenatally and a patent urachus was suspected but could not be documented. With bladder contraction, urine moves retrograde through the urachus into the base of the cord. In this case, urine dissected through the Wharton jelly rather than forming a cyst. Resection of the entire tract is necessary as there is increased risk of infection and malignant transformation in any remnants. Pink is genital tubercle (becomes glans of penis in males and clitoris in females); green is labioscrotal swelling; and blue is cloacal folds and membrane. In the female fetus, the genital tubercle points caudal (down), while in the male fetus, it points cranial (up). There are bilateral soft tissue mounds that may represent the labia or scrotum and a central phallus that may be a clitoris or penis. Although there has been significant virilization, the vagina, uterus, and ovaries (not shown here) are present. Note that the tip of the penis is normally curved, without prepuce folds, making hypospadias a less likely diagnosis. The diagnosis after delivery was "buried penis," from abundance of abdominal wall and penile skin. It has been called the tulip sign with the 3 petals formed by the small penis and the scrotal sacs. Li Y et al: Canalization of the urethral plate precedes fusion of the urethral folds during male penile urethral development: the double zipper hypothesis. This cyst remained stable in utero but was excised postnatally, as it was > 5 cm in size. Pediatric ovaries are intraabdominal, thus more mobile than adult ovaries and at increased risk for torsion. Complex ovarian cysts are much more likely to have internal hemorrhage, which is strongly associated with torsion. The umbilical arteries flank the location of the bladder, indicating that the mass is laterally placed in the abdomen. Fetal hydrops in this case was thought to be caused by anemia from the hemorrhage. Interestingly there was no torsion, but it should always be considered when hemorrhage is present. Differential considerations included a liver mass, but the imaging features were not typical of either a congenital hepatic hemangioma or a mesenchymal hamartoma. There was no apparent adverse impact on fetal well-being, and the infant was delivered at term. Excessive secretion occurs in response to maternal circulating hormones causing vaginal distention, which can be quite marked. The uterus may also expand with fluid (hydrometrocolpos) but, due to its thicker wall distension, is not as significant as the vagina and may not be seen in utero. The normal, hyperintense, meconium-filled rectum is seen as separate structure, excluding a cloacal anomaly. In this case, there was severe oligohydramnios and the fetus had secondary pulmonary hypoplasia. Posterior Urethral Valves Duplicated Collecting System With Obstruction (Left) In this case of renal duplication, the upper moiety is markedly dilated and separate from the mildly dilated lower moiety. The drooping lily sign is also seen, as the lower pole collecting system is inferiorly displaced by the obstructed upper pole.
Purchase nolvadex 20 mg with visa. MSc Women's Health (Full Version).
References
- Zorgniotti AW: Testis temperature, infertility, and the varicocele paradox, Urology 16(1):7n10, 1980.
- Soreide O, Lillestol J, Christensen O, et al: Abdominal aortic aneurysms: survival analysis of four hundred thirty-four patients, Surgery 91(2):188-193, 1982.
- Mishra Y, Mehta Y, Mittal S, et al. Mammary coronary artery stenosis without coronary artery bypass through minithoracotomy: one year clinical experience. Eur J Cardiothorac Surg. 1998;14(Supplement 1):S31-S37.
- Siddiqui MA, Perry CM, Scott LJ: Oxybutynin extended release: a review of its use in the management of overactive bladder, Drugs 64(8):885, 2004.