
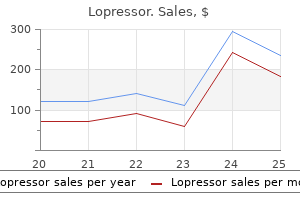
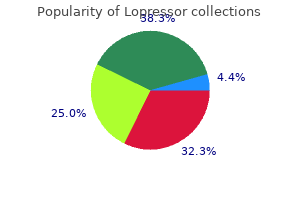
Lopressor
| Contato
Página Inicial
Peter Faulhaber, MD, MA
- Associate Professor of Radiology
- Case Medical Center
- Case Western Reserve University
- Director
- Clinical PET
- University Hospitals Case Medical Center
- Cleveland, Ohio
Although the basal ganglia continue to be among the least understood of all brain structures heart attack the song buy lopressor from india, their mysteries are now yielding to modem neurobiological techniques for elucidating neurochemistry and connections pulse pressure 99 lopressor 25 mg purchase without a prescription. For example arteria thoracoacromialis purchase 12.5 mg lopressor visa, the basal ganglia contain virtually all of the major neuroactive agents that have been discovered in the central nervous system blood pressure chart diastolic high safe lopressor 50 mg. Although the reason for this biochemical diversity remains elusive hypertension 38 weeks pregnant purchase 12.5 mg lopressor with amex, such knowledge can be used to treat some fonns of basal ganglia disease. Indeed, the discovery that the brains of patients with Chapter 14 · the Basal Ganglia 305 Parkinson disease are deficient in dopamine quickly led to the development of drug replacement therapy. Knowledge about connections of the basal ganglia with the rest of the brain has led to a major revision of the traditional views of basal ganglia organization and function. Discoveries about basal ganglia circuitry and pathways have even led to therapeutic neurosurgical and neurophysiological procedures. This is a form of electrical neuromodulation that can be used to improve many of the disabling signs of basal ganglia disease. This article first considers the constituents of the basal ganglia and their three-dimensional shapes, partly from a developmental context. Next, their functional organization is surveyed, emphasizing the distinctive roles of the basal ganglia in movement control, cognition, and emotions. Organization and Development of the Basal Ganglia Separate Components of the Basal Ganglia Process Incoming Information and Mediate the Output the many components of the basal ganglia are best learned, in a general way, from the outset; then their functional and clinical anatomy can be mastered. The components of the basal ganglia can be divided into three categories: input, output, and intrinsic nuclei (Table 14-1). The input nuclei receive afferent connections from brain regions other than the basal ganglia, in particular the cerebral cortex, and in turn project to the intrinsic and output nuclei. The functions of the striatum do not correspond precisely to its component anatomical parts. Most of the caudate nucleus participates in cognition and eye movement control, whereas the putam. Emotions are mediated by the nucleus accumbens, together with adjoining ventromedial parts of the caudate nucleus and putamen; the emotional striatum is commonly termed the ventral striatum. Given that the striatum is really a composite of three nuclei, it is not surprising that it has a complex shape and diverse functions. The output nuclei project to regions of the diencephalon and brain stem that are not part of the basal ganglia. As we will learn later, the external segment of the globus pallidus, the subthalamic nucleus and the substantia nigra pars compacta are involved in diverse motor, cognitive and emotional functions, whereas the ventral pallidum and ventral tegmental area are primarily involved in emotions. The Complex Shapes and Fractionation of Basal Ganglia Components Are Understood by How the Basal Ganglia Develop Learning the numerous components and subdivisions of the basal ganglia is a challenge. Taking a developmental perspective helps to understand two key features of the anatomy of the basal ganglia: the complex three-dimensional shape and fractionation of the components of the basal ganglia into subdivisions. The caudate nucleus develops a C-shape, largely as a consequence of cerebral cortex development. This expansion and change in shape are produced by the birth and migration of cells along predetermined axes. This imparts a distinctive shape of the caudate nucleus in relation to the shapes of the other two striatal components. The reason for learning these components is that the head is a robust anatomical landmark, bulging into the lateral ventricle. A second developmental process contributes to formation of some of the basal ganglia subdivisions. Nuclei of the basal ganglia are shown in relation to the thalamus and intemal capsule. The tail ofthe caudate nucleus is separated from the putamen by additional projection fibers. In addition to being part of the same structure but separated by the internal capsule. Schematic diagrams of the cerebral hemisphere, lateral ventrlde, and strlatum accompany each age. The nudeus aCaJmbens Is located ventromedlally primarily on the medial strlatal surface. Drawing of coronal sllce tttrough the posterior llmb of the lntemal capsule showing path of a descending cortlul axon. However, many neurons in the ventral pallidum have connections and a neurochemistry similar to the globus pallidu. Functional Anatomy of the Basal Ganglia Direct and Indirect Pathways Form Common Circuits Throughout All Functional Divisions of the Basal Ganglia Whereas the basal ganglia have a daunting complexity, there is a logic to the connections that helps explain their overall actions. From the str1atum, the direct path mrgets the output nuclei (bottom), whidl, in tum, project to the thalamus (right) and then back to the mrtex. In addition to the direct loop beck to the cerebral mrtex, output nuclei also project to brain stem nuclei. The shading over the Input and output nuclel represent structures within the basal ganglia. It Is Important to note that whereas the basal ganglia receive Input from all areas of cortex It projects back only to the frontal lobe. These differential projections confer the distinctive functions of the basal ganglia (discussed below). The external segment of the globus pallidus and the subthalamic nucleus are part of a basal ganglia circuit that receives input from other basal ganglia nuclei and in turn projects back. Information that is processed by these intrinsic nuclei use the indirect path to the thalamus. Connections of both the direct and indirect paths with the brain stem target primarily motor control centers that are important in gait control and for saccadic eye movements. There are many different dopamine receptor subtypes, and, depending on the particular subtypes present on the postsynaptic neuron, dopamine either depolarizes or hyperpolarizes striatal neurons. The output nuclei are the globus pallldus Internal segment, the substantla nlgra pars retlculata, and part of the ventral pallldum. Whereas the basal ganglia receive input from all cortical areas, the return path from the thalamus ls directed only to the frontal lobe. Note, dopamlnerglc cell groups innervate both the cerebral cortex and the striatum. The neurotransmitters of the basal ganglia are shown In relaUon to the organlzaUon of basal gang Ila circuits. By contrast, when the balance shifts more to indirect path functions, debilitating akinesia, bradykinesia, and rigidity can occur. Clinical and experimental evidence suggest that similar differential actions of the direct and indirect paths also influence the non. We consider below how the differential actions of the direct and indirect paths occur, in the context of the diversity of neurotransmitter actions in the basal ganglia. The excitatory neurotransmitter glutamate is used by corticostriatal neurons (the major input to the basal ganglia), thalamic neurons that project to the cerebral cortex, and the projection neurons of the subthalamic nucleus. The axons of these neurons project to the two segments of the globus pallidus, the ventral pallidum, and the substantia nigra pars reticulata. Medium spiny neurons also contain neuropeptides, and a distinct neuropeptide is present in neurons marking the direct (enkephalin) and indirect (substance P) paths. Thus, the output of the basal ganglia, similar to that of the cerebellar cortex, is inhibitory. Neurons in the substantia nigra pars compacta and the ventral tegmental area contain dopamine. The activity and function of the postsynaptic targets of these nuclei, the striatum and portions of the frontal lobe, are under important regulation by dopamine. Acetykholine is another common neurotransmitter in the basal ganglia; it is present in striatal interneurons. Striatal cholinergic interneurons play an important role in regulating diverse basal ganglia functions, including plasticity. Parkinson Disease is aHypokinetic Movement Disorder In Parkinson disease, movement becomes impoverished. As discussed earlier, the direct path promotes movements, and the indirect path inhibits movements. Projection neurons ofthe putamen in the direct path synapse on neurons in the internal segment of the globus pal lid us, which project to the ventrolatera I and ventral anterior nuclei of the thalamus. However, because the output of the internal segment ofthe globus pallid us is also inhibitory, the amount of inhibition of the thalamus from the internal segment of the globus pallidus is reduced. Inhibition of an inhibitory signal is termed disinhibition; functionally, this double negative is equivalent to excitation. The thalamic response shown is transiently released from inhibition and fires a burst of action potentials; hence, accelerating thalamocortical activity. In a motor behavior such as reaching for a glass of water, neurons in premotor areas, as well as corticospinal tract neurons in primary motor cortex, are thought to be excited by the actions of the direct path. The indirect path has the opposite effect on the thalamus and cerebral cortex as the direct path. Because the output ofthe external segment ofthe globus pallidus is inhibitory, indirect path neurons of the putamen disinhibit the subthalamic nucleus, resulting in a burst of action potentials. This period of disinhibition will, in turn, excite the internal segment of the globus pallidus and substantia nigra pars reticulata (which are both inhibitory) and thereby increase the strength of the inhibitory output signal directed to the thalamus. Increased striatal dopamine enhances the excitatory effects of the direct path on cortical motor areas and diminishes the inhibitory effects of the indirect path. Because of these different actions on striatal neurons, the combined effect of dopamine on both paths is to reduce the inhibitory output of the basal ganglia, thereby reducing inhibition of the thalamus. The power of this model is that it helps to explain the mechanisms of some hypokinetic and hyperkinetic signs seen in basal ganglia disease. Together these effects would drastically reduce the thalamic signals to the cortex. For the premotor and motor cortical areas, this would reduce cortical outflow along the corticospinal and corticobulbar tracts and reduce production of motor behaviors ie, hypokinesia). This reduces basal ganglia inhibitory outflow and triggers greater thalamic outflow to the cortex. This nucleus normally exerts an excitatory action on the internal segment of the globus pallidus. When the subthalamic nucleus becomes lesioned, the internal segment of the globus pallidus would be expected to inhibit the thalamus less (thin dashed line), thereby increasing outflow to the cerebral cortex. The model does not predict the pattern of the complex hyperkinetic responses; like why there are flailing ballistic movements with hemiballism or chorea in Huntington disease. In addition, patients exhibit a resting tremor, and when an examiner moves their limbs, a characteristic stiffness or rigidity can be noted. This name derives from the presence ofthe black pigment neoromelanin, a polymer of the catecholamine precursor dihydroxy-phenylalanine (or dopa), which is contained in the neurons of the pars compacta. Not surprisingly, neuromelanin is not present in the substantia nigra pars compacta of people who die from the effects of Parkinson disease. Dopaminergic neurons in other parts of the central nervous system are also destroyed in Parkinson disease. Dopamine loss in the basal ganglia, however, apparently produces the most debilitating neurological sjgns. Riied neuronal cell bodies and terminals Indicate Inhibitory actions, and open cell bodies Indicate excitatory actions. Neural activity for each circuit can be followed, beginning with a phasic excitatory input from the cortex and the rei;ulting phasic chilnge in the thalamus. The thickness of the llnes lndlartes relatlve changes In the number of neurons and strength of connections brought about as a consequence of disease. Thicker means stronger connections and mere activity; thinner means fewer and weaker connections. These paths follow only tonic dlanges in neural actiViltion, because phasic changes are not well dlaracterized. The diffuse tan areas highlight the anatomical components located within the basal ganglia. They discovered that a certain kind of synthetic heroin produces a permanent clinical syndrome in humans that is remarkably similar to Parkinson disease. Involuntary distal limb movements, such as writhing of the hand, or athetolia, may also occur. This is translated into huntingtin having an excessively long 314 Section Ill · Motor Systems polyglutamine repeat. This mutation, which is present in all cells of the body but apparently affecting primarily medium spiny neuron function, making them particularly vulnerable to cell death. This mutation also leads to the dysfunction and death of neurons in other brain regions, including the cortex. Interestingly, several other neurodegenerative diseases are associated with a polyglutamine repeat mutation. Another hyperkinetic disorder is hemiballism (see the clinical case in this chapter). This remarkable clinical disturbance occurs after damage to the subthalamic nucleus, an intrinsic basal ganglia nucleus. Hemiballism causes patients to make uncontrollable, rapid ballistic (or flinging) movements of the contralateral limbs. These movements are produced by motion at proximal limb joints, such as the shoulder and elbow. Functionally Distinct Parallel Circuits Course Through the Basal Ganglia As introduced earlier, an important aspect of basal ganglia circuitry is the parallel anatomical loop organization, with distinct loops serving different functions.
Immediately after crossing the midline arteria frontalis- 12.5 mg lopressor for sale, the fibers ascend to the thalamus in the medial lemniscus arrhythmia high blood pressure discount 25 mg lopressor fast delivery. Axons from the gracile nucleus decussate ventral to axons from the cuneate nucleus and ascend in the ventral part ofthe medial lemniscus blood pressure medication usa purchase generic lopressor canada, compared with axons from the cuneate nucleus hypertension definition 12.5 mg lopressor visa. Because of this pattern blood pressure medication manufacturers order lopressor paypal, the somatotopic organization of the medial lemniscus in the medulla resembles a person standing upright. Axons in the medial lemniscus ascend uninterrupted through the brain stem and synapse in the thalamus. Vertebral artery infarction produces mechanosensory deficits on the contralateral side of the body. This type of infarction also destroys axons of the corticospinal tract in the pyramid, producing a movement impairment (see Chapter 10). Four levels through the splnal cord are shown, rostrocaudally from top to bottcm: a section rostral to the cervlcal enlargement, a section through the cervlcal enlargement. Aschematic slice through the postcentral gyrus, showing the somatotoplc organlutlon of the primary somatfc sensory cortex. The territory receiving Input from the ventral posterior lateral nucleus Is shaded darkef than the tefrltory receiving Input from the ventral posterior medial nudeus. The ventral posterior nucleus is important in discriminative aspects of the mechanical sensations, su. The shape of the thalamus and brain stem can be discerned, but not the component nuclei. This thalamocortical projection forms the basis of a body map on the postcentral gyrus, the sensory homunculus, originally described in the human by the Canadian neurosurgeon Wilder Penfi. Local circuit cormections, both excitatory and inhibitory, use this information to construct the representations of the various body parts on the sensory map. Rather, the portions of the body used in common discriminative tactile tasks, such as the fingers, have a disproportionately greater representation on the map than ai:eas that are not as important for touch, such as the elbow. It was once thought that these differences were fixed, established genetically to determine the discriminative capacity of different body parts. We now know that the body map of the brain is not static but is also dynamically controlled by the pattern of use of different body parts in touch exploration. Most of the excitatory connections within a local area of cortex remain somewhat confined to a vertical slice of cortex. For example, in the primary auditory cortex, neurons within a column are sensitive to the same frequency of sound, and in the motor cortex, neurons in a column participate in controlling movement of the same joint, or sets of joints. As discussed in Chapter 2, pyramidal neurons in different layers project to different targets. One function of these callosal connections may be to join the representations of each half of the body in the primary somatic sensory cortex of each hemisphere. A8 in other cortical areas, regions of the primary somatic sensory cortex with a different cytoarchitecture have different functions. Area 3a processes information from mechanoreceptors located in deep structures, such as the muscles and joints, and plays an important role in limb position sense. Areas 3b and 1 process information from mechanoreceptors of the skin, and are important in texture discrimination. Area 2 receives information from both deep structures and the skin and is important in discrimination of the shape of grasped objects. Higher-Order Somatic Sensory Cortical Areas Are Located in the Parietal Lobe, Parietal Opert11lum, and Insular Cortex Projections from the primary sensory cortical area distribute the information to multiple cortical regions, although these other areas may also receive direct thalamic inputs. Although sequential pathways from one region to the next can be identified, the primary and higher-order sensory areas are also extensively interconnected and the operations of any one set ofconnections are dependent on the operations of others. The higher-order sensory areas typically project to cortical regions that receive inputs from the multiple sensory modalities and are termed association areas. One such multimodal convergent zone is the large expanse of cortex at the junction of the parietal, temporal, and occipital lobes. There are three major projection streams for processing mechanosensation from primary somatic sensory cortex: ventral, for recognizing manipulated objects; dorsal (and posterior), for localization of objects and body spatial awareness; and rostral, for movement control the ventral and dorsal projections comprise the "what" and "where" pathways, respectively. Similar to the primary area, the secondary somatic sensory cortex is somatotopically organized. The llght green region corresponds to the areas beneath tile surface, In the Insular cortex and the parietal and temporal operculum. Aschematic sectfon cut perpendicular to the medlolateral axis of tile postcentral gyrus. In addition to the awareness of object location, the projection to the posterior parietal cortex plays two other major functions. A lesion of this region in the nondominant hemisphere (typically the right hemisphere) produces a complex syndrome termed sensory neglect in which the individual neglects the contralateral half of the body. For example, a patient may fail to dress one side of her body or comb half of her hair. Second, portions of the posterior parietal cortex receive visual and auditory inputs as well as somatic sensory information. These areu are involved in integrating somatic sensory, visual, and auditory information for perception and attention. The "where" pathway, together with the rostral projection, targets the motor areu of the frontal lobe, especially the motor cortex. This projection is important for using mechanoreceptive sensory information to guide reaclllng movements and for object manipulation by the hands. The muscle spin& is the key receptor for muscle length and the Golgi tendon organ. They receive somatic sensory information and transmit it from the periphery to the spinal cord. Neurons sensitive to root ganglion neurons enter the spinal cord via the dorsal root. The afferent information carried by adjacent dorsal roots overlaps nearly completely on the body surface. The gracile fascicle is a tract that carries axons from the leg and lower trunk, and the cuneate fascicle carries axons from the upper trunk, arm, neck, and back of the head. The majority of the axons in the dorsal columns are central branches of dorsal root ganglion neurons. Efferent projections from the somatic sensory cortical areas arise from neurons whose cell bodies are from specific cortical layers. Cortical connections of the somatosensory fields of the lateral sulcus of macaques: evidence for a corticolimbic pathway for touch. A brief taxonomy of tactile illusions and demonstrations that can be done in a hardware store. Projection pattern of functional components of thalamic ventrobasal complex on monkey somatosensory cortex. Cutaneous excitatory and inhibitory input to neurones of the postsynaptic dorsal column system in the cat. A 25-year-old man was in an automobile accident and suffered a severe spinal cord injury. Focusing only on mechanosensation, he had no sense of touch on his right leg and lower trunk, to the level of the umbilicus. From which of the listed body regions does the gracile nucleus receive mechanoreceptive inputf A. The medial lemniscus-in the medulla, at the level where there is a fourth ventricle-receives its blood supply from which of the following arteries Branches of the middle cerebral artery Branches of the anterior cerebral artery Branches of the posterior cerebral artery Branches of the basilar cerebral artery B. Which of the following statements best describes the organization of dermatomes associated with adjacent dorsal roots Dermatomes are adjacent, with minimal overlap, so that loss of one dorsal root gives rise to a loss of somatic sensation within the dermatome boundary, as shown in the dermatome maps. Dermatomes overlap partially, but loss of one dorsal root does not give rise to a noticeable loss of sensation. Dermatomes overlap partially, so that loss of one dorsal root typically gives rise to a noticeable loss of sensation within the dermatomal boundaries. Complete the following analogy: the face area of the primary somatic sensory cortex is to the leg area, as A. Dermatomes overlap nearly completely, so that loss of one dorsal root typically does not give rise to a noticeable loss of sensation. This is followed by tingling on her right back, then right palm, fingers, and finally the right side of the face. Which of the following best describes the locations in the brain of the start and end of the seizure Start: left ventral posterior medial nucleus; end: left ventral posterior lateral nucleus D. Start: left ventral posterior lateral nucleus; end: left ventral posterior medial nucleus. The patient reported, at the time, that as the cigarette he was holding burned down, he noticed that his right Index and middle fingers had sustained a burn, although he felt no pain. He reported that he noticed no other sensory, especially touch, or motor problems at that time. Over the next year, he began experiencing reduced right-hand grip strength In addition to the sensory loss. At this time, upper extremity tactile sensation and limb proprioception were now affected. Answer the following questions based on your reading of this chapter and prior chapters, inspection ofthe images, and consideration of the neurological signs. Distinguish the neural systems that mediate pain and temperature sensations from touch and proprioception. Identify the anatomfcal location of the accumulated fluid that Is producing the hyperlntense signal. What are the key differences In the location of axons of the pain and temperature pathway and the touch/ proprioception pathway and how does their locations explain the neurological signs Explain why the patient initially experienced only a loss of pain sensation but later experienced a loss of strength and touch7 Box 5-1. The classical distribution of pain and temperature loss in cervical syringomyelia is across the arms bilaterally. Importantly, the syrinx Is large enough also to damage motor neurons, producing hand weakness (Agure S-1C; lighter region corresponds to the enlarged syrinx). The cavity would have been fluid-filled during life, showing more clearly the damage produced by the syrlnx. Clinical casa: 4 t -yHr-old man with bums an flnger tlpsand bllahlral uppar utnimlty analgnll. Splnal cord cross section showing the patterns of terminations of small-and large-diameter axons and how the components of the anterolateral system dewssate and ascend. The darker-tinted region Is affected by the formation of a syrlnx when the patient first noticed the sensory Impairment. The lighter, enlarged, region corresponds to the syrinx when weakness was noticed. The central darkened region corresponds to the size of the syrinx when the patient first noticed pain loss, without additional neurological signs. One year later, because of Its enlarged size, the syrlnx extends Into the dorsal columns, uli that evoke these sensations are good predictors of tissue harm and body homeostasis. We sense the itch of a mosquito bite and quickly swat at it to prevent further biting. Pain and itch of a more persistent or recurring P ain, temperature, and itch are our protective senses. Stim- nature typically brings a patient to visit a physician, who will use this lnfonnation diagnostically. These sensory receptor neurons have specific connections with central nervous system structures that, when they become active, orchestrate a complex set of physiological and behavioral events. The evoked perceptions allow us to recogniu precisely stimulus modality and where on our body it occurred. The emotions produced by the protective senses help us identify the context in which the stimuli were received, the negative valance of abdominal pain after eating tainted food or the positive side of a cool tropical breeu. The protective senses mobilize our actions, to help ensure removal of the stimulus, to prevent bodily harm. Not surprisingly, the pain, temperature, and itch systems connect directly with diverse brain regions, much more so than for touch. Unique to our protective senses is that they engage areas of the cerebral cortex that are more lmown for their involvement in emotion than sensation. Unfortunately, our protective senses can be easily fooled; they can be activated into a persistent state of false alarm under pathological conditions. In this article, we will examine the neural systems for pain, temperature, and itch. However, as we learn more about temperature sense and itch, it appears that all three protective senses engage similar spinal cord and brain circuits. We first examine the systems in overview and then consider the different levels of sensory processing, from the periphery to the cerebral cortex. Surgical destruction of the anterolateral system spares touch and limb position senses but renders people insensitive or less sensitive to pain. Termed an anterolateral cordotomy, this procedure was commonly used to treat intractable pain before effective analgesics became available. The anterolateral system also mediates a residual, or crude, sense of touch after damage to the dorsal column-medial lemniscal system.
Increased numbers of basophils blood pressure exercise cheap lopressor 100 mg with mastercard, eosinophils blood pressure 0f 165 buy lopressor 50 mg with visa, and immature myeloid cells are observed blood pressure eyes purchase lopressor 50 mg otc. Platelet counts are usually less than 1000 × 109/litre pulse pressure quizlet effective 25 mg lopressor, but higher counts may be seen heart attack instrumental cheap lopressor 12.5 mg buy. The progression to polycythaemia vera-related myelofibrosis is characterized by the appearance of a leucoerythroblastic blood picture with the presence in the peripheral blood of teardrop red cells (dacrocytes), immature myeloid cells, megathrombocytes, and nucleated red blood cells. Bleeding time and platelet aggregation studies are frequently, but not always, abnormal. Prolongation of prothrombin and partial thromboplastin times are frequently encountered, usually reflecting a laboratory artefact due to erythrocytosis (the volume of plasma in the collection tube might be too small relative to the amount of citrate anticoagulant present in these tubes). Low levels persist in two-thirds of patients after normalization of the haematocrit. Elevations in leucocyte alkaline phosphatase (70%), serum vitamin B12 levels (40%), and serum vitamin B12 binding proteins (70%) are common, as are hyperuricaemia and increased histamine levels. Bone marrow examination reveals a hypercellular marrow with trilineage growth (panmyelosis) with prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes. Reticulin is often seen, but is not predictive of evolution into the myelofibrotic phase. Cytogenetic abnormalities have been observed in 25% of patients, but none is characteristic. A recent study using fluorescence in situ hybridization analyses has shown that abnormalities involving chromosome 9 rearrangements are common, being present in up to 53% of patients with polycythaemia vera. Other chromosomal abnormalities involving chromosomes 1, 5, 7, 8, 12, and 13 have been associated with disease progression. Approach to the patient with polycythaemia It is wise to avoid the temptation of diagnosing polycythaemia on the basis of a single blood count unless extremely high haematocrit levels are observed. Heavy smokers with mild polycythaemia should be asked to stop smoking and their counts repeated after a few weeks. Once a genuine elevation of haemoglobin or haematocrit has been established, the next step is to decide whether this represents an absolute increase in total red cell mass, or merely a relative phenomenon. A blood volume study with direct quantitation of both red cell mass and plasma volume can be helpful in making this distinction if available. In patients with extreme degrees of erythrocytosis (haematocrit >55% in men and >49. If absolute polycythaemia is confirmed, it is essential to elucidate whether it is the consequence of a primary myeloproliferative disorder such as polycythaemia vera or a secondary condition. The presence of leucocytosis, thrombocytosis, or splenomegaly is suggestive of polycythaemia vera as the cause for the elevated red cell mass. Arterial blood gases and the direct determination of oxygen saturation in arterial blood, if decreased, may aid in the recognition of a chronic pulmonary or congenital cardiovascular abnormality. Otherwise, causes for a physiologically inappropriate polycythaemia should be sought. There is a small but definite group of patients in whom a specific cause for polycythaemia remains elusive, despite appropriate diagnostic testing. Regular, continued surveillance is recommended for all noncategorized patients, as some of them develop polycythaemia vera in the future. Management of polycythaemia vera the two main goals in the management of patients with polycythaemia vera involve the confirmation of the diagnosis and reduction of the red cell mass. The untoward effects of an increased red cell mass on tissue blood flow occur independently from the specific cause of the polycythaemia. It is thus reasonable to recommend that all patients with uncorrectable erythrocytosis be offered phlebotomy. The main therapeutic goals are the maintenance of well-being and the prevention of complications for as long as possible. Several therapeutic strategies have resulted in dramatic increases in the survival of patients. Historical evidence suggests a median survival of approximately 18 months in untreated patients with polycythaemia vera whereas with appropriate management, survival of over 10 years is now common. The main therapeutic objective is the reduction of the haematocrit to a normal level. Every possible effort should be made to discourage patients with polycythaemia vera from smoking. A regimen of phlebotomies should be prescribed as soon as the diagnosis has been clearly established. It is often feasible to remove between 350 and 500ml of blood every other day until the desired haematocrit level is attained. Many haematologists still target 42% for women, though this is not based on prospective data. Once the target haematocrit level is achieved, a maintenance regimen should be instituted. Venesection is preferred in those younger individuals without critical elevations in their platelet counts. Myelosuppressive therapy should be considered in elderly patients who are intolerant of phlebotomies, and in younger individuals with repeated thrombotic episodes and extremely high platelet counts. There is controversy regarding what represents the optimal myelosuppressive agent. A major concern has been the possible association between exposure to some of these agents and the development of leukaemia. Hydroxycarbamide is useful for the management of patients with polycythaemia vera and represents the first-line therapy especially in older patients in whom phlebotomy alone is insufficient or intolerable, due to its minimal leukaemogenic potential. It should, however, be used with great caution in patients formerly treated with radioactive 32P or alkylating agents as the risk of leukaemia is higher. Low-dose aspirin (81100mg/day) administered to patients with polycythaemia vera has been shown to decrease the risk of arterial and venous events. Although there is no overall survival benefit, no significant increased risk of bleeding was reported. In younger patients, given their potential long-term survival, strong consideration should be given to the use of phlebotomy therapy in combination with low-dose aspirin, as well as with other apparently nonleukaemogenic interventions such as interferon- and anagrelide. In two recent studies, one in polycythaemia vera patients and another in essential thrombocythaemia patients, hydroxyurea has been shown to be nonleukaemogenic, and can be used as an alternative to phlebotomy or in combination with it. Interferon-2a and pegylated forms of interferon have been shown to be effective in controlling the blood counts and symptoms (especially pruritus). In patients with a history of thrombosis where uncontrolled thrombocytosis is a problem, anagrelide, an inhibitor of megakaryocytic maturation, has proven effective. Best available therapy included therapeutic phlebotomy as well as various pharmacological interventions including hydroxycarbamide at tolerable doses, interferon-, immunomodulators, and anagrelide. It is unclear what impact ruxolitinib will have on thrombotic risk and transformation to myelofibrosis or acute leukaemia, which should become clearer with long-term follow-up and populationbased studies. Refractory aquagenic pruritus can be managed in the majority of cases with ruxolitinib. At present, oral melphalan should be used only in patients who are incapable of complying with the other forms of therapy or are unwilling or unable to return for follow-up. Elective surgery should only be undertaken after adequate and sustained control of the blood counts has been achieved. When emergency surgery is required, the patient should be phlebotomized rapidly until a normal haematocrit is achieved, and platelets should be available in case excessive operative bleeding occurs. Patients should be mobilized promptly, and the use of prophylactic doses of low molecular weight heparin should be considered unless contraindicated. Dental extractions are associated with an increased bleeding risk and should only be pursued in patients with good haematological control. A particularly high-risk intervention is splenectomy, which has an operative mortality rate of approximately 9%. The haematocrit should be normalized and platelet count maintained below 400 × 109/litre before splenectomy. Although no prospective studies have been done, prophylactic low molecular weight heparin is probably warranted in all patients undergoing splenectomy during the perioperative period. Due to the high probability of expanding extramedullary haematopoiesis with rapid development of liver enlargement after splenectomy, patients should receive hydroxycarbamide therapy postoperatively. In patients with polycythaemia-related myelofibrosis, the management is quite similar to that for primary myelofibrosis. Allogeneic stem cell transplantation is now a curative option for patients with myelofibrosis, both primary and secondary to other myeloproliferative neoplasms, and should be considered in appropriately selected patients. Pregnant patients with polycythaemia vera experience an increased incidence of fetal loss, with 30% of pregnancies culminating in spontaneous abortions. Unexpectedly, pregnancy in patients with polycythaemia vera is frequently associated with a gradual normalization of blood values, and it is not unusual for a woman who has required extensive therapy for control of her disease to no longer require phlebotomies during pregnancy. Both low- and high-risk essential thrombocythaemia/polycythaemia vera pregnant patients should be treated with therapeutic phlebotomy to maintain the haematocrit at less than 45% or midgestation-specific range, low-dose aspirin, and provided with low molecular weight heparin for 6 weeks postpartum. For women with previous thrombosis or pregnancyrelated complications, low molecular weight heparin should be extended throughout the pregnancy unless there were previous bleeding issues. Additionally, interferon- has been considered the most appropriate cytoreductive agent during pregnancy for women with a history of thrombosis. Prognosis the outcome of patients with secondary polycythaemia is usually related to the prognosis of the underlying disorder. In polycythaemia vera, the nature and severity of the complications during the clinical course of the disease are the most important determinants of outcome. Disease duration is also important, as long-term survival is strongly associated with progression to myelofibrosis or acute leukaemia. As previously emphasized, prompt and appropriate therapy results in dramatic improvements in survival. Young patients should be initially managed with phlebotomy and low doses of aspirin. Supplemental therapy with interferon, anagrelide, or hydroxyurea might be required in patients with serious haemorrhagic or thrombotic episodes. The use of either hydroxycarbamide or melphalan appears warranted in the treatment of elderly patients who, because of their age, have a limited survival. Pathogenesis of thrombosis in essential thrombocythemia and polycythemia vera: the role of neutrophils. Philadelphia chromosome-negative myeloproliferative disorders: biology and treatment. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Genetic basis and molecular pathophysiology of classical myeloproliferative neoplasms. Normal megakaryocytopoiesis Platelets are released from megakaryocytes, whose development is principally regulated by thrombopoietin. Thrombopoietin production is increased by a wide variety of stimuli, which explains the many causes of secondary thrombocytosis. Clinical features-many patients (usually in late middle age) are asymptomatic at diagnosis, but common manifestations include (1) thrombotic episodes: (a) venous thromboses, including of the hepatic veins; (b) arterial thromboses, including stroke, myocardial infarction, transient ischaemic attacks, erythromelalgia (redness and burning pain in the extremities), and (occasionally) frank arterial thrombosis with gangrene; (2) bleeding episodes; and (3) moderate splenic enlargement. Alternatively, diagnosis can be met when the first three major criteria are present and the one minor criterion, namely the presence of another clonal marker or absence of evidence for reactive thrombocytosis. Treatment-this requires risk stratification based on the age of the patient and any prior history of thrombosis, with treatment being reserved for those at a high risk of developing complications and not introduced simply on the basis of platelet counts alone unless there is extreme thrombocytosis (>1500 × 109/litre). Introduction Thrombocytosis refers to a platelet count elevated above the accepted normal range (>450 × 109/litre). The widespread use of automated cell counters has made the identification of platelet count abnormalities a relatively common event. The clinical consequences of elevated platelet counts are usually determined by the cause of the thrombocytosis, ranging from the uneventful recognition of a laboratory abnormality, to medical emergencies such as lifethreatening thrombosis or haemorrhage. During times of thrombopoietic stress, there is increased production of thrombopoietin by the spleen and bone marrow. Inappropriately elevated levels of thrombopoietin may be observed in essential thrombocythaemia. This is probably not due to excessive production but rather impaired thrombopoietin clearance associated with decreased expression of the thrombopoietin receptor by megakaryocytes and platelets. Molecular abnormalities in the thrombopoietin gene, however, have been identified in several families with an autosomal dominant form of hereditary thrombocytosis where serum thrombopoietin levels are significantly elevated. This syndrome has been shown to be due to a mutation in a portion of the thrombopoietin gene, which plays a crucial role in regulating its expression. Pathophysiology and classification of thrombocytosis Thrombocytosis can occur in response to many underlying clinical conditions (secondary or reactive), or as a consequence of a primary abnormality in bone marrow function (primary). Reactive or secondary thrombocytosis accounts for over 80% of all recognized cases of thrombocytosis, iron deficiency being the most common cause. Short-lived, secondary thrombocytosis may be observed in situations such as trauma, acute bleeding, major surgery, or after strenuous physical exercise. Longer-term thrombocytosis Normal megakaryocytopoiesis An understanding of disorders of platelet production requires knowledge of the regulatory events that occur during normal megakaryocytopoiesis. Megakaryocyte development is a complex process in which a wide variety of regulatory signals work in concert to direct a highly specific response to thrombopoietic demand. Thrombopoietin acts at different levels of megakaryocyte maturation ranging from the proliferation and survival of haematopoietic stem cells/progenitor cells to megakaryocyte maturation, but does not significantly affect the release of platelets from megakaryocytes; thrombopoietin levels are regulated by the total mass of platelets and megakaryocytes, and thrombopoietin is cleared by binding to receptors on the surface of these cells. Primary thrombocytosis by contrast is associated with a group of bone marrow disorders including chronic myeloid leukaemia, essential thrombocythaemia, polycythaemia vera, primary myelofibrosis, and the myelodysplastic syndromes. The level of elevation of platelet numbers is not helpful in differentiating a reactive from a primary process. An abnormality of thrombopoietin production or of the thrombopoietin receptor has been suggested as the basis of several familial disorders associated with thrombocytosis.
The cause for the contraction in the plasma volume is poorly understood arrhythmia sounds discount lopressor 12.5 mg buy online, but autonomic dysregulation with changes in venous capacitance may be responsible heart attack bpm lopressor 100 mg order otc. The usual range of haemoglobin levels in these individuals is between 160 and 180g/litre with haematocrits ranging from 48 to 55% prehypertension at 25 years old discount 12.5 mg lopressor fast delivery. Most of these patients seek medical evaluation for an unrelated condition blood pressure chart in uk buy 12.5 mg lopressor visa, and are incidentally found to have increased haemoglobin and haematocrit values arteria facial cheap 12.5 mg lopressor. Suitable advice regarding weight reduction, control of hypertension, and smoking cessation is usually provided to these patients. Overfilling blood collection tubes can cause artefact, or pseudopolycythaemia, due to inadequate sample collection. Polycythaemia vera, the most common primary polycythaemia, is caused by an acquired defect in haematopoietic stem cells resulting in an excessive proliferation of myeloid cells. Documentation of such an increased red cell mass may require a blood volume study with direct determination of both the red cell mass and plasma volume if available. This test is presently available in select referral centres and the need for its performance Relative polycythaemias these disorders are characterized by an elevated haemoglobin or haematocrit level, which occurs as the result of contraction in plasma volume. A haematocrit value greater than 60% in men and greater than 55% in women, however, is almost always associated with absolute erythrocytosis. In such cases, it is usually unnecessary to perform blood volume studies to be assured that the patient has an absolute polycythaemia. The definitive treatment of chronic mountain sickness is descent to lower altitudes or sea level. Phlebotomy and acetazolamide therapy are recommended for affected individuals who must remain at high altitudes. Chronic pulmonary disease Pulmonary diseases are a common cause of secondary polycythaemia. Not every patient with hypoxia secondary to respiratory disease develops polycythaemia; however, the presence of concurrent inflammation or infection may blunt the marrow response to hypoxia. It is important to be aware that smoking itself may also contribute significantly to the polycythaemia associated with chronic respiratory disease. Phlebotomy may be indicated in patients with relatively high haematocrit levels (5560%), given the known deleterious effects of hyperviscosity. Chronic oxygen therapy in patients with severe chronic obstructive pulmonary disease has resulted in relief of hypoxia and modest reductions of haematocrit levels. Smoking cessation is both diagnostic and therapeutic as the erythrocytosis will resolve. Up to 25% of patients with unexplained polycythaemia are subsequently found to have sleep apnoea. Common symptoms include loud snoring, breathing pauses, feelings of nonrefreshing sleep, and excessive daytime sleeping. In these conditions, significant degrees of hypoxia may occur without evident parenchymal pulmonary disease. Diseases affecting the central nervous system may also impair respiratory centre function and trigger hypoventilation. These defects have been described in association with encephalitis, cerebrovascular accidents, and drug intoxication. Impaired skeletal muscle function of the chest wall or diaphragm may also sufficiently compromise alveolar ventilation to trigger polycythaemia. The role of phlebotomy is unclear, but not unreasonable in patients with significant elevations in haematocrit and associated cardiovascular or cerebrovascular disease. Effective treatment includes surgically induced weight loss, nasal continuous positive airway pressure ventilation, and, occasionally, the use of respiratory stimulants. Hypobaric hypoxia At high altitudes, the barometric pressure and, consequently, the ambient oxygen tension are reduced, resulting in alveolar and arterial hypoxia. Natives of the Andes (South America) who live above 4200m have been reported to have haematocrit values 30% higher than individuals who live at sea level. Acutely, changes in minute ventilation, heart rate, blood flow, and haemoglobinoxygen affinity occur as an individual reaches a high altitude. Only very small quantities of the hormone are subsequently required to sustain the red cell mass under normal circumstances. Healthy highlanders develop pulmonary hypertension, right ventricular hypertrophy, and increased amounts of smooth muscle cells in distal pulmonary arterial branches, which leads to increased pulmonary vascular resistance and pulmonary artery pressures as compared to individuals who live at sea level. Due to these adaptive changes, healthy highlanders are able to perform physical activities similar to or often even more strenuous than those living at sea level. On the other hand, many individuals living at high altitude do not demonstrate an increased haemoglobin concentration. Chronic mountain sickness is a pathological loss of adaptation to high altitude by highlanders that occurs in native or lifelong residents living above 2500m. They suffer from headaches, fatigue, impaired exercise tolerance, cyanosis, clubbing, right heart failure, and absolute polycythaemia. The prevalence of chronic mountain sickness is higher in men than in women and increases with altitude, ageing, associated lung disease, history of smoking, and air pollution. The chronic response to high altitudes is probably determined by poorly defined genetic factors, which likely contribute to the development of chronic mountain sickness. The major mechanism underlying chronic mountain sickness is relative hypoventilation, since healthy highlanders characteristically hyperventilate. Some children with congenital heart disease may develop extreme haematocrit values (80%), which leads to a significant risk of a thrombotic event, especially during periods of dehydration due to hyperviscosity and sludging within the microcirculation. The treatment of erythrocytosis in patients with cyanotic congenital heart disease is controversial and should be individualized. Phlebotomy may be indicated in some instances where it has been shown to improve cerebral blood flow and neurological symptoms and to increase exercise capacity. To date, there is no consensus defining the precise target haematocrit values for therapeutic phlebotomy in the management of patients with these disorders. It is also important to note that serial phlebotomy will cause iron deficiency and subsequent microcytosis. Microcytosis may actually worsen the symptoms of hyperviscosity and a trial of iron replacement may be warranted. Carbon monoxide intoxication Chronic carbon monoxide intoxication most commonly occurs as a consequence of smoking. Other less common causes include work-related exposures such as those seen in caisson workers, truck drivers, or tunnel toll-collectors. Carbon monoxide has a much higher affinity for haemoglobin than oxygen does, thereby reducing the amount of oxygen that can be bound and transported by haemoglobin. It also shifts the oxygenhaemoglobin dissociation curve to the left, decreasing the ability of haemoglobin to release oxygen to peripheral tissues. Polycythaemia due to chronic carbon monoxide intoxication may be associated with an increased risk of thromboembolic phenomena. Phlebotomy may be indicated in patients with very high haematocrit values (>5560%). The decreased oxygen-carrying capacity associated with carbon monoxide intoxication is not detected by standard blood gas measurements; therefore, a direct measure of carboxyhaemoglobin levels is required. Individuals with chronic carbon monoxide poisoning may experience neuropsychiatric and cardiac abnormalities. The treatment is smoking cessation or removal of the patient from the source of carbon monoxide. High-affinity haemoglobins At least 50 haemoglobin variants exhibit increased avidity for oxygen. Oxygen transport by haemoglobin occurs as a function of the oxygenhaemoglobin affinity curve. This function is represented by a sigmoid curve and is a reflection of the initial binding of oxygen by deoxygenated haemoglobin occurring with significant difficulty. As oxygen molecules are bound to normal haemoglobin, further binding is facilitated by structural changes that occur in the haemoglobin molecule. High-affinity haemoglobin variants arise when mutations alter key amino acid residues in regions of haemoglobin that affect these rearrangements, or at the interface between and chains. Increases in oxygen affinity result in a shift of the oxygen dissociation curve to the left. Consequently, haemoglobin binds oxygen more readily and retains more oxygen at lower Po2 levels. This ultimately results in decreased delivery of oxygen to tissues where capillary Po2 is low (3545mmHg). Oxygen affinity by variant haemoglobin is usually measured as the P50o2, which represents the partial oxygen pressure at which 50% of haemoglobin is saturated with oxygen. This analysis is necessary for the identification of patients with high-affinity haemoglobins. Highaffinity haemoglobins are associated with lower than normal values of P50o2; values below 17mmHg are usually diagnostic of such an abnormal haemoglobin. Haemoglobin electrophoresis or highperformance liquid chromatography may, on occasion, aid in the recognition of an abnormal haemoglobin, but many high-affinity haemoglobins display normal electrophoretic mobility or retention times. Conversely, the presence of an abnormal band per se does not provide information regarding oxygen affinity. A study of family members is important, but a negative family history does not negate the diagnosis since there is a high rate of spontaneous mutations. Most patients with high-affinity haemoglobins have mild polycythaemia and are asymptomatic since the compensatory polycythaemia results in normal oxygen delivery to tissues. Phlebotomy therapy of such patients has been reported to be of no value and has been shown to reduce exercise tolerance. Methaemoglobinaemia Hereditary methaemoglobinaemia may be associated with a mild polycythaemia. Methaemoglobin results from the oxidation of ferrous ions (Fe2+) to the ferric state (Fe3+). Oxygen does not bind reversibly to methaemoglobin, resulting in a left shift of the oxygen dissociation curve, impaired oxygen delivery, and chronic tissue hypoxia. This disorder should be suspected in patients with familial polycythaemia with a low P50o2 in the absence of a mutant haemoglobin. Chuvash polycythaemia Chuvash polycythaemia is a recognized form of congenital and familial polycythaemia endemic to the Chuvash population of the Russian Federation, which has also been reported to occur in a variety of other racial and ethnic groups. The roles of both aspirin and venesection in the treatment of Chuvash polycythaemia are unclear. In contrast to the patients with Chuvash polycythaemia, patients with mutations of prolyl hydroxylases do not have the clinical consequences described previously. Patients with hypertension and renal artery stenosis have a higher incidence of erythrocytosis than similarly hypertensive patients without renal artery disease. Unusual patients with glomerulonephritis may also occasionally present with an elevated haematocrit. Post-renal transplant polycythaemia is defined as a persistently elevated haematocrit higher than 51% after renal transplantation without an elevation of the white blood cell or platelet count. Between 5 and 13% of patients have been reported to develop erythrocytosis 8 to 24 months after renal transplantation. Approximately 60% of patients with post-transplant erythrocytosis experience headaches, plethora, lethargy, and dizziness and approximately 10 to 20% develop thromboembolic complications. Angiotensin-converting enzyme inhibitors have proved useful in controlling post-transplant polycythaemia, but phlebotomy may still be required in patients with haematocrit levels over 55 to 60% to rapidly decrease the risk of thrombotic complications. Polycythaemia occurs in 1% of patients with renal carcinomas, 9 to 20% of patients with cerebellar haemangioblastomas, and 10% of patients with hepatomas. Resection of the tumour, if feasible, may be associated with regression of the polycythaemia. Therapeutic phlebotomy is recommended in patients with extreme increases in the haematocrit. While the erythrocytosis associated with these agents may resolve with time, in other cases, phlebotomy may be needed if the agents require continuation. In the autosomal dominant form of the disease, family members have plethora, headaches, dizziness, nosebleeds, and exertional dyspnoea. Polycythaemia vera Polycythaemia vera is a clonal, chronic progressive haematological malignancy characterized by excessive proliferation of erythroid, myeloid, and megakaryocytic elements in the bone marrow. The other myeloproliferative neoplasms include essential thrombocythaemia and primary myelofibrosis. This mutation accounts for the cytokine hypersensitivity, which characterizes haematopoietic progenitors from patients with this disorder. In contrast to those with other haematological malignancies, patients suffering from polycythaemia vera may enjoy prolonged survival, provided that the excessive production of red cells and platelets is controlled. Epidemiology Polycythaemia vera was thought to be a rare disorder, with an estimated yearly incidence in the Western world between 5 and 17 cases per million population. Recent data suggest that its prevalence might be higher than previously expected with rates of at least 300 cases per million population being reported. A very low incidence of two cases per year per million population has been reported in Japan. These differences suggest that environmental as well as genetic factors might be important. Polycythaemia vera is slightly more common in men than in women, with a male/female ratio of 1. The average age at diagnosis is 60 years; it is very rare in individuals younger than 30 years of age. Biological and molecular aspects the exaggerated production of red cells, granulocytes, and platelets in polycythaemia vera suggests that the fundamental defect occurs at the level of the pluripotent haematopoietic stem cell. The clonal, and thereby malignant, nature of polycythaemia vera was first established by the cellular analysis of blood cell production in African American women heterozygous for X-linked glucose-6-phosphate dehydrogenase isoenzymes. These results have been confirmed using restriction fragment length polymorphisms of the active X chromosomes. Polycythaemia vera progenitor cells are also hypersensitive to other cytokines such as stem-cell factor, interleukin-3, and granulocytemacrophage colony-stimulating factor.
As the frequency of the sound source decreases blood pressure chart high systolic low diastolic lopressor 100 mg purchase overnight delivery, the location of the peak amplitude of the wave on the basilar membrane shifts continuously toward the cochlear apex blood pressure chart pdf lopressor 100 mg purchase online. This results in the preferential low-frequency activation of hair cells that are located closer to the cochlear Chapter 8 · the Auditory System 173 apex pulse pressure heart generic lopressor 12.5 mg without prescription. Although the mechanical properties of the basilar membrane are a key determinant of the auditory tuning of hair cells and the tonotopic organization of the organ of Corti blood pressure chart to download purchase 50 mg lopressor otc, other factors play important roles hypertension and heart disease quality 50 mg lopressor. For example, the length of the hair bundle varies with position within the cochlea. The bundles act as miniature tuning forks: the shorter bundles are tuned to high frequencies (and are located on hair cells at the cochlear base), whereas the longer bundles are tuned to low frequencies (and are located on hair cells at the apex). The electrical membrane characteristics of hair cells also contribute to frequency tuning. As is discussed in the next section, the tonotopic organization underlies the topography of connections in the central auditory pathways. To understand how the anatomical connections between the anteroventral cochlear nucleus and the superior olivary complex contribute to this function, consider how sounds in the horizontal plane are localized. A sound is recognized as coming from one side of the head or the other by two means, depending on its frequency. Low-frequency sounds activate the two ears at slightly different times, producing a characteristic interaural time difference. The farther a sound source is located from the midline, the greater the interaural time difference. For high-frequency sounds, the interaural time difference is very small and is thus an ambiguous cue. A high-frequency sound arriving at the distant ear is softer than at the closer ear. This is because sound energy is absorbed by the head, resulting in an interaural intensity difference. This is the duplex theory of sound localization because the mechanisms for low and high frequencies differ. Neurons in the medial superior olivary nucleus are sensitive to interaural time differences, and in accord with the duplex theory, they respond selectively to low-frequency tones. Individual neurons in the medial superior olive receive monosynaptic connections from the ventral cochlear nuclei on both sides. This segregation of inputs is thought to underlie the sensitivity to interaural time differences. In contrast, neurons in the lateral superior olivary nucleus are sensitive to interaural intensity differences, and they are tuned to high-frequency stimuli. Here the structure ofthe external ear is important the ridges in the auricle reflect sound pressure in complex ways, creating sound spectra that depend on the direction of the source. Specialized neurons within the dorsal cochlear nucleus appear to use this information to determine the elevation of the sound source. Not surprisingly, the ascending projection ofthe dorsal cochlear nuclei bypasses the superior olivary complex to reach the inferior colliculus directly. The dorsal and ventral cochlear nuclei are each tonotopically organized and have distinctive functions. In addition, some of the neurons in the posteroventral component engage a system for regulating hair cell sensitivity through efferent connections to outer hair cells. The ventral cochlear nucleus projects bilaterally to the superior olivary complex. Whereas we know much about the physiological characteristics of neurons in the dorsal cochlear nucleus-many process the spectral characteristics of sounds-its perceptional functions are not as well understood as for the ventral cochlear nucleus. The dorsal cochlear nucleus is thought to be important for vertical sound localization, which depends on spectral information (see next section), and for analyzing the complex features sounds. It projects directly to the contralateral inferior colliculus, bypassing the superior olivary complex. Most of the axons from each division of the cochlear nucleus decussate and reach the superior olivary complex or the inferior colliculus by one of three paths, all located in the caudal pons. Second, the dorsal acoustic stria carries the axons from the dorsal cochlear nucleus, as they cross to project to the inferior colliculus. Third, some axons of the posterior division of the ventral cochlear nucleus decussate in the intermediate acoustic stria. The cochlear nucleus is the most central site in which a lesion can produce deafness in the ipsilateral ear. Lesions of the other central auditory nuclei do not produce deafness, because at each of these sites there is convergence of auditory inputs from both ears. Myelln·mlned transverse sectfons through the rostnil poM (A) the caudal pons 8) and atthe level of the cochlear nuclei In the medulla (Q. These neurons receive auditory information from the ventral cochlear nucleus (primarily the posteroventral subdivision) and give rise to axons that project back to the cochlea via the vestibulocochlear nerve. This olimrochlMr projection regulates the sensitivity of the peripheral auditory system. This system is thought to improve auditory signal detection, to help the listener attend to particular stimuli in a noisy background, and to protect the peripheral auditory system from damage caused by overly loud sounds. Key amnectforu between the (antero) ventral mc:hlear nucleu1 in the medulla and the 5uperior ollvary c:omplex in the pon. Within the superior olrvary complex, neurons with open cell bodies and terminals are excltiltary, whlle those with blilck-tllled cell bodies and terminals are inhibitory. There are separate medial and lateral efferent control systems; both use acetylcholine as their neurotransmitter but affect sensitivity differently. The medial system originates from neurons near the medial superior olivary nucleus and synapse directly on outer hair cells. In vitro studies have shown that outer hair cells contract when acetylcholine is directly applied to the receptor cell. This mechanical change can modulate cochlea sensitivity and frequency tuning by boosting the basilar membrane traveling wave. The other olivocochlear efferent system originates more laterally in the superior olivary nucleus and synapses on the auditory afferent fi. This system affects auditory afferent activity directly, not through a mechanical action on the basilar membrane. The acoustic reflexes are another mechanism by which auditory sensitivity can be adjusted in response to a loud sound. When these muscles contract, they limit movement of the middle ear bones and dampen the oscillations of the tympanic membrane to sounds. Paralysis of the muscles can result in sounds being perceived as louder than normal, a condition termed hyperacusis. Because the acoustic reflexes are mediated by brain stem circuitsinterneurons in the ventral cochlear nucleus and motor neurons in the facial and trigeminal motor nuclei-they can be used as clinical tests of brain stem function. Many of the axons in the lateral lemniscus, especially those from part of the ventral cochlear nucleus, also send collateral (ie, side) branches into the nudeu& of the lateral lemni1c:u. The nucleus of the lateral lemniscus contains mostly inhibitory neurons that project to the inferior colliculus. The inferior colliculus is an auditory relay nucleus where virtually all ascending fibers in the lateral lemniscus synapse. It is not a sensory relay nucleus but, rather, participates in visuomotor control (see Chapters 7 and 12). Three-component parts comprise the inferior colliculus: the central and external nuclei and the dorsal cortex. The central nucleus of the inferior colliculus is the principal site of termination of the lateral lemniscus. This nucleus receives convergent input from three major sources: (1) pathways originating from the superior olivary nuclei, (2) the direct pathway from the clonal cochlear nudem, and (3) axons from the nu. The central nucleus, receiving convergent information from the ventral and dorsal cochlear nuclei for horizontal and vertical sound source localization, respectively; it contains a complete map of auditory space. The Inferior colllcull and medlal genlculate nuclei are shown on the surface view of the brain stem (A) and In myelln-stalned transvefSe sections through the rostral Bf) and caudal B. As in the somatic sensory and visual systems, lamination is used in the auditory system for packaging neurons with similar functional attributes or connections. The central nucleus gives rise to a tonotopically organized ascending auditory pathway to the thalamus, which continues to the primary auditory cortex. Animal studies suggest that the external nudeus may participate in acouaticomotor functio~ such as orienting the head and body axis to auditory stimuli. This function of the external nucleus may also use somatic sensory information, which is also projected to this nucleus from the spinal cord and medulla, via the spinotectal and trigeminotectal tracts. The brachium of the superior colliculus brings afferent information to the superior colliculus, whereas that of the inferior colliculus is an efferent pathway carrying a:mns away from the inferior colliculus to the medial geniculate nucleus (see next section). It receives the major ascending auditory projection from the central nucleus of the inferior colliculus. Although not observable on the myelin-stained section, the ventral division of the medial geniculate nucleus is laminated. Like the central nucleus of the inferior colliculus, individual laminae in the medial geniculate nucleus contain neurons that are maximally sensitive to similar frequencies. The other divisions of the medial geniculate nucleus (dorsal and medial) receive inputs from the three components of the inferior colliculus as well as somatic sensory and visual information. Rather than relaying auditory information to the cortex, they seem to serve more integrated. The primary auditory cortex (cytoarchitectonic area 41) is located in the temporal lobe within the lateral sulcus. The primary cortex, receiving direct thalamic inputs from the medial geniculate nucleus, processes basic auditory stimulus attributes. This organization of multiple representations of the receptor sheet may be similar to the primary somatic sensory cortex. As in other sensory cortical areas, the primary auditory cortex has a columnar (or vertical) organization: Neurons sensitive to similar frequencies are arranged ac:ross all six layers, from the pial surface to the white matter. Within the primary cortex, neurons represent other features of auditory stimuli besides frequency, including particular binaural interactions, stimulus timing, and additional tuning characteristics. It has a tonotopic org;mization, from high frequencies medially (represented;is the less transp;irent region in the figure to low frequencies laterally (more transparent region). The second;iry auditory cortex surrounds the primary cortex; the higher-order auditory areas surround the $4! The secondary areas receive their principal input from the primary areas and, in tum, provide information to higher-order areas. Not surprisingly, primary cortex neurons respond to simple pure tones as well as the tonal qualities of more complex sounds. The green region corresponds approxillliltely to the primary <iuditory cortex; this area responds to both pure and complex tones (le, relatlvely nonselecttve). The surrounding yellow area corresponds to secondary auditory cortex Oe, surrounding belt), which responds preferentlally to complex sounds. Hlerarchlail organlzaUon of the human auditory cortex revealed by function al magnetic resonance Imaging. Research in animals, using anatomical tracing techniques, and in humans, using noninvasive functional imaging techniques, has revealed a dorsal pathway for localizing sound sources and using sounds to guide movements. Receiving converging information from the somatic sensory and visual systems, together with this auditory information, the posterior parietal lobe constructs a representation of extrapersonal space that the brain uses to help establish where we are and where stimuli occur in relation to the world around us. Rostral Secondary and Higher-Order Auditory Areas Give Rise to Projections for Processing the Linguistic Characteristics of Sounds A second cortical auditory pathway is involved in processing nonspatial characteristics of sounds. In addition to serving a linguistic function, it is thought that the connections between the rostral superior temporal gyrus and ventral frontal lobe are important for identifying the source of speech: who is speaking o. Remarkably, words can be spoken well but their positions in sentences are often meaningless. Separate ·vmat" and *where· pathways orfgln1te from ~he auditory cortex and project to different regions of the prefrontll cortex and parletal cortex. C"llhlped pithways connect llngulstlc areu of the superior temporal gyrus with the p1rtetal and frontal lobes. Dissociating the human language pathways with high angular resolution diffusion flbl! However, modern neuropsychological studies point to significant speech disorders with rostral superior temporal gyrus lesions. Homotopic areas in the right hemisphere are important for the rhythm, intonation, and emphasis of speech, not for choosing the correct words or for structuring proper sentences. For example, damage to the right superior temporal gyrus can impair understanding intonation and emotional content, whereas damage to the right inferior frontal gyrus impairs the ability to convey emotion in speech. Interestingly, damage to the linguistic areas of both hemispheres impairs the understanding and production of sign language. Neurons in the superior olivary complex project to either the ipsilateral or the contralateral inferior colliculus via the lateral lemniscus. The posteroventral nucleus is involved in regulating hair cell sensitivity, together with the olivary cochlear system. Sensitivity to sound is also regulated by the acoustic reflexes, whereby the stapedius and tensor tympani muscles contract in response to loud sounds to dampen tympanic membrane oscillations. The central nucleus, the principal auditory relay nucleus in the inferior colliculus, has a precise tonotopic organization. They are organized into a receptive sheet within the cochlea this sheet has a precise tonotopic organization: Receptors sensitive to high frequencies are located near the cochlear base, and those sensitive to low frequencies are located near the apex. The hair cells are innervated by the peripheral processes of bipolar cells, whose cell bodies are located in the spiral ganglion.
Discount 12.5 mg lopressor mastercard. Qi Gong for High Blood Pressure (YMAA) Lee Holden.
References
- Ito S, Tanaka A, Arakawa M, et al: [Influence of thiopental administration on peripheral circulation during cardiac surgery with extracorporeal circulation], Masui 41(1):59-66, 1992.
- Dearani JA, Ommen SR, Gersh BJ, et al. Surgery insight: Septal myectomy for obstructive hypertrophic cardiomyopathy-the Mayo Clinic experience. Nat Clin Pract Cardiovasc Med. 2007;4:503-512.
- Lasagna LC, Mosteller F, Von Felsinger JM, Beecher HK. The study of the placebo response. Am J Med. 1954;16(6):770-779.
- Oddis CV. Idiopathic inflammatory myopathies: a treatment update. Curr Rheumatol Rep. 2003;5(6):431-436.
- Every NR, Parsons LS, Hlatky M, et al, for the Myocardial Infarction Triage and Intervention Investigators: A comparison of thrombolytic therapy with primary coronary angioplasty for acute myocardial infarction. N Engl J Med 1996;335:1253-1260.