
Caduet
| Contato
Página Inicial
Richard A. Harrigan, MD
- Professor, Department of Emergency Medicine, Temple University,
- Philadephia, PA, USA
This includes development of end-stage organ damage cholesterol good foods caduet 5 mg free shipping, possible seizure does cholesterol medication make you tired discount 5 mg caduet fast delivery, stroke cholesterol tea order 5 mg caduet mastercard, or renal failure and obstetrical complications including fetal growth restriction cholesterol not bad purchase caduet with a visa, preterm delivery cholesterol medication and vitamins buy caduet 5 mg otc, placental abruption, and stillbirth. Prognosis for treated patients r Even when adequately treated, there is a risk of recurrent preeclampsia and related complications in subsequent pregnancies and long-term maternal health risks. Follow-up tests and monitoring r In subsequent pregnancies, lab assessment of renal and liver function and level of proteinuria should be evaluated early and repeat as the clinical situation warrants. Emergent therapy for acute-onset, severe hypertension during pregnancy and the postpartum period. Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. Source American College of Obstetricians and Gynecologists Date/full reference American College of Obstetricians and Gynecologists, Task Force on Hypertension in Pregnancy. American College of Obstetricians and Gynecologists Preeclampsia/Eclampsia 19 International society guidelines Title Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. Evidence Type of evidence Multicenter, randomized placebo-controlled trial Title and comment Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate Comment: this trial demonstrated that magnesium sulfate reduces the risk of eclampsia by half without harmful maternal/fetal effects. Randomized, placebo-controlled trial Magnesium sulfate in women with mild preeclampsia: a randomized controlled trial. Comment: this trial showed that use of magnesium sulfate did not impact disease progression in women with preeclampsia without severe features. Comment: this trial showed that for women who have nonsevere hypertension at 3437 weeks gestation, immediate delivery might reduce small risk of maternal outcomes at expensive of increasing neonatal respiratory distress syndrome. Expectant monitoring until 37 weeks can therefore be justified until clinical situation deteriorates. Comment: this meta-analysis performed in 2015 of individual patient data from 75°000 women with preeclampsia found that 16% developed recurrent preeclampsia and 20% developed hypertension in a subsequent pregnancy. Comment: this meta-analysis demonstrated that women with a history of preeclampsia/eclampsia double their risk of future cerebrovascular disease and cardiovascular mortality. Comment: this meta-analysis showed that in women at high risk for development of preeclampsia, the maximal effect of aspirin occurs with initiation < 16 weeks gestation and the effect is dose dependent (with studies showing a dose of up to 150 mg associated with greater reduction in risk of preeclampsia and fetal growth restriction as compared to lower doses). The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. Those screening positive then undergo a 100 g 3-hour fasting diagnostic glucose tolerance test. They should be monitored with glucose fingersticks every morning fasting and 1 hour postprandial. If fingersticks are well controlled (generally <95 fasting and <140 postprandial), the patient can be managed for the duration of her pregnancy with tight diet control. There is no threshold at which clinicians should initiate medical management, whether with oral or injectable medication. Oral medication is often used initially for patients given the greater ease of use. Glyburide and metformin are increasingly used, though they have not been approved by the Food and Drug Administration for this indication. Often, patients who require increasing doses of medication based on their glycemic logs will continue to need higher doses of oral medication, be switched to insulin, or require higher doses of insulin as their insulin resistance increases throughout the third trimester. This timing may also decrease the risk for shoulder dystocia compared to later delivery. Postpartum screening and management is recommended for women with gestational diabetes. Should this be suspected, hospitalization and management with a multidisciplinary team including endocrinology and maternal-fetal medicine is warranted. Managing the hospitalized patient r Fingerstick testing should continue to be performed, including fasting and 1 hour postprandial. Table of treatment Treatment Conservative Medical Comments Dietary control; initial therapy for all patients, continued therapy in patients meeting glucose goals Glyburide 2. Psychological Prevention/management of complications r Noncompliance patients who are noncompliant with fingersticks, medications, or visits may warrant r Prevention of further obstetric/fetal complications is achieved through regular testing starting at 32 weeks among women who are controlled with medication. These women are also delivered by 39 weeks gestation (vs 41 weeks gestation for those who are diet controlled). Variation in prevalence of gestational diabetes mellitus among hospital discharges for obstetric delivery across 23 states in the United States. The economic burden of elevated blood glucose levels in 2012: diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Fraction of gestational diabetes mellitus attributable to overweight and obesity by race/ethnicity, California, 20072009. Impact of twin gestation and fetal sex on maternal risk of diabetes during and after pregnancy. Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. American College of Obstetricians and Gynecologists 2015; Centers for Disease Control and Prevention 2020 Etiology r Each viral infection in pregnancy is caused by a unique organism, which leads to characteristic maternal and fetal clinical manifestations. Fetal: Intrauterine growth restriction, polyhydramnios, nonimmune hydrops fetalis, periventricular calcifications, echogenic bowel, microcephaly, hepatic calcifications, enlarged cisterna magna. Neonatal: Sensorineural hearing loss, hepatosplenomegaly, chorioretinitis, periventricular intracranial calcifications, thrombocytopenia, microcephaly, intellectual disability. Maternal: Reticular truncal rash ("erythema infectiosum") and peripheral arthropathy; 20% of adults are asymptomatic. Maculopapular erythematous rash starting on the face and spreading to trunk and extremities. Neonatal: Congenital cataracts, cardiac malformations, radiolucent bone disease, sensorineural hearing loss, extramedullary hematopoiesis ("blueberry muffin" lesions). Maternal: Viral prodrome (high fever up to 105°F, malaise) with conjunctivitis, coryza, and cough. Pregnant women are at increased risk of hospitalization and pneumonia, diarrhea, and encephalitis. Fetal: Spontaneous abortion, stillbirth, low birth weight, preterm birth Neonatal: Rash within 10 days of birth, wide spectrum of disease Maternal: Up to 60% asymptomatic. Acute retroviral syndrome (fever, lymphadenopathy, pharyngitis, maculopapular rash, myalgia/arthralgia, weight loss, headache), mucocutaneous ulcers. Maternal: Painful genital ulcers, dysuria, fever, tender inguinal lymphadenopathy, headache, myalgias, urinary retention. Neonatal: Thrombocytopenia, mucocutaneous vesicles or scarring, transaminitis, conjunctivitis, hypotension, jaundice, disseminated intravascular coagulation, apnea. An abdominal examination is necessary to identify hepatic tenderness or hepatomegaly with acute hepatitis infection. Potential pitfalls/common errors made regarding diagnosis of disease is laboratory based. Treatment Treatment rationale r Many viral illnesses in pregnancy are self-limited and only supportive care is required. First-line treatment of hepatitis B in pregnancy is tenofovir disoproxil fumarate, a nucleotide reverse transcriptase inhibitor. Hepatic function and hepatitis viral load should be monitored with tenofovir treatment for hepatitis B. Pretreatment monitoring of hematologic parameters, renal function, and metabolic status may be indicated. Serial obstetric ultrasounds for fetal growth and to evaluate for congenital infections/anomalies are recommended with acute infection during pregnancy. Antiviral medications may be used to decrease vertical transmission of hepatitis B, varicella, and herpes simplex. Natural history of untreated disease r Most viral illnesses in pregnancy are self-limited and will resolve with supportive care only. Prognosis for treated patients r Maternal prognosis is good for self-limited viral infections in pregnancy. Cytomegalovirus, parvovirus B19, varicella zoster, and toxoplasmosis in pregnancy. Viral Infections and Pregnancy 35 Suggested websites Centers for Disease Control and Prevention. It is associated with risk of bleeding, which can be massive and life threatening and patients are counseled to practice pelvic rest and contact their providers in case of bleeding. Cesarean delivery is required for patients diagnosed with placenta previa that does not resolve. This disorder is further subclassified based on the degree of invasion of the placenta. Placenta accreta describes a placenta that is abnormally adherent to the uterine myometrium. Placenta percreta describes a placenta that invades through the myometrium and serosa of the uterus and possibly into adjacent organs such as the bowel or bladder. Attempts to detach the placenta from the uterine wall can cause life-threatening hemorrhaging so often a cesarean hysterectomy is performed at time of delivery. It may also present with painless vaginal bleeding thought to be caused by cervical dilation or expansion of the lower uterine segment, both of which can disrupt the placental attachment. Screening r Placenta previa: Placentas are localized during routine ultrasounds performed during pregnancy for assessment of fetal anatomy or gestational age. If placental location is unknown, ultrasound should be considered in any woman who presents after 20 weeks gestation with vaginal bleeding. Primary prevention r Cesarean delivery and other intrauterine surgical procedures have been shown to be associated with abnormal placentation such as a previa or accreta, therefore avoiding these surgeries may help decrease the chance of having an abnormal placenta. Magnetic resonance imaging may be used to supplement ultrasonography in determining the placental boundaries and presence or absence of invasion into maternal tissue. Differential diagnosis Differential diagnosis Placental abruption Features A portion of the placenta prematurely detaches causing abdominal pain and bleeding, placenta not overlying the cervical os, may see fetal distress on monitoring or contractions Fetal blood vessels course over the cervical os, may cause bleeding that is life threatening to the fetus Vasa previa Typical presentation r Often placenta previas are asymptomatic. If associated with a placenta previa, the accreta may cause painless bleeding in the second or third trimester. The main clinical presentation is at the time of delivery when the placenta does not cleanly detach from the uterus after delivery of the neonate and can lead to massive hemorrhage. Physical examination r Placenta previa: Clinicians should avoid digital vaginal exam if placenta previa is suspected. Disease severity classification r Any placenta that is morbidly adherent to the uterus by invading into the uterine wall is described as a placenta accreta. There are further subcategories of placenta accreta that describe how invasive the placenta is. Placenta increta describes a placenta that invades only into the myometrium, whereas a placenta percreta describes a placenta that invades through the myometrium and serosa of the uterus and possibly into adjacent organs such as the bowel or bladder. List of imaging techniques r Placenta previa: Transvaginal ultrasound is sufficient for diagnosing placenta previa. Magnetic resonance imaging may be useful if ultrasonography is inconclusive or to better delineate the extent of placental invasion, especially if adherent to the posterior uterus that may be difficult to assess on ultrasound. Potential pitfalls/common errors made regarding diagnosis of disease nancy at the uterus grows and placenta remodels. If the antenatal course is not complicated by bleeding, a planned cesarean delivery is usually performed between 36 and 37 weeks. Surgical planning with a multidisciplinary team of maternalfetal medicine specialists, anesthesiologists, neonatologists, and other surgeons should be performed. If placenta accreta is diagnosed prenatally, a planned cesarean delivery should occur between 34 and 36 weeks. The usual treatment is cesarean hysterectomy; however, uterine conservation with delayed removal of the placenta is possible if massive hemorrhage is not occurring and the patient is a good candidate for such conservative management. Once proven to be stable without additional bleeding, they may be discharged home. If these patients experience a second bleed, many clinicians opt to keep the patients hospitalized until delivery. Managing the hospitalized patient r Patients hospitalized with placenta previas or accretas should be treated as preoperative patients until deemed stable. Once a patient has proven to be stable without further vaginal bleeding, she can usually resume normal activities such as having a normal diet, ambulating and having intermittent fetal and contraction monitoring. If the fetus is < 34 weeks gestational age, a course of betamethasone is given for fetal lung maturity in the event premature delivery is indicated. If a placenta previa causes a life-threatening hemorrhage or the fetus shows signs of distress, cesarean delivery is indicated. Otherwise, a planned cesarean delivery should take place between 36 and 37 weeks gestation. Morbidly adherent placenta Treatment Conservative Comments After cesarean delivery, a placenta may be left in situ to avoid hysterectomy. Caution should be taken as a placenta left in situ may cause delayed life-threatening hemorrhage, resulting in emergent surgery and hysterectomy. A planned cesarean hysterectomy from 34 to 36 weeks is recommended and ideally takes place in a tertiary care center with a multidisciplinary team and intensive care unit in the event of massive hemorrhage. Interventional radiology may place intravascular balloon catheters into the internal iliac arteries prior to cesarean delivery to decrease perfusion of the uterus after delivery. Maternal mortality related to a placenta previa is estimated to be less than 1% in countries with adequate medical resources. The association of placenta previa with history of cesarean delivery and abortion: a metaanalysis. Balloon occlusion of the hypogastric arteries in the management of placenta accreta: A case report and review of the literature. Although some degree of nausea/vomiting, constipation, and heartburn is experienced by a majority of women, fewer women will experience chronic debilitating or life-threatening disease.
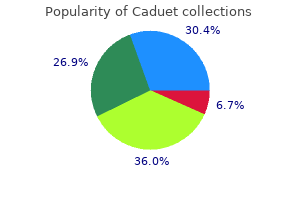
The prevalence of each of the variations cholesterol medication powder order genuine caduet on-line, expressed as percentage of adult patients cholesterol medication in the news purchase caduet line, is provided for each variant quest cholesterol test quality 5mg caduet. Whole-brain oxygen consumption (50 mL/min) represents approximately 20% of total body oxygen utilization cholesterol readings chart nz buy caduet 5 mg mastercard. The cell population of the brain is also heterogeneous in its oxygen requirements cholesterol chart for males discount caduet 5mg amex. The maximum reduction occurs with the dose that results in electrophysiologic silence. At this point, the energy utilization associated with electrophysiologic activity has been reduced to zero, but the energy utilization for cellular homeostasis persists unchanged. Even within the range over which autoregulation normally occurs, a rapid change in arterial pressure will result in a transient. However, the space constraints imposed by the noncompliant cranium and meninges require that blood flow not be excessive. These mechanisms, which include myogenic, chemical, and autonomic neural factors, are listed in Table 11. Note that there is considerable intersubject variation in the limits of the autoregulatory plateau; the extent of this variation is depicted by the arrows. The autoregulatory curve should not be considered fixed and static but as a dynamically changing response to the cerebral circulation to changes in blood pressure. The limits of autoregulation and the autoregulatory plateau are conceptual frameworks for the purpose of analysis. The precise mechanisms by which autoregulation is accomplished and its overlap with neurovascular coupling are not known. Their processes make contact with neurons, and these processes may serve as conduits for the coupling of increased neuronal activity to increases in blood flow. Oxygen modulates the relative contribution of these pathways, and in the setting of reduced oxygen tension at the tissue level, the release of adenosine can contribute to vascular dilation. The net result therefore on vascular tone is determined by the relative contribution of multiple signaling pathways. These neurotransmitters may also potentially be involved in neurovascular coupling. They involve a complex physiologic process regulated, not by a single mechanism, but by a combination of metabolic, glial, neural, and vascular factors. Synaptic activity leads to glutamate release, activation of glutamatergic receptors, and calcium entry in neurons. However, above 42°C, a dramatic reduction in cerebral oxygen consumption occurs, an indication of a threshold for a toxic effect of hyperthermia that may occur as a result of protein (enzyme) denaturation. Anesthesia and the brain: clinical, functional, metabolic, and vascular correlates. The cerebrovascular responsiveness to Paco2 is influenced significantly by blood pressure. Hypercarbia induces cerebral vasodilation and, consequently, the autoregulatory response to hypertension is less effective. Consequently, a patient who has had a sustained period of hyperventilation or hypoventilation deserves special consideration. The mechanisms mediating cerebral vasodilation during hypoxia may include neurogenic effects initiated by peripheral and neuraxial chemoreceptors, as well as local humoral influences. A reduction in arterial oxygen content, and therefore cerebral oxygen delivery, can be achieved either by a reduction in Pao2 (hypoxemic hypoxia) or by a reduction in hemoglobin concentration (anemia, hemodilution). The response to hypoxia is synergistic with the hyperemia produced by hypercapnia and acidosis. An extracranial sympathetic influence via the superior cervical ganglion, as well as parasympathetic innervation via the sphenopalatine ganglion, certainly exists in animals. The intraaxial pathways likely result from innervation arising from several nuclei, including the locus coeruleus, the fastigial nucleus, the dorsal raphe nucleus, and the basal magnocellular nucleus of Meynert. During shock, a sympathetically mediated vasoconstrictive effect shifts the lower end of the autoregulatory curve to the right. The nature and influence of such pathways in humans are not known, and their manipulation for the purposes of clinical management remains to be systematically investigated. However, this may result not only from a reduction in viscosity but also as a compensatory response to reduced oxygen delivery. In patients with focal cerebral ischemia, a hematocrit of 30% to 34% will result in optimal delivery of oxygen. However, manipulation of viscosity in patients with acute ischemic stroke is not of benefit in reducing the extent of cerebral injury. Therefore, viscosity is not a target of manipulation in patients at risk as a result of cerebral ischemia, with the possible exception of those with hematocrit values higher than 55%. The currently available data, however, indicate that this view is now outmoded and is in need of revision. Cardiac output in turn is dependent on adequate circulatory volume, cardiac preload, contractility, afterload, and heart rate and rhythm. Arterial blood gas tensions affect vasomotor tone, and both hypercarbia and hypoxia attenuate autoregulation. The contribution of the sympathetic nervous system is of importance in the cerebrovascular response to hypertension. At the same time, sympathetic nerves reduce the vasodilatory capacity of the cerebral vessels during hypotension. Anesthetics modulate autoregulation by a number of means, including suppression of metabolism, alteration of Cardiac output neurovascular coupling to a higher flowmetabolism ratio, suppression of autonomic neural activity, and by direct effect on cerebral vasomotor tone, and alteration of cardiac function and systemic circulatory tone. Given the multitude of factors that determine the capacity of the cerebral circulation to respond to changes in perfusion pressure, the premise that cerebral autoregulation is static is now untenable. Rather, cerebral autoregulation should be viewed as a dynamic process and that the morphologic form of the autoregulatory curve is the result of the integration of all the variables that affect cerebrovascular tone in an interdependent manner. Anesthetic agents in particular affect autoregulation at multiple levels: suppression of metabolism, alteration in arterial blood gas tensions, direct cerebral vasodilation, suppression of autonomic activity, and modulation of cardiovascular function. There is considerable variation in lower and upper limits as well as the plateau of the autoregulatory curve. The autoregulatory curve depicted in blue was derived from 48 healthy human subjects. Paco2, Arterial partial pressure of carbon dioxide; Pao2, arterial partial pressure of oxygen. These data are consistent with the premise that the capacity of the cerebral circulation to adapt to increases in blood pressure is considerably greater than adaptation to hypotension. Selection of the target range based on the baseline pressure, after due consideration of comorbid conditions that may impact cerebrovascular and cardiovascular performance, may be preferable. In attempts to maintain adequate perfusion pressure, the traditional approach of systemic vasoconstriction, for example with 1-agonists, is reasonable. However, the adequate maintenance of circulatory volume and of cardiac output should also be considered; administration of agents that can also increase cardiac output may be of value. This may be of particular relevance in patients with compromised cardiac function. Catecholamine Agonists and Antagonists Numerous drugs with agonist and antagonist activity at catecholamine receptors (1, 2, 1, 2, and dopamine) are in common use. A drug may have direct effects on cerebral vascular smooth muscle or indirect effects mediated by the cerebral autoregulatory response to changes in systemic blood pressure (or both types of effects). Collectively, these data suggest that norepinephrine and phenylephrine maintain cerebral perfusion. The actions of anesthetics are discussed in the "Effects of Anesthetics on Cerebral Blood Flow and Cerebral Metabolic Rate" section. In the absence of direct measurement of brain tissue oxygenation, a modest reduction in Sco2 in the face of increasing arterial blood pressure cannot be taken as evidence of impairment of cerebral oxygenation. In addition, phenylephrine did not decrease SjVo2, a more global measurement of cerebral oxygenation. Although unlikely, the concern is that 1-agonists might reduce cerebral perfusion in the injured brain. This class of drugs includes dexmedetomidine and clonidine, with the latter being a significantly less specific and less potent 2-agonist. However, the well-known effect of dexmedetomidine in decreasing arterial blood pressure merits careful consideration if used in patients who are critically dependent on collateral perfusion pressure, especially in the recovery phase of an anesthetic. In two investigations in humans, propranolol, 5 mg intravenously,43 and labetalol, 0. Vasoconstriction of the cerebral circulation is not observed even when dopamine is administered in doses of up to 100 g/kg/min. The administration of fenoldopam leads to systemic vasodilation and a decrease in arterial blood pressure. Cerebral vessels are richly endowed with calcium channels, in particular the L-type calcium channel. Its use in both the cardiac and neurologic patient populations has increased significantly given its rapid titratability. In the surgical setting and in the neurocritical care unit, these drugs are administered to control arterial blood pressure acutely. Dendrite branching and volume decrease progressively, and the number of dendritic spines is reduced by approximately 25% to 35%. Ketamine Midazolam Diazepam Remifentanil Sufentanil Fentanyl Morphine Etomidate Propofol Thiopental -80 -60 0. The data are derived from human investigations and are presented as percent change from nonanesthetized control values. Barbiturates, for example, cause relaxation of isolated cerebral * Note a well-entrenched misuse of terminology. References to "reduced compliance" in this text would more correctly be rendered as "increased elastance. However, morphine can cause a substantial release of histamine in individual patients. An evaluation of the surgical field in patients undergoing craniotomy to whom alfentanil was administered did not reveal any adverse events. The inconsistencies in the literature may largely arise because the control states entailed paralysis and nominal sedation in many studies, often with N2O alone. Comparable effects related to reduction of arousal may occur and can be clinically important. However, they should be viewed as nonspecific effects of sedation or pain control, or both, rather than specific properties of narcotics. The following discussion emphasizes investigations in which control measurements were unlikely to have been significantly influenced by arousal phenomena. Furthermore, conditions in the surgical field, including pressure under brain retractors101 and the state of brain relaxation, revealed no adverse influences attributable to sufentanil. Investigations of moderate doses of remifentanil in patients have revealed effects similar to those of other synthetic narcotics (with the exception of its substantially shorter duration of action). Quantitatively, the effects of remifentanil appear to be similar to those of sufentanil. Remifentanil was administered with other drugs that might influence cerebral hemodynamics. It appears that benzodiazepines should be safe to administer to patients with intracranial hypertension, provided that respiratory depression (and an associated increase in Paco2) or hypotension do not occur. Flumazenil should be used cautiously to reverse benzodiazepine sedation in patients with impaired intracranial compliance. Commercially available formulations of ketamine contain both the (S)- and (R)-ketamine enantiomers. Although large doses of lidocaine can produce seizures in humans, lidocaine-induced seizures have not been reported in anesthetized humans. Nonetheless, lidocaine doses should be adjusted to achieve serum levels less than the seizure threshold (>5-10 g/mL) in awake humans. All volatile anesthetics, in a manner similar to intravenous sedative-hypnotic drugs, suppress cerebral metabolism in a dose-related fashion. Of the commonly used volatile anesthetics, the order of vasodilating potency is approximately halothane enflurane > desflurane isoflurane > sevoflurane. Volatile anesthetics possess intrinsic vasodilatory activity, and they not only modify cerebral autoregulation, but they also produce a dose-dependent decrease in arterial blood pressure. The best information concerning the cerebrovascular effects of volatile anesthetics is obtained in studies during which a nonanesthetized (awake) control state is used. The latter changes, which are reversible, suggest interference with oxidative phosphorylation by halothane. Methods that assess global hemodynamic effects reveal greater changes than those that emphasize the cortical compartment. Sevoflurane may cause less impairment of the autoregulatory response to increasing blood pressure than other volatile anesthetics. These data also suggest that caution must be exercised in the administration of volatile anesthetics in pathologic conditions, such as traumatic brain injury, in which metabolism is already reduced. Nonetheless, isoflurane, desflurane, or sevoflurane are preferred because the margin for error is probably wider than with halothane. In sharp contrast, when N2O is administered in combination with intravenous drugs, including barbiturates, benzodiazepines, narcotics, and propofol, its cerebral-vasodilating effect is attenuated or even completely inhibited. These findings are, doubtless, the product of differences in species, methods, depth of background anesthesia, and interactions with simultaneously administered anesthetics. Despite the inconsistencies that are evident, the vasodilatory action of N2O can be clinically significant in neurosurgical patients with reduced intracranial compliance. However, N2O-induced cerebral vasodilation can be considerably blunted by the simultaneous administration of intravenous anesthetics. By contrast, the addition of N2O to a volatile drugbased anesthetic can modestly increase cerebral metabolism and blood flow.
Dual hypocretin receptor antagonism is more effective for sleep promotion than antagonism of either receptor alone cholesterol levels printable chart buy caduet 5 mg. Gabaergic neurons with alpha2-adrenergic receptors in basal forebrain and preoptic area express c-Fos during sleep cholesterol levels percentage discount caduet 5mg otc. Melanin-concentrating hormone neurons discharge in a reciprocal manner to orexin neurons across the sleep-wake cycle cholesterol ratio more important than total discount caduet uk. Characterization and mapping of sleep-waking specific neurons in the basal forebrain and preoptic hypothalamus in mice cholesterol test nhs 5 mg caduet order visa. Reliability and validity of the Brief Insomnia Questionnaire in the America insomnia survey cholesterol ratio in india cheap caduet 5mg on line. Validation of the International Restless Legs Syndrome Study Group Rating Scale for restless legs syndrome. A comparative contrast of clinimetric and psychometric methods for constructing indexes and rating scales. Using fitness trackers and smartwatches to measure physical activity in research: analysis of consumer wrist-worn wearables. Practice parameters for the indications for polysomnography and related procedures: an update for 2005. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. Canadian Thoracic Society guidelines: diagnosis and treatment of sleep disordered breathing in adults. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnea. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Identification and characterization of a sleepactive cell group in the rostral medullary brainstem. Validation of the Pittsburgh Sleep Quality Index and the Epworth Sleepiness Scale in older black and white women. Assessment of predictive ability of Epworth scoring in screening of patients with sleep apnoea. Body mass index, gender, and ethnic variations alter the clinical implications of the Epworth Sleepiness Scale in patients with suspected obstructive sleep apnea. Reliability and validity of the Pittsburgh Sleep Quality Index and the Epworth Sleepiness Scale in older men. Preoperative identification of sleep apnea risk in elective surgical patients, using the Berlin questionnaire. Pediatric sleep questionnaires as diagnostic or epidemiological tools: a review of currently available instruments. Digital sleep logs reveal potential impacts of modern temporal structure on class performance in different chronotypes. Total sleep time obtained from actigraphy versus sleep logs in an academic sleep center and impact on further sleep testing. Psychometric evaluation of the Insomnia Symptom Questionnaire: a self-report measure to identify chronic insomnia. Sleep apnea-plus: prevalence, risk factors, and association with cardiovascular diseases using United States populationlevel data. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. Increase in prevalence of overweight in Dutch children and adolescents: a comparison of nationwide growth studies in 1980, 1997 and 2009. Unplanned admission after day surgery: a historical cohort study in patients with obstructive sleep apnea. Risk assessment of obstructive sleep apnea in a population of patients undergoing ambulatory surgery. Obstructive sleep apnea and postoperative complications among patients undergoing gynecologic oncology surgery. Relation of sleepiness to respiratory disturbance index: the sleep heart health study. Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Obstructive sleep apnea and diabetic neuropathy: a novel association in patients with type 2 diabetes. Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. Obstructive sleep apnea: brain structural changes and neurocognitive function before and after treatment. Effect of mild, asymptomatic obstructive sleep apnea on daytime heart rate variability and impedance cardiography measurements. Health, social and economical consequences of sleep-disordered breathing: a controlled national study. Understanding phenotypes of obstructive sleep apnea: applications in anesthesia, surgery, and perioperative medicine. Postoperative respiratory muscle dysfunction: pathophysiology and preventive strategies. Upper airway collapsibility, dilator muscle activation and resistance in sleep apnoea. Effects of opioids given to facilitate mechanical ventilation on sleep apnea after extubation in the intensive care unit. Pharyngeal patency in response to advancement of the mandible in obese anesthetized persons. Contribution of body habitus and craniofacial characteristics to segmental closing pressures of the passive pharynx in patients with sleep-disordered breathing. Lateral position decreases collapsibility of the passive pharynx in patients with obstructive sleep apnea. Sitting posture decreases collapsibility of the passive pharynx in anesthetized paralyzed patients with obstructive sleep apnea. Alterations in upper airway cross-sectional area in response to lower body positive pressure in healthy subjects. Lower body positive pressure increases upper airway collapsibility in healthy subjects. Attenuation of obstructive sleep apnea by compression stockings in subjects with venous insufficiency. Nocturnal rostral fluid shift: a unifying concept for the pathogenesis of obstructive and central sleep apnea in men with heart failure. Influence of lung volume dependence of upper airway resistance during continuous negative airway pressure. Lung volume dependence of pharyngeal cross-sectional area in patients with obstructive sleep apnea. Analysis of volume displacement and length changes of the diaphragm during breathing. Anatomy of pharynx in patients with obstructive sleep apnea and in normal subjects. Within-breath control of genioglossal muscle activation in humans: effect of sleep-wake state. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. The effect of tonsillectomy on obstructive sleep apnea: an overview of systematic reviews. Lingual tonsillectomy for treatment of pediatric obstructive sleep apnea: a meta-analysis. Acute upper airway responses to hypoglossal nerve stimulation during sleep in obstructive sleep apnea. Medical therapy for obstructive sleep apnea: a review by the Medical Therapy for Obstructive Sleep Apnea Task Force of the Standards of Practice Committee of the American Academy of Sleep Medicine. Clinical practice guideline: polysomnography for sleep-disordered breathing prior to tonsillectomy in children. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation scientific statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on CardioVascular Nursing. In collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health). Predictors of sleep-disordered breathing in community-dwelling adults: the sleep heart health study. The current prevalence of sleep disordered breathing in congestive heart failure patients treated with betablockers. Hypocapnia and increased ventilatory responsiveness in patients with idiopathic central sleep apnea. The obesity-hypoventilation syndrome revisited: a prospective study of 34 consecutive cases. The dual role of the orexin/hypocretin system in modulating wakefulness and respiratory drive. The effect of sleep onset on upper airway muscle activity in patients with sleep apnoea versus controls. Lateral pharyngeal wall collapse associated with hypoxemia in obstructive sleep apnea. Ventilatory efficacy of mouth-to-mouth artificial respiration, airway obstruction during manual and mouth-to-mouth artificial respiration. Mask ventilation during induction of general anesthesia: influences of obstructive sleep apnea. Expiratory flow limitation during sleep in heavy snorers and obstructive sleep apnoea patients. Lateral sleeping position reduces severity of central sleep apnea/Cheyne-Stokes respiration. Termination of respiratory events with and without cortical arousal in obstructive sleep apnea. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea-hypopnoea syndrome: a systematic review and economic analysis. Impact of multilevel surgical treatment on mean platelet volume in patients with obstructive sleep apnea syndrome. Fat accumulation, leptin, and hypercapnia in obstructive sleep apnea-hypopnea syndrome. Prevalence and mechanisms of diurnal hypercapnia in a sample of morbidly obese subjects with obstructive sleep apnoea. Surgical stimulation induces changes in brain electrical activity during isoflurane/nitrous oxide anesthesia. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. The ventrolateral preoptic nucleus is not required for isoflurane general anesthesia. Sleep deprivation potentiates the onset and duration of loss of righting reflex induced by propofol and isoflurane. State-specific effects of sevoflurane anesthesia on sleep homeostasis: selective recovery of slow wave but not rapid eye movement sleep. Brain functional connectivity differentiates dexmedetomidine from propofol and natural sleep. Disturbances in the circadian pattern of activity and sleep after laparoscopic versus open abdominal surgery. Sleep disturbances after posterior scoliosis surgery with an intraoperative wake-up test using remifentanil. Effects of propofol on sleep quality in mechanically ventilated critically ill patients: a physiological study. Day or night administration of ketamine and pentobarbital differentially affect circadian rhythms of pineal melatonin secretion and locomotor activity in rats. Obstructive sleep apnea is not a risk factor for difficult intubation in morbidly obese patients. Do patients with obstructive sleep apnea have an increased risk of desaturation during induction of anesthesia for weight loss surgery Meta-analysis of the association between obstructive sleep apnoea and postoperative outcome. Postoperative outcomes in obstructive sleep apnea patients undergoing cardiac surgery: a systematic review and metaanalysis of comparative studies. Obstructive sleep apnea predicts adverse perioperative outcome: evidence for an association between obstructive sleep apnea and delirium. Sleep-disordered breathing and postoperative outcomes after elective surgery: analysis of the nationwide inpatient sample. Sleep-disordered breathing and postoperative outcomes after bariatric surgery: analysis of the nationwide inpatient sample. Intermediate acting non-depolarizing neuromuscular blocking agents and risk of postoperative respiratory complications: prospective propensity score matched cohort study. A brief review of non-invasive monitoring of respiratory condition for extubated patients with or at risk for obstructive sleep apnea after surgery. Post operative capnostream monitoring in patients with obstructive sleep apnoea symptoms-case series. Continuous positive airway pressure mitigates opioid-induced worsening of sleep-disordered breathing early after bariatric surgery. Knowledge gaps in the perioperative management of adults with obstructive sleep apnea and obesity hypoventilation syndrome. Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and postanesthesia care assessment.
The state commonly referred to as "unconsciousness" is in itself heterogeneous cholesterol chart by age and weight buy cheap caduet 5mg on-line, with evidence for distinct states of unresponsiveness and unconsciousness cholesterol test machine walgreens buy caduet on line. Although this heterogeneity of anesthetic actions complicates a mechanistic understanding cholesterol lowering recipes order caduet 5 mg line, it does open the possibility of developing substate-specific drugs good cholesterol foods hdl order caduet 5 mg otc. Failure to find a correlation between quantitative electroencephalographic activity and immobility in response to noxious stimulation led to the somewhat radical (at the time) hypothesis that immobility was not a cerebral cortexmediated phenomenon cholesterol test hdl ldl ratio buy 5 mg caduet overnight delivery. In the 25 years since the identification of the spinal cord as the site of anesthetic-induced immobility, research has centered on pharmacologic, genetic, and complex network approaches. Current efforts are focused on identifying the molecular, cellular, and anatomic substrates for this effect. Work with ex vivo preparations that attempt to preserve parts of the complex spinal cord circuitry suggests that anesthetic inhibition of afferent (noxious sensory) input to the dorsal horn plays a subordinate role to the suppression of the efferent (motor) output from the ventral horn, although this may vary by specific agent. This motor output is coordinated by neuronal networks organized in so-called central pattern generators that control the activity of cholinergic motoneurons. Research is being conducted in animal models and human subjects and commercial interests are working to develop effective depth-of-anesthesia monitors. These efforts reflect increasing interest, and progress, in "consciousness science" in general. However, what is commonly referred to as unconsciousness under anesthesia might be more accurately described as unresponsiveness, a condition that could also encompass states of self-awareness without environmental awareness (as in dreaming) or environmental awareness without recall. They can generally be divided into those that address "bottom-up" changes in the brain stem circuitry that controls arousal,52,53 versus "top-down" changes in the thalamocortical circuits that integrate information. Other information-based approaches use symbolic analysis,58 transfer entropy,59 chaos theory,60 and more. The rich connectivity of the cerebral cortex and its hierarchical organization are especially suited to enable high levels of information integration in the human brain. Anesthetics might act by interfering with the operational synchronicity and coherence of corticothalamic networks. Consequent disruption of functional and effective connectivity has been observed during natural slow-wave63 and midazolam-induced loss of responsiveness. Animal66,67 and human68 data implicate activity in the -band throughout the cortex as a network-level target of general anesthetics. Anesthetic actions on cortical information processing probably consist not merely of suppression of responses but of reduced complexity and variability reflected counterintuitively in the increased reliability and precision of evoked responses. The molecular and cellular mechanisms underlying this effect remain undefined, but the preferential suppression by isoflurane of cortico-cortical responses in brain slices in vitro73,74 supports a top-down mechanism wherein the anesthetic acts directly on the thalamocortical circuitry. By contrast, "bottom-up" theories attribute changes in consciousness to anesthetic modulation of subcortical arousal nuclei. There is substantial overlap between the centers whose activity is altered during natural slowwave sleep and the state of general anesthesia. Thalamic theories of anesthetic-induced unconsciousness81,82 incorporate aspects of both top-down and bottom-up mechanisms, reflecting not only the intermediate position of this structure in the hierarchical organization of the brain but also the different connection patterns of "sensory relay" versus higher-order "nonspecific" thalamic nuclei. Perhaps the closest analogue in rodents to explicit memory in humans is medial temporal lobedependent learning of temporal and spatial sequences known as hippocampus-dependent spatial learning. Other learning paradigms, such as fear conditioning to tone, are by contrast independent of the hippocampus. Isoflurane and the nonimmobilizer F6 both inhibit hippocampus-dependent learning at about half the concentration necessary for disrupting hippocampus-independent learning. Effects on other structures, such as the amygdala, may be relevant to anesthetic impairment of implicit or other types of memory. For example, -rhythms (4-12 Hz) are clearly important for hippocampus-dependent learning and memory. Isoflurane and the nonimmobilizer F6 have comparable effects on -rhythms at amnesic concentrations while having different receptor-level profiles and opposite effects on sedation. Freezing in anticipation of a noxious stimulus is a measure of learning in rats; less freezing indicates less learning. Left, the learning protocol involves preequilibration of rats in the equilibration chamber to isoflurane or the nonimmobilizer F6 at the desired concentration before placement into the training chamber. For testing of memory to tone, training and testing take place in different chambers. Right, hippocampusdependent learning (fear conditioning to context, closed symbols) is inhibited by isoflurane (purple circles) at lower concentrations than hippocampusindependent learning (fear conditioning to tone, purple squares). This differential sensitivity is mirrored by the nonimmobilizer F6 (blue circles and blue squares for context and tone, respectively). Isoflurane antagonizes the capacity of flurothyl or 1,2-dichlorohexafluorocyclobutane to impair fear conditioning to context and tone. Short-term memory resists the depressant effect of the nonimmobilizer 1-2-dichlorohexafluorocyclobutane (2N) more than long-term memory. The synchronization between amygdalar and hippocampal -rhythms that occurs during fear memory retrieval indicates that this principle might also apply to other forms of memory and their impairment by anesthetics. There is no clear mechanistic or clinical separation between sedation and hypnosis. By contrast, even though sedation can be difficult to separate from amnesia, for intravenous anesthetics there may be separate but overlapping substrates for these two end points. Anesthetic effects on other cortical107 and subcortical structures32 may also contribute to anesthetic-induced sedation and hypnosis. This criterion requires comparable in vivo and in vitro sensitivities and depends on the anesthetic end point under consideration. Recent evidence for persistent effects of inhaled anesthetics demonstrable in the absence of continued anesthetic exposure is challenging the notion of reversibility for certain effects. Expression of the target in appropriate anatomic locations to mediate the specific anesthetic end point. For example, immobilization by inhaled agents appears to involve primarily actions in the spinal cord independent of actions in the brain. Concordant stereoselectivity of anesthetic effects in vivo and on the target in vitro. Without a specific pharmacologic antagonist of anesthesia, correlation between the stereoselective actions of general anesthetics in vivo and in vitro is a useful test of pharmacologic relevance of putative molecular targets. Appropriate sensitivity or insensitivity to anesthetic and nonanesthetic compounds. Anesthetic halogenated cyclobutanes together with structural analogs that do not produce anesthesia at concentrations predicted to be anesthetic by the Meyer-Overton correlation (nonimmobilizers) can be used to discriminate relevant volatile anesthetic targets in vitro. F6 is interesting in that it lacks sedative and immobilizing effects but does possess amnesic effects, hence use of the more accurate term nonimmobilizer, making it a useful pharmacologic tool for discriminating targets for these actions. Predictable effects of genetic manipulations targeted to putative molecular targets. The effects of targeted deletion of specific molecules implicated as anesthetic targets (knockout mutations) or genetic engineering to introduce specific mutations that modify anesthetic sensitivity (knockin mutations) in model organisms provide powerful approaches to test the roles of putative molecular targets of anesthetic action. The existence of multiple targets and redundancy among ion channel subtypes makes this a more challenging experimental approach for inhaled anesthetics compared with intravenous anesthetics (discussed later). An element of amphiphilicity (possessing both polar and nonpolar characteristics) is also required for effective interaction with these cavities, as indicated by improvements in the Meyer-Overton correlation with more amphipathic solvents (possessing both hydrophobic and hydrophilic properties). Consequently most anesthetic binding sites have been identified in well-characterized model proteins for which three-dimensional atomic resolution structuressuch as luciferase110 and serum albumin111are available but are not themselves relevant to anesthesia. These studies indicate that anesthetics bind in pockets with both nonpolar and polar noncovalent chemical interactions. Occupation of a site, or sites, by an anesthetic provides a plausible mechanism for alteration of receptor and ion channel function by selectively binding to a particular conformation. However, because anesthetics act by binding only to certain transient conformational states, the relevance of necessarily static crystal structures will have to be assessed with care. X-ray structure of general anaesthetics bound to a pentameric ligand-gated ion channel. The amino acid backbone is displayed in ribbon format and outlined by the transparent solvent-accessible molecular surface. Refinement of these molecular models will continue to provide new insights in the molecular basis for general anesthetic action that can be experimentally tested. Molecular Targets of Inhaled Anesthetics Ion channels have emerged as the most promising molecular targets for inhaled anesthetics. Although the molecular mechanisms of receptor modulation by inhaled anesthetics are not clear, these receptors have been key to our understanding of anestheticreceptor interactions. Activated receptors conduct chloride ions, driving the membrane potential toward the Cl- equilibrium potential. Both receptors are inhibitory (except in some cases during development) because the Cl- equilibrium potential is usually more negative than the normal resting potential. Channel opening also reduces membrane resistance and "shunts" excitatory responses. They are composed of and subunits but functional homomeric receptors can be formed by certain subunits. A detailed understanding of these interactions is crucial to a pharmacologic description of this essential drug class. In contrast to findings in invertebrate giant axons,136 axonal conduction in small (0. The Na+ channel family consists of nine homologous pore-forming subunits with distinct cellular and subcellular distributions. Alteration of any of these mechanisms can affect the many cellular processes regulated by the second-messenger actions of Ca2+, including synaptic transmission, gene expression, cytotoxicity, and muscle excitation-contraction coupling. Excitable cells translate their electrical activity into action by Ca2+ fluxes mediated primarily by voltage-gated Ca2+ channels in the plasma membrane. Cloning and sequencing to identify their pore-forming subunits has allowed molecular classification of these functionally identified channel subtypes. Inhibition of presynaptic voltage-gated Ca2+ channels coupled to transmitter release has been proposed as a mechanism by which volatile anesthetics reduce excitatory transmission. At higher doses, a role for Ca2+ channel inhibition in the negative inotropic effects of volatile anesthetics is well established. The force of myocardial contraction is determined by the magnitude of cytosolic Ca2+ increase after electrical excitation, the responsiveness of the contractile proteins to Ca2+, and sarcomere length. Negative inotropic effects of volatile anesthetics are mediated by reductions in Ca2+ availability, Ca2+ sensitivity of the contractile proteins, and rate of cytosolic Ca2+ clearance. Volatile anesthetics reduce the Ca2+ transient and shorten action potential duration in cardiomyocytes primarily by inhibiting L-type (Cav1. It is often associated with mutations in RyR1 and the physically associated L-type Ca2+ channel (Cav1. They regulate electrical excitability, muscle contractility, and neurotransmitter release. They are important in determining input resistance and in driving repolarization after action potentials; thus they determine excitability and action potential duration. Given the large diversity in K+ channel structure, function, and anesthetic sensitivity, it is not surprising that there is considerable diversity in their sensitivity and response to inhaled anesthetics,171 from relatively insensitive (voltage-gated K+ channels Kv1. Volatile anesthetic activation of certain "leak" K+ channels was first observed in the snail Lymnaea,173 although the molecular identity of the affected ion channels was unknown. Activation of K2P channels by volatile and gaseous anestheticsincluding xenon, nitrous oxide, and cyclopropanewas subsequently observed in mammals. Anesthetics have complex actions on intracellular cell signaling pathways, which include processes downstream from cell surface receptors and ion channels, including effects on second messengers, protein phosphorylation pathways, and other regulatory mechanisms. In contrast to inotropic receptors that directly couple to ion-selective channels, G proteins act as indirect molecular switches to relay information from activated plasma membrane receptors to appropriate intracellular targets. Heterotrimeric G proteins consist of a large -subunit and a smaller /-subunit dimer, each expressed as multiple isoforms with distinct properties and downstream targets. G proteins regulate a plethora of downstream effectors to control the levels of cytosolic second messengers such as Ca2+, cyclic adenosine monophosphate, and inositol triphosphate. These, in turn, regulate effector proteins such as ion channels and enzymes, either directly or via second messengerregulated protein phosphorylation pathways. Ca2+ is a ubiquitous second messenger that regulates a number of downstream effectors, often mediated by the multifunctional Ca2+-binding protein calmodulin. As volatile anesthetics have profound effects on intracellular Ca2+ concentrations via their effects on both plasma membrane and intracellular Ca2+ channels, transporters, Protein Phosphorylation Phosphorylation of proteins on specific serine, threonine, or tyrosine hydroxyl groups, a posttranslational modification involved in the regulation of many anesthetic-sensitive receptors and ion channels, is pivotal to synaptic plasticity. Phosphorylation is controlled by the balance of activity between protein kinases and phosphatases, several of which are plausible anesthetic targets. An important role for effects of volatile anesthetics and xenon on cell signaling mechanisms has been discovered for anesthetic-induced preconditioning in the heart and brain against ischemic damage. A comparison of the effects of three mechanistically diverse anesthetics (isoflurane, propofol, and ketamine) on critical intracellular protein phosphorylation signaling pathways that are known to integrate multiple second messenger systems reveals both shared and agent-specific actions in vivo. Gene Expression the ability of general anesthetics to alter gene expression in the brain was first observed for the highly reactive immediate early genes c-fos and c-jun. For example, exposure of neonatal rats to general anesthesia led to reduced histone 3 acetylation and delayed cognitive deficits that could be reversed by a histone deacetylase inhibitor. Nevertheless much valuable information has been obtained using these approaches because they allow changes in neuronal activity to be attributed to specific cellular and molecular targets. The intrinsic excitability of spinal motoneurons was reported to be little affected by halothane,214 but changes in hippocampal pyramidal neuron excitability were shown to be substantial and complex. Threshold can be increased or decreased, and regional differences and dose-dependent effects on firing patterns have been observed. Considerable diversity exists for each of these factors in different types of neurons, and membrane properties differ not only between neurons but also between compartments. Moreover, anesthetic effects vary with the state of the individual neuron-that is, whether it is hyperpolarized or depolarized, stimulated by synaptic inputs, or quiescent.
Buy caduet 5 mg. The Egg Cholesterol Myth: Are Eggs High In Cholesterol?.
References
- Raza A, Reeves JA, Feldman EJ, et al. Phase 2 study of lenalidomide in transfusion-dependent, low-risk, and intermediate-1 risk myelodysplastic syndromes with karyotypes other than deletion 5q. Blood 2008;111(1):86-93.
- Mala T, Bohler G, Mathisen O, et al. Hepatic resection for colorectal metastases: can preoperative scoring predict patient outcome? World J Surg. 2002;26(11):1348-1353.
- Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297:845-50.
- Wilson DW, Reeves AG, Gazzaniga M. Central commissurotomy for intractable generalized epilepsy: series two. Neurology 32: 687-697, 1982.
- Hoerter J, Gonzalez-Barroso MD, Couplan E, et al. Mitochondrial uncoupling protein 1 expressed in the heart of transgenic mice protects against ischemic-reperfusion damage. Circulation 2004;110:528-33.