
Alprostadil
| Contato
Página Inicial
David Rubenstein, M.D.
- Division of Cardiology
- Elmhurst Hospital Center
- Elmhurst, NY
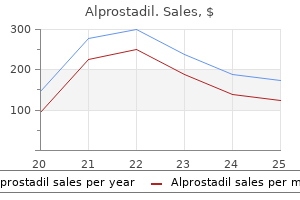
In some cases symptoms kennel cough , authorisation is specific to certain indications medicine 968 , while in others the choice of indication may be dictated by the physician (Abuhasira et al symptoms lung cancer . No analytical controls are mandatory and no legal protection or guarantees regarding the composition and quality is required medications covered by medi cal . An obligatory testing and basic regulatory framework to determine the indication area medicine 751 m , daily dosage, route of administration, maximum recommended daily dose, packaging, shelf life, and stability is also not required. Much of the ongoing confusion results from whether such products should be regulated as a food, a supplement, or medicine. However, physicians considering prescribing cannabis related products should be fully aware of the relevant legislation in relation to the heath care service for their specific geographical location. Since the situation can be complex, provision and use of guidelines from recognised national professional associations and or governmental bodies can be extremely helpful. In both, to prescribe a cannabis related product for medicinal use for epilepsy, the prescriber must be on the Specialist Register (Reference: Section 34D of the Medical Act 1983) and the prescription should be made by a consultant paediatric neurologist. It states: "If the patient asks for a treatment that the doctor considers would not be of overall benefit to them, the doctor should discuss the issues with the patient and explore the reasons for their request. If, after discussion, the doctor still considers that the treatment would not be 2 Epileptic Disord, Vol. But they should explain their reasons to the patient, and explain any other options that are available, including the option to seek a second opinion". Over a hundred different cannabinoid compounds have been isolated from the cannabis plant, for which various chemovars exist (Cannabis indica, ruderalis, and particularly sativa being the most common). Galenic products are available in the form of cannabis decoction filter bags and cannabis extracts as oils, creams, and supplement capsules. It is important to emphasise that these products demonstrate significant variation with regards to content, which is dependent not only on the initial source of the plant. Terpenes represent the largest group (with more than 100 different molecules) of cannabis phytochemicals; these can easily cross cell membranes and the blood-brain barrier. Moreover, a synergistic effect between cannabinoids and terpenes has been hypothesised, but not proven (Russo, 2011; AizpuruaOlaizola et al. Moreover, laboratory analyses have shown that the cannabinoid content is often not reflected on the marketing label (Vandrey et al. A number of studies have investigated the effect of oral cannabis extracts on intractable epilepsy, based on parental reporting. Interestingly, the overall responder rate (47%) for patients who had moved to Colorado for treatment was greater than that (22%) of those who were already living in Colorado, indicating a possible positive reporting bias and the need for appropriately controlled studies. Long-term data from studies on prenatal and adolescent exposure to cannabis products indicate, however, a possible negative and lasting effect on cognitive and, particularly, behavioural functions (Lagae, 2020). In 2017 and 2018, the first randomised controlled trials for pharmaceutically prepared Epidiolex were published for Dravet syndrome and Lennox-Gastaut syndrome, respectively (Devinsky et al. While such reform is clearly welcomed, it cannot come fast enough for those who may benefit. More serious effects included developmental regression, abnormal movements and status epilepticus. More long-term effects regarding cannabis-derived products have generally been gathered based on Epileptic Disord, Vol. The bioavailability of oral oil formulations is limited (<6%) due to extensive first pass metabolism in the liver (Bialer et al. This programme was continued and interim data on >600 patients over a 96-week period were published in 2018 by Szaflarski et al. With these very encouraging results, shortly after the initial launch of this programme, controlled trials for Epidiolex were established for Dravet syndrome (Devinsky et al. Median percent reduction of Lennox-Gastaut syndrome total seizures and monthly drop seizures based on the two controlled trials (Thiele et al. At 10 mg/kg/day, the median percentage reduction in total seizure frequency was similar at 36. The interim data after 48 weeks of treatment revealed a 48-60% median decrease in drop seizure frequency and a 48-57% median decrease in monthly total seizure frequency relative to baseline (figure 1). During the open-label extension programme, the median percent reduction of total seizures continued at between 39% and 51% over a 48-week period (figure 2). Of the 201 patients who completed the study, total seizure frequency was decreased by 48% (p=0. Median percent reduction of Dravet syndrome total seizures and convulsive seizures based on the controlled trial of Devinsky et al. A general positive trend for quality of life (particularly in Lennox-Gastaut syndrome patients), sleep behaviour (particularly in Dravet syndrome patients) and adaptive behaviour was reported. There were also particular improvements in the socialisation domain and communication domain for Dravet syndrome and Lennox-Gastaut syndrome patients, respectively. Elevated liver enzymes were reported in 12% (n=9) and 25% (n=18) in the 25 mg/kg/day and 50 mg/kg/day, respectively (of those, 81% were also taking valproate). In openlabel studies, doses mostly up to 25 mg/kg/day were used, and in the controlled studies, higher doses up to 50 mg/kg/day were used. The studies on LennoxGastaut syndrome, however, show that a significant proportion of children respond to doses of as little as 10 mg/kg/day. If the drug is well tolerated but not sufficiently effective, the dose should be slowly increased in increments of 5 mg/kg/day, as long as it is tolerated, up to a maximum of 20-25 mg/kg/day (table 4). A toxic benzodiazepine level may manifest as fatigue, somnolence, ataxia, a decrease in cognitive function or behavioural changes. If a significant increase in benzodiazepine level is observed, the dose of clobazam should be reduced (and then checked), according to an estimate based on linear kinetics. These included, in particular, somnolence, pyrexia, convulsion, rash, lethargy and elevated transaminases (>three times the normal upper limit). Moreover, in >79-100% of the cases with elevated transaminases, patients were concomitantly taking valproate. Adverse events based on randomised, double-blind, placebo-controlled trials (the most frequent adverse events are highlighted in grey). Finally, biochemical markers of toxicity should be measured, particularly regarding liver enzymes in conjunction with valproate (Gaston et al. It does, however, add to the arsenal of available add-on drugs against these severe forms of epilepsy, in some cases offering substantial benefits. Medical use of cannabis and cannabinoids containing products - Regulations in Europe and North America. Evolution of the cannabinoid and terpene content during the growth of cannabis sativa plants from different chemotypes. Galenic preparations of therapeutic cannabis sativa differ in cannabinoids concentration: a quantitative analysis of variability and possible clinical implications. Guidance on the use of cannabis-based products for medicinal use in children and young people with epilepsy. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Long-term cannabidiol treatment in patients with Dravet syndrome: an open-label extension trial. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Perceived efficacy of cannabidiol-enriched cannabis extracts for treatment of pediatric epilepsy: a potential role for infantile spasms and Lennox-Gastaut syndrome. Dosing strategies for antiepileptic drugs: from a standard dose for all to individualised treatment by implementation of therapeutic drug monitoring. Long-term safety and efficacy of cannabidiol in children and adults with treatment resistant Lennox-Gastaut syndrome or Dravet syndrome: Expanded access program results. A Phase 1, Open-Label, Pharmacokinetic Trial to Investigate Possible Drug-Drug Interactions Between Clobazam, Stiripentol, or Valproate and Cannabidiol in Healthy Subjects. The role of cannabinoids in epilepsy treatment: a critical review of efficacy results from clinical trials. Parental reporting of response to oral cannabis extracts for treatment of refractory epilepsy. Therapeutic effects of cannabinoids in animal models of seizures, epilepsy, epileptogenesis, and epilepsy-related neuroprotection. Quality of Life in Childhood Epilepsy in pediatric patients enrolled in a prospective, open-label clinical study with cannabidiol. Cannabinoid-based therapies and brain development: potential harmful effect of early modulation of the endocannabinoid system. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: expanded access program results. Quality traits of "cannabidiol oils": cannabinoids content, terpene fingerprint and oxidation stability of European commercially available preparations. Chemical profiles of cannabis sativa medicinal oil using different extraction and concentration methods. Efficacy of artisanal preparations of cannabidiol for the treatment of epilepsy: practical experiences in a tertiary medical center. Anyone considering the use of clomipramine hydrochloride or any other antidepressant in a child, adolescent, or young adult must balance this risk with the clinical need. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction in risk with antidepressants compared to placebo in adults aged 65 and older. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Families and caregivers should be advised of the need for close observation and communication with the prescriber. It is freely soluble in water, in methanol, and in methylene chloride, and insoluble in ethyl ether and in hexane. This fact must be considered in assessing the estimates of the pharmacokinetic parameters presented below, as these were obtained in individuals exposed to doses of 150 mg. Children under 15 years of age had significantly lower plasma concentration/dose ratios, compared with adults. Obsessions are recurrent, persistent ideas, thoughts, images, or impulses that are ego dystonic. Compulsions are repetitive, purposeful, and intentional behaviors performed in response to an obsession or in a stereotyped fashion, and are recognized by the person as excessive or unreasonable. The maximum dose was 250 mg/day for most adults and 3 mg/kg/day (up to 200 mg) for all children and adolescents. Myocardial Infarction Anafranil is contraindicated during the acute recovery period after a myocardial infarction. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a longstanding concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Table 1 Drug-Placebo Difference in Number of Cases of Suicidality Age Range per 1000 Patients Treated Increases Compared to Placebo <18 14 additional cases 18-24 5 additional cases Decreases Compared to Placebo 25-64 1 fewer case 65 6 fewer cases No suicides occurred in any of the pediatric trials. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression. The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, Page 6 of 27 10 2012. Prescriptions for clomipramine hydrochloride should be written for the smallest quantity of capsules consistent with good patient management, in order to reduce the risk of overdose. Screening Patients for Bipolar Disorder A major depressive episode may be the initial presentation of bipolar disorder. It should be noted that clomipramine hydrochloride is not approved for use in treating bipolar depression. All reports with methylene blue that provided information on the route of administration involved intravenous administration in the dose range of 1 mg/kg to 8 mg/kg. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection) or at lower doses. Treatment with Anafranil and any concomitant serotonergic agents should be discontinued immediately if the above events occur and supportive symptomatic treatment should be initiated. Seizures During premarket evaluation, seizure was identified as the most significant risk of Anafranil use. The observed cumulative incidence of seizures among patients exposed to Anafranil at doses up to 300 mg/day was 0. Although dose appears to be a predictor of seizure, there is a confounding of dose and duration of exposure, making it difficult to assess independently the effect of either factor alone. Caution should be used in administering Anafranil to patients with a history of seizures or other predisposing factors. Rare reports of fatalities in association with seizures have been reported by foreign postmarketing surveillance, but not in U. In some of these cases, Anafranil had been administered with other epileptogenic agents; in others, the patients involved had possibly predisposing medical conditions. Thus a causal association between Anafranil treatment and these fatalities has not been established. Physicians should discuss with patients the risk of taking Anafranil while engaging in activities in which sudden loss of consciousness could result in serious injury to the patient or others. Cardiovascular Effects Modest orthostatic decreases in blood pressure and modest tachycardia were each seen in approximately 20% of patients taking Anafranil in clinical trials; but patients were frequently asymptomatic. Nevertheless, caution is necessary in treating patients with known cardiovascular disease, and gradual dose titration is recommended.
Collection of sputum specimens more often early in treatment for assessment of the treatment response and at the end of treatment is optional treatment definition . The duration of the continuationphase regimen hinges on the microbiological status at the end of the intensive phase of treatment; thus medications safe in pregnancy , obtaining a sputum specimen at the time of completion of 2 months of treatment is critical if sputum culture conversion to a negative result has not already been documented treatment skin cancer . The culture result of a sputum specimen obtained at the completion of the intensive phase of treatment (2 months) has been shown to correlate with April 2018 Volume 31 Issue 2 e00038-17 cmr medications ending in zole . In patients treated for 6 months symptoms genital herpes , having both cavitation on the initial chest radiograph and a positive culture at the completion of 2 months of therapy have been associated with rates of relapse of approximately 20%, compared with a rate of 2% among patients with neither factor. Heat fixing is one option, with the use of a slide warmer at 65°C to 75°C for at least 2 h once the slides are air dried (75). Testing of additional specimens provides only a marginal improvement in sensitivity (examination of a third sputum specimen increased the sensitivity between 2% and 5%) (164, 168). Researchers from Johns Hopkins University evaluated a more rapid, commercially available auramine O stain that may be more cost-effective and efficient (169). A systematic review (164) showed that the sensitivity of fluorescence microscopy was 10% higher than that of conventional carbol fuchsinstained sediments. One hundred sixty-seven laboratories participated in a per-laboratory comparison of results. A comparison of prestained Ziehl-Neelsen versus prestained Kinyoun smears for the evaluation of differences in reading capabilities of participants revealed a significantly better performance of the Ziehl-Neelsen staining method (P 0. Similar results as to the lack of sensitivity of Kinyoun staining compared to routine, hot Ziehl-Neelsen staining under field conditions have also been reported (171). Depending on the mycobacterial species, different morphologies may be April 2018 Volume 31 Issue 2 e00038-17 cmr. These organisms may not always be acid fast with carbol fuchsin (1), auramine O (175), or auramine-rhodamine stain (175). Growth Detection Solid mycobacterial cultures are generally held 6 to 8 weeks, and protocols for liquid media usually require a minimum of 6 weeks of incubation before cultures can be discarded as negative (1). Receipt of interim negative reports earlier than 6 weeks could assist clinicians in considering alternative diagnoses and could alter the timing and prioritization of public health interventions. However, laboratories should analyze their own time-to-detection data to make informed protocol decisions. Since many mycobacteria are slowly growing organisms, cultures can be examined for colony formation less frequently than routine bacterial cultures. All solid media should be examined within 3 to 5 days after inoculation to determine if there is contamination. In general, cultures should be examined twice per week for the first 2 weeks and then at weekly intervals. Also, it is advisable to subculture the broth on a blood or chocolate agar plate to rule out contamination. Probes are single-stranded oligonucleotides that can have various sizes but are generally less than 50 bp. Although probe-based detection and identification methods are more expensive than conventional culture and identification methods, they have increased accuracy and decreased turnaround times relative to conventional biochemical methods (179). Bacterial strains may possess polymorphisms that prevent hybridization (180, 181), or there may be similar sequences among strains that result in cross-reactivity (182, 183). Additional disadvantages are the limited number of commercial probes available and the inability to probe clinical specimens directly. In many larger laboratories, sequence-based identification has become a primary method to rapidly identify mycobacteria. Clinical Microbiology Reviews identification over those of conventional methods, but initial growth of an isolate is still required prior to identification by sequencing. The entire gene is 1,550 bp, including the conserved and variable regions, but a discriminatory sequence can generally be obtained by using 500 bp (185). Universal primers complementary to the conserved regions permit the amplification of the gene from all bacterial species, and the resulting amplicon contains a unique sequence. Further differentiation may be required for some of these groups for epidemiological or clinical reasons. Sequence results are more robust than the results of conventional biochemical methods because they are less subjective given a comprehensive and accurate database for comparison. The spectral data are then compared to a database to determine the likely identity of the organism. A preextraction step must occur, usually involving bead beating or vortexing in ethanol, formic acid, and acetonitrile; the extracted proteins are then spotted onto the plate (194, 195). Unfortunately, this delay increases the time to reporting compared to what can be achieved with sequencing. Conventional Biochemicals Identification of mycobacteria has traditionally relied on phenotypic characteristics such as the growth rate, colony morphology and pigmentation, optimal growth temperature, and reactions in a battery of biochemical tests. Many of these tests require growth on solid media, are poorly reproducible, and can take several weeks of incubation before species-level identification can be done (204). In addition, variability in phenotypic characteristics can be seen within strains of a species. With the development of molecular methods for the identification of mycobacteria, there are close to 200 recognized Mycobacterium species (6). Many of these new species have not been characterized biochemically and cannot be reliably identified by using biochemical methods. Clinical Microbiology Reviews It is now recommended that laboratories not rely on biochemical methods for the identification of Mycobacterium species (132, 205). If these capabilities are not available locally, isolates should be referred to a reference laboratory (205). In programs using ofloxacin or levofloxacin and moxifloxacin, possible testing is for moxifloxacin only at both concentrations (0. For programs using only moxifloxacin, testing is performed with the higher concentration (2. Most growth-based conventional methods test the susceptibility of the microorganism to a critical concentration of the drug. The critical concentration (Table 12) represents the lowest concentration of the drug that inhibits 95% of wild-type strains of M. Essentially, the critical concentration differentiates antimicrobialsusceptible from antimicrobial-resistant strains and is based on international convention (215, 216). However, it is a labor-intensive method, with the calculation of resistance by performing colony counts, which requires skilled staff. Clinical Microbiology Reviews In addition, there is a longer turnaround time, up to 3 weeks, than those of broth-based methods. This method uses a 96-well plate that is inoculated with a series of dilutions of first- and second-line drugs (a total of 12 drugs are provided, each with a minimum of 7 dilutions on the standard plate). If testing is performed in-house, it is important to have a robust quality assurance program, which includes elements such as quality control, proficiency testing and performance monitoring (as discussed in Quality Assurance, below), and appropriate biosafety practices (as discussed in Biosafety, above). A summary of the most commonly used growth-based methods in the United States is provided in Table 13. If molecular methods for the detection of resistance are not performed, the specimen/isolate may be referred to a laboratory that has the capability to perform this testing, such as a reference laboratory or a local or state public health laboratory. Note that testing of specimen types other than sputum must be carefully verified as a laboratory-developed test for off-label usage (225). This rapid test can be performed directly on the specimen or from culture isolates (184, 226). Sequencing methods can be used to target a variety of genes to determine mutations associated with resistance. A review by Brown-Elliott and colleagues (54) provides additional important recommendations and updates. First, submitting and referral laboratories should be familiar with shipping guidelines for infectious substances. Ideally, mycobacteria that have been identified can be referred by using primary liquid cultures (rather than waiting for solid medium, although this can also be sent). There are several reasons for discordant results, including but not limited to the following: the culture is not pure; the isolate itself may consist of subpopulations; comparison of results from different methods. Quality assurance programs and indicators ensure that laboratories monitor and improve their clinical testing services through ongoing analysis and assessment. This section discusses several quality assurance features that laboratories should consider integrating into their quality management program in the mycobacteriology laboratory. Within the quality plan, several parameters should be addressed, including general laboratory systems and preanalytical, analytical, and postanalytical phases of testing. A clear process that addresses the development and use of quality indicators is effectively described in this document, along with other meaningful tools related to process improvement. Specimen Collection A robust quality assurance program begins with adequate specimen collection. It is incumbent on the laboratory to appropriately communicate specimen requirements to the health care provider to ensure the best-quality outcome for the patient. This communication should be regular in some capacity, since providers change and knowledge can be forgotten. Provider instructions are a crucial component to ensure that adequate specimens are collected, labeled, and transported appropriately for processing. Communication with the provider as to which specimens will be rejected is important and should be reinforced on an ongoing basis. It is known that the volume of sputum can directly impact the ability of the laboratory to recover and isolate mycobacteria from a specimen and that submission of a specimen of 3 ml may negatively impact April 2018 Volume 31 Issue 2 e00038-17 cmr. If specimens that are 5 ml are routinely submitted, there should be a mechanism in the laboratory to monitor appropriate specimen collection (see "Acceptable Specimens and Rejection Criteria," above), and the laboratory should consider a quality monitor to assess specimen volume and have a mechanism for provider feedback if specimen requirements are not being followed (103). It is recommended that the provider be notified of unsatisfactory specimens as soon as possible or within 24 h. Instructions to the provider should clearly state that sputum from deep in the respiratory tract is the optimal specimen, as opposed to saliva. Monitoring the number of specimens per patient can also be part of a robust quality assurance program. In larger systems, tracking the numbers of specimens per patient could be onerous unless an electronic mechanism to do so is readily available. Specimen delivery can also be broken down into many segments to monitor how effectively specimens are being transported to the laboratory for processing, especially if the laboratory is in a remote location compared to either the hospital or outpatient facilities. The faster a result is provided to the health care provider, the sooner the patient can be appropriately treated, which will augment patient care, prevent the unnecessary spread of infection to others, and/or allow the patient to be released from isolation sooner (103, 158). Another quality assurance indicator in the mycobacteriology laboratory is providing appropriate feedback to the health care provider. This not only will enhance quality and patient care but also can positively impact the laboratory so that time is not wasted processing inappropriately submitted specimens (243). Since many health care institutions have electronic medical records, direct feedback about specimen rejection via the hospital information system can be a rapid way to educate the provider. Specimen Processing and Decontamination Specimen management is very important across all clinical laboratory disciplines. If these numbers cannot be met, laboratories should consider referring specimens to a reference laboratory for testing. After an extensive review performed in 2000, it was determined that the median false-positive rate due to cross-contamination in the mycobacteriology laboratory was approximately 3. A cross-contamination event not only can result in a patient being treated with an inappropriate course of antibiotics but also can mask the true underlying condition or disease of the patient (245, 246). Laboratory practices should be in place not only to mitigate cross-contamination but also to uncover a contamination event if it occurs. The laboratory understanding of a root-cause analysis can be crucial to investigations related to contamination events (132). There are several steps/processes that can be integrated into the specimenprocessing procedure that will reduce errors associated with cross-contamination. However, the inclusion of a positive control in the processing of patient specimens is discouraged due to the risk of cross-contamination (1). To resolve whether a cross-contamination event has occurred, laboratories can send out the isolates from the single-positive patient and the sentinel (possible source specimen from a known positive patient) for genotyping. This definitive approach can truly make a difference in patient management and improve the quality of testing in the laboratory. An extensive list of measures related to specimen processing and decontamination can be found in the 2013 Association for Public Health Laboratories document Mycobacterium tuberculosis: Assessing Your Laboratory (103). Culture Growth There are several indicators to assess the efficiency of the decontamination and digestion procedures, since these steps ultimately affect organism recovery. Contamination of media for culture growth should be monitored within the mycobacteriology laboratory. Some contamination of culture medium is expected, but a general approximation is that contamination rates are 2 to 5% for solid media and 7 to 8% for liquid media containing antimicrobials (140, 247). Monitoring the contamination rate assists in ensuring that digestion and decontamination procedures are adjusted appropriately (75). If a contamination rate of 5 to 8% is observed, monitoring the time of transport of the specimen to the laboratory may be prudent, as delays in specimen submission may be occurring. However, if the positivity rate decreases compared to anticipated percentages, this might mean that the decontamination procedure is too stringent, resulting in false-negative cultures. All these quality monitors are important for assessing the robustness of the processes and procedures in the mycobacteriology laboratory (103). Mycobacteria can be present in water, and autoclaving does not necessarily destroy the acid-fast properties of an organism. In conclusion, there are several approaches to assessing and monitoring quality within the mycobacteriology laboratory. Consultation with other colleagues is also prudent when looking for new avenues for continuous quality improvement, in addition to many of the references in this section. Table 15 lists several quality monitors that may be appropriate for laboratories that test specimens for mycobacteria, and benchmarks can be found in Table 4. Alternatively, blood may be collected into a mononuclear cell preparation tube and processed within 8 h of collection.
Evidence Summary Patients with a previous attack of cellulitis medicine advertisements , especially involving the legs medications you can give your cat , have annual recurrences rates of about 8%20% [65 67] medicine hat tigers . Edema symptoms zinc deficiency adults , especially lymphedema and other local risk factors such as venous insufficiency treatment 02 binh , prior trauma (including surgery) to the area, and tinea pedis or other toe web abnormalities [6571], increase the frequency of recurrences. Other predisposing conditions include obesity, tobacco use, a history of cancer, and homelessness [66, 67, 71]. Addressing these factors might decrease the frequency of recurrences, but evidence for any such a benefit is sparse. For patients with recurrences despite such efforts, antimicrobial prophylaxis may reduce the frequency of future episodes. Two randomized trials using twice-daily oral penicillin or erythromycin demonstrated a substantial reduction in recurrences among the antibiotic recipients compared to controls [72, 73]. In a study of patients with recurrent cellulitis involving arm lymphedema caused by breast cancer treatment, 2. The duration of therapy is indefinite, and infections may recur once prophylaxis is discontinued. For example, a recent double-blind comparative trial demonstrated that phenoxymethyl-penicillin given as 250 mg Downloaded from cid. Systemic corticosteroids (eg, prednisone 40 mg daily for 7 days) could be considered in nondiabetic adult patients with cellulitis (weak, moderate). Evidence Summary Treating the inflammation in these infections by combining antimicrobial therapy with either a nonsteroidal anti-inflammatory agent (ibuprofen 400 mg 4 times daily [qid] for 5 days) or systemic corticosteroids significantly hastens clinical improvement compared with antimicrobial therapy alone [60, 61]. A randomized, double-blind, placebo-controlled trial involving 108 adult nondiabetic patients, demonstrated that an 8-day course of oral corticosteroids in combination with antimicrobial therapy led to a significantly more rapid clinical resolution of cellulitis (primarily of the legs) than antimicrobial therapy alone [61, 62]. Long-term follow-up of these patients showed no difference in relapse or recurrence [61, 62]. The benefits of systemic corticosteroids in this situation are consistent with their efficacy and safety as adjunctive treatment in other infections [63]. The clinician must ensure that a deeper infection such as necrotizing fasciitis is not present. A brief course of systemic antimicrobial therapy is indicated in patients with surgical site infections following clean operations on the trunk, head and neck, or extremities that also have systemic signs of infection (strong, low). Diagnosis and treatment of organ space infections in the abdomen are discussed in other guidelines. Flat, erythematous skin changes can occur around or near a surgical incision during the first week without swelling or wound drainage. The cause is unknown but may relate to tape sensitivity or other local tissue insult not involving bacteria. Numerous experimental studies and clinical trials demonstrate that antibiotics begun immediately postoperatively or continued for long periods after the procedure do not prevent or cure this inflammation or infection [8188]. Accordingly, fever or systemic signs during the first several postoperative days should be followed by direct examination of the wound to rule out signs suggestive of streptococcal or clostridial infection (see section on necrotizing soft tissue infections and clostridial myonecrosis), but should not otherwise cause further manipulation of the wound. White blood cells may not be evident in the drainage in most clostridial and some early streptococcal infections. Another rare cause of early fever and systemic signs following operation is staphylococcal wound toxic shock syndrome [89, 90]. Fever, hypotension, abnormal hepatic and renal blood studies, and diarrhea are early findings. Appropriate treatment is to open the incision, perform culture, and begin antistaphylococcal treatment. Two contain simple, unreferenced, recommendations to open an infected wound without using antibiotics [96, 98]. Thus, if there is <5 cm of erythema and induration, and if the patient has minimal systemic signs of infection (temperature <38. Studies of subcutaneous abscesses found little or no benefit for antibiotics when combined with drainage [18, 21, 100, 101]. Incision and drainage of superficial abscesses rarely causes bacteremia [102], and thus prophylactic antibiotics are not recommended. The antibiotic choice is usually empiric but can be supported by Gram stain, culture of the wound contents (Table 2), and the site of surgery. If the operation was a clean procedure that did not enter the intestinal or genital tracts, S. Infections following surgical operations on the axilla also have a significant recovery of gram-negative organisms, and those in the perineum have a higher incidence of gram-negative organisms and anaerobes [100, 103, 104]; antibiotic selections should provide coverage for these organisms (Table 3). Infections developing after surgical procedures involving nonsterile areas such as colonic, vaginal, biliary, or respiratory mucosa may be caused by a combination of aerobic and anaerobic bacteria [18, 87, 88, 101]. These infections can rapidly progress and involve deeper structures than just the skin, such as fascia, fat, or muscle (Tables 3 and 4). What Is the Preferred Evaluation and Treatment of Necrotizing Fasciitis, Including Fournier Gangrene These deep infections involve the fascial and/or muscle compartments and are potentially devastating due to major tissue destruction and death. Antibiotics for Treatment of Incisional Surgical Site Infections Surgery of Intestinal or Genitourinary Tract Single-drug regimens Ticarcillin-clavulanate 3. The initial lesion can be trivial, such as a minor abrasion, insect bite, injection site (as in drug addicts), or boil, and a small minority of patients have no visible skin lesion. As it progresses, there is systemic toxicity, often including high temperatures, disorientation, and lethargy. Examination of the local site typically reveals cutaneous inflammation, edema, and discoloration or gangrene and anesthesia. A distinguishing clinical feature is the wooden-hard induration of the subcutaneous tissues. In cellulitis, the subcutaneous tissues are palpable and yielding; in fasciitis the underlying tissues are firm, and the fascial planes and muscle groups cannot be discerned by palpation. A broad erythematous tract is sometimes evident along the route of the infection, as it advances proximally in an extremity. If there is an open wound, probing the edges with a blunt instrument permits ready dissection of the superficial fascial planes well beyond the wound margins. Most infections are community acquired and present in the limbs, with approximately two-thirds in the lower extremities. There is often a predisposing condition, such as diabetes, arteriosclerotic vascular disease, venous insufficiency with edema, venous stasis or vascular insufficiency, ulcer, or injection drug use. Cases of necrotizing fasciitis that arise after varicella or trivial injuries, such as minor scratches or insect bites, are usually due to S. The mortality in patients with group A streptococcal necrotizing fasciitis, hypotension, and organ failure is high, ranging from 30% to 70% [109, 110]. Severe pain may be the initial clinical symptom with little cutaneous evidence due to the deep infection. Polymicrobial infection is most commonly associated with 4 clinical settings: (1) perianal abscesses, penetrating abdominal trauma, or surgical procedures involving the bowel; (2) decubitus ulcers; (3) injection sites in illicit drug users; and (4) spread from a genital site such as Bartholin abscess, episiotomy wound, or a minor vulvovaginal infection. Although many specific variations of necrotizing soft tissue infections have been described based on etiology, microbiology, and specific anatomic location of the infection, the initial approach to diagnosis, antimicrobial treatment, and surgical intervention is similar for all forms and is more important than determining the specific variant. Early in the course, distinguishing between a cellulitis that should respond to antimicrobial treatment alone and a necrotizing infection that requires operative intervention is critical but may be difficult. Necrotizing Fasciitis Necrotizing fasciitis is an aggressive subcutaneous infection that tracks along the superficial fascia, which comprises all the tissue between the skin and underlying muscles [106, 107]. Most of the organisms originate from the bowel or genitourinary flora (eg, coliforms and anaerobic bacteria). However, features that suggest involvement of deeper tissues include (1) severe pain that seems disproportional to the clinical findings; (2) failure to respond to initial antibiotic therapy; (3) the hard, wooden feel of the subcutaneous tissue, extending beyond the area of apparent skin involvement; (4) systemic toxicity, often with altered mental status; (5) edema or tenderness extending beyond the cutaneous erythema; (6) crepitus, indicating gas in the tissues; (7) bullous lesions; and (8) skin necrosis or ecchymoses. The most important diagnostic feature of necrotizing fasciitis is the appearance of the subcutaneous tissues or fascial planes at operation. The fascia at the time of direct visual examination is swollen and dull gray in appearance with stringy areas of necrosis; a thin, brownish exudate may be present. Extensive undermining of surrounding tissues is usually present, and the tissue planes can be readily dissected with a gloved finger or a blunt instrument. Several clinical scoring systems have been proposed, but all of these are more useful for excluding necrotizing soft tissue infections than identifying them. A definitive bacteriologic diagnosis is best established by culture and Gram stain of deep tissue obtained at operation or by positive blood cultures. Cultures of the superficial wound may be misleading because results may not reflect organisms in the deep tissue infection. Direct needle aspiration of an area of cutaneous inflammation may yield fluid for Gram stain and culture. In suspected cases a small, exploratory incision made in the area of maximum suspicion can be useful for excluding or confirming the diagnosis. Gram stains of the exudate will demonstrate the pathogens and provide an early guide to antimicrobial therapy. If a necrotizing infection is present, it will be obvious from the findings described above. If there is no necrosis on exploratory incision, the procedure can be terminated with very little risk or morbidity to the patient. Biopsy for frozen section analysis may also be used to make the diagnosis, but, if enough suspicion exists to do a biopsy, the diagnosis is usually evident on gross inspection without histologic confirmation. Treatment Surgical intervention is the primary therapeutic modality in cases of necrotizing fasciitis and is indicated when this infection is confirmed or suspected. Most patients with necrotizing fasciitis should return to the operating room 2436 hours after the first debridement and daily thereafter until the surgical team finds no further need for debridement. Although discrete pus is usually absent, these wounds can discharge copious amounts of tissue fluid, and aggressive fluid administration is a necessary adjunct. In the absence of definitive clinical trials, antimicrobial therapy should be administered until further debridement is no longer necessary, the patient has improved clinically, and fever has been absent for 4872 hours. Among the many choices is vancomycin, linezolid, or daptomycin combined with one of the following options: (1) piperacillintazobactam, (2) a carbapenem (imipenem-cilastatin, meropenem, and ertapenem), (3) ceftriaxone plus metronidazole, or (4) a fluoroquinolone plus metronidazole (Table 4). Once the microbial etiology has been determined, the antibiotic coverage should be appropriately modified. Necrotizing fasciitis and/or streptococcal toxic shock syndrome caused by group A streptococci should be treated with both clindamycin and penicillin. Clindamycin was found to be superior to penicillin in animal models, and 2 observational studies show greater efficacy for clindamycin than lactam antibiotics [112, 113]. Penicillin should be added because of potential resistance of group A streptococci to clindamycin. Interestingly, in the United States, no resistance to clindamycin was found from invasive strains of group A streptococci in Chicago [117]. As extracellular streptococcal toxins have a role in organ failure, shock, and tissue destruction, neutralization of these toxins theoretically could be beneficial. This variant of necrotizing soft tissue infection involves the scrotum and penis or vulva [121, 122]. Eighty percent of patients have significant underlying diseases, particularly diabetes mellitus. Clinical Features Fournier gangrene usually occurs from a perianal or retroperitoneal infection that has spread along fascial planes to the genitalia; a urinary tract infection, most commonly secondary to a urethral stricture, that involves the periurethral glands and extends into the penis and scrotum; or previous trauma to the genital area, providing access of organisms to the subcutaneous tissues. Bacteriology the pace of infection can begin insidiously or abruptly with fever and pain, erythema, and swelling in the genitalia [121, 122]. As the disease progresses, cutaneous necrosis and crepitus, indicating gas in the soft tissue, may develop. The testes, glans penis, and spermatic cord are typically spared, as they have a separate blood supply. Staphylococcus aureus and Pseudomonas species are sometimes present, usually in mixed culture. Treatment As with other necrotizing infections, prompt, aggressive surgical debridement is necessary to remove all necrotic tissue, sparing the deeper structures when possible. Repeat imaging studies should be performed in the patient with persistent bacteremia to identify undrained foci of infection (strong, low). Antibiotics should be administered intravenously initially, but once the patient is clinically improved, oral antibiotics are appropriate for patients whose bacteremia cleared promptly and those with no evidence of endocarditis or metastatic abscess. Evidence Summary Pyomyositis is the presence of pus within individual muscle groups, caused mainly by S. Presenting findings are localized pain in a single muscle group, muscle tenderness, and fever. The disease typically occurs in an extremity, but any muscle group can be involved, including the psoas or trunk muscles. Initially, it may not be possible to palpate a discrete fluctuance because the infection is deep within the muscle, but the area may have a firm, "woody" feel, along with pain and tenderness. Group A streptococci, Streptococcus pneumoniae, and gram-negative enteric bacteria are other possible etiologic agents [127]. Muscle inflammation and abscess formation are readily noted; other sites of infection such as osteomyelitis or septic arthritis may also be observed or a venous thrombosis detected [130, 131]. A broader spectrum of organisms causes pyomyositis in patients with underlying conditions [126], and empirical coverage with vancomycin plus 1 of the following is recommended: (a) piperacillin-tazobactam, (b) ampicillinsulbactam, or (c) a carbapenem antimicrobial. In the absence of a definitive etiologic diagnosis, broadspectrum treatment with vancomycin plus either piperacillintazobactam, ampicillin-sulbactam, or a carbapenem antimicrobial is recommended (strong, low). Definitive antimicrobial therapy along with penicillin and clindamycin is recommended for treatment of clostridial myonecrosis (strong, low). Evidence Summary Clostridial gas gangrene or myonecrosis is most commonly caused by Clostridium perfringens, Clostridium novyi, Clostridium histolyticum, or Clostridium septicum. Increasingly severe pain beginning within 24 hours at the injury site is the first reliable clinical symptom. The infected region becomes tense and tender, and bullae filled with reddish-blue fluid appear. Gas in the tissue, detected as crepitus or by imaging, is usually present by this late stage. Signs of systemic toxicity, including tachycardia, fever, and diaphoresis, develop rapidly, followed by shock and multiple organ failure. Spontaneous gangrene, in contrast to trauma-associated gangrene, is principally associated with the more aerotolerant C.
Possible intrauterine fetal death [1 treatment tendonitis , 2] Over the past 50 years symptoms before period , there has been a decrease in perinatal mortality from hemolytic disease: from 50 to 25% with exchange transfusions symptoms neuropathy , from 25 to 16% with early delivery treatment viral pneumonia , from 16 to 13% with the introduction of amniocentesis medicine ethics , to 3% or less after the beginning of the application of invasive methods of diagnosis and treatment (cordocentesis, intrauterine transfusion). However, it is not possible to completely prevent the morbidity and mortality of newborns from the hemolytic disease [3, 4]. Arbelaez-Garcia, the antigen-antibody complex that forms in the fetal blood upon receipt of maternal antibodies, can acquire antigenicity properties and cause the enhanced synthesis of immunoglobulins A and M by cells associated with its immunocompetence [1, 6]. However, many questions regarding the immunological aspects of pregnancy remain poorly understood. Developing chronic hypoxic conditions of the fetoplacental complex due to immunological incompatibility lead to the persistent syndrome of secondary placental insufficiency [8]. With isserological incompatibility of the blood of the mother and the fetus, the maturation of the placenta is often disturbed [9]. Untimely diagnosis and inadequate therapy lead to disability of the child due to neurological disorders, somatic disorders, changes in immunological reactivity, fetal death is possible [10, 11,12]. It should be noted that grade 2 anemia was observed two times more often than in the control group. Cardiovascular diseases Epidemic hepatitis Varicose veins Chronic tonsillitis Chr. The same trend was observed for rheumatism, chronic tonsillitis and, acute respiratory viral infections during pregnancy, as an infectious-inflammatory process and also as one of the possible factors of immunization. All these complications of the course of this pregnancy were clinically and instrumentally diagnosed with placental dysfunction in 77. Isosensitization for group factors is not indifferent for a pregnant woman and, as a rule, plays a triggering role in the development of several complications. Manual examination of the uterine cavity for a placental defect, possibly associated with a high percentage of intrauterine infection, was more than two times more likely than the control group. Anemia during pregnancy, urinary tract infection, and thyroid disease was identified as a regional pathology by 24. More than two-thirds of newborns were born in a state of asphyxiation and every second newborn in severe asphyxiation. Thus, premature detachment of a normally located placenta, as the most severe obstetric complication, was observed in almost half of women in labor (48. Manual examination of the uterine cavity regarding a placental defect, possibly associated with a high percentage of intrauterine infection, was more than two times more likely than the control group. Intravenous immunoglobulin in isoimmune haemolytic disease of newborn: an updated systematic review and meta-analysis Arch Dis Child Fetal Neonatal Ed 2014; 99:F325F331. Sabita Basu, Ravneet Kaur, and Gagandeep Kaur // Hemolytic disease of the fetus and newborn: Current trends and perspectives. New possibilities for the treatment of fetoplacental insufficiency // Reproductive health in Belarus. Blood group management & clinically significant antibodies: Rh D negative & Rh D positive women//King Edward Memorial Hospital Obstetrics & Gynaecology. The most terrible outcome of childbirth is a high percentage of perinatal losses, which leads to severe medical and social problems in such women. The course of pregnancy often takes place against the background of anemia, chronic pyelonephritis, thyroid diseases, acute respiratory viral infections, and exacerbation of chronic foci of somatic diseases. Also, pregnancy is complicated by persistent symptoms of the threat of termination of pregnancy on the background of placental dysfunction and intrauterine infection. All of the above, of course, affects the condition of the fetus and the outcome of childbirth, and as a result of this, childbirth often occurs in childbirth, prenatal rupture of membranes, premature detachment of a normally located placenta, and weakness of labor. In connection with which, more often, delivery is resolved promptly, and more often, operational benefits in childbirth (manual examination of the uterine cavity) are used. Anti-M induced severe haemolytic disease of foetus and newborn in a Malay woman with recurrent pregnancy loss//Malaysian J Pathol 2017; 39(1): 73 76. The credentials of Fellow and Associate designations signify that the researcher has gained the knowledge of the fundamental and high-level concepts, and is a subject matter expert, proficient in an expertise course covering the professional code of conduct, and follows recognized standards of practice. The credentials are designated only to the researchers, scientists, and professionals that have been selected by a rigorous process by our Editorial Board and Management Board. Fellows are elected for life through a peer review process on the basis of excellence in the respective domain. Each year, the Open Association of Research Society elect up to 12 new Fellow Members. Career Credibility Exclusive Reputation Designation Get honored title of membership Fellows can use the honored title of membership. Career Credibility Reputation Premium Tools Access to all the premium tools To take future researches to the zenith, fellows receive access to all the premium tools that Global Journals have to offer along with the partnership with some of the best marketing leading tools out there. They can also participate in the same organized by another institution as representative of Global Journal. Career Credibility Financial Early Invitations Early invitations to all the symposiums, seminars, conferences All fellows receive the early invitations to all the symposiums, seminars, conferences and webinars hosted by Global Journals in their subject. Also, they can earn up to 70% of sales proceeds from the sale of reference/review books/literature/publishing of research paper. Career Credibility Exclusive Reputation And Much More Get access to scientific museums and observatories across the globe All members get access to 5 selected scientific museums and observatories across the globe. All researches published with Global Journals will be kept under deep archival facilities across regions for future protections and disaster recovery. The primary objective is to recognize the leaders in research and scientific fields of the current era with a global perspective and to create a channel between them and other researchers for better exposure and knowledge sharing. Members are most eminent scientists, engineers, and technologists from all across the world. Associates are elected for life through a peer review process on the basis of excellence in the respective domain. Each year, the Open Association of Research Society elect up to 12 new Associate Members. Career Credibility Exclusive Reputation Designation Get honored title of membership Associates can use the honored title of membership. Additionally, the profile is also partially maintained by our team for better visibility and citation. Career Credibility Reputation Premium Tools Access to all the premium tools To take future researches to the zenith, fellows receive access to almost all the premium tools that Global Journals have to offer along with the partnership with some of the best marketing leading tools out there. In both the cases, it is mandatory for him to discuss with us and obtain our consent. Career Credibility Financial Early Invitations Early invitations to all the symposiums, seminars, conferences All associates receive the early invitations to all the symposiums, seminars, conferences and webinars hosted by Global Journals in their subject. Financial And Much More Get access to scientific museums and observatories across the globe All members get access to 2 selected scientific museums and observatories across the globe. We usually recommend authors submit their research using any standard format they are comfortable with, and let Global Journals do the rest. Authors who are not able to submit manuscript using the form above can email the manuscript department at submit@globaljournals. Before and during Submission Authors must ensure the information provided during the submission of a paper is authentic. Manuscript submitted must not have been submitted or published elsewhere and all authors must be aware of the submission. Declaration of Conflicts of Interest It is required for authors to declare all financial, institutional, and personal relationships with other individuals and organizations that could influence (bias) their research. Policy on Plagiarism Plagiarism is not acceptable in Global Journals submissions at all. Substantial contributions to the conception and acquisition of data, analysis, and interpretation of findings. Drafting the paper and revising it critically regarding important academic content. Changes in Authorship the corresponding author should mention the name and complete details of all co-authors during submission and in manuscript. We support addition, rearrangement, manipulation, and deletions in authors list till the early view publication of the journal. We also believe in flexible copyright terms where copyright may remain with authors/employers/institutions as well. Acknowledgments Contributors to the research other than authors credited should be mentioned in Acknowledgments. Declaration of funding sources Global Journals is in partnership with various universities, laboratories, and other institutions worldwide in the research domain. Authors are requested to disclose their source of funding during every stage of their research, such as making analysis, performing laboratory operations, computing data, and using institutional resources, from writing an article to its submission. This will also help authors to get reimbursements by requesting an open access publication letter from Global Journals and submitting to the respective funding source. Our professional layout editors will format the entire paper according to our official guidelines. This is one of the highlights of publishing with Global Journals-authors should not be concerned about the formatting of their paper. Global Journals accepts articles and manuscripts in every major language, be it Spanish, Chinese, Japanese, Portuguese, Russian, French, German, Dutch, Italian, Greek, or any other national language, but the title, subtitle, and abstract should be in English. The following is the official style and template developed for publication of a research paper. The names of first main headings (Heading 1) must be in Roman font, capital letters, and font size of 10. The names of second main headings (Heading 2) must not include numbers and must be in italics with a font size of 10. Structure and Format of Manuscript the recommended size of an original research paper is under 15,000 words and review papers under 7,000 words. Review papers are reports of significant research (typically less than 7,000 words, including tables, figures, and references) A research paper must include: a) b) c) d) e) A title which should be relevant to the theme of the paper. A summary, known as an abstract (less than 150 words), containing the major results and conclusions. Resources and techniques with sufficient complete experimental details (wherever possible by reference) to permit repetition, sources of information must be given, and numerical methods must be specified by reference. Design has been recognized to be essential to experiments for a considerable time, and the editor has decided that any paper that appears not to have adequate numerical treatments of the data will be returned unrefereed. Authors should carefully consider the preparation of papers to ensure that they communicate effectively. Papers are much more likely to be accepted if they are carefully designed and laid out, contain few or no errors, are summarizing, and follow instructions. They will also be published with much fewer delays than those that require much technical and editorial correction. The Editorial Board reserves the right to make literary corrections and suggestions to improve brevity. All manuscripts submitted to Global Journals should include: Title the title page must carry an informative title that reflects the content, a running title (less than 45 characters together with spaces), names of the authors and co-authors, and the place(s) where the work was carried out. Author details the full postal address of any related author(s) must be specified. It should be clear and concise and must contain the objective of the paper and inferences drawn. Many researchers searching for information online will use search engines such as Google, Yahoo or others. By optimizing your paper for search engines, you will amplify the chance of someone finding it. Global Journals has compiled these guidelines to facilitate you to maximize the webfriendliness of the most public part of your paper. Keywords A major lynchpin of research work for the writing of research papers is the keyword search, which one will employ to find both library and internet resources. Up to eleven keywords or very brief phrases have to be given to help data retrieval, mining, and indexing. An effective keyword search requires a strategy: planning of a list of possible keywords and phrases to try. One should start brainstorming lists of potential keywords before even beginning searching. Ask, "What words would a source have to include to be truly valuable in a research paper It may take the discovery of only one important paper to steer in the right keyword direction because, in most databases, the keywords under which a research paper is abstracted are listed with the paper. Numerical Methods Numerical methods used should be transparent and, where appropriate, supported by references. Abbreviations Authors must list all the abbreviations used in the paper at the end of the paper or in a separate table before using them. Formulas and equations Authors are advised to submit any mathematical equation using either MathJax, KaTeX, or LaTeX, or in a very high-quality image. Please give the data for figures in black and white or submit a Color Work Agreement form. For scanned images, the scanning resolution at final image size ought to be as follows to ensure good reproduction: line art: >650 dpi; halftones (including gel photographs): >350 dpi; figures containing both halftone and line images: >650 dpi. Color charges: Authors are advised to pay the full cost for the reproduction of their color artwork. Hence, please note that if there is color artwork in your manuscript when it is accepted for publication, we would require you to complete and return a Color Work Agreement form before your paper can be published. Also, you can email your editor to remove the color fee after acceptance of the paper. Choosing the topic: In most cases, the topic is selected by the interests of the author, but it can also be suggested by the guides. This may be done by asking several questions of yourself, like "Will I be able to carry out a search in this area Also, you might have to do a lot of work to find all the rises and falls of the various data on that subject.
Complete all registration information on the response form medications ok during pregnancy , including your name symptoms breast cancer , mailing address medications used to treat migraines , phone number treatment 5th disease , and e-mail address symptoms internal bleeding , if available. Select your answers to the questions, and mark the corresponding letters on the response form. Questions with more than one correct answer will instruct you to "Indicate all that apply. Department of Agriculture; and the Center for Food Safety and Applied Nutrition, Food and Drug Administration. Each physician should claim only those hours of credit that he/she actually spent in the educational activity. The goal of this report is to provide health-care providers with guidance and patient-education materials regarding foodborne illness. After completing this continuing education activity, the reader should be able to 1) differentiate between the six etiologic agents that should be considered regarding manifestations of foodborne illness; 2) describe four criteria to consider when treating a diagnosed foodborne illness; 3) summarize the reporting requirements for foodborne illness; and 4) identify three groups of persons who are at higher risk for foodborne illnesses. To receive continuing education credit, please answer all of the following questions: 1. Which of the following provide important clues to the possible etiology of a food-associated illness Using a food thermometer to check the internal temperature of food before eating it. What is the appropriate method to use in determining if a hamburger is cooked to a proper temperature Determining if a hamburger is cooked to a proper temperature is not necessary because it is too small. When a foodborne outbreak is suspected, who would be a helpful contact at the health department Intentional contamination of food is uncommon, but which of the following would make you suspect that such an act had occurred. Norovirus infection, which often results in nausea, vomiting, and watery/large-volume diarrhea within 2448 hours, can be caused by. Each month, approximately how many patients with a foodborne illness do you treat After reading this report, I am confident I can differentiate between the six etiologic agents that should be considered regarding manifestations of foodborne illness. After reading this report, I am confident I can describe four criteria to consider when treating a diagnosed foodborne illness. After reading this report, I am confident I can summarize the reporting requirements for foodborne illness. After reading this report, I am confident I can identify three groups of persons who are at higher risk for foodborne illnesses. The teaching strategies used in this report (text, figures, and tables) were useful. Remember, you must answer all of the questions to receive continuing education credit! Failure to complete these items can result in a delay or rejection of your application for continuing education credit. Box E-Mail Address Phone Number]B]B]B]B]B]B]B]B]B]B]B]B]B [[[[[[[[[[[[[]C]C]C]C]C]C]C]C]C]C]C]C]C [[[[[[[[[[[[[]D]D]D]D]D]D]D]D]D]D]D]D]D [[[[[]E]E]E []F]E]E or 14. Overall, the presentation of the report enhanced my ability to understand the material. The availability of continuing education credit influenced my decision to read this report. To receive an electronic copy each week, send an e-mail message to listserv@listserv. The reporting week concludes at close of business on Friday; compiled data on a national basis are officially released to the public on the following Friday. The patient was given antibiotics for 14 days, with no improvement, according to her. Due to personal reasons, no follow up was done until she came back after seven months later, with an extensive mass involving all four quadrants of the breast, with nipple invasion. The baby was addressed to pediatrics for a complementary malformation examination. Examination of the placenta was negative, and after three weeks, the patient was sent again to oncology to complete the rest of chemotherapy. She later underwent a modified radical mastectomy, a complement of radiation, and hormonal therapy (tamoxifen) was given. Case 2: Thirty-nine years old patient, with no history of cancer, Gravida 3 Para 3, two vaginal births, with 27 gestational weeks of pregnancy. Seven months before, the patient had noticed (in the left breast) a retro areolar and superior lump associated with skin inflammation. The scan showed aninfiltration of the left mammary gland, with thickened skin associated with pectoral muscle infiltration and multiple axillary nodes with a costal lesion. The patient underwent neoadjuvant chemotherapy consisting of paclitaxel, Adriamycin, and cyclophosphamide. Discussion the diagnosis of breast cancer associated with pregnancy concerns every breast cancer appearing during pregnancy and lactation, and about a year in post-partum [2-3]. Some delay concerning the diagnosis of breast cancer in pregnant patients is frequently caused by changes in breast tissue that occurs during pregnancy [4]. Breast disorders related to pregnancy are usually benign, but because of the seriousness of pregnancy-associated with breast cancer and the risk of a delayed diagnosis, during this period, all masses must be carefully evaluated [5]. Also, the physician must proceed to a careful local and systemic examination as would be done in a non-pregnant woman, followed by an imaging study if a lump is clinically suspected. An initial diagnosis can be made by using breast ultrasound, as this method is considered safe and has high sensitivity and specificity [6]. If there are any suspicious features or ultrasound is not enough, then it is prudent to proceed with bilateral mammography (with abdominal shielding) to exclude bilateral and multicentric disease. Also, mammography is considered safe for the fetus, since the breast radiation around three mGy, so fetal exposure is about 0. In our cases, we especially relayed on ultra-sonography results that were positive. In our case, we used Tru-Cut biopsy, and the results were in favor of invasive ductal carcinoma, as reported in studies showing that 7090% are Invasive ductal carcinoma, followed by invasive lobular carcinoma [8]. The frequency of inflammatory breast cancer is increasing, and the histologic score system (Scarff, Bloom Richardson grading system) is also high. Radiographic examinations for staging purposes should be avoided during pregnancy and used only when the estimated risk of metastatic disease is high, and if the results can change the therapeutic decision. In this situation, a liver ultrasound is recommended if there is any suspicion of liver metastases. According to clinical and imaging examination, the patient can best aged like a non-pregnant woman. The modality of treatment involved surgery associated with adjuvant or neoadjuvant chemotherapy. Mastectomy can be done under general anesthesia and can be performed at any gestational age with minimal risk to the fetus. After 20 weeks, the patient should be positioned with left lateral uterine displacement to avoid aortocaval compression [8]. But preferably in the second and third trimesters, to not delay radiation therapy that can be used until after delivery [8]. Chemotherapy is administered considering gestational age and can be safely initiated during the second and third trimesters. In our oncology institute, anthracyclines, especially cyclophosphamides, Adriamycin with or without 5-fluorouracil are the most commonly used medications. After 35 weeks chemotherapy may result in fetal toxicity increases the chances of spontaneous labor and at the time of delivery some bleeding problems, sepsis, or death may occur. Consequently, the time interval of three weeks is recommended between the last chemotherapy session and the delivery. Our two patients underwent neoadjuvant chemotherapy before modified radical mastectomy. Post-natal, radiotherapy, and hormonal therapy were given depending on the stage and hormone receptor status. Some authors suggest random ultrasonography checkup in each semester of pregnancy with weight evaluation and also fetal doppler [14]. Vaginal delivery is preferred since post-partum anti-neoplastic treatment can be resumed immediately, while at least a one-week interval is recommended after cesarean section. Breastfeeding is generally not recommended during chemotherapy as drugs are excreted in human milk. Also, cyclophosphamide treatment might cause transient neutropenia in the new born. But It becomes possible three weeks after the end of chemotherapy; breastfeeding should not be contraindicated to women who have completed chemotherapy with momentous time before delivery. From the neonatal perspective [16], breastfeeding with contralateral breast after the end of treatment is possible. Regarding fertility, chemotherapy has ovarian toxicity that may cause transitory amenorrhea or even precocial menopause. There are different factors influencing this toxicity, like the age, the type of cytotoxic, the duration of treatment, and accumulated doses [17]. Women must be informed before starting the treatment, of the risk of menopause and the impact on fertility. The oncologic follow-up concerning breast cancer requires a clinical examination, mammography with ultrasonography every 6th to 12 months, for three years, then every year. Before starting a new pregnancy after breast cancer: Liver sonography, chest X-ray, or thoracic, abdominal scan must be realized [18]. In the case of using anthracyclines or trastuzumab in high doses,heart ultrasonography is required because of the high risk of cardiac insufficiency related to pregnancy [19]. The Conception can be accepted 2 or 3 years after treatment or five years when tamoxifen is prescribed (but three months after the end of treatment) [20]. Cancer-associated with pregnancy represents a unique clinical scenario that requires a delicate balance of risks and bene for both fits maternal and fetal well-being, as well as a multidisciplinary discussion and close monitoring by an expert team. The Management of Breast Cancer during Pregnancy in the Maternity Ward of Rabat in Morocco- A Case Report 3. Radiation dose to organs and tissues from mammography: Monte Carlo and phantom study. The safety of lymphatic mapping in pregnant breast cancer patients using Tc-99m sulfur colloid. Breast carcinoma during pregnancy International recommendations from an expert meeting. Trastuzumab administration during pregnancy: A systematic review and meta-analysis. Breast cancer treatment and ovarian failure: risk factors and emerging genetic determinants. Pregnancy after breast cancer: a need for global patient care, starting before adjuvant therapy. Birth preparedness and complication readiness is a comprehensive package which aims at promoting timely access to skilled maternal and neonatal services. Objective: To assess birth preparedness and complication readiness among antenatal women in a tribal area, central zone Kerala. Methodology: this was a community based cross-sectional study carried out in a tribal area during January June 2019 among 60 tribal antenatal women using a questionnaire based interview. Keywords: antenatal women, birth preparedness, complication readiness, cross sectional study, tribal area. Birth Preparedness and Complication Readiness among Antenatal Women in a Tribal Area of a Central District, Kerala Jerry Rachel & Catherin Nisha Abstract- Background: Obstetric complications and maternal deaths following childbirth becomes a burden on many women and their families. It focuses on the active preparation and decision making process in the delivery of pregnant ladies and their families. Methodology: this was a community based cross-sectional Results: the mean age of the antenatal women was 24. Conclusion: In this study birth preparedness was inadequate and the antenatal women are planning to deliver in healthcare facility. Almost two third of the women had the birth of their last child in hospital facility. Introduction bstetric complications and maternal deaths following childbirth becomes a burden on many women and their families(1). Maternal deaths accounts to almost 303,000 in 2015 and most deaths are reported from Sub Saharan Africa (66%) and then from South Asia (22%)(2). Birth preparedness and complication readiness is a comprehensive package Author: Post graduate student. Author: Associate Professor, Department of Community Medicine, Amala Institute of Medical Sciences, Thrissur, Kerala. It focuses on the active preparation and decision making process in the delivery of pregnant ladies and their families(3). The risk of sudden and unpredictable life threatening complications is equal to all the pregnant women. Around the world, different cultural beliefs are practiced and the deficiency in awareness leads to lack of preparation for the delivery and only takes action when the labour begins(4). India has major breakthrough in reducing maternal mortality ratio by 77%, from 556 per 100,000 live births in 1990 to 130 per 100,000 live births in 2016. Kerala performs better in delivery of antenatal check up services than any other states in India(8). World Health Organization state that women in developing countries sustain short term or long term morbidities due to pregnancy and child birth. India being a developing country is in the fore front in carrying the burden of maternal mortality(10). The proposition of birth preparedness and complication readiness in third world countries with substantive illiteracy, incompetent infrastructure, poor transportation, delayed access to medical fraternity have the capacity to reduce the maternal and neonatal mortality and morbidity drastically. Nevertheless, optimum utilization of such services comes from demand by the women and the community.
. Explain generalized anxiety disorder panic disorder and social anxiety. disorder?.
References
- Davis JE. Aesthetics and Reconstructive Otoplasty. New York: Springer-Verlag; 1987; p. 77-87.
- Eri L, Tveter K: A prospective placebo-controlled study of the antiandrogen Casodex as treatment for patients with benign prostatic hyperplasia, J Urol 150:90n94, 1993.
- Wohlgemuth SD, Gaddy MC. Surgical implications of actinomycosis. South Med J 1986; 79: 1574-1578.
- Royster RL, Butterworth JF, Prough DS, et al: Preoperative and intraoperative predictors of inotropic support and long-term outcome in patients having coronary artery bypass grafting, Anesth Analg 72:729, 1991.
- Webster J, Marshall F, Abalalla M, et al: Randomized comparison of percutaneous angioplasty vs. continued medical therapy for hypertensive patients with atheromatous renal artery stenosis. Scottish and Newcastle Renal Artery Stenosis Collaborative Group, J Hum Hypertens 12:329n335, 1998.
- Hsieh C, Chen R, Fang J, et al: Diagnosis and management of bladder injury by trauma surgeons, Am J Surg 184:143n147, 2002.
- Efremidis M, Pappas L, Sideris A, et al. Management of atrial fibrillation in patients with heart failure. J Card Fail 2008;14:232.
- Morris MI, Daly JS, Blumberg E, et al. Diagnosis and management of tuberculosis in transplant donors: a donorderived infections consensus conference report. Am J Transplant 2012; 12: 2288-2300.