
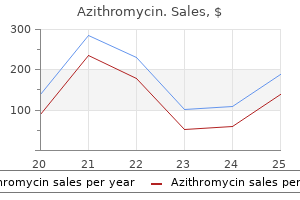
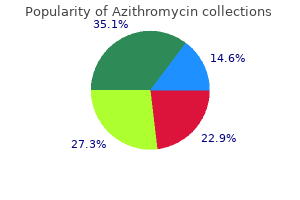
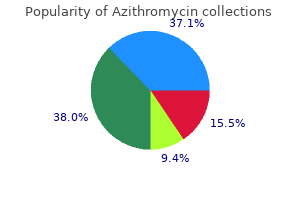
Azithromycin
| Contato
Página Inicial
Joel C. Rosenfeld MD, MEd, FACS
- Associate Clinical Professor of Surgery, University of Pennsylvania School of
- Medicine, Philadelphia, Pennsylvania
- St. Luke? Hospital and Health Network,
- Bethlehem, Pennsylvania
The most obvious one relates to the functions of the male and female sexual organs through which procreation occurs and the survival of the species is assured as well as to behaviors that serve to attract the opposite sex and ultimately lead to mating infection tooth extraction 250 mg azithromycin otc. A more ambiguous meaning has been proposed by some psychol ogists are you contagious on antibiotics for sinus infection effective azithromycin 250 mg, for whom the term is equated with all growth and development bacterial nomenclature purchase azithromycin with visa, the experience of pleasure antibiotics for acne bad for you generic azithromycin 100 mg buy on-line, and survival antimicrobial resistance mechanisms azithromycin 250 mg buy without prescription. Much of now discredited Freudian psychoanalytic theory centers on the sexual development of the child and, on the basis of questionable observations, espouses the view that repression of the sexual impulse and the psychic conflicts resulting therefrom are the main sources of neurosis and possibly psychosis. The timetable of menarche and other aspects of sexual development show considerable variation. If sexu ality is not allowed natural expression, it often becomes a source of worry and preoccupation. Perverse derangements of psychosexual function are another matter entirely and are not addressed here. The vocabulary increases, 18 months the child knows 6 to 20 words; by 24 months, 50 to 200 words; by 3 years, 200 to 400 words. By 4 years, the child is normally capable of telling stories, but with little distinction between fact and imagination. Also by that age, children can indicate spatial and temporal relationships and start to inquire about causality. Here there must be an association of graphic symbols with the auditory, visual, and kinesthetic images of words already acquired. Usually the written word is learned by associating it with the spoken word rather than with the seen object. The integrity of the superior gyrus of the tem poral lobe (Wernicke area) and contiguous parietooccipi tal areas of the dominant hemisphere are essential to the establishment of these crossmodal associations. Writing is learned soon after reading, the audiovisual symbols of words being linked to cursive movements of the hand. The tradition of beginning grade school at 5 or 6 years is based not on an arbitrary decision but on the empirically determined age at which the nervous system of the aver age child is ready to learn and execute the tasks of read ing, writing, and, soon thereafter, calculating. Once language is fully acquired, it is integrated into all aspects of complex action and behavior. Every plan for the solution of a problem must be cast into language, and the final result is analyzed in verbal terms. Anthropologists see in all this a grander scheme wherein the individual recapitulates the language devel opment of the human race. They point out that in primitive peoples, language consisted of gestures and the utterance of simple sounds expressing emotion and that, over periods of time, movements and sounds became the conventional signs and verbal symbols of objects. Historically, signs and spoken language were the first means of human communication; graphic records appeared much later. Native Americans, for instance, never reached the level of syllabic written language. Most psychiatrists exclude from the defi nition of homosexuality those patterns of behavior that are not motivated by specific preferential desire, such as the incidental homosexuality of adolescents and the situ ational homosexuality of prisoners. According to the early reports of Kinsey and colleagues, approxi mately 4 percent of American males are exclusively homosexual and 8 percent have been "more or less exclu 3 years, sometime between the ages of 16 and 65. More recent estimates, both in men and women, range from 1 to 5 percent (see LeVay and Hamer). These widely vari able figures share a problem with all estimates derived from surveys and questionnaires: they cannot count people who do not wish to be counted. Swaab and Hofman have reported that the preoptic zone is three times larger in heterosexual males than it is in females, but it is about the same size in homosexual males as it is in females. If confirmed, these findings, which have been disputed by Byne and others, would support the view that homosexuality has a bio logic basis. Pooled data from mately the covariation of most personality traits: cism versus emotional stability; introversion; (1) neuroti (2) extraversion versus (3) openness to experience versus aver sion to change; (4) agreeableness versus irascibility; and (5) conscientiousness versus unscrupulousness, and all five of these are heritable, as discussed in Chap. By nature, some children from the beginning seem to be happy, cheerful, and unconcerned about immediate frustrations; others are the opposite. By the third month of life, Birch and Belmont recognized individual differences in activity-passivity, regularity-irregularity, intensity of action, approach withdrawal, adaptivity-unadaptivity, high-low thresh old of response to stimulation, positive-negative mood, high-low selectivity, and high-low distractibility. Ratings at this early age were found to correlate with the results of examinations made at age 5 studies in men show that approxi 57 percent of identical twins (and 13 percent of brothers) of homosexual men are also homosexual. Kagan and Moss the inheritance pattern of male homosexuality comes from the maternal side, implicating a gene on the X chro mosome (LeVay and Hamer) but to suggest there is a simple genetic connection is oversimplified. The most widely held current view is that homosexuality is not a mental or a personality disorder, though it may at times lead to secondary reactive disturbances. The stud ies of Kinsey and colleagues indicate that a homosexual orientation cannot be traced to a single social or psycho logic root. Instead, as indicated above, homosexuality seems to arise from a deep-seated predisposition, biologic in origin and as ingrained as heterosexuality. Scarr and associates have also demonstrated the strong genetic influence on personality development. Chapter 51 discusses disorders of personality and the genetic predisposition to certain personality traits further. Involved also are genetic and environmental factors, for one cannot adapt to society except in the presence of other people; i. The roots of social behavior are traceable to certain instinctive patterns that are progres sively elaborated by conditioned emotional reactions. Personality, the most inclusive of all psychologic terms, encompasses the entirety of psychologic traits that dis tinguish one individual from every other. One has but to observe the resemblances between parent and child to confirm this view. Just as no two persons are physi cally identical, not even monozygotic twins, so, too, do they differ in any other refined quality one chooses to measure, particularly those that determine behavior and modes of thinking. Strictly speaking, the normal person is an abstraction, just as is a typical example of any disease. It is in nonphysical attributes that individuals dis play the greatest differences. Here reference is made to their variable place on a scale of energy, capacity for effective work, sensitivity, temperament, emotional responsivity, aggressivity or passivity, risk taking, ethi cal sense, flexibility, and tolerance to change and stress. The sources of these social reactions are even more obscure than those of tem perament, character, and intelligence. In children, difficulty in social adaptation tends first to be manifest by an inability to take their places in a classroom. The development of adult gonadal function and the further evolution of psychosex ual impulses create a bewildering array of new challenges in social adaptation. As social roles change, as intellectual and physical capacities first advance and later recede, new challenges demand new adaptations. The most severe forms of delayed motor development, those associated with spasticity and athe tosis, are usually manifestations of prenatal and perinatal diseases of the brain subsumed under the term cerebral palsy; these are discussed in Chap. In assessing developmental abnormalities of the motor system in the neonate and young infant, the fol lowing maneuvers, which elicit certain postures and reflexive movements, are particularly useful: 1. A loud noise, slapping the bed, or jerking one leg will have the same effect, causing an elevation and abduction of the arms followed by a clasping movement to the midline. This response is present in newborns and infants, it wanes after 2 months and is no longer elicitable after about 5 months of age, and its absence before that time or persistence afterwards indicates a disorder of the motor system. An absent or inadequate Moro response on one side is found in infants with hemiplegia, bra chial plexus palsy, or a fractured clavicle. Persistence of the Moro response beyond 4 or 5 months of age is noted only in infants with severe neurologic defects. The tonic neck reflex consisting of extension of the arm and leg on the side to which the head is passively turned and flexion of the opposite limbs, if obligatory and sustained, is a sign at any age of pyramidal or extrapyramidal motor abnormality. Barlow reports that he has obtained this reflex in 25 percent of devel opmentally delayed infants at 9 to 10 months of age. Fragments of the reflex, such as a brief extension of one arm, may be elicited in 60 percent of normal infants at 1 to 2 months of age and may be adopted spontaneously by the infant up to 6 months of age. As with the Moro response, persistence beyond this age represents a malfunction of the nervous system. The placing reaction in which the foot or hand, brought into contact with the edge of a table, is lifted automatically and placed on the flat surface, is pres ent in all normal newborns. Its absence or asymmetry in infants younger than 6 months of age indicates a motor abnormality. In the Landau maneuver, the infant, if suspended hor izontally in the prone position, will extend the neck and trunk and will break the trunk extension when the neck is passively flexed. This reaction is present by age 6 months; its delayed appearance in a hypo tonic child is indicative of a faulty motor apparatus. If an infant is held prone in the horizontal position and is then dropped toward the bed, an extension of the arms is evoked, as if to break the fall. This is known as the parachute response and is elicitable in most 9-month-old infants. The detection of gross delays or abnormalities of motor development in the neonatal or early infantile period of life is aided little by tests of tendon and plantar reflexes. Arm reflexes are always rather difficult to obtain in infants, and a normal neonate may have a few beats of ankle clonus. However, a consistent extension of the great toe and fanning of the toes on stroking the side of the foot is abnormal at any age. The early detection of cerebral palsy is hampered by the fact that the corticospinal tract is not fully myelinated until 18 months of age, allowing only quasivoluntary movements up to this time. For this reason, a congenital hemiparesis may not be evident until many months after birth. Even then it is manifest only by subtle signs, such as holding the hand in a fisted posture or clumsiness in reaching for objects and in transferring them from one hand to the other. Later, the leg is seen to be less active as the infant crawls, steps, and places the foot. Early hand dominance should always raise the suspicion of a motor defect on the opposite side. In the upper limb, the charac teristic catch and yielding resistance of spasticity is most evident in passive abduction of the arm, extension of the elbow, dorsiflexion of the wrist, and supination of the forearm; in the leg, the change in tone is best detected by passive flexion of the knee. However, the time of appear ance and degree of spasticity are variable from child to child. The stretch reflexes are hyperactive, and the plantar reflex may be extensor on the affected side. With bilateral hemiplegia, the same abnormalities are detect able, but there is a greater likelihood of pseudobulbar manifestations, with delayed, poorly enunciated speech. Later, intelligence is likely to be impaired (in 40 per cent of hemiplegias and 70 percent of bilateral hemiple gias). In diparesis or diplegia, hypotonia gives way to spasticity and the same delay in motor development except that it predominates in the legs. Aside from the hereditary spastic paraplegias, which may become evident in the second and third years, the common causes of weak spastic legs are prematurity and matrix hemorrhages. Developmental motor delay and other abnormalities are present in a large proportion of infants with hypotonia. When the "floppy" infant is lifted and its limbs are pas sively manipulated, there is little muscle reactivity. Hypotonia, if generalized and accompanied by an absence of tendon reflexes, is most often a result of Werdnig-Hoffmann disease (an early life loss of anterior horn cells, a type of spinal muscular atro phy), although the range of possible diagnoses is large and includes diseases of muscle, nerve, and the central nervous system (see Chaps. Under such conditions one does well to deal with the immediate illnesses and defer pronouncements about the status of cerebral function. The brain proves to be simultaneously affected in 25 percent of patients with serious forms of congenital heart disease and an even higher proportion of patients with rubella and coxsackie B viral infections. In a disease such as cystic fibrosis, where the brain is not affected, it is advisable to depend more on the analysis of language development than on assessment of motor function, because muscular activity may be generally enfeebled. The other causes of this type of neonatal and infantile hypotonia include muscular dystrophies and congenital myopathies, mater nal myasthenia gravis, polyneuropathies, Down syn drome, Prader-Willi syndrome, and spinal cord injuries, each of which is described in its appropriate chapter. Hypotonia that arises in utero may be accompanied by congenital fixed contractures of the joints, termed arthro gryposis, as discussed in Chap. Delays in Sensory Development Failure to see and to hear are the most important sensory defects affecting the infant and child. When Infants who will later manifest a central motor defect can sometimes be recognized by the briskness of their tendon reflexes and by the postures they assume when lifted. In the normal infant, the legs are flexed, slightly rotated externally, and associated with vigorous kicking movements. The hypotonic infant with a defect of the motor projection pathways may extend the legs or rotate them internally, with dorsiflexion of the feet and toes. Exceptionally, the legs are firmly flexed, but in either instance relatively few movements are made. When hypotonia is a fore runner of an extrapyramidal both senses are affected, a severe cerebral defect is usually respon sible; only at a later age, when the child is more testable, does it become apparent that the trouble is not with the peripheral sensory apparatus but with the central inte grating mechanisms of the brain. Failure of development of visual function is usually revealed by strabismus and by disorders of ocular move ments, as described in Chap. Any defect of the refrac tive apparatus or the acuity of the central visual pathways results in wandering, jerky movements of the eyes. The optic discs may be atrophic in such cases, but it should be pointed out that the discs in infants tend naturally to be paler than those of an older child. However, involuntary choreic movements usually do not appear in the upper limbs before matures and by In congenital hypo 5 to 6 months of age and often are plasia of the optic nerves, the nerve heads are extremely small. Faulty vision becomes increasingly appar ent in older infants when the normal sequences of hand inspection and visuomanual coordination fail to emerge. With respect to hearing, again there is the difficulty in evaluating this function in an infant. Normally, after a few weeks of life, alert parents notice that the child makes a brisk startle to loud noises and a response to other sounds.
She reports a curious comfort from being tightly swaddled and has a highly developed emotional sensibility to the experiences of cattle antibiotics for acne keloidalis nuchae purchase 100 mg azithromycin free shipping, which has allowed her success in reforming and designing abattoirs generic antibiotics for acne generic 250 mg azithromycin mastercard. It is in the latter group antibiotic resistance mortality order cheap azithromycin, representing the mildest degrees of autism antibiotic yellow tablet 500 mg azithromycin free shipping, that one finds eccentrics antibiotic resistance virulence 500 mg azithromycin order fast delivery, the mirthless, flat personalities, unable to adapt socially and habitually avoiding eye con tact but sometimes possessing certain unusual aptitudes the autistic child is ostensibly normal at birth and may continue to be normal in achieving early behavioral sequences until 18 to 24 months of age. In some instances, the abnormality appears even before the first birthday and the child is identified as different in some way by the mother; or, if there had been a previously autistic child, she recognizes the early behavioral char acteristics of the disorder. Motor developments, on the other hand, pro ceed normally and may even be precocious. Occasionally the onset appears to have a relationship to an injury or an upsetting experience. Regardless of the time and rapidity of onset, the autistic child exhibits a disregard for other persons; this is typically quite striking but can be subtle in milder cases. Little or no eye contact is made, and the child is no more interested in another person than in an article of furniture. Insistence on constancy of environment may reach a point where the patient becomes distraught if even a single one of his posses sions has been moved from its original place and remains distressed until it is replaced. Rutter, who has written extensively on the subject, says that the degree of language impairment and lowered intelligence predicts outcome; those who do not speak by 5 years of age will never learn to speak well. Bolton and Griffiths have made the intriguing observation that autistic traits in patients with tuberous sclerosis correspond to the finding of tubers in the temporal lobe, and DeLong and Heinz point out that patients with seizures from bilateral (but not unilateral) hippocampal sclerosis may fail to develop (or may lose) language ability as well as failing to acquire social skills after a period of normal development, in a manner similar to autism. An increased concentration of platelet serotonin and low serum serotonin is detected in many but not all patients; also, serum oxytocin is reduced. Most of these children are physically normal except for a slightly larger head size, on average, but with no other somatic anomalies. The genetic microdeletions and microduplications described earlier have given few hints as to the biologic cause. The significance of cerebellar vermal changes, reported originally by Courchesne and colleagues, remains uncertain (Filipek). In the few brains examined postmortem, no lesions of any of the conventional types have been found. In 5 brains studied in serial sections by Bauman and Kemper, small ness of neurons and increased packing density were observed in the medial temporal areas (hippocampus, subiculum, entorhinal cortex), amygdala and septal nuclei, and mammillary bodies. In a subsequent review of the neuropathology, Kemper and Bauman concluded that three changes stood out: a curtailment of the normal development of neurons in the limbic system; a decrease in the number of Purkinje cells that appears to be con genital; and age-related changes in the size and number of the neurons in the diagonal band of Broca (located in the basal frontal and septal region), as well as in the cer ebellar nuclei and inferior olive. The latter changes were inferred from studying the brains of autistic children who died at different ages, and they gave the appearance of a progressive or ongoing pathology that continues into adult life. In the typical case, the outcome is bleak, although many less affected children show improvement in social relationships and schoolwork when given a serotonin reuptake inhibitor, sometimes in very small doses (DeLong; Filipek, personal communication). Administration of the peptide secretin had produced a number of anecdotal successes, but this could not be reproduced in controlled studies. In addition, serious behavioral changes such as self-injurious activities, aggression, and severe tantrums have been treated with drugs such as risperidone. These represent a therapeutic advance but, as pointed out by Hollander and colleagues in their review of the drug treatment of autism, the patients studied were selected for the severity and type of their symptoms for which reason these medications cannot be expected to be of help to all autistic individuals. Psychiatric and social counseling may help the family to maintain gentle but firm support of the patient so that he can acquire, to the fullest extent possible, good work habits and a congenial personality. Social factors that contribute to underachieve ment must be sought and eliminated if possible. Well-run institutions are usually better than community homes because they offer many more facilities (medical, educational, recreational). Patients in this group, if stable in temperament and relatively well adjusted to society, can work under supervision, but they rarely become vocationally indepen dent. For the more severely cognitively impaired, special training in hygiene and self-care is the most that can be expected. Whereas the need will be all too apparent in the gravely impaired by the first or second year of life, the less-severely affected are difficult to evaluate at an early age. Aicardi J, LeFebvre J, Lerique-Koechlin A: A new syndrome: Spasm in flexion, callosal agenesis, ocular abnormalities. Bailey A, LeCouteur A, Gottesman A, et al: Autism as a strongly genetic disorder: Evidence from a British twin study. Cellini E, For leo P, Ginestroni A, et al: Fragile X permutation with atypical symptoms at onset. Chlari H: Uber Veranderungen des Kleinhlrns infolge von Hydro cephalie des Grosshirns. Cobb S: Haemangioma of the spinal cord associated with skin naevi of the same metamere. Barker E, Wright K, Nguyen K, et al: Gene for von Recklinghausen neurofibromatosis in the pericentromeric region of chromosome 17. Cowan F, Rutherford M, Groenendaal F, et al: Origin and timing of brain lesions in term infants with neonatal encephalopathy. Cnlange A, Zeller J, Rostaing-Rigattierei S, et al: Neurologic com plications of neurofibromatosis type 296:1602, 2006. Dennis J: Neonatal convulsions: Aetiology, late neonatal status and long-term outcome. Dyken P, Krawiecki N: Neurodegenerative diseases of infancy and Ann Neuro/ 13:351, 1983. Hack M, Taylor G, Klein N, et al: School-age outcomes in ciUldren with birth weight under 750 g. Kalter H, Warkany J: Congenital malformations: Etiologic factors and their role in prevention. Iangiec tasies capillaires cutanee et conjonctivales symetrique a disposi tion naevoide et des troubles cerebelleux. Nissenkorn A, Michelson M, Ben-Zeev B, Lerman-Sagie T: Inborn errors of metabolism. Ounsted C, Lindsay J, Richards P (eds): Temporal Lobe Epilepsy, 1 948-1 986: A Biological Study. Sinha S, Davies J, Toner N, et al: Vitamin E supplementation reduces frequency of periventricular hemorrhage in very pre mature babies. Weber F, Parkes R: Association of extensive haernangiomatous nae vus of skin with cerebral (meningeal) haemangioma, especially cases of facial vascular naevus with contralateral hemiplegia. Wyburn-Mason R: Vascular Abnormalities and Tumors of the Spinal Cord and Its Membranes. Zupan V, Gonzalez P, Lacaze-Masmonteil T, et al: Periventricular leukomalacia: Risk factors revisited. It is also not an entirely satisfactory term med ically, as it implies an inexplicable decline from a previous level of normalcy to a lower level of function-an ambigu ous conceptualization of disease that satisfies neither a clinician nor a scientist. Moreover, it gives no hint as to the fundamental causation of a process and in all likelihood combines a number of mechanisms under cerebral cortex, motor system, extrapyramidal apparatus, or cerebellum, which are representative of the structures that are the targets of damage in this class of disease. The basis of aging changes is also explainable at the neuronal level, but the nature of these alterations is not understood. A fundamental problem is the distinction of these aging deteriorations from degenerative disease. However, their separation is of fundamental importance in diagnosis and therapeutics. One has to reconcile the fact that most degenerative diseases manifest themselves in later life, leading to the tentative conclusion that some aspect of the aging process is entwined with the cellular degenera tions of disease. Moreover, a long-standing uncer tainty pertains to certain degenerative conditions such as Alzheimer disease, which becomes so prevalent in later age as to offer the possibility that the disease is an invari able aspect of aging rather than an acquired perturbation in cellular function. For most degenerative diseases of the nervous system, however, this inevitability of occurrence with aging is clearly not the case. For example, the propor tional incidence of Alzheimer pathologic change decreases continuously from age 1 nondescript term. It would be tempting to attribute all progressive disease of the nervous system that are of unknown cause of cases by germ line genetic changes. All are currently called degenerative, but this nosology may be a transitional diseases of mundane type are caused in a proportion to degeneration. The problem is that many degenerative method of holding a place while awaiting more refined understanding. What is lacking at the moment is a precise subcellular mechanism for cellular loss; that is knowledge that a protein aggregates within or between cells is not equivalent to understanding the cause of an illness. Gowers in 1902 suggested the term abiotrophy to encom pass the degenerative diseases, by which he meant a lack of "vital endurance" of the affected neurons, resulting in their premature death. This concept embodies an unproven hypothesis-that aging and degenerative changes of cells are based on the same process. Understandably, contempo aging the diverse processes of cellular diseases that are rary neuropathologists are reluctant to attribute to simple constantly being revealed by ultrastructural and molecular genetic techniques. It is increasingly evident that many of the diseases included in this category depend on genetic factors. Some appear in more than one member of the same family, in which case they may be properly designated as heredodegenerative. Even more diseases, not differing in any fundamental way from the heredo degenerative ones, occur sporadically; that is as isolated instances but still, genetic factors such as single nucleo tide polymorphisms and copy number variations are often involved in pathogenesis. This polemic regarding aging and degen erative disease is irresolvable and exposes difficulties with meaning of the term "disease. The answer is probably "no," as there are distinctive cellular and subcellular features of degenerative diseases Degeneration is nonetheless used as a clinical and pathologic term that refers to a process of neuronal, myelin, or tissue breakdown, the degradative products of which evoke a reaction of phagocytosis and cellular astrogliosis. What characterizes the degenerative disease as much as the loss of cells is the concentration of damage in functionally related cells, or systems; for example the Much new and essential information has been gained regarding the biologic derangements that lead to neuro nal death and dysfunction as a result of investigating the inherited forms of degenerative diseases. The application of the techniques of molecular genetics to these diseases has given stunning results. This approach holds promise for effective treat ment of what heretofore have been considered progres sive and incurable diseases. It has been proposed that all degenerative diseases be classified according to their genetic and molecular abnor malities. However, when one notes the diversity of patho logic change that may accompany a single, seemingly unitary gene abnormality or, reciprocally, the diversity of genetic defects that may underlie a single phenotype, both clinically and for scientific reasons as mentioned ear lier, but such information is often difficult to obtain. The family may be small or widely scattered, so that the patient is unaware of the health of other members. Furthermore, it may not be realized that an ill ness is hereditary if other members of the family have a much more or much less severe, or a different form of the disorder than the patient. Sometimes only the careful examination of other family members will disclose the presence of a hereditary disease. Also, it should be remembered that familial occurrence of a disease does not necessarily mean that it is inherited, but may indicate instead that more than one member of a fam ily had been exposed to the same infectious or toxic agent. Many symptoms of degenerative disease, while not currently curable, can be alleviated by skillful management. In other words, the practice of creating new disease categories to encompass all the molecular and pathologic changes associated with a particular type of neuronal degeneration offers no great advantage in practice. For example, certain diseases are unified by the deposition of proteins such as tau and have been termed "tauopathies," "synucleinopathies," "amyloidopathies," and so forth. We endorse a more useful clinical approach that is based on an awareness of constellations of clinical features that relate to degeneration of neural systems. Until such time as the causation of the degenerative neu rologic diseases is known, there must be a name and a place for a group of diseases that are united only by the common attribute of gradually progressive disintegration of a part or parts of the nervous system. General Pathologic and Pathogenic Featu res Most of the degenerative diseases, as emphasized in the earlier general comments, are characterized by the selective General Clinical Characteristics of Degenerative D iseases the diseases included in the degenerative category have involvement of anatomically and physiologically related systems of neurons. The selective vulnerability of cer J tain systems of neurons is not an exclusive property of the degenerative diseases; several different processes of known cause have similarly circumscribed effects on the nervous system. Contrariwise, in many degenerative dis eases, the pathologic changes are somewhat less selective and eventually quite diffu se. As one would expect of any pathologic process that is based on the slow wasting and loss of neurons, not only the cell bodies but also their dendrites, axons, and myelin sheaths disappear, unaccompanied by an intense tissue reaction or cellular response. These findings distinguish the neuronal atrophies from other large classes of progressive disease of the nervous system, namely, tumors, infec tions, and processes of inflammatory type. A skillfuly taken l history will reveal that there had been subtle symptoms for some time but had attracted little attention. Whether trauma or other stress can actually evoke or aggravate a degenerative disease is a question that canno t be answered with certainty; at present, evidence to this effect is largely anecdotal. Instead, these degenerative disease processes, by their very nature, appear to develop de novo, without relation to known antecedent events, and their symptom atic expressions are late events in the pathologic process, occurring only when the degree of neuronal loss exceeds the ability of a system to function at a clinically acceptable level. Irreversibility and steady progression of clinical manifestations when measured over periods of months or years is another feature common to the neurodegen erative conditions. However, several of these diseases sometimes display periods of relative stability. Among these mechanism is apoptosis, a term borrowed from embryology to specify the mechanisms that lead to neuronal degeneration. The original meaning of the term refers to a naturally occur ring cell death during development that is driven by the expression of genes over a short period of time. The process of neuronal degeneration is quite different in that it refers to a series of changes in mature neurons that occur over a protracted period of time, leading to cell death and often leaving a discrete glial scar, but not to regional tissue necrosis. In some models of degenerative disease, cell loss involves activation of morphology are not apoptotic in the original sense of the term. It is increasingly apparent that mechanisms other than programme d cell death will prove central to under standing the degenerative diseases, and that the clinical specialized genes, although the time course and cellular the mechanisms by which they interfere with cellular function and potentially cause cell death are major areas of research in the degenerative diseases. Although this is the most elementary mode of classification of naturally occurring phenomena, it is a necessary prelude to diagnosis and scientific study and preferable to a purely genetic or molecular classification. It is certainly an improvement on a haphazard listing of diseases by the names of the neurologists or neuropa thologists who first described them. For reasons given in the introduction to this chapter, this approach remains the most effective in analyzing the problem presented by an individual patient. Syndrome of progressive dementia, other neurologic signs absent or inconspicuous A. Frontotemporal dementias-Pick disease, includ ing behavioral variant, primary progressive apha sias (several types) D.
Ischemic strokes are classified by the underlying cause of the vascular occlusion antibiotic 2012 best buy azithromycin. One of three main processes is usually operative: (i) atherosclerosis with superimposed thrombosis affecting large cerebral or extracerebral blood vessels pipistrel virus azithromycin 250 mg without prescription, (ii) cerebral embolism access virus buy azithromycin once a day, and (iii) occlusion of small cerebral vessels within the parenchyma of the brain antibiotic treatment for sinus infection cheap 500 mg azithromycin with mastercard. There are many other pathologic processes that lead to ischemic brain damage hm 4100 antimicrobial cheap azithromycin 500 mg online, not all associated with occlusion of cerebral vessels, including arterial dissection, infl ammatory conditions such as vasculitis, thrombosis of cerebral veins and dural sinuses, in situ thrombosis of large or small cerebral vessels due to hypercoagulable conditions, vasospasm from any of several mechanisms, unusual types of embolic materials such as fat, tumor, cholesterol, and several unique diseases that involve the cerebral vasculature (see further on). The causes of stroke are so numerous that the listing given in Table 34-1 offers only a guide to the remainder of this chapter. As helpful is knowledge of the major causes of stroke by each epoch of age, particularly in childhood and young adults, a subject taken up in a later section and summarized in Table 34-2. The second broad category consists of hemorrhage, which occurs either within the substance of the brain, intracerebral hemorrhage, or contained within the sub arachnoid spaces and ventricular system, subarachnoid hemorrhage. The causes of the first category are numerous and 778 include chronic hypertension, coagulopathies that arise endogenously or as a result of anticoagulant medications, vascular malformations of the brain, cranial trauma, and hemorrhage that occurs within the area of an ischemic stroke. Subarachnoid hemorrhage has fewer fundamental causes, the most corrunon being the rupture of a develop mental aneurysm arising from the vessels of the circle of Willis, but also includes cerebral trauma and arteriove nous malformations, and rarer processes. In its mildest form, a stroke may consist of a trivial and transient neurologic disorder insufficient for the patient even to seek medical attention. Most embolic strokes occur suddenly and the deficit reaches its peak almost at once. Thrombotic strokes tend to evolve some what more slowly over a period of minutes or hours and occasionally days; in the latter case, the stroke usually progresses in a saltatory fashion, i. In cerebral hemorrhage, also abrupt in onset, the deficit may be virtually static or steadily progressive over a period of minutes or hours, while sub arachnoid hemorrhage is almost instantaneous. It follows that gradual downhill course over a period of several days or weeks will usually be traced to a nonvascular disease. There are, however, many exceptions, such as the additive effects of multiple vascular occlusions and the progression that is caused by secondary brain edema surrounding large infarctions and cerebral hemorrhages. Atherosclerotic thrombosis Transient ischemic attacks Embolism Hypertensive hemorrhage Ruptured or unruptured saccular aneurysm or arteriovenous malformation Arteritis a. Meningovascular syphilis, arteritis secondary to pyogenic and tuberculous meningitis, rare infective types (typhus, schistosomiasis, malaria, mucormycosis, etc. Autoimmune vasculopathies (polyarteritis nodosa, lupus erythematosus), necrotizing arteri tis. Wegener arteritis, temporal arteritis, Takayasu disease, granulomatous or giant cell arteritis of the aorta, and giant cell granuloma tous angiitis of cerebral arteries Cerebral thrombophlebitis: secondary to infection of ear, paranasal sinus, face, etc. Antiphospholipid arteriopathy, plasma C-protein deficiency, and other coaguJopath. Hemiplegia stands as the most typical sign of cerebrovascular diseases, whether in the cerebral hemisphere or brainstem, but there are many other manifestations, occurring in recog nizable combinations. These include paralysis, numbness, and sensory deficits of many types on one side of the body, aphasia, visual field defects, diplopia, dizziness, dysarthria, and so forth. The neurovascular syndromes enable the physician to localize the lesion-sometimes so precisely that even the affected arterial branch can be specified-and to indicate whether the lesion is an infarct or a hemorrhage. This group of diseases has also provided the most instructive approach to localization in neurology. First, the clinician must determine whether the event is a stroke rather than some other process that may have a similar sudden onset, such as migraine, seizure, or syncope. Second, if the event is considered likely to be a stroke Source: Reproduced by permission from Salam- Adams and Adams. In the last decades, extraordinary imaging technol ogy has been introduced that allow the physician to make physiologic distinctions among normal, ischemic, and infarcted brain tissue. Salvageable brain tissue in the acute phase of stroke can be delineated by these methods. To identify such ischemic but not yet infarcted tissue is a maj or goal of modern acute stroke medicine. In particular, diffusion-weighted magnetic resonance imaging has already altered the understanding and management of stroke patients. The introduction of effective treatments for acute stroke has led to greater dependence on these sophis ticated imaging techniques, but the authors believe it remains essential for the neurologist to understand the details of the cerebral vascular anatomy and the corre sponding stroke syndromes for several reasons. In cases in which the imaging does not reveal a stroke, the clinician remains dependent on careful history and neurologic examination. Furthermore, in many parts of the world, imaging techniques are unavailable at the pace necessary to initiate acute treatment. Finally; understand ing the detailed anatomy helps the neurologist under stand how the nervous system functions, lessons which are applicable to many other categories of illness other than stroke. Despite these valuable imaging and therapeutic advances in stroke neurology, three points should be made. First, all physicians have a role to play in the prevention of stroke by encouraging the reduction of risk factors, such as hypertension, smoking, and hyper lipidemia and the identification of signs of potential impending stroke, such as transient ischemic attacks, atrial fibrillation, and carotid artery stenosis. Second, careful clinical evaluation integrated with the newer test ing methods still provides the most powerful approach to this category of disease. Finally, there has been a departure from the methodical clinicopathologic stud ies that have been the foundation of our understanding of cerebrovascular disease. Increasingly; randomized trials involving several hundred and even thousands of patients and conducted simultaneously in dozens of institutions have come to dominate investigative activity in this field. These multicenter trials have yielded highly valuable information about the treatment of a variety of cerebrovascular disorders, both symptomatic and asymp tomatic. Most large studies show only modest or marginal differences between treated and control groups and correspondingly give guidance in large populations. These multicenter studies will be critically appraised at appropriate points in the ensuing discussion. The three criteria by which the stroke is identified should be reemphasized: (1) the temporal profile of the clinical syndrome, (2) evidence of focal brain disease, and (3) the clinical setting. The first distinction is to separate ischemic from hemorrhagic stroke; features that are characteristic of the latter such as headache and vomiting at the onset, rapid progression to coma, and sever hypertension are emphasized in the later section on cerebral hemorrhage. Often, however, the distinction is not so clear because sudden onset of a focal neurologic problem is the core syndrome of both processes. There are few categories of neurologic disease whose temporal profile mimics that of the cerebrovascular disor ders. A seizure may be followed by a prolonged focal deficit (Todd paralysis) but is rarely the initial event in a stroke; the setting in which these symptoms occur and their subsequent course clarify the clinical situa tion. Tumor, infection, inflammation, degeneration, and nutritional deficiency are unlikely to manifest themselves precipitously, although rarely a primary or metastatic brain tumor produces a focal deficit of abrupt onset (see later). In multiple sclerosis and other demyelinative diseases, there may be an abrupt onset or exacerbation of symptoms, but for the most part they occur in a different age group and clinical setting. Conversely, a stroke-like onset of cerebral symptoms in a young adult should always raise a suspicion of demy elinative disease. A stroke developing over a period of several days usually progresses in a stepwise fashion, increments of deficit being added abruptly from time to time. A slow, gradual, downhill course over a period of 2 weeks or more indicates that the lesion is probably not vascular but rather neoplastic, demyelinative, infectious (abscess) or granulomatous, or a subdural hematoma. In regard to the focal neurologic deficits of cerebrovas cular disease, many of the nonvascular diseases may produce symptoms that are much the same, and the diagnosis cannot rest solely on this aspect of the clinical picture. Nonetheless, specific patterns of neurologic signs are so highly characteristic of vascular occlusion-e. Conversely; certain disturbances are hardly ever attributable to ischemic stroke-e. Finally, the diagnosis of cerebrovascular disease should always be made on posi tive data, not by exclusion. A brain tumor, especially a rapidly growing glioblas toma or lymphoma, may produce a severe hemiplegia rapidly. Also, the neurologic deficit caused by cancer metastatic to the cerebrum may evolve rapidly, almost at a stroke-like pace. The presence of the tumor and its effects on the cerebrum may make it difficult for the patient to articulate a clear history. A lack of detailed history may also be respon sible for the opposite diagnostic error, i. Contrariwise, certain manifestations of stroke may be incorrectly interpreted as evidence of some other neu rologic disorder. Headache, at times severe, often occurs as a prodrome of a thrombotic stroke or subarachnoid hemorrhage; unless this is appreciated, a diagnosis of migraine may be made. Dizzy spells, vertigo, vomiting, or brief intermittent lapses of equilibrium as a result of vascular disease of the brainstem may be ascribed to vestibular neuritis, Meniere disease, Stokes-Adams syncope, or gas troenteritis. A strikingly focal monoplegia of cerebral origin, causing only weakness of the hand or arm or foot drop, is not infrequently misdiagnosed as a peripheral neuropathy or plexopathy. The burden of stroke has far wider implications when viewed from an international perspective. In developed countries, stroke mortality is only surpassed by cardiac ischemic diseases and close to equivalent to the cancers collectively (mainly lung cancer) in the most recent Global Burden of Disease study undertaken in 2004. Stroke remains among the five leading causes of death across every income group in most countries in the last comprehensive review by the World Health Organization in 2004. They cause sig nificant physical, emotional, and cognitive disabilities among survivors, accounting for 3. Risk Factors for Stroke this is an area of major public health importance in that several modifiable factors are known to increase the liability to stroke. The most important of these are hyper tension, atrial fibrillation, diabetes mellitus, cigarette smoking, and hyperlipidemia. Others, such as systemic diseases associated with a hypercoagulable state and the use of contraceptives, also contribute, but only in special circumstances. Hypertension is also the most readily recognized factor in the genesis of primary intracerebral hemorrhage. It appears that the stroke-producing poten tial of hypertension is as much the product of heightened systolic pressure, as of diastolic pressure (Rabkin et al). The cooperative studies of the Veterans Administration (see Freis et al) and the report by Collins and associ ates (collating 14 randomized trials of antihypertensive drugs) convincingly demonstrated that the long-term control of hypertension decreased the incidence of both ischemic infarction and intracerebral hemorrhage. It has been found that simple measures such as the use of hydrochlorothiazide for blood pressure control may be, overall, the most effective. The presence of congestive heart failure and coronary atherosclerosis also increases the probability of stroke. As for embolic strokes, the most important risk factors are structural cardiac disease and arrhythmias, mostly atrial fibrillation, which increases the incidence of stroke about 6-fold, and by 18-fold if, as was common in the past, there is also rheumatic valvular disease. Weinberger and colleagues and Roehmholdt and coworkers found diabetic patients to be twice as liable to stroke as age-matched nondiabetic groups. The importance of long-duration cigarette smok ing in the development of carotid atherosclerosis has long been known and was quantitated by Ingall and colleagues. The interactions between diabetes and hyper tension on the one hand, and intracerebral hemorrhage and atherothrombotic infarction on the other, as well as the association of cardiac disease and cerebral embolism, Epidem iology of Cerebrovascu lar Diseases Stroke, after heart disease and cancer, is the third most common cause of death in the United States. Every year there are in the United States approximately 700,000 cases of stroke-roughly 600,000 ischemic lesions and 100,000 hemorrhages, intracerebral or subarachnoid-with 1 75,000 fatalities from these causes combined. Since 1950, coincident with the introduction of effective treatment for hypertension, there has been a substantial reduction in the frequency of stroke. During this period, the incidence of coronary artery disease and uncontrolled hyperten sion also fell significantly. In the last two decades, according to the American Heart Association, the mortality rate from stroke has declined by 12 percent, but the total number of strokes may again be rising. Stroke assumes importance both because of its high rate of mortality and the residual disability that it causes. Numerous clinical trials have also shown a marked reduction in stroke incidence with the use of cholesterol-lowering drugs. Subsidiary factors, such as low potassium intake and reduced serum levels of potassium, are associated with an increased stroke rate in several studies, including one in which we participated, but the mechanism of this effect is obscure (Green et al); a detri mental effect on blood pressure is possible. Public health measures designed to detect and reduce the aforemen tioned risk factors offer the most intelligent long-range approach to the prevention of cerebrovascular disease. Finally, in keeping with the emerging field of genetic risk factors in human disease, several genetic loci have been found that putatively impart a risk of stroke in various populations. The largest of these, reported by Ikram and associates, has implicated a polymorphism on chromo some 12, encompassing several genes that have putative connections to vascular disease. However, other groups, such the International Stroke Genetics Consortium, were unable to confirm this. It seems likely that more refined definitions of stroke subtypes and careful genotyping of circumscribed populations will be necessary if genetic risk factors for stroke are to be be found that are not sim ply markers for vasculopathy, inducing diseases such as diabetes, hyperlipidemia, and hypertension. This is a starkly different profile from the abrupt onset of stroke that characterizes the embolic mech anism discussed further on. In thrombosis, a partial stroke may occur and even recede temporarily for several hours, after which there is rapid progression to the completed deficit-or several fleeting episodes may be followed by a longer one and, hours or a day or two later, by a major or only one part, such as a limb or one side of the face, the other parts becoming involved serially in step-like fashion until the stroke is fully developed. Sometimes the deficit is hand or arm or dimness of vision, lasting 5 to 10 min, occur spontaneously or are brought on by standing or walking. Several parts of the body may be affected at once Each of the partial attacks may reproduce the profile of In other words, the principle of intermittency seems to characterize the thrombotic process from beginning to end. Also characteristic of atherothrombotic events in many, but not all cases, is the occurrence of the stroke during sleep; the patient awakens paralyzed, either during the night or in the morning. Unaware of any difficulty, he may arise and fall helplessly to the floor with the first step. This is the story given by half of our patients with thrombotic strokes, as well as by a smaller number with embolic strokes. Most deceptive are the few instances, in which the neurologic disorder evolves very gradually, over several days or longer ("slow stroke"). This error can usually be avoided by a careful analysis of the course of the illness, which will disclose an uneven, saltatory progression. There are also cases-and these are usually instances of pure motor hemiplegia-in which the evolution of a thrombotic stroke is evenly progressive over a period of days. It is likely also that the abrupt development of a thrombus on an atherosclerotic plaque in a distal cerebral vessel (beyond the circle of Willis) can also cause a fairly sudden or at least rapid evolution of stroke, but this is not characteristic.
Azithromycin 250 mg order with amex. Kirby Bauer Antibiotic Testing Method: Microbiology.
References
- Dimauro S, Lamperti C. Muscle glycogenoses. Muscle Nerve 2001; 24: 984n99.
- Potter EL: Bilateral renal agenesis, J Pediatr 29:68n76, 1946. Potter EL: Facial characteristics of infants with bilateral renal agenesis, Am J Obstet Gynecol 51:885n888, 1946. Potter EL: Pathology of the fetus and the newborn, Chicago, IL, 1952, Year Book. Potter EL: Bilateral absence of ureters and kidneys: a report of 50 cases, Obstet Gynecol 25:3n12, 1965.
- Weir IH, Muller NL, Chiles C, et al. Wegener's granulomatosis: findings from computed tomography of the chest in 10 patients. Can Assoc Radiol J 1992;43(1):31-4.
- Sinclair AM, Isles CG, et al. Secondary hypertension in a blood pressure clinic. Arch Intern Med 1987;147(7):1289-1293.
- Kendler KS, Myers J, Zisook S. Does bereavement-related major depression differ from major depression associated with other stressful life events? Am J Psychiatry 2008;165(11):1449-55.
- Stein EA, Ballantyne CM, Windler E, et al. Efficacy and tolerability of fluvastatin XL 80 mg alone, ezetimibe alone, and the combination of fluvastatin XL 80 mg with ezetimibe in patients with a history of muscle-related side effects with other statins. Am J Cardiol. 2008;101:490-6.
- Romao RL, Figueroa V, Salle JL, et al: Laparoscopic ureteral ligation (clipping): a novel, simple procedure for pediatric urinary incontinence due to ectopic ureters associated with non-functioning upper pole renal moieties, J Pediatr Urol 10(6):1089n1094, 2014.
- Wahlund, K. (2003). Temporomandibular disorders in adolescents. Epidemiological and methodological studies and a randomized controlled trial. Swedish Dental Journal Supplement, (164), 2n64.