
Acarbose
| Contato
Página Inicial
Cornelia Liu Trimble, M.D.
- Professor of Gynecology and Obstetrics
https://www.hopkinsmedicine.org/profiles/results/directory/profile/0007730/angelo-demarzo
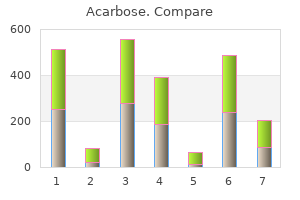
A number of clinical trials are underway to establish the safety diabetes test rite aid order 25 mg acarbose with visa, tolerability and effectiveness of these new compounds diabetic diet kcal purchase cheapest acarbose. More intensive treatment including bone marrow transplantation is sometimes attempted in younger patients with poor prognosis disease diabetes diet chinese recipes acarbose 50 mg order without prescription. The IgM paraprotein may have unusual physical properties such as causing red cell agglutination (cold agglutinins) or precipitating in cold temperatures (cryoglobulin) diabetes university order acarbose 25 mg without prescription. Systemic symptoms such as fever diabetes type 2 or 1 worse purchase genuine acarbose on line, weight loss and night sweats may occur, particularly if the lymphoma undergoes high-grade transformation. Treatment A combination of an alkylating agent such as cyclophosphamide and prednisolone together with the monoclonal antibody rituximab is a favoured first-line therapy. The disorder typifies the so-called low-grade lymphomas, being indolent in its clinical course but remaining incurable. The t(14;18) translocation is thought to arise in early B cells, which then move into the germinal centre of the lymph node follicle where they acquire additional mutations, causing follicular lymphoma. Most patients present with widespread lymphadenopathy, bone marrow infiltration and hepatosplenomegaly. Occasionally, this lymphoma presents in an extranodal fashion, the gastrointestinal tract and the skin being among the sites where this may occur. The clinical course alternates between stable periods when patients remain well, and periods of progressive disease requiring therapy. Therapy is required, however, in patients with systemic symptoms, critical organ failure or bulky disease. Furthermore, there is evidence that maintenance rituximab (given every 2 or 3 months over a period of 2 years) benefits patients who have achieved at least a partial response to either firstor second-line therapy by roughly doubling the time to progression. Frail, usually older patients can be treated with the single oral alkylating agent chlorambucil, with or without rituximab. Low-grade lymphomas are often extremely radio-sensitive and radiotherapy can be useful for treating localized or bulky disease. This lymphoma entity is more common in males and generally presents in older patients with a median age of 60 years. Patients with the disorder present with widespread lymphadenopathy, hepatosplenomegaly and bone marrow involvement and in some cases abnormal lymphocytes can be seen in the peripheral blood. Some series have reported a very high incidence of gastrointestinal involvement (80%). Systemic symptoms are unusual, most patients feeling reasonably well at the time of presentation. The disorder may be suspected on microscopy of the blood and bone marrow and diagnosis is assisted by immunophenotyping. Hairy cell leukaemia behaves in an indolent manner and responds well to treatment with single-agent drugs such as 2-chlorodeoxyadenosine (cladribine) or pentostatin. It typifies an aggressive but potentially curable lymphoma, and represents approximately one-third of all lymphomas. Histologically, the disorder is characterized by the presence of sheets of large cells of B-cell origin. The disorder probably includes a variety of different lymphoma types and in this sense is a catch-all category for those lymphomas that do not obviously fit into other definitions. Patients present with rapidly progressive disease, featuring night sweats, fever, weight loss and lymphadenopathy or with extranodal lymphoma involving sites such as the gastrointestinal tract, the testis, brain or bone. Treatment is with combination chemotherapy, which can induce remission in approximately 80% of cases, and as many as 60% of patients will attain a sustained remission beyond 3 years. Radiotherapy is often given to sites of bulky disease or residual masses after the completion of chemotherapy. Infection with malaria is thought to play an important part in the pathogenesis of this form of Burkitt lymphoma, probably by chronic antigen stimulation. The hairy cells have bean-shaped nuclei and abundant clear cytoplasm (appearing like a halo around the nucleus). The treatment is administered every 3 weeks for a total of six or eight courses on an outpatient basis. Relapsed patients can be offered high-dose chemotherapy and peripheral blood stem cell rescue 96 Cumulative proportion surviving Neoplastic disorders of lymphoid cells 1. Note that the survival difference is more pronounced for patients with low-risk disease. This type of lymphoma belongs to the group of marginal zone lymphomas, as the malignant cells are thought to derive from the marginal zone of the lymphoid follicle. Some, but by no means all, are associated with the presence of Helicobacter pylori. Eradication of the bacterium using combination antibiotic therapy often leads to eradication of the lymphoma. In those cases that cannot be treated successfully with antibiotics, gentle oral chemotherapy or involved field radiotherapy will usually control the disease. High-grade transformation may occur and is treated in the usual way with combination chemotherapy. Other common sites to be involved with this lymphoma include the thyroid gland, salivary glands, the lungs and the spleen. Mycosis fungoides and Sézary syndrome these disorders are T-cell cutaneous lymphomas. Mycosis fungoides is an indolent disorder characterized by plaques or nodules affecting the skin. The disorder may eventually become systemic, and when this happens the prognosis is very poor. Sézary syndrome is characterized by generalized erythroderma and circulating abnormal lymphoid cells with cerebriform nuclei (Sézary cells) in the peripheral blood. The differentiating cells of the malignant clone have the morphology of plasma cells or plasmacytoid lymphocytes, have clonally rearranged immunoglobulin genes (see Chapter 6) and usually secrete a monoclonal immunoglobulin (IgG or IgA), a monoclonal light chain, or both. Such monoclonal proteins are called paraproteins; they consist of structurally identical molecules and therefore produce a discrete monoclonal band (M band) on serum protein electrophoresis. Activation of osteoclasts by molecules secreted from stromal cells, and from the myeloma cells themselves, causes bone destruction that leads to multiple well-defined osteolytic lesions, and radiological changes resembling those of generalized osteoporosis and hypercalcaemia. Some patients with IgA paraproteins (which tend to dimerize) and a few patients with high levels of IgG3 paraproteins have a substantially raised plasma viscosity and may develop hyperviscosity syndrome. Light chains are filtered through the glomeruli and are found in the urine; they may damage the renal tubules. In 10% of patients, the abnormally folded paraprotein is converted into deposits of amyloid in various tissues. Levels of normal immunoglobulin are reduced and in advanced disease there is a reduction in circulating T cells. Clinical features the age-standardized incidence of myeloma is about 40 per million of the population per year. During ths phase, although a paraprotein is detectable on Haematology Lecture notes, Tenth Edition. As the disease advances and the bone marrow becomes infiltrated with malignant plasma cells secreting monoclonal immunoglobulin, a number of secondary changes may be found. Bone destruction the most common presenting symptom is bone pain, usually over the lumbar spine. Compression fractures of the vertebrae may damage the spinal cord or spinal roots and cause neurological symptoms. Renal failure Renal failure may be found at presentation or develop during the course of the disease. Chronic renal failure commonly results from the obstruction of distal renal tubules by proteinaceous casts, leading to tubular atrophy and interstitial fibrosis (myeloma kidney). Renal dysfunction may also result from the toxic effects of light chains on tubule cells, the deposition of light chains in glomeruli and amyloidosis. Acute renal failure may be precipitated by dehydration or use of analgesics, or be caused by hypercalcaemia or hyperuricaemia. Bacterial infections Respiratory tract infections are common in patients with myeloma. The lack of normal antibodies (acquired hypogammaglobulinaemia) results in infections caused by capsulated organisms, commonly Streptococcus pneumoniae and Haemophilus. Bone marrow failure Anaemia is common in myeloma and is usually normocytic or macrocytic. Hypercalcaemia Hypercalcaemia causes symptoms such as anorexia, vomiting, lethargy, stupor and coma. Amyloidosis Peripheral neuropathy, macroglossia, cardiomegaly, diarrhoea and carpal tunnel syndrome suggest amyloidosis. Peripheral neuropathy may also be caused by infiltration of nerves by plasma cells or by a direct toxic effect of the paraprotein. IgA myeloma is more likely to cause hyperviscosity, as IgA has a tendency to form dimers. The serum uric acid is raised in about half of cases (and may contribute to the renal damage). Some aspirates may show only a slight increase in plasma cells (510% of nucleated marrow cells, as compared with 0. The cells did not react with antibody against chains and were therefore monoclonal in origin. In 12% of patients with myeloma, a paraprotein cannot be detected in either serum or concentrated urine (non-secretory myeloma). This simple and cost-effective method uses the serum albumin and serum 2 -microglobulin levels to define three groups of differing outcome with treatment. Patients whose malignant plasma cells harbour certain abnormalities such as t(4;14) or del 17p13 are at much higher risk of progression and have shorter overall survival. Diagnosis this is often based on the finding of at least two of the following three features: be determined by immunofixation. In 50% of patients with myeloma, the paraprotein is IgG, in 25% it is IgA, in 20% it is light chain only, and in 12% it is IgD or IgE. Over half of patients with an IgG- or IgA-secreting myeloma have monoclonal light chains in their urine; in two-thirds of these patients the light chain is 1 A monoclonal Ig in the serum or monoclonal light chains in the urine or both. Of note, however, is the differentiation between myeloma proper and indolent or smouldering myeloma. The latter satisfies the diagnostic criteria Plasma cell myeloma and other paraproteinaemias 101 for myeloma, but is not associated with evidence of significant end-organ damage. At present, there is no indication for the treatment of patients with indolent or smouldering myeloma. Treatment Treatment should be reserved for patients in whom there is evidence of organ damage, for instance anaemia, extensive lytic or other significant bone lesions or renal dysfunction. Treatment requires a multidisciplinary approach involving haematologists, radiation oncologists and specialist nurses. Anaemia is a common finding at presentation or progression, or may be secondary to treatment. Patients who require frequent transfusion may benefit from subcutaneous erythropoietin. Adequate hydration and a good urine flow must be maintained in an attempt to reduce the risk of paraprotein precipitation in the renal tubules and consequent renal damage; haemodialysis may be required in the event of renal failure. Patients with high paraprotein levels may also develop hyperviscosity syndrome and plasma exchange can be used to reduce rapidly the effect of this problem. Bacterial infections, caused by the associated acquired hypogammaglobulinaemia, require prompt treatment with antibiotics. Bone pain and fractures and hypercalcaemia cause significant morbidity and mortality in patients with myeloma, and long-term therapy with bisphosphonates has been shown to reduce bone pain and progression of skeletal lesions. Stratification of patients according to their outcome risk (see above) and their eligibility for high dose therapy (based on age, performance status, etc. For those patients who are transplant eligible, initial treatment begins with combination induction chemotherapy usually incorporating a proteasome inhibitor such as bortezomib (Velcade) together with an immunomodulatory drug such as thalidomide or lenalidomide (Revlimid). Thus, the so-called triplet regimen of bortezomib, lenalidomide and low-dose dexamethasone is favoured by some centres as induction therapy. The treatment is consolidated in responding patients with autologous bone marrow transplantation. Many other regimens (doublets and triplets) are used which variously incorporate an immunomodulatory drug, a proteasome inhibitor or an alkylating agent such as cyclophosphamide. Whichever combination of drugs is selected, they are almost always given in combination with dexamethasone. Patients unable to receive high-dose therapy because of co-morbidities are usually treated with similar induction regimens such as the doublet lenolidamide and dexamethasone (Rd) or other drug combinations incorporating those agents cited. The duration of remission may be long (>3 years), particularly in those patients fit enough to receive high-dose therapy. Over 90% of patients will relapse, however, and require retreatment, usually using a combination of drugs not used in the first-line therapy. Patients who achieve long remissions after autologous transplantation may be offered a second transplant. Many of the agents are myelosuppressive so careful monitoring of blood counts is required. Both bortezomib and the immunomodulatory drugs can cause significant peripheral neuropathy. Spinal cord compression caused by a vertebral or a paravertebral mass requires urgent assessment, and decompression laminectomy followed by radiotherapy is usually the treatment of choice. Bone fractures, which are a common complication, are best treated by orthopaedic fixation followed by radiotherapy. Chemotherapy Cytotoxic drugs are reserved for patients with bone lesions, hypercalcaemia, bone marrow failure or renal dysfunction.
These products have not shown superior diabetes signs feet order 50 mg acarbose visa, clinically significant outcome in hospitalized patients in randomized controlled trials managing diabetes 3 ps acarbose 25 mg purchase amex. The level of glycemic control associated with enhanced outcome is best achieved with insulin oral diabetes medications heart failure 50 mg acarbose order mastercard, as opposed to carbohydrate restriction diabetes mellitus type 2 abbreviation discount 50 mg acarbose free shipping. Furthermore diabetes diet bangla buy acarbose 50 mg low price, gastric feedings with high fat formulas in the diabetic patient with gastroparesis may delay gastric emptying and increase risk of aspiration. Surgical complications of enteral access include leaks, tube dislodgement, volvulus, soft tissue infection, and bowel necrosis. Should one delay nutrition support longer in obese patients assuming they have increased reserves Obese patients have more fat, but during stress all patients become hypermetabolic and break down endogenous protein stores to mobilize amino acids for gluconeogenesis, protein production, and adenosine triphosphate. As with patients who are of normal weight, patients who are obese require high protein nutritional supplementation to meet increased nitrogen demands. Dilution delays the attainment of feeding goals and increases the likelihood of bacterial contamination. With moderate to severe diarrhea, consider feeding reduction, antidiarrheal agents, and stool studies for clostridium difficile. Evaluate the medication profile for sorbitol-containing elixirs, laxatives, stool softeners, and prokinetic agents. Some success has been reported with soluble fiber or lactobacillus probiotics (yogurt) in antibiotic-associated diarrhea. Most 1 kcal/mL formulas (standard) contain 85% water by volume, whereas 2 kcal/mL formulas contain 70% water. For example, if the total calculated need for fluid is 2400 mL for a 60-kg patient and 2400 cc of the tube feeding provides approximately 2000 mL of free water, write an order to give 200 mL of water to the patient twice daily. Continuous infusion is best in the patient who is critically ill requiring postpyloric feedings. Cyclic feedings or nocturnal feedings are useful for the patient who is on concurrent oral intake and in transition to full oral support, or for those requiring feeding-free periods for physical therapy or activities of daily living. Substrates delivered enterally are better tolerated, are associated with fewer metabolic and hepatic complications, and help preserve normal mucosal integrity. Should you discontinue enteral feeding at midnight on all patients undergoing elective surgery with general anesthesia The American Society of Anesthesiologists recommends that healthy adults cease intake of solids for at least 6 hours and liquids for 2 hours before undergoing elective procedures. Should actual, ideal, or adjusted body weight be used in nutrition calculations for the patient with obesity Clinical studies show therapeutic or preventive use of varied probiotic strains for antibiotic-associated diarrhea, rotavirus-associated diarrhea and pouchitis. Results are promising for irritable bowel syndrome, ulcerative colitis, and side-effect reduction in antibiotic therapy for helicobacter pylori. Ultimately, maintaining positive nitrogen balance may be more important than achieving positive kilocalorie balance. Early enteral feeding, with its known benefits, may not easily occur through a gastric feeding in the early stages of injury. Postpyloric feedings deliver more kilocalories, more timely return to anabolism, and promote a lower rate of infectious complications than continuous gastric feeding. There is controversy that administering arginine in patients with sepsis, who have upregulated expression of inducible nitrous oxide synthase (iNos), will result in excessive nitrous oxide production and resultant exaggerated vasodilation and oxidant stress. Should formula with increased fish-oil formula be used in patients who are going into acute respiratory distress syndrome A randomized controlled trial comparing standard, moderate-fat polymeric formula and a high omega-3 formula is needed. Parenteral nutrition is the provision of protein as amino acids (4 kcal/g), dextrose (3. If a multiple-port catheter is used, a "virgin port" should be reserved exclusively for nutrient infusion. When prolonged parenteral nutrition infusion is necessary in the postacute setting, consider a long-term access device such as a Hickman or Broviac catheter. This may not be necessary, however, when the central venous catheter is placed under sterile conditions and the patient and caretakers deliver meticulous care. If enteral nutrition is not tolerated, parenteral nutrition should be considered no sooner than 7 days into the hospitalization. In extremely rare instances of pancreatitis caused by congenital hyperlipidemia, lipids should be withheld. Patients who are fed parenterally may develop hyperglycemia as a result of increased stress and the inflammatory response, limited mobility, concurrent steroid therapy, and excessive kilocalorie intake. Evaluate information on the home glucose control regimen from the medication history. A continuous insulin infusion is often necessary during critical illness to achieve adequate glycemic control. Theoretically, fat emulsions are employed to prevent essential fatty acid deficiency. In reality, this condition is rare, takes several weeks to develop, and requires only 3%4% of kilocalories as linoleic acid (or 10% of kilocalories as a standard fat emulsion). Fat emulsions are also used to provide additional kilocalories once glucose delivery exceeds 5 kcal/kg per minute. When delivered in total-nutrientadmixtures (3-in-1 solutions) lipid emulsions are stable for 24 hours. When infused as a sole nutrient, limit hang times to <12 hours to prevent bacterial growth. Avoid fat emulsions with hyperlipidemiainduced pancreatitis and when serum triglycerides are significantly elevated. Refeeding syndrome occurs when a patient is moderately to severely malnourished and has limited substrate reserves, usually as a result of chronic alcoholism, anorexia nervosa, postbariatric surgery, or chronic starvation. When presented with a large nutrient load, the patient rapidly develops a clinically significant decline in serum K, phosphorus (P), Ca, and Mg because of compartment shifts or increased utilization of these ions. Hyperglycemia is common as a result of blunted basal insulin secretion (see Kraft). Provide ample quantities of K, P, Ca, and Mg with the initial parenteral mixture, within the solubility limits of the solution. Reduce the initial kilocalorie load by 25% of goal by limiting dextrose kilocalories. Monitor blood glucose four times daily, and serum K, P, Ca, and Mg daily for 5 days after initiating feeding, while advancing kilocalories to goal levels. With acceptable fluid and electrolyte balance, reduce frequency to one to two times weekly. The adequacy of the nutrition regimen may be assessed by evidence of proper wound healing, maintenance of hydration status, preservation of body cell mass, and a timely repletion of constitutive protein levels. In more ambulatory patients, and those on home therapy, a cyclic or nighttime infusion schedule (12- to 18-hour cycle) increases patient freedom. Many third-party payers do not provide more reimbursement for parenteral therapy than enteral in the hospital setting. Current lipid formulations available in the United States are made from either soybean oil or a mixture of soybean and safflower oil; thus, they are predominately polyunsaturated (omega-6) fat. Glucose kilocalories are the most cost-effective kilocalories, followed by standard amino acid kilocalories, then lipid calories. Lipid infusions exceeding 1 g/kg of body weight are associated with decreased immunocompetence and impaired oxygenation in patients who are critically ill. Glutamine, the amino acid found in greatest concentration in muscle and plasma, decreases after surgery, injury, or stress. It plays a role as a metabolic substrate for rapidly replicating cells, maintains the integrity and function of the intestinal barrier, and protects the enterocyte from free radical damage. Glutamine is not included in standard amino acid solutions because of limited solubility and stability. Enteral supplementation may reduce infectious complication rates and decrease hospital stay in surgical patients. Parenteral glutamine should be used cautiously or not at all in the critically ill patients. Should recombinant growth hormone, glutamine, and a modified diet be used routinely to maximize gut adaptation after intestinal resection Until further research occurs, this expensive therapy should not be routine, and intensive nutrition and pharmacologic management should remain the mainstay of care. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. Prediction of resting metabolic rate in critically ill adult patients: results of a systematic review of the evidence. Effect of enteral feeding with eicosapentaenoic acid, gamma-linoleic acid, and antioxidants in patients with acute respiratory distress syndrome. Urinary urea nitrogen: too sensitive for calculating nitrogen balance studies in surgical clinical nutrition. Glutamine supplementation in serious illness: a systematic review of the evidence. Effects of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically ventilated patients with severe sepsis and septic shock. Arginine infusion in patients with septic shock increases nitric oxide production without haemodynamic instability. Reduced citrulline production in sepsis is related to diminished de novo arginine and nitric oxide production. Because humans hibernate a little at night, we are cool (36°C) just before rising in the morning; after revving our engines all day, we are hot at night (38°C). A rare, life-threatening response to inhaled anesthetics or some muscle relaxants. Abnormal calcium metabolism in skeletal muscle produces heat, acidosis, hypokalemia, muscle rigidity, coagulopathy, and circulatory collapse. Rare, familial (autosomal dominant with variable penetrance), catastrophic response to inhaled anesthetics or muscle relaxants 2. Clinical manifestations: Core temperature >40°C, trismus, hypercapnia, tachycardia, tachypnea, hypertension, cardiac dysrhythmias, metabolic acidosis, hypoxemia, myoglobinuria, or coagulopathy 4. Management: Halt anesthetic; administer dantrolene over 48 hours, supplemental sodium bicarbonate; actively cool patient 4. Aspirin, acetaminophen, and ibuprofen are cyclooxygenase inhibitors that block the formation of prostaglandin E2 in the hypothalamus and effectively control fever. Patients are more comfortable, however, and the surgeon receives fewer calls from the nurses. A transplant patient with a temperature of 38°C requires scrutiny, whereas a healthy medical student with an identical temperature of 38°C 24 hours after an appendectomy can be ignored. Order blood cultures, urine Gram stain and culture, and sputum Gram stain and culture. Look at old and current intravenous sites for evidence of septic thrombophlebitis. What is the most common cause of fever during the early postoperative period (13 days) Why does a little atelectasis cause fever, whereas a lot of atelectasis (pneumothorax) does not The most likely explanation is that sterile atelectasis (and early postoperative lung collapse typically is not infected) has nothing to do with fever. Vital capacity was measured in a large group of patients 24 hours after various surgical procedures. An upper abdominal incision was the worst, followed by lower abdominal incision, then (counterintuitively) thoracotomy, median sternotomy, and extremity incision. Each milliliter of human saliva contains 108 aerobic and anaerobic, gram-positive and gram-negative bacteria. The incision must be examined in a patient with a fever (39°C) <12 hours after surgery. Look for a foul-smelling, serous discharge in a particularly painful wound (all incisions hurt) with or without crepitus. Gram stain of the serous discharge for gram-positive rods confirms or excludes the diagnosis of clostridial infection. The mainstay of therapy is aggressive surgical debridement of necrotic tissue (skin, muscle, and fascia). Hemolytic streptococcal gangrene, idiopathic scrotal gangrene, and gram-negative synergistic necrotizing cellulitis are distinct entities but have been lumped into the single category of necrotizing fasciitis. A shotgun approach to potentially life-threatening infections when the patient is seriously ill and the surgeon is seriously concerned: a. Clostridial infection involves underlying muscle resulting in myonecrosis or gas gangrene. Nonclostridial infection involves subcutaneous fascia (also known as necrotizing fasciitis). Similar management: Fluid and electrolyte resuscitation, antibiotics (high-dose penicillin for clostridial infection, broad-spectrum triples for necrotizing fasciitis), and aggressive surgical debridement of necrotic tissue. Urologic instrumentation at the time of surgery may accelerate the process considerably. Germs crawl up the outside of the urethral catheter, and by 57 days after surgery, most patients harbor infected urine. Septic thrombophlebitis (from an intravenous line) and occult (usually intraabdominal) abscesses tend to present about 2 weeks after surgery.
Purchase 50 mg acarbose mastercard. Sleep Disturbances Obesity and Type 2 Diabetes: Interacting Epidemics.
Unfortunately the patient suffered progressive mental status decline despite aggressive management of intracranial pressure and maximal doses of antifungals juvenile diabetes in dogs symptoms acarbose 50 mg with visa. He experienced slow diabetes insipidus merck effective acarbose 25 mg, progressive decline diabetic bread buy cheap acarbose 25 mg online, leading to death 13 days after initiation of antifungal therapy diabetes definition gcse safe 25 mg acarbose. The patient in this case was highly immunocompromised and presented with cellulitis and headache diabetes virus purchase generic acarbose on-line. Given the high mortality associated with cryptococcal infection, rapid and accurate diagnosis is important. Unfortunately, despite these efforts and the use of aggressive therapy, many such patients succumb to infection. A large number of species has been described, but the number of species associated with human disease is relatively limited, with A. Aspergilli are environment fungi whose spores are inhaled, producing a wide range of diseases including allergic hypersensitivity reactions, primary pulmonary disease, or highly aggressive disseminated disease. A preliminary diagnosis of infection is made by observation of the fungus in tissue (typical appearance is branching, septate [divided into compartments], nonpigmented [hyaline] hyphae) and confirmed by growth of the mold in 2 to 5 days in culture. Identification of the individual species is by the morphologic appearance of the mold growing in culture (color of the colonies, arrangement of spores on the fruiting structures attached to the hyphae). The patient was a 34-year-old woman who presented with 2-day history of weakness, dizziness, left calf pain, and black tarry stools. Her past medical history was significant for diabetes leading to renal failure, for which she received a cadaveric renal transplant in 2002. She was placed on an immunosuppressive regimen of alemtuzumab, tacrolimus, sirolimus, and prednisone. Physical examination revealed a tender venous cord palpable in the popliteal fossa. The patient was given four units of packed red blood cells, and empirical treatment with gatifloxacin. On hospital day 6, vesicular rash developed on the buttocks and left calf, cultures of which were positive for herpes simplex virus, and she was placed on acyclovir. On hospital day 12, the patient exhibited decreased responsiveness, became obtunded, and was intubated for respiratory distress. Culture of bronchoalveolar lavage fluid was positive for Aspergillus species, and viral inclusion bodies suggestive of cytomegalovirus were seen. Multiple acute infarcts in the frontal lobe and cerebellum were seen on a magnetic resonance imaging scan of the brain. This case serves as an extreme example of disseminated aspergillosis in an immunocompromised host. He was placed on broad-spectrum antibacterial agents but remained febrile for 96 hours. To combat a potential fungal infection, voriconazole was added to the therapeutic regimen. After 1 week of treatment, the patient was still febrile and neutropenic, and his antifungal therapy was changed to caspofungin. Initially the rash developed on the upper extremities and consisted of papular, erythematous, plaquelike lesions with centers that became necrotic. Blood cultures and skin biopsy specimens were sent to the laboratory for analysis. The laboratory report indicated that the blood cultures were positive for "yeast", based on the presence of budding cells and pseudohyphae. Despite the antifungal therapy, the lesions increased in number over the next 2 weeks and spread throughout the extremities, trunk, and face. The neutropenia and fever persisted, and he died approximately 3 weeks after the initial diagnosis. The combination of skin lesions and positive blood cultures are typical findings in fusariosis. Although "yeast" was reported from the blood cultures, closer examination revealed the microconidia and hyphae of Fusarium. Likewise, the appearance of septate hyphae in the skin biopsy could represent a number of different hyaline molds, including Fusarium. All parasites are classified as eukaryotic, some are unicellular and others are multicellular, some are as small as 4 to 5 m in diameter and others are up to 10 meters in length, and some are amorphous with minimal features whereas others have characteristic structures, such as a head, body, and legs. The epidemiology of these diseases is equally challenging, with some parasites spread from person to person while others require a complex series of hosts for development into infectious forms. The difficulties confronting students are not only an understanding of the spectrum of diseases caused by parasites but also an appreciation of the epidemiology of these infections, which is vital for developing a differential diagnosis and an approach to the control and prevention of parasitic infections. With literally hundreds of parasites associated with human disease, the student needs some help in organizing the most relevant information. In this article and subsequent ones, I will concentrate on only the most common parasites associated with human disease, recognizing that avirulent parasites, particularly those classified in the kingdom Protozoa, can colonize humans and create confusion when detected in clinical specimens. In this chapter, I first provide a classification structure for the parasites and then a view of the parasites from the perspective of the diseases they cause. I also provide an overview of the antiparasitic agents that can be used to treat these infections. In the subsequent chapters, I provide a more detailed view of the biology, epidemiology, clinical disease, diagnosis, and treatment of these organisms. The last kingdom, Animalia, includes all eukaryotic organisms that are not Protozoa, Stramenopila, or Fungi. Enterobius vermicularis Trichuris trichiura Ascaris lumbricoides Strongyloides stercoralis Necator americanus Ancylostoma duodenale Brugia malayi Wuchereria bancrofti Loa loa Onchocerca volvulus Trichinella spiralis Toxocara canis Ancylostoma braziliense Trematodes (flatworms) Fasciolopsis buski Fasciola hepatica Opisthorchis sinensis (also known as Clonorchis sinensis) Paragonimus westermani Schistosoma spp. The goal of this section and subsequent chapters is to give the physician the tools to develop this differential diagnosis. Because both parasites and humans are eukaryotic, many antiparasitic agents also act on human metabolic pathways; that is, these agents can pose a risk of toxicity. Differential toxicity is achieved by preferential uptake, metabolic alteration of the drug by the parasite, or differences in susceptibility between host and parasite. The following is a summary of the major antiparasitic agents and clinical indications. Clinical Indications Trypanosomiasis, leishmaniasis Malaria prophylaxis and therapy pathways that are unique for the rapidly proliferating parasites. In contrast, agents used for treatment of the helminth infections target unique metabolic pathways in the nonproliferating adult worms. Because the student may not be familiar with the antiparasitic Drug Class Antiprotozoal Agents Heavy metals Examples Melarsoprol, sodium stibogluconate, meglumine antimoniate Aminoquinoline analogs Chloroquine, mefloquine, quinine, primaquine, halofantrine, lumefantrine Folic acid antagonists Sulfonamides, pyrimethamine, trimethoprim Inhibitors of protein synthesis Clindamycin, spiramycin, paromomycin, tetracycline, doxycycline Diamidines Pentamidine Nitromidazoles Metronidazole, benznidazole, tinidazole Nitrofurans Phosphocholine analog Sulfated naphthylamine Thiazolides Antihelminth Agents Benzimidazoles Tetrahydropyrimidine Piperazine Avermectins Prazinoisoquinoline Phenol Quinolone Organophosphate Sulfated naphthylamidine Nifurtimox Miltefosine Suramin Nitazoxanide Mebendazole, thiabendazole, albendazole Pyrantel pamoate Piperazine, diethylcarbamazine Ivermectin Praziquantel Niclosamide Bithionol, oxamniquine Metrifonate Suramin Toxoplasmosis, malaria, cyclosporiasis Malaria, babesiosis, amebiasis, cryptosporidiosis, leishmaniasis Leishmaniasis, trypanosomiasis Amebiasis, giardiasis, trichomoniasis, trypanosomiasis Trypanosomiasis Leishmaniasis Trypanosomiasis Cryptosporidiosis, giardiasis Broad-spectrum antihelminthic for nematodes and cestodes Ascariasis, pinworm, hookworm Ascaris and pinworm infections Filarial infections, strongyloidiasis, ascariasis, scabies Broad-spectrum antihelminthic for cestodes and trematodes Infesting tapeworm Paragonimiasis, schistosomiasis Schistosomiasis Onchocerciasis the following table is a list of primary and secondary treatments for the most common parasites. Cystoisospora belli Cyclospora cayetanensis Giardia duodenalis note that for many of the groups of parasites, the same antiparasitic agents are used for treatment. Primary Antiparasitic Agents Metronidazole Miltefosine Miltefosine; amphotericin B Chloroquine; refer to current Centers for Disease Control and Prevention recommendations Clindamycin + quinine; atovaquone + azithromycin Pyrimethamine + sulfadiazine Sodium stibogluconate; meglumine anti- Pentamidine; amphotericin B monite; miltefosine Suramin; pentamidine; malarsoprol (for central nervous system disease) Benznidazole; nifurtimox Albendazole Mebendazole Albendazole; mebendazole; pyrantel pamoate Albendazole; mebendazole; pyrantel pamoate Ivermectin Albendazole; mebendazole Diethylcarbamazine Diethylcarbamazine Diethylcarbamazine Ivermectin Mebendazole (adult worms only) Praziquantel Triclabendazole Praziquantel Praziquantel Praziquantel Praziquantel Praziquantel Niclosamide Bithionol Albendazole Triclabendazole Oxamniquine Mebendazole; pyrantel pamoate Albendazole; pyrantel pamoate Secondary Antiparasitic Agents 157 Babesia microti Toxoplasma gondii Leishmania spp. Classification of protozoa is complex but the easiest way to organize these parasites Group Intestinal amoeba Coccidia Parasite Entamoeba histolytica Cyclospora cayetanensis Cryptosporidium spp. Reservoir Humans Humans Humans Humans Humans, beavers, muskrats Humans Environment Environment Humans Rodents Cat Rodents, dogs Domestic animals, humans, cattle, sheep, wild game Wild animals Vector - - - - - - Flagellates Free-living amoeba Blood and Tissue Protozoa Mosquito Tick - Sandfly Tsetse fly Reduviid bug the protozoa listed in this chapter are certainly not a comprehensive list of all protozoa or even all protozoa associated with human disease; however, the most important species are included in this chapter. Although not common in the United States, infections can be acquired when traveling to countries with poor hygienic standards. The patient initially presented with intermittent fever followed by right upper quadrant pain and diarrhea. On admission to the hospital, he was afebrile with an elevated white blood cell count and abnormal liver function tests. He underwent colonoscopy, and multiple discrete ulcers were detected in the rectum and colon. The diagnosis of amebic colitis was confirmed by the demonstration of numerous trophozoites on histopathologic examination of colon biopsy specimens. Ultrasound examination of the abdomen revealed a large heterogeneous mass within the liver, consistent with an abscess. Percutaneous drainage of the abscess obtained chocolate-like pus, and examination of a biopsy from the margin of the abscess revealed only a necrotic material, without evidence of amebae. The patient was treated with metronidazole followed by iodoquinol to eradicate the luminal amebae. Subsequent history revealed he traveled to Thailand 2 months before the onset of the present illness. The patient improved rapidly on antiamebic therapy and was discharged on antiretroviral therapy. Cyclospora infections in the United States are typically associated with food-related outbreaks such as with raw fruits or vegetables shipped from countries with poor hygienic conditions. Cryptosporidium in particular is associated with large outbreaks when drinking water or recreational waters are contaminated. Many species of Cryptosporidium infect a variety of animals, but Cryptosporidium hominis and Cryptosporidium parvum are most commonly associated with human infections. Epidemiology · Worldwide distribution · Infection most commonly associated with contaminated water or fecal-oral, oral-anal transmission · Small (46 m), spherical, infectious oocysts containing sporozoites are excreted in feces · Ingested sporozoites attach to brush border of epithelial cells lining the small intestine where they establish disease · Well-documented outbreaks associated with contaminated water such as in reservoirs or recreational water parks and pools · Asymptomatic carriage · Symptomatic disease similar to disease with Cyclospora · Enterocolitis characterized by watery diarrhea with remission after 10 days in immunocompetent patients · More severe enterocolitis in immunocompromised patients. In the fall of 1998 an outbreak of gastroenteritis among university students was reported to the Department of Health. Preliminary findings suggested that the illness was associated with eating at one of the campus cafeterias; four employees of this cafeteria had a similar illness. In a case control study of 88 case patients and 67 control patients, eating in 1 or 2 cafeterias was associated with diarrheal illness. One ill food handler with laboratory-confirmed cryptosporidiosis 163 prepared raw produce on the days surrounding the outbreak. This outbreak illustrates the potential for cryptosporidiosis to cause food-borne illness. Epidemiologic and molecular evidence indicate that an ill food handler was the likely outbreak source. Wild animals are an important reservoir for this parasite and their feces can contaminate many streams and lakes as well as drinking water such as from wells. The patient was unsuccessfully treated five times with metronidazole and albendazole without improvement of diarrhea or cyst shedding. Although combined antiretroviral therapy was also administered, it was ineffective, and viral genotypic analysis found mutations associated with high resistance to most antiretroviral drugs. The patient was subsequently treated for giardiasis with nitazoxanide, which resulted in resolution of the diarrhea and negative results of tests for stool cyst shedding. Nitazoxanide may be considered as a useful alternative therapy for resistant giardiasis. However, carriage of this organism increases the risk of infection and transmission of other sexually transmitted diseases and places pregnant women at increased risk of premature delivery. Epidemiology human pathogens capable of causing overwhelming and rapidly fatal disease, but fortunately are relatively uncommon. Epidemiology · Worldwide distribution · Common in soil and freshwater lakes and rivers; in tap water and bottle water; can contaminate dialysis fluids and contact lens cleaners · Infections of the eye most commonly associated with improperly cleaned contact lenses used by patients with mild preexisting trauma to the cornea. In contrast with the protozoa discussed previously, all the blood and tissue protozoa require important vectors for transmission of disease: the Anopheles mosquito for malaria (Plas modium) and the tick for babesiosis (Babesia). Five species of Plasmodium are responsible for malaria in humans: Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium knowlesi, with the first two species the most common. In 2013 the World Health Organization estimated that there were almost 200 million cases of malaria and 500,000 deaths, primarily children in Africa. Approximately 1500 cases of malaria occur in the United States each year, mainly in travelers and immigrants from endemic areas, although transmission in the United States is well documented. A B Giemsa stain of peripheral blood with infection with (A) Plasmodium falciparum and (B) Babesia microti. The patent was a 59-year-old man who presented with a 1-day history of high-grade fever after recently returning from Guyana in South America. He noted that his symptoms were similar to those of a malaria infection 5 years previously, also acquired in Guyana. A peripheral blood smear as a part of the initial workup showed numerous red blood cells with schizonts consistent with Plasmodium infection, with more than 5% parasitemia. The patient was started on quinine and doxycycline oral therapy because of the concerns regarding chloroquine-resistant malaria. During the next 4 days the patient developed more severe thrombocytopenia and nonoliguric renal failure, acute respiratory failure, and circulatory failure, despite a decrease in parasitemia to less than 0. The patient gradually improved and was treated with primaquine to prevent relapse. This case shows that although it is unusual, severe respiratory and circulatory compromise may complicate P. This case also emphasizes the importance of chemoprophylaxis and personal protective measures for anyone planning a trip to a malariainfested region. Many species of Babesia cause human disease worldwide, but the focus in this chapter is the most common species in the United States responsible for disease, with almost 2000 cases reported annually. Shortly afterward she became febrile and neutropenic, and treatment with broad-spectrum antibiotics was started. After resolution of neutropenia (1 month posttransplantation), confusion and lethargy developed. Imaging studies of the brain revealed microinfarcts in both hemispheres and the midbrain. When toxic epidermal necrolysis developed, the sulfadiazine was discontinued and clindamycin was begun. Histopathologic findings and immunohistochemical staining confirmed a diagnosis of disseminated toxoplasmosis. Disseminated toxoplasmosis is rare, especially after autologous stem-cell transplantation. The likely cause of reactivation and dissemination of Toxoplasma in this patient was the cell-mediated immunosuppression associated with Hodgkin disease and its treatment. In addition to the brain, the heart, liver, and lungs are frequently involved in cases of disseminated toxoplasmosis.

Others include contraction and deformity of the chest wall blood glucose for non diabetics 50 mg acarbose purchase overnight delivery, spontaneous drainage through the chest wall (empyema necessities) diabetes health magazine generic 25 mg acarbose otc, bronchopleural fistula diabetes symptoms young adults buy acarbose once a day, osteomyelitis diabetes x syndrome buy 50 mg acarbose free shipping, pericarditis blood glucose 200 level acarbose 25 mg buy overnight delivery, mediastinal or subphrenic abscess, sepsis, and death. None of these outcomes is particularly appealing, so in the absence of overwhelming contraindications, all empyemas warrant therapy. A lung abscess is a localized site of infection located within the lung tissue with associated tissue necrosis. There are many potential lung infections that can produce lung abscesses, but anaerobic infections remain the most frequent types of pathogens. Unlike abscesses in other areas of the body, most lung abscesses do not require drainage and can be treated with systemic antibiotic therapy. A chest radiograph typically shows upper lobe infiltrates, with or without cavitation, and can be misdiagnosed as a neoplastic process. Positive acid-fast bacilli ("red snappers") smear in sputum sample; sensitivity improves with bronchoalveolar lavage specimens. Initial therapy consists of a 6-month regimen with isoniazid, rifampin, and pyrazinamide for the first 2 months and then isoniazid and rifampin for another 4 months. This lung tissue is resistant to drug penetration and can "spill" organisms into healthy lung tissue. Surgery is indicated for localized disease, and in combination with drug therapy, it results in sputum conversion in 95% of patients with relapse rates of <5%. The three stages of empyema are the exudative stage (low viscosity fluid), fibrinopurulent stage (transitional phase with heavy fibrinous deposits and turbid fluid), and organizing stage (capillary ingrowth with lung trapping by collagen). Medical and surgical treatment of parapneumonic effusions: an evidence-based guideline. Traditionally, lung cancer has been stratified histologically as squamous/epidermoid, adenocarcinoma, and small/large cell lung cancers. Our current ability to profile cancers at the molecular level appears to have both prognostic and therapeutic value. The most important distinction is between small cell and nonsmall cell carcinoma because of fundamental differences in tumor biology and clinical behavior (Table 83. Patients with small cell lung cancer are classified as having either limited or extensive disease. Limited means that all known disease is confined to one hemithorax and regional lymph nodes, including mediastinal, contralateral hilar, and ipsilateral supraclavicular nodes. Extensive describes disease beyond these limits, including brain, bone marrow, and intraabdominal metastases. With small cell or neuroendocrine carcinoma, the small cell type is usually extensive at presentation, and 5-year survival is 5%. Neuroendocrine carcinoma, which is well differentiated, is known as atypical carcinoid and has a good prognosis but is not benign. A family history of lung cancer probably increases the risk of getting lung cancer. Furthermore, a large array of important biomarkers that influence prognosis have been identified in lung cancer cells and lung cancer tissue. The thinking is as follows: Lung cancer accounts for more cancer deaths than other cancers. Of interest, the presence of a paraneoplastic syndrome does not influence the ultimate curability of the lung cancer. Does the staging system for lung cancer have prognostic and therapeutic importance Pulmonary · Spirometry: Ventilation/perfusion screening; if borderline, must leave patient with approximately 800 mL forced expiratory volume after resection · Arterial blood gas analysis ii. Cardiac · Electrocardiogram · History of myocardial infarction, prior intervention iii. Cardiopulmonary · Able to walk a flight of stairs; if yes, will tolerate lobectomy · Maximal oxygen consumption <15 mL/kg per minute 11. Unfortunately, 75% of patients present with advanced disease and are not candidates for resection. Even lower-stage disease or tumors at high risk of recurrence may benefit from newer chemotherapeutic regimens. Radiation therapy is effective palliative, but not curative, therapy for lung cancer. Some-but not all-clinical trials have shown some benefit from preoperative chemoradiation treatment in advanced-stage lung cancer. What is the survival rate of patients treated for non-small cell lung cancer at 5 years Also, if stage Ia (small tumor, no positive nodes) cancer is not resected, survival decreases from 70% to 7%. Mediastinoscopy is a staging procedure in which the paratracheal, subcarinal, and proximal peribronchial lymph nodes are sampled from a small incision made in the suprasternal notch. Is malignant pleural effusion or recurrent nerve involvement with tumor an absolute contraindication to surgical resection for lung cancer Rarely, a small malignant pleural effusion will occur in the presence of a pleurally based but resectable primary tumor. Conversely, both King George V and Arthur Godfrey had successful surgical resections in the face of recurrent nerve involvement with tumor. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell carcinoma. Multiple other screening trials have not proven to be so optimistic; lung screening remains controversial. The most common causes of a pulmonary nodule are either neoplastic (carcinoma, 60%70% of resected nodules) or infectious (granuloma). Pulmonary nodules may also represent lung abscess, pulmonary infarction, arteriovenous malformations, resolving pneumonia, pulmonary sequestration, and hamartoma. Thus, whereas lung cancer is rare (although it does occur) in 30-year-old individuals, in 50-year-old smokers the chance that a solitary pulmonary nodule represents malignancy is 50%60%. Typically, a solitary nodule presents incidentally as a finding on routine chest radiograph. In several large series, more than 75% of lesions were surprise findings on routine chest radiograph. Accordingly, an extensive workup for a primary site of cancer other than the lung is not indicated. Calcification in the nodule generally is associated with benign disease (the opposite of breast cancer). Specifically, whereas central, diffuse, or laminated calcifications are typical of a granuloma, calcifications with more dense and irregular "popcorn" patterns are associated with hamartomas. Unfortunately, eccentric foci of calcium or small flecks of calcium may be found in malignant lesions. This is called Hounsfield attenuation and improves the accuracy of predicting the presence of malignancy. What social or clinical findings suggest that a nodule is malignant rather than benign Unfortunately, none of these findings is sufficiently sensitive or specific to influence the workup. Both increasing age and a long smoking history predispose patients to lung cancer. Thus, the fact that the patient is the president of the spelunking club (histoplasmosis), has a sister who raises pigeons (cryptococcosis), grew up in the Ohio River Valley (histoplasmosis), works as sexton for a dog cemetery (blastomycosis), or just took a hiking trip through the San Joaquin Valley (coccidioidomycosis) is interesting associated history but does not affect the workup of a solitary pulmonary nodule. If the nodule is new, it is more likely to be malignant, whereas if the nodule has not changed in the past 2 years, it is less likely to be malignant. If a patient presents with a treated prior malignancy and a new solitary pulmonary nodule, is it safe to assume that the new nodule represents metastatic disease Even in patients with known prior malignancies, <50% of new pulmonary nodules are metastatic. Thus, the workup should proceed exactly as for any other patient with a new solitary pulmonary nodule. A complete travel and occupational history is interesting but does not affect the evaluation. Because of the peripheral location of most nodules, bronchoscopy has a diagnostic yield of <50%. As indicated previously, percutaneous needle biopsy has a diagnostic yield of approximately 80% but rarely alters the subsequent management. The mainstay of management in patients who can tolerate surgery is resection of the nodule, usually by minimally invasive thoracoscopic lobectomy if cancer is suspected. Although several series have suggested that wedge excision of the nodule is sufficient, an anatomic lobectomy remains the procedure of choice for a known cancer of the lung. A solitary node that turns out to be metastatic cancer should be wedged out with likely benefit. Unfortunately, the recurrence rate even for stage I tumors or a small nodule is 30% over 5 years. A solitary pulmonary nodule or coin lesion is <3 cm and is discrete on chest radiograph. Meta-analysis of positron emission tomographic and computed tomographic imaging in detecting mediastinal lymph node metastases in nonsmall cell lung cancer. Solitary pulmonary nodules: pathological outcome of 150 consecutively resected lesions. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. The correct term should be dissecting aortic hematoma because the lesion is not an aneurysm. Blood passes into the media, creating a hematoma that separates the intima from the media or adventitia. It is unclear whether the inciting event is the intimal tear or blood from the media tearing through the intima. Hence, an intimal tear is not a prerequisite because 5%13% of patients do not have one. Suspicion is the most important factor because no one feature is common to patients presenting with aortic dissections. In any patient who presents with severe knifelike, ripping chest and back pain, the diagnosis of aortic dissection should be considered. In addition, the dissecting hematoma can encircle the lumen or actually cleave the takeoff of the subclavian or femoral vessels, resulting in the loss of pulses or systolic variation between arms. Neurologic findings, including paraplegia and hemiplegia, may also be present because of similar flap occlusion of the great vessels. Widened mediastinum and loss of aortic knob silhouette-a hematoma surrounding the aorta makes the aortic outline blurry-are helpful findings. On the other hand, unlike these modalities, angiography allows for visualization of the coronary arteries or estimation of aortic valvular insufficiency. The decision to use one modality over the other lies in the stability of the patient and the modalities available at a given institution. Angiography may be used in stable patients to define the coronary anatomy and valvular architecture, although studies show that in-house mortality is not improved with coronary angiography. DeBakey type I involves the ascending aorta and propagates to at least the aortic arch. The Stanford classification has both therapeutic and prognostic value: · Ascending (type A) involves only the ascending or both the ascending and descending aorta. Ascending dissections are twice as common as descending dissections and often begin at the right lateral wall and involve the aortic arch in 30%. Who cares whether a dissection involves the ascending (type A) or descending (type B) aorta Ascending dissections require early surgical correction to avoid extension into the coronary or carotid arteries, rupture into the pericardium (tamponade), or both. Descending dissections do not involve the ascending aorta and currently are managed with a stent graft as the primary solution. Propranolol or labetalol is particularly important because it decreases the contractility of the myocardium (dp/dt), thereby decreasing the shearing force that prevents propagation of the dissection down the aorta. What are the principles and advantages of surgical management of acute aortic dissection To restore flow to any branches of the aorta that have been sheared off and receive blood flow from a false lumen d. To protect the heart during these maneuvers and to restore coronary blood flow if a coronary artery has been sheared off. To look for tears in the transverse aortic arch Technique: Use of deep hypothermia circulatory arrest with or without retrograde cerebral perfusion is in vogue at present. This technique allows the arch to be inspected and the distal anastomosis of the Dacron graft to be sewn accurately to the distal ascending aorta in an open fashion. To restore blood flow to branches of the aorta fed by the false channel Technique: Surgery is performed using partial cardiopulmonary bypass, or the clamp and run technique, in which the aorta is crossclamped and the graft is sewn in as fast as possible (see Controversies). Endovascular repair with stents is gaining popularity, and in some clinical situations may be the better choice (see Controversies). Of patients who survive the operation, two-thirds die within 7 years because of comorbid cardiac and cerebrovascular disease. Initial surgical management: · Approximately 25% of patients initially treated medically need an operation eventually. Initial medical management: · Medical management has a lower in-hospital mortality rate (10%15%). What is the preferred management of aortic insufficiency in ascending dissections Partial left atrial-to-femoral artery bypass For: · Allows unloading of the heart · Allows distal perfusion to avoid visceral ischemia · Allows as much time as needed to complete anastomosis Against: · Requires heparinization b.
References
- Mori M, Sakaguchi H, Akazawa K, Tsuneyoshi M, Sueishi K, Sugimachi K. Correlation between metastatic site, histological type, and serum tumor markers of gastric carcinoma. Hum Pathol 1995;26:504.
- Domizio P, Owen RA, Shepherd NA, et al. Primary lymphoma of the small intestine. A clinicopathological study of 119 cases. Am J Surg Pathol 1993;17(5):429-442.
- Eckhardt MD, van Venrooij GE, Boon TA: Symptoms, prostate volume, and urodynamic findings in elderly male volunteers without and with LUTS and in patients with LUTS suggestive of benign prostatic hyperplasia, Urology 58(6):966n971, 2001.
- Im JG, Webb WR, Han MC, Park JH. Apical opacity associated with pulmonary tuberculosis: highresolution CT findings. Radiology 1991;178(3):727-31.