
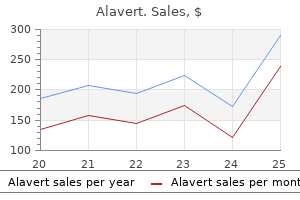
Alavert
| Contato
Página Inicial
Sharon Krystofiak, M.S., M.T. (A.S.C.P.), C.I.C.
- Infection Preventionist
- Infection Control and Hospital
- Epidemiology
- University of Pittsburgh Medical Center Presbyterian
- Pittsburgh, Pennsylvania
American Association of Clinical Endocrinologists Medical Guide lines for Clinical Practice for developing a diabetes mellitus comprehensive care plan allergy testing uk london discount alavert 10 mg online. Evaluation allergy shots for cats 10 mg alavert purchase overnight delivery, Treatment allergy dogs buy alavert cheap, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline allergy symptoms watery eyes alavert 10 mg purchase. Guidelines Committee of the International Union of Angiology; Scientific Committee of the International Union of Angiology; Council of Vascular Medi cine of the International Union of Angiology allergy medicine nasacort alavert 10 mg on-line. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice lor developing a diabetes mellitus comprehensive care plan. Primary prewntion of cardiovascular disease and type 2 diabetes in patients at metabolic risk: an endocrine society clinical practice guideline. Adjuvant Therapy for the Node-Positive Patient Prophylaxis I Prevention of Breast Cancer. These same cells, also called reticu locytes, can be quanti fied by special stains or flow cytometry, yield ing a reticulocyte count. The hemoglobin is catabolized into its heme (protoporphyrin ring+ iron) and globin components. Excluding hemorrhage and rare sequestration, all anemias can be broadly classified as either hypoproliferative or survival defects. Several images of normal blood smears and marrow aspirates are shown for your review on the next page (I mage 8-1 through Image 8-6). Ferroportin itself is controlled by hepcidin, the key regulator hormone for iron hemostasis. Hepcidin levels are decreased in low iron states and increased in iron overload states. Hepcidin binds ferroportin, causing a decrease in the release of iron into the bloodstream. So, high levels of hepcidin cause decreased iron absorption, while low levels allow for increased iron absorption. Hepcidin is also an acute phase protein that is increased in response to inflammatory cytokines (especially interleukin-6). Transferrin is a blood plasma protein that binds iron and transports it to the tissues. Transferrin receptors on cells bind this iron-containing transferrin and absorb it into vesicles. Look at the measurements of the red cell indices for density (normochromia or hypochromia) and size (microcytosis or macrocytosis). Certainly, you can look at the smears yourself rather than relying on the hematology lab for measurements and descriptions. Prior to interpretation, the reticulocyte count needs to be adjusted for the degree of anemia by correcting for the hematocrit and the reticulocyte maturation time (reticulocyte production index). Erythropoietin level is typically above normal but is lower than would be expected for the degree of anemia. In addition, there is no real increase in erythropoiesis in response to the higher erythropoietin level. In equilibrium conditions, serum ferritin level is a good indicator of total iron stores. It is low in iron deficiency anemia, high-normal to high in anemia of chronic disease, and high in hemochromatosis. Ferritin is also an acute-phase reactant and can be elevated with inflammation or chronic disease, although inflammation generally should lead to only a 3x increase in ferritin levels. Additionally, a high ferritin level is often a side effect of certain malignancies, especially hematologic cancer. T hese are distinct and different from spur cells (Image 8-13), which are seen in liver diseases. Howell-Jolly bodies are the result of fragmentation of the nucleus (karyorrhexis), causing the formation of small black "pellets. Anemia of hypometabolic states can result from deficiencies in thyroid hormone, glucocorticoids, testosterone, or growth hormone and may be one of the High/high-normal Normal presenting features of hypothyroidism, primary adrenal insufficiency, or pituitary disease (hypogonadism or panhypopituitarism). This can be congenital due to abnormal stem cells or acquired due to viral infection, thymoma (paraneoplastic), autoimmunity, lymphoprolifera tive disorders, or drugs. Marrow infiltrative disorders: Fibrosis, granulomas, or malignancy can cause changes in the peripheral blood smear, including teardrop cells, as well as immature red and white blood cells. Once you diagnose iron deficiency anemia, you must pursue the etiology: · Characterize the lab values in iron deficiency anemia vs. Signs and symptoms include fatigue, pallor, weakness, irritability, and poor exercise tolerance. Beeturia occurs in - 75% of patients with iron deficiency when eating beets leads to excreting red urine (also in- 10% of normal population). These tetramers are covalently linked to heme, a complex of ferrous iron and protoporphyrin. Thalassemias are inherited disorders characterized most commonly by absent or decreased production of either the a chain (a-thalassemia) or the chain (-thalassemia) leading to decreased production of hemoglobin tetramers and fewer red blood cells. In addition, there is unbalanced globin chain synthesis, and homotetramers are > 97. Mutations may be deletional or nondeletional and affect many different aspects of transcription and translation. The clinical manifestations correlate with the number of a-genes that are affected: the more loci affected, the worse the symptoms. Iron therapy does not improve the microcytosis, and, even worse, it can cause second ary hemochromatosis. The microcytosis can be evalu ated further with a hemoglobin electrophoresis (normal in a-thalassemia and increased A2 component in -thalassemia). In clinical practice, adult patients with a microcytosis and normal iron studies are assumed to have thalassemia, and the electrophoresis is rarely ordered. Nonetheless, it is helpful to confirm the diagnosis with Hgb electrophoresis if there is some doubt. Unpaired chains form 4 tetramers called HbH-these form inclusions in peripheral cells but not in the marrow. Clinical features are intermediate and variable and can include moderately severe hemolytic anemia but often with avoidance of transfusions until adulthood. There are 3 categories of -thalassemia: -thalassemia minor (heterozygotes): mild or no anemia, with a disproportionately high number of microcytes. In most patients, this disorder has 2- to 3-fold elevations of HbA2 (a2o2) and slight increases in HbF (a2y2) on hemoglobin electrophoresis. The remaining, highly insoluble a-globin precipitates into homotetramers, or inclusion bodies, which are toxic to erythrocytes and cause them to die within the marrow. Surviving erythrocytes carry inclusion bodies that are detected by the spleen, leading to removal of the erythrocytes and chronic hemolytic anemia. The resulting severe anemia (developing over the I 51 year of life) results in elevated erythropoietin levels and thus, erythroid hyperplasia. If the erythroid hyperplasia is severe, it can lead to extramedullary hematopoiesis in the liver and spleen and an expanded bone marrow with the latter, giving children "chipmunk facies. Think about a megaloblastic process in patients who present with a macrocytic anemia, pancytopenia, and slight indirect hyperbilirubinemia (from the continuous low-level intramedullary hemolysis). In addition to anemia, deficiencies in B12 also produce gastrointestinal effects (smooth sore tongue, diarrhea) and neurological deficits (ranging from paresthesias to frank psychosis). B12 deficiency may be present without 3) -thalassemia intennedia (homozygous): Not all patients with homozygous defects of -globin production have the full clinical severity described above. The term "-thalassemia intermedia" is used to convey this hetero geneity and to describe those patients who range from the asymptomatic to the transfusion-dependent states. If you highly and extravascular hemolysis, released hemoglobin is quickly bound to haptoglobin and then engulfed by macrophages. The resultant low level of haptoglobin can be used to diagnose hemolysis-but does not help distinguish the type. The Schilling test, in which the fate of radiolabeled B12 ingested by the patient is fol lowed, was previously used to confirm the diagnosis but is rarely used and generally not available anymore. Treat B12 deficiency with daily injections for folate deficiency with daily oral replacement. Heme loses of the iron and is converted more of the to bilirubin and cleared in the urine or stool. Urine hemosiderin high = 1 week, then weekly injections for 1 month, then monthly. Common oxidative stressors are infections, medications (including dapsone, sulfa drugs, and antimalarials), fava beans, and diabetic ketoacidosis. Other hematologic findings (and buzzwords) include Heinz bodies (chunks of dena tured hemoglobin) on special smears and "bite cells" in peripheral blood. Patients are asymptomatic or demonstrate renal papillary necrosis, painless hematuria, and isosthenuria. Splenic sequestration is common and can occur both in children and adults (unlike in sickle cell anemia), because the spleen does not always undergo early autoinfarction. Pyruvate kinase deficiency and other enzyme deficiencies within the glycolytic pathway are subject to hemolytic crisis without exposure to oxidative stress. You can screen prospective parents for the carrier state and provide genetic counseling. Exchange transfusion is sometimes required for treatment of priapism, cerebral sickling, aplastic crisis, and acute chest syndrome. Occasionally, more conservative ther apy with a simple transfusion and/or supportive care treats these presentations. A partial exchange transfusion program is reserved for those with a history of stroke. Medications such as hydroxyurea are used to increase HbF production, which offers some protection against sickle crisis. Hereditary Spherocytosis and Elliptocytosis Sickle cell syndromes result from a mutation in the Val) -globulin gene (6Giu, in which valine is substi tuted in place of glutamine. Know that parvovirus 8 19 may cause either a pure red cell aplasia or a worsening of anemia by decreasing erythropoiesis in the face of chronic hemolysis. Recurrent tissue infarction, microinfarcts of and the these are autosomal dominant disorders of the R8C cytoskeleton that result in loss of membrane flexibility and are associated with chronic hemolysis. These disorders of spherocytosis and elliptocytosis are seen in Northern European populations. Complications may include cholelithiasis, due to bilirubin stones, and splenomegaly. Think about these disorders in patients who demonstrate evidence of hemolysis and have spherocytes or elliptocytes on their peripheral smear. Recurrent infarcts of the spleen lead to functional asplenia with increased risk of infection from encapsu Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus injluenzae, and from Salmonella. To protect against these organisms, penicillin prophylaxis is used in children until age 5. Sophisticated molecular membrane studies (usually available at research institutions) can be done to make a definitive diagnosis. Acute chest syndrome (chest pain and desaturation of oxygen) is thought to represent microinfarctions of the lung. The acute chest syndrome is a hematologic emergency which may require red cell exchange transfusion. Instead, the complement components whose binding they induce are detected with a positive direct result using antibodies to C3 (indicates ability to fix complement), not IgG (because the hemolysis is caused by antibodies to IgM). These IgM autoantibodies may be secondary to: · · Which virus is implicated in the development of aplastic crisis or worsening of anemia in patients with sickle cell disease The result is the loss of a membrane-bound protein, which, when present, anchors other proteins to the cell membrane. Some of these anchored proteins serve to protect the cell against complement-mediated lysis. Clinical presentation includes a variable degree of intravascular hemolysis, which may lead to chronic hemo globinuria and iron deficiency. Classic symptoms include episodic abdominal pain and chest pain due to diffuse esophageal spasms that coincide with hemoglobinuria. Rarely, transformations to aplastic anemia, acute leukemia, and myelofibrosis occur. Eculizumab, an antibody to C5 terminal component, has been shown to decrease hemolysis and the need for transfusion. Penicillin bound to red cells may elicit an antibody response that can cause hemolysis. Quinine, methyldopa, and certain cephalosporin antibiotics are also known culprits. Sequestration this type of anemia occurs with overactive, often enlarged spleens in a variety of disorders, especially portal hypertension where red cells, white cells, and platelets may be sequestered. In early childhood with HbS/C and HbS/-thalassemia (before splenic infarction and fibrosis are seen), splenic sequestration may occur. And remember again, any Fe deficiency anemia is considered to be due to blood loss until proven otherwise. These antibodies induce hemolysis either by stimu lating macrophages and other cells in the spleen and reticuloendothelial system to gradually snip portions of membrane away (causing spherocytes) or by causing complement-mediated destruction. Symptoms include head ache, dizziness, dyspnea, tachypnea, tachycardia, and obtundation. Cirrhosis causes spur cell anemia (Image page Red cells change shape and are hemolyzed. Alcohol abuse is associated with nutritional (megaloblastic) anemias, especially folate. Viral hepatitis can cause anemia through direct inhibition of the marrow and via autoimmune hemolysis. Cutaneous porphyrias cause either acute nonblistering or chronic Cancer Patients Cancer patients may have coexisting causes of anemia.
This is just proximal to the area where the 3 tendinous extensions of the gracilis allergy symptoms cough treatment generic alavert 10 mg overnight delivery, sartorius allergy store order 10 mg alavert visa, and semi-tendinous muscles insert into the medial aspect of the tibial tuberosity allergy testing qld health alavert 10 mg with visa. Radiographs are usually not necessary allergy medicine you can drink with cheap alavert 10 mg online, but can assist in excluding diseases that present similarly allergy forecast nyc purchase generic alavert online, such as idiopathic, monoarticular, benign synovial tumor that causes recurrent hemarthrosis, usually of the knee in young adults. Patients have recurrent bleeding into the knee, resulting in a darkly pigmented joint aspirate. There is no known etiology, although it seems to be associated with osteopenia and osteoarthritis. Weight-bearing pain is present initially on the medial aspect of the knee, and symptoms often resolve with conservative management, including protected weight bearing and analgesics. Look for evidence of a spondyloarthropathy in any patient who presents with plantar fasciitis. Recurrent steroid injections should be avoided because they cause fat pad atrophy. By imaging, you are ruling out: ·Disk herniation · Spinal stenosis · Compression fracture ·Malignancy ·Infection Muscle Strain More than 50% of adults experience at least I episode of back strain at some time. Classic presentation is agonizing, lower back pain with a history of lifting a heavy object or making a sudden movement. Physical exam typically reveals guarding of movement due to pain and no true muscle weakness or neurologic deficit. These include a moderately prolapsed disk, catching of the synovial membrane in a facet joint, transient subluxation with ligament strain, and basic muscle strain. General Approach to Lower Back Pain Evidence-based practice guidelines issued by the American College of Physicians in 2007, and updated in than bed rest. Surgery is usually not required; studies show that in non-emergent patients initially considered surgical candidates, conservative treatment is just as effective as surgery in the long term. Nonspecific lower back pain, sometimes called lumbago, is diagnosed when the patient gives the classic history and has no red flags to suggest a more serious etiol ogy. The main things you need to worry about when it comes to back pain red flags are infections (disci tis, osteomyelitis, paraspinal abscesses) and cancer (principally, prostate cancer and multiple myeloma). Treat others conservatively for I = Disk Herniation Herniation presents with local or radicular pain-and with weakness, if severe. Classic disk pain is worse when sitting or bending and better when standing or lying. Neurologic deficits or intractable pain are indications for surgery month and then. This loss of bony continuity is visible, especially on the oblique view of a lumbar x-ray film. Although it was formerly thought to be congenital, spondylolysis is now thought to be more likely secondary to a stress fracture during childhood. Which patients should get urgent imaging of the spine if they present with lower back pain What diagnosis should you consider in injection drug users who present with pain in their buttocks Studies on the specificity and clinical correlation of antiribosomal Abs in systemic lupus erythematosus sera. Occasionally, spondylolisthesis results in sciatica, but generally it does not affect the nerves of the cauda equina. Autoantibodies against ribosomal proteins found with high frequency in patients with sys temic lupus erythematosus with active disease. The stenosis of the spinal canal in the lumbar region may cause a crimping or claudication-like symptom due to nerve compression of the cauda equina. Symptoms typically consist of a progressively severe, heavy, aching sensation in the lower extremities after walking or standing several minutes. Symptoms of spinal stenosis worsen with back extension (descending stairs) and improve with back flexion (ascending stairs, leaning forward on a grocery cart). This entity must be distinguished from ischemic claudication, which presents as pain with ambulation classically relieved with rest and associated with obvious vascular disease on examination. Pseudoxanthoma elasticum: genetics, clinical manifestations and therapeutic approaches. Think about infectious sacroiliitis in an injection drug user who presents with buttock-area pain. Rheumatoid arthritis disease activity mea sures: American College of Rheumatology recommendations for use in clinical practice. American College of Rheu matology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Treating rheumatoid arthritis to target: recommendations of an international task force. Cardiovascular safety of non steroidal anti-inflammatory drugs: network meta-analysis. Updating the American College of Rheumatol ogy revised criteria for the classification of systemic lupus erythematosus. Combination therapy for pain management in inflammatory arthritis (rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, other spondyloarthri tis). British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of rheumatoid arthritis (after the first 2 years). Evaluation of diagnostic criteria for ankylosing spondylitis: a proposal for modification of the New York criteria. Comparison of recommendations for the use of anti-tumour necrosis factor therapy in ankylosing spondylitis in 23 countries worldwide. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. Guidelines of care for the treat ment of psoriasis and psoriatic arthritis: case-based presenta tions and evidence-based conclusions. Guidelines of care for the man agement of psoriasis and psoriatic arth ritis: section 4. Guide lines of care for the management and treatment of psoriasis with traditional systemic agents. Point: Hydroxyapatite crystal deposition is intimately involved in the pathogenesis and pro gression of human osteoarthritis. Counterpoint: Hydroxyapatite crystal deposition is not intimately involved in the pathogenesis and progres sion of human osteoarthritis. European League Against Rheu matism recommendations for calcium pyrophosphate deposi tion. Part I: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Viscosupplementation for osteoar thritis of the knee: a systematic review of meta-analysis. Differentiation of post-strepto coccal reactive arthritis from acute rheumatic fever. Hereditary hemochromatosis: a neglected diagnosis in orthopedics: a series of 7 patients with ankle arthritis, and a review of the literature. Pathogenic Neisseriae: gonorrhea, neonatal ophthal mia and meningococcal meningitis. European League Against Rheumatism recommendations for monitoring patients with systemic lupus erythematosus in clinical practice and in observational studies. Mixed connective tissue disease: an overview of clinical manifestations, diagnosis and treatment. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Antiphospholipid syndrome: laboratory detec tion, mechanisms of action and treatment. Committee on Practice Bulletins-Obstetrics, American College of Obstetricians and Gynecologists. SpringerLink (Online service), International Congress on Antiphospholipid Antibodies, Erkan, D. Antiphospholipid syndrome: Insights and highlights ji-om the 13th International Congress on Antiphospholipid Antibodies. Antiphospho1ipid syndrome: laboratory detection, mechanisms of action and treatment. Nailfold capillaroscopy is useful for the diagnosis and follow-up of autoimmune rheumatic diseases. Systemic sclerosis - a systematic over, view: part I - disease characteristics and classification, patho physiologic concepts, and recommendations for diagnosis and surveillance. Treatment of systemic sclerosis complications: what to use when first-line treatment failsa consensus of systemic sclerosis experts. Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treat ment. Epidemiology and etiology of Wegener granulomatosis, microscopic polyangiitis, Churg-Strauss syndrome and Goodpasture syndrome: vasculitides with frequent lung involvement. Aortitis: imaging spectrum of the infectious and inflammatory conditions of the aorta. Large- and small-vessel vasculitis: a critical digest of the 2010-2011 literature. Review of current therapies for second ary hypertrophic pulmonary osteoarthropathy. Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Examination of the elbow: linking diagnosis, prognosis, and outcomes as a framework for maximizing therapy interventions. Medications for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physi cians clinical practice guideline. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American Col lege of Physicians and the American Pain Society. Comprehensive evi dence-based guidelines for interventional techniques in the management of chronic spinal pain. We at MedStudy do our best to review and include in this publication accurate discussions of the standards of care and methods of diagnosis. MedStudy further disclaims any and all liability for damages and claims that may result from the use of information or viewpoints presented. In MedStudy material, you will see the non-possessive form when the proper name is followed by a common noun;. Example: In cases of suspected Cushing syndrome, the dexamethasone suppression test is performed to suppress production of cortisol. Functionally, it is comprised of the anterior pituitary and the posterior pituitary, each of which participates in different hormonal axes. It controls the output of the posterior pituitary (neurohypophysis) by direct nerve stimulation. Thirst begins when serum osmolality exceeds 295 mOsm/L and becomes more intense as serum osmolality increases. Negative feedback decreases the deviation from an ideal normal value and is important in maintaining homeostasis. Example: Primary hypothyroidism means the thyroid gland is diseased and not producing thyroxine. Tertiary refers to disease of the gland that controls the gland that controls the primary gland. Secondary hyperaldosteronism means that the disease is in the gland that controls aldosterone release. The hypothalamus stimulates pituitary hormone secretion, which then stimulates target organ hormone production. Target organ hormones negatively feed back to both the pituitary and the hypothalamus. Common mass effect symptoms include headaches, diplo pia or visual field defects (bitemporal hemianopsia, most commonly), and seizures. Especially suspect a pituitary adenoma when a patient presents with multiple hormone abnormalities, such as a mixture of hypothyroid and adrenal insufficient symp toms. Pituitary tumors are due to the abnormal proliferation of cells of the anterior pitu itary. The first step in evaluating a pituitary tumor is to determine whether it is functionally abnormal and whether it is secreting an abnormal amount of any of the various hormones. Finding these subunits indicates that a pituitary mass is definitely pituitary in origin (vs. However, they may cause symptoms secondary to mass effect and impingement on the optic nerve. When and how to properly order these hormone tests is discussed in their representative sections that follow. Lactotrophs (prolactinomas)-> hyperprolactinemia; tied with gonadotrophs as the most common type of macroadenomas · Gonadotrophs -> variable presentation: o Mass effect+ clinically silent Mass effect+/- gonadotropin deficiency/ partial panhypopituitarism Mass effect+/- gonadotropin hypersecretion; tied with lactotrophs for most common type of macroadenomas o o © 2014 MedStudy-Piease Report Copyright Infringements to copyright@medstudy. They are usually microadenomas roadenomas (< 1 em in diameter), but they can also be space-occupying mac (2: I em in diameter) associated with visual What is meant by positive and negative feedback regulation in endocrine diseases Decreased libido is the earliest symptom of a prolactinoma in males and is often ignored; so men tend to present later with visual field defects. Long-standing, unrecognized disease is associated with decreased skeletal bone mineralization in both men and women. Treatment for these tumors is started when the size of the tumor causes neurologic symptoms (headaches, visual field disturbances) or when hypogonadism exists. Microadenomas usually do not increase to · What is the formula to estimate serum osmolality No treatment is needed for empty sella syndrome if no hormone deficiencies are associated. Of course, the sella may actually be "empty," and the patient may have hypopituitarism.
This raises norepinephrine levels allergy forecast okc alavert 10 mg purchase on line, which can cause cardiac remodeling allergy warning label alavert 10 mg mastercard, lead to arrhythmias allergy medicine-kenalog generic alavert 10 mg without prescription, and increase mortality risk austin allergy forecast yesterday order alavert overnight delivery. Mortality is clearly improved by carvedilol (65% relative risk reduction) allergy shots for horses buy alavert in united states online, metoprolol succinate, and bisoprolol (35%). Previously, it was taught that starting these drugs while patients are decompensated is contraindicated. Current guidelines recommend initiation of beta blockade at any stage of heart failure, once adequate diuresis has been achieved and intravenous diuretics have been discontin ued. Carvedilol (Coreg) is a nonselective beta-blocker that also has some alpha-blocker effect. They decrease systemic vascular resistance, pulmonary capillary wedge pressure, right atrial pressure, and end-diastolic and end-systolic dimensions; and they improve cardiac performance, as evidenced by increased cardiac output and stroke volume, and by improved fractional shortening, as determined by echocardiogra phy. In addition, they reverse the remodeling in the myocytes, which causes progression of heart failure. If a loop diuretic given twice daily in doses equivalent to furosemide 100-200 mg/d is inadequate, a thiazide diuretic or metolazone can be added, which results in a synergistic effect. This combination can result in severe hypokalemia, so close monitoring is necessary. Nitrates are occasionally used next (good venodilator, moderate arterial dilator -remember the nightly 6-hour nitrate-free window to prevent tolerance (discussed under Anti-Anginal Drugs on page 5-12). Hydralazine and lsosorbide Dinitrate · In what population is hydralazine dinitrate beneficial Hydralazine is an afterload reducer (arterial vasodilator); it also increases heart rate. Hydralazine is fre quently used with nitrates to get the added benefit of decreased preload. Anticoagulation More notes on diuretics: · Thiazides mainly block Na+ and Cl- resorption in the · · · · distal convoluted tubule and, to a minor extent, block Na+ resorption in the proximal tubule. Spironolactone competitively inhibits aldosterone (so, is K+ sparing) and is being used increasingly in the management of chronic heart failure. Eplerenone is similar to spironolactone but more selective for the mineralocorticoid receptor. Furosemide (Lasix), bumetanide (Bumex), torsemide (Demadex), and ethacrynic acid are the loop diuretics. Table 5-13: Drugs that Increase D1goxm Level Alprazolam Amiodarone Abx: Macrolides and tetracycline CyclospMin Diphenoxylate or propantheline (decrease bowel motility) Indomethacin Itraconazole (antifungal). With azotemia, do not use spironolactone or triamterene because these can cause hyperkalemia; thiazides are not effective, but furosemide usually is. It is started after the above therapies are established and the patient is still symptomatic. It does not cause thrombocytopenia (unlike amrinone), and it is not associated with tachycardia. Rarely used: Prazosin and minoxidil are also afterload reducers but are associated with rapid development of tolerance and fluid retention. Ventricular dyssynchrony is caused by electrical disturbances that cause the heart to pump blood in an inefficient way. Long-term use of positive inotropic drugs is potentially harmful, except as palliation for patients with end-stage disease (Stage D) who cannot be stabilized with optimal medical therapy. You can also see it in patients with hyperthyroidism, beri beri, carcinoid, or anemia. Remember, though, these patients often have a normal cardiac output at the time of diagnosis-because of the worsening ventricular failure! Emergency Treatment for Severe Heart Failure [Know:] With severe ventricular failure, patients may require short-term treatment with inotropes (dopamine, dobutamine, and milrinone). Dobutamine is another inotropic agent that can be used for severe ventricular failure. It does not have the vasoconstrictor activity of dopamine and actually has some vasodilatory effects. Both Dressler syndrome and postpericardiotomy syndrome are autoimmune processes that occur several weeks after the precipitating event. Patients with pericarditis commonly present with very severe chest pain, sometimes pleuritic, which (classically) improves when leaning forward. The pain is retro-sternal and left precordial, and referred to the neck, arms, or left shoulder. Do not treat idiopathic pericarditis with steroids because there can be a relapse when they are stopped. Constrictive pericarditis must be differentiated from restrictive cardiomyopathy (page the signs and symptoms can be similar. Pericardiectomy often does not have good results and is tried only after medical treatment options have been exhausted. On the other hand, pericardiocentesis rarely helps in diagnosis but is often used to treat viral, idiopathic, neoplastic, hypothyroid, and renal failure-related tam ponade. A lateral chest x-ray that shows calcification over the right ventricle is pathognomic for constrictive pericarditis. The pericardium can be of normal thickness in -20-25% of cases of constrictive pericarditis. In both tamponade and constrictive pericarditis, cardiac cath shows the same pressure during diastole in all 4 chambers. You can often make the differentia tion between tamponade and constrictive pericarditis at the bedside using these hallmark signs (see tamponade below). Constrictive pericarditis must be treated with an open thoracotomy and pericardiectomy. Compare and know the difference between this and constrictive pericarditis (above). If there is a> 2:1 left-to-right (pulmonary/systemic) shunt, a surgical closure is done, even if the patient is asymp · What are the 2 clinical hallmarks of constrictive pericarditis Patients with ostium primum atrial septal defect may have a loud pansystolic murmur 2° to mitral and/or tricuspid regurgitation. Know that the magnitude of any shunt does not depend on the total blood flow rate, but is commonlyly a constant ratio of pulmonic to systemic flow (Qp/Qs). It is the most common form of congenital heart disease found initially in adults (F> M), excluding a bicuspid aortic valve. The left-to-right shunt causes diastolic overloading of the right ventricle and increased pulmonary blood flow with inspiration and expiration. They are uncommon in adults because most have either closed spontaneously or have been surgically closed in childhood. Other associated anomalies include mitral valve problems, left ventricular myocardium problems, and membranes in the left atrium. Notice that all of the heart problems associated with coarctation of the aorta are left-sided! The classic physical findings are either a delayed fem oral/brachial pulse (feeling the brachial and femoral pulses, there is a distinct delay in femoral pulse) or an absent femoral pulse. Patients can have upper-body hypertension and can get hypertensive aneurysmal dilatation and rupture of the circle of Willis. Look for rib notching on chest x-ray due to the collateral vessels getting very large and eroding the ribs. Turner syndrome is associated with coarctation of the aorta and a bicuspid aortic valve. These two are covered extensively in Pulmonary Medicine, Book 2, so we will cover the other causes here. This can present as exertional chest pain or exertional syncope in a young, otherwise healthy individual. Syncope after exercise can occur in "normal" people, but syncope during exercise is never normal. With anomalous coronary artery, there is an abnormal course of I of the 2 coronary arteries between the 2 great vessels, the pulmonary artery and aorta. At rest, there is plenty of room for the vessel to pass without compromise; however, in extreme exercise, the cardiac output can increase 4-8-fold. This expands the elastic pulmonary artery and aorta, resulting in compression of the coronary artery as it courses between the great vessels. Most patients treated for acute pulmonary thromboembolism do not develop chronic pulmonary hypertension. Next most common are coronary anomalies (17%)-although this is a more likely cause in the 30-40-year-old group. It is absolutely contraindicated in the I st trimester; although, to be safe, most physicians do not give it at all during pregnancy. Although heparin is not contraindicated, it does cause increased morbidity and mortality in mother and child. A maternal a rubella infection during pregnancy is common cause among of supravalvular aortic is stenosis, not a · What is the only effective treatment for Eisenmenger syndrome Previously it was called idiopathic pulmonary has 1: alone, pregnancy is associated with increased risk; refer these patients to a high-risk obstetrician. F low murmurs and S3 gallops are also common, and the jugular venous pressure increases. The World Health O rganization reorganized causes of pulmonary hypertension into 5 groups of which! Treatment: Calcium channel blockers (in patients who are "reactive" to vasodilator testing) and sildenafil (Viagra, Revatio) are helpful. In aortic stenosis and dilated cardiomyopathy, patients are typically kept at bed rest. A lead tracing is positive if the wave of depolarization spreads toward the positive pole of that lead, and it is negative if it spreads away from the positive pole. On the horizontal plane, it is recorded via electrodes placed in the V l -6 position. Occasionally, a V3R and V4R (placed same as V3 and V4, except on the right side of the chest) are used to better monitor the right side of the heart. You divide 300 by 6 and get 50, but you know the heart rate is actually a little faster because the inter val is not quite 6 big squares. If both are prominent, you can quickly tell in which quadrant the mean vector lies. This is because the wave of depolarization through the atrium is toward V1 in the right atrium (left side of P wave) and somewhat away from V1 in the left atrium (right side of P wave). With right atrial preponderance, (enlargement, hypertrophy, overload), the right atrial (initial) portion of the P wave is widened, and therefore overlaps onto the left atrial portion of the P wave. If seen, it is usually a < 1 mm, rounded deflection in the same direction as the T wave. If the U wave is prominent, there is an increased tendency for torsades de pointes. Prominent U waves are present with hypokalemia, bradycardia, digitalis, and amiodarone. The pulmonary hypertension may result in right atrial preponderance with associated P wave changes (see previous discussion). Subendocardial ischemia (especially if downsloping or flat), such as seen in classic angina. R eciprocal depression in V1-2 with some inferior wall Mls-especially those with lateral or posterior extension. Population I 0,000; sensitivity = 25%; specificity 95%; find all the other numbers. It is thought that rela tive coronary insufficiency (increased muscle mass > increase in size of the capillary bed) may be a factor in this prolonged activation. Another factor may be the overgrowth of the muscle mass relative to the Purkinje system. For greater ease of use, intrinsicoid deflection is often called the "R peak time. These 2 fast conduction pathways travel down the interven tricular septum, and one then goes to the right ventricle, while the other one-functionally if not anatomically splits again and proceeds to the anterior and posterior sections of the left ventricle. If conduction in one of these pathways is blocked, the depolarization downstream to that pathway is delayed because the myocardial tissue in that area can then be depolarized only via the depo larization wave from much more slowly conducting adjacent myocardial tissue. The septal depolarization is left to right but directed superiorly, causing a small Q wave in the inferior leads. This also causes lead I to record a large R wave and the inferior leads to record a large S wave. More on this is discussed next and under the previous Arrhythmia topic on page 5-38. No P waves: "irregularly irregular" rhythm Clinically: varying pulse pressure and no a · · waves · Atrial fibrillation is the result of multiple ectopic foci firing continuously or disorganized atrial activity. No P waves are seen, although there is loud, chaotic atrial "noise" throughout the tracing. Atrial flutter (Type · · A ventricular escape beat may occur if the sinus pause is long enough, and no atrial or junctional pacemakers kick in. Complete (3rd degree) heart block has an atrial beat marching independently of a junctional or ventricular escape beat. This results in the "sawtooth"-appearing P wave with an atrial rate of 300 bpm (but it varies between 240 and 340 bpm). If a junctional pacemaker focus takes over the rhythm, this is termed a "junctional (escape) rhythm. The first P wave is visible, the second is just peeking out of the previous T wave, and the third is fused with the previous T wave. Cardiac physical diagnosis in the digital age: an important but increasingly neglected skill (from stethoscopes to microchips). Complications associated with pulmonary artery catheters: a comprehensive clinical re view. Cardiac stress testing for the diagnosis and management of coronary artery disease: a reference for the primary care physician. Left bundle-branch block artifact on single photon emission computed tomography with technetium Tc 99m (Tc-99m) agents: mechanisms and a method to decrease false-positive interpretations. Role of the pulmonary artery catheter in diagnosis and management of heart failure.

Look out for these complications: lung abscess allergy symptoms chest pain generic alavert 10 mg line, pneumatoceles allergy symptoms yellow jacket 10 mg alavert buy visa, and empyema in the patient with history of parapneumonic effusion allergy testing panel generic alavert 10 mg buy. Treatment: For susceptible pneumococcus allergy shots vs nasal spray alavert 10 mg order free shipping, many drugs are effective allergy medicine walgreens order alavert 10 mg without prescription, including tetracyclines, macrolides, peni cillin, cephalosporins, and respiratory quinolones. Streptococcus pneumoniae Pneumococci live in the nose and throat of up to 40% of healthy children. Any adult who has contact with chil dren, day care centers, and other crowded conditions (military barracks, dormitories, homeless shelters, pri sons) is at risk for becoming colonized and subsequently infected with Streptococcus pneumoniae. Upper respiratory inflamma tion from a cold virus, in the colonized patient, then sets the stage for bacterial pneumonia and/or sinusitis. Current recommendations include a booster vaccine for patients over 65 years of age if > 5 years have elapsed since initial vaccination. Presentation is typical for pneumonia with fever, dyspnea, and cough; but patients with staph may have hemoptysis with salmon pink sputum, and diffuse lung infiltrates and/or pneumatoceles. Diagnosis: As with other pneumonias, diagnosis is supported when a good sputum sample shows the organ < 2 years of age because the protein conjugate is more effective at stimulating the immune system in this age group. Haemophilus influenzae Haemophilus influenzae may be encapsulated or unencapsulated ("nontypeable"). A good sputum sample often shows you the organism on Gram stain-pleomor phic gram-negative coccobacilli. Definitive diagnosis is made when you grow the organism in culture from a normally sterile site. Complications include empyema (frequent), an immune complex type of glomerulonephritis, and pericarditis. Daptomycin is ineffective for respiratory infections; do not use it to treat staph pneumonia! But if the immune system or skin barrier breaks down, the staph can cause a problem. Be aware of some buzzwords classically asso ciated with gram-negative pneumonia: "currant jelly sputum" (bloody sputum that resembles jelly) and the "bulging fissure sign" (an x-ray finding in Klebsiella pneumonia that is associated with a lobar infiltrate). Treatment: If you suspect Pseudomonas based on under lying chronic disease or hot tub exposure, empirically treat with 2 antipseudomonal drugs- I of which should be a broad-spectrum antipseudomonal penicillin. Once culture results are available, with susceptibility results, narrow the regimen. Moraxella catarrhalis Moraxella catarrhalis colonizes the mouth and upper · Describe the microbiologic characteristics of Moraxella. In a large study, Moraxella never caused pneumonia in healthy indi · What are the extrapulmonary manifestations of infection with Mycoplasma pneumoniae Treatment: Know that many enteric gram negatives are either innately resistant to ampicillin or have acquired ampicillin resistance. When you suspect gram-negative pneumonia, your empiric antibiotic choice should be broad in spectrum; i. Once cultures identify your organism, you can narrow treatment based on resistance testing-often an oral quinolone is adequate to finish therapy. The x-ray pattern is variable, ranging from lobar infiltrates to diffuse involvement, and even interstitial disease in some cases. Diagnosis is typically simple because a quality sputum sample shows an overwhelming number of obvious organisms that are described as gram-negative cocci. It is useful to look at the Gram stain yourself because the organisms line up side-by-side and look like a pair of kidneys (not usually reported by the micro tech on the Gram stain result). Treatment monia: is straightforward because the bug is or generally susceptible to most drugs used to treat pneu doxycycline, macrolides, cephalosporins, amoxicillin/clavulanic acid. Up to 90% of isolates pro duce a -lactamase, which breaks down penicillins but not cephalosporins. Patients who are infected with this organism in their lungs have an underlying illness that allows their alveoli and air ways to stay moist. And most often, the underlying disease process requires either chronic or intermittent antibiotic use, such that drug pressure selects for coloni zation with resistant and hearty gram negatives. A sputum Gram stain with many polys + sputum culture that grows the organism suggests infection. These organisms require special culture media+/- serologic tests to establish diagnosis. Incubation is 2-3 weeks, and onset of dyspnea, cough, and fever is typically insidious, although occasionally presentation can mimic pneumococcal dis ease. Diagnosis is made by measuring acute and convalescent IgM antibody titers using enzyme immunoassay. If the convalescent titer rises by:=::: 4x the acute titer, then you can make the diagnosis retrospectively with sitivity and specificity. Cold agglutinins are nonspecific IgM antibodies that support the diagnosis in settings of high clinical suspicion but have low sensitivity and specificity. Treatment of Diagnosis: Preferred diagnostic tests for Legionella pneumophila pneumonia are sputum culture on special media (buffered charcoal yeast extract agar, but results take longer than 3 days) and the urinary antigen test using enzyme immunoassay. Patients sometimes take a long time Coccidioides immitis infection (coccidioidomycosis) is (> 6 months) to fully recover! Typical history includes recent travel to Arizona and "got caught in a dust storm. The fatigue and arthralgias can linger; thus, infection has been termed "desert rheumatism. Treatment of coccidioidomycosis: the common, self-limited form usually does not require treatment and may leave thin-walled lung cavities. Symptoms are similar to Mycoplasma pneumonia with the addition of pharyngitis and hoarseness. Often, there is a biphasic illness; the patient presents with a sore throat that is negative for group A strep; then 2-3 weeks later, hoarseness and pneumonia develop. Again: Sore throat - pneumonia + hoarseness = Chlamydophila Chlamydophila pneumoniae. Treatment: Effective antibiotic therapy includes doxycycline or macrolides for 3 weeks. Presentation can be similar to , and is often confused with, B if there is hemoptysis or hilar enlargement on chest x-ray. The disease begins Histoplasmosis is uncommon, except in endemic areas of the southern and midwestern U. It is associated with soil animals (chickens) and cave-dwelling animals, such as bats. With acute disease, the chest x-ray shows hilar adenopathy and focal alveolar infiltrates. Heavy expo sure ("epidemic," disseminating form) is suggested by a chest x-ray revealing multiple nodules in addition to the hilar adenopathy. Image 3-16: Methenamine silver stain of pathology specimen shows the broad-base budding of biasto yeasts Viruses Influenza · Describe the microbiologic characteristics of Blastomyces. Complement Think primary viral pneumonia in a patient who has typical influenza symptoms with progressive worsening but with scant sputum production. No treatment is indicated for the usual disease, although some recommend itraconazole. It is usually acquired by middle-aged men in the central, southeast, and mid Atlantic states. This is the patient who gets influenza the mixed viral and bacterial pneumonia seen with influ More common than either of the above presentations is Progression can be indolent to severe. Blastomycosis is more pyogenic than the others, and Diagnosis of blastomycosis: No skin test is available. In this situation, the patient coughs up purulent nia, but time does not lapse between obvious flu and and wanes between improvement and exacerbation. X-rays show areas of consolidation, and sputum may Treatment of blastomycosis: · assay-especially recommended is an assay that distin not I 00% sensitive, however, and false negatives are done only at specialized labs. The rapid tests are Diagnose influenza A and B with rapid antigen detection Indolent: observation or oral itraconazole. Mild-to-moderate: itraconazole x 6 months; also can use ketoconazole or fluconazole. Severe: amphotericin B; then may switch to itracon itraconazole (as with histoplasmosis, previous). Empiric treatment of influenza requires use of zanamivir (Relenza) or oseltamivir (Tamiflu) because most cases of influenza A/H3N2 have acquired resistance to amantadine and rimantadine. Quantitative cultures are often used to help differentiate contaminated culture material from true infection. A threshold for culture growth is accepted for each type of specimen; when growth exceeds the threshold, pneu monia is considered present. Treatment: the antibiotic used for aspiration pneumonia · Name the drug options for empiric treatment of influenza. Risk factors for aspiration include seizures, alcoholism, esophageal abnormalities, and swallowing problems. Typical organisms that live in the mouth are anaerobes, but alcoholics have a high inci dence of gram-negative enterics. Lung abscess as a focus of metastatic infection can occur with right-sided staph endocarditis in injection drug abusers and in dialysis and chemotherapy patients who have chronic venous access. Abscesses present as an indolent cough with purulent, often fetid, sputum (especially in anaerobic infections), although abscesses due to metastatic staph are more acute. The chest x-ray typically shows cavitary lesions (in the upper lobes and posterior segment of the lower lobes in cases of aspiration). Treatment with clindamycin is preferred over -lactams because mouth anaerobes often make -lactamases. If gram-negative organisms are suspected, use a combination -lactam/-lactamase inhibitor drug, such as ampicillin-clavulanic acid. When a patient aspirates, it is not necessary to start antibiotics immediately because stomach contents often cause only a chemical pneumonitis. Even so, observe the patient carefully because cavitating pneumonia and/or empyema can develop. Most common infection-causing bacteria are Fusobacterium nucleatum, Bacteroides melaninogenicus, and anaerobic streptococci. Common presenting signs of reactivation tuberculosis include fever, weakness, night sweats, and weight loss. The chest x-ray may show an upper lobe infiltrate and hilar lymphadenopathy (Image 3-19 and Image 3-20). Not much yellow highlighting is shown here because you must know this entire section perfectly! Miliary tuberculosis is the term given to uncontrolled hematogenous spread of M tuberculosis. The clinical picture is variable-from overwhelming disease with multisystem organ failure (in primary infection) to chronic wasting (in reactivation infection). The classic chest x-ray is a faint and diffuse reticulonodular infiltrate (Image 3-21). Cell-mediated immunity kicks in to arrest dissemination and growth of organisms during this initial stage. In the lung, the granulomas sometimes © 2014 MedStudy-Piease Report Copyright Infringements to copyright@medstudy. The tuberculin skin test is contraindicated only if there has been a necrotic skin reaction to previous tests. Report all persons with current reactivation tuberculosis or suspected current reactivation tuberculosis to the appropriate state or local health department. The reading is based on the diameter of the indurated/swollen area not the erythematous area-measured perpendicular to the long axis of the forearm (Image Was the test placed too soon The following list shows how a particular diameter of induration may be significant in one group and insignificant in another. Nursing home patients and staff Patients with diabetes, silicosis, malignancy, and malnutrition "New converters" (discussed next) · · "New Converter" and the Booster Effect the terms "new converter" and "booster effect" are used to discuss certain patients who are monitored with yearly skin tests;. Any inflammatory dis ease of the eyes is at least a relative contraindication for ethambutol. All of these species are sometimes found incidentally in the sputum of healthy individuals. What do you do for the healthy patient with a single sputum sample positive for M. Radiographs often are difficult to interpret because of the underlying lung disease. Labs indicate systemic disease with leukopenia, anemia, and elevated transaminases-and blood cultures for mycobacteria are often positive. Patients with immune defi ciencies can have disseminated disease that starts with a skin infection. Some post-surgical patients have gotten infected plastic surgery sites after exposing their healing wounds to soil and water;. Think about these organisms if you see the classic history of recent plastic surgery, travel with exposure to sand and water, and indolent drain age from the surgical site. Culprit organisms include Corynebacterium jeikeium, and (Candida and Aspergillus). During the first 30 days, patients most commonly get the usual nosocomial infections-especially gram-negative pneumonias and Legionella. After 4 months, think of P jiroveci, encapsulated organisms, fungus (Aspergillus and Candida), and viral infections. Bacterial pneumonia is the most frequent cause of death in immunodeficient patients. These patients are especially suscep tible to encapsulated organisms, including S. A patient returns from a vacation to Mexico with complaints of chronic drainage from a recent tummy tuck incision.
Any patient with vitreous detachment should be referred to an ophthalmologist allergy relief vitamins discount 10 mg alavert with mastercard, who looks for current retinal detachment and also defects that allergy levels in chicago generic alavert 10 mg, when repaired allergy zucchini symptoms trusted 10 mg alavert, may forestall future retinal detachment allergy symptoms mimic flu purchase cheap alavert. The eye with vitreous hemorrhage must be examined by ultrasound to check for retinal detachment allergy medicine covered by insurance 10 mg alavert buy. Vessels may be blanched by alkali solution in severe injury, paradoxically creating the appearance of a "white and quiet" eye. Conjunctivitis may be bacterial, viral (most common cause), chemical, or allergic. Workup should include evalua tion of certain key differentiating features-acuity, pain, and photophobia (light sensitivity). Other features to assess are preauricular adenopathy, amount and type of discharge, and the location and amount of redness. Significant findings: 1) Decreased visual acuity may indicate a serious problem requiring prompt consultation. Check for an affer ent pupillary defect (seen more often in serious eye conditions). Motor: 2 branches, 2) Photophobia is a key feature of iridocyclitis (and other more serious conditions), which should be evaluated promptly (within 24 hours) for possible intensive topical steroid treatment. The superior branch supplies the superior rectus and the levator palpebrae superioris (eyelid muscle). The inferior branch innervates the infe rior rectus, inferior oblique, and the medial rectus. If the eye is not dilated, the patient probably has diabetic vascular disease affecting only the somatic branches. Ciliary flush (red near comeal limbus only in a sun ray-like pattern) suggests iridocyclitis, keratitis, or angle closure glaucoma and warrants referral to an ophthalmologist. In patients who have photophobia, foreign body sensation, and/or vision complaints, consider the more serious conditions of anterior uveitis, keratitis, or acute closed-angle glaucoma. If there is pain, instill fluo rescein to check for corneal abrasion and evert, inspect, and swab the upper lid, looking for a foreign body. Any abnormal finding, except perhaps a small corneal abrasion, requires consultation. If there is no pruritus, it is more likely dry eye (keratoconjunctivitis sicca, see next page). You can make a presumptive diagnosis with symptoms of ocular pain, photophobia, and a ciliary flush with a normal cornea and normal intraocular pressure. Slit Alkali Injury Alkali injury is a special form of trauma where treatment delay of minutes can devastate the eye. Alkali rapidly penetrates the cornea and enters the anterior chamber, where it wreaks havoc. Treatment: steroids (to reduce inflammation and scarring) and cycloplegics (to prevent synechiae). Any contact lens wearer with conjunctivitis should immediately discon tinue use of the lenses. Start these patients on topical gatifloxacin to cover Pseudomonas and gram-positives, and refer to an ophthalmologist. Acanthamoeba is a known cause of infection with Keratoconjunctivitis Sicca (Keratitis) this is most common in the elderly and in middle-aged women. It may be an early sign of systemic inflammatory disease, including Graves disease, rheumatoid arthri tis, and sarcoidosis. Treat most cases with artificial tears (electrolyte solutions, methylcellulose, or other f01mulations). Infectious Keratitis Think about bacterial keratitis in patients who wear contact lenses and who present with a painful eye that is difficult to keep open. Non-lens wearers can also get bacterial keratitis, especially if immunocompromised. On exam, the eye is red with a mucoid discharge and a visible white spot (corneal opacity) that is easily seen with a penlight. Patients have diffuse conjunctival hyperemia and pro fuse watery discharge (often with other signs/symptoms of a viral infection). Adenovirus is one of the most common etiologies, especially in the summer around swimming pools. Bacterial Conjunctivitis Bacterial conjunctivitis may be caused by staph, strep, H. Most cases of bacterial conjunctivitis resolve in 5 days even without treatment; but we do treat and follow closely because the patient can develop vision loss. Treat uncomplicated cases with topical erythromycin, sulfa, or polymyxin/trimethoprim (drops or ointment; drops are preferred for adults because vision is blurry for Viral keratitis can be caused by reactivation of latent herpes simplex. Risk factors for reactivation include laser eye treatments and a compromised immune system. Know that topical steroids can seriously exacerbate the infection, so do not prescribe any topical steroids for an eye unless you are certain that the underlying diagnosis is not herpes keratitis. Again: Remember Acanthamoeba in contact lens wearers who use tap water for lens cleaning! Remember: patients have sulfa allergy, so worsening Some conjunctivitis after sulfa treatment may be due to allergy. If complicated, obtain cultures, initiate treatment with gatifloxacin or moxifloxacin, and refer to an ophthalmologist. Aminoglycosides are not used much anymore because they irritate the cornea and cause inflammation after a few days. Patients present with decreased visual acuity, hazy cornea, pain, and hypopyon (layering of white cells visible in the anterior chamber). Patients who use extended-wear contact lenses have an impaired ability to fight conjunctivitis and are at high risk for developing vision-threatening complications. Always consider an ophthalmology referral at presentation if the patient wears contact lenses. Pseudomonas conjunctivitis can progress to corneal © 2014 MedStudy-Piease Report Copyright Infringements to copyright@medstudy. Treat it with warm compresses and a topical ophthalmologic · What virus is usually responsible for conjunctivitis The ophthalmologist does vitrectomy and cultures the vitreous fluid; then intraocular antibiotics are injected (vancomycin + ceftazidime or amikacin). Systemic antibiotics are added in severe cases, although utility is controver sial. It is important to choose antibiotics that cross the blood-brain barrier; otherwise, the drugs do not reach the vitreous fluid. Candida endophthalmitis is seen more commonly because of the widespread use of prolonged intrave nous access and cases of fungemia. Bacterial and fungal endophthalmitis present similarly, which is the reason why cultures are of paramount importance in postsurgical patients. Risk factors for candidemia include long-term venous access, neutropenic immuno compromise, long-term broad-spectrum antibiotics, and corticosteroid treatment. Know that injection drug users who dilute drugs (usually heroin) in contaminated lemon juice are at increased risk. Conductive hearing loss occurs because something blocks sound from entering the inner ear. Periorbital and Orbital Cellulitis Periorbital cellulitis usually is a rapidly progressive cellulitis of the periorbital area, which may become orbital if not treated. The key physical exam finding is normal extraocular muscle movement, without associated diplopia or pain. If the patient has disconjugate gaze, diplopia, or pain with eye movement, it is probably the result of infection that has moved into the orbital space. It may be caused by viral infections, ototoxic drugs, meningitis, cochlear oto sclerosis, Meniere disease, acoustic neuromas, or aging (presbycusis). Chalazion Chalazion is caused by obstruction of one of the tarsal (meibomian) glands forming a small nodule found in the tarsus under the eyelid. Presbycusis is characterized by bilateral symmetrical sensorineural hearing loss in the frequencies > 2,000 Hz. Meniere disease is an uncommon condition that stems from excess production or decreased drainage of endo lymphatic fluid. Patients have tinnitus, fullness in the ear, and, in more severe cases, progressive hearing loss (which is frequently one-sided) until deaf, at which time symptoms stop! Diagnosis is made with the combination of typical clinical symptoms and demonstration of sensorineural hearing loss on audiometry. Chronic treatment includes avoidance of caffeine and salt, with the addition of diuretics if symptoms continue. With sensorineural hearing loss, both air and bone conduction are decreased, but the air conduction is perceived as being louder. The patient tells you whether the sound lateralizes to one side or stays in the middle. He eventually made it to the moon after a If the sound is perceived as being in the middle, the patient either has normal hearing or the hearing loss is symmetrical. If the sound lateralizes, there is either a conductive hearing loss in the ipsilateral ear or sensorineural loss in the opposite ear. Patients usually present with tinnitus, unilateral hearing loss, and gait imbalance. There is suggestion that earlier steroids may allow for a larger percentage to have hearing return to them. Currently, data do not support any increased incidence of sexual abuse in anorexics. Physical exam may show erosive skin lesions on the fingers where the teeth cause injury during attempts to induce vomiting. The most common lab abnormalities are hypokalemia and metabolic alkalosis from vomiting and laxative use. Treatment is again supportive, with the focus on slowly decreasing the amount of food eaten and decreasing the frequency of binge-eating episodes. These patients have a distorted self-image and, despite often extreme weight loss, they not only deny thinness but complain of feeling fat. This is a "soft" criterion because many young individuals have a similar self-perception, although without the weight loss. These patients are at risk for sudden death from ventricular tachyarrhythmias, especially when refeeding. Treatment: It is important to establish a supportive advisor role with the patient. Patients are very resistant to psychotherapy, and outpatient supportive care death, often works just as well as inpatient therapy. Explain the dangers of starvation, such as sudden and set realistic, short-term goals for weight gain. Generalized anxiety disorder is associated with substance abuse and other psychiatric diagnoses: obsessive-compulsive disorder, depression, panic disorder, and social phobias. Somatic complaints are common (fatigue, memory problems, tension, and inability to sleep). Know that several brief encouraging follow-up visits to a primary care physi cian has the same effect as prescribing benzodiazepines. Anorexics are more likely to abuse drugs and have comorbid anxiety, obsessive-compulsive, and/or personality disorders. Bulimia Bulimia is the term used for binge eating of large amounts of food, followed by purging-either with vomiting or with laxatives. It may be a variant of anorexia nervosa, and many bulimia patients have a history of anorexia in their past. Bulimia patients are typically Panic disorder is diagnosed when 4 attacks have occurred within I month, or 1 or more attacks are fol lowed by I month of intense fear of another attack. These patients often have phobic avoidances of places or situations associated with attacks. Treat for 6-9 months for initial therapy, with a 2-4 week taper after improvement. Ongoing treatment with antidepressant medications is also very acceptable in patients with recurrent depression. Bipolar Disorder Bipolar disorder is characterized as a major depression with at least I episode of mania or hypomania. Most manic patients are euphoric and have inflated self esteem, decreased need for sleep, and pressured speech. Some patients are just irritable, pos sibly also paranoid-this is termed dysphoric mania. While manic episodes can be quite dramatic, most disability associated with bipolar disorder stems from depression. Bipolar patients have high rates of suicide, anxiety disorders, and substance abuse. Treatment of bipolar disorder is usually accomplished with mood stabilizing medications such as antipsy chotics (quetiapine, olanzapine), lithium, and seizure medications (divalproex sodium, lamotrigine, carbam azepine), either alone, or in combination. Antidepressant medications are generally not helpful in patients with bipolar disorder. Antidepressants also carry the risk of "switching" the patient into a manic phase of illness. The atypical drugs are associated with weight gain, diabetes, and hyperlip idemia. Know that many of the antiepileptic drugs are associated with increased risk of suicide. The neu roleptics most commonly involved are haloperidol, piperazine, phenothiazines, and thiothixene. Bromocriptine is the drug of choice, but you may also use amantadine and dantrolene. Serotonin drugs can cause derangement in thermoreg ulation-a condition termed "serotonin syndrome.
Alavert 10 mg buy on-line. Allergy Treatment in Homeopathy.
References
- Wada M, Kato T, Yuki N, et al. Gadolinium-enhancement of the spinal posterior roots in acute sensory ataxic neuropathy. Neurology. 1997;49(5):1470-1471.
- Moncada S, Palmer RM, Higgs EA. Nitric oxide: Physiology, pathophysiology, and pharmacology. Pharmacol Rev. 1991;43(2):109-142.
- Kamei S, Sekizawa T, Shiota H, et al. Evaluation of combination therapy using aciclovir and corticosteroid in adult patients with herpes simplex virus encephalitis. J Neurol Neurosurg Psychiatry. 2005;76(11):1544-1549.
- Boeck S, Ankerst DP, Heinemann V. The role of adjuvant chemotherapy for patients with resected pancreatic cancer: systematic review of randomized controlled trials and meta-analysis. Oncology 2007;72(5-6):314-321.