
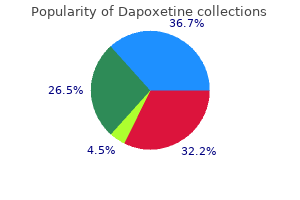
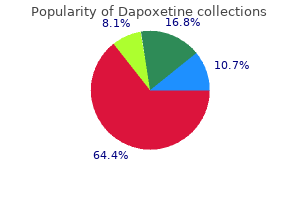
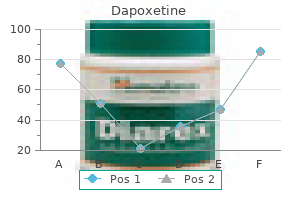
Dapoxetine
| Contato
Página Inicial
J. Eric Jelovsek, MD
- Assistant Professor of Surgery, Associate Staff, Center of Urogynecology and
- Reconstructive Pelvic Surgery, Co-Site Director OB/GYN Residency, Department
- of Obstetrics and Gynecology, Obstetrics, Gynecology, and Women?
- Health Institute, Cleveland Clinic, Cleveland, Ohio
This technique is most often employed in rectal resections erectile dysfunction treatment success rate purchase generic dapoxetine, but may be used for colocolostomy or small bowel anastomoses erectile dysfunction and marijuana buy dapoxetine 90 mg low cost. An end-to-side configuration is useful when one limb of bowel is larger than the other erectile dysfunction caused by nerve damage order dapoxetine 30 mg otc. A side-to-end anastomosis is used when the proximal bowel is of smaller caliber than the distal bowel erectile dysfunction effects on relationship purchase dapoxetine 90 mg mastercard. A side-to-end anastomosis may have a less tenuous blood supply than an end-to-end anastomosis erectile dysfunction treatment herbal buy dapoxetine on line. A side-to-side anastomosis allows a large, wellvascularized connection to be created on the antimesenteric side of two segments of intestine. Any of the configurations described earlier may be created using a hand-sutured or stapled technique. Hand-sutured anastomoses may be single layer, using either running or interrupted stitches, or double layer. A double-layer anastomosis usually consists of a continuous inner layer and an interrupted outer layer. After distal rectal or anal canal resection, a transanal, hand-sewn coloanal anastomosis may be necessary to restore bowel continuity. This can be done in conjunction with an anal canal mucosectomy to allow the anastomosis to be created at the dentate line. Linear cutting/stapling devices are used to divide the bowel and to create side-to-side anastomoses. Circular cutting/stapling devices can create end-to-end, end-to-side, or side-to-end anastomoses. These instruments are particularly useful for creating low rectal or anal canal anastomoses where the anatomy of the pelvis makes a hand-sewn anastomosis technically difficult or impossible. Following resection of the colorectum, a stapled end-toend colorectal, coloanal canal, or ileal pouchanal canal anastomosis may be created by one of two techniques. With the open purse-string technique, the distal rectal stump purse-string is placed by hand, and the assembled circular stapler is inserted into the anus and guided up to the rectal purse-string. A purse-string is placed in the distal end of the proximal colon; the proximal colon is placed over the anvil and the purse-string tightened. With the alternative double-staple technique, the distal rectum or anal canal is closed with a transverse staple line. The circular stapler is inserted through the anus without its anvil until the cartridge effaces the transverse staple line. The stapler is opened, causing the trocar to perforate through the rectal stump adjacent to the transverse staple line. After firing and removing the stapler, the resulting anastomotic rings should be inspected to ensure that they are intact. A gap in an anastomotic ring suggests that the circular staple line is incomplete and the anastomosis should be reinforced with suture circumferentially, if technically feasible. Most surgeons will also leak test an anastomosis by instilling water or saline into the pelvis and insufflating the rectum with air via a proctoscope or alternatively instilling methylene blue or betadine into the rectum to look for extravasation. After resection of the rectosigmoid and placement of purse-string sutures proximally and distally, the stapler is inserted into the anal canal and opened. Rectal purse-string suture is tied to secure the rectal stump to the rod of the stapler, and the colonic purse-string is tied to secure the colon to the anvil of the stapler. Because the abdominal landmarks in a supine, anesthetized patient may be dramatically different from those in an awake, standing, or sitting patient, the stoma site should always be marked with a tattoo, skin scratch, or permanent marker preoperatively, if possible. In an emergency operation where the stoma site has not been marked, an attempt should be made to place a stoma within the rectus muscle and away from both the costal margin and iliac crest. In emergencies, placement high on the abdominal wall is preferred to a low-lying site. For all stomas, a circular skin incision is created and the subcutaneous tissue dissected to the level of the anterior rectus sheath. The anterior rectus sheath is incised in a cruciate fashion, the muscle fibers separated bluntly, and the posterior sheath identified and incised. Four sutures incorporating the cut end of the ileum, the seromuscular layer at the level of the anterior rectus fascia, and the subcuticular edge of the skin are placed at 90° to each other. The sutures are tied to produce stomal eversion, and (C) simple sutures from the cut edge of the bowel to the subcuticular tissue complete the maturation of the ileostomy. The size of the defect depends on the size of the bowel used to create the stoma, but should be as small as possible without compromising the intestinal blood supply (usually the width of two to three fingers). The abdominal incision is usually closed and dressed prior to maturing the stoma to avoid contaminating the wound. In order to make appliance use easier, a protruding nipple is fashioned by everting the bowel. Three or four interrupted absorbable sutures are placed through the edge of the bowel, then through the serosa, approximately 2 cm proximal to the edge, and then through the dermis (Brooke technique). A temporary ileostomy is often used to "protect" an anastomosis that is at risk for leakage (low in the rectum, in an irradiated field, in an immunocompromised or malnourished patient, and during some emergency operations). A segment of distal ileum is brought through the defect in the abdominal wall as a loop. A divided loop may also be created by firing a linear cutting/stapler across the distal limb of the loop flush with the skin followed by maturation of the proximal limb of the loop. The advantage of a loop or divided loop ileostomy is that subsequent closure can often be accomplished without a formal laparotomy. An elliptical incision is created around the stoma and the bowel gently dissected free of the subcutaneous tissues and fascia. A hand-sewn or stapled anastomosis can then be created and the intestine returned to the peritoneal cavity. A flexible endoscopy exam and a contrast enema (Gastrografin) are recommended prior to closure to ensure that the anastomosis has not leaked and is patent. In cancer patients receiving adjuvant chemotherapy, ileostomy closure should be delayed until the chemotherapy is completed. A permanent ileostomy is sometimes required after total proctocolectomy or in patients with obstruction. The end of the small intestine is brought through the abdominal wall defect and matured. Stoma necrosis may occur in the early postoperative period and is usually caused by skeletonizing the distal small bowel and/or creating an overly tight fascial defect. Limited mucosal necrosis above the fascia may be treated expectantly, but necrosis below the level of the fascia requires surgical revision. The creation of an ileostomy bypasses the fluidabsorbing capability of the colon, and dehydration with fluid and electrolyte abnormalities is not uncommon. Ideally, ileostomy output should be maintained at less than 1500 mL/d to avoid this problem. The somatostatin analogue, octreotide, has been used with varying success in this setting. Obstruction may occur intra-abdominally or at the site where the stoma exits the fascia. Parastomal hernia is less common after an ileostomy than after a colostomy but can cause poor appliance fitting, pain, obstruction, or strangulation. A variety of techniques to repair these hernias have been described, including local repair (either with or without mesh), laparoscopic repair, and stoma resiting. Prolapse is a rare, late complication and is often associated with a parastomal hernia. The bulkiness of the colon makes a loop colostomy awkward for use of an appliance, and prolapse is more likely with this configuration. An abdominal wall defect is created and the end of the colon mobilized through it. Because a protruding stoma is considerably easier to pouch, colostomies should also be matured in a Brooke fashion. Tacking the distal end of the colon to the abdominal wall or tagging it with permanent suture can make identification of the stump easier if the colostomy is closed at a later date. Closure of an end colostomy has traditionally required a laparotomy, but increasingly minimally invasive techniques have been adopted. The stoma is dissected free of the abdominal wall and the distal bowel identified. Colostomy necrosis may occur in the early postoperative period and results from an impaired vascular supply (skeletonization of the distal colon or a tight fascial defect). Like ileostomy necrosis, limited suprafascial necrosis may be followed expectantly, but necrosis below the fascia requires surgery. Retraction may also occur but is less problematic with a colostomy than with an ileostomy because the stool is less irritating to the skin than succus entericus. Parastomal hernia is the most common late complication of a colostomy and requires repair if it is symptomatic. Dehydration is rare after colostomy, and skin irritation is less common than with ileostomy. Functional Results Function following segmental colonic resection and primary anastomosis is generally excellent. A small percentage of patients following subtotal or total colectomy and ileosigmoid or ileorectal anastomosis may experience diarrhea and bowel frequency. This is especially true if the patient is elderly, if significant length of small bowel has been resected, and if residual proctocolitis is poorly controlled. In general, the more distal the anastomosis, the greater is the risk of troublesome diarrhea and frequency. However, some patients develop significant diarrhea after right colectomy due to malabsorption of bile acids; in these cases, bile acid binding resins. Function following anterior resection is highly dependent on the level of anastomosis, the use of pre- or postoperative pelvic radiation, and underlying sphincter function. Following low anterior or extended low anterior resection, some surgeons 1194 prefer to construct a short (5-cm) colon J-pouch to anastomose to the distal rectum or anal canal or, alternatively, a transverse coloplasty to increase the capacity of the neorectum. The reservoirs are thought to lessen urgency, frequency, and incontinence, but some patients have difficulty initiating defecation, and long-term superiority over a "straight" anastomosis has yet to be proven. In addition, these reservoirs can be technically difficult, especially in an obese male with a narrow pelvis. The physical and psychological problems associated with a permanent Brooke ileostomy led to development of the continent Kock pouch ileostomy. Unfortunately, complications, especially complications related to valve slippage, are common. Despite variations of technique designed to improve the function of the continent ileostomy, most surgeons have abandoned this operation and instead perform restorative proctocolectomy with ileal pouchanal anastomosis. Although ileal pouchanal reconstruction is anatomically appealing, functional outcome is far from perfect. Pouchitis occurs in nearly 50% of patients who undergo the operation for chronic ulcerative colitis, and small bowel obstruction is not uncommon. Other less common complications include difficulties with pouch evacuation, pouch-anal and/or pouch-vaginal fistula, and anal stricture. Despite these drawbacks, the vast majority of patients are satisfied and prefer ileal pouch anal reconstruction to permanent ileostomy. Pouchitis is an inflammatory condition that affects both ileoanal pouches and continent ileostomy reservoirs. Symptoms include increased diarrhea, hematochezia, abdominal pain, fever, and malaise. Some believe pouchitis results from fecal stasis within the pouch, but emptying studies are not confirmatory. Antibiotics (metronidazole ± ciprofloxacin) are the mainstays of therapy, and most patients will respond rapidly to either oral preparations or enemas. Reintroduction of normal flora by ingestion of probiotics and/or an elemental diet have been suggested as a possible treatment in refractory cases. Occasionally, pouch excision is necessary to control the symptoms of chronic pouchitis. Postoperative epidural anesthesia provides excellent pain relief and improves pulmonary function. General anesthesia is required for the vast majority of intra-abdominal procedures. In patients with significant comorbid disease, an anesthesia consultation may be appropriate. Anorectal procedures may be performed in lithotomy or in the prone jackknife position. Some surgeons prefer the prone jackknife position because exposure may be better, especially for anterior lesions. Distal posterior lesions can usually be accessed from either position, but more proximal posterior lesions are better accessed in the prone position. The rationale for bowel preparation is that decreasing the bacterial load in the colon and rectum will decrease the incidence of postoperative infection. Mechanical bowel preparation uses cathartics to rid the colon of solid stool the night before surgery. Magnesium citrate solutions are generally better tolerated but are more likely to cause fluid and electrolyte abnormalities. Preparatory formulations have been recently introduced in tablet form in an attempt to improve tolerance. However, these methods of bowel cleansing require ingestion of 40 or more tablets with water over several hours. To date, these formulations have not been proven to be superior to the more traditional products. The addition of oral antibiotics to the preoperative mechanical bowel preparation has been thought to decrease postoperative infection by further decreasing the bacterial load of the colon. However, the regimens used (neomycin, erythromycin, or metronidazole) frequently caused gastrointestinal upset that interfered with the mechanical preparation, and many surgeons have abandoned oral antibiotic prophylaxis. In contrast, longstanding, convincing data support the efficacy of parenteral antibiotic prophylaxis at the time of surgery.
Of those who were treated with dilation erectile dysfunction doctor tampa cheap 30 mg dapoxetine otc, only 54% were doing well erectile dysfunction types purchase 90 mg dapoxetine, while 16% required redilation erectile dysfunction 21 years old discount dapoxetine 90 mg with visa, and 22% eventually required surgical myotomy to obtain relief erectile dysfunction doctors in texas buy dapoxetine 60 mg with visa. If simultaneous esophageal contractions are associated with the sphincter abnormality erectile dysfunction doctors raleigh nc 30 mg dapoxetine with mastercard, the so-called vigorous achalasia, then the myotomy should extend over the distance of the abnormal motility as mapped by the preoperative motility study. Failure to do this will result in continuing dysphagia and a dissatisfied patient. The best objective evaluation of improvement in the patient following either balloon dilation or myotomy is a scintigraphic measurement of esophageal emptying time. However, some degree of dysphagia may persist despite improved esophageal emptying, due to disturbances in esophageal body function. When an antireflux procedure is added to the myotomy, it should be a partial fundoplication. Either scissors or a hook-type electrocautery can be used to initiate the incision in the longitudinal and circular muscle. After completion, the muscle edges are separated bluntly from the esophageal mucosa for approximately 50% of the esophageal circumference. Either an anterior hemifundoplication augmenting the angle of His (Dor) or posterior partial fundoplication (Toupet) can be performed. The Dor type fundoplication is slightly easier to perform, and does not require disruption of the normal posterior gastroesophageal attachments (a theoretical advantage in preventing postoperative reflux). It is the ultimate minimally invasive myotomy as it requires no incisions through the skin. The procedure begins by division of the short gastric vessels in preparation for fundoplication. Once completed, Critical analysis of the results of therapy for motor disorders of the esophagus requires objective measurement. The use of symptoms alone as an endpoint to evaluate therapy for achalasia may be misleading. The propensity for patients to unconsciously modify their diet to avoid difficulty swallowing is underestimated, making an assessment of results based on symptoms unreliable. Insufficient reduction in outflow resistance may allow progressive esophageal dilation to develop slowly, giving the impression of improvement because the volume of food able to be ingested with comfort increases. Given that the goal of therapy is to eliminate the outflow resistance of a nonrelaxing sphincter, measurement of improvements in esophageal baseline pressure and scintigraphic transit time may be better indicators of success, but are rarely reported. Eckardt and associates investigated whether the outcome of pneumatic dilation in patients with achalasia could be predicted on the basis of objective measurements. Approximately 50% of the patients studied had postdilatation sphincter pressures between 10 and 20 mmHg, with a 2-year remission rate of 71%. More important, 16 of 46 patients were left with a postdilatation sphincter pressure of >20 mmHg, and had an unacceptable outcome. Overall, only 30% of patients dilated remained in symptomatic remission at 5 years. Bonavina and colleagues reported good to excellent results with transabdominal myotomy and Dor fundoplication in 94% of patients after a mean follow-up of 5. No operative mortality occurred in either of these series, attesting to the safety of the procedure. Malthaner and Pearson reported the long-term clinical results in 35 patients with achalasia, having a minimum follow-up of 10 years Table 25-10). Twentytwo of these patients underwent primary esophageal myotomy and Belsey hemifundoplication at the Toronto General Hospital. Excellent to good results were noted in 95% of patients at 1 year, declining to 68%, 69%, and 67% at 10, 15, and 20 years, respectively. Two patients underwent early reoperation for an incomplete myotomy, and three underwent an esophagectomy for progressive disease. They concluded that there was a deterioration of the initially good results after surgical myotomy and hiatal repair for achalasia, which is due to late complications of gastroesophageal reflux. Ellis reported his lifetime experience with transthoracic short esophageal myotomy without an antireflux procedure. One hundred seventy-nine patients were analyzed at a mean followup of 9 years, ranging from 6 months to 20 years. He also observed that the level of improvement deteriorated with time, with excellent results (patients continuing to be symptom free) decreasing from 54% at 10 years to 32% at 20 years. Both studies document nearly identical results 10 to 15 years following the procedure, and both report deterioration over time, probably due to progression of the underlying disease. The addition of an antireflux procedure if the operation is performed transthoracically has no significant effect on the outcome. The outcome of laparoscopic myotomy and hemifundoplication has been well documented. Richter and coworkers reviewed published reports to date, including 254 patients with an average success rate of 93% at 2. Intraoperative complications consist largely of mucosal perforation, and have been more likely to occur after botulinum toxin injection. The incidence of objective reflux disease as evidenced by abnormal acid exposure is <10%. A number of randomized clinical trials in the past decade have compared the outcomes of laparoscopic Heller myotomy to pneumatic dilation and to botulinum toxin injection. In each of these trials, laparoscopic Heller myotomy and partial fundoplication was superior to the alternative treatment. Lastly, a randomized clinical trial examining the need for fundoplication following Heller myotomy demonstrated a great deal more reflux in patients without fundoplication, and no better swallowing in the Heller-only group. The best treatment for achalasia is a laparoscopic Heller myotomy and partial fundoplication. Esophageal Resection for End-Stage Motor Disorders of the Esophagus Patients with dysphagia and long-standing benign disease, whose esophageal function has been destroyed by the disease process or multiple previous surgical procedures, are best managed by esophagectomy. Fibrosis of the esophagus and cardia can result in weak contractions and failure of the distal esophageal sphincter to relax. The loss of esophageal contractions can result in the stasis of food, esophageal dilatation, regurgitation, and aspiration. In these situations esophageal replacement is usually required to establish normal alimentation. Before proceeding with esophageal resection for patients with end-stage benign disease, the choice of the organ to substitute for the esophagus. The choice of replacement is affected by a number of factors, as described later in the section on Techniques of Esophageal Reconstruction. If minimally invasive esophagectomy is to be performed, thoracoscopic dissection should be combined with abdominal dissection. Its incidence is highly variable, ranging from approximately 20 per 100,000 in the United States and Britain, to 160 per 100,000 in certain parts of South Africa and the Honan Province of China, and even 540 per 100,000 in the Guriev district of Kazakhstan. The environmental factors responsible for these localized high-incidence areas have not been conclusively identified, though additives to local foodstuffs (nitroso compounds in pickled vegetables and smoked meats) and mineral deficiencies (zinc and molybdenum) have been suggested. In Western societies, smoking and alcohol consumption are strongly linked with squamous carcinoma. Other definite associations link squamous carcinoma with longstanding achalasia, lye strictures, tylosis (an autosomal dominant disorder characterized by hyperkeratosis of the palms and soles), and human papillomavirus. Once a nearly uniformly lethal disease, survival has improved slightly because of advances in the understanding of its molecular biology, screening and surveillance practices, improved staging, minimally invasive surgical techniques, and neoadjuvant therapy. It now occurs not only considerably more frequently, but in younger patients, and is often detected at an earlier stage. These facts support rethinking the traditional approach of assuming palliation is appropriate in all patients. The historical focus on palliation of dysphagia in an elderly patient with comorbidities should change when dealing with a young patient with dependent children and a productive life ahead. Rarely, it arises in the submucosal glands, and forms intramural growths that resemble the mucoepidermal and adenoid cystic carcinomas of the salivary glands. This risk is similar to the risk for developing lung cancer in a person with a 20-pack-per-year history of smoking. Extension of the primary tumor into the tracheobronchial tree can occur primarily with squamous cell carcinoma and can cause stridor, tracheoesophageal fistula and resultant coughing, choking, and aspiration pneumonia. Rarely, severe bleeding from the primary tumor or from erosion into the aorta or pulmonary vessels occurs. In these communities, the most prominent early symptom is pain on swallowing rough or dry food. In patients that present with back pain at the time of esophageal cancer diagnosis, there is usually distant metastasis or celiac encasement. Dysphagia usually presents late in the natural history of the disease, because the lack of a serosal layer on the esophagus allows the smooth muscle to dilate with ease. As a result, the dysphagia becomes severe enough for the patient to seek medical advice only when more than 60% of the esophageal circumference is infiltrated with cancer. Tracheoesophageal fistula may be present in some patients on their first visit to the hospital, and more than 40% will have evidence of distant metastases. With tumors of the cardia, anorexia and weight loss usually precede the onset of dysphagia. The physical signs of esophageal tumors are those associated with the presence of distant metastases. Put simply, one needs to determine if the disease is confined to the esophagus, (T1T2, N0), locally advanced (T13, N1), or disseminated (any T, any N, M1). If cancer is confined to the esophagus, removal of the tumor with adjacent lymph nodes may be curative. Very early tumors confined to the mucosa (T in situ, T1a, intramucosal cancer) may be addressed with endoscopic treatment. When the tumor is locally aggressive, modern therapy dictates a multimodality approach in a surgically fit patient. Multimodality therapy is either chemotherapy followed by surgery or radiation and chemotherapy followed by surgery. When given before surgery, these treatments are referred to as neoadjuvant or induction therapy. If the patient has dysphagia, as many do, the most rapid form of palliation is the endoscopic placement of an expandable esophageal stent. This is often referred to as M1a disease, indicating that these patients should not be treated with therapy directed toward locally advanced cancer. The most common sites of esophageal cancer metastases are lung, liver, and peritoneal surfaces, including the omentum and small bowel mesentery. Occasionally, diagnostic laparoscopy and jejunostomy tube placement may precede induction chemoradiation in the patient with severe dysphagia and weight loss from a locally advanced cancer. Experience with esophageal resection in patients with early stage disease has identified characteristics of esophageal cancer that are associated with improved survival. Factors known to be important in the survival of patients with advanced disease, such as cell type, degree of cellular differentiation, or location of tumor in the esophagus, have no effect on survival of patients who have undergone resection for early disease. Most surgeons agreed that the 1983 tumor, nodes, and metastasis system left much to be desired. Clinical Approach to Carcinoma of the Esophagus and Cardia the selection of a curative vs. The selection of surgical therapy for patients with carcinoma of the esophagus depends not only on the anatomic stage of the disease and an assessment of the swallowing capacity of the patient, but also on the location of the primary tumor. They are almost always squamous cell cancer, with a rare adenocarcinoma arising from a congenital inlet patch of columnar lining. These tumors, particularly those in the postcricoid area, represent a separate pathologic entity for two reasons: (a) They are more common in females and appear to be a unique entity in this regard; and (b) the efferent lymphatics from the cervical esophagus drain completely differently from those of the thoracic esophagus. Cervical esophageal cancer is frequently unresectable because of early invasion of the larynx, great vessels, or trachea. Radical surgery, including esophagolaryngectomy may occasionally be performed for these lesions, but the ensuing morbidity makes this a less than desirable approach in the face of uncertain cure. Thus, for most patients with cervical esophageal cancer, stereotactic radiation with concomitant chemotherapy is the most desirable treatment. Wong has shown that local recurrence at the anastomosis can be prevented by obtaining a 10-cm margin of normal esophagus above the tumor. Anatomic studies have also shown that there is no submucosal lymphatic barrier between the esophagus and the stomach at the cardia, and Wong has shown that 50% of the local recurrences in patients with esophageal cancer who are resected for cure occur in the intrathoracic stomach along the line of the gastric resection. Considering that the length of the esophagus ranges from 17 to 25 cm, and the length of the lesser curvature of the stomach is approximately 12 cm, a curative resection requires a cervical division of the esophagus and a >50% proximal gastrectomy in most patients with carcinoma of the distal esophagus or cardia. Unresectable tumor invading other adjacent structures, such as aorta, vertebral body, trachea, etc. Algorithm for the evaluation of esophageal cancer patients to select the proper therapy: curative en bloc resection, palliative transhiatal resection, or nonsurgical palliation. Resection for cure of carcinoma of the esophagus in a patient older than 80 years is rarely indicated, because of the additional operative risk and the shorter life expectancy. Despite this general guideline, octogenarians with a high performance status and excellent cardio-pulmonary reserve may be considered candidates for esophagectomy and recent case series have established its success in highly selected patients. It is in this group of patients that the lesser physiologic impact of minimally invasive surgery may reduce the morbidity and mortality associated with open two- or three-field esophagectomy. Location Incidence Cervical Upper thoracic Middle thoracic 8% 3% 32% Lower thoracic 25% Cardiopulmonary Reserve. Patients undergoing esophageal resection should have sufficient cardiopulmonary reserve to tolerate the proposed procedure. The respiratory function is best assessed with the forced expiratory volume in 1 second, which ideally should be 2 L or more.
The perianal space surrounds the anus and laterally becomes continuous with the fat of the buttocks impotence libido order dapoxetine from india. It is continuous with the perianal space distally and extends cephalad into the rectal wall erectile dysfunction test yourself 60 mg dapoxetine buy with visa. The ischiorectal space (ischiorectal fossa) is located lateral and posterior to the anus and is bounded medially by the external sphincter erectile dysfunction meditation 90 mg dapoxetine otc, laterally by the ischium impotence while trying to conceive order dapoxetine with american express, superiorly by the levator ani erectile dysfunction diabetes pathophysiology discount dapoxetine amex, and inferiorly by the transverse septum. The two ischiorectal spaces connect posteriorly above the anococcygeal ligament but below the levator ani muscle, forming the deep postanal space. The supralevator spaces lie above the levator ani on either side of the rectum and communicate posteriorly. A perianal abscess is the most common manifestation and appears as a painful swelling at the anal verge. Spread through the external sphincter below the level of the puborectalis produces an ischiorectal abscess. These abscesses may become extremely large and may not be visible in the perianal region. Digital rectal exam will reveal a painful swelling laterally in the ischiorectal fossa. Intersphincteric abscesses occur in the intersphincteric space and are notoriously difficult to diagnose, often requiring an examination under anesthesia. Perianal space A Peritoneum Rectorectal space Rectosacral fascia Supralevator space Levator ani m. A palpable mass is often detected by inspection of the perianal area or by digital rectal examination. Occasionally, patients will present with fever, urinary retention, or lifethreatening sepsis. The diagnosis of a perianal or ischiorectal abscess can usually be made with physical exam alone (either in the office or in the operating room). Pain is typically described as being deep and "up inside" the anal area and is usually exacerbated by coughing or sneezing. The diagnosis is made based on a high index of suspicion and usually requires an examination under anesthesia. Once identified, an intersphincteric abscess can be drained through a limited, usually posterior, internal sphincterotomy. Anorectal abscesses should be treated by drainage as soon as the diagnosis is established. If the diagnosis is in question, an examination and drainage under anesthesia are often the most expeditious ways both to confirm the diagnosis and to treat the problem. Delayed or inadequate treatment may occasionally cause extensive and life-threatening suppuration with massive tissue necrosis and septicemia. Antibiotics are only indicated if there is extensive overlying cellulitis or if the patient is immunocompromised, has diabetes mellitus, or has valvular heart disease. A Perianal Abscess Most perianal abscesses can be drained under local anesthesia in the office, clinic, or emergency room. A skin incision is created, and a disk of skin excised to prevent premature closure. B Ischiorectal Abscess An ischiorectal abscess causes diffuse swelling in the ischiorectal fossa that may involve one or both sides, forming a "horseshoe" abscess. Simple ischiorectal abscesses are drained through an incision in the overlying skin. The source of sepsis is commonly an undrained or inadequately drained cryptoglandular abscess or a urogenital infection. Patients often have signs of systemic toxicity and may be hemodynamically unstable. A high index of suspicion is necessary because perineal signs of severe infection may be minimal and prompt surgical intervention can be lifesaving. Surgical débridement of all nonviable tissue is required to treat all necrotizing soft tissue infections. Multiple operations may be necessary to ensure that all necrotic tissue has been resected. Broad-spectrum antibiotics are frequently employed, but adequate surgical débridement remains the mainstay of therapy. Colostomy may be required if extensive resection of the sphincter is required or if stool contamination of the perineum makes wound management difficult. Despite early recognition and adequate surgical therapy, the mortality of necrotizing perineal soft tissue infections remains approximately 50%. Supralevator Abscess this type of abscess is uncommon and can be difficult to diagnose. Because of its proximity to the peritoneal cavity, supralevator abscesses can mimic intra-abdominal conditions. Digital rectal examination may reveal an indurated, bulging mass above the anorectal ring. It is essential to identify the origin of a supralevator abscess prior to treatment. If the abscess is secondary to an upward extension of an intersphincteric abscess, it should be drained through the rectum. If it is drained through the ischiorectal fossa, a complicated, suprasphincteric fistula may result. If a supralevator abscess arises from the upward extension of an ischiorectal abscess, it should be drained through the ischiorectal fossa. Drainage of this type of abscess through the rectum may result in an extrasphincteric fistula. If the abscess is secondary to intra-abdominal disease, the primary process requires treatment and the abscess is drained via the most direct route (transabdominally, rectally, or through the ischiorectal fossa). The fistula usually originates in the infected crypt (internal opening) and tracks to the external opening, usually the site of prior drainage. The course of the fistula can often be predicted by the anatomy of the previous abscess. A complex, recurrent, or nonhealing fistula should raise the suspicion of one of these diagnoses. Patients present with persistent drainage from the internal and/or external openings. Although the external opening is often easily identifiable, identification of the internal opening may be more challenging. In general, fistulas with an external opening anteriorly connect to the internal opening by a short, radial tract. Fistulas with an external opening posteriorly track in a curvilinear fashion to the posterior midline. However, exceptions to this rule often occur if an anterior Perianal Sepsis in the Immunocompromised Patient the immunocompromised patient with perianal pain presents a diagnostic dilemma. Because of leukopenia, these patients may develop serious perianal infection without any of the cardinal signs of inflammation. While broad-spectrum antibiotics may cure some of these patients, an exam under anesthesia should not be delayed because of neutropenia. Any indurated area should be incised and drained, biopsied to exclude a leukemic infiltrate, and cultured to aid in the selection of antimicrobial agents. Fistulas are categorized based on their relationship to the anal sphincter complex, and treatment options are based on these classifications. The goal of treatment of fistula in ano is eradication of sepsis without sacrificing continence. Because fistulous tracks encircle variable amounts of the sphincter complex, surgical treatment is dictated by the location of the internal 10 and external openings and the course of the fistula. The external opening is usually visible as a red elevation of granulation tissue with or without concurrent drainage. Care must be taken to avoid creating an artificial internal opening (thus often converting a simple fistula into a complex fistula). Treatment of a transsphincteric fistula depends on its location in the sphincter complex. The four major categories of fistula in ano (left side of drawings) and the usual operative procedure to correct the fistula (right side of drawings). High transsphincteric fistulas, which encircle a greater amount of muscle, are more safely treated by initial placement of a seton (see below). Extrasphincteric fistulas are rare, and treatment depends on both the anatomy of the fistula and its etiology. In general, the portion of the fistula outside the sphincter should be opened and drained. Complex fistulas with multiple tracts may require numerous procedures to control sepsis and facilitate healing. Proctoscopy should be performed in all cases of complex and/or nonhealing fistulas to assess the health of the rectal mucosa. A seton is a drain placed through a fistula to maintain drainage and/or induce fibrosis. Cutting setons consist of a suture or a rubber band that is placed through the fistula and intermittently tightened in the office. Tightening the seton results in fibrosis and gradual division of the sphincter, thus eliminating the fistula while maintaining continuity of the sphincter. A noncutting seton is a soft plastic drain (often a vessel loop) placed in the fistula to maintain drainage. The fistula tract may subsequently be laid open with less risk of incontinence because scarring prevents retraction of the sphincter. Fibrin glue and a variety of collagen-based plugs also have been used to treat persistent fistulas with variable results. In this procedure, the fistula is identified in the intersphincteric plane (usually by placement of a lacrimal probe), divided, and the two ends ligated. Early reports have shown success with this technique, but long-term outcome is not yet known. With the patient in the prone position, installation of methylene blue into the rectum while a tampon is in the vagina may confirm the presence of a small fistula. Rectovaginal fistulas are classified as low (rectal opening close to the dentate line and vaginal opening in the fourchette), middle (vaginal opening between the fourchette and cervix), or high (vaginal opening near the cervix). Low rectovaginal fistulas are commonly caused by obstetric injuries or trauma from a foreign body. Mid-rectovaginal fistulas may result from more severe obstetric injury, but also occur after surgical resection of a midrectal neoplasm, radiation injury, or extension of an undrained abscess. The treatment of rectovaginal fistula depends on the size, location, etiology, and condition of surrounding tissues. Because up to 50% of fistulas caused by obstetric injury heal spontaneously, it is prudent to wait 3 to 6 months before embarking on surgical repair in these patients. If the fistula was caused by a cryptoglandular abscess, drainage of the abscess may allow spontaneous closure. Low and mid-rectovaginal fistulas are usually best treated with an endorectal advancement flap. If a sphincter injury is present, an overlapping sphincteroplasty should be performed concurrently. High rectovaginal, colovaginal, and enterovaginal fistulas are usually best treated via a transabdominal approach. The diseased tissue, which caused the fistula (upper rectum, sigmoid colon, or small bowel), is resected and the hole in the vagina closed. Healthy tissue, such as omentum or muscle, frequently is interposed between the bowel anastomosis and the vagina to prevent recurrence. Fistulas resulting from radiation damage are not amenable to local repair with an advancement flap because of damage to the surrounding rectal and vaginal tissues. Such mid- and high rectovaginal fistulas are occasionally repaired successfully with a transabdominal approach in which healthy tissue (omentum, muscle, or nonradiated bowel) is interposed between the damaged rectum and vagina. Because differentiating radiation damage from malignancy can be extremely difficult, all fistulas resulting from radiation should be biopsied to rule out the presence of cancer. Pruritus ani (severe perianal itching) is a common problem with a multitude of etiologies. Surgically correctable (anatomic) causes include prolapsing hemorrhoids, ectropion, fissure, fistula, and neoplasms. Infections may be caused by fungus (Candida species and Epidermophyton organisms), parasites (Enterobius vermicularis [pinworms], Pediculus pubis [a louse], and Sarcoptes scabiei [scabies]), bacteria (Corynebacterium minutissimum [erythrasma] and T. Noninfectious dermatologic causes include seborrhea, psoriasis, and contact dermatitis. Contact dermatitis can be particularly troublesome because many over-the-counter topical agents used by patients to relieve itching may exacerbate the problem. Occasionally, systemic diseases such as jaundice and diabetes may present with pruritus ani. Despite the myriad of causes, the majority of pruritus ani is idiopathic and probably related to local hygiene, neurogenic, or Diagnosis. Patients describe symptoms varying from the sensation of passing flatus from the vagina to the passage of solid stool from the vagina. Large fistulas may be obvious on anoscopic and/or vaginal speculum examination, but smaller fistulas may be difficult to locate. Treatment focuses on removal of irritants, improving perianal hygiene, dietary adjustments, and avoiding scratching. Biopsy and/or culture may be required to rule out an infectious or dermatologic cause.
It controls the flow of bile erectile dysfunction medication online pharmacy proven 90 mg dapoxetine, and in some cases pancreatic juice erectile dysfunction at age 64 buy generic dapoxetine 90 mg line, into the duodenum erectile dysfunction inventory of treatment satisfaction questionnaire order 30 mg dapoxetine free shipping. The extrahepatic bile ducts are lined by a columnar mucosa with numerous mucous glands in the common bile duct erectile dysfunction filthy frank purchase dapoxetine pills in toronto. The density of nerve fibers and ganglia increases near the sphincter of Oddi impotence yahoo order dapoxetine overnight, but the nerve supply to the common bile duct and the sphincter of Oddi is the same as for the gallbladder. Isolated congenital absence of the gallbladder is very rare, with a reported incidence of 0. Before the diagnosis is made, the presence of an intrahepatic bladder or anomalous position must be ruled out. Duplication of the gallbladder with two separate cavities and two separate cystic ducts has an incidence of about one in every 4000 persons. This occurs in two major varieties: the more common form in which each gallbladder has its own cystic duct that empties independently into the same or different parts of the extrahepatic biliary tree, and as two cystic ducts that merge before they enter the common bile duct. Duplication is only clinically important when some pathologic processes affect one or both organs. A left-sided gallbladder with a cystic duct emptying into the left hepatic duct or the common bile duct and a retrodisplacement of the gallbladder are both extremely rare. A partial or totally intrahepatic gallbladder is associated with an increased incidence of cholelithiasis. Small ducts (of Luschka) may drain directly from the liver into the body of the gallbladder. If present, but not recognized at the time of a cholecystectomy, a bile leak with the accumulation of bile (biloma) may occur in the abdomen. Variations of how the common bile duct enters the duodenum are described in earlier, in the Bile Ducts section. Anomalies of the hepatic artery and the cystic artery are quite common, occurring in as many as 50% of cases. In about 20% of patients, the right hepatic artery comes off the superior mesenteric artery. The right hepatic artery may be vulnerable during surgical procedures, in particular when it runs parallel to the cystic duct or in the mesentery of the gallbladder. Cystic artery from right hepatic artery (accessory or replaced) from superior mesenteric artery, about 10%. Two cystic arteries, one from the right hepatic, the other from the common hepatic artery, rare. Two cystic arteries, one from the right hepatic, the other from the left hepatic artery, rare. The cystic artery branching from the right hepatic artery and running anterior to the common hepatic duct, rare. The normal adult consuming an average diet produces within the liver 500 to 1000 mL of bile a day. Vagal stimulation increases secretion of bile, whereas splanchnic nerve stimulation results in decreased bile flow. Hydrochloric acid, partly digested proteins, and fatty acids in the duodenum stimulate the release of secretin from the duodenum that, in turn, increases bile production and bile flow. Bile flows from the liver through to the hepatic ducts, into the common hepatic duct, through the common bile duct, and finally into the duodenum. Bile is mainly composed of water, electrolytes, bile salts, proteins, lipids, and bile pigments. Sodium, potassium, calcium, and chlorine have the same concentration in bile as in plasma or extracellular fluid. The pH of hepatic bile is usually neutral or slightly alkaline, but varies with diet; an increase in protein shifts the bile to a more acidic pH. The primary bile salts, cholate and chenodeoxycholate, are synthesized in the liver from cholesterol. They are conjugated there with taurine and glycine and act within the bile as anions (bile acids) that are balanced by sodium. Bile salts are excreted into the bile by the hepatocyte and aid in the digestion and absorption of fats in the intestines. The remainder is dehydroxylated (deconjugated) by gut bacteria, forming secondary bile acids deoxycholate and lithocholate. These are absorbed in the colon, transported to the liver, conjugated, and secreted into the bile. Eventually, about 95% of the bile acid pool is reabsorbed and returned via the portal venous system to the liver, the so-called enterohepatic circulation. Five percent is excreted in the stool, leaving the relatively small amount of bile acids to have maximum effect. Cholesterol and phospholipids synthesized in the liver are the principal lipids found in bile. The synthesis of phospholipids and cholesterol by the liver is, in part, regulated by bile acids. The color of the bile is due to the presence of the pigment bilirubin diglucuronide, which is the metabolic product from the breakdown of hemoglobin and is present in bile in concentrations 100 times greater than in plasma. Once in the intestine, bacteria convert it into urobilinogen, a small fraction of which is absorbed and secreted into the bile. Gallbladder Function the gallbladder, the bile ducts, and the sphincter of Oddi act together to store and regulate the flow of bile. The main function of the gallbladder is to concentrate and store hepatic bile and to deliver bile into the duodenum in response to a meal. In the fasting state, approximately 80% of the bile secreted by the liver is stored in the gallbladder. This storage is made possible because of the remarkable absorptive capacity of the gallbladder, as the gallbladder mucosa has the greatest absorptive power per unit area of any structure in the body. It rapidly absorbs sodium, chloride, and water against significant concentration gradients, concentrating the bile as much as 10-fold and leading to a marked change in bile composition. This rapid absorption is one of the mechanisms that prevent a rise in pressure within the biliary system under normal circumstances. Gradual relaxation as well as emptying of the gallbladder during the fasting period also plays a role in maintaining a relatively low intraluminal pressure in the biliary tree. The epithelial cells of the gallbladder secrete at least two important products into the gallbladder lumen: glycoproteins and hydrogen ions. The mucosal glands in the infundibulum and the neck of the gallbladder secrete mucus glycoproteins that are believed to protect the mucosa from the lytic action of bile and to facilitate the passage of bile through the cystic duct. This mucus makes up the colorless "white bile" seen in hydrops of the gallbladder resulting from cystic duct obstruction. The transport of hydrogen ions by the gallbladder epithelium leads to a decrease in the gallbladder bile pH. The acidification promotes calcium solubility, thereby preventing its precipitation as calcium salts. Gallbladder filling is facilitated by tonic contraction of the sphincter of Oddi, which creates a pressure gradient between the bile ducts and the gallbladder. In response to a meal, the gallbladder empties by a coordinated motor response of gallbladder contraction and sphincter of Oddi relaxation. Other hormonal and neural pathways also are involved in the coordinated action of the gallbladder and the sphincter of Oddi. Defects in the motor activity of the gallbladder are thought to play a role in cholesterol nucleation and gallstone formation. The vagus nerve stimulates contraction of the gallbladder, and splanchnic sympathetic stimulation is inhibitory to its motor activity. Parasympathomimetic drugs contract the gallbladder, whereas atropine leads to relaxation. Neurally mediated reflexes link the sphincter of Oddi with the gallbladder, stomach, and duodenum to coordinate the flow of bile into the duodenum. Antral distention of the stomach causes both gallbladder contraction and relaxation of the sphincter of Oddi. Hormonal receptors are located on the smooth muscles, vessels, nerves, and epithelium of the gallbladder. Vasoactive intestinal polypeptide inhibits contraction and causes gallbladder relaxation. Patients treated with somatostatin analogues and those with somatostatinoma have a high incidence of gallstones, presumably due to the inhibition of gallbladder contraction and emptying. Other hormones such as substance P and enkephalin affect gallbladder motility, but the physiologic role is unclear. It is a complex structure that is functionally independent from the duodenal musculature and creates a high-pressure zone between the bile duct and the duodenum. The sphincter of Oddi is about 4 to 6 mm in length and has a basal resting pressure of about 13 mmHg above the duodenal pressure. On manometry, the sphincter shows phasic contractions with a frequency of about four per minute and an amplitude of 12 to 140 mmHg. In 1924, the diagnosis of gallstones was improved significantly by the introduction of oral cholecystography by Graham and Cole. During fasting, with the sphincter of Oddi contracted and the gallbladder filling. In response to a meal, the sphincter of Oddi relaxed and the gallbladder emptying. If associated with an elevation of bilirubin, alkaline phosphatase, and aminotransferase, cholangitis should be suspected. Cholestasis, an obstruction to bile flow, is characterized by an elevation of bilirubin. In patients with biliary colic or chronic cholecystitis, blood tests will typically be normal. Ultrasound will show stones in the gallbladder with sensitivity and specificity of >90%. Stones are acoustically dense and reflect the ultrasound waves back to the ultrasonic transducer. Polyps may be calcified and reflect shadows, but do not move with change in posture. The patient has acute cholecystitis if a layer of edema is seen within the wall of the gallbladder or between the gallbladder and the liver in association with localized tenderness. When a stone obstructs the neck of the gallbladder, the gallbladder may become very large, but thin walled. The extrahepatic bile ducts are also well visualized by ultrasound, except for the retroduodenal portion. Dilation of the ducts in a patient with jaundice establishes an extrahepatic obstruction as a cause for the jaundice. Frequently, the site and, sometimes, the cause of obstruction can be determined by ultrasound. Small stones in the common bile duct frequently get lodged at the distal end of it, behind the duodenum, and are, therefore, difficult to detect. A dilated common bile duct on ultrasound, small stones in the gallbladder, and the clinical presentation allow one to assume that a stone or stones are causing the obstruction. Periampullary tumors can be difficult to diagnose on ultrasound, but beyond the retroduodenal portion, the level of obstruction and the cause may be visualized quite well. Ultrasound can be helpful in evaluating tumor invasion and flow in the portal vein, an important guideline for resectability of periampullary and pancreatic head tumors. It is dependent upon the skills and the experience of the operator, and it is dynamic. Obese patients, patients with Oral Cholecystography Once considered the diagnostic procedure of choice for gallstones, oral cholecystography has largely been replaced by ultrasonography. It involves oral administration of a radiopaque compound that is absorbed, excreted by the liver, and passed into the gallbladder. Stones are noted on a film as filling defects in a visualized, opacified gallbladder. Oral cholecystography is of no value in patients with intestinal malabsorption, vomiting, obstructive jaundice, and hepatic failure. Biliary scintigraphy provides a noninvasive evaluation of the liver, gallbladder, bile ducts, and duodenum with both anatomic and functional information. Uptake by the liver is detected within 10 minutes, and the gallbladder, the bile ducts, and the duodenum are visualized within 60 minutes in fasting subjects. The primary use of biliary scintigraphy is in the diagnosis of acute cholecystitis, which appears as a nonvisualized gallbladder, with prompt filling of the common bile duct and duodenum. Evidence of cystic duct obstruction on biliary scintigraphy is highly diagnostic for acute cholecystitis. False-positive results are increased in patients with gallbladder stasis, as in critically ill patients and in patients receiving parenteral nutrition. Filling of the gallbladder and common bile duct with delayed or absent filling of the duodenum indicates an obstruction at the ampulla. Biliary leaks as a complication of surgery of the gallbladder or the biliary tree can be confirmed and frequently localized by biliary scintigraphy. Through the catheter, a cholangiogram can be performed and therapeutic interventions done, such as biliary drain insertions and stent placements. It has a sensitivity and specificity of 95% and 89%, respectively, at detecting choledocholithiasis. It is the test of choice in evaluating the patient with suspected malignancy of the gallbladder, the extrahepatic biliary system, or nearby organs, in particular, the head of the pancreas. Computed tomography scan of the upper abdomen from a patient with cancer of the distal common bile duct. Once the endoscopic cholangiogram has shown ductal stones, sphincterotomy and stone extraction can be performed, and the common bile duct cleared of stones. In the hands of experts, the success rate of common bile duct cannulation and cholangiography is >90%.
Natural orifice translumenal endoscopic surgery applications in clinical practice drugs used for erectile dysfunction buy generic dapoxetine 90 mg on-line. Risk factors associated with perforated appendicitis in elderly patients presenting with signs and symptoms of acute appendicitis erectile dysfunction and proton pump inhibitors purchase line dapoxetine. Acute appendicitis in the octogenarians and beyond: a comparison with younger geriatric patients erectile dysfunction doctor exam 90 mg dapoxetine buy. Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss erectile dysfunction protocol free download pdf dapoxetine 90 mg order with amex. Overview of outcomes of laparoscopic and open Roux-en-Y gastric bypass in the United States impotence from prostate removal 60 mg dapoxetine buy otc. Optimum duration of prophylactic antibiotics in acute non-perforated appendicitis. The efficacy of postoperative oral antibiotics in appendicitis: a randomized prospective double-blinded study. Natural behavior and surgical treatment of appendiceal carcinoids: an analysis of 2,376 consecutive emergency appendectomies. A retrospective clinicopathological analysis of appendiceal tumors from 3,744 appendectomies: a single-institution study. Are we missing diagnostic opportunities in cases of carcinoid tumours of the appendix Carcinoid tumour of the appendix: an analysis of 1,485 consecutive emergency appendectomies. Incidence and odds ratio of appendicitis as first manifestation of colon cancer: a retrospective analysis of 1873 patients. Primary malignant neoplasms of the appendix: a population-based study from the Surveillance, Epidemiology and End Results program, 19731998. Appendiceal neoplasms with peritoneal dissemination: outcomes after cytoreductive surgery and intraperitoneal hyperthermic chemotherapy. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peritonei syndrome Survival and health outcomes after cytoreductive surgery with intraperitoneal hyperthermic chemotherapy for disseminated peritoneal cancer of appendiceal origin. Leukaemia and lymphoma of the appendix presenting as acute appendicitis or acute abdomen. The liver is the largest gland in the body and performs a diverse spectrum of functions. Computed tomography and magnetic resonance imaging with contrast enhancement constitute the mainstays for the radiologic evaluation of the liver. Acute liver failure rapidly progresses to hepatic coma and death even with maximal medical therapy. Cirrhosis is the end result of chronic hepatic insult, and further deterioration can lead to the development of end-stage liver disease, which carries a high mortality rate. Acute variceal bleeding should be managed with aggressive resuscitation and prompt endoscopic diagnosis with hemorrhage control. The transjugular intrahepatic portosystemic shunt procedure can be considered for cases refractory to medical treatment. In most instances, these lesions can be reliably diagnosed by their characteristic features on imaging. Many options exist for the treatment of hepatocellular carcinomas, and these cases are best managed by a multidisciplinary liver transplant team. Under a protocol with strict eligibility criteria, patients with unresectable tumors can be considered for liver transplantation following neoadjuvant chemoradiation, with survival rates that compare favorably with the rates for resection. The resectability of colorectal cancer metastases to the liver is primarily determined by the volume of the future liver remnant and the health of the background liver and not actual tumor number. Laparoscopic liver resections can be performed safely by experienced surgeons in selected patients and have been shown to produce comparable morbidity and mortality rates to open resections. According to Greek mythology, Zeus was furious with the Titan Prometheus because he gave fire to mortals. In return, Zeus chained Prometheus to Mount Caucasus and sent his giant eagle to eat his liver during the day, only to have it regenerate at night. Although this is folklore, the principles are correct that after hepatic resection, the remnant liver will hypertrophy over weeks to months to regain most of its original liver mass. There are scattered reports of liver surgery for battlefield injuries, but the first recorded elective hepatic resection was done in 1888 in Germany by Langenbuch. There followed reports of liver resections in the United States (Tiffany, 1890) and Europe (Lucke, 1891), as well as the first large series of hepatic resections by Keen in 1899. Work by Rex, Cantlie, and others laid the groundwork for experimental and clinical reports in the 1950s by Couinaud, Hjortsjo, Healey, Lortat-Jacob, and Starzl. It resides in the right upper abdominal cavity beneath the diaphragm and is protected by the rib cage. The round ligament is the remnant of the obliterated umbilical vein and enters the left liver hilum at the front edge of the falciform ligament. The falciform ligament separates the left lateral and left medial segments along the umbilical fissure and anchors the liver to the anterior abdominal wall. The left and right triangular ligaments secure the two sides of the liver to the diaphragm. Extending from the triangular ligaments anteriorly on the liver are the coronary ligaments. The right coronary ligament also extends from the right undersurface of the liver to the peritoneum overlying the right kidney, thereby anchoring the liver to the right retroperitoneum. These ligaments (round, falciform, triangular, and coronary) can be divided in a bloodless plane to fully mobilize the liver to facilitate hepatic resection. The hepatoduodenal ligament is known as the porta hepatis and contains the common bile duct, the hepatic artery, and the portal vein. This passage connects directly to the lesser sac and allows complete vascular inflow control to the liver when the hepatoduodenal ligament is clamped using the Pringle maneuver. Hepatic ligaments suspending the liver to the diaphragm and anterior abdominal wall. The left lateral and left medial segments also are referred to as sections as defined in the Brisbane 2000 terminology, which is outlined later in the section titled "Hepatic Resection. Couinaud divided the liver into eight segments, numbering them in a clockwise direction beginning with the caudate lobe as segment I. Most surgeons still refer to segment I as the caudate lobe, rather than segment I. Arterial anatomy of the upper abdomen and liver, including the celiac trunk and hepatic artery branches. Additional functional anatomy was highlighted by Bismuth based on the distribution of the hepatic veins. The three hepatic veins run in corresponding scissura (fissures) and divide the liver into four sectors. The main scissura contains the middle hepatic vein and separates the right and left livers. The left scissura contains the course of the left hepatic vein and separates the left posterior and left anterior sectors. Hepatic Artery the liver has a dual blood supply consisting of the hepatic artery and the portal vein. The hepatic artery delivers approximately 25% of the blood supply, and the portal vein approximately 75%. The common hepatic artery then divides into the gastroduodenal artery and the hepatic artery proper. The right gastric artery typically originates off of the hepatic artery proper, but this is variable. This "classic" or standard arterial anatomy is present in only approximately 76% of cases, with the remaining 24% having variable anatomy. It is critical to arterial (and anatomic variants to 1 understand thecomplicationsbiliary)operating on the liver, avoid surgical when gallbladder, pancreas, or adjacent organs. When there is a replacement or accessory right hepatic artery, it travels posterior to the portal vein and then takes up a right lateral position before diving into the liver parenchyma. In approximately 3% to 10% of cases, there exists a replacement (or accessory) left hepatic artery coming off of the left gastric artery and running obliquely in the gastrohepatic ligament anterior to the caudate lobe before entering the hilar plate at the base of the umbilical fissure. Another important point is that the right hepatic artery passes deep and posterior to the common bile duct approximately 88% of the time but crosses anterior to the common bile duct in approximately 12% of cases. Portal Vein the portal vein is formed by the confluence of the splenic vein and the superior mesenteric vein. The main portal vein traverses the porta hepatis before dividing into the left and right portal vein branches. The left portal vein also provides the dominant inflow branch to the caudate lobe (although branches can arise from the main and right portal veins also), usually close to the bend between the transverse and umbilical portions. The division of the right portal vein is usually higher in the hilum and may be close to (or inside) the liver parenchyma at the hilar plate. Twenty percent to thirty-five percent of individuals have aberrant portal venous anatomy, with portal vein trifurcation or an aberrant branch from the left portal vein supplying the right anterior lobe being the most frequent. The portal vein drains the splanchnic blood from the stomach, pancreas, spleen, small intestine, and majority of the colon to the liver before returning to the systemic circulation. The portal vein pressure in an individual with normal physiology is low at 3 to 5 mmHg. The portal vein is valveless, however, and in the setting of portal hypertension, the pressure can be quite high (20 to 30 mmHg). This results in decompression of the systemic circulation through portocaval anastomoses, most commonly via the coronary (left gastric) vein, which produces esophageal and gastric varices with a propensity for major hemorrhage. Another branch of the main portal vein is the superior pancreaticoduodenal vein (which comes off low in an anterior lateral position and is divided during pancreaticoduodenectomy). Closer to the liver, the main portal vein typically gives off a short branch (posterior lateral) to the caudate process on the right side. It is important to identify this branch and ligate it during hilar dissection for anatomic right hemihepatectomy to avoid avulsion. The portal vein is formed by the confluence of the splenic and superior mesenteric veins. The coronary (left gastric) vein drains into the portal vein in the vicinity of the confluence. This can be a source of torrential bleeding if control of it is lost during right hepatectomy. The hepatic vein branches bisect the portal branches inside the liver parenchyma. The cystic duct itself also has a variable pattern of drainage into the common bile duct. This can lead to potential injury or postoperative bile leakage during cholecystectomy or hepatic resection, and the surgeon needs to expect these variants. Neural Innervation and Lymphatic Drainage Bile Duct and Hepatic Ducts Within the hepatoduodenal ligament, the common bile duct lies anteriorly and to the right. It gives off the cystic duct to the gallbladder and becomes the common hepatic duct before dividing into the right and left hepatic ducts. In general, the hepatic ducts follow the arterial branching pattern inside the liver. The right anterior hepatic duct usually enters the liver above the hilar plate, whereas the right posterior duct dives behind the right portal vein and can be found on the surface of the caudate process before entering the liver. The left hepatic duct typically has a longer extrahepatic course before giving off segmental branches behind the left portal vein at the base of the umbilical fissure. Considerable variation exists, and in 30% to 40% of the parasympathetic innervation of the liver comes from the left vagus, which gives off the anterior hepatic branch, and the right vagus, which gives off the posterior hepatic branch. The sympathetic innervation involves the greater thoracic splanchnic nerves and the celiac ganglia, although the function of these nerves is poorly understood. The denervated liver after hepatic transplantation seems to function with normal capacity. As described by Couinaud in 1957, the bifurcation of the hepatic ducts has a variable pattern in approximately 40% of cases. This is particularly important for resection of hilar cholangiocarcinoma, which has a high incidence of lymph node metastases. One crucial role is the processing of absorbed nutrients through the metabolism of glucose, lipids, and proteins. The liver maintains glucose concentrations in a normal range over both short and long periods by performing several important roles in carbohydrate metabolism. In the fasting state, the liver ensures a sufficient supply of glucose to the central nervous system. The liver can produce glucose by breaking down glycogen through glycogenolysis and by de novo synthesis of glucose through gluconeogenesis from noncarbohydrate precursors such as lactate, amino acids, and glycerol. In the postprandial state, excess circulating glucose is removed by glycogen synthesis or glycolysis and lipogenesis. The liver also plays a central role in lipid metabolism through the formation of bile and the production of cholesterol and fatty acids. Protein metabolism occurs in the liver through amino acid deamination, resulting in the production of ammonia as well as the production of a variety of amino acids. In addition to metabolism, the liver also is responsible for the synthesis of most circulating plasma proteins. Among these proteins are albumin, factors of the coagulation and fibrinolytic systems, and compounds of the complement cascade. Furthermore, the detoxification 2 of many substances through drug metabolism occurs in the 1270 liver, as do immunologic responses through the many immune cells found in its reticuloendothelial system. In the liver, it is conjugated to glucuronic acid to form bilirubin diglucuronide in a reaction catalyzed by the enzyme glucuronyl transferase, making it water soluble. The majority of conjugated bilirubin is excreted in the intestine as waste, because the intestinal mucosa is relatively impermeable to conjugated bilirubin. However, it is permeable to unconjugated bilirubin and urobilinogens, a series of bilirubin derivatives formed by the action of bacteria.
Order dapoxetine 60 mg without a prescription. Treatment for Erectile Dysfunction in young males or men natural treatment.
References
- Von Wendt L, Simila S, Hirvasniemi A, Suvanto E. Nonketotic hyperglycinemia. A clinical analysis of 19 Finnish patients. Monogr Hum Genet 1978;9:58.
- Leonard MP, Canning DA, Epstein JI, et al: Local tissue reaction to the suburethral injection of glutaraldehyde cross-linked bovine collagen in humans, J Urol 143:1209, 1990. Leonard MP, Dharamsi N, Williot PE: Outcome of gastrocystoplasty in tertiary pediatric urology practice. Presented at Section on Urology meeting, American Academy of Pediatrics, Washington, DC, 1999.
- Leventhal BG, Wittes RE. Research Methods in Clinical Oncology. New York: Raven Press; 1988.
- Suh, R.S., Faerber, G.J., Wolf, J.S. Predictive factors for applicability and success with endoscopic treatment of upper tract urothelial carcinoma. J Urol 2003;170:2209-2216.
- Lawson, R.K., Murphy, J.B., Taylor, A.J., Jacobs, S.C. Retrograde method for percutaneous access to kidney. Urology 1983;22:580-582.
- Stone ME. Current status of mechanical circulatory assistance. Semin Cardiothorac Vasc Anesth 2007; 11:185-204.
- Lu W, Tao Y, Wisniewski AB, et al: Different outcomes of hypospadias surgery between North America, Europe and China: is patient age a factor? Nephrourol Mon 4(4):609n612, 2012.
- Pugh TJ, Ballonoff A, Rusthoven KE, et al. Cardiac mortality in patients with stage I and II diffuse large B-cell lymphoma treated with and without radiation: a Surveillance, Epidemiology, and End-Results analysis. Int J Radiat Oncol Biol Phys 2010:76(3):845-849.