
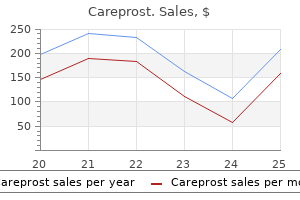
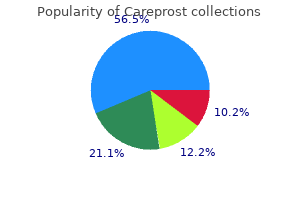
Careprost
| Contato
Página Inicial
Christopher V. Chien, MD
- Cedars Sinai Medical Center &
- University of California
- Los Angeles
- Los Angeles, California
Older children with some degree of speech perception should also have specific speech perception testing results that are obtained while wearing appropriate amplification (Table 163 medicine wheel native american order careprost 3 ml mastercard. The reader should always seek up-to-date treatment 02 academy buy generic careprost from india, detailed information on a case-by-case basis prior to considering candidacy treatment bronchitis purchase 3 ml careprost fast delivery. For young children medicine valley high school careprost 3 ml order on line, it remains critically important to recognize the importance of early intervention in the form of appropriately fit amplification and/or cochlear implantation in the development of speech perception treatment toenail fungus buy cheapest careprost, speech production, and spoken language (5). While these studies clearly document the fact that earlier is better, this must be balanced against the reality that cochlear implants, in their current format. With this in mind, it remains important to defer cochlear implantation until the age where developmentally appropriate behavioral audiometric results are valid (usually 7 to 9 months of age for visual reinforcement audiometry). One clear indication for very early implantation might include a history of meningitis with ongoing ossification. Irrespective of the type of intervention, early diagnostic and therapeutic auditorybased speech therapy is critical in assessing progress in spoken language development this single factor remains of paramount importance in deciding whether to proceed with implantation in the very young. Temporal Bone Imaging in Cochlear Implantation Diagnostic imaging of the temporal bone and brain is critical in patients considering cochlear implantation to (a) identify the etiology of hearing loss, (b) define surgical anatomy and the potential for complications or sequelae from surgery, and (c) identify factors that negatively impact upon prognosis for performance using the device. Cochlear obstruction can occur following previous cochlear inflammation in the setting of meningitis and the degree of labyrinthine obstruction that is due to ossification. In lncom· plete partition, there are normal cochlear external dimensions, but decreased or absent partitioning. Surgery for Cochlear Implantation Setup Cochlear implant swgay is performed under general anesthesia and typically takes between land 2 hours to complete. Patients with significant medical comorbidity should have a prior anesthetic risk assessment. A first-generation cephalosporin is sufficient as ear pathogens such as StreptDcoccus pneumoniae, Haemophilw infiuenme, and Pseudomonas aeruginosa should be unwual in routine cases. Receiver-Stimulator Placement and Fixation Following a skin incision, a subperiosteal pocket is created in the proposed region for the inte:rnal receiver-stimulator that is bounded inferiorly by the lambdoid suture and is Preparation the patient is situated in a supine position with the head turned to expose the postauricular region. Locating the receiver-stimulator too close to the pinna can result in unwanted interaction between the magnetic headpiece and the speech. Moreove:t placement too close to the mastoid can be problematic if skin retraction in to the mastoid results in unwanted device exposure. The use of manufacwrer-specific device templates prior to the incision can help locate the proper position. Focal injection of methylene blue through the skin and on to the bone allows for identification of the bony position for the internal device after skin elevation. Locating the device relative to the mastoid cavity following bony exposure can be ineffec:tive since mastoid size varies considerably among individual of all ages. The:final position of the receiverstimulator usually is significantly superior and posterior to the pinna. The long axis of the device creates roughly a 45-degree incline from the horizontal through the zygomatic arch. Chapter 163: Cochlear Implants and Other Implantable Auditory Prostheses 2633 strictly sized for the device being implanted (69). A bony depression can be created according to the device templates and the device fixed to bone by any one of a variety of methods (70). For adults, nearly all techniques are sufficient, while for children, simple suturing of the periosteum provides rigid fixation to bone and avoids intra- or transcortical drill holes or screws that might put the underlying dura or venous sinuses at risk (71). Electrode Insertion A smooth, resistance-free insertion of the proposed electrode array in to patent scala tympani is the goal of most implantations. The reader is referred to the individual surgical manuals for details regarding usage of the various devices. The facial recess is opened maximally using the horizontal semicircular canal, fossa incudis, chorda tym pan~ and facial nerve as landmarks. The round window niche overhang is initially identified as a bony, rounded ridge located inferior to the oval window niche and anterior-inferior to the stapedius tendon. The niche is always located posterior to Jacobson nerve on the cochlear promontory and 1 to 2 mm inferior to the oval window. It is very important to recognize that limited opening of the facial recess can result in an inferior view towards the hypotympanum with a resulting look at the air cell system rather than the promontory and round window region. Cochleostomy When describing the surgical technique for cochleostomy creation, one should keep the basic objectives in mind: open scala tympani (and not scala vestibuli), minimize collateral trauma to physiologically relevant intracochlear structures, and provide a relatively straight insertion trajectory along the longitudinal axis ofthe basal turn in an effort to allow for buckle-free electrode insertion. Currently, a variety of differing cochleostomy techniques exist that can be adapted to the clinical situation depending on the following: the electrode array to be used, the cochlear morphology, and the desire for hearing preservation (72). Such a cochleostomy is always round window related and might actually communicate with the round window membrane if higher insertion forces are not anticipated. For very long electrode arrays that are designed for complete cochlear coverage, a cochleostomy that has circumferential bony walls or a round window membrane insertion is acceptable. In these cases, cochlear length rather than cochleostomy location probably determines whether insertion resistance will be encountered. All devices have telemetry programs that allow for measurement of electrode impedances and electrically evoked compound action potentials. If a substantial number of circuits are found to be open, replacement of the device should be considered to insure that an adequate number of electrodes are available for stimulation. In such cases, the result of these measures has been shown to correlate with future performance on open-set speech perception measures (67,74). Moreovet; threshold determination for electrically evoked compound action potentials might identify a useful stimulation starting point for very young children. Special Surgical Considerations Inner Ear Malformations Congenital inner ear malformations are common (10o/o to 20%) among children undergoing cochlear implantation (75). Labyrinthine anomalies have the potential to adversely affect the electrode-neural interface, reduce electrode array insertion depths, predispose to cerebrospinal fluid gusher through the cochleostomy, and be associated with facial nerve anomalies that can create access problems for scala tympani. Similar to cases without malformations, a round window-related cochleostomy can usually be created. The bony overhang covering the actual window has to be removed to expose the actual membranous window. B: lllun-ation of typical insertion trajectories through the different round window alignments. In these cases, the window faces essentially posterior fadlltmlng a direct Insertion through the window. In these cases, the electrode can take a trajectory heading towards the bony modiolus. In such instanas, creating a largu cochlear opening and tightly packing connective tissue around the electrode array is sufficient Cerebrospinal fiuid divemion iJ not needed if the leak iJ controlled intraoperatively. Imaging that reveals a hypoplastic cochlea should be expected to have limited electrode insertion depths and for these cases, shorter arrays are helpful. Children with absent semicircular canals or external auditory canal atresia can create significant issues for cochlear access since the facial nerve is often times displaced anteriorly. Inner Ear Obstruction Cochlear obstruction can occur following inner ear infiammation from meningitis, immune-mediated ear disease, otitis media with labyrinthitis, or trauma. In these cases, the cochlear lumen can be narrowed or obliterated with fibrous tissue or bone. In cases of ongoing meningitis, intervention should be considered in the early stages so as to avoid total obstruction and inability to implant the ear(s) in question. The l~m~ral semicircular canal typically used as a surgical landmark cannot be used. Instead this single opening Into the cavity should allow the surgeon to curl the electrode Inside to generate an optimal electrode-neurallnterfaw. Approach to implantation of the obstructed cochlea should be considered in a stepwise manner. In cases of short segment obstruction resulting from either fibrosis or bone (1 to 3 mm), a typical round window-related cochleostom:y can be created by drilling through the short segment of obstruction. If more than 3 mm of drilling fails to reveal a patent cochlear lumen, a scala vestibuli insertion should be considered by moving superiorly, above. Rarely, severe fust tum ossification can make both scala tympani and vestibuli inaccessible at the cochlear base. In this situation, the trough created near the round window can be used for a short array. Great care should be exercised to avoid inadvertent injw:y to the undmurface of the labyrinthine segment of the facial nerve. Following such insertions, communication with the individual programming the device is critical to insure that proper pitch assignment is made for the retrograde electrodes. Finally, in cases of diffuse obstruction, a circummodiolar drill out is possible (76,77). Otitis Media Active otitis media is a contraindication to cochlear implantation in that inttacochlear or device exposure to viable bacteria can result in suppurative labyrinthitis with subsequent meningitis and ossification. In children, consideration of active middle ear disease is common in the winter months. There are some advocates for subtotal petrousectomy with blind sac closure in the setting of otitis media to avoid future considerations for this problem. There also remains considerable dispute regarding the significance of otitis media with effusion. Specifically, the nerve (arroW) runs onr 1he round window niche and the coc:hleostomy can be seen anterior to the nerve. In such cases, active middle ear disease should be cleared or controlled prior to implantation. One option is to consider early blind sac closure with or without obliteration and staged implantation. This avoids the long-term issues of tympanic membrane retraction, granulation, infection, and electrode exposure within a tympanic membrane perforation. Complications might be broadly categorized in to those that are medical/surgical in nature and those that are device-related. Historically, medical/surgical complications were more common than device-related issues. Minimal approaches to skin incisions and proper device location and immobilization have been key in reducing such complications. Careful attention to the surgical details described above can avoid or at least minimize many of the surgical complications outlined. Common and potentially unavoidable complications include taste disturbance from chorda tympani nerve manipulation or sacrifice (-10%), transient dizziness (-10% of adults and less common in children), and subcutaneous seroma (10%) (78). The vestibular effects of cochlear implantation have long been a concern among otologic surgeons. For children, the risk of vestibular loss remains quite small since most pediatric patients have limited, peripheral vestibular function preoperatively. Subcutaneous seroma, while common early after cochlear implant surgery nearly always resolves without the need for any intervention. Device-related complications include receiver-stimulator hard failures, suspected device malfunction. Hard failure refers to a total lack of function of the device despite properly functioning external equipment. Hard failures results from internal, receiver-stimulator problems and require revision surgery to alleviate the issue. Suspected device malfunction or soft failure is significantly more difficult to diagnose and refers to the situation where despite the presence of auditory percepts, the patient experiences aversive symptoms such as pain, shocking. Following complete exchange of the external equipment and confirmation of electrode location within the cochlear lumen by imaging. Open circuits can occur early or in a delayed fashion following cochlear implant surgery. A value judgment of electrode number and location is needed to insure adequate stimulation is available for performance. The details of revision cochlear implantation and reliability are often times complex. Fortunately, in most instances, revision cochlear implantation results in a functioning device that restores access to sound. Parents of such children should be made aware of these possible delays prior to surgery (81). Meningitis in Cochlear Implant Recipients the incidence of meningitis in cochlear implant recipients is greater than that of an age-matched cohort in the general population (82, 83). Risk factors in this population include young age, the presence of inner ear malformations, and the use of a two-part electrode system. The risk of meningitis also appears to be higher among individuals with sensorineural hearing loss without a cochlear implant although this risk appears lower than that of implanted Device-Related Internal Hard Failure. It remains diffirult to detennine whether cochlear implantation per se confers an increase risk of meningitis in subjects without the factors cited above. All potential routes of spread (middle ear, inner ear, hematogenous) should be considered in such a patient. Recent animal investigations into the mechanisms of meningitis following cochlear implantation suggest that all three routes are viable sources for such an infection (85). These works also support the need to create a relatively atraumatic cochlear opening, insert the electrode array without trauma to reduce the potential for inner ear to subarachnoid space communication, and form an adequate seal at the cochleostomy with connective tissue to prevent the direct spread of infection along the array. Early and adequate treatment of otitis media is also important in preventing meningitis in implanted patients. Clinical Results Cochlear implantation is an auditory intervention that restores sound awareness for nearly all individuals that receive the device. Depending on a variety of factors and expectations, there remains a wide range of performance outcomes that are achievable through cochlear implantation. These include enhancement of lipreading and improvements in speech perception and music appreciation (87-89). Improved speech perception can result in appropriate development of spoken language and educational achievement for children and improved communication skills for adults (5,6).
Grafts Full-thickness skin grafts require a vascularized reoptent bed and medications with codeine cheap careprost 3 ml fast delivery, as such medicine lake order 3 ml careprost visa, will rarely be utilized for internal 2896 Section X: Facial Plastic and Reconstn symptoms you need glasses purchase careprost amex. B: Nasal septum pivoted anteriorly along posterior septal angle to provide dorsal and tip support medications venlafaxine er 75mg discount 3 ml careprost. C:: Additional sidewall support from c:onc:hal autilage grafting and shape with a tip graft medications you cant donate blood purchase generic careprost from india. Inferior turbinate flap Labial mucosal flap (small caudal defects) Pericranial flap Distant microvascular flap 3. In both cases, the skin portion of the graft is closely adhered to the cartilage with little intervening fat thus making it an excellent option for composite grafts. The graft should be finnly secured to the undersurface of the resurfacing flap, entirely obliterating any potential dead space that might arise. Cutaneous Epithelium Cutaneous epithelium is an additional source for internal lining repair and has some distinct advantages. Large amounts of tissue can be mobilized to inside the nose with little morbidity. There is additional thickness and bulk to this type of flap, and it is important to thin the skin paddle aggressively prior to transposition. Perhaps the greatest concern is the mobilization of sun-exposed and potentially actinically injured skin to the intranasal portion of the nose, especially considering the high nature of recurrence or metachronous lesions. The intranasal examination postoperatively is best performed by the otolaryngologist and with a nasal endoscope. A second epithelial flap can be elevated and transposed for internal lining repair. These are associated with extra morbidity but may represent a viable option for advanced cases (38). Distant tissue through microvascular transfer is a more dramatic means of bringing lining to within the nose. It should be viewed as a preliminary step requiring subsequent stages for thinning and sculpting (39-41). The distal portion of the primary resurfacing flap can be folded on itself to wrap around a cartilage graft and provide internal lining. This utilizes cutaneous epithelium and is subject to the same guidelines in terms of risk of transferring actinically injured skin. The additional morbidity may be minimal for small lining defects since the source of skin may be the superior portion of the forehead. Moreover, this portion of the forehead flap may include the frontal hair and have to be trimmed regularly. There is concern over the vascularity of this distal part of the flap, particularly after folding it on itself, but the robust vascular perfusion appears to be 5. Grafts from the hard palate have more intrinsic rigidity and may be applied for intermediate size defects. A composite graft of skin and cartilage from the ear is extremely versatile and can be liberally applied to fullthiclmess nasal defects. It may be the technique of choice for lining deficits of the distal one-third of the nose. Perhaps 1he greatest shortcoming has to do with the free margin of the ala Although the inttanasallumen may be functionally adequate, the alar rim often takes on an unnaturally thick and straight appearance when using thiJ method. It utilizes the cutaneous epithelium from the upper nose and turns it in 180 degrees, so that it faces intranasally. Elevation begins superiorly in 1he subdermal plane and descends deeper aa one proceeds inferiorly in order to create a flap with a healthy subcutaneous pedicle. In some cases, this llap adds no additional morbidity; at times, the "tum-in· flap represents skin that would be discarded during 1he completion of the nasal aesthetic subunits. Intranasal Tissue It is ideal to replace tissue with like tissue, and inttanasal mucosa has several options that provide a thin, pliable, robust, and ph:ysiologic lining for 1he full-thickness nasal defect. It is rare for a primacy cutaneous malignancy to invade so far posteriorly that it disrupts the head of the inferior turbinate. A: Full-1hlc:kness right nasal defect wft:h lining deficit of middle 1hlrd and ala. The lnpedided "bucket-handle" mucosal flap ia an excellent option for relatively small lining defects along the alar lobule. It utilizes intranasal mucosa immediately above the defect and hinges it inferiorly as a flap based medially and laterally. The anterior septal artecy territory doea not dependably extend laterally to the sidewall, and the lateral pedicle must be maintained. Wide undermining is critical in order to allow complete mobilization inferiorly without superior traction and recoil. The extent of undermining should be to the nasal bones, where the secondru:y donor site defect is allowed to heal by second intention. Placing a skin graft to this Chapter 177: Nasal Reconstruction 2903 location is an alternative, but rarely necesscuy. Any superior retraction will inevitably lift the free alar margin and compromise the alar base symmetry. The contralateral septal mucosa can be used via a swinging, composite septal flap, based on the dorsal septum and the branches of the anterior ethmoid artery. It is an excellent means of providing both intranasal lining and cartilaginous framework to the middle third of the nose. It does not have sufficient size to provide structural framework to the alar lobule. The cartilage is typically straight and can also assist with dorsal support to that area as it rests on the boney ledge of the piriform aperture. A full-thickness incision is then made through the septum, creating a swinging door of cartilage and contralateral septal mucosa. There is a tendency for the flap to swing back medially, and this is resisted by securing the cartilage to the boney aperture. The ipsilateral septal mucosa can be used for alar lining for larger defects or can be replaced to reconstruct the resultant septal perforation. The ipsilateral, septal mucosa flap is a large flap for complex internal lining defects of the nose. First described by Millard (15) in 1967, it is a thin and dependable flap based on the septal branch of the superior labial artery. The entire septal mucosa is lifted off the cartilage and mobilized to line the lower two-thirds of the nose. Tremendous care should be observed to stay in the correct subperichondrial plane, especially if there coexist septal spurs or fractures. The pedicle to this mucosal flap may cross the nasal vestibule and cause nasal obstruction. The critical prerequisite for this flap is the preservation of the anterior/ inferior portion of the septum and the nasal sill, as this functions as the flap base. The bar has been set and it is nothing less than full restoration of normal function and complete aesthetic acceptance. The expectations for both minor and major nasal repair include symmetry, natural contour, excellent color and texture match, and a final product that remains inconspicuous to the casual observer. The major tenets that have been realized today include the wide application of the subunit principle, liberal and nonanatomic cartilage grafting, and addressing each of the three layers of the nose diligently and independently. The robust nature of the forehead flap has expanded its applications and lifted the outcomes of major nasal resurfacing. Anticipating resultant scars and vectors of tension are the subtle nuances oflocal flaps that ensure a pleasing result · Using a reconstructive algorithm can assist with flap selection and avoiding pitfalls. The forehead flap is a robust flap that remains the workhorse for resurfacing large defects. Pericranial Flap the pericranial flap is a thin and versatile flap often used by neurosurgeons for anterior cranial defects. It can also be elevated for internal nasal lining and transferred as part of the forehead flap. The pericranium should be covered with a skin or mucosal graft because, although epithelialization will occur eventually, wound contracture and desiccated cartilage may present problems. The pericranium is based on the same pedicle as the forehead flap but is more tenuous and a wider pedicle base may be needed. Thlnsaaions of the Fourth International Qmgms of Plastic and Reconstructive Swxery. Anatomical study of furehead flap with its pedide based on rutaneous branch of supratrochlear artery and its application in nasal reconstruction. Total Nasal Reconstruction: a 6-year experience with the three-stage forehead flap wmbined with the septal pivot flap. An alternative method fur reronstruction of large intranasal lining defects: the farina method revisited. Microvascular repair ofheminasal, subtotal and total nasal defects with a folded radial furearm flap and a fullthickness forehead flap. Carpue J, An account of two successful operations fur restoring a lost nose from the integuments of the forehead. The repair of nasal defects with the median forehead flap primary closure of the furehead wound. Aesthetic ronsiderations in nasal reconstruction and the role of modified nasal subunits. Hadlock Rehabilitation of the paralyzed face remains a challenging problem for otolaryngologists, and its proper management may require input from facial plastic surgeons, head and neck reconstruction specialists, otologists, and adjunct medical personnel. Following viral nerve insult, traumatic nerve injury, or intentional sacrifice with repair or cable grafting, regenerative results vary greatly and can lead to hypofunction, hyperfunction, aberrant regeneration, or a combination of these phenomena. In the upper face, they include brow ptosis, leading to a visual field deficit and hygiene issues related to skin desquamation onto the cornea. In additio~ loss of a blink reflex leads to corneal exposure of the affected eye, there is lacrimal gland hypo- or hyperfunction, and lower lid paralysis results in ectropion as well as poor lacrimal punctal function. In the central zone of the face, patients may suffer with unilateral nasal obstruction, upper lip ptosis, lack of oral commissure excursion with smiling, oral incompetence to both liquids and solids, and articulation problems. In the lower face, lower lip weakness also contributes to oral incompetence, and platysmal synkinesis can restrict smiling and lead to superficial torticollis symptoms. Herein, we review the management of facial nerve deficits and describe the surgical management of each distinct zone of the paralyzed face, with regard to recovery potential, prognosis, and patient factors that contribute to surgical decision making. We emphasize the systematic assessment of each facial zone as a critical step to ensure comprehensive management of the paralyzed face (1). According to the Sunderland classification system (2), level 1 injury has no microanatomic disruption but a simple temporary dysfunction of the membrane sodium channels, resulting in transient inability of the nerve to transmit impulses. In level 2 injury, axons are disrupted, though their individual endoneuria] channels are not. Level4 injury implies total perineurial disruption, where only the outer epineurial sheath is intact, and spontaneous recovery is generally poor. No spontaneous recovery is expected from this injury without surgical intervention. Management of Neural Discontinuity In cases of complete facial nerve disruption, reestablishment of direct nerve continuity is required for restoration of muscle function. When injury occurs within the temporal bone, thorough exposure of the site of injury is recommended, and surgical repair is indicated when 50% of the diameter of the facial nerve appears to have been violated (3). After facial nerve injury or sacrifice, if a tensionless neurorrhaphy is not possible because of a gap between the cut edges, then a nerve graft is employed to bridge the 2905 2906 Sec:tion X: Facial Plastic and Reconstructive Surgery neural defect. For short nerve gaps in the absence of head and neck malignancy, the great auricular neiVe ia a convenient choice. This often does not require a separate incision from the primar:y facial nerve exposure incision. The resulting anesthesia to the ipsilateral auricle ia well tolerated, and the nerve ia of adequate diameter and aliber to provide a suitable graft. The nerve is removed from the leg via a short incision adjacent to the lateral malleolus and can be harvested through a series of stair-step incisions, a minimally invasM! The resulting segment of anesthetic skin on the dorsum of the foot does not pose a significant clinical problem. For total facial nerve reconstruction from the main trunk to the peripheral branches, the medial antebrachial cutaneous nerve is most appropriate. There are at least four reliable branches, and it provides adequate length to graft the entire facial nerve, from the geniculate ganglion to the medial bolder of the parotid gland. Though not fully established as more efficacious, it is now becoming commonplace to further reinforce the repair using:fibrin glue stabilization (5). Reinnervation Techniques When the reestablishment of neural continuity is not possible based upon absence of an adequate proximal facial nerve stump at the brainstem, or severe comminution within the temporal bone. The hypoglossal facial transfer is most often used, though investigators have studied the utility of 1he spinal accessory nerve. The advantages of 1he hypoglossal ner:ve as a donor for reinneJ:vation techniques include its location, close to the exttatemporal facial nerve; its dense population of motor axons; and 1he relative acceptability of 1he resultant hemitongue wealmess. Elimination of the cable graft provides a theoretical regenerative advantage by reducing from two neurorrhaphies to one. The main trunk of the facial nerve and the pes anserinus are identified using standard facial nerve landmarb. The hypoglossal ner:ve is identified deep to the posterior belly of the digastric muscle and is followed anteriorly, to just beyond the branching of the descendens hypoglossi. The hypoglossal nerve is sharply transected and reflected superiorly to meet the facial netve.
If the physician pr~ to remain in a film-based medium medicine youth lyrics buy careprost no prescription, it would be advised to consider using a digital camera or a Polaroid for immediate feedback and to ensure that the necessary image has been obtained medicine q10 purchase careprost with visa. Also treatment 2 go order careprost 3 ml fast delivery, use of a digital camera and/or Polaroid facilitates immediate patient dialogue that would oth medications ranitidine careprost 3 ml purchase. Nevertheless medications hypothyroidism careprost 3 ml buy online, the initial setup cost for digital photography can be quite high due to the associated hardware requirements, for example. Today, most offices already use computers, so few additional hardware expenditure is typically required. Moreover, the cost of technology is rapidly tumbling, and the lack of consumables will offset initial outlay very rapidly, unless every photograph is printed, for instance. No accurate comparison can be made between a digital pixel and the silver-halide grain of film, but this argument really borders on arcane academic banter and lacks any practical clinical import. This section discusses input devices (digital cameras and scanners (to convert 35-mm images over to digital)), image processing and storage compression, archiving, and morphing), and output devices (printers and projectoiS) (5). Obviously, a high-quality; aspherical lens achieve~ commensurate value as in 35-mm photography. Unltke 35-mm photography, the digital camera body can be as Important as the quality of the lens In obtaining superlative photographic results. Chapter 171: Pictorial Documentation: Digital Imaging and Traditional Photography 2781 which would be analogous to the 35-mm film plate. However, these higher bits are not superfluous, but the added data undergo a selection process for the best bits of color information to yield a 24-bit output product. Unfortunately, due to the smaller compression ratio (typically 2:1 or 3:1), file sizes can be quite large on the order of several megabytes. Scanners Scanners are used to convert a 35-mm library or select printed images into the digital medium. The former consists of a specialized camera housed below a dear glass panel with a hard, opaque cover that scans an image in a linear fashion to convert it into a digital version. The flatbed scanner benefits from versatility (ability to scan multiple media, like photographs, tables, graphs, text. Film scanners are dedicated to scanning only slides or negatives and can do so often very quickly and at a higher resolution. Optical resolution simply refers to the number of pixels per inch (ppi) and can be achieved by a straightforward pixel per pixel output or manipulated by a process known as interpolation, which can prove to be inferior. Most scanners offer an optical resolution between 300 to 4,800 ppi and an interpolated resolution of 0 to 1,900 ppi. Generally, 300-ppi scanning is sufficient for printed materials, whereas a 72-ppi resolution is adequate for web or monitor display. Bit depth refers to the maximum number of colors that each pixel of an image can display. Color balancing and fine adjustment of hues and brightness, just as if you had sent film to a processing laboratory, should be considered proper. Further, cropping extraneous elements in an image so long as the image integrity has not been undermined should be deemed acceptable as well these powerful tools underscore the strengths of the digital 2782 Section X: Facial Plastic and Reconstructive Surgery format. Intentional editing, or morphing, allows alteration of a digital image so that the surgeon can communicate with the patient an intended aesthetic result. Care should be taken to avoid overpromising and to remind the patient of the shortcomings in accuracy of a digitally morphed image. Morphing can be particularly effective when demonstrating to a patient the change in nasal profile and/or change in the neck and chin region for two principal reasons. Second, the soft tissues are contrasted against a blue background, making image alterations relatively straightforward (as compared with moving skin over skin in a frontal view). Archiving the lack of physical space that a digital library takes up is also an undeniable benefit Howev~ the physician would be wise to select a good archiving program early so that the growing catalog of digital images can be easily organized and subsequently retrieved. Browser-type software permits simple retrieval of graphic images and is usually bundled free with purchased digital cameras. On the other hand, catalog software often permits more sophisticated handling of many file types (text, graphic, video, and audio) and can attach metadata to a file. Metadata refers to the descriptive text that can be attached to a file to facilitate its retrieval, for example, ·susan Smith," "Crooked Nose," etc. Parameters that define a high-quality printer are as follows: printer resolution expressed in dots per inch (dpi) with a good printer having upward of 1,440 dpi; the number of color inkwells (3 being a relatively low number and 6 being a favorable number); and the size of the ink droplets (3 to 4 pL are superior to 6 to 18 pL). Dye-sublimation printers, or dye-subs, work by depositing vaporized ink lifted from a colored ribbon onto a specialized paper to achieve a more continuous-toned print. Unfortunately, these printers are more expensive and can only print a predetermined size, for example, 5 x 7 or 8 x 10 inch. Color laser printers can produce high-quality images at a faster rate than inkjet printers. However, initial cost outlay for a laser printer can be considerably higher than a standard inkjet Office volume and cost expenditure will dictate which printer is best suited for the job. The one major limitation that still faces the conversion of on-screen to printed digital images concerns color correction. Projectors Scientific, marketing, and business conferences have attested to the advent of the digital revolution: increasingly, digital projectors are preferred to traditional slide projectors for effective communication. The ability to embed animation and video footage during a digital presentation has made the digital format an unquestionably superior medium of communication. Clearly, portability is important Storage Digital imaging permits infinite backup without the considerable expense associated with copying film transparencies or negatives. Backing up data should occur on a daily or weekly basis, and data should be stored both on premises and off site to ensure maximal protection. Many options exist for data storage including magnetic drives, magnetic-optical drives, optical drives, tape drives, and hard drives. Generally, tape and magnetic media are preferred for large storage backups, whereas optical media are better suited for smaller file-to-file storage. Output Devices Printers Three principal types of printers exist for photographic reproduction: inkjet, dye-sublimation, and color laser. Inkjet printers comprise the majority of printer sales and can provide high-quality print resolution. They function by spraying small amounts of ink onto the paper in halftones Chapter 171: Pictorial Documentation: Digital Imaging and Traditional Photography 2783 for someone seeking this option. If several computers are intended for use with one projector, then the projector should be matched to the computer monitor with the highest resolution. The contrast ratio that describes the range of brightest whites to darkest blacks is also a valuable feature with a range of 100:1 (low) to 2,000:1 (high). Zoom lenses permit image size adjustment without the burden of having to move the unit Digital keystone correction adjusts the image to reduce distortions that arise from aiming the projector at the wall from an angle. Lamp life can range from 40 to 40,000 hours, with the majority falling between 1,000 and 2,000 hours. Photographic documentation should always be obtained in any cosmetic or reconstructive endeavor but may also serve as a reliable tool for other types of head and neck surgical procedures on an individual case-by-case basis. The rise of digital photography has transformed the landscape of scientific and professional communication. Stallworth the biotechnology of implants in otolaryngology and head and neck surgery has expanded rapidly, and fadal, head, and neck implants now include autologous biomaterials, metals, polymers, synthetics, and tissue-engineered materials. Since the range of requirements for implants ranges from bone replacement and stabilization implants to soft tissue fillers, the sdence of surgical implantology now involves cell surface physics, molecular level biochemistry, and tissue engineering. Biomaterials, both biologic and synthetics, for osseous and soft tissue augmentation are becoming increasingly important in reconstructing defects of traumatic, congenital, extirpative. Well-differentiated cells, such as chondroblasts, osteoblasts, and epithelial cells, require substrate characteristics distinct from those needed by less differentiated cells, such as fibroblasts. Focal contacts represent adhesion sites to specific extracellular matrix proteins adsorbed on the implant surface. Focal contacts typically occur in low-motility cells, such as fibroblasts and epithelial cells. The composition of the substrate (the adsorbed layer of protein on the implant surface) is crudal for tight cellular adhesion. Proteins such as fibronectin, vitronectin, cold-insoluble globulin, and possibly proteoglycans provide the necessary substrate for this adhesion. The extracellular matrix contains collagen, elastin, and fibronectin interwoven into a hydrated network of glycosaminoglycan chains. The glycosaminoglycan chains are long, negatively charged polysaccharide chains that link proteins to form giant proteoglycan molecules. Interaction with cell membrane receptors provides linkage for cellular attachment to adsorbed extracellular matrix on the surface of a biomaterial. Tissue cells do adhere to the implant surface-not directly but by means of a complex series of protein attachments. When implants are placed in fadal soft tissue, the primary tissue reaction includes protein adsorption and cellular attachment. Within the first week, the fibroblast lays down immature collagen on the implant surface, or interstices. The usual response to a soft tissue implant is production of a fibrous capsule or collagen fiber ingrowth. A smooth implant such as silicone more often elidts dense capsule formation than does a porous implant If an implant is too reactive, has surface contamination, or is biodegradable, the host tissue response usually is aggressive macrophage activity, increased vascularity, breakdown of the overlying skin, and extrusion of the implant. The presence of inflammatory cells such as neutrophils and macrophages suggests poor tissue response to the implanted material. The first stage is formation of a small hematoma and a cascade of chemical breakdown products. Because cortical bone is avascular, most blood products come from the marrow-containing spaces of the bone. Extracellular processes and cell functioning can be affected by soluble and insoluble particles from the implant and by the mechanical influence of the implant itself. The third stage of repair is 2784 Chapter 172: Grafts and Implants in Facial, Head, and Neck Surgery 2785 remodeling, which affects the implant-host tissue interface and occurs over weeks or months. Appropriate stress levels must be imposed on the bone adjacent to the implant Bone-binding intensity can be measured according to the shear or torque forces needed to produce failure. Bone is the main contributor to tensile strength of bonding; other tissues are less important. The basal lamina in contact with a bone implant contains type N collagen, laminin, and proteoglycans. These constituents of the ground substance are deposited in or adjacent to the mineralized layer. Mineralization of the ground substance seems to be important for transmission of compression and for shear and tensile loads. Metallic Implants Metallic devices can be composed of a single metal or an alloy of several metals. Alloys are developed to improve qualities of the original metal by adding other metals with characteristics that improve biocompatibility or mechanical attributes. The principal metals used in facial implants are titanium, stainless steel, and tantalum. Metals are crystalline materials with well-defined, orderly, three-dimensional arrangements of atoms that form a microscopic lattice characteristic of each metal. The lattice can be modified by means of heating, cooling, hardening, or altering the physical properties of the metal to achieve a particular result. Metallic biomaterials are characterized by elastic modulus, tensile strength, percentage elongation, compressive strength, shear strength and modulus, and strain. Stress is the ability of a material to withstand a given load per cross-sectional area. The material must be designed to meet the functional requirements of the dental or maxillofacial implant. The properties of bulk material, however, can differ from those of the implant surface at the tissue-implant interface because of surface alterations by design or physicochemical reaction. The materials and clinical applications for facial, head, and neck implants are summarized in Table 172. They provide information about the bulk material independent of shape or thickness. These can be used to predict the response of the material to mechanical forces on an implant in a particular use. The forces of shear, compression, tension, torsion, and bending must be considered in selection of a material for an implant. In vitro loading studies are performed to assess how a material responds to long-term wear. Most metals relax with time, and the relaxation can cause metal fatigue and implant failure. A relatively brittle metal, such as stainless steel, can function well initially but with longterm use can fail because of fatigue. All metals corrode when exposed to living tissue; the gradual result is failure of many metal implants. Stainless steel, an alloy of iron, chromium, nickel, molybdenum, and manganese, resists corrosion well. Titanium and its alloys are among the most biocompatible metallic implants used today. It is rather soft and when not anchored to bone can be deformed by loading forces. Used in mandibular reconstruction and for anchoring screws in facial applications, titanium performs well. Tantalum and vanadium have been used as bone trays for mandibular reconstruction, but the mechanical properties are not as good as those of titanium. Tantalum and vanadium are not strong, can fatigue rapidly, and must be removed after the mandible heals. Some metallic implants, such as stainless steel, have a better stress response than does bone. Metal implants may have to be removed after the bone is stabilized to allow growth and development.
However medications ending in pam cheap careprost online american express, the supraclavicular skin is usually less sun exposed medications and grapefruit interactions purchase careprost line, creating a color discrepancy between the recipient skin and the skin graft medicine 2 times a day purchase 3 ml careprost free shipping. In addition medications for ocd purchase careprost 3 ml with visa, the supraclavicular skin can be much thicker than most facial ski~ and judicious thinning of the graft is usually required medicine keeper buy careprost 3 ml mastercard. There are occasions when skin grafts are used to repair defects even when it is anticipated that the graft will result in a contour depression or noticeable color discrepancy. These situations arise when caring for debilitated patients who have life-threatening illnesses. In addition, in patients who have malignancies showing aggressive growth patterns and tumor persistence or recurrence is a primary concern, skin grafts may be used as a temporary covering for a several years to facilitate tumor surveillance. Locations particularly amenable to skin grafting include the temple, medial canthus, philtrum, and portions of the nose. The ideal nasal defects perhaps most amenable to a skin graft are separated from the free margin of the nostril by 5 mL and located in thin-skinned areas of the nose, such as the cephalic sidewalls, cephalic dorsum, and infratip lobule. Shallow wounds in these areas are typically completely filled by a full-thickness skin graft, thereby establishing confluent contour with the surrounding skin. The areas of the nose covered with thicker skin tend to heal with a contour depression and noticeable textural discrepancies between graft and adjacent facial skin. This is because the facial skin in these areas tends to have a more sebaceous nature than the graft. If a full-thickness graft has been performed and a contour depression exists, the appearance can be improved by subsequent placement of a dermal fat graft after the skin graft has healed. Their technique involves the placement of dermal tissue in linear strips within the wound bed, leaving adequate exposure of the underlying wound bed to provide nourishment to an overlying skin graft (35). Defects located on the lateral nasal ala immediately adjacent to the nasal facial sulcus can be repaired with a number of options. If the defect extends into the cheek, the cheek component of the defect is usually repaired with a cheek advancement flap. The alar component can be repaired with a cheek or paramedian forehead flap if the defect is large. For smaller defects, especially in very young patients where preservation of regional flaps is desired, fullthickness skin grafts and composite grafts are considered for the alar portion of the defect. Full-thickness grafts are best suited for superficial defects not extending to the nostril border. In the case of deep alar defects, skin grafts do not lend any structural support, and subsequent nasal valve collapse may lead to compromise of the nasal airway. One option for patients with deep alar defects is the transfer of subcutaneous cheek tissue in the form of a hinge flap. The flap partially fills the defect and facilitates placement of an alar batten graft deep to the hinge flap. A full-thickness graft can then be placed as external covering over the hinge flap, thereby completing a single-stage reconstruction. When defects of the nasal sidewall extend to the medial cheek, the cheek component of the defect is reconstructed Chapter 173: Local Cutaneous Flaps and Grafts with a cutaneous advancement flap. The flap ia advanced and anchored in place at the nasal facial sulcus with deep sutures that pass from the medial border of the flap to the periosteum of the nasal sidewall. The cheek advancement flap facilitates positioning scars along the junctional zone between the aesthetic regions of the cheek and nose. Technique-Facial Cutaneous Grafts All patients undergoing skin grafting receive preoperative intravmous antibiotia, followed by 1 week of oral antibiotia. Additional beveling of the defect may be performed if the skin graft is substantially thinner than the depth of the recipient site. A template is made of the recipient site by outlining the periphery of the wound with a swgical marker and pressing a nonadherent dressing pad over the marking. If the defect is round, the shape is often modified by excising skin to create angulated bordm, which improves the contour outcome. In addition, movement and transfer of adjacent facial skin are performed if this is foWld helpful in isolating the defect to a single facial aesthetic unit. In addition, delay provides an improved vasallar recipient site for the graft (36), which ia especially important in areas of exposed periosteum or perichondrium. The acellular dermal graft wound matrix may be placed at the time of tissue resection, and wound care is dependent on the tJpe of acellular dermal graft employed. Following development of sufficient granulation tissue, any epithelium is removed prior to grafting and the tissue is cross-hatched so that myofibrils are released. A; Open nasal defect following Mohs excision of skin cancar~o nasal laxity; (B) preauricular donor site delineated; 2816 Section X: Facial Plastic and Reconstn. Chapter 173: Local Cutaneous Flaps and Grafts 2817 imbibition during the first 24 hours after transfer, followed by vascular inosculation. The graft is excised and all subcutaneous tissue is removed using curved scissors. The graft is transferred to the recipient site and secured with absorbable sutures as well as a bolster. A week or two later, when the graft has survived and is well adhered to the recipient site. If the entire graft dies, it will separate from the recipient site within several weeks. More commonly, the deeper portion of the graft will survive while the more superficial portion forms an eschar, which remains fixed to the wound bed. When this occurs, reepithelialization will occur from the wound edges and from the viable deeper dermal component of the graft Often, sufficient dermis survives to prevent the development of a depressed scar following complete healing; however, color and textural differences between facial skin and the graft are usually more apparent than when the graft survives completely. Adjunctive procedures to optimize aesthetic appearance may be performed after grafting. Resurfacing procedures for full-thickness skin grafts are an option, and usually most of the facial skin within the aesthetic units surrounding the graft is resurfaced as well. Facial Composite Grafts Composite grafts contain two or more tissue layers and often are unsuccessful secondary to high metabolic demands. They obtain their nourishment through plasma edges of the graft begins by the third day (38,39,40). Composite grafts were first described by Konig (41), who used composite auricular grafts to repair alar defects, noting a 53% graft survival. Composite grafts have been used to repair nasal columellar defects (42,43) and deficiencies in nasal lining (44). During the first half of the 20th century, Limberg (45) advocated the cavum and cymba of the concha as the preferred donor site for repair of the nose. Symonds and Crikelair (46) also used composite auricular grafts for nasal reconstruction, reporting an 89% graft survival rate. The auricle is an excellent source for composite grafts for facial reconstruction, especially for nasal defects, because it provides a contoured graft of skin and cartilage. Certain segments of the auricle loosely replicate the delicate topography of the columella. For both anatomic sites, the skin is tightly adherent to the underlying cartilage and/or fibrofatty tissue. Common auricular donor sites are helical crus, helical rim, antitragus, and fossa triangularis. The helical crus provides a good contour match for small alar rim defects and provides the option of incorporating in the graft a segment of preauricular skin. The traditional recommendation is to limit the size of composite grafts to 1 em or less (47). Considerably larger grafts may be successful if they are placed in a vascular recipient site and the graft is designed so that no portion is more than 1. Tills technique involves insetting the border of the graft between two layers of tissue at the recipient site (37). This method of graft attachment has the effect of increasing surface contact between graft and recipient site by 50% (51). A hinge flap developed at the recipient site also increases the surface area for attaching a composite graft (52). The use of perioperative corticosteroids is beneficial in enhancing survival of composite grafts in animals. Rabbits treated with preoperative and postoperative methylprednisolone demonstrated improved graft survival compared to animals receiving no steroids or postoperative doses only. Attempts to salvage compromised grafts with delayed administration of steroids were not successful (53,54). Cooling reduces biologic requirements and improves graft survival in irradiated, atrophic, or scarred recipient sites. Conley demonstrated that constant application of ice compresses for 14 days effected a fall in skin temperature from 3 8 oF to 17 oE Grafts ranged in size from 1 x 1 em to 2 x 2 em. Of twelve composite grafts transferred to the nose and treated with ice compresses, ten survived completely. Five of the grafts had been placed in recipient sites with scarring or postirradiation fibrosis (55). The nasal sldn in these areas is extremely thin, lacldng subcutaneous fat, and is tightly adherent to the underlying cartilage or fibrous connective tissue. Composite auricular grafts obtained from the helical crus provide grafts with thin sldn attached to a delicate segment of cartilage, providing structural support and sldn that closely resembles the adjacent nasal skin of the columella and facet Perhaps more commonly. Composite grafts can be used to maintain structural integrity at the nasal valve and provide a smooth continuous border to the alar rim. Weisberg and Becker describe the use of auricular composite grafts with stabilizing struts for repair of such defects. Complications include partial or complete graft loss, contracture, pigmentary changes, and contour abnormalities. Contour abnormalities may be addressed with a debulldng or scar revision procedures. Establishing a consistent perioperative routine is the first step in preventing complications. Appropriate preoperative counseling of the patient will reduce the likelihood of complications, and informed consent should include an open discussion of potential problems that may occur. Immediate and regular postoperative evaluations of the patient will facilitate early recognition and treatment of complications. Some complications are reversible, and expeditious treatment may prevent a reversible complication from becoming an irreversible one. Technique-Facial Composite Grafts Patient selection is an important consideration. The use of composite grafts is generally limited to small defects in patients who do not use tobacco and have no systemic illnesses that would compromise graft revascularization. Patients receive antibiotics and wound preparation similar to that described when performing sldn grafts. In addition, prednisone is administered on the day of surgery and a steroid taper is provided postoperatively. Improved survival rate is noted if grafting is delayed until the facial defect has partially healed by secondary intention. The facial defect is then prepared by removing any epithelium and subepithelial scar tissue, and a template is created that measures several millimeters larger than the defect in all dimensions. Harvesting a graft that is slightly larger than the defect accommodates for the inevitable contraction of the graft. Whenever possible, a flap of soft tissue hinged on a border of the defect is developed to enhance surface contact with the graft. A composite graft containing sldn and cartilage is harvested from the region of the auricle that most closely matches the contour and thickness of the nose at the defect site. The graft is placed in cold saline, and the donor site is dosed primarily using polydioxanone or poliglecaprone sutures to approximate the edges of the auricular cartilage and polypropylene sutures for the sldn. The graft is transferred to the recipient site and secured in place with simple absorbable sutures, limiting the degree of manipulation of the graft. Limiting the number of sutures used to fix the graft in place is thought to be beneficial in enabling earlier and more abundant vessel ingrowth. Successful grafts transition in color during the first week: blanched at initial transfer, pink color at 6 hours, darker by 24 hours, and gradual development of a pink color in 3 to Bleeding Common causes of bleeding from facial reconstruction using local flaps are drug-associated coagulopathy and inadequate hemostasis. Patients are questioned preoperatively concerning use of all prescription and over-thecounter medications that may contribute to perioperative bleeding. Bleeding may also be associated with hypertensive events, hepatic or renal failure, vomiting, straining, or alterations in the hematopoietic system. Bipolar electrocoagulation is used to control bleeding from smaller vessels and larger arterial vessels are securely ligated when interrupted. Drains are rarely used with local cutaneous flaps, with the exception of extensive cervicofacial flaps or ear reconstruction. A compression dressing that conforms to the anatomical contour of the surgical site to facilitate adherence of the facial flap to the recipient site is typically left in place for 48 hours. The dressing consists of nonadherent gauze, cotton balls, and expandable mesh tape. Patients are instructed to keep their head elevated, especially at night, for the first 48 hours after surgery. Hematomas may cause compromise of local flap vascularity by inducing vasospasm, stretching the subdermal plexus, or separating the flap from the surface of the recipient site (57 -59). Furthermore, iron compounds in a hematoma may promote free radical production leading to flap necrosis (60,61). Hematoma formation also predisposes to infection, which may compromise flap vascularity secondary to inflammatory edema (62,63). Small hematomas may sometimes be aspirated through the suture line using a syringe attached to a large-bore needle. If the hematoma recurs, it may be necessary to return the patient to the operating room for thorough drainage and irrigation. In that setting, the wound is opened at a dependent portion, the hematoma is evacuated, bleeding vessels are controlled, and irrigation is performed.
Thia problem can be prevented by repeatedly checking the tension on all sutures during surgery treatment 02 academy order careprost 3 ml on line. Reverse telephone ear can occur from overzealous tightening of the superior and inferior third of the ear treatment deep vein thrombosis careprost 3 ml purchase fast delivery. It is appropriate for use with patients who have only a small amount of antihelical cartilage medications for bipolar disorder buy careprost discount. Again medicine journals impact factor buy careprost 3 ml with visa, this technique requires an experienced surgeon and carries a recurrence rate of 4% (11) schedule 8 medications victoria order cheap careprost. Mustarde tflchnfque Advantages Very normal-appearing antihelical fold can be created, which sutures can hold indefinitely. Pitanguy tec:hnique Advantage Patient can have small amount of antihelical cartilage. Fuma canehill mastofd suture technique Advantage Permanent retraction of auricle is facilitated. Clinical Indicators for Plastic Repair of the External Ear Sttategy IndicatoiS (one of the following) Congenital or traumatic amputation. These clinical indicators are educational statements that have been drafted to assist surgeom in their practice and to promote discussion. The definition of microtia has been the subject of numerous publications, as clinidam have attempted to define the different grades that exist this section focuses on the grades of microtia for which swgeons can initiate surgical reconstruction with a high degree of success. Tanzer (12,13) published the first article on auricular reconstruction using autogenous rib cartilage in 1959. Shortly after, in 1966, Cronin (14) popularized the use of Silastic as an implant matf! The concomitant atresia complicates the classification schemes, yet many tty to include it as a critf! Gill also inco~porated into his system the degree of pneumatization of the mastoid because this finding seemed to predict the relative success of operative interventions. The Jahrsdoerfcr scale, based on temporal bone cr:findings, assesses nine different parameters that are used in making the determination of candidacy for swger:y. Fernandez stated that the stapes and oval window complex account for 3 out of 10 points possible. Scores of 6 through 10 range from marginal to excellent candidates for swgery, whereas a score of:five or less usually points to a poor outcome. In 1974, Rogers (18) published a classification 8 13tem that divided congenital auricular defects into four groups: 1. Macrotia Lopear Cup ear Prominent ear In 1977, Tanzer (19) proposed a clinical classification of auricular defects that has been well documented in virtually all articles that have been published since then: 1. Without atresia of the external auditoty canal Chapter 191: Congenital Auricular Malformation 3169 3. Prominent ear Weerda (20) from Europe in 1988 combined all of the classifications into a concise document. Definitions proposed by Marx and Tanzer and modified by Rogers (21) were presented. Average definition: Most structures of a normal auricle are recognizable (minor deformities). Surgical definition: Reconstruction normally does not require the use of additional skin or cartilage. Surgical definition: Partial reconstruction requires the use of some additional skin and cartilage (synonym: second-degree microtia [Marx]) A. Surgical definition: Total reconstruction requires the use of skin and large amounts of cartilage (synonyms: complete hypoplasia group n, peanut ear, third-degree microtia [Marx]); normally there is concomitant congenital atresia A. Unilateral: One ear is normal; no middle-ear reconstruction is performed on any child; auricle reconstruction is begun at age 5 or 6 years. Bilateral: Bone-conduction hearing aid before the fust birthday; middle-ear surgery at age 4 years without transposition of the vestige; bilateral reconstruction of the auricle at age 5 or 6 years C. Anotia these recommendations can be questioned, however, and there are alternatives. In addition, even in bilateral cases, middle-ear surgery can follow the fust two stages of auricular reconstruction rather than being the fust procedure (22). Surgical Reconstruction of Auricular Deformities In cases of congenital microtia and concomitant atresia, there should be complete coordination between the otologist and the plastic surgeon. Aguilar, in 1996, (17) presented the concept of the Integrated Auricular Reconstruction Protocol. The work of the plastic surgeon should be performed first, and the operation should be staged to facilitate total reconstruction of the microtia-atresia complex. Despite advances made in technique and imaging in recent decades, disagreement remains on several key issues: the prime time for surgery in general, when to operate on cases of unilateral atresia. Alao, moat clinidana think that surgery should be inatigated earlier in cues of unilateral atresia with evidence of cholesteatoma, infection. Opiniona differ in regard to cases of grade 0 and 10 unilateral atresia in patients with normal hearing in the other ear. Jaluadoe:rfer beli~ that the benefit of binaural hearing aceeds the riak of fadal neiVe injury and other complicationa. De Ia Cruz also favors early operationa on unilateral atresia& if cr findingB point to a favorable outcome. Bilateral microtia and atresia cases can be started at an earlier age, but only if sufficient costal c:a:rtilage exists to foJm a new ear. Neither irradiated cartilage nor Silastic baa stood the test of time: irradiated c:a:rtilage reabso:rbs, and Silastic t. Furthmno:re, Silastic implants are notorious for their inability to withstand ttauma In 1997, Williams etal. Animal model revealed that thae implants are well tolerated u replacements for nati~ cartilage in auricular reconstruction. Polyethylene implants tolerated wound exposure u early as 4 daya afte:r implantation and showed the ability to heal the&e wounds by secondacy intention and to support skin grafts. Authors surmised that this is because of the e:xtent of fibrovascular ingrowth from surrounding tissue, which allows the implant material to act more lila= native tissue and le! At the Univei5ity of Antwerp (Wdrijk) in the year 2000, Somers (24), at a Politzcr Society Meeting, described major breakthroughs in reconstructive surgery af the auricle, opening new possibilities in the rehabilitation of patients with an absent auricle. Somers reported on clinicians who had adopted 33 bo~anchored prostheses and performed 22 total auricular reconstructions. Postoperatively; patients were satisfied with their prosthesis and wore it all day without discomfort. The Brent technique was found to be safe with good results, but the modification by Nagata had two advantages: two operative stages inatead of four and a better definition of the reliefs of structure as the antihelix, aus anterior and posterio~ and antitragus tragus. Surgical Planning and Treatment Preoperative planning should include photographs of the patient Most important ia the proper preparation of the template. The site af implantation of the cartilage framework on the side of the head should be properly measured to avoid malpositioning af the ear. If radiologic aamination has not already been done, it should be ordered before swgery. Although a cr scan is unnecessary for the microtia, it does provide important anatomical information to the swgical team. Note that the dissection of the cartilage is atraperichondrial, and there is no stripping of perichondrium at any point during rib harvesting. Stainleaa-ated 5-0 wire ia wed to anchor the eighth rib to the sixth and a~nth rib complex. The most common complication that can oa:ur from stage I procedure is atelectasis; other complications include pleural tear (which should be appreciated intraoperatively in usual circumstances), pneumothorax, pneumomediastinum, chest wall aberration. To avoid protiWlion of the lobul~ the incision on the back of the ear should be f. The inferiorly based pedicle flap is quite thin; thus, great care should be taken in its handling. Moreovet the amount of scarring and the pouible compromise to blood ftow make complications harder to avoid. Complications Complications are possible during the swgical reconsuuction, as listed in Table 191. Placement of the cartilage graft causes severe strain on the overlying skin, which can cause skin necrosis. Finally, the possibility of keloid formation is higher when the graft is harvested from the abdomen or the buttocks. Complications can occur with each of the techniques described, even in the hands of experienced surgeons. Swgical correction of congenital microtia requires commitment by the facial plastic sw:geon, who should be performing more than five to ten operations per year to maintain proficiency. The team approach as described in this chapter is invaluable to the families; failure to offer this approach is a significant disservice to the patient. Many projects are being undertaken to develop biologic ear cartilage framework (26-29) for implantation. How~ the technology still has to overcome iasues such as tissue rejection and integrity of form. With the recent advances in composite tissue allotransplantation (30,31), it ia possible that patients may receive an ear transplantation in the future for severe defects. Chapter 191: Congenital Auricular Malformation 3175 · Every surgeon should learn multiple approaches to otoplasty to be able to offer each patient the best chance for success. Atresia repair should be performed after the plastic surgery, because this allows for the movement of the framework to the proper site. Presurgical confirmation of craniofacial implant locations in children requiring implant-retained auricular prosthesis. Use of a Silastic frame fur total and subtotal reconstruction of the external ear: preliminary report. Auricular repair with autogenous rib cartilage grafts: two decades of experience with 600 cases. Formation of tissue engineered composite construct of cartilage and skin using high density polyethylene as inner scaffold in the shape of human helix. During evolution, with the adoption of an upright posture and with verticalization of the face, the chin became an important facial feature. The events contributing to the evolutionary development of the chin in humans are open to speculation; however, the importance of the chin in the overall appearance of the face cannot be overstated (2). Facial beauty arises from symmetry and balanced proportion of all facial features. Although standards of facial beauty are often determined by social media and are time-adjusted, certain elegant features are not affected by time trends. For this reason, it is not surprising that no United States president has ever had a weak chin. A strong chin helps support the soft tissues of the lower face, and a well-projected chin improves the cervical skin and contributes to a well-defined cervicomental angle (3). It is important to analyze the chin in three dimensions in order to determine if the deformity is horizontal, vertical, or related to transverse discrepancy or asymmetry (4). Surgical correction of aesthetic deformities of the chin can be performed either by chin augmentation with an implant or by osteotomy and advancement (or reduction) of the bony mentum (5). More complex problems of the mentum, such as transverse asymmetry or significant vertical dysmorphia, usually require bony osteotomy of the mentum (genioplasty) with repositioning of the chin into a more ideal three-dimensional position. This article oudines the pertinent anatomy and classification of chin deformities and describes an algorithm for correction of these problems. Specifically, the chin should be evaluated as it relates to other skeletal and soft tissue structures, including the lips, teeth, nose, and soft tissues of the neck. A detailed history of past trauma, orthodontic treatment, or prior oral surgery is essential. This is important because many patients with dental malocclusion and underlying facial skeletal abnormalities are treated with orthodontics. It is also important to identify any past dental extractions, as these can impact future surgical decisions. Physical examination of the chin should include inspection and palpation of the chin itself and of the adjacent structures such as the lips, teeth, and nose (6). The entire face should be observed at rest and during animation to evaluate the mentalis soft tissue mound and its support. In many patients with either horizontal or vertical microgenia, the mentalis muscle hypertrophies in an effort to create lip competence (7). Evaluation of patients being considered for chin surgery should include three-dimensional analysis of the chin: (a) vertical (superior-inferior), (b) horizontal (anteriorposterior), and (c) transverse. Analysis should consist of systematic inspection, clinical photographs, and possible radiographic examination (8). If the ph:ysical evaluation and clinical photographa show a minor deformity requiring augmentation with an alloplast. The panoramic radiograph shows the cortical outline of the mandible and the vertical mandibular height the Panora also delineates the position of the tooth roots and of the inferior alveolar canals and mental foramina. It is important to know the exact position of the mental foramen and canal preoperatively so intraoperative damage to the mental neiVe can be prevented 9). The inferior alveolar nerve, a branch of the third division of the fifth (trigeminal) cranial nerve, travels through the mandibular canal and exits the mental foramen as the mental nerve (10). The mental nerve supplies sensation to the skin and mucous membranes of the lower lip and chin. The mandibular canal is often located 2 to 3 mm below the level of the mental foramen. Bony osteotomies should therefore be performed at least 5 mm below the mental foramen to avoid injury to the neurovascular bundle.
Purchase 3 ml careprost with visa. Heal Your Headaches Naturally - Top 10 Tips - Easy Recipes.
References
- Nyhan WL, Rice-Asaro M, Acosta P. Advances in the treatment of amino acid and organic acid disorders. In: Desnick RJ (ed.). Treatment of Genetic Diseases. New York: Churchill Livingstone; 1991, 45.
- Stein N, Sprenger C, Scholz J, et al. White matter integrity of the descending pain modulatory system is associated with interindividual differences in placebo analgesia. Pain. 2012;153(11):2210-2217.
- Chandrasoma P: Pathological basis of gastroesophageal reflux disease. World J Surg 27:986, 2003.
- Gunn SA, Gould TC: The relative importance of androgen and estrogen in the selective uptake of Zn65 by the dorsolateral prostate of the rat, Endocrinology 58(4):443n452, 1956.
- De Jonghe P, Timmerman V, Fitzpatrick D, Spoelders P, Martin J-J, Van Broeckhoven C. Mutilating neuropathic ulcerations in a chromosome 3q13-q22 linked Charcot-Marie-Tooth disease type 2B family. J Neurol Neurosurg Psychiatry. 1997;62: 570-573.
- Keyserling HF, Provenzale JM. Atypical imaging findings in a nearfatal case of posterior reversible encephalopathy syndrome in a child. AJR Am J Roentgenol 2007;188:219-21.
- Shackcloth MJ, Poullis M, Jackson M, et al. Intrapleural instillation of autologous blood in the treatment of prolonged air leak after lobectomy: a prospective randomized controlled trial. Ann Thorac Surg 2006; 82: 1052-1056.