
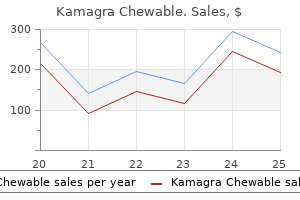
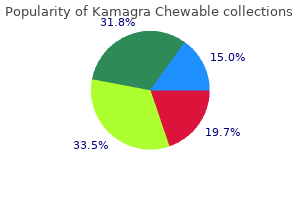
Kamagra Chewable
| Contato
Página Inicial
Mihir K. Bhayani, MD
- Fellow, Department of Head and Neck Surgery
- University of Texas MD Anderson Cancer Center
- Houston, Texas
Effect of antioxidant vitamin supplementation on cardiovascular outcomes: a meta-analysis of randomized controlled trials impotence exercises for men kamagra chewable 100 mg visa. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: systematic review and meta-analysis of randomised controlled trials erectile dysfunction cause kamagra chewable 100 mg order online. Coenzyme Q versus hypertension: does CoQ decrease endothelial superoxide generation Nutraceuticals impotence is the cheap kamagra chewable 100 mg without a prescription, vitamins erectile dysfunction guilt in an affair order 100 mg kamagra chewable with visa, antioxidants erectile dysfunction herbal buy kamagra chewable in india, and minerals in the prevention and treatment of hypertension. The relationship between coenzyme Q10, oxidative stress, and antioxidant enzymes activities and coronary artery disease. Effects of coenzyme Q10 supplementation (300 mg/day) on antioxidation and anti-inflammation in coronary artery disease patients during statins therapy: a randomized, placebo-controlled trial. Effects of coenzyme Q10 supplementation on inflammatory markers (high-sensitivity C-reactive protein, interleukin-6, and homocysteine) in patients with coronary artery disease. Effect of coenzyme Q10 administration on endothelial function and extracellular superoxide dismutase in patients with ischaemic heart disease: a double-blind, randomized controlled study. Coenzyme Q10 in the treatment of hypertension: a meta-analysis of the clinical trials. Effects of coenzyme Q10 on vascular endothelial function in humans: a meta-analysis of randomized controlled trials. Long-term effects of resveratrol supplementation on suppression of atherogenic lesion formation and cholesterol synthesis in apo E-deficient mice. Resveratrol toxicity: effects on risk factors for atherosclerosis and hepatic oxidative stress in standard and high-fat diets. Resveratrol improves myocardial perfusion in a swine model of hypercholesterolemia and chronic myocardial ischemia. A new insight into resveratrol as an atheroprotective compound: inhibition of lipid peroxidation and enhancement of cholesterol efflux. Upregulation of endogenous antioxidants and phase 2 enzymes by the red wine polyphenol, resveratrol in cultured aortic smooth muscle cells leads to cytoprotection against oxidative and electrophilic stress. Effect of resveratrol, a natural polyphenolic compound, on platelet activation induced by endotoxin or thrombin. Inhibitory effects of resveratrol on platelet activation induced by thromboxane a(2) receptor agonist in human platelets. Long-term resveratrol administration reduces metabolic disturbances and lowers blood pressure in obese Zucker rats. Resveratrol and small artery compliance and remodeling in the spontaneously hypertensive rat. Grape resveratrol increases serum adiponectin and downregulates inflammatory genes in peripheral blood mononuclear cells: a triple-blind, placebo-controlled, one-year clinical trial in patients with stable coronary artery disease. Cardioprotection by resveratrol: a human clinical trial in patients with stable coronary artery disease. Consumption of flavonoid-rich foods and increased plasma antioxidant capacity in humans: cause, consequence, or epiphenomenon Pomegranate juice consumption inhibits serum angiotensin converting enzyme activity and reduces systolic blood pressure. Favorable effects of concord grape juice on endothelial function and arterial stiffness in healthy smokers. Chocolate and blood pressure in elderly individuals with isolated systolic hypertension. Short-term administration of dark chocolate is followed by a significant increase in insulin sensitivity and a decrease in blood pressure in healthy persons. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide: a randomized controlled trial. Blood pressure is reduced and insulin sensitivity increased in glucose-intolerant, hypertensive subjects after 15 days of consuming high-polyphenol dark chocolate. Dark chocolate or tomato extract for prehypertension: a randomised controlled trial. Effect of dark chocolate on arterial function in healthy individuals: cocoa instead of ambrosia Chocolate consumption in relation to blood pressure and risk of cardiovascular disease in German adults. The effectiveness and cost effectiveness of dark chocolate consumption as prevention therapy in people at high risk of cardiovascular disease: best case scenario analysis using a Markov model. Tea catechins and polyphenols: health effects, metabolism, and antioxidant functions. Impaired L-arginine transport and endothelial function in hypertensive and genetically predisposed normotensive subjects. Asymmetric dimethylarginine, oxidative stress, and vascular nitric oxide synthase in essential hypertension. Short-term treatment with L-arginine prevents the smoking-induced impairment of endothelial function and vascular elastic properties in young individuals. Blood pressure and metabolic changes during dietary L-arginine supplementation in humans. Long-term N-acetylcysteine and L-arginine administration reduces endothelial activation and systolic blood pressure in hypertensive patients with type 2 diabetes. Oral arginine improves blood pressure in renal transplant and hemodialysis patients. Adverse effects of supplemental L-arginine in atherosclerosis: consequences of methylation stress in a complex catabolism The effect of L-arginine and creatine on vascular function and homocysteine metabolism. Mitochondrial decay in the aging rat heart: evidence for improvement by dietary supplementation with acetyl-L-carnitine and/or lipoic acid. Acetyl-L-carnitine fed to old rats partially restores mitochondrial function and ambulatory activity. Effects of L-carnitine supplementation on oxidative stress and antioxidant enzymes activities in patients with coronary artery disease: a randomized, placebo-controlled trial. Alpha-lipoic acid as a dietary supplement: molecular mechanisms and therapeutic potential. Lipoic acid as a potential therapy for chronic diseases associated with oxidative stress. Investigations on the pharmacokinetics of alpha-lipoic acid in healthy volunteers. Ameliorating hypertension and insulin resistance in subjects at increased cardiovascular risk: effects of acetyl-L-carnitine therapy. In vivo downregulation of T helper cell 1 immune responses reduces atherogenesis in apolipoprotein E-knockout mice. Selective interleukin-12 synthesis defect in 12/15-lipoxygenase-deficient macrophages associated with reduced atherosclerosis in a mouse model of familial hypercholesterolemia. Interleukin-10 and pentoxifylline inhibit C-reactive protein-induced tissue factor gene expression in peripheral human blood monocytes. A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic efficacy. Pentoxifylline reduces pro-inflammatory and increases anti-inflammatory activity in patients with coronary artery diseaseea randomized placebo-controlled study. Multiple inhibitory effects of garlic extracts on cholesterol biosynthesis in hepatocytes. Water-soluble organosulfur compounds of garlic inhibit fatty acid and triglyceride syntheses in cultured rat hepatocytes. Cholesterol-lowering effect of garlic extracts and organosulfur compounds: human and animal studies. Garlic reduces plasma lipids by inhibiting hepatic cholesterol and triacylglycerol synthesis. The effects of time-released garlic powder tablets on multifunctional cardiovascular risk in patients with coronary artery disease. Ginkgo biloba extract improves coronary artery circulation in patients with coronary artery disease: contribution of plasma nitric oxide and endothelin-1. Effects of pycnogenol on endothelial function in patients with stable coronary artery disease: a double-blind, randomized, placebo-controlled, cross-over study. A prospective study of consumption of carotenoids in fruits and vegetables and decreased cardiovascular mortality in the elderly. Vitamin E and vitamin C supplement use and risk of all-cause and coronary heart disease mortality in older persons: the Established Populations for Epidemiologic Studies of the Elderly. Antioxidant consumption and risk of coronary heart disease: emphasis on vitamin C, vitamin E, and beta-carotene: a statement for healthcare professionals from the American Heart Association. Effect of a traditional Mediterranean diet on lipoprotein oxidation: a randomized controlled trial. The relationship between dose of vitamin E and suppression of oxidative stress in humans. Treatment of asymptomatic adults with elevated coronary calcium scores with atorvastatin, vitamin C, and vitamin E: the St. Effect of vitamins C and E on progression of transplant-associated arteriosclerosis: a randomised trial. Randomised trial of alpha-tocopherol and beta-carotene supplements on incidence of major coronary events in men with previous myocardial infarction. Effects of long-term daily low-dose supplementation with antioxidant vitamins and minerals on structure and function of large arteries. Lack of effect of long-term supplementation with beta carotene on the incidence of malignant neoplasms and cardiovascular disease. Mortality associated with low plasma concentration of beta carotene and the effect of oral supplementation. Low-dose aspirin and vitamin E in people at cardiovascular risk: a randomised trial in general practice. Probucol and multivitamins in the prevention of restenosis after coronary angioplasty. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial. Early vitamin C and E supplementation and cardiac allograft vasculopathy: 10-year follow-up from a randomized, controlled study. Effect of high-dose alpha-tocopherol supplementation on biomarkers of oxidative stress and inflammation and carotid atherosclerosis in patients with coronary artery disease. Effects of hormone replacement therapy and antioxidant vitamin supplements on coronary atherosclerosis in postmenopausal women: a randomized controlled trial. Pentoxifylline decreases serum level of adhesion molecules in atherosclerosis patients. This subsequently decreases blood supply downstream, which can manifest in a variety of clinical presentations including ischemic heart disease, peripheral vascular disease, and stroke [1]. The underlying pathology is a chronic process that occurs at points of disturbed blood flow, such as branch points [2]. Approaches to managing atherogenesis are centered around minimizing the risk factors that contribute to plaque progression. Gene therapy is the process where genetic material is transfected to a new host where it will alter the phenotype of the cell. Certainly, it is not in use currently in clinical practice, but animal studies have shown promise that this technique may act as an adjunct to current practice. It is characterized by endothelial dysfunction [3], vascular inflammation [4], and oxidative stress [5], resulting in the formation of a plaque below the endothelium. Stable plaques are those with a thick fibrous cap made of strong connective tissue. Over time, further inflammatory cells accumulate within the cap, weakening the fibrous material and making it prone to rupture [7]. Rupture can lead to complete occlusion of the vessel through thrombus formation or downstream occlusion from an embolism. As plaque formation involves an array of steps, so too are there a large number of genes that can be targeted [8]. Vectors carrying genes can be delivered systemically, potentially initiating change throughout the vascular endothelium, or locally. As a rule, nonviral vectors are generally less effectual, as they interact less efficiently with host cells compared with viral vectors [9]. The inflammatory response potentiates platelet aggregation, and thus can result in thrombus formation at the area of treatment [11]. Viral vectors include adenovirus, adeno-associated virus, lentivirus, retrovirus, and herpes simplex virus. Adenoviruses are used most commonly to deliver genes in atherosclerosis as they grow high titers and express genes in nonmitotic cellsdideal for targeting the endothelium [12]. However, there exist several disadvantages, notably, their high immunogenicity and formation of neutralizing antibodies [15]. They do not induce an inflammatory response and can carry genetic material of vast quantities, yet are limited by poor uptake into cells and subsequently poor entry into the nucleus to enable transcription [19]. Some of the processes targeted, such as inflammation, are not uniquely seen in atherosclerosis. Therefore, altering these genes may change many other pathophysiological pathways. Drug-eluting stents are already in use, coated with drugs such as tacrolimus, which reduce in-stent restenosis [23]. As both grafts and stents are outside the body 304 Coronary Artery Disease for some time and are deployed at a local site of plaque formation, these are very interesting prospects for transferring gene therapy to clinical practice. Neointimal hyperplasia was reduced 2 weeks postinjury in the transfected groups compared with controls. The vessels of these mouse models produced large quantities of superoxide, which may explain these findings [29].
The explanation should include the nature o the examination and what the patient can expect impotence 25 years old order kamagra chewable 100 mg otc, how long it will take erectile dysfunction medications causes symptoms order 100 mg kamagra chewable free shipping, the need to remain still impotence group purchase kamagra chewable online, and reassurance that the technologist will be monitoring the patient throughout the procedure vyvanse erectile dysfunction treatment safe kamagra chewable 100 mg. Breathing instructions should be given impotence exercises for men buy kamagra chewable once a day, and breathing can be rehearsed i required. I a clinical history has not already been provided by the re erring physician, the technologist should take one. The equipment can appear intimidating to a patient, and a thorough explanation by the technologist can alleviate ears and ensure a success ul diagnostic procedure. Additional parameters important to the examination are contained in the selected protocol and include kilovoltage, milliamperage, pitch, f eld o view, slice thickness, table indexing, reconstruction algorithms, and display windows. Axial scans are viewed as though the viewer were acing the patient and looking at the scan rom the oot end o the patient. Care ul selection o the volume o the injection and the rate o ow peak ensures optimal vascular and organ enhancement levels. Injecting a saline bolus at this time allows or increased duration o contrast enhancement as the pooled contrast material is ushed rom the veins and the contrast medium bolus is propelled orward. The injector automatically switches to a saline syringe a ter the contrast medium has been injected. Re er to Chapter 14 or in ormation regarding venipuncture, contrast medium contraindications, and reactions. T communicate optimal patient imaging strategies to re erring o physicians, and to be available or consultation 4. Ideal exposure actors, slice thickness, and critical organ dose-sparing measures must be employed. The highest radiation exposure occurs nearest the patient because o the scatter produced in the patient- possible, it is desirable to maintain i maximum distance rom the source. These iodinated contrast media usually are administered as bolus injections but may be introduced slowly via an intravenous in usion. Oxygen must be in constant supply because total oxygen deprivation or 4 minutes can lead to permanent brain cell damage. Similarly, glucose must be continually available because carbohydrate storage in the brain is limited. Glucose, oxygen, and certain ions pass readily rom the circulatory blood into extracellular uid and then into brain cells. Still others, such as proteins, most antibiotics, and contrast media, do not pass at all rom the normal cranial capillary system into brain cells. Brain tissue di ers rom other tissues in that it possesses a natural barrier to the passage o certain substances. Patient dose is related to pitch: a lower pitch results in a higher dose (slice overlap). This technique allows the minimum dose required per slice to be determined by the scanogram; each slice then is obtained with the use o optimal mAs. Dose to radiosensitive organs (eyes, breasts, pelvis, and thyroid) also can be reduced by applying bismuth shields to the patient. In 2007, the Alliance or Radiation Sa ety in Pediatric Imaging in a joint e ort with the Society or Pediatric Radiology, American College o Radiology, American Society or Radiologic T echnologists, and American Association o Physicists in Medicine implemented the Image Gently campaign. The Image Gently campaign asks that every member o the health care team take the ollowing pledge: · T make the Image Gently message a priority in sta commuo nications this year · T review the protocol recommendations and, where necessary, o implement adjustments to our processes · T respect and listen to suggestions rom every member o the o imaging team on ways to ensure changes are made · T communicate openly with parents1 o In October 2010, the American College o Radiology, Radiological Society o North America, American Society o Radiologic T echnologists, and American Association o Physicists in Medicine jointly developed the Image Wisely campaign to promote the reduction o radiation exposure to adult patients. Rotation is corrected by aligning the midsagittal plane perpendicular to the oor o the room. Two anatomic structures that are compared are the external auditory canals and zygomatic arches or symmetry. Ensuring the proper positioning o the head allows or a more accurate assessment o anatomy and pathology without the in uence o positional asymmetry. Movement o the head and neck or correction o tilt and rotation should not be per ormed in a patient with a suspected cervical spine injury. A scanogram must be obtained be ore the procedure is begun to allow the technologist to determine the range o the scan. In addition to window setting or so t tissue and bone, there are other special processing algorithm s (mathematical calculations and processes applied during image reconstruction) or demonstration o specif c anatomy. Included with the axial images is the corresponding lateral skull radiograph showing the slice level. The patient has a history o cancer that has metastasized to the brain as demonstrated by the three separate lesions. Contrast medium enhancement is necessary or most suspected neoplasia because o possible breakdown o the normal blood-brain barrier, as described in the discussion o contrast media and the blood-brain barrier. A subdural hematoma is a blood clot that orms between the dura mater and the sur ace o the brain as a result o damage to cerebral venous circulation. A subarachnoid hemorrhage may be traumatic or nontraumatic and represents bleeding into the subarachnoid space. Ce re b ro va scu la r Accide n t (Stro ke) A cerebrovascular accident may be caused by a rupture or occlusion o an artery in the brain. Common pathologic indications include the ollowing: · Congenital abnormalities · T rauma · In ection or abscess · T umors o the nasopharynx, oropharynx, parotid gland, and larynx Be ore the procedure begins, metallic objects must be removed, and the patient is positioned supine on the table. A scanogram, or scout image, is obtained to determine the range o the examination, usually rom the skull base to the thoracic inlet, with the use o 2- to 3-mm slices. The patient should be instructed to re rain rom swallowing and rom causing any orm o upper airway movement. T help distinguish the o esophagus rom surrounding so t tissue, the patient may be asked to swallow low-density radiopaque esophageal paste. When extremities are imaged, it is desirable to image both extremities or comparison purposes. Intravenous contrast media may be help ul in assessing tumors, and an intra-articular injection o contrast medium (negative or positive) may be required to study the joints. Clinical applications include assessment o trauma to the ace, spine, pelvis, shoulder, and knee and evaluation o congenital abnormalities and trauma. This technique requires high contrast between the lumen and surrounding tissues so that the internal sur aces o the structure o interest can be identif ed or image ormatting. Most endoscopic applications rely on air as the contrast medium o choice; however, depending on the procedure, there may be an indication or another contrast medium. It is use ul in the investigation o colon pathology, including polyps, tumors, diverticula, and other de ects and strictures within the large intestine. Be ore the procedure is begun, the patient must undergo bowel preparation to ensure that no ecal debris in the large intestine may obscure anatomy or pathology. T provide the required contrast, air or carbon dioxide is instilled o into the large intestine through a small tube inserted into the rectum. This gas serves to distend the large intestine to demonstrate the intestinal wall completely. Because no sedation is (typically) required, the patient is able to leave and resume normal diet and activities a ter the procedure. Risks or the procedure are related to bowel preparation, rectal tube insertion, and colon insu ation. Feedback rom patients typically indicates that they f nd the virtual endoscopy procedure less uncom ortable and pain ul than conventional colonoscopy. Be ore the procedure is per ormed, solid ood should be withheld rom the patient or 8 to 12 hours, but the patient should be well hydrated. Under uoroscopic guidance, an intestinal catheter is inserted nasally and is advanced distal to the duodenojejunal exure. Although uncom ortable or the patient, this nasal approach usually is better tolerated than the oral approach. Use o an electromechanical injector and a high injection rate are necessary to ensure rapid and equal small bowel distention. An intravenous injection o iodinated contrast medium o ten is given during this procedure to gain additional clinical in ormation. Two commonly used substances include a dilute barium sul ate solution and a methylcellulose preparation. I there is risk o per oration or leakage, the barium sul ate solution is contraindicated. With in ormation rom the data set rom the volumetric acquisition, an image is created rom the brightest voxels. The image is best viewed in animated ormat because this shows sur ace in ormation best, although depth and occlusion in ormation is lost. Calcif ed plaque, which occurs in chronic coronary artery disease, also may be visualized. The patient table or couch is stationary, with the body section that is being imaged positioned in the gantry. Partially reconstructed images can be obtained and displayed at the rate o 8 to 12 images per second. T echnical advances have provided improved image quality and speed- and will continue to do so. Depending on the site or biopsy, the patient may be positioned supine, prone, or lateral. The patient is scanned to localize the tumor, the area is prepared and anesthetized, and the needle is placed. Possible complications associated with the procedure include in ection, hemorrhage, pneumothorax (rom a transpleural puncture or a lung lesions), and pancreatitis (i a pancreatic biopsy is per ormed). For percutaneous abscess drainage, the patient is scanned to localize the abscess, the area is prepared and anesthetized, and the needle is placed. When the needle is in optimal position, a guidewire is placed, ollowed by a catheter. The catheter is sutured into place, and the abscess drains or approximately 24 to 48 hours. Linear attenuation coef cient: Numeric expression o the decrease in radiation intensity that ollows transmission through matter. Networking: Hardware and so tware that allow computers to be connected or the purpose o sharing resources and interacting. Slip rings: Devices that transmit electrical energy and allow continuous rotation o the x-ray tube or volumetric acquisition. Voxel: V olume element; corresponds to a three-dimensional tissue volume, having height, width, and depth; each pixel represents a voxel when an image is viewed. Windowing: Adjustment o the window level and window width (brightness and image contrast) by the user. Workstation: Computer that serves as a digital post-processing station or an image review station. The use o other imaging modalities o ten provides a level o detail that can exceed f uoroscopic or conventional imaging. However, the special procedures discussed in this chapter are still being per ormed in medical centers and clinics, and technologists should have a basic understanding o them. When these procedures are per ormed in the general imaging department, it is important or the technologist to ollow Image Gently and Image Wisely guidelines or principles (see Chapter 1). Advances in imaging technology provide an avenue or physicians and technologists to reduce medical radiation exposure greatly. Fe mur Arthrograms o the shoulder and knee, the most common arthrography procedures being per ormed today, are described and illustrated in this chapter. The knee is subject to considerable stress, especially during sports activities, and many o the pathologic processes that occur in the knee are due to trauma. Any arthrographic procedure should be thoroughly explained to the patient be ore the examination to preclude patient anxiety. The patient should be advised o any complications and must sign an in ormed consent orm. Typically, image acquisition is obtained during f uoroscopy through digital spots or last image hold. The sling is used to provide lateral or medial stress to "open up" the appropriate area o the joint to visualize the meniscus better during f uoroscopy. The technologist should be aware o any speci c accessory equipment needs a particular physician may have to ensure that the procedure is e ciently per ormed. With the site prepared, draped, and anesthetized, the physician introduces the needle through the skin and underlying tissues into the joint space. I the f uid appears abnormal (cloudy), it should be sent to the laboratory or assessment. When all the f uid has been aspirated, the contrast agent or agents are injected into the joint. With the contrast agent injected, the knee is gently f exed, which produces a thin, even coating o the so t tissue structures with the positive medium. I the radiographs appear normal, the patient is directed to exercise the shoulder, and the radiographs are repeated. The physician manipulates the joint and takes f uoroscopic spot images as the area o interest is demonstrated by the contrast agent. Shoulder arthrography is indicated when a patient presents with chronic pain or generalized weakness and when tears in the rotator cu are suspected. Contrast injection is monitored under f uoroscopic control, and conventional imaging is done with the overhead x-ray tube. As with the knee arthrogram, the technologist should be aware o any speci c accessory equipment needs a particular physician may have to ensure that the procedure is e ciently per ormed. A double-contrast study demonstrates speci c areas better, such as the in erior portion o the rotator cu, when images are obtained with the patient upright. A ter the area has been anesthetized, the physician uses f uoroscopy to guide the needle into the joint space.
Cheap kamagra chewable 100 mg with visa. Erectile Dysfunction Natural Ayurvedic Remedies.
The cervix is the distal cylindrical portion that projects into the vagina erectile dysfunction pills australia kamagra chewable 100 mg order, ending as the external os impotence quotes the sun also rises proven kamagra chewable 100 mg. The middle layer erectile dysfunction drugs prostate cancer trusted kamagra chewable 100 mg, the m yom etrium erectile dysfunction treatment delhi purchase kamagra chewable overnight delivery, consists o smooth muscle and constitutes most o the uterine tissue erectile dysfunction doctor in bangalore order kamagra chewable 100 mg without prescription. The outer sur ace o the uterus, the serosa, is lined with peritoneum and orms a capsule around the uterus. The uterine tubes are approximately 10 to 12 cm in length and 1 to 4 mm in diameter. They are subdivided into our segments: (1) the proximal portion o the tube, the interstitial segment, communicates with the uterine cavity. The distal in undibulum portion o the uterine tubes containing the mbriae opens into the peritoneal cavity. It is absorbed easily by the patient, does not leave a residue within the reproductive tract, and provides adequate visualization. However, this medium causes pain when injected within the uterine cavity, and the pain may persist or several hours a ter the procedure. In the past, oil-base contrast medium that allowed or maximal visualization o uterine structures was used. However, it has a very slow absorption rate and persists in the body cavities or an extended time. It also introduces the risk that an oil embolus may orm that could reach the lungs. The amount o contrast medium to be introduced into the reproductive tract varies depending on physician pre erence. Injection o contrast medium may dilate or straighten a narrowed, tortuous, or occluded uterine tube. Abnormal uterine bleeding, pelvic pain, and pelvic ullness are typical symptoms exhibited by patients. A third indication is evaluation o the uterine tube a ter tubal ligation or reconstructive surgery. T avoid the possibility o that the patient may be pregnant, the examination typically is per ormed 7 to 10 days a ter the onset o menstruation. Other contraindications include acute pelvic inf ammatory disease and active uterine bleeding. Patie ntPre paratio n Departmental protocol should determine the requirements or patient preparation. These procedures may include proper bowel preparations to ensure adequate visualization o the reproductive tract unobstructed by bowel gas or eces. Preparation may include a mild laxative, suppositories, or a cleansing enema, or some combination o these, be ore the procedure. In addition, the patient may be instructed to take a mild pain reliever be ore the examination to alleviate some o the discom ort associated with cramping. T prevent displacement o the uterus and uterine tubes, the o patient should be instructed to empty her bladder immediately be ore the examination. The procedure and possible complications should be explained to the patient, and in ormed consent must be obtained. In some instances, the physician also may per orm a manual pelvic examination be ore the radiographic procedure is begun. I available, gynecologic stirrups should be attached to the table to assist the patient in the lithotomy position. The tray contains the equipment and ancillary materials required or the procedure. An additional instrument that may be requested by the physician is a tenaculum (an instrument with a hooked clamp or gathering and holding tissues and structures in place). I gynecologic stirrups are unavailable, the patient bends her knees and places her eet at the end o the table. The patient is draped with sterile towels; with sterile technique, a vaginal speculum is inserted into the vagina. Dilation with a balloon catheter helps to occlude the cervix, preventing contrast medium rom f owing out o the uterine cavity during the injection phase. A tenaculum may be necessary to aid in insertion and xation o the cannula or catheter. When cervical placement o the cannula or catheter has been obtained, the physician may remove the speculum and place the patient in a slight T rendelenburg position. A syringe lled with contrast medium is attached to the cannula or balloon catheter. Using f uoroscopy, the physician slowly injects contrast medium into the uterine cavity. I the uterine tubes are patent (open), contrast medium f ows rom the distal ends o the tubes into the peritoneal cavity. Fluoroscopy, conventional or digital radiography, or a combination o both may be used. I f uoroscopy is unavailable, ractional injection o contrast medium is implemented, with a radiograph per ormed a ter each raction to document lling o the uterine cavity and uterine tubes and contrast medium within the peritoneum. The shape and contour o the contrast agent are assessed to detect possible pathologic processes. Because most conditions demonstrated by this procedure occur in the lumbar and cervical areas, myelography o these areas o the spine is most common. Use o shoulder rests and ankle restraints together rather than separately is advised. The oot rest is used to support the patient when the table is moved to the upright position. The number and sizes o grid cassettes used depend on the level o the spinal canal that is being examined. I the pathologic process impinges on the spinal cord, patient symptoms may include pain and numbness, o ten in the upper or lower limbs. The lesions most commonly demonstrated by myelography include herniate nucleus pulposus, which is the m ost com m on clinical in ication for m yelography; cancerous or benign tum ors; cysts; and (in the case o trauma) possible bone fragm ents. I a lesion is present, myelography identi es the extent, size, and level o the pathologic process. In the past, air or gas (radiolucent) and oil-based iodinated (radiopaque) media were used or myelography. Water-soluble contrast media provide excellent radiographic visualization o the nerve roots, are easily absorbed into the vascular system, and are excreted by the kidneys. Absorption begins approximately 30 minutes a ter injection, with good radiopacity evident up to about 1 hour a ter injection. A ter 4 to 5 hours, the contrast medium has a hazy radiographic e ect, and it is radiographically undetectable a ter 24 hours. T reduce anxiety and relax the patient, an injectable o sedative or muscle relaxant usually is administered 1 hour be ore the examination. The type and amount o premedication used are determined by the radiologist who per orms the procedure. Be ore the examination, the physician should explain the procedure and possible complications to the patient, and an in ormed consent must be signed by the patient. For example, during examination o the cervical area with the patient prone or in T rendelenburg position, the chin is hyperextended to prevent the medium rom f owing into the cranial region o the subarachnoid space. The contrast agent is injected through the spinal needle into the subarachnoid space. When the injection has been completed, the needle is removed, and images are acquired. O these two locations, the lumbar area is sa er and easier on the patient and is used most o ten or the procedure. Flexion o the spine widens the interspinous space, which acilitates introduction o the spinal needle. The radiologist may use f uoroscopy to acilitate needle placement a ter the puncture site has been selected. With the area anesthetized, the spinal needle is introduced through the skin and underlying tissues into the subarachnoid space. This movement acilitates the f ow o contrast medium to the area under examination. Images may be obtained with the use o conventional or digital technology, depending on available equipment. A ter f uoroscopy, the technologist takes conventional radiographs that are appropriate or the area under examination, as requested by the radiologist. Additional positions and projections that may be considered routine or special are included. Be ore routine radiography begins, the radiologist adjusts the table tilt as needed to concentrate the contrast medium to the level o the spinal cord that is being radiographed. I needed, a small positioning sponge or olded linen may be placed between the head and the arm to maintain alignment. The patient may rest the head on the hands, or a small positioning sponge or olded linen may be placed between the hands and the head to maintain alignment o the spine. T demonstrate best the entire spinal o canal o the thoracic region, an projections should be taken in both right an left lateral ecubitus positions, in addition to the vertical beam lateral position as described and illustrated. The radiologist, under f uoroscopic control, adjusts the angulation o the table to concentrate the contrast medium in the lumbar area. The physician manipulates the table and obtains f uoroscopic spot images as the area o interest is demonstrated by the contrast agent. The usual long bone radiograph produces signi cant magni cation and elongation because o the divergent x-ray beam. A long ruler with radiopaque markings is placed on the tabletop directly beside or under each limb. However, this procedure is more commonly per ormed in chil ren, who sometimes evelop ifferences in the length of their lim bs during periods o bone growth. This di erence is most common or the lower limbs but also can occur with the upper limbs. Orthoroentgenography is a common and accurate way to diagnose and monitor limb length discrepancies. I the condition is too severe, it can be corrected by shortening one limb or lengthening the other. Limb shortening can be done through an operation called an epiphysio esis (ep-i- z-e-od-e-sis), which results in a premature usion o the epiphysis that retards the growth o that limb. Limb lengthening also can be done surgically by cutting and lengthening the shorter limb and stabilizing it until new bone growth occurs. The method should be selected according to departmental protocol, but some re erences suggest that i the lower limb length discrepancy is greater than 1 inch (2. Ensure that ruler is placed high enough portrait so that the exposure at both ends includes calibrated reading portions o the ruler. The ruler is placed under each limb, and it is important that neither the arm nor the ruler be moved between exposures. This image allows the physician to determine limb length discrepancies and lower extremity alignment. Measurements can also be made to determine hardware requirements in cases where surgery has been indicated. Some surgical appliance manu acturers have developed so tware with the capability to overlay the prosthesis or other appliance on the image receptor itsel to acilitate surgical planning. However, conventional linear tomograms are still obtained or certain procedures such as intravenous urography (see Chapter 14). Previous editions o this textbook and physics and imagingrelated textbooks provide an in-depth description o tomography. The resulting radiograph, called a tom ogram, demonstrates a clear image o an object lying in a speci c plane, with blurring o the structures located above and below the speci c plane. T rmino lo gy e Because the tomogram represents a section o the body, this type o imaging sometimes is termed bo y section ra iography. Because terminology may di er, ollowing is a list o terms and their de nitions as used in this textbook: Blur: Area o distortion o objects outside the object plane. Exposure angle (or exposure am plitude): T otal distance the x-ray tube travels during the actual exposure. There is an inverse relationship between the exposure angle and section thickness. The level or height o the ulcrum is measured in centimeters or inches rom the tabletop. Object plane (focal plane): Plane in which the target anatomy is clear and in relative ocus. Sectional thickness: Thickness o the object or ocal plane (variable, controlled by exposure angle). Tom ographic angle (or tom ographic am plitude): T otal distance the x-ray tube travels. ImagingEquipme nt Linear tomography is accomplished when the equipment moves in one direction, and this equipment remains the most prevalent tomographic unit in imaging departments. This procedure uses a basic x-ray table, with the bucky tray and radiographic tube connected by a metal connecting arm or rod. The height o the ulcrum may be adjusted manually or electronically, depending on the type o equipment. Because the tube moves along the longitudinal axis o the table, the longitudinal tube lock must be opened (unlocked). The bucky tray and the tube angle locks must be open to permit these items to move reely. Common eatures o the control apparatus regulate the ollowing: · Exposure angle (determines object plane thickness or sectional thickness) · T ube travel speed (in inches/ sec or cm/ sec) (determines velocity tube travels) · T ube center/ preparation · Fulcrum level (determines object plane) Some units are designed so that all eatures except the ulcrum level adjustment are included on a control apparatus located in the x-ray room control area. In these units, it is common or the ulcrum level to be the adjustable type that is located directly on the ulcrum attachment connected to the x-ray table. On other units, the exposure angle selector may be located in the x-ray table area rather than in the control booth area.
Adenovirus mediated endothelial nitric oxide synthase gene transfer prevents restenosis of vein grafts erectile dysfunction 2015 discount kamagra chewable 100 mg with amex. Adenovirus-mediated gene transfer of human inducible nitric oxide synthase in porcine vein grafts inhibits intimal hyperplasia erectile dysfunction natural order kamagra chewable american express. Local delivery of gene vectors from bare-metal stents by use of a biodegradable synthetic complex inhibits in-stent restenosis in rat carotid arteries impotence lack of sleep buy kamagra chewable on line amex. Preclinical evaluation of inducible nitric oxide synthase lipoplex gene therapy for inhibition of stent-induced vascular neointimal lesion formation erectile dysfunction rates age buy discount kamagra chewable online. Local adenoviral-mediated inducible nitric oxide synthase gene transfer inhibits neointimal formation in the porcine coronary stented model erectile dysfunction doctors naples fl discount kamagra chewable 100 mg free shipping. Microsatellite polymorphism in promoter of heme oxygenase-1 gene is associated with susceptibility to coronary artery disease in type 2 diabetic patients. Correlation of antioxidants with lipid peroxidation and lipid profile in patients suffering from coronary artery disease. Adenovirus-mediated heme oxygenase-1 gene transfer inhibits the development of atherosclerosis in apolipoprotein eedeficient mice. Inhibition of graft arteriosclerosis development in rat aortas following heme oxygenase-1 gene transfer. Heme oxygenase-1 gene expression increases vascular relaxation and decreases inducible nitric oxide synthase in diabetic rats. Extracellular superoxide dismutase overexpression reduces cuff-induced arterial neointimal formation. Extracellular superoxide dismutase accelerates endothelial recovery and inhibits a in-stent restenosis in stented atherosclerotic Watanabe heritable hyperlipidemic rabbit aorta. Gene transfer of manganese superoxide dismutase reverses vascular dysfunction in the absence but not in the presence of atherosclerotic plaque. Retardation of atherosclerosis by overexpression of catalase or both Cu/Zn-superoxide dismutase and catalase in mice lacking apolipoprotein E. Adenovirus-mediated gene transfer of human platelet-activating factor-acetylhydrolase prevents injury-induced neointima formation and reduces spontaneous atherosclerosis in apolipoprotein E-deficient mice. Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. Wild-type apo A-I and apo A-I(Milano) gene transfer reduce native and transplant arteriosclerosis to a similar extent. Helper-dependent adenoviral vector-mediated long-term expression of human apolipoprotein A-I reduces atherosclerosis in apo E-deficient mice. Long-term stable expression of human apolipoprotein A-I mediated by helper-dependent adenovirus gene transfer inhibits atherosclerosis progression and remodels atherosclerotic plaques in a mouse model of familial hypercholesterolemia. Studies on protective effects of human paraoxonases 1 and 3 on atherosclerosis in apolipoprotein E knockout mice. Adenovirus mediated expression of human paraoxonase 2 protects against the development of atherosclerosis in apolipoprotein E-deficient mice. Adenovirus-mediated expression of human paraoxonase 3 protects against the progression of atherosclerosis in apolipoprotein E-deficient mice. Gene delivery of paraoxonase-1 inhibits neointimal hyperplasia after arterial balloon-injury in rabbits fed a high-fat diet. Human paraoxonase-1 overexpression inhibits atherosclerosis in a mouse model of metabolic syndrome. Overexpression of lecithin:cholesterol acyltransferase in transgenic rabbits prevents diet-induced atherosclerosis. Nuclear factor kappaB: a potential therapeutic target in atherosclerosis and thrombosis. The peroxisome proliferator-activated receptorgamma is a negative regulator of macrophage activation. Anti-monocyte chemoattractant protein-1 gene therapy inhibits restenotic changes (neointimal hyperplasia) after balloon injury in rats and monkeys. New anti-monocyte chemoattractant protein-1 gene therapy attenuates atherosclerosis in apolipoprotein E-knockout mice. Local delivery of anti-monocyte chemoattractant protein-1 by gene-eluting stents attenuates in-stent stenosis in rabbits and monkeys. Anti-monocyte chemoattractant protein-1 gene therapy limits progression and destabilization of established atherosclerosis in apolipoprotein eeknockout mice. Effect of a peroxisome proliferator-activated receptor gamma sumoylation mutant on neointimal formation after balloon injury in rats. Adeno-associated virus vector-mediated interleukin-10 gene transfer inhibits atherosclerosis in apolipoprotein E-deficient mice. Interleukin-10 overexpression in macrophages suppresses atherosclerosis in hyperlipidemic mice. Lipoprotein metabolism in the macrophage: implications for cholesterol deposition in atherosclerosis. Reduced atherosclerotic lesions in mice deficient for total or macrophage-specific expression of scavenger receptor-A. Prevention of graft coronary arteriosclerosis by antisense cdk2 kinase oligonucleotide. Inhibition of intimal hyperplasia after vein grafting by in vivo transfer of human senescent cell-derived inhibitor-1 gene. Overexpression of p53 increases lumen size and blocks neointima formation in porcine interposition vein grafts. Adenoviral delivery of a constitutively active retinoblastoma mutant inhibits neointima formation in a human explant model for vein graft disease. Gene transfer of tissue inhibitor of metalloproteinase-2 inhibits metalloproteinase activity and neointima formation in human saphenous veins. Inhibition of late vein graft neointima formation in human and porcine models by adenovirus-mediated overexpression of tissue inhibitor of metalloproteinase-3. A novel urokinase receptor-targeted inhibitor for plasmin and matrix metalloproteinases suppresses vein graft disease. Antagonism of miR-33 in mice promotes reverse cholesterol transport and regression of atherosclerosis. Short-term safety and curative effect of recombinant adenovirus carrying hepatocyte growth factor gene on ischemic cardiac disease. New approaches in advance atherosclerosis in coronary arteries based on stem cell therapy may offer novel avenues to reduce the prevalence coronary disease worldwide [2]. Until recently, the heart was considered as a solid organ with limited regenerative capacity and hypertrophy of cardiomyocytes was considered the unique adaptive mechanism in myocardial injury [3]. Careful experimental activity confuted this traditional view showing a continuous cellular turnover of cardiomyocytes [3e5]. At the same time, the capacity of extracardiac stem cells to differentiate after myocardial infarct and improve functional recovery gave birth to numerous preclinical and clinical research efforts studying the rational of cell-based cardiac therapy. Application of stem cell-based treatment in clinical cardiology could improve standards of care for many patients [6]. As indicated in experimental studies, these cells expressed cardiac-specific proteins and evaluated their ability to engraft when injected into damaged myocardium and improve myocardial performance by forming stable grafts over several weeks after implantation [7,8]. It has been shown that human-induced pluripotent stem cells can differentiate into functional cardiomyocytes and these cells may be suitable for therapeutic application [9] while preclinical studies have proved that they have the ability to differentiate into myocytes with the structural and functional properties of cardiomyocytes [10]. Stem-Cell Therapy 321 into specialized cells and repair the tissue in which they are found. In human heart, these stem cells are intrinsically programmed to generate cardiac tissue [11]. The latter two are markers of primitive stem cells, whereas linþ cells are committed to a particular lineage. Their multipotentiality allows them to differentiate along the three main cardiac lineages: myocytes, endothelial cells, and smooth muscle cells [14]. After their injection in the ischemic heart, the formation of the above-mentioned cell types contributes to the regeneration of myocardium and the improvement of its contractility [17]. They are a subset of the total mononuclear cell population that possesses an enhanced potential for differentiation within the endothelial-cell lineage [18]. They have been shown to predict independently the progression of coronary artery disease and death from cardiovascular causes and might, therefore, be a useful tool for risk stratification [19]. However, these observations must be interpreted with caution and further clinical investigations are needed. Preclinical data from a variety of experimental studies have demonstrated the capacity for myoblasts to engraft and form striated myotubules, after their intramural implantation or arterial delivery. Subsequently, they enhance the function of the damaged myocardium after transplantation into infarcted myocardium [24,25]. Lately, preliminary human studies focusing on patients with ischemic heart disease indicate successful myoblast transplantation into the scar of the infarcted myocardium [26,27]. However, skeletal myoblasts fail to build classic cell-to-cell connections with cardiomyocytes [28] and they have arrhythmiogenic potential, which has been reported in several trials [26]. Similarly, administration of mesenchymal stem cells onto scarred myocardium repaired cardiac performance to nearly normal level [36,37]. Furthermore, the number of cells that can be obtained from an individual is quite small; however, these cells can be expanded in culture [38]. Thus, it is 324 Coronary Artery Disease feasible that cells isolated from very small fragments of human myocardium and expanded many-fold in vitro could reach numbers appropriate for in vivo transplantation while retaining their differentiation potential [41]. Moreover, compared to the other adult stem cells in the heart, they appear to be in the most primitive stage of differentiation. Experimental models of myocardial infarction have demonstrated a reduction in the cell death rate, induction of endogenous repair mechanisms, and the contribution of new cells to the injured myocardium, resulting in satisfactory improvement of myocardial remodeling [42]. However, the absolute number of newly differentiated cardiomyocytes was low and most likely insufficient to make substantial direct contributions to left ventricular structure and function [43]. The results from large clinical trials albeit the good safety profiles have demonstrated divergent findings in cardiac function in patients with myocardial infarction [49e55]. Different methods have been employed to deliver stem cells to the damaged myocardium. The most frequent are intracoronary and intramyocardial approaches with diverse advantages and disadvantages for each one (Table 3. Most of the studies have used intracoronary delivery as preferred administration route [49]. Cells are delivered over the lumen of an inflated over the wire balloon catheter placed in the reopened coronary artery after percutaneous coronary intervention [56]. The direct delivery to the infarcted myocardium and the relatively low invasiveness are the main advantages. Direct intramyocardial injection of cells has also been used, especially in models of chronic ischaemic cardiomyopathy, and facilitates cell delivery despite the potential arrhythmiogenic effects, and the need for concomitant open heart surgery [57]. Most of the studies have resulted in beneficial outcomes for the cardiac function. Furthermore, this improvement was coupled with a concomitant decrease in infarct size and an increase in the left ventricle viable mass, implying the robust regeneration of myocardial tissue. Despite the favorable results observed in some individuals treated with stem cells, certain clinical expectations were not achieved because the levels of improvement in cardiac tissue structure or functionality were less than those previously observed in experimental trials [66]. Beyond these landmark studies, there are more than 20 smaller trials in the field of stem Stem-Cell Therapy 329 cell transplantation currently published. Albeit several challenges, such as optimization of the therapeutic protocols and technological improvement of stem cell delivery devices, it is believed that the current ongoing studies will accelerate the further development and acceptance of stem cell therapy and the optimal selection of stem cell type. Clinical trials have shown only a modest or negligible improvement of cardiac function [39]. First, the rather small number and the selection of patients, and their preparation have to be considered. Second, factors related to the cell administration, such as the injection of an insufficient number of cells, the biodistribution of injected cells, the use of wrong cell type, the extent of cellular differentiation of these cells within the target area, the use of an inappropriate delivery method, or possible inappropriate timing relative to the age of the infarct [67]. Despite all efforts, the specific cell types conferring therapeutic effects have not been yet defined [68,69]. Intense debate is focused on definition of specific markers of endothelial and other vascular progenitor cells. Moreover, differences between animal models and humans, including the absence of comorbidities in the animal model, should be considered [39]. Last, results of chronic postinfraction studies are less supportive for stem cell therapy than acute myocardial infarction studies. Compared to chronic disease, several trials in acute phase of myocardial infarction found that cell treatment significantly improved left ventricular function [71]. Damaged myocardium can regenerate from the stem cells that enter the cell cycle, contributing to changes in the myocardial mass. Early animal studies reported very promising results for stem cell therapy, with robust remasculinization. However, despite intensive research, the principal mechanisms have not yet been fully elucidated. Moreover, there is an ongoing debate in the field of basic stem cell research as to which cell type is more suitable. This lack of knowledge translates into the currently available clinical trials, which were only partially able to reproduce the groundbreaking findings from animal studies. There is a need to put even more efforts in order to clarify the principal regenerative properties of different stem cells and to develop promising approaches for their clinical application. It is important to emphasize in specific patient-related factors that may have an impact on cell therapy outcomes, such as severity of atherosclerosis or cardiovascular risk factors. Although cell therapy holds therapeutic promise for clinical applicability, further clinical trials powered to detect differences in mortality and to identify the most beneficial approaches are warranted in order conclude whether stem cell transplantation will eventually join the standard therapeutic armamentarium and improve both the mortality rate and quality of life. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Genetically selected cardiomyocytes from differentiating embronic stem cells form stable intracardiac grafts.
References
- Patel, H.R., Ribal, M.J., Arya, M., Nauth-Misir, R., Joseph, J.V. Is it worth revisiting laparoscopic three-dimensional visualization? A validated assessment. Urology 2007;70:47-49.
- Review. Mosmann TR, Moore KW. The role of IL-10 in cross-regulation of TH1 and TH2 responses. Immunol Today. 1991;12:A49-ASeder RA, Gazzinelli R, Sher A, et al. Interleukin 12 acts directly on CD4 T cells to enhance priming for interferon gamma production and diminishes interleukin 4 inhibition of such priming. Proc Natl Acad Sci U S A. 1993;90:10188-1Farrar JJ, Benjamin WR, Hilfiker ML, et al. The biochemistry, biology, and role of interleukin 2 in the induction of cytotoxic T cell and antibody-forming B cell responses. Immunol Rev. 1982;63:129-166.
- Sergeant N, Buee L. TAU models. In Animal Models of Dementia, eds. P.P. De Deyn, D. Van Dam. Springer Science + Business Media, New York, 2010; pp. 449-468.
- Marks LS, Gittelman MC, Hill LA, et al: Rapid efficacy of the highly selective a1A-adrenoceptor antagonist silodosin in men with signs and symptoms of benign prostatic hyperplasia: pooled results of 2 phase 3 studies, J Urol 181:2634n2640, 2009. Marks LS, Gittelman MC, Hill LA, et al: Silodosin in the treatment of the signs and symptoms of benign prostatic hyperplasia: a 9-month, open-label extension study, Urology 6:1318n1322, 2009. Marschall-Kehrel D, Feustel C, Persson de Geeter C, et al: Treatment with propiverine in children suffering from nonneurogenic overactive bladder and urinary incontinence: results of a randomized placebo-controlled phase 3 clinical trial, Eur Urol 55(3):729n736, 2009.
- Kawasaki K, Kohno M, Inenaga C, et al. Chordoid glioma of the third ventricle: a report of two cases, one with ultrastructural findings. Neuropathology 2009; 29:85-90.