
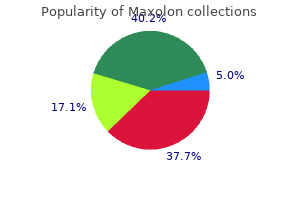
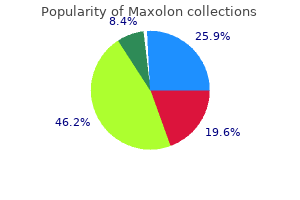
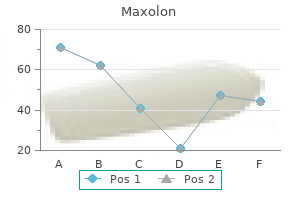
Maxolon
| Contato
Página Inicial
Michael K. Cahalan, MD
- Professor and Chair of Anesthesiology
- University of Utah School of Medicine
- Salt Lake City, Utah
Finally gastritis symptoms spanish 10 mg maxolon fast delivery, multiple lentigines gastritis diet and treatment generic 10 mg maxolon amex, which are small tan chronic gastritis remedies maxolon 10 mg buy line, dark brown gastritis zunge maxolon 10mg on-line, or black flat lesions sample gastritis diet plan effective 10mg maxolon, may be associated with various syndromes, including Peutz-Jeghers syndrome, a rare inherited disorder with mucocutaneous lentigines and intestinal polyps. Usually, the clinical history and appearance of a pigmented lesion will allow a clinical diagnosis to be made. In certain instances, a skin biopsy may be needed to make a definitive diagnosis through histologic examination. The lesions are categorized on the basis of their projected estimated size in adulthood into small, medium, and large size. Neurocutaneous melanocytosis is a proliferation of melanocytes within the leptomeninges or brain parenchyma. This proliferation can remain asymptomatic or undergo malignant change leading to symptomatic neurologic deterioration. Common- or Banal-Acquired Melanocytic Nevi Acquired melanocytic nevi may appear after the first 6 to 12 months of life and increase in number throughout childhood and adolescence. Both genetic predisposition and environmental factors can play a role in the development of acquired melanocytic nevi. Individuals with a family history of multiple nevi and lighter complexion are at higher risk of developing more acquired melanocytic nevi. Typical "common"- or "banal"-acquired melanocytic nevi may range in color from pink to light brown to dark brown and can be raised or flat. They are generally smaller than 6 mm in diameter, are symmetric, have even pigmentation with a regular outline/border, and can occur on any area of the body. Individuals with many acquired melanocytic nevi often have a predominant nevus type that shares the same general size, shape, and color. A melanocytic nevus that clearly stands out as different from the predominant nevus type, known as the "ugly duckling sign," may warrant evaluation by a dermatologist and excision for histologic examination. Atypical Melanocytic Nevi and Dysplastic Nevi Acquired melanocytic nevi that do not have a uniform clinical appearance, as seen in common- or banal-acquired melanocytic nevi, have been labeled as atypical melanocytic nevi. An atypical nevus refers to atypical clinical appearance of a nevus, while the term dysplastic nevus refers to atypical histologic findings on biopsy. These terms are often used interchangeably even though they refer to different atypical features. The clinical appearance of an atypical melanocytic nevus can include a size larger than 5 mm, irregular border, asymmetric shape, and variable pigmentation. Common locations of atypical nevi in children include the trunk and scalp, but they can occur anywhere on the body. Studies have shown that individuals with many atypical or dysplastic nevi are at higher risk of developing melanoma. Therefore, recognizing patients with this type of nevus phenotype is important, since these individuals may benefit from being followed by a dermatologist. If an atypical nevus changes or has worrisome features, full excision for histologic evaluation is necessary to rule out melanoma. Melanoma Pediatric melanoma is an uncommon but potentially life-threatening malignancy. As the incidence of melanoma in the pediatric population is increasing, specifically in adolescents, clinicians need to be aware of the possible clinical presentation of melanoma in children. Younger children with melanoma can present with a rapidly enlarging amelanotic (pink or red) raised papule or nodule that may be clinically confused with a pyogenic granuloma or Spitz nevus. Melanoma Risk Factors · Family history of melanoma · Light-colored eyes · Fair skin that burns easily · Multiple atypical or dysplastic nevi · Large congenital melanocytic nevus · History of significant sun exposure and sunburns · Underlying genetic disorder, such as xeroderma pigmentosum · History of immunosuppression · Indoor tanning bed use Chapter 52 · Pigmented Lesions 575 Box 52-3. Symptoms such as bleeding, itching, ulceration, or pain in a melanocytic nevus are additional worrisome signs. If a lesion appears clinically suspicious for a melanoma, referral to a dermatologist for evaluation and complete excision of the lesion and histologic examination is required. If melanoma develops within a small- or medium-sized nevus, it usually does not occur until adolescence. Excision of a worrisome lesion within a large nevus is often warranted to rule out melanoma. In some instances, prophylactic removal of part or most of the large nevus by an experienced pediatric plastic surgeon may be considered. Magnetic resonance imaging with contrast of the brain and spine of an infant with a large nevus and multiple satellite nevi will help assess for neurocutaneous melanocytosis. Individuals with numerous acquired melanocytic nevi need to be followed periodically with full body skin examinations for changes in their nevi. Patients with clinically atypical or dysplastic melanocytic nevi may benefit from evaluation and monitoring by a dermatologist, because these individuals are at higher risk of developing melanoma. Patients or their parents also need to watch and follow their nevi for changes over time, because melanoma is often initially noted by the patients themselves. Patients also need to monitor themselves for the rapid growth of new, clinically atypical lesions, since many cases of melanoma arise de novo. Pediatricians should follow head circumference and neurologic examination closely in infants with neurocutaneous melanocytosis. Following clinically over time those lesions that are uniform in appearance or in a location that would be difficult to remove is reasonable over routine excision in infancy or childhood. If a change is noted within a nevus, evaluation by a dermatologist and excision of the atypical region or removal of the entire nevus may be needed. Pediatricians also need to recognize which children are at higher risk of developing melanoma and encourage those individuals and their families to routinely perform self-skin examinations (see Box 52-3). Clinical presentation, epidemiology, pathogenesis, histology, malignant transformation, and neurocutaneous melanosis. The dysplastic nevus: from historical perspective to management in the modern era: part I. Melanoma in children and teenagers: an analysis of patients from the National Cancer Data Base. Indoor tanning and risk of melanoma: a case-control study in a highly exposed population. The possibility of a systemic disorder should be considered in patients presenting with generalized pruritus without an obvious source. Therapy should be directed toward the underlying cause along with extensive education on appropriate skin care. Overview Pruritus can be defined as a sensation that elicits the desire to scratch and is most commonly referred to as itching. It occurs in the setting of many disease processes and can originate from numerous organ systems. As the most common of all dermatologic concerns, it can interfere with sleep, concentration, and daily function; severity can range from being an annoyance to physically debilitating. Pruritus is classified as acute (ie, lasting <6 weeks) or chronic (ie, lasting >6 weeks). The International Forum for the Study of Itch divides pruritus into 2 primary tiers, the first tier used when origin of the itch is unknown and the second tier for known etiologies of pruritus (Box 53-1). Dermatologic Disorders Atopic Dermatitis Atopic dermatitis is a chronic inflammatory disorder of the skin. Pruritus of atopic dermatitis can have a significant effect on quality of life if left untreated. The hallmark of this disease is allokinesis, in which a normally innocuous stimulus induces intense pruritus. Examples of such stimuli can include sweating, temperature change, and skin contact with certain types of clothing or fibers. Another hallmark of this condition is a vicious "itch-scratch" cycle in which excoriations from scratching induce intense pruritus. Physical findings include sparing of the central face (headlight sign), xerosis (dryness), creases under the lower eyelids (Morgan folds), periorbital darkening, and accentuation of the palmar skin lines. In infants, it often presents on the cheeks and extensor surfaces of the arms and legs. Older children have the more typical flexural surface involvement of the antecubital and popliteal fossae, back of the neck and hands, wrists, and ankles. Treatment is directed at decreasing skin dryness using moisturizers, avoiding excessive bathing, and education on appropriate skin products. Avoiding fragrant or dye-containing soaps, detergents, and fabric softeners can be helpful. The inflammation can be treated with topical corticosteroids, preferably ointments over lotions because of the high water concentration and emollience. Starting with low-potency topical steroids and moving up in strength is the standard treatment, being sure to avoid oral or systemic steroids because of rebound flares and long-term adverse effects. Symptomatic treatment with antihistamines (Table 53-1) is important for breaking the itchscratch cycle of this disease. Children with atopic dermatitis are at high risk for multiple widespread skin infections, including molluscum contagiosum, herpes simplex (specifically, eczema herpeticum), and Staphylococcus aureus. H1-Antihistamines With Pediatric Oral Dosing Trade Name First Generation Benadryl Diphenhydramine Symptomatic relief of allergic symptoms caused by histamine release; anti-motion sickness; antitussive; mild nighttime sedative; adjunct to epinephrine in the treatment of anaphylaxis Treatment and prevention of nausea, vertigo, and vomiting associated with motion sickness 2<6 y: 6. Xerosis is characterized by dry, scaly skin and most commonly occurs on the lower extremities. Risk factors for development of xerosis include genetic predisposition, frequent bathing, and ambient high temperatures with low humidity (which is common inside heated homes during cold winter months). Primary treatment of xerosis is limitation of factors that dry the skin and increasing moisture. Contact Dermatitis Contact dermatitis arises from direct skin contact with any foreign substance. Primary irritant contact dermatitis is a nonallergic reaction to prolonged or repetitive contact with a variety of irritants, which can include detergents, soaps, saliva, acidic products, or excrement. Common examples of allergic triggers include metals (eg, nickel, chromium), oleoresin from plants (eg, poison ivy, oak, or sumac), and topical medications (eg, neomycin, bacitracin). Irritant contact dermatitis treatment involves restoring water and lipid to the skin surface using moisturizers at least twice daily (Table 53-2). Allergic contact dermatitis must be treated for at least 14 to 21 days, and the offending allergen must be identified and avoided to prevent recurrence. Dermatitis of less than 10% of skin surface can be treated with topical corticosteroids of moderate potency in ointment preparations for 2 to 3 weeks. If the dermatitis involves greater than 10% of the skin surface, systemic steroids are necessary. The typical lesion is well circumscribed, blanchable, raised, and erythematous with central pallor. The lesions may enlarge and coalesce, transiently appearing and disappearing and resolving most often over a few hours. Acute urticaria is defined as lasting less than 6 weeks, while chronic urticaria refers to persistent or recurring lesions lasting 6 weeks or more. Acute urticaria is usually an allergic reaction, while chronic urticaria has various causes including systemic disorders. Common causes of acute urticaria include allergens (eg, foods, medications, pollens, stinging insects), physical factors (eg, cold, heat, pressure as in dermographism, exercise induced), and infections. Papular urticaria is a common cause in children, primarily from stinging insects (eg, fleas, mosquitoes, bedbugs) and characterized by papular or vesicular linear clusters. Unlike in adults, the association of chronic urticaria with malignancy is not well established in children, so evaluation for malignancy is usually not necessary. However, if malignancy is suspected, the patient should be referred to an oncologist. Types of Moisturizers Type Occlusive Mechanism Blocks transepidermal water loss Indication Xerosis Atopic dermatitis Prevention of irritant contact dermatitis Xerosis Ichthyosis Examples Petrolatum Zinc oxide Lanolin Mineral oil Silicones Messy Comedogenic May cause folliculitis (mineral oil) or dermatitis (lanolin) May cause irritation (urea, lactic acid) Humectant Attracts water to the stratum corneum Urea Alpha-hydroxy acids Glycerin Sorbitol Lactic acid Cholesterol Squalene Fatty acids Ceramides Natural moisturizing factor Emollient Smoothes skin Decreases skin roughness Possible skin rejuvenation Not always effective Unproven benefits; may improve skin moisturization and barrier function Replacement of deficiencies in "raw materials" of the intact stratum corneum Claims to replenish essential skin components Treatment of urticaria focuses on avoiding underlying triggers and histamine blockers (see Table 53-1). If maximal doses of H1-receptor antagonists do not relieve symptoms, an H2-receptor antagonist, such as ranitidine or cimetidine, may be added. For severe or refractory cases, oral glucocorticoids may be used in short bursts (0. If there are any signs or symptoms of anaphylaxis (eg, angioedema, respiratory distress, or gastrointestinal distress), a self-injectable epinephrine pen should be prescribed. Chronic urticaria or refractory cases should be referred to an allergist for further evaluation and management. Miliaria Rubra More commonly referred to as prickly heat or heat rash, miliaria rubra is caused by blocked eccrine sweat glands at the granular layer of the skin. The rash is characterized by intense erythema with maculopapular vesicles and pruritus. It occurs in hot, humid environments often on intertriginous areas or surfaces of the body covered by clothing. Tinea cruris (or jock itch) typically presents with bilateral, crescent-shaped lesions extending from the inguinal folds to upper thighs. Most fungal skin infections are treated with topical antifungal creams (eg, miconazole, clotrimazole, terbinafine). However, tinea capitis requires oral therapy (eg, griseofulvin, fluconazole, terbinafine, or itraconazole). Viral infections (ie, chickenpox, molluscum) and bacterial infections (ie, folliculitis) are also recognized causes of pruritus. Insect Bites and Infestations Insect bites (especially mosquitos, fleas, and scabies) can be markedly pruritic. Some children develop papular urticaria, a delayed hypersensitivity reaction to insect bites that is more common in warmer months. The rash of papular urticaria is characterized by erythematous or umbilicated papules most commonly found in groups on the trunk and extensor surfaces of the extremity. Scabies is a common infestation in the pediatric population caused by the mite Sarcoptes scabiei. The pathognomonic finding is the threadlike burrow (ie, thin gray, red, or brown line 215 mm long) produced from the mite traveling through the epidermis. Most often lesions are located on the intertriginous areas of the neck, axillae, groin, and webs of fingers and toes.
However gastritis diet what to eat discount maxolon 10 mg buy, the effect was not due to the injection itself but to the anesthetic agents used gastritis diet �������� purchase maxolon 10 mg mastercard. That is gastritis diet �������� buy cheap maxolon on line, the cytotoxic anesthetic agents bound to the enamel matrix in the developing tooth germ gastritis diet for children maxolon 10mg buy free shipping. The same effect would seemingly be produced by an infiltration injection next to the developing tooth gastritis ginger ale best purchase for maxolon. Precautions Do not use intraligamentary injections in painful necrotic teeth with periapical radiolucencies or teeth exhibiting cellulitis or abscess formation. The intraosseous technique had a quicker onset and a shorter duration of anesthesia. Although not studied, patients taking oral bisphosphonates may be able to receive intraligamentary injections. Nusstein and coauthors62 compared infiltration and intraosseous injections in the maxillary lateral incisor using 1. Beneito-Brotons and coauthors63 and Peñarrocha-Oltra64 and coauthors also showed a faster onset and shorter duration with intraosseous anesthesia. The anesthetic solution is present in the cancellous bone with the intraosseous injection initially and is then depleted by absorption into the general circulation. The anesthetic solution with the infiltration injection is deposited in the soft tissues and then passes through the barriers of the periosteum and cortical bone. The soft tissue reservoir of local anesthetic solution with the infiltration injection allows a more favorable infusion of anesthetic solution over time. You will feel some vibrations and possibly your heart may beat a 132 Intraosseous Anesthesia little faster. We should not say, "We are going to drill through your gum and bone and then give you " a shot of the anesthetic. Intraosseous injection systems There are two intraosseous systems that have been extensively studied clinically-the Stabident system (Fairfax Dental) and the X-Tip system (Dentsply Maillefer). Three other anesthetic systems have been available-the Anesto system (Innovadontics), the Comfort Control Syringe (Dentsply), and the IntraFlow (Pro-Dex), which is no longer marketed. Note: Videos and information on the various systems are available at the manufacturer websites. A point approximately 2 mm below the intersection of these lines is selected as the perforation site. With the point gently resting against bone, the handpiece is activated at full speed while pushing the perforator with light pressure against bone and then slightly withdrawing the perforator and then pushing it against the bone. This action is continued until a "breakthrough" into the cancellous bone is achieved (taking approximately 2 to 5 seconds) or the perforator is placed to length. However, in mandibular anterior teeth, the perforator should not be inserted to full length because it may go through the lingual surface. Clinical tip: A sterile endodontic rubber stopper can be placed on the injector needle to provide a better seal with the mucosal tissue. The needle can be bent at the hub to a 60- to 80-degree angle to allow for ease of insertion in posterior teeth. Then, without taking your eyes away from the target site, have the assistant hand the syringe to you and place the needle in the same pathway as the perforator. If the needle will not enter the perforation site, reperforate the same site and try again. Sometimes placing a periodontal probe into the perforator hole makes it easier to visualize the angle of needle entry. Once the needle fully enters the perforation, a full cartridge of anesthetic solution is slowly delivered over a 1- to 2-minute time period with light pressure. If back pressure is encountered, the needle is rotated approximately a quarter turn and deposition is reattempted. If this attempt is unsuccessful, the needle should be removed and checked for blockage. If the needle is not blocked, it is reinserted, or the site is opened with a new perforator and the injection is repeated. The incidence of a difficult perforation with the Stabident perforator is around 24%. The drill (a special hollow needle) leads the guide sleeve through the cortical plate, where it is separated and withdrawn. Technique With the patient in a reclining position, the area of perforation is determined as explained for the Stabident system. If the site is in alveolar mucosa, the site is approximately 3 to 7 mm inferior to the Stabident perforation site. The following describes use of the X-Tip system if the site is in alveolar mucosa. The alveolar mucosal soft tissue adjacent to the determined perforation site is anesthetized by infiltration. Five minutes after the infiltration injection, pressure is applied at the determined perforation site with a periodontal probe. If the patient feels pain, an additional amount of anesthetic solution is administered. The guide sleeve of the X-Tip system is secured against the drill via finger pressure as the red protective covering is withdrawn. The alveolar mucosa is pulled taut using the fingers of the other hand to minimize engaging the mucosal tissue during rotation of the perforator. The perforator is pushed through the alveolar mucosa until the X-Tip contacts bone. With the drill held at a 90-degree angle to the bone, the slow-speed handpiece is activated at full speed while pushing the perforator lightly against bone and then slightly withdrawing the perforator and then pushing it against bone. This action is continued until a "breakthrough" feeling is observed or the perforator is placed to length. The handpiece is always activated while the perforator is within bone to prevent lodging or breakage that might occur if the perforator is allowed to stop rotating. Clinical tip: A sterile endodontic rubber stopper can be placed on the injector needle to provide a better seal with the guide sleeve. Before inserting the 27-gauge X-Tip needle into the guide sleeve, the needle can be bent at the hub to a 60- to 80-degree angle to allow for ease of insertion in posterior teeth. A standard syringe is held in a pen-grip fashion, the needle is inserted into the guide sleeve to its hub, and the anesthetic solution is delivered slowly over a 1- to 2-minute time period with light pressure. If back pressure (greater than light finger pressure on the syringe handle to deliver the solution) is encountered on solution deposition, the needle is rotated approximately a quarter turn and deposition is reattempted. If not blocked, reinsert the needle through the guide sleeve and deposit the solution. Upon completion of solution deposition, the guide sleeve is removed using a hemostat. The guide sleeve can be left in place if the clinician anticipates that additional anesthetic is needed during the appointment. Therefore, even though the X-Tip perforation is performed in a more apical location, the two systems are clinically comparable for ease of perforation. Guide sleeve removal Guide sleeve removal with the X-Tip system was rated as easy (removal within 5 seconds) 68% of the time. Although difficult removal is based on time, it is worth mentioning that guide sleeve removal required both effort and time in approximately 12% to 17% of patients. Activate the press button and fit the needle changer onto the protective cap of the injection needle. Once the penetration site is selected and anesthesia administered, place the needle through the mucosa and start the drill by stepping on the rheostat. Apply firm pressure to the handpiece and advance the rotating perforator through the cortical plate. Once the perforation is accomplished, stop the motor and rotate the locking knob counterclockwise. If the anesthetic solution is not being delivered (dosage lever does not depress), rotate the needle and assembly head after activation of the motor. If still blocked, remove the needle by activating the motor and try another perforation site after adding another needle and cartridge of anesthetic. Once the desired anesthetic dosage has been delivered, start the motor by stepping on the foot pedal. The needle will begin rotating again and can be withdrawn in a single, smooth motion. It is sometimes difficult to administer intraosseous anesthesia in molars with the Anesto system because of the straight-line access required with this device. The problem is that the presettings may not allow enough anesthetic solution to be delivered for certain types of injections. No objective studies have evaluated the Comfort Control Syringe system in clinical dentistry. However, it is questionable if the short injector part of the needle would penetrate through the cortical bone in posterior teeth. Considerations Drilling into tooth with perforation this should not be a major concern because quite a bit of pressure and time is required when encountering a tooth root. Once this resistance is noticed, and the perforator is not advancing, withdraw the perforator and select another site. There should be little consequence to making a small superficial hole in the surface of the tooth. Pulp safety Clinical studies have shown no effect on the pulp following intraosseous injections. To counteract this, simply place a gloved finger over the first perforation site to keep the anesthetic solution from flowing out of the hole-just like the little Dutch boy at the dike. Lip numbness the manufacturers of Stabident and X-Tip state that there is a lack of lip anesthesia when the intraosseous injection is given. Replogle and coauthors66 and Coggins and coauthors67 also reported lip anesthesia when using 1. Lip numbness is most likely related to the initial intramedullary deposition with extravasation of local anesthetic solution from the mental foramen. It is probably not related to numbing the inferior alveolar nerve within the bone. A preliminary study demonstrated with computer tomography that a Stabident injection of 1. This effect probably occurs in humans as well and accounts for the lip numbness (mental nerve anesthesia). Pain of perforation and solution deposition When using the Stabident or X-Tip system as a primary method in asymptomatic subjects, Coggins and coauthors,67 Replogle and coauthors,66 and Gallatin and coauthors65 reported an approximately 23% incidence of moderate pain for perforation in various maxillary and mandibular teeth. Generally, the clinician should be aware that moderate pain may be experienced when using the intraosseous injection technique. As a supplemental technique in asymptomatic patients, only 3% of the patients will have pain with perforation and needle insertion. There is less potential for pain when the intraosseous injection is used as a supplemental technique. Perforator separation and breakage In about 1% of uses of the Stabident and X-Tip systems, the metal perforators separate from the plastic shank during use. The separation usually occurs during a difficult perforation (eg, dense cortical bone), and it is likely that the metal is heated excessively due to friction with the bone, causing the plastic hub to melt slightly. No perforator breakage (ie, metal perforator breaking into parts) has been reported in numerous studies. If the clinician does not feel comfortable performing the procedure, referral to an endodontist is indicated. Optimal injection site selection Location It is important to remember that a site distal to the tooth to be anesthetized will result in the best anesthesia. This recommendation is based on the numerous studies that show the greatest anesthetic effect for a distal injection. Attached gingiva or alveolar mucosa Both the Stabident and X-Tip intraosseous systems instruct the user to locate the perforation site in attached gingiva. The gingival site allows the perforation to be made through a minimal thickness of cortical bone and is generally equidistant between adjacent root structures. However, because the guide sleeve remains in place with the X-Tip system, two studies have successfully used it in alveolar mucosa at a more apical location. If the Stabident system is used apically in alveolar mucosa, it is almost impossible to find the hole to deliver the anesthetic solution. Therefore, the clinician may want to consider using the X-Tip in an apical location in specific clinical situations. Furthermore, if the Stabident system fails, the clinician may want to consider using the X-Tip apically to achieve pulpal anesthesia. Replogle and coauthors66 reported a similar success rate for the mandibular first molar using a lidocaine formulation. The higher success rate in the study by Gallatin and coauthors65 may be related to back pressure occurring in the earlier studies by Coggins and coauthors67 and Replogle and coauthors. Chamberlain and coauthors77 found that 95% of patients were successfully anesthetized for restorative procedures when using the Stabident system. Sixou and Barbosa-Rogier78 found a clinical success rate of 92% in children and adolescents using an intraosseous system. The lateral incisor has a more rapid decline of pulpal anesthesia when compared with the first molar. Therefore, 3% mepivacaine is not as successful as 2% lidocaine with 1:100,000 epinephrine. There is a shorter duration of pulpal anesthesia with 3% mepivacaine or solutions with reduced vasoconstrictor concentrations (eg, 1. In general, the duration of pulpal anesthesia of 20 to 30 minutes is a drawback to using the technique as a primary injection technique. Clinicians will appreciate the immediate onset and the duration of pulpal anesthesia.
Additionally gastritis diet tips discount 10mg maxolon overnight delivery, extension of infection from the epiphysis into joint space may also occur gastritis symptoms breathing cheap maxolon 10mg overnight delivery, and is more common in children younger than 18 months of age (up to 75% in neonates) because of presence of bridging vessels from the epiphysis to physis gastritis stool cheap maxolon 10mg buy on line. Staphylococcus aureus is the most frequent pathogen identified in the setting of osteomyelitis and septic arthritis gastritis symptoms and treatments generic 10 mg maxolon, but other pathogens play a role in different age groups and clinical settings (Table 5-1) scd diet gastritis buy maxolon 10mg on line. Streptococcus pyogenes, Kingella kingae, and Streptococcus pneumoniae are other relatively commonly encountered organisms. Although S pneumoniae has become a less frequent pathogen with widespread immunization, it continues to be seen occasionally in young children. Some data suggest that K kingae is the most frequent cause of osteomyelitis and septic arthritis in the toddler age group, between 15 months and 3 years of age. Nasal colonization is close to 30% in those who attend day care in this age group. Infection with K kingae is often preceded with a viral upper respiratory tract infection and is presumably the portal of entry for hematogenous spread. Osteomyelitis and septic arthritis in the neonate is a different disease entity than in the older child. Neonates are more likely to have polymicrobial infection or multifocal infection (20%50%) and to develop permanent sequelae Table 5-1. In addition to bacteremia, the risk factors for neonatal disease include prematurity, indwelling catheters, fetal scalp electrodes, and repeated heel sticks. The causative pathogens are somewhat different than for older children as well, with Streptococcus agalactiae (also called group B Streptococcus), enteric gram-negative organisms (eg, Escherichia coli), and Candida species of clinical importance in addition to S aureus. Neisseria gonorrhoeae is also a known cause of neonatal osteomyelitis and septic arthritis. Neisseria gonorrhoeae may also cause septic arthritis in adolescents with an associated sexually transmitted infection. It is more common in girls than boys and considered a feature of disseminated infection that usually stems from cervicitis. The knee is the joint most commonly affected, with shoulder and hip being involved uncommonly. However, joint fluid cultures are less frequently positive than with other etiologies of septic arthritis. Mycobacterium tuberculosis is an uncommon cause of osteomyelitis and septic arthritis, and osteoarticular disease accounts for approximately 1% of disease manifestations in patients infected with this organism. This infection differs from the other more common bacteria by its ability to remain dormant or cause low-grade symptomatology for years. Low-grade fevers and weight loss are more common features in addition to pain and swelling at the site of infection compared with other more common pathogens. Lower thoracic vertebrae are the most common bones involved in this infection (as seen in Pott disease) followed by the long bones and hands and feet. Salmonella species and other gram-negative enteric organisms are typically uncommon pathogens, but increase in frequency in the setting of hemoglobinopathies (eg, sickle cell disease), which is thought to be related to enteric translocation of bacteria. Soil pathogens, such as Pseudomonas aeruginosa, Nocardia species, nontuberculous Mycobacteria species, and fungal organisms (eg, Aspergillus species), play a role in soil-contaminated wounds, penetrating injuries, and occasionally the immunocompromised host. Patients with chronic decubitus ulcers are also at risk for bone infection with environmental pathogens, and in the setting of sacral ulcer, gram-negative enteric and anaerobic organisms are frequent pathogens. Actinomyces species are a well-recognized cause of mandibular osteomyelitis (ie, lumpy bumpy jaw syndrome), related to tooth extraction, caries, oral surgery, or oral trauma. Although not typically a pathogen in the healthy host, coagulase-negative staphylococci and Propionobacterium acnes may be the causative agent in the setting of spinal hardware, prosthetic joint, or external fixators. Oral anaerobes from humans (Eikenella corrodens), cats (Pasturella multocida), or dogs (Capnocytophaga species) may cause bone or joint infection in the setting of a penetrating bite wound. Other anaerobic organisms, such as Fusobacterium 68 Succinct Pediatrics necrophorum, Bacteroides fragilis, Peptostreptococcus, and Clostridium species, are rare causes of bone and joint infection. Additionally, Bartonella henselae (ie, cat-scratch disease) is a rare cause of granulomatous bone infection in patients with a history of kitten or cat exposure, even without a recognized scratch event. The differential diagnosis of acute osteomyelitis and septic arthritis is large and includes oncologic processes such as leukemia, osteosarcoma, Ewing sarcoma and other primitive neuroectodermal tumors, and neuroblastoma. Non-oncologic possibilities include Gaucher disease, polyarteritis nodosa, serum sickness, and, extremely rarely, scurvy. Central nervous system disease, birth trauma with neuropathy, and violent trauma should also be considered in the differential for neonates with pseudoparalysis. The median age of onset is slightly older at 10 years (versus 5 years for bacterial osteomyelitis), with girls being more often affected than boys. Clinical Features Common clinical features of bone and joint infection include fever, pain, edema, erythema, and decreased range of motion of the affected area. Point tenderness over the metaphysis is also typically noted in bone infections, while severely limited range of motion is a more common feature of septic arthritis. Referred pain is common in both osteomyelitis (eg, abdominal pain in vertebral osteomyelitis) and septic arthritis (eg, knee pain in septic hip) and can make determining the focus of infection difficult. Other subtle differences on physical examination may provide diagnostic clues when the site of infection is not readily obvious on clinical examination. Infection in the upper extremity leads to a decrease in voluntary movement and sometimes complete refusal to use the extremity. Infection in the lower extremity often leads to a refusal to bear weight in that extremity. Nonambulatory infants may keep their leg in flexion and external rotation when held upright on Chapter 5 · Osteomyelitis and Septic Arthritis 69 examination, or may exhibit only asymmetric movements. Spinal osteomyelitis may be suspected by an inability to bend forward toward the toes. Other nonspecific presenting symptoms may include anorexia, malaise, and vomiting. Long bones of the appendicular skeleton are the most commonly affected (75%90%) in the setting of osteomyelitis, with multifocal disease occurring in 5% of cases outside the neonatal period. In the setting of osteomyelitis, it is imperative to carefully examine the adjacent joint for evidence of concomitant septic arthritis, because up to 30% of joints surrounding the affected bone may be affected. The knee is the most commonly affected joint in the setting of septic arthritis, followed by the hip and then ankle. Polyarticular infection is uncommon (<10%), but occurs with Neisseria meningitidis, N gonorrhoeae, and Salmonella species. Concomitant cellulitis or myositis may also be present in the setting of bone and joint infection and can make it difficult to determine whether there is an underlying osteomyelitis or septic arthritis based on clinical examination findings. Vertebral osteomyelitis presents in a nonspecific manner, which often leads to a delay in diagnosis. Infants may present with sepsis, while older children generally have concerns of abdominal, leg, chest, or back pain. Point tenderness should be present over the infected area, and surrounding soft-tissue swelling may be seen. Neurologic deficits related to spinal cord compression may be present at diagnosis and occur in up to 20% of cases. Pelvic osteomyelitis accounts for 6% to 9% of bone infections and is similar to vertebral infection in that it often presents with symptoms that are nonlocalizing, which may lead to delayed diagnosis. The ilium and ischium are the 2 most common bones involved, and pain in the hip, leg, and buttock are often seen. Septic hip is oftentimes considered in this setting; however, in converse to septic arthritis, movement of the hip joint is less restricted, pain is elicited with pelvic girdle rocking, and point tenderness over the affected bone is commonly seen in pelvic osteomyelitis. Evaluation Bacteremia is present in approximately 50% of cases of osteomyelitis and slightly less prominent in septic arthritis (40%). Bacteria may also be identified from bone aspirate, or synovial fluid, in 60% of infections. K kingae is a fastidious organism whose growth is enhanced by inoculation of aspiration specimens into a blood culture bottle. Polymerase chain reaction testing is also available for K kingae, with a high degree of sensitivity. Cell counts within the joint fluid should be analyzed in addition to obtaining specimens for culture. Inflammatory markers, such as C-reactive protein level and erythrocyte sedimentation rate, are elevated in greater than 90% of infections. C-reactive protein level should peak on the second day and typically normalizes after 1 week of appropriate therapy. Erythrocyte sedimentation rate tends to peak a little later (35 days) and lowers more slowly with normalization at 35 weeks. Marrow changes related to infection appear low in signal intensity on T1 images and high on T2. Gadolinium enhancement helps delineate abscesses and soft-tissue involvement, which is especially useful in certain clinical situations when it is difficult to distinguish between type of infection on physical examination, or the presence of more than one type is suspected. Bone scan has the ability to show abnormalities in both the affected bone and joint prior to appearance on plain radiograph. Increased uptake in the metaphysis is indicative of osteomyelitis, while increased uptake on both sides of a joint indicates articular infection. The sensitivity is between 80% and 100% and most useful in the setting of suspected multifocal infection. Plain radiograph may show abnormalities such as periosteal elevation, a lytic lesion, and new bone formation in as few as 10 days into the course of infection. In the setting of articular infection, plain radiograph may reveal a widening of the joint space and displacement of fat planes surrounding the joint. Sclerosis of the bone may be seen when infection has been present for longer than 1 month. In patients who have undergone multiple previous radiographies or other radiation exposures, reducing further exposure should also be a consideration. Surgical debridement is imperative in the setting of septic hip, but arthrocentesis may be sufficient for infection in other joints. Surgical management not only aids in delineating an organism and thus optimal antimicrobial therapy but also allows for improved antimicrobial penetration into the bone or joint, and serves to hasten clinical recovery. Antimicrobial therapy should be empirically initiated to provide coverage for the typical pathogens according to age and mechanism of infection. In addition, local susceptibility patterns should be taken into consideration when choosing therapy. In the hospitalized patient, parenteral therapy is typically initiated, including anti-staphylococcal penicillins (eg, oxacillin), firstgeneration cephalosporins (eg, cefazolin), or clindamycin. All of these agents possess good bone penetration and provide good S aureus coverage. Further, in some communities the resistance rate to clindamycin is rising for both methicillin-susceptible S aureus Table 5-2. Fluoroquinolones are not recommended routinely for children with bone and joint infections but are sometimes necessary in the setting of infection related to soil-contaminated wound or sacral decubitus ulcer. Gentamicin or a thirdgeneration cephalosporin (eg, cefotaxime) should be a part of the empiric therapy regimen in neonates. Additionally, a third-generation cephalosporin should be used in the setting of N meningitidis or N gonorrhoeae articular infection. Disease caused by M tuberculosis is treated with surgical debridement when an abscess is present or stabilization surgery in the setting of spinal instability. Therapy length is not often determined at diagnosis but is determined over time involving multiple factors, including response to therapy, surgical intervention, extent of disease, specific pathogen, and chronicity of infection. The guideline further recommends 4 to 6 weeks of therapy for osteomyelitis and 3 to 4 weeks for septic arthritis in children, which may be longer if contiguous osteomyelitis is present (occurs in 75% of neonates and 30% in older children). However, 10% to 25% of children with articular infection will develop long-term sequelae, including decreased joint mobility, chronic dislocation, and avascular necrosis of the femoral head. Risk factors for development of sequelae because of septic arthritis are listed in Box 5-1. Risk Factors for Permanent Sequelae Following Septic Arthritis · · · · · · Infant <6 mo Adjacent bone infection Hip or shoulder infection 4 d delay in joint decompression and antibiotic therapy Prolonged time to synovial fluid sterilization Infection with Staphylococcus aureus or a gram-negative bacillus Adverse effects related to prolonged antimicrobial therapy may also occur, and patients should be monitored clinically and with laboratory testing specific to the antibiotic in use. Laboratory monitoring may provide early clues of a developing adverse effect and is important for defining the duration of therapy (see Table 5-2). A subset of patients with S aureus disease from a Panton-Valentine leukocidin-producing strain are more likely to develop more severe disease and phlebothrombosis as a complication. Involvement of a hematologist is important in this setting to initiate and manage anticoagulation therapy and provide guidance regarding testing for an underlying hypercoagulable state. In addition, Panton-Valentine leukocidin-producing strains may increase the risk of developing chronic infection. Acute osteomyelitis develops into chronic infection in less than 5% of cases, and this is more often associated with non-hematogenous osteomyelitis (eg, hardware-associated infection). The patient may have a prolonged asymptomatic period followed by recrudescence of pain, edema, and sinus tract formation that does not improve, or only partially improves with prolonged antimicrobial therapy. Polymicrobial infection is often present in such cases, making surgical debridement for culture and to remove necrotic bone and tissue the key to management. Skin grafts and muscle flaps are used to enhance blood flow in some traumatic wounds and in wounds with impaired sensation (eg, decubitus ulcers). Antibiotic-impregnated beads or cement material is sometimes placed at the time of debridement to enhance antibiotic delivery to the area and promote stability of the bone. Additionally, intraarticular antibiotics have been used in the setting of infected joint prosthesis. Treatment of an infected joint prosthesis somewhat depends on timing of onset related to surgery, length of symptoms prior to diagnosis, and the surgical Chapter 5 · Osteomyelitis and Septic Arthritis 75 approach to address the infected hardware. Retrospective review of osteoarticular infections in a pediatric sickle cell age group. Specific real-time polymerase chain reaction places Kingella kingae as the most common cause of osteoarticular infections in young children. Current understanding of the pathogenesis and management of chronic recurrent multifocal osteomyelitis. Clinical practice guidelines for the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children.
Probable reactive node Size d 1 cm Size fluctuates Malignancy should be excluded Size > 2 or 3 cm Supraclavicular location 407 Mobile History of malignancy Appears with upper respiratory Progressive increase in size tract infection Tender No B symptoms Fixed Matted Systemic/B symptoms Persistent Cervical Lymphadenopathy Most patients seen in the outpatient department referred by their general practitioner will fall into this category gastritis diet ������ 10 mg maxolon purchase with amex, loosely defined as lymphadenopathy persisting >6 weeks gastritis problems maxolon 10mg online. Most clinically benign nodes can be managed expectantly gastritis diet ����� maxolon 10 mg order fast delivery, but if worrisome features (especially size over 2 or 3 cm gastritis diet 7 up cake cheap maxolon online visa, supraclavicular location gastritis diet ���������� purchase cheap maxolon line, history of malignancy, or presence of B symptoms) are present then excision biopsy is warranted. Pel-Ebstein fever, the classic intermittent fever associated with Hodgkin disease, occurs at variable intervals of days to weeks and lasts for 12 weeks before resolving. A variety of specific chronic infections may be associated with persistent neck lymphadenopathy: · Cat scratch disease: Granulomatous condition occurring some weeks after a cat scratch and inoculation with Bartonella henselae, presenting with chronic tender cervical lymphadenitis, mild fever, and malaise. Serology for diagnosis is helpful, as is culture or polymerase chain reaction examination of any discharging material, but surgical management may lead to persistent drainage and poor wound healing. Infection is environmentally-acquired, usually with insidious presentation of an enlarged lymph node present for weeks or months. Untreated, these often drain spontaneously, forming a sinus tract leading to severe scarring but usually eventual spontaneous resolution 12 years later. Complete surgical excision of the infected lymph node without antibiotic therapy is the ideal treatment. Curettage may be useful in these cases, as may long-term antibiotics (rifampicin/ clindamycin). Lymphadenopathy may be localized or generalized, persisting for a number of months. A variety of systemic illnesses can also present with persistent cervical lymphadenopathy, with some examples listed in Table 36. These may often be associated with constitutional symptoms of pyrexia and weight loss, hepatosplenomegaly, and/or mediastinal lymphadenopathy. Branchial Cleft Cysts Branchial cleft anomalies comprise the second most common congenital neck mass in children. These lesions result from incomplete obliteration of the branchial clefts and pouch during embryogenesis. Presentation Branchial cysts and sinuses may be diagnosed on history and physical examination alone, particularly if there is an external pit. They often present as a sudden lateral neck swelling, with tenderness, erythema, and pain. Ultrasonography may be less useful for third branchial anomalies as it may be difficult to define hypopharyngeal lesions. Embryology the branchial apparatus is made of six grooves, arches, and pouches, consisting of ectoderm, mesoderm, and Chapter 36: Neck Lump(s) Table 36. Weight loss, pyrexia Diagnosis of exclusion Full blood count, lymph node biopsy 409 Lung and salivary inflammation, rash neurological Chest radiograph, angiotensin converting signs enzyme Fever, rash, weight loss, bone pain, vomiting, Biopsy seizures Table 36. From the 4th to 8th week of gestation, four well-defined branchial arches (two are rudimentary) are visible in the cervical area of the embryo. Branchial anomalies typically lie inferior to the structures of the associated arch. A branchial cyst forms when a branchial groove remnant forms an epithelial-lined space without communicating with the skin or mucosa. They are variably located, extending from the postauricular area or parotid, to submandibular area, superior to the hyoid. Parotid and postauricular lesions may present as an enlarging mass after infection, with associated erythema and pain. They may course superiorly, inferiorly, or through the branches of the facial nerve if in close proximity to the superficial lobe of the parotid gland. Second Branchial Anomalies: Second branchial arch anomalies are the most frequent (9095%) branchial anomaly, with sinuses most common, followed by cysts, and then fistulae. Fistulae are typically diagnosed in infancy or childhood and present as chronic drainage from an opening along the anterior border of the sternomastoid in its lower third. They course superior and lateral to the common carotid artery, between the internal and external carotid arteries, then lateral and superior to the glossopharyngeal and hypoglossal nerves to penetrate the middle pharyngeal constrictor muscle and open into the tonsillar fossa. Third arch anomalies penetrate the platysma and continue through the thyroid, along the carotid sheath, and over the superior laryngeal nerve, deep to the glossopharyngeal nerve, and behind the internal carotid artery. They pierce the thyrohyoid membrane and enter the upper lateral piriform fossa wall. Fourth Branchial Anomalies: the course is similar to a third anomaly except that they course under the superior laryngeal nerve and above the recurrent laryngeal and hypoglossal nerves. They then return to the chest to pass around the aortic arch on the left and subclavian artery on the right before ascending to enter the larynx near the cricothyroid joint or through the lower horn of the thyroid cartilage. Classically, they present as recurrent left-sided (87%) neck abscesses or suppurative thyroiditis before the age of 10 years. Direct laryngoscopy has a positive predictive value of 82% and 90% for third and fourth branchial anomalies, respectively. Management Previously, complete surgical excision was recommended, and this continued to be true for first and second branchial lesions. However, recent evidence suggests that in third and fourth arch anomalies, endoscopic obliteration of the opening of the tract is sufficient to prevent recurrence or reinfection. Excision of the cyst is not always indicated and needle drainage of the infection or the cyst contents is frequently all that is required. Vascular anomalies Vascular tumors Benign Locally aggressive Malignant Vascular malformations Simple Capillary malformation Lymphatic malformations Venous Malformations Combined Arteriovenous malformations present in the neck area. We will cover the more common forms, which Hemangioma Infantile hemangiomas are common, benign vascular tumors, but must be differentiated from the more aggressive forms of vascular tumors (Table 36. The incidence is increased (23%) in premature babies with a birth weight < 1,200 g. Sixty percent of infantile hemangiomas occur in the head and neck region and 20% will be associated with other lesions in the brain, gastrointestinal tract, or liver. They grow rapidly during infancy and have three distinct clinical, microscopical, and immunohistochemical phases. The proliferative phase lasts 69 months and after 12 months the tumors tend to shrink, fade, and flatten (involution phase). More than 50% children have complete resolution by the age of 5 years with further improvement until age of 12 years (involuted phase). Almost half of the children have some residual abnormality such as residual fibrofatty tissue, redundant skin, yellow discoloration, or telangiectasia (Abramowicz and Padwa, 2012). They can be subclassified in terms of the pattern of presentation and depth of the lesion. There has been a significant management shift when propranolol was discovered to have a positive beneficial effect in reducing the proliferative phase of this condition, and many cases have avoided destructive local growth and surgical extirpation. Congenital Hemangioma Congenital hemangiomas are rare vascular tumors that are fully grown at birth and do not behave in the same way as infantile hemangiomas. Rapidly involuting congenital hemangiomas are raised, red-violaceous lesions with central telangiectasia, superficial ulceration, and a peripheral pale halo. They appear in head and neck, including the airway, behind the ear, or on the scalp. Vascular Malformations Vascular malformations result from abnormal embryonic development. Slow-flow vascular malformations may cause bony deformation and fast-flow lesions may cause osteolysis. Venous Malformations Venous malformations are the most common vascular anomaly and result from abnormal venous development. They consist of thin walled, dilated channels with normal endothelium but deficient in smooth muscle. They generally arise under skin, but can also be present in other tissues and organs. Presentation Venous malformations are typically bluepurple in color but this depends on the depth of the lesion and the degree of expansion of the affected vessels. More superficial lesions are darker in color, often maroon red, while deeper lesions are bluish. If the child cries or lies down, the lesion expands and the color can become intense. Generally, the indications for intervention are lesions causing pain, creating deformity, producing gastrointestinal bleeding, affecting vision, or obstructing vital structure. Sclerotherapy: the infiltration of substances such as absolute alcohol, 3% sodium tetradecyl sulfate, and bleomycin, can cause shrinkage in 7590% lesions. Surgical resection: It may be indicated to improve contour and function or as primary treatment in small lesions that are not amenable to sclerotherapy due to their position such as the eye. Management involves selective embolization, sclerotherapy, surgical resection, and reconstruction. Embolization is never curative but may allow temporary control and is useful preoperatively to reduce blood loss. They occur in 1 in 2,0004,000 live births and are most commonly isolated lymphatic lesions but may combine with arterial or venous vasculature to form a mixed lymphovascular lesion. Cystic lymphatic malformations are said to be benign in growth but their infiltrative growth pattern causes significant impact on surrounding tissues. They are described as microcystic or macrocystic (or combined) depending on the size of the malformed channels. Arteriovenous Malformation Arteriovenous malformations result from abnormal communication between arteries and veins without the normal capillary bed. Progression is indicated by the onset of pain, pruritus, or enlargement and they may undergo rapid expansion following trauma (including attempted ligation) or during puberty. Clinical progression proceeds from quiescence, through expansion, destruction, and decompensation as described by the Schobinger staging system. Magnetic resonance imaging shows dilated feeding arteries and draining veins with flow voids. Presentation Cystic lymphatic malformations present as a soft, compressible cystic mass, which transilluminate and may be small or extensive. They may occur anywhere in the body but commonly arise in the head and neck region, where they involve the neck, tongue, cheek, and cervicofacial region. Two-thirds of children with cervicofacial lymphatic malformations require a tracheostomy for airway maintenance. Good oral hygiene should be maintained to prevent infection and long-term antibiotics considered in patients with greater than three infections in a year. Small lesions may be observed, but those encroaching on vital structures, causing deformity or pain, require treatment. As many of these lesions seem to expand significantly with localized infections, children with adenotonsillar infections may require surgical ablation of these areas. It arises from undifferentiated mesenchymal tissue with potential for malignant skeletal myogenesis and is broadly divided into embryonal and alveolar varieties. It has bimodal presentations with peaks in incidence between the ages of 2 and 4 years, and 12 and 16 years. Thirty-five percent childhood rhabdomyosarcomas occur in the head and neck region. These are typically embryonal and comprise 13% of pediatric head and neck malignancies. Seventy-five percent head and neck rhabdomyosarcomas occur in the orbit or parameningeal areas and the remainders are collectively named nonorbital nonparameningeal tumors. Embryonal rhabdomyosarcomas are further subdivided into botryoid and spindle cell types and are the most common form in the head and neck region. They occur slightly more frequently in males and have a better prognosis than alveolar, which is typically found in extremities. Like other soft tissue sarcomas, imaging findings in rhabdomyosarcoma may be nonspecific. Sclerotherapy is the mainstay of treatment for large macrocystic or mixed lesions. Injection of a sclerosing agent such as ethanol, bleomycin, or doxycycline after aspiration, induces scarring of the cyst wall and shrinkage of the lesion. Recent literature has suggested a role for sirolimus in several cases of lymphatic malformations to stabilize and induce involution of these lesions while undergoing sclerotherapy. Surgery is indicated for small isolated lesions and in lesions resistant to sclerotherapy. Biopsy is required to confirm the diagnosis; for small discrete lesions, this can be done either by needle aspiration, incisional or excisional biopsy. Tumors can be further subtyped for prognostic information using immunohistochemistry and cytogenetics. Traditionally, rhabdomyosarcomas were treated surgically with relatively poor prognosis. The development of multiagent chemotherapy regimens has improved survival significantly. Patient have two or more of: · Two or more neurofibromas of any type, or one or more plexiform neurofibromas · Freckling of the groin or axilla · Six or more café-au-lait spots (>0. Neurofibromatosis type 1 is an autosomal dominant disorder but up to 50% cases may be due to spontaneous mutation of a tumor suppressor gene on chromosome 17. It occurs with an incidence of one in 4,000 and is diagnosed when two of nine criteria are met (Table 36. Histologically, neurofibromas were considered peripheral nerve sheath tumors characterized by an increase in endoneural matrix and proliferation of Schwann cells. Cutaneous lesions are uncommon in children and generally do not appear until adolescence. Chapter 36: Neck Lump(s) Selective tumor excision or debulking is the mainstay of treatment as cure is not possible. Adjuvant chemotherapy may be considered in large lesions but no protocols have demonstrated significant benefit thus far. Neurofibromatosis type-2 is less common and generally presents with central nervous system neurofibromas.
B (S&F ch35) Biliary complications occur in about 25% of liver transplant patients and include bile leaks and strictures gastritis symptoms after eating order maxolon 10mg amex. These can be treated with endoscopic therapy if a duct-to-duct anastomosis present gastritis diet ������ buy generic maxolon 10 mg online. If a choledochojejunostomy is present gastritis chronic erosive generic maxolon 10 mg on-line, percutaneous or surgical therapy is indicated gastritis diet 7 up calories buy maxolon 10 mg overnight delivery. Currently gastritis healing buy maxolon with paypal, recurrence of hepatitis C occurs in most liver allografts and progresses to cirrhosis within 5 years. Invasive fungal infections occur more commonly in liver transplant patients compared to other solid organ transplants, particularly when antifungal prophylaxis is not given and the mortality is high. If there are two equally matched c donors available, the uninfected donor would be best. Treatment of chronic hepatitis B with entecavir or tenofovir in the donor is indicated to prevent passage of the virus. The patient does not complain of dysphagia, and therefore, an esophageal stricture is less likely. Recurrences occur in 50% of patients after surgery, usually at the anastomotic site. C (S&F ch36) Progressive systemic sclerosis mainly affects the smooth muscle in the lower two thirds of the esophagus. These abnormalities may be seen in other diseases as well, such as amyloidosis, diabetes, chronic alcoholism, esophageal candidiasis, severe reflux, hypothyroidism, or other connective tissue diseases. Abnormally low pharyngeal contraction and upper esophageal sphincter pressure is suggestive of polymyositis. Simultaneous contractions throughout the esophagus are seen in diffuse esophageal spasm. C (S&F ch36) Cholelithiasis occurs in 70% of sickle cell patients and is due to pigmented stones from elevated bilirubin excretion due to chronic hemolysis. Delayed gastric emptying is not likely in this patient, and therefore, a gastric emptying study is not indicated. The treatment for this is aimed at reducing mast cell degranulation and controlling pathologic mast cell infiltration, by the use of H1 and/or H2 receptor antagonists, oral disodium cromoglycate, or glucocorticoids. Delayed gastric emptying is not characteristic of this disorder, and therefore, metoclopramide would not be helpful. Although there are eosinophils present in the biopsy specimens, the presence of mast cells are not typical for eosinophilic gastroenteritis. C (S&F ch36) this case is most consistent with hepatic dysfunction due to sepsis, which usually occurs within a few days after 74 Topics Involving Multiple Organs the onset of bacteremia. Bilirubin levels are mostly direct and typically peak between 5 mg/dL and 10 mg/dL. The picture is not consistent with choledocholithiasis or acute cholecystitis, as neither are suggested by the ultrasound imaging. The serum aminotransferases are typically significantly elevated in ischemic hepatitis. Biopsy of the lesion is not recommended as the pathology is usually nonspecific and there is a risk of bleeding. Angiography is the next best step in localizing the source and treating the bleeding. Capsule endoscopy would be helpful if bleeding is suspected to be in the small bowel. A right hemicolectomy would be reserved for instances in which the angioectasia is identified and a colonoscopy and angiography are unsuccessful or cannot be performed. Thalidomide, which has antiangiogenic effects, may be helpful, but it is not the next best step in management. Caput medusae (distended epigastric veins) and aphthous ulcers are not manifestations of this disease. C (S&F ch37) Therapy with a nonselective -blocker, such as propranolol, confers a lower rebleeding rate at 12 months in patients with bleeding from portal hypertensive gastropathy. If the lesion is identified, it should be marked with tattoo to easily identify it in the case that it rebleeds. Therapeutic techniques include injection therapy, heater probe, band ligation and hemoclip. Endoscopic bleeding can usually be achieved by use of multiple modalities; however, in a small subset of cases, surgery is required to control bleeding. Fistulas can occur when abdominal aortic aneurysm repairs are performed and usually occur in the third or fourth portions of the duodenum. Celiac disease, chronic pancreatitis, and small bowel bacterial overgrowth may present with diarrhea and signs of malabsorption, but the other clinical symptoms are not consistent with these diseases. Sarcoidosis may have some overlapping symptoms but overall is not consistent with the above scenario. C (S&F ch36) the clinical scenario suggests lupus vasculitis, which typically affects medium to small arteries, with the jejunum and ileum being the most commonly involved segments of the bowel. Glucocorticoids are usually effective, although cyclophosphamide may be used in more severe cases. The presentation of lupus vasculitis can range from mild symptoms to an acute abdomen. Complications include ischemia, infarction, stricture formation, bleeding, and perforation. C (S&F ch36) this case is consistent with neutropenic enterocolitis or typhlitis, which is a necrotizing process involving the terminal ileum, cecum, and ascending colon. Ischemic colitis is possible but less likely, given the location of the colon involvement. Acute appendicitis is also possible, but there is no comment on the appearance of the appendix in the imaging exam and, given the clinical history, neutropenic enterocolitis is more likely. When sepsis is present in this disease process, gram-negative bacteria are the most frequently identified pathogens. Management includes intravenous fluids, transfusion of blood and platelets, granulocyte colony-stimulating factors, and broad-spectrum antibiotics. E (S&F ch37) Observation is best in this case, as the patient is asymptomatic with very low risk of bleeding. A tagged red blood cell scan would not be as helpful in establishing the diagnosis and could delay it. C (S&F ch37) the clinical scenario describes that of superior mesenteric artery syndrome, which occurs with compression of the duodenum due to a narrowing of the wall of the aorta and the superior mesenteric artery to less than 25 degrees. Superior mesenteric artery syndrome has been associated with marked rapid weight loss in adults, rapid growth in children, and full body casts with immobilization. B (S&F ch37) Klippel-Trenaunay syndrome is composed of a vascular nevus of the lower limb, varicose veins only on the affected side, hypertrophy of the tissues of the affected limb, and a variety of vascular lesions. Endoscopic therapy with thermal ablation can be helpful when lesions are localized. Diffuse intestinal hemangiomatosis is defined by numerous cavernous type lesions, which affect the stomach, small bowel and colon, as well as skin and soft tissues of the head and neck. Osler-Weber-Rendu (hereditary hemorrhagic telangiectasia) is characterized by telangiectasias of the skin and mucous membranes and does not have orthopedic abnormalities present. C (S&F ch37) the clinical presentation combined with a pulsatile mass in the abdomen is consistent with a ruptured abdominal aortic aneurysm. Pancreatic edema and stranding suggests pancreatitis, which is not likely based on the normal lipase. Small bowel protruding through an abdominal wall defect is suggestive of an incarcerated abdominal wall hernia, which was not detected on physical exam in this patient. Initial treatment includes argon plasma coagulation, with antrectomy reserved for severe refractory cases. C (S&F ch38) Pseudomyxoma peritonei is a clinical condition in which cancerous cells (mucinous adenocarcinoma) produce abundant mucin or gelatinous ascites. Liver, kidney, uterus, and cervical cancer are not associated with pseudomyxoma peritonei. The unicentric form of the disease usually involves the central lymph node of the mediastinum or mesentery. A (S&F ch38) Retroperitoneal fibrosis is more common in men and usually presents as a retroperitoneal mass. Mesentric cysts are typically large and fluid filled and can be treated with excision of the cyst. It can develop during pregnancy or estrogen therapy and regress by hormone withdrawal. A (S&F ch38) Staphylococcus epidermidis contamination of the indwelling catheter is the most common etiology for peritonitis in patients receiving peritoneal dialysis. Other choices, including Pseudomonas, fungal infection, Mycobacterium tuberculosis, and E. D (S&F ch38) Chlamydia peritonitis can present with fever, abdominal pain, and abdominal distention with presence of ascites. Laparoscopic evaluation is often needed to establish the diagnosis by specific findings of perihepatic adhesions, also called "violin slings" or "bridal veil" adhesions that extend from abdominal wall to liver. However, a history of pelvic inflammatory disease and characteristic findings during laparoscopy does not favor the diagnosis of this condition. Starch peritonitis has been described in the past and develops secondary to irritation from glove powder. This condition is unlikely to develop in a patient with no history of recent laparotomy. E (S&F ch39) Pregnancy is associated with an alteration in bile composition and increased size of the bile acid pool, which would lead to greater residual gallbladder volumes. Progesterone has a direct inhibitory effect on gut smooth muscles, leading to slow motility and prolonged intestinal transit time. Breast-feeding by mothers with chronic hepatitis B does not impose any additional risk of viral transmission as long as the baby has had appropriate immunoprophylaxis. Treatment with tenofovir in the third trimester of pregnancy is safe and effective in preventing vertical hepatitis B viral transmission. Phenothiazines and vitamin B6 have been shown to reduce symptoms in those who failed initial pharmacotherapy. D (S&F ch39) Methotrexate is a class X medication and could be used with caution in patients during childbearing age. The optimum period to abstain from this medication before conception is unknown, but a minimum of 6 months is recommended. Evidence regarding human use of azathioprine and its metabolites has failed to show teratogenicity seen in animal studies. This can differentiate between peritoneal carcinomatosis and tuberculosis peritonitis. Cytology will be positive in more than 90% of the cases of peritoneal carcinomatosis. Secondary bacterial peritonitis usually is polymicrobial and is associated with high neutrophil counts in ascites fluid. Zinc salt does not appear to be teratogenic, and some experts favor its use during pregnancy. Intrahepatic cholestasis of pregnancy usually presents with mild jaundice (bilirubin <5 mg/dL) and elevated serum bile acids. Liver biopsy shows microvesicular fatty infiltration of the liver that is most prominent in hepatocytes surrounding central veins. Most affected women recover completely with supportive care and delivery, and they do not need liver transplantation. Laboratory blood work may show evidence of increased serum aminotransferase levels, fragmented red blood cells on blood smears, as well as decreased platelet counts. Abdominal imaging may be helpful in making the diagnosis by showing evidence of intrahepatic hemorrhage and infarction. This condition should be suspected in a pregnant patient who present with abdominal pain, distension, and cardiovascular collapse. Other options are not associated with spontaneous hepatic rupture during pregnancy. C (S&F ch39) Progesterone directly inhibits gut smooth muscles and results in slower motility. Maternal alkaline phosphatase levels are normally elevated during the third trimester, largely due to placental production. C (S&F ch40) Radiation enteritis could result in fibrosis and narrowing of the intestinal lumen due to stricture formation. Small intestinal bacterial overgrowth can be seen in patients who underwent radiation as a result of dilated loops and stasis proximal to stricture. A trial of antibiotics is recommended to treat small intestinal bacterial overgrowth and to control diarrhea. Hyperbaric oxygen therapy and subcutaneous octreotide therapy may reduce risk of acute and chronic radiation enteritis. Antidiarrheal agents and a low residue diet will help to control symptoms of diarrhea but will not help with treating the underlying etiology of diarrhea. D (S&F ch40) Combining chemotherapy with radiation increases the risk of radiation-induced injury. Other risk factors include thin patients (possibly due to the larger amount of bowel in the pelvis); vasculopathy in patients with comorbid conditions, such as history of diabetes, peripheral vascular disease, hypertension, and cardiovascular disease; as well as a history of collagen vascular disease. Radiation treatment in the prone position with external compression is associated with less toxicity possibly due to exclusion of small bowel from the radiation field. Additionally, radiation dose and volume of the bowel exposed to radiation are important determinants of the severity of radiation-induced toxicity. D (S&F ch40) this patient has radiation colitis with telangiectasias noted on endoscopy. Coagulation techniques, such as argon plasma coagulation, are useful for the treatment of bleeding secondary to radiationinduced colorectal ulcerations. Glucocorticoid suppositories can be helpful for radiation proctitis and can be considered for longterm management.
Cheap maxolon 10 mg line. Top 20 Foods To Avoid For Gastritis.
References
- Chowdhury T, Mendelowith D, Golanov E et al. Trigeminocardiac reflex: The current clinical and physiologic knowledge. J Neurosurg Anesthesiol 2015;27(2):136-147.
- Dauerman HL. The early days after ST-segment elevation acute myocardial infarction: reconsidering the delayed invasive approach. J Am Coll Cardiol. 2003;42:420-423.
- Joshi, H.B., Okeke, A., Newns, N. et al. Characterization of urinary symptoms in patients with ureteral stents. Urology 2002;59:511-516.
- Gupta NP, Singh P, Nayyar R: Outcomes of robot-assisted radical prostatectomy in men with previous transurethral resection of prostate, BJU Int 108(9):1501n1505, 2011.
- Shoskes, D. A. (2003). Treatment response to conventional and novel therapies in chronic prostatitis. Current Urology Reports, 4(4), 311n315.
- Van der Ven LT, Roholl PJ, Gloudemans T, et al. Expression of insulin-like growth factors (IGFs), their receptors and IGF binding protein-3 in normal, benign and malignant smooth muscle tissues. Br J Cancer 1997;75(11):1631-40.