
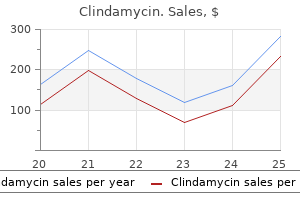
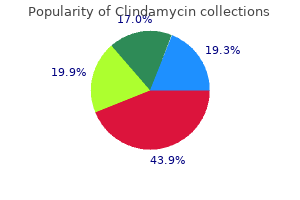
Clindamycin
| Contato
Página Inicial
Sean H. Rhyee, MD, MPH
- Assistant Professor of Emergency Medicine
- Division of Medical Toxicology
- University of Massachusetts Medical School
- Worchester, Massachusetts
- Formerly, Fellow, Medical Toxicology
- Rocky Mountain Poison & Drug Center
- Denver, Colorado
These molecules have essential functions for tissue integrity and intercellular communication antibiotics iv generic clindamycin 150 mg buy line. L1 can promote axon growth through both homophilic and heterophilic binding antimicrobial zone of inhibition evaluation trusted clindamycin 300 mg, and it is implicated in diverse processes such as myelination and migration bacteria 2 types generic clindamycin 150 mg overnight delivery, playing a role in synaptic plasticity antibiotics for sinus infection clindamycin buy clindamycin 300 mg on-line. Telencephalin may be involved in signaling specific subsets of growing axons to make proper synaptic connections antibiotic misuse cheap clindamycin on line. Agents such as inflammatory mediators and bacterial endotoxins can stimulate the endothelium to Integrins Integrins are a large family of membrane glycoproteins consisting of heterodimers between a and b subunits. By binding to the integrin b subunit, intracellular regulatory proteins talin and the kindlins can modulate the affinity of integrins for ligand binding. Cadherins Cadherins form zipper-like structures between adjacent cells via homophilic binding to other cadherins in a calciumdependent manner. Classic cadherins, such as the N-, P-, and E-cadherins, localize in adherence junctions to form an adhesion belt and build a connection with the actin-containing cytoskeleton. Cadherins are involved not only in cell-to-cell adhesion but also in morphogenesis and histogenesis. In the developing nervous system, cadherins are implicated in multiple functions in building neuronal structures. For example, N-cadherin plays roles in neurulation, the regionalization of neuroectoderm, neuronal migration, and axon growth and fasciculation. Recent studies indicate that cadherins are also involved in the development of sensory neurons, including visual and olfactory systems. Inflammatory episodes in the central nervous system are associated with the pathogeneses of a variety of neurological diseases, including ischemic brain injury and autoimmune neuropathies. Takeichi M (2007) the cadherin superfamily in neuronal connections and interactions. Selectins Selectins are cell surface lectins that have evolved to mediate the adhesion of leukocytes to endothelial cells and platelets under flow. Three selectins have been identified: L-selectin (leukocyte selectin), P-selectin (platelet selectin), and E-selectin (endothelial selectin). For example, Cell and Tissue Culture M Dragunow, University of Auckland, Auckland, New Zealand r 2014 Elsevier Inc. Introduction the development of various methods to culture cells from the brain, spinal cord, and other regions of the body has had a major impact on the neurological sciences. Cell and tissue culture studies of the brain and spinal cord are major contributors to the understanding of brain function and in particular have driven research into the pharmacological, electrophysiological, and biochemical aspects of neural cell function. These methods of cell and tissue culture have been developed and refined over many decades, providing a fundamental technique underpinning research in the biological sciences. For example, for pharmacological studies, cells can be exposed directly to test compounds without intervening pharmacokinetic factors altering drug response. For biochemical studies, homogenous cell populations can be easily collected and analyzed. Overall, cell and tissue culture allow for simplified and direct scientific experiments. Most cell culture of nervous system tissue uses the dissociated cell culture method, which uses a combination of mechanical and enzymatic cell dissociation. Some are simply based on adherence to the tissue culture flasks, size exclusion, and density centrifugation, whereas others use techniques such as magnetic cell sorting to isolate cells of interest using magnetically tagged cell surface-specific antibodies. Dissociated cells are generally maintained in special media with various supplements (including serum) that vary depending on the cell type being studied. For experiments, cells are often plated, once they reach confluency in the flasks, into microplates These sorts of methods have been the mainstay of cell and tissue culture techniques. Limitations of cell and tissue culture methods include the artificial nature of the cellular environment, for example, the use of artificial conditions to maintain cell viability and growth. In addition, the substrate used to grow cells can have a major influence on their biology, and therefore experimental results may vary depending on the conditions used to grow the cells. Because it is difficult to determine which cell culture conditions accurately model the intact tissue, the relevance of in vitro studies cannot be guaranteed. Furthermore, the simplified two-dimensional growth environment, although an advantage in many ways for pharmacological and biochemical analysis, is also a disadvantage as it does not model the in vivo situation. Three-dimensional cultures are now more widely used to try to model better cell life in the three-dimensional matrix of the brain interstitial environment, and importance of their use has been highlighted by observed differences in cell behavior and biology. There is a tradeoff with throughput, which is much higher in two-dimensional cultures. Furthermore, even three-dimensional cultures cannot model the complex three-dimensional cellular anatomy of the intact brain. To accomplish this, slice, organotypic, and explants cultures have been successfully developed to maintain and study in vitro anatomy and cellular complexity. Where interrogation of a single cell is desired and especially if the cell is in short supply, recently developed lab-on-chip methods may provide a powerful technology. These miniaturized methods not only allow cell composition to be studied but also allow released molecules to be assayed. Microfluidic devices that might one day allow for the addition of an array of compounds to different individual cells would greatly increase the throughput and applicability of these methods. One of the limitations of cell culture studies that utilize rodent tissue (majority of studies) for neurological research is that many are undertaken using brain tissue of embryonic or early postnatal animals. This is partly due to the high viability of cells derived from embryonic and early postnatal tissues. Thus, many in vitro models are generated from embryonic rodent tissue to model neurological disorders, many of which develop in the adult (or often aged) human brain. Clearly, great caution is needed when attempting to translate the results of such studies to human brain disorders. Recent studies suggest that even cultured astrocytes show marked biochemical (and presumably functional) variability depending on which brain region they are derived from. Thus, it is conceivable that a compound might affect hippocampal astrocytes differently to neocortical astrocytes, and care needs to be taken when generalizing results. Cell Lines Versus Primary Cells A major limitation of primary cell cultures is the yield of cells. To overcome this problem, cell lines have been developed that can be readily bulked. Of course, these cell lines generally express oncogenes that confer their immortality and 630 Encyclopedia of the Neurological Sciences, Volume 1 doi:10. Another potential problem with cell lines is that they invariably change with passage and also may become contaminated with other cell lines. Therefore, it is very important that cell lines are routinely characterized and validated to maintain their authenticity and that passage numbers are well documented. Cell lines have been successfully generated from embryonic tissues, although it has proved more difficult to immortalize brain cells from adults, and methods for this still need to be optimized. Cell lines provide an important tool for studying the signalling processes that underpin neural functioning, such as neurotransmitter receptor internalization, although it is always desirable to validate any effects observed in cell lines with studies using primary cells. Prolonged postmortem delay is a limitation for tissue culture studies, although some cell types, such as microglia, meningeal fibroblasts, and neural stem cells, are readily grown from postmortem brain tissue. Improved methods for isolating and maintaining such cultures are needed, as are methods such as lab-on-chip and single-cell biochemical analysis techniques for maximizing the information derived from human brain cell cultures. Inducible Pluripotent Stem Cells and Direct Production of Neurons From Peripheral Cells Recently, researchers have developed methods to generate large numbers of neurons and astrocytes from induced pluripotent stem cells derived from a range of peripheral tissues, although most commonly from skin fibroblasts. Even more recently, researchers using related methods have managed to convert fibroblasts directly to neurons, without a stem cell intermediate stage. These methods of cell engineering provide many opportunities for drug testing as well as for eventual cell therapy. These methods of generating neural cells from peripheral tissues are particularly suited to developing models of brain disorders with strong genetic components However, a major shortcoming of these methods and models, apart from the obvious artificial expression of gene cocktails, is that the derived cells (such as neurons and astrocytes) have a completely different context to those that they are trying to model. The recognition of noncellautonomous influences on degeneration in brain disorders This is where developing methods to culture from diseased adult human brain can be very useful to validate (or otherwise) studies generating neuronal and other cells from peripheral tissues. Adult Human Brain Cell Culture Perhaps the greatest application of in vitro cell and tissue culture methods, and one that has not yet been fully developed, recognized, or exploited, is the culture of cells from the adult human brain. The reason that such studies are vital is that failure to translate therapies from animal models to humans, which has plagued the neurological sciences in particular for neurodegenerative disorders, might be partly due to species differences. Indeed, there are many examples of species differences in cell culture studies, particularly between rodents (which comprise the bulk of cell culture studies) and humans. For example, rodent astrocytes proliferate in vitro, whereas human astrocytes derived from biopsy adult brain specimens do not. Although most studies utilizing human brain tissue generate dissociated cultures (mainly of microglia, astrocytes, and meningeal fibroblasts), slice culture methods have been successfully applied to postmortem human brain tissue. Furthermore, methods for the isolation, culture, and use of adult human brain cells from donors with neurological disorders provide disease-specific material both for examining the biochemical basis of brain diseases and for testing potential therapies. Another major advantage of studies from the human brain is that the variation between subjects is maintained and studied. This is very important because rodent cell culture studies take tissue from animals that have a very similar genetic and environmental (epigenetic) background. This is done to reduce biological variation so that when, for example, drugs are tested in such models, the variability in response can be more easily attributed to the intervention. This has obvious advantages, but the disadvantage of this approach is that most categories of brain disorders contain people with a wide variation in genetic and environmental (epigenetic) backgrounds. The source of the tissue for such adult human brain cell cultures is largely dependent on donated tissue from biopsy 632 Cell and Tissue Culture Neural Stem Cell Cultures the recent explosion of in vivo studies on neurogenesis has been mirrored by a similar explosion of in vitro studies. Neurosphere assays as well as the expansion and differentiation of neural stem cells in adherent cultures have generated a wealth of data on the factors that regulate the proliferation, survival, and differentiation (into neurons, astrocytes, and oligodendrocytes) of neural stem cells. This area is proving to be a fertile area of study and has provided a boost in the number of studies using in vitro techniques. In particular, in vitro neurosphere assays are widely used to quantify stem cells and evaluate the influence of various factors on neurogenesis. However, these assays must also be interpreted with caution as other cells, apart from true stem cells, can form spheres in vitro, including cells derived from many tissues of the body. However, to identify a neuron with certainty, patch clamping to show typical neuronal electrophysiological conductances is required. Cell culture platforms are also ideal for high-throughput drug screening and are amenable to robotics, allowing for the testing of chemical libraries containing millions of compounds. Methods of Interrogating Brain Cells in Culture A number of methods, such as gene arrays, reverse transcription polymerase chain reaction, Western blotting, immunocytochemistry, and patch clamping, are used routinely to measure electrophysiological and biochemical parameters in cultured brain cells. A large number of routine methods are also available for assessing cell viability. More recently, highcontent analysis methods have been developed for extracting complex information High-content analysis is particularly suited to the neurological sciences where phenotypic changes often involve morphological changes The combined technologies of brain cell culture and high-content analysis provide a powerful platform for studying mechanistic aspects of brain disorders and for screening molecules for eventual drug development for treating neurological disorders. Cell Characterization Using Cell Type-Specific Markers Fundamental to all cell and tissue culture studies is identification of the cell type(s) grown and used in experiments and in screening platforms. For example, default proliferating cells grown from adult human brain that undergo passage have been confused in some studies with adult human astrocytes, which are now known not to proliferate in vitro. Furthermore, markers such as nestin, which have been used to identify neural stem cells, are also expressed by other cell types in the brain and other organs. This means that immunostaining using antibodies to nestin cannot be used as a definitive marker of neural stem cells. Perhaps the best way to determine cell type is to use a number of markers and colabel cells. In addition to these types of control, it is also very important for researchers to verify immunocytochemical staining with Western blotting as cross-reactivity of primary and secondary antibodies can generate false-positives in immunocytochemical studies. Future Directions and Challenges the techniques of cell and tissue culture have and will continue to have major impacts on the neurological sciences. Direct cellular reprogramming to generate almost any cell of interest, including neurons, will have a major impact on drug screening and potential cellular therapy. New technologies for automating and bulk culturing allow for greatly increased throughput, which is especially important for drug screening purposes. Lab-on-chip nanotechnologies are greatly expanding cell and tissue culture methods and will be particularly important for intensively studying rare cells (such as those derived from neurologically normal and diseased adult human brains). As these techniques become more sensitive with increased throughput and are more readily available, they are likely to be widely used for research into neurological disorders. New materials and engineering methods are also being developed allowing for cellular patterning to model brain circuitry and predict the activity of neural networks. Other engineering-type methods are attempting to interface patterned neurons with computer technologies in the fields of artificial intelligence and robotics. In addition to these engineering-type and lab-on-chip approaches, it will also be very important to further develop and refine methods to isolate, grow, and study adult human brain cells from neurologically normal controls and from neurologically impaired brain material. These in vitro studies of adult human brain cells are likely to have a major impact on our understanding of the cell biology of the normal and diseased human brain. This work combined with methods to test compounds on such adult human brain cell cultures has an important place in drug development for neurological disorders. Methods of Manipulating Cells In Vitro In vitro cell cultures are excellent platforms for studying gene function by either expressing a gene of interest or knocking down a gene of interest. These types of studies have been very informative in determining normal gene function in neural cells as well as the function of mutant genes Cell and Tissue Culture 633 See also: Astrocytes. Stem Cells and Neurogenesis Further Reading Dragunow M (2008) the adult human brain in preclinical drug development. Gibbons H and Dragunow M (2010) Adult human brain cell culture for neuroscience research. Pastrana E, Silva-Vargas V, and Doetsch F (2011) Eyes wide open: A critical review of sphere-formation as an assay for stem cells. Rubakhin S, Romanova E, Nemes P, and Sweedler J (2011) Profiling metabolites and peptides in single cells. However, the point at which damaged cells become irreversibly injured, or dead, is surprisingly difficult to identify. Moreover, all cells die, and some cell injuries may merely hasten the aging process.
The acute treatment of hyperammonemic crises often involves hemodialysis in order to quickly reduce ammonia levels virus upper respiratory infection buy discount clindamycin 150 mg. Long-term management of urea cycle defects generally requires a protein-restricted diet virus 2014 fall 300 mg clindamycin order fast delivery, including replacement of natural protein with preparations of essential amino acids virus joint pain buy clindamycin 150 mg on-line. Administration of benzoate antibiotic bladder infection clindamycin 300 mg buy line, phenylacetate infection from antibiotics cheap clindamycin 150 mg mastercard, or phenylbutyrate increases the excretion of nitrogen by alternative routes. Treatment of seizures with valproic acid should be avoided because this drug may worsen hyperammonemia. Despite careful dietary and pharmacological treatment, the long-term prognosis for cognitive function in patients with severe urea cycle defects is poor. Liver transplantation is an option that may be employed to provide a source of hematopoietic stem cells with intact urea cycle function. Because these particular amino acids are not synthesized by human beings, many of these disorders may be effectively treated by carefully reducing the dietary intake of the relevant amino acid(s) and avoiding catabolism. Biotin can be used to treat multiple carboxylase deficiency due to either biotinidase deficiency or a partial loss of holocarboxylase synthetase activity. Because these amino acids are synthesized within the human body, restricting the dietary intake of the offending amino acid may not be sufficient to prevent disease progression. Thus, these disorders can be more difficult to treat than those involving essential amino acids. Further details of two of the main defects of catabolism of nonessential amino acids are given as follows: Tyrosinemia: Disorders of tyrosine catabolism include at least five different conditions. These may be ameliorated to some extent by restricting the dietary intake of both tyrosine and its precursor, phenylalanine. This compound prevents the accumulation of the toxic tyrosine metabolites, fumarylacetoacetate, maleylacetoacetate, and succinylacetone by blocking the catabolism of tyrosine at an earlier step. It may be possible to treat other metabolic disorders using the same general strategy of blocking a preceding step in the affected pathway. Later-onset forms cause milder symptoms including seizures, cognitive impairment, ataxia, chorea, and hyperactivity. Oral treatment with supplemental serine usually stops the seizures and ameliorates some of the other features of the disorder. Serine deficiency may also be caused by dysfunction of other enzymes in this biosynthetic pathway, including phosphoserine aminotransferase and phosphoserine phosphatase. D-1-pyrroline-5-carboxylate synthase deficiency D-1-Pyrroline-5-carboxylate (P5C) synthase catalyzes the reduction of glutamate to P5C, a critical step in the biosynthesis of proline, ornithine, citrulline, and arginine. Metabolic studies have shown these patients to have paradoxical preprandial episodes of hyperammonemia and low plasma levels of proline, ornithine, citrulline, and arginine. The connective tissue abnormalities might reasonably be attributed to the deficiency of proline, which is a major constituent of collagens. Disorders of Amino Acid Synthesis Serine deficiency Very few disorders of amino acid biosynthesis are known. These patients have congenital microcephaly and develop spastic quadriplegia, psychomotor retardation, and intractable seizures. The pathogenesis of these symptoms most likely involves not only a deficiency of serine in the brain but also deficiencies of various serine derivatives such as glycine, serine phospholipids, sphingomyelins, or cerebrosides. In the Amino Acid Disorders Disorders of Amino Acid Transport 145 Confirmation and further delineation of this fascinating syndrome await the identification of additional patients. Homocystinuria the biochemical pathway that humans use to synthesize cysteine serves simultaneously as the catabolic pathway for methionine and as a source of the important methyl donor Sadenosylmethionine. Homocysteine, an intermediate in this pathway, accumulates in each of the several forms of homocystinuria. Clinical features may include subluxations of the lenses of the eyes, intellectual impairment, psychiatric disorders, a marfanoid body habitus (long fingers and other skeletal abnormalities reminiscent of Marfan syndrome), fair complexion, and predisposition to thromboembolism, especially in the brain. A variety of specific transport mechanisms catalyze the movement of amino acids across biological membranes. Some of these transport proteins operate on groups of structurally related amino acids, whereas others recognize only one specific amino acid. These transport mechanisms may be specific to certain cell types and may even be localized to precise regions of the plasma membrane. For example, lysinuric protein intolerance is caused by deficiency of a dibasic amino acid transporter found on the basolateral membrane of renal and intestinal epithelial cells. When this transporter is defective, intestinal absorption and renal tubular reabsorption of lysine, arginine, and ornithine are impaired. Therefore, urinary excretion of these amino acids is high and their plasma levels are low. Patients with this disorder suffer from protein intolerance and episodes of hyperammonemia that result from having insufficient arginine and ornithine for proper functioning of the urea cycle. Other clinical features may include poor growth, osteoporosis, immune deficiencies, alveolar proteinosis, pulmonary fibrosis, or intellectual impairment. The occurrence of intellectual impairment is most likely related to the severity of the episodes of hyperammonemia. Treatment involves moderate dietary protein restriction and replacement of urea cycle intermediates through oral citrulline administration. Amino acid transport mechanisms may also be specific to certain subcellular organelles. For example, cystinosis is a lysosomal storage disease caused by mutations in a lysosomal membrane protein. The diagnosis of cystinosis can be made by demonstrating increased cystine content in lymphocytes. Treatment with cysteamine helps remove cystine from lysosomes through the formation of mixed disulfides (which are recognized by another transport protein) and slows progression of the disease, but kidney transplantation is often necessary. Chronic extrarenal manifestations may also occur, including ocular problems, hypothyroidism, diabetes, myopathy, or encephalopathy. Hartnup disease is inherited as an autosomal-recessive trait with a prevalence of approximately 1 in 30 000 people. These patients have decreased intestinal absorption and renal tubular reabsorption of many neutral amino acids including tryptophan. However, population screening suggests that the vast majority of patients with Hartnup disease remain asymptomatic. Human cells require nicotinamide, which may be synthesized from either tryptophan or niacin. Treatment with niacin has been reported to improve the symptoms of Hartnup disease in some patients, and it is likely that sufficient dietary niacin intake is one of the factors that accounts for the lack of symptoms in Hartnup disease. Defects in the metabolism of these compounds are discussed elsewhere in this encyclopedia. Patients with these autosomal-recessive creatine deficiency syndromes manifest similar neurological symptoms, including intellectual impairment, seizures, hypotonia, dystonia, and speech delay, along with autistic and autoaggressive behaviors. Treatment with oral creatine monohydrate gradually restores brain creatine concentrations to nearly normal levels and may result in significant clinical improvement, particularly in the context of an early diagnosis. Ammonia J Albrecht, Polish Academy of Sciences, Warsaw, Poland r 2014 Elsevier Inc. General Characteristics of Ammonia Metabolism in Mammals Peripheral Tissues the major proportion of ammonia in the circulating blood comes from urea and protein-derived amino acids that are degraded by large-bowel bacteria. In healthy individuals endowed with an intact, functional liver having undisturbed access to circulating blood, ammonia is effectively neutralized in the process of urea synthesis occurring mainly in periportal hepatocytes. However, skeletal muscles also avidly release ammonia to the blood, rendering their net contribution to ammonia clearance negligible. The incompleteness of the urea cycle in the brain renders amidation of glutamate to glutamine by glutamine synthetase as the only efficient way in which bloodborn ammonia is neutralized. The almost exclusive location of ammonia neutralization in astrocytes and the involvement of astrocytic-neuronal ammonia shuttle in neurotransmission are the key determinants of ammonia neurotoxicity. Hyperammonemic Encephalopathies Hyperammonemic encephalopathies encompass a heterogeneous group of diseases of different and often complex etiologies. Glu released from neurons is taken up by astrocytes where it reacts with ammonia to close the cycle. The blood ammonia burden in cirrhotic patients is aggravated by increased glutamine degradation to glutamate and ammonia in the intestinal and kidney tissues of these patients. The mutation gives rise to an increased number of glutaminase molecules and thus may enhance glutamine degradation and ammonia production. Other causes include overexposure to hepatotoxic drugs other than paracetamol (anesthetics, cordarone, isoniazid, heroin, cocaine, excess of vitamin A) and infections (brucellosis, congenital or tertiary syphilis). Mortality due to liver cirrhosis ranks notably high among the different causes of death. Ammonia induces astrocytic swelling by a vicious cycle of cytotoxic mechanisms encompassing oxidative stress (generation of free oxygen and nitrogen radicals), impairment of energy metabolism, and intracellular osmotic imbalance. There is extensive vacuolization (spongiosis) of the neuropil (crossed short arrows), prominent perivascular (short arrows), and perineuronal vacuolization (crossed long arrows), all features highly characteristic of swollen astrocytic processes. Ammonia also contributes to the increase in the inhibitory serotoninergic transmission by promoting the recruitment from blood to the brain of tryptophan, the amino acid precursor of serotonin. Metabolic traps such as phenylacetate, which combines with glutamine or benzoate that promotes formation of hippuric acid from ammonia, have been used to increase renal ammonia excretion in patients with urea cycle deficits. Cellular and Molecular Mechanisms of Ammonia Toxicity the mechanisms are extremely complex, because ammonia interferes with a large spectrum of metabolic processes in the See also: Astrocytes. In the past, amphetamines were used to treat a variety of conditions, including obesity, depression, hyperkinesis in children, or narcolepsy. Currently, methamphetamine is used for the treatment of attention-deficit hyperactivity disorder but, is also a commonly used street drug. An amphetamine derivative used as drug of abuse, methylenedioxymethamphetamine (ecstasy), is discussed separately. Amphetamines and methamphetamine are available as powder, capsules, tablets, or fluids, and as such they can be swallowed, snorted, injected intravenously, or smoked. Main effects of acute administration are wakefulness, decreased sense of fatigue, elevation of mood, self confidence, increased ability to concentrate, increased physical performance, elation, and euphoria. Amphetamine also increases the rate and depth of respiration and suppresses appetite by acting in the lateral hypothalamic feeding centers. The acute toxic effects of amphetamines are usually an extension of the pharmacological effects. They may include restlessness, dizziness, tremor, irritability, insomnia, confusion, anxiety, delirium, and hallucinations. Such psychotic aspects may be due to an increased release of serotonin from nerve terminals, or to direct effects on serotoninergic neurons. Chronic exposure to amphetamine or methamphetamine can lead to significant toxic effects on the dopaminergic and serotoninergic systems, as evidenced by animal and human studies. These include loss of amine transporters, decreased dopamine and serotonin levels, and loss of other dopaminergic or serotoninergic markers. Methamphetamine has been shown in animal studies to damage dopaminergic neurons, and this would predispose to parkinsonism, although this hypothesis has not been demonstrated in humans. The mechanisms underlying the degeneration of dopaminergic terminals have been proposed to be related to the ability of methamphetamine to cause the release of dopamine. Released dopamine can undergo enzymatic and nonenzymatic oxidation, which can result in the formation of reactive oxygen species. Thus, oxidative stress would be the key mechanism of neurotoxicity, and this is supported by findings that antioxidants attenuate the effects of methamphetamine. Another hypothesis is that methamphetamine-induced release of dopamine and serotonin leads to the formation of known neurotoxic moieties such as 6-hydroxydopamine and 5,7-dihydroxytryptamine. The former has been detected in rat brain following methamphetamine administration. Norepinephrine Further Reading Buttner A (2011) Review: the neuropathology of drug abuse. It has a similar position in nonprimates, such as rats and cats, in which the temporal lobes are not as well developed. The amygdala in all mammals is anatomically complex, consisting of numerous nuclei that often merge with their neighbors as well as with adjacent nonamygdalar regions. It is customary to categorize the amygdalar nuclei into groups that exhibit distinctive anatomical or functional characteristics. Recent studies, however, indicate that the central and medial nuclei exhibit anatomical and histochemical characteristics that are distinct from those of the rest of the corticomedial group. Therefore, here the amygdalar nuclei will be divided into three main groups: the basolateral, cortical, and centromedial nuclear groups. In addition, attenuated portions of the centromedial nuclear group extend forward (along the main fiber pathways associated with the amygdala) to become continuous with a brain region called the bed nucleus of the stria terminalis, which is located in the septal region adjacent to the anterior commissure. Cell Types and Neurotransmitters the cell types in the basolateral and cortical nuclear groups are very similar to each other. Most of the neurons in both groups are termed pyramidal cells because they resemble the pyramidal neurons in the cerebral cortex. They have large pyramidshaped cell bodies and dendrites that exhibit a dense covering of dendritic spines. The latter structures are in synaptic contact with incoming axons from the cerebral cortex and thalamus. In addition, local branches of pyramidal cell axons synapse with neighboring pyramidal and nonpyramidal neurons. Pyramidal cells are thought to utilize the amino acid glutamate as an excitatory neurotransmitter. The remaining cell types in the basolateral and cortical nuclear groups are nonpyramidal neurons.
However antibiotics you cannot take with methadone order clindamycin on line amex, stereotactic biopsy targets based on preoperative imaging may be altered when compared with the presteroid images antibiotic for staph proven clindamycin 150 mg. Preoperative use of corticosteroids should be avoided in patients suspected of Pain Headaches are common in patients with brain tumors and typically reach peak intensity on awakening antibiotics for dogs for dog bites clindamycin 150 mg order overnight delivery. Restriction of drugs that alter platelet function (nonsteroidal anti-inflammatory drugs) is important to preclude excessive problems with operative control of bleeding infection lymph nodes purchase clindamycin american express. The choice of operative procedure for resection of a neuroepithelial tumor depends on its location infection after dc 150 mg clindamycin buy mastercard, size, gross characteristics, histological characteristics, the sensitivity of the tumor to radiation, and the preoperative neurological and medical condition of the patient. Contemporary neurosurgical methods, including frameless navigational systems, intraoperative imaging, ultrasonography, and functional mapping enable the neurosurgeon to achieve optimal cytoreduction of the tumor with minimal postoperative neurological morbidity. Biopsy Diagnostic biopsy is most often accomplished with a closed stereotactic procedure performed in a patient under a general anesthetic. The use of image-guided stereotactic biopsy techniques allows optimal acquisition of diagnostic tissue material with low rates of morbidity and mortality. As physiological neuroimaging techniques increasingly facilitate targeting of the most representative portions of the intracranial tumors, the diagnostic yield from stereotactic biopsies is likely to continue to improve. In current practice, stereotactic biopsy is limited to a subgroup of patients harboring suspected glial tumors, depending on the characteristics of the lesion. For example, depth, small size, multiplicity, diffuseness, or the clinical condition of the patient can all suggest a stereotactic biopsy. However, an incorrect pathological diagnosis is not unusual in cases of tumors of glial origin, and the misdiagnosis usually consists of misinterpreting a high-grade glial tumor as a low-grade glioma. Although the incidence of this problem varies in different series, it may be significantly reduced by serial sampling along the entire radius of the lesion and beyond. Close collaboration with an experienced neuropathologist is essential to the diagnostic efficiency of stereotactic biopsies. Importantly, the only randomized clinical trial comparing stereotactic biopsy versus microsurgical resection for the initial management of patients with gliomas demonstrated a significant survival benefit in favor of surgical resection. Anesthetic risks such as cardiac, pulmonary, and metabolic disturbances need to be determined and treated if necessary. Other conditions that could increase the risk of surgery such as bleeding problems, infections, or any other baseline illnesses should also be diagnosed and treated appropriately. Brain relaxation from hyperventilation, osmotic diuretics, and cerebrospinal fluid drainage can be critical for controlling intracranial pressure and preventing unintended injury. Appropriate use of these options requires planning and communication with the anesthesiologist so that the patient is protected. Patients undergoing motor or language mapping of the brain during an awake craniotomy require specific attention to comfort and access so that the appropriate information can be obtained in a cooperative patient. Several surgical instruments and monitoring devices have been applied to tumor surgery to facilitate tumor identification and resection at the tumor margin with surrounding brain and to map primary motor, sensory, and language cortices. Stereotactic localization with frameless systems has gained almost universal acceptance at major brain tumor centers for comparing intraoperative findings with preoperative imaging. Alternatively, intraoperative ultrasonography remains a helpful adjunct in localizing subcortical tumors obscured by the normal cortical surface. The operating microscope is an essential tool for tumor surgery, providing optimal illumination and magnification to help identify variations in color, texture, and vascularity that can help distinguish tumor from brain. Another essential instrument for actual tumor removal is the ultrasonic aspirator. Intraoperative neurophysiological monitoring with somatosensory-evoked potentials for identification of the primary sensory cortex, Rolandic sulcus, and motor cortex is commonly used when lesions bordering the somatosensory cortex are resected. Intraoperative stimulation mapping of cortical and subcortical tissue in and around a tumor will identify functional tissue, and its preservation will minimize the risk of permanent postoperative deficits. Resection of tumor located near or within functional brain areas may not be safe even if the surgeon remains within the radiographic boundaries of the tumor. In addition to its use to determine functional cortical sites, stimulation mapping is the only available method that provides reliable identification of descending subcortical motor, sensory, and language tracts. Because of the tendency of infiltrative gliomas to invade underlying white matter tracts, it is important to identify both cortical motor sites and their descending pathways. Regardless of the gross appearance and consistency of the tumor, functional tissue may also reside within the mass itself and must be identified with stimulation mapping before definitive resection. For intraoperative mapping, the patient is placed in the position appropriate for the area to be exposed. An intravenous propofol or alfentanil drip maintains the sedative-hypnotic anesthesia. Oxygen is administered through a nasal cannula in case of a decrease in arterial oxygen saturation. Prophylactic antibiotics are used routinely and are given during the induction phase of anesthesia. As always, a preoperative pause by the surgical team is necessary to confirm the operative site before incision. The area of the scalp around the incision is infiltrated with a local anesthetic consisting of lidocaine (0. The craniotomy should be sufficient to expose the tumor and, in some cases, the surrounding brain, including areas where language is likely to be located, providing adequate cortex for language mapping. For patients with an intractable seizure disorder, electrocorticography is often performed before tumor resection. In appropriate patients recording along the hippocampus is obtained after removal of the lateral temporal cortex and entry into the temporal horn of the lateral ventricle. Strip electrodes can also be used for the orbitofrontal cortex or under the bone flap if the cortical exposure is inadequate. After the dura is opened, stimulation mapping should begin by first identifying the motor cortex. A constantcurrent generator is used to produce biphasic square-wave pulses at 60 Hz and a 1. The current necessary to evoke motor movement depends on the anesthetic condition of the patient, with lower currents used when the patient is awake. The motor strip is stimulated with the patient asleep at a starting current of 4 mA, which is then reduced to 2 mA when stimulating with the patient awake. The amplitude of the current is adjusted in 1- to 2-mA increments until motor movements are identified. The use of multichannel electromyographic recordings, in addition to visual observations of motor movements, improves sensitivity, permitting the use of lower stimulation levels to evoke motor activity. It has never been necessary to use a current above 16 mA to evoke a sensory or motor response. Its application abruptly stops seizure activity originating from the irrigated cortex without using shortacting barbiturates. After the motor cortex has been identified, the descending tracts may be found using similar stimulation parameters. Descending motor and sensory pathways may be followed into the internal capsule and inferiorly to the brainstem and spinal cord. This process is especially important during resection of infiltrative glial tumors because functioning motor, sensory, or language tissue can be located within macroscopically obvious tumor or surrounding infiltrated brain. Determination of the subcortical pathways is important when removing a deep tumor within or adjacent to the corona radiata, internal capsule, insula, supplementary motor area, and thalamus. Because current spread from the electrode contacts is minimal during bipolar stimulation, resection is stopped when movement occurs or paresthesias are evoked. Cortical language localization, through object naming and reading, varies across individuals and does not follow any reproducible pattern across the population. This concept was challenged by some early studies in which electrocortical stimulation was used. Thus, after bone removal under propofol anesthesia, these patients are kept awake during language mapping. The electrocorticography equipment is placed on the field and attached to the skull after the motor pathways have been identified. The presence of such after-discharge potentials indicates that the stimulation current is too high and must be decreased 1 or 2 mA until no after-discharge potentials follow stimulation. Using this ideal stimulation current, object-naming slides are presented and changed every 4 s. To ensure that there are no stimulation-induced errors in the form of anomia and dysnomia, each cortical site is checked three times. All cortical sites essential for naming are marked on the surface of the brain with sterile numbered tickets. Consistent application of this protocol vastly improves the reliability of a negative stimulation map. However, with the exception of those brain tumor surgeons whose specialized practices routinely employ intraoperative mapping, a generous exposure is necessary to enable stimulation of a positive control, typically along the motor cortex. A final postresection stimulation of cortical sites should be performed to confirm that the pathways are intact. It also ensures that the underlying functional tracts have been preserved if subcortical responses have not been obtained. The distance of the resection margin from the nearest language site is the most important factor in determining improvement in preoperative language deficits, the duration of postoperative language deficits, and whether the latter are permanent. Significantly fewer permanent language deficits occur if the distance from the resection margin to the nearest language site is more than 1 cm. One of the largest studies till date reviewed 500 consecutive, newly diagnosed glioblastoma patients treated with standard adjuvant therapy regimens after image-guided microsurgical resection. In our practice, the extent of resection is based on the functional nature of the tissue, not on its perceived biological aggressiveness. Prognostic Significance of Surgery Seizure Control In evaluating the efficiency of surgery for brain tumors, seizure outcome, quality of life, and survival rates appear to be the most important criteria. In such cases, removal of the tumor alone usually controls the epilepsy, with or without the need for additional anticonvulsants. However, younger patients with indolent tumors may have seizure activity that is refractory to medical therapy. The literature suggests that acceptable seizure control may be achieved with lesionectomy alone in patients with tumor-associated epilepsy. Serial electroencephalographic analysis has documented that independent seizure foci may lose their epileptogenic activity after various lesions are excised. Results of published studies do not support the use of electrocorticography during tumor resection to maximize control of epilepsy associated with a tumor. Extent of Resection the contemporary literature is increasingly instructive in understanding the value of microsurgical extent of resection. Introduction Primary benign and malignant brain tumors are common and occur with an incidence of 12. Intracranial neoplasms, or new tissue growths, represent the most common solid tumors in children younger than 15 years of age. Sporadic Brain Tumors the initiation and progression of brain tumors is associated with a variety of molecular genetic alterations. Oligodendrogliomas are tumors composed predominantly of neoplastic oligodendrocytes. They are most commonly located in the cerebral white matter and deep gray structures. Oligodendrogliomas have a lesser tendency to undergo malignant transformation than astrocytomas. They are thought to arise from the ependymal or subependymal cells surrounding the ventricles, the central canal, or within the filum terminale. Loss of chromosome 6p is common in the pediatric ependymoma, in addition to 17p and 22q abnormalities. Common genetic abnormalities in medulloblastomas are gains of portions of chromosome 1 and deletion of 1q, 6q, 11p, and 16q. Glial Tumors Gliomas are a heterogeneous group of mostly sporadic neoplasms derived from glial cells. Depending on their morphology and histology, gliomas are classified into several subgroups, the most important being astrocytic tumors (including the glioblastoma), oligodendroglial tumors, mixed gliomas (oligoastrocytomas), and ependymal tumors. Pilocytic astrocytomas constitute a separate clinical and histopathological entity and are the most common astrocytic tumors in children. Meningiomas the meningioma is a tumor composed of neoplastic meningothelial (arachnoid) cells. Several histological variants are recognized, such as meningothelial, fibrous (fibroblastic), transitional, and psammomatous meningioma. The frequency of meningioma increases with advancing age, and meningiomas are more common in women. Although meningiomas are frequently attached to the dural membranes, they may occur in unusual sites, such as within the ventricular space. Other chromosomal abnormalities associated with tumorigenesis and increased grade of meningiomas include loss of heterozygosity for chromosome 1p, loss of 14q, deletion of 9p21, and abnormalities of chromosome 10 and 17q. Radiation-induced meningiomas are more often multiple and have higher recurrence rates than standard meningiomas. Schwannomas Schwannomas are encapsulated and sometimes cystic tumors composed of spindle-shaped neoplastic Schwann cells. Vestibular schwannomas are also referred to as acoustic schwannomas or neuromas and commonly occur as single tumors on the vestibular branch of the eighth cranial nerve. Brain Tumors and Inherited Tumor Syndromes Brain tumors may occur as part of known inherited cancer syndromes. However, the majority of these tumors are asymptomatic and show little progression. Gliomas may also occur less frequently in the brainstem and hypothalamus, and they rarely occur in the cerebellum or the spinal cord.
Unlike the nuclei of the basolateral and cortical nuclear groups antibiotic resistant virus in hospitals cheap 300 mg clindamycin with amex, the cell types of the centromedial group do not resemble those of the cerebral cortex antibiotic for diverticulitis buy 300 mg clindamycin amex. Neurons in the lateral part of the central nucleus have ovoid cell bodies and dendrites with an extremely dense covering of dendritic spines antibiotic 600 mg buy genuine clindamycin on line. They closely resemble the medium-sized spiny neurons of the adjacent caudate and putamen bacteria 4 pics 1 word best order for clindamycin. Neurons in the medial nucleus and medial part of the central nucleus are spiny bacteria mod 151 clindamycin 150 mg order amex, but they have a lower spine density than neurons in the lateral central nucleus. Although most of the spiny neurons in the centromedial amygdala are probably projection neurons that send axons to other brain regions, other aspiny neurons have been seen that may function as interneurons. In general, it appeared that these amygdalectomized monkeys exhibited a specific type of visual agnosia characterized by the inability to recognize the emotional or behavioral significance of sensory stimuli. Subsequent studies revealed that animals with amygdalar lesions also did not respond appropriately to auditory, somatosensory, and olfactory cues. Thus, it appears that the amygdala is critical for producing appropriate behavioral responses to biologically relevant sensory stimuli and events in the external world. In fact, the amygdala is thought to constitute an essential link between brain regions that process sensory information The cortical and medial nuclei receive olfactory information from the olfactory cortex and the main and accessory olfactory bulbs. The latter structure is part of the vomeronasal system, which is involved in detecting special odors (pheromones) that are produced by individuals of the same species. Pheromones elicit hormonal and behavioral responses involved in species-specific reproductive and social activities. The amygdala receives visual and auditory information from the temporal lobe, somatosensory and viscerosensory (including gustatory) information from the insular lobe, and polysensory information from the prefrontal cortex and hippocampal region (including the subiculum, cornu Functional Anatomy of the Amygdala In a classic study performed in 1939, Kluver and Bucy found that bilateral lesions of the amygdalar region rendered monkeys remarkably tame and hypoemotional. These nonolfactory inputs primarily target the basolateral and, to a lesser extent, centromedial amygdala. The basolateral, but not the centromedial amygdalar nuclei, have reciprocal projections back to these same cortical regions. It has been suggested that these amygdalocortical projections may be important for attention to emotionally and behaviorally significant stimuli and for the storage of emotional memories. Connections with Subcortical Brain Regions the amygdala has connections with several subcortical regions, including the basal forebrain, diencephalon, and brainstem. Others course in a thin fiber bundle termed the stria terminalis, which takes a more circuitous route dorsal to the internal capsule. Projections from the dorsal thalamus to the amygdala arise mainly from the midline thalamic nuclei and medial part of the medial geniculate nucleus and adjacent posterior thalamic nuclei. These projections, which terminate primarily in the basolateral and central amygdalar nuclei, convey auditory, somatosensory, viscerosensory, and visual information to the amygdala. Amygdalothalamic projections are more limited and consist of projections from the central nucleus to the midline thalamic nuclei and from the basolateral amygdala to the mediodorsal thalamic nucleus. Because the latter nucleus has extensive reciprocal connections with the prefrontal cortex, it provides an indirect link by which the amygdala can influence the activity of the prefrontal region. In each of these affective states, the amygdala appears to elicit a coordinated response consisting of autonomic, endocrine, and behavioral components by way of its projections to various subcortical regions, especially the hypothalamus. Interestingly, many of the hormones secreted by the glands targeted by pituitary hormones can affect the activity of the amygdala via receptors expressed by amygdalar neurons. Thus, there is a very high density of estrogen and androgen receptors in the medial and cortical nuclei. Glucocorticoid receptors are located in all portions of the amygdala, but particularly high levels are found in the centromedial nuclear group. All connections are reciprocal except those to the caudate and nucleus accumbens, which do not have projections back to the amygdala. Lesion studies indicate that the projections of the basolateral amygdala to the striatum are important for controlling behavior related to the reinforcing properties of sensory stimuli. The central nucleus is the main amygdalar region exhibiting connections with the brainstem and basal forebrain. Among these targets are several brainstem areas involved in visceral function, including the parabrachial nucleus, dorsal vagal nucleus, and nucleus solitarius. It also has projections to the periaqueductal gray and reticular formation, which are important for pain modulation and behavioral responses to stress. In addition, the central nucleus innervates several brain regions that give rise to neurotransmitter-specific fiber systems that target the amygdala and other forebrain areas. These regions include the locus ceruleus (which provides a noradrenergic innervation of the amygdala and cortex), substantia nigra and ventral tegmental area (which provide a dopaminergic innervation of the amygdala and striatum), raphe nuclei (which provide a serotonergic innervation of the amygdala and cortex), and nucleus basalis (which provides a cholinergic innervation of the amygdala and cortex). The latter region is also innervated by portions of the basolateral nuclear group. These transmitter-specific systems are activated in certain behavioral states, particularly during stress, and can modulate amygdalar activities related to emotion, attention, and memory. Functional and Clinical Significance of the Human Amygdala Consistent with the results of animal experiments, recent investigations of the human amygdala have shown that it is critical for the recognition of the emotional significance of auditory, visual, and olfactory stimuli, including facial expressions, vocal intonation, and expressive body movements. It has also been demonstrated that electrical stimulation of the human amygdala elicits fear, rage, or other emotions. Investigations in humans have shown that the amygdala is important for learning conditioned emotional responses (usually fear) to sensory stimuli and events. These findings are in agreement with results of numerous animal studies showing that the amygdala is essential for Pavlovian fear conditioning to simple sensory cues and complex sensory representations, such as the context in which an emotional event has occurred. Additional investigations in humans and animals have demonstrated that the release of noradrenaline in the amygdala is essential for the formation and recall of memories involving emotional events. The amygdala exhibits degeneration in schizophrenia, and recording studies have detected abnormal activity in the amygdala in this condition. There is evidence that dopamine levels are increased in the amygdala in schizophrenia and that this brain region may be one of the main sites of action of atypical antipsychotic drugs Consistent with numerous rodent studies implicating the amygdala in fear and anxiety, there is evidence that anxiety disorders in humans, such as posttraumatic stress disorder, are associated with excessive activity in the amygdala. Moreover, studies in animals and humans have shown that the amygdala has very high levels of benzodiazepine receptors, which is critical for the anxiolytic actions of these drugs. Recent positron emission tomography investigations have demonstrated that there is increased activity in the human amygdala in major depression and that administration of antidepressive medication, which modulates levels of noradrenaline and serotonin in the amygdala, causes a decrease in amygdalar activity that is associated with amelioration of depressive symptoms. This article is a revision of the previous edition article by Ming Cheng, Kris A Smith, volume 1, p 128, r 2003, Elsevier Inc. Amygdalohippocampectomy is a cranial surgery for seizure control that selectively removes the mesial temporal lobe structures with minimal resection of the lateral temporal cortex. Unlike the standard temporal lobectomy, amygdalohippocampectomy is designed to remove only the portion of the temporal lobe that is generating the seizures. The hippocampus contains neurons with specific properties that create an especially low threshold for neuronal damage. When damaged, these cells and cells in the nearby amygdala become the focus of temporal lobe seizures. This condition is known as mesial temporal sclerosis, even when the original damaging events to the hippocampus may have occurred many years previously. By removing the mesial structures only, the surgeon decreases the risk of injury to areas involved with language, cognition, and vision. Failure of seizure control after an amygdalohippocampectomy may be caused by bilateral seizure foci, misdiagnosed temporal neocortical epilepsy, or an extratemporal seizure focus. An approach to remove the amygdala and anterior 3 cm of the hippocampus alone was described as early as 1958 with good seizure control and neuropsychological outcomes. However, the technical difficulty of the procedure led to its abandonment, especially in the setting of successful outcomes of the anterior temporal lobectomy. As microneurosurgical techniques advanced, surgeons developed new methods to perform the amygdalohippocampectomy. Yasargil and Wieser introduced the transsylvian technique in which dissection of the sylvian fissure and a small incision in the temporal stem at the limen insula spared the optic pathways. However, this incision at the temporal stem disconnected tracts between the frontal lobe and the lateral temporal structure. Niemeyer, Bello, and Olivier described a lateral transtemporal corticectomy to reach the temporal horn and mesial temporal structures. Although this approach was less technically demanding, it requires transection of functional temporal cortex. The subtemporal approach allows resection of the mesial temporal lobe structures while minimizing transection of normal temporal lobe and disconnection via the temporal stem. Over the past 10 years at Barrow Neurological Institute, Phoenix, Arizona, a minimal access subtemporal amygdalo- hippocampectomy to treat patients with mesial temporal sclerosis has been used. The use of frameless stereotactic magnetic resonance imaging guidance allows identification of the trajectory to the tip of the temporal horn of the lateral ventricle and a cortical incision into the fusiform gyrus or collateral sulcus. Entry into the temporal horn allows identification of anatomical landmarks of the posterior inferior surface of the amygdala as well as the choroidal fissure overlying the hippocampus. Ultrasonic aspiration is used to resect the uncus, amygdala, hippocampus, and parahippocampal gyrus posteriorly to the plane of the collicular plate. Based on neuropsychological testing, most patients who underwent this surgery demonstrated either stable or improved verbal fluency and visual memory scores. Although memory declined in a small portion of the patients because the hippocampus was removed, testing 8 months later showed significant improvement in their contralateral memory ability. Functions involving extrahippocampal structures such as cognitive efficiency and executive functioning appeared to benefit many patients who have significantly improved test scores at delayed follow up. Even with slightly different approaches performed at multiple centers, amygdalohippocampectomy has been demonstrated to be a safe and efficacious treatment for medically refractory temporal lobe epilepsy caused by mesial temporal sclerosis. The minimally invasive subtemporal approach is preferred for maximum preservation of cognitive function as well as a small and cosmetically pleasing incision. Amyloidosis and Amyloid Proteins the term amyloidosis refers to a heterogeneous group of disorders characterized by the extracellular deposition of insoluble fibrils in different tissues and organs leading to cellular damage, organ dysfunction, and eventually death. Clinically, amyloid diseases can be classified as systemic (when several organs are affected by amyloid deposits) or localized (when amyloid lesions are restricted to a single organ or tissue). Amyloid fibrils are composed of self-assembled, low-molecular weight peptides usually representing fragments of larger precursor molecules physiologically present in body fluids. In humans, 24 different proteins are known to self-assemble and form fibrillar amyloid structures. As shown in Table 1, their precursor molecules are totally unrelated proteins codified in different chromosomes and exhibiting a wide variety of biological functions. Despite these differences, all amyloid proteins share a number of biochemical and structural properties. Collectively, they are products of normal genes, although several amyloid precursors have been shown to contain abnormal amino acid substitutions that can impose an increased potential for selfaggregation. In general, amyloids are rich in b-pleated sheet secondary structure, a conformation largely responsible for their high tendency to aggregate and polymerize and for their tinctorial characteristics with Congo red or thioflavin S. All these molecules selfassemble into long, unbranched, B8-nm-wide twisted fibrils that are highly insoluble and show poor antigenic properties. Ab deposits in the brain parenchyma are termed amyloid plaques or senile plaques (neuritic plaques contain Ab and hyperphosphorylated tau). In comparison to soluble Ab, dispersible Ab is not in solution but represents larger nonfibrillar, protofibrillar, or fibrillar Ab aggregates that are in mixture with the extra- or intracellular fluid. Soluble and dispersible Ab aggregates are thought to represent the forms of Ab that induce neurodegeneration. Monomers and dimers are released after denaturation of the high-molecular weight oligomers, for example, by sodiumdodecylsulfate treatment. The classical cored plaque (arrow) with a central amyloid core (A) is distinguished from the diffuse plaque (arrowhead) consisting of diffuse fibrillar Ab deposits. The nerve is swollen at the site of the lesion indicative for the amyloidoma type of amyloid neuropathy. Primary amyloidosis is caused by a plasma cell neoplasm that often shows only small groups of neoplastic cells with a monoclonal expression of the amyloidogenic immunoglobulin chain, here l-light chains (arrows). Earlier affected regions are marked in black or gray (darkest phase 1 lightest gray phase 4). The Flemish mutation, a C to G transversion at codon 692, results in an Ala to Gly substitution at position 21 and a clinical phenotype of presenile dementia and cerebral hemorrhage. Many of the pathogenic missense mutations described outside the amyloid Ab sequence cluster closer to the amino acids recognized by the b- and g-secretases that release the amyloidogenic peptide from the precursor molecule. At codons 670 and 671, at the b-secretase processing site, the Swedish double-mutation shows Lys to Met and Asn to Leu substitutions, respectively. An Ile to Val substitution at codon 716 and various missense mutations occurring at codon 717 have been described. Denaturation of high-molecular Ab-aggregates leads to a release of lowmolecular Ab-oligomers, such as dimers, trimers, etc. The infectious etiological agent is devoid of nucleic acids and was called prion to denote its proteinaceous nature and distinguish it from viruses and viroids. Several mutations of the PrP gene are known to cause inherited human prion diseases. Extensive cortical spongiform change, gliosis, and neuronal loss are common, although not invariable features of these disorders. Seven Amyloidosis 163 pedigrees have been described in small rural communities of western Iceland. Although brain involvement is the main clinicopathological feature, silent amyloid deposits are also present in peripheral tissues, such as skin, lymph nodes, spleen, salivary glands, and seminal vesicles. Strokes are rare after the age of 50 years, and cognitive decline followed by dementia may occur in those cases that survive the hemorrhagical episodes. The mutation has been detected in Finnish, Dutch, American, and Japanese families. A different mutation has been described in patients of Danish and Czech origin suffering the same disorder. Personality changes are the earliest manifestations, with the patients becoming either irritable or depressed. Pseudobulbar palsy and dysarthria are universal and all patients progress to a chronic vegetative state: They become mute, unresponsive, quadriplegic, and incontinent.
A high-frequency alternating current is then passed through the needle for a microsecond antibiotics for uti gonorrhea order cheap clindamycin on line. Practitioners should be members of the British Institute and Association of Electrolysis antibiotics in livestock clindamycin 300 mg purchase overnight delivery. The light is absorbed by melanin in the hair shaft and the heat generated damages the follicle virus scanner free purchase clindamycin now. Dark-skinned patients are at risk of developing hyperpigmentation after treatment antibiotic infusion therapy clindamycin 300 mg without a prescription. Intense pulse light is also an effective means of hair removal and works in a similar way to lasers antibiotic resistance the need for global solutions clindamycin 150 mg free shipping. Several treatments are necessary, as only follicles in anagen (growth phase) respond. Eflornithine (Vaniqa) cream is an ornithine decarboxylase inhibitor that reduces hair growth over a 2- to 4-month period. Either the foetal lanugo hair is not lost before birth or it regrows at some later stage. When confined to the lumbosacral area (fawn tail) it may be a marker of an underlying spina bifida. Some drugs cause hypertrichosis in all patients to a greater or lesser degree: ciclosporin diazoxide minoxidil. The following drugs occasionally cause hypertrichosis: diphenylhydantoin minocycline penicillamine psoralens. The trigger is often a stressful event and alopecia areata itself is often very distressing, especially if it affects a large area. There may be one or several bald patches on the scalp or on any other hairy area Only pigmented hairs are affected, so normal white or grey hairs will remain in the middle of a bald area. Alopecia incognito (diffuse alopecia areata) causes rapid diffuse thinning of scalp hair and may be confused with telogen effluvium (see p. If there is any doubt as to the diagnosis, a scalp biopsy is helpful to distinguish between the two. Alopecia areata is a common autoimmune disease and spans all ages and ethnic groups. It is worth asking about a family history of autoimmune disease and checking blood sugar and autoimmune profile including thyroid antibodies. This is more likely if the hair loss is extensive or occurs in an ophiasis pattern (margin of scalp). Treatment currently available is unsatisfactory but includes the following options. Side effects include skin atrophy, which is usually temporary, and it may cause hypopigmentation in individuals with darker skin types. Application of potent skin sensitisers to the bald areas: Diphencyprone is the drug most commonly used. It is most effective in those whose hair loss has been present for less than 1 year. The whole scalp is then painted with a diluted solution of the lowest concentration (0. If it works, it is painted on the bald areas once a week until regrowth of hair is well established. Diphencyprone is degraded by light so patients have to keep their heads covered for 24 hours after treatment. Any hair growth may be lost if treatment is stopped, so maintenance is usually required. Potential side effects should be discussed with patients before starting treatment. Continued use of systemic steroids is not justified for alopecia areata because of long-term complications (see p. Future treatments include abatacept, a drug available for the treatment of rheumatoid arthritis. It is currently being trialled in the United States for alopecia totalis and alopecia universalis. Referral to a clinical psychologist can play an important role in helping patients come to terms with their hair loss. It is often due to Trichophyton tonsurans (caught from other children) or Microsporum canis (caught from kittens or puppies). If the skin is red or if there is associated ringworm on the face or neck, it is more likely to be due to animal ringworm. There will be a history of other children with similar hair loss (in human ringworm), or a new kitten or puppy whose fur is falling out (in animal ringworm). The diagnosis is confirmed by pulling out the short, broken hairs, and sending them for mycology. There is no need for topical treatment as well, as this is ineffective, since treatment applied to the surface cannot get into the hair shaft As human-acquired tinea capitis is contagious, and adults may act as carriers, all family members and possibly classmates should be screened for evidence of infection. If the child has a kerion, the crusts should be softened with arachis oil and then removed. If Staphylococcus aureus is grown, treat with flucloxacillin as well as with the antifungal. If the diagnosis is in doubt, a biopsy from the abnormal area will show empty anagen follicles and melanin pigment casts. Often the parent(s) have not noticed the child twisting the hairs around one of the fingers or pulling them out but will do so once you tell them what is happening. It is best for them not to make a big thing of it, particularly not to punish the child for it, and to give the child as much love and security as they can during the difficult time. Once the time of trauma is over, the child will nearly always stop pulling the hair out and the hair will regrow normally. In teenagers who pull out their hair the cause is often less obvious, but most will need psychiatric help to resolve the problem. Minoxidil can be helpful in boosting growth where there are still active follicles to improve volume but in many patients the hair loss is so advanced that a wig may be necessary. It causes hair loss at the temples and sometimes the crown and is due to the hair being tightly pulled back, tied up, plaited, braided or straightened with hot combs. It is important to ask about hair styling practices when Afro-Caribbean or African patients, usually woman, present with hair loss. It often involves the underlying subcutaneous fat leaving a depression in the skin. Pulsed methyl prednisolone followed by methotrexate or mycophenolate mofetil are preferred. There is a slow progressive scarring alopecia with pustules and crusts around the affected hairs. It is important, therefore, to start treatment as soon as possible to minimise the hair loss. In lupus the skin over the bald patches is usually red and scaly and there may be follicular plugging. It results in a progressive scarring alopecia of the fronto-temporo-parietal hairline. Often the process has been going on for many years before patients notice that their frontal hairline has moved back. Often these patients have associated eyebrow loss and may have also lost hair elsewhere, Prominent follicles with perifollicular erythema and scale may be seen along the frontal hairline. The cause is not known but it is thought that hormones may play a role, given that the majority of patients affected are postmenopausal women. Sometimes nothing is seen histologically except the replacement of hair follicles with scar tissue. Doxycycline 100 mg daily has been found to be partially effective in lichen planus. Anti-androgens such as finasteride 5 mg weekly and dutasteride 500 g weekly may help in stabilising, and in some cases improving, frontal fibrosing alopecia. Before griseofulvin was introduced in 1958, radiotherapy was the usual treatment for scalp ringworm. Many of these patients are now developing basal cell and squamous cell carcinomas on their bald scalps. Hot combing, chemical straightening and hot oil treatments used to straighten black curly hair can all result in permanent hair loss, particularly if aggravated by tight or corn-rolling styling that applies additional traction to hair roots. Patients may describe noticing increased hair in the shower, on their hairbrush or on the pillow. A false negative result may occur if the patient has washed his or her hair within 48 hours. Some patients may notice continued intermittent shedding known as chronic telogen effluvium. They should be reassured that this will not result in baldness, although it may unmask an underlying genetic predisposition to a patterned hair loss. Once the drug is discontinued, hair will usually regrow normally, although permanent alopecia may sometimes occur, especially after docetaxel for breast cancer (1 in 30 risk). The effect of dihydrotestosterone is a shortening of the anagen growth phase and a corresponding increase in telogen hairs. Gradually the hair follicles get smaller and terminal hairs are replaced by vellus hairs. The amount of hair loss and the age of onset is genetically determined (from mother or father). Decreased hair density from the crown forward with normal hair density at the back and sides occurs. An androgen-secreting tumour should be considered in women with male pattern alopecia if it is very extensive or if there is a change in the menstrual cycle. For a few, who cannot come to terms with their baldness, the following are available (not under the National Health Service). This does not produce regrowth of normal terminal hair, but of long vellus hair in about a third of those who use it. If treatment is stopped, the longer hair will fall out, so once started it will need to be continued indefinitely. One-third of men will have marked regrowth of hair, one-third will have moderate regrowth and one-third will have little regrowth. Patients should be warned that there have been cases of prolonged sexual side effects even after stopping treatment. Hair transplants: hairs are taken from the occipital area or sides of the scalp by punch biopsy. Follicular units (containing one to four follicles) are transplanted into the bald areas. Anti-androgens: Dianette is an option, particularly if there is associated polycystic ovarian syndrome. Spironolactone: start with 50 mg bid and increase to 100 mg bid depending on side effects. Premenopausal women should be counselled against becoming pregnant on this treatment. Other treatments that have been found to be helpful include topical oestrogens, topical prostaglandins Unfortunately, on stopping treatment with any of the drugs listed here, the hair loss will reoccur. Hair transplants: although expensive, this is an effective treatment in selected patients. There are numerous structural abnormalities of the hair shaft that cause hair to break off short. The diagnosis is made by running your hands through the scalp and feeling the thick, heaped-up scales, which are not shed because the scale binds to the hair. The plaques may extend away from the hairline onto the forehead, neck or around the ears, causing social embarrassment. Seborrhoeic eczema typically starts in the scalp, causing fine scaling (dandruff). This is associated with scaling behind and in front of the ears, in the external auditory meatus and on the face (see p. It is useful to alternate with an anti-yeast shampoo, such as ketoconazole (Nizoral) shampoo. If that is not enough, or if the scalp is very itchy, a topical steroid lotion or gel can be applied every night until it is clear. Topical scalp lotions contain alcohol, so warn the patient that it will sting if the skin is broken. Apply dry, massage into the scalp and leave on for 10 minutes before rinsing off backwards two to three times a week. Thick plaques of psoriasis on the scalp or pityriasis amiantacea require something to soften up the scale. Because it makes a mess, the head should be covered overnight with a scarf or shower cap to keep the ointment off the pillow. The treatment is repeated each night and washed off each morning until the scalp is clear. Once it is clear, the treatment can be done once a week or once a fortnight to keep it clear. Seborrheoic eczema is treated with ketoconazole (Nizoral) shampoo two to three times weekly. It usually presents as an acute weeping eczema at the hair margins and on the forehead, face and neck, rather than in the scalp itself. If it is very weepy, dry up any exudate by soaking the scalp in a diluted potassium permanganate or aluminium acetate solution (see p. Once it is better, refer to a dermatologist for patch testing to establish the cause. Sometimes the cause is a staphylococcal folliculitis, which can be confirmed by taking a swab.
Generic clindamycin 300 mg amex. Shopping Cart and High Chair Spray with Essential Oils - How-To Tuesday.
References
- Furlani D, Klopsch C, Gabel R, et al: Intracardiac erythropoietin injection reveals antiinflammatory potential and improved cardiac functions detected by Forced Swim Test. Transplant Proc 2008;40:962-966.
- McKhann GM, Cornblath DR, Griffin JW, et al. Acute motor axonal neuropathy in northern China: the spectrum of neuropathologic changes in clinically defined cases. Brain. 1995;118(Pt 3):577-595.
- Byrd JC, Dodge RK, Carroll A, et al. Patients with t(8;21)(q22;q22) and acute myeloid leukemia have superior failure-free and overall survival when repetitive cycles of high-dose cytarabine are administered. J Clin Oncol 1999;17(12):3767-3775.
- Abdool Z, Th aker R, Sultan AH, Oliver RS. Prospective evaluation of outcome of vaginal pessaries versus surgery in women with symptomatic pelvic organ prolapse. Int Urogynaecol J. 2011;22:273-8.
- Ychou M, Desseigne F, Guimbaud R, et al. Randomized phase II trial comparing FOLFIRINOX (5FU/leucovorin [LV], irinotecan [I] and oxaliplatin [O]) vs gemcitabine (G) as first-line treatment for metastatic pancreatic adenocarcinoma (MPA). First results of the ACCORD 11 trial. J Clin Oncol 2007;25:4516.
- Stevens SM, Elliott CG, Chan KJ, et al. Withholding anticoagulation after a negative result on duplex ultrasonography for suspected symptomatic deep venous thrombosis. Ann Intern Med. 2004;140:985-991.