
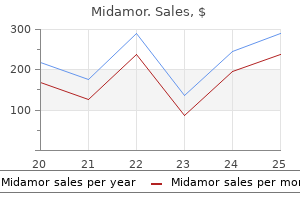
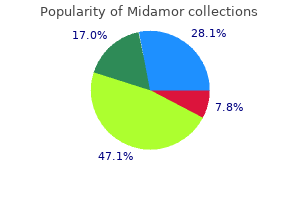
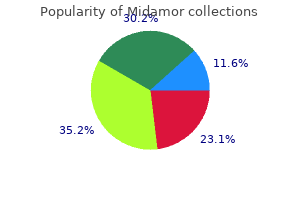
Midamor
| Contato
Página Inicial
Ali Mahtabifard, MD
- Attending Surgeon
- Cedars-Sinai Center for Chest Diseases
- Associate Director, Thoracic Surgery
- Residency Program
- Cedars-Sinai Medical Center
- Los Angeles, California
The endometrium from now on may be referred to as decidua blood pressure solution scam midamor 45 mg buy overnight delivery, which provides the breeding ground for the growing embryo and the developing placenta blood pressure chart 19 year old purchase 45 mg midamor. Once the blastocyst has completely penetrated the decidua blood pressure levels low purchase midamor toronto, the mass of syncytiotrophoblast rapidly increases by ongoing proliferation and fusion of underlying cytotrophoblasts heart attack move me stranger discount 45 mg midamor fast delivery. The syncytiotrophoblast forms a complete layer over the surface of the blastocyst pulse pressure method 45 mg midamor mastercard, whereas the site at the implantation pole achieves considerable thickness and develops extensions that deeply invade the decidua. After implantation, primary placental villi, composed of a cytotrophoblast core with a covering of syncytiotrophoblast, are being developed (10). At the distal ends of the developing villi, cytotrophoblasts penetrate the syncytiotrophoblast and form cell columns, which attach the developing placenta to the decidua. With disaggregation of trophoblast plugs at the end of the first trimester, maternal blood flow is initiated into the intervillous space. Recent microanatomical surveys on first trimester decidua basalis sections challenged this doctrine and extended the current view by showing extravillous trophoblast subpopulations in several luminal structures, including uterine spiral arteries, veins, glands, and to a minor extent, uterine lymphatic vessels (1012). While the functional significance for invasion into lymphatic vessels remains unclear, arteries, veins, and glands have to be connected to the intervillous space to guarantee successful placentation. However, the type of invasion into arteries may differ compared to invasion into uterine veins and glands. According to a recent opinion, uterine veins and glands are invaded to be connected to the intervillous space of the placenta without a massive remodeling of their vessel walls (13). In normal pregnancy, trophoblast invasion into the maternal decidua gives rise to conversion of distal segments of spiral arteries into widened conduits (a) Aberrant trophoblast invasion and inadequate spiral artery remodeling, with absence of any dilation at the distal ends of the arteries, leads to high-speed jets that enter the intervillous space (b). While these high-speed jets can nowadays be visualized reliably using pulsed-wave Doppler ultrasonography, computational models of blood flow from spiral artery openings suggest that jets of flow observed by ultrasound are likely correlated with increased porosity of the intervillous space near the opening of the spiral arteries (15). Accordingly, mega-jets, which penetrate more than half the placental thickness, may only be possible when spiral arteries open to regions of the placenta with very sparse villous structures (15). This assumption further suggests that the velocity of the incoming blood flow from converted spiral arteries influences development and architecture of villous trees. The turbulent blood flow, including high-velocity jets and vortices combined with elevated blood pressure in the proximal intervillous space may contribute to an increased wall shear stress at the villous surface. Histological examinations revealed potential villous damage, which appeared as cytokeratinpositive particles in the intervillous space, but in a more pronounced way in veins of intercotyledonary septa that drain the intervillous space (16). Inadequate spiral artery remodeling may be the result of both shallow invasion and a reduced number of invaded trophoblasts. This assumption is based on numerous histological surveys on hysterectomy and postmortem specimens of uteri with in situ placentas as well as placental bed biopsies, consisting of both decidual and myometrial tissue. Among such studies, severely impaired trophoblast invasion has been shown in fullthickness uterine wall samples obtained from early onset preeclamptic pregnancies combined with intrauterine growth restriction (17). A plethora of soluble factors, including cytokines, chemokines, and growth factors, is secreted from decidual macrophages and stromal cells, as well as uterine natural killer cells and even uterine glandular epithelial cells. Moreover, these factors could regulate recruitment of macrophages and natural killer cells as well as other less abundant immune cells into the placental bed. At the same time, decidual stroma cells are suggested to secrete some anti-invasive factors that might be essential to counteract the effects 14 Great obstetrical syndromes of invasion-promoting factors and restrain exaggerated invasion. Beside high-velocity jets, fluctuations in placental oxygen concentrations resulting from intermittent perfusion of the intervillous space are currently discussed as a consequence of inadequate spiral artery remodeling (22). While fluctuations in intervillous blood flow can be explained by periodic vasoconstriction of spiral arteries that might even occur during normal human pregnancies, it seems reasonable that such events occur more frequently and more pronounced in placental beds with less remodeled spiral arteries, due to the preservation of smooth muscle within their distal ends. The consequence of such fluctuations may be a decreased oxygen tension within the affected area, which probably could not be compensated by supply from adjacent spiral arteries. However, when vasoconstriction of spiral arteries declines, inflow in the intervillous space is restored, and the local oxygen tension steeply rises. Importantly, such fluctuations in oxygen tension are associated with an ischemia-reperfusion type of injury, which is well documented for other organs such as heart and brain (22). In normal pregnancies, this is accompanied by an increase in fasting insulin levels rising between weeks 25 and 33 of pregnancy (24), a result of structural, i. If the degree of insulin resistance exceeds ß-cell capacity to mount adequate responses, i. In many instances, the ß-cell defect is already present before pregnancy (28), and pregnancy only unmasks this defect. In obese women, a considerable proportion (23%) is already insulin resistant around week 15 of pregnancy (30). This requires ß-cell adaptation beyond that of a pregnancy that begins without insulin resistance. Both insulin resistance and ß-cell adaptation in pregnancy are, among others, determined by placental hormones (31). Many of the studies have been conducted in rodent models and may have limited validity for humans because of distinct species differences in islets and ß-cells (33) as well as in lactogenic hormones and their receptors (34). Evidence in humans is less convincing, but recent studies using human material have also supported the role of placental peptides and hormones to facilitate islet and ß-cell adaptation to pregnancy (32,35,36). Placental lactogen was among the first candidate regulators of islet adaptation in pregnancy (37). Several placental hormones and peptides are involved in establishing physiologic maternal insulin resistance and pancreatic changes characteristic of the catabolic phase in the second half of pregnancy. Leptin transcriptionally represses insulin in human pancreatic islets outside pregnancy (40). Although its main function is to regulate appetite/ satiety, leptin may also contribute to reducing pancreatic synthesis of insulin, although ß-cell leptin resistance has been proposed. Hepatocyte growth factor is a cytokine produced by the human placenta in both trophoblast and endothelial compartments (47). Its higher placental levels in obesity (48) may have a positive effect on islet development, regeneration, and ß-cell expansion, on which its signaling receptor is located. Outside pregnancy, kisspeptin is a hypothalamic peptide and increases glucose-stimulated insulin secretion (49). During pregnancy, its circulating levels increase by 1000-fold, likely because of placental production (50,51). Placental peptides and hormones not only affect the maternal pancreas but have also been implicated in the physiological changes of insulin resistance. The pituitary is the prominent site of growth hormone production outside pregnancy. There may be several reasons for the discrepancy between in vitro effects of single hormones and the results of clinical studies: (1) conditions and designs of the in vitro experiments do not reflect the in vivo situation; (2) in vivo effects comprise the whole endocrine/paracrine system, and effects of each hormone may not be additive, but competitive; and (3) pancreatic function is already impaired before pregnancy and cannot be adequately changed for the benefit of maintaining homeostasis within pregnancy. If this were correct, then any derangement of maternal glucose homeostasis early in pregnancy may have consequences for fetal growth and development through the fetal glucose steal phenomenon (63). The early pregnancy period is also a key period for placental development (compare also the previous and [64]). Any alteration in trophoblast and placental growth as well as cellular differentiation may track until the end of pregnancy and contribute to excess neonatal adiposity (65,66). It is pertinent that in early pregnancy, maternal insulin may have a stimulatory role on placental growth (66), but this will be an indirect rather than a direct effect (67). At this time of gestation, placental insulin receptors are mainly located on the microvillous membrane of the syncytiotrophoblast exposing it to maternal insulin, whereas the proliferating cytotrophoblast is located subjacent to the syncytiotrophoblast and expresses very few, if any, insulin receptors. As gestation advances, the insulin receptor location shifts to become more prominent on the fetoplacental endothelium (68). This endothelium responds not only to insulin but also to other fetal signals that in their totality serve to facilitate placental adaptation to protect fetal development. Other examples of fetal signals are oxysterols, which result from oxidative cholesterol modification (69). The fetal signals for these responses may be generated before week 32 in pregnancy, at least for the often-found placental hypervascularization, as the placental surface area correlates with the day-to-day variation in maternal blood glucose levels only between weeks 12 and 32 of gestation and not thereafter (70). It is not difficult to predict that the first trimester of pregnancy will more and more become the focus of research (77). ReFeRenceS In recent years, immense effort has been put into preeclampsia screening tests, which now are reported to predict the risk of the development of preeclampsia from as early as 11 weeks of gestation. On the basis of an algorithm, which incorporates maternal history, mean arterial blood pressure, uterine artery Doppler pulsatility index, and placental biomarkers, preeclampsia can be detected with 54% and early onset preeclampsia even with 96%, at a false-positive rate of 10% (72,73). While induction of labor and hence removal of the placenta seem to be the only way to treat preeclamptic symptoms at the moment, many trials have been conducted to test the effectiveness of cost-effective drugs such as heparin, vitamin D, or aspirin. Low-dose aspirin (<150 mg), when commenced once daily after the first trimester, has been shown to reduce the risk of preeclampsia and fetal growth restriction by 24% and 20%, respectively, when given to women who are at risk of preeclampsia (74). Based on such data, the administration of low-dose aspirin has now been recommended for women with one major risk factor or two moderate risk factors for preeclampsia, as per guidelines from the National Institute for Health and Care Excellence, United Kingdom. However, it should be emphasized at this point that neither the detailed pathologic mechanisms behind preeclampsia, nor the particular mode of action of such drugs in preventing (rather than treating) preeclampsia are fully understood. Thus, further basic as well as applied research is required to decipher the etiology of different subtypes of preeclampsia. In vitro studies are hampered by difficulties in obtaining human tissue samples, whereas clinical studies are confounded by multiple factors that cannot be controlled for. Moreover, they also struggle with segregating the distinct roles of each hormone and peptide with their often overlapping functions, as well as with separating maternal and placental contributions, as both are sources of most hormones. It is unclear if they are significant placental signals for maternal metabolic homeostasis. Both conditions have been related to an increased risk of perinatal morbidity and mortality (2,57) and long-term health consequences (810). Actually, there are no universally accepted criteria for the diagnosis of abnormal fetal growth (1,11). However, this approach misclassifies a large proportion of fetuses as it does not distinguish between those fetuses that are constitutionally large or small from those with a pathologic growth pattern. Moreover, there is not a single cut-off that acts as an absolute distinguisher between high and low risk for adverse perinatal outcome (2). Nonetheless, despite its methodological limitations, dichotomization of fetal weight has proved useful to define groups at higher risk, and it is the current standard in prenatal care in most clinical scenarios. Yet, there is a trend to accept that future gold-standard definitions of abnormal fetal growth should incorporate other functional parameters, such as fetal Doppler or growth velocity (14). It prompts further investigations, such as umbilical artery Doppler study, which has been shown to reduce stillbirth and increase preterm delivery without increasing neonatal mortality (22). It also alerts clinician and mother about the increased risk involved, enabling deliberations on the optimal timing of delivery. Small fetuses and newborns have poorer perinatal outcome, including a higher risk of intrauterine fetal death. Most of these cases correspond to "constitutional" healthy fetuses that merely represent the end of the spectrum of healthy babies. This condition is associated with deficient placental function, worse perinatal outcome, and higher rates of long-term cardiovascular and metabolic diseases (1517). Fetal macrosomia, commonly defined as birth weight >4000 g (1,23), is also present in more than 10% of gestations (3), and it is associated with several delivery complications including birth trauma, shoulder dystocia, and perinatal asphyxia (3,24). While this could lead to an increase in sensitivity, it also could be associated with a lower specificity and an increase in false-positive rates. Regarding management, once fetal macrosomia is suspected, an elective cesarean section can be done to avoid complications related to vaginal delivery. However, the number of interventions needed to prevent one complication makes this approach clinically and economically unsound (27). Recently, induction of labor for impending macrosomia has been proposed to prevent complications, without increasing the cesarean section and instrumental delivery rates (23). This has put the spotlight on improving prediction of excessive fetal weight or macrosomia before labor onset for proper counseling and decision-making. As gestation advances, the capacity of the uteroplacental system to meet fetal demands gradually declines (28); in early stages, this dysfunction could not be enough to be reflected by Doppler parameters (29,30). On the other side, maternal nutritional and metabolic status has also been shown to have direct influences in placental function and pregnancy outcome (32). Higher rates of macrosomia and adverse perinatal outcomes have been described in obese patients (33). It has been argued that a cross-sectional assessment of estimated fetal weight would be unable to capture the behavior of the fetal-maternal dynamic, rendering a poor performance to current screening strategies. It has been proposed to incorporate the estimation of fetal growth velocity in prenatal care as this would better reflect the evolution of this relation (19,35,36). Yet, if growth velocity adds additional information over knowing fetal size alone, it is still a matter of research (3740). Nonetheless, despite implementation of multiple 20 Normal and abnormal fetal growth strategies and wide availability of ultrasound, detection rates remain low. On the other side, a systematic review and meta-analysis published by Coomarasamy et al. However, it could be argued that this conclusion is based on studies from almost 20 years ago, when expertise and technology were not valid in contemporary practice. Furthermore, many of the studies involved no change in management if a diagnosis of abnormal fetal growth was made, which again does not reflect current practice. Finally, almost 12% of the pregnancies were scanned before 34 weeks, when the diagnostic performance is poorer (45). More recently, a large prospective study (35) was published involving 3,977 nulliparous women, in which serial scanning was performed at 28, 32, and 36 weeks, and the results were concealed to participants and treating clinicians. On the other side, induction of labor for suspected fetal macrosomia results in a lower birth weight and fewer birth A longitudinal approach has been proposed to be more appropriate because the progressive and dynamic nature of the condition is likely to be more amenable to be detected by serial assessments than by cross-sectional evaluation (49). To date, few studies have evaluated in the general population whether longitudinal assessment improves the identification of fetuses at risk for late-onset growth abnormalities and their related morbidity (5054), reporting conflicting results. More recently, two studies conducted by our group focused on the performance of longitudinal growth assessment for the prediction of abnormal fetal growth in the general population. Besides methodological issues, biologically, it could be speculated that although it seems intuitive that longitudinal assessment is more suitable to capture the dynamic nature of growth problems, what really determines the performance in predicting birth weight is the size achieved by the fetuses at term. Indeed, for clinically based outcomes (such as longterm cardiac [5557] and neurological [5862] outcomes or metabolic syndrome in childhood, linked to neonatal catch-up growth [63] and fetal overgrowth [10,64]) perhaps longitudinal growth assessment rather than size would have better performance. It is known that the use of fetal versus neonatal curves allows the association between growth restriction and neonatal complications (66) to emerge clearly, as well as the association with longterm neurological sequelae (67).
You and your partner are quickly escorted to a large office in the rear blood pressure below 100 purchase 45 mg midamor with amex, where you find the patient blood pressure normal lying down midamor 45 mg purchase overnight delivery. A coworker of the patient tells you that he looks terrible and is reporting chest pain blood pressure of 10060 purchase 45 mg midamor visa. Upon additional questioning by your partner blood pressure after eating cheap midamor 45 mg amex, she admits that she and the patient were doing cocaine before the patient exhibited these symptoms heart attack karaoke 45 mg midamor purchase otc. The patient has no motor or sensory deficits, but his pupils are 8 mm and reactive to light. Management Intoxication with cocaine results in an adrenergic response, with the resultant clinical findings of tachycardia, hypertension, dilated pupils, hyperthermia, and agitation. The initial treatment for the agitation includes the use of benzodiazepines such as diazepam (Valium), midazolam (Versed), or lorazepam (Ativan). Haloperidol (Haldol) is the second-line drug used in patients who do not respond to the benzodiazepines or who are psychotic. Cocaine can produce serious cardiovascular complications such as tachycardia, hypertension, chest pain, and myocardial ischemia. Up to this point the treatment for cocaine intoxication is similar to therapy for amphetamine use. You place him on supplemental oxygen and provide three doses of sublingual nitroglycerin and one aspirin. Despite these drug interventions, the patient still reports chest pain that rates as a 7 on a scale of 1 to 10. Because the chest pain seen with cocaine intoxication is often ischemic in nature, the drug therapy used in other forms of chest pain is indicated-administration of nitroglycerin. Adverse Effects: Headache, hypotension, bradycardia, lightheadedness, flushing, cardiovascular collapse, methemoglobinemia. Contraindications: Hypotension, severe bradycardia or tachycardia, rightsided myocardial infarction, increased intracranial pressure, intracranial bleeding, patients taking any medications for erectile dysfunction (such as sildenafil [Viagra], tadalafil [Cialis], or vardenafil [Levitra]), known sensitivity to nitrates. Use with caution in anemia, closed-angle glaucoma, hypotension, postural hypotension, uncorrected hypovolemia. Platelets are formed elements of the blood that, when activated, are responsible for the formation of small plugs that seal blood vessels, such as in the case of a laceration. In the case of ischemic chest pain, the activated platelets form small plugs that occlude the flow of blood vessels in the heart. The spasm of the coronary arteries and occlusion with platelet plugs result in the heart muscle not receiving the critical amount of oxygen. Administering aspirin inhibits the enzyme cyclooxygenase and impairs platelet function for the life of the platelet, which is 7 days. Phentolamine is an alpha adrenergic blocker aimed at reducing systemic blood pressure and vasoconstriction of the coronary arteries. When the patient is given phentolamine, the drug binds to the alpha receptor, preventing the cocaine molecule from producing its clinical effects of vasoconstriction and hypertension. Alpha receptors do not produce an increase in heart rate (chronotropy) or forcefulness of heart contraction (inotropy). Hypertension from cocaine should not be treated with beta blockers because they can exacerbate the coronary artery vasoconstriction and result in an increased chance of death. The best method of stopping these seizures is administrating a benzodiazepine, such as diazepam, followed by a loading dose of phenytoin. Action: Prevents the formation of a chemical known as thromboxane A2, which causes platelets to clump together, or aggregate, and form plugs that cause obstruction or constriction of small coronary arteries. In the management of angina, morphine reduces stimulation of the sympathetic nervous system caused by pain and anxiety. You arrive to find a 23-year-old man who is well-known to the police as a heroin abuser. His blood pressure is 72/52 mm Hg, heart rate is 112 beats/min, and respirations are 12 breaths/min and very shallow. His upper extremities have multiple needle tracks, as well as small, circular scars that appear to be from previous skin abscesses. As you roll the patient to inspect his back, you find a bag that contains drug paraphernalia, needles, and a substance that looks like heroin. Overdose can occur with any type of opiate use, in either medical or abuse settings. Heroin, a common drug of abuse and overdose, is classified as an opiate and is responsible for the majority of opiaterelated overdoses. Overdose typically occurs with heroin use because the quantity of heroin in any given sample can vary greatly. Heroin is also more soluble in fat, allowing the drug to reach higher levels in the system more rapidly than other forms of opiates. Patients with an opiate/narcotic overdose typically have a depressed level of consciousness, hypotension, and respiratory depression. Management Naloxone (Narcan), a drug known as a competitive antagonist, binds to the opiate receptor to prevent the opiate from exerting its effects of altered mental status, hypotension, and respiratory depression. Naloxone should be administered in a dose or manner that is appropriate for the situation. Too much naloxone may cause a violent narcotic withdrawal syndrome, with agitation, restlessness, vomiting, and other related signs and symptoms. Certain synthetic opioids or potent illicit opioid compounds may require higher doses, repeated administration, or continuous infusions of naloxone to keep the patient breathing. In many multidrug overdose or poisoning situations, it may be advisable to allow opioid effects to predominate, rather than reversing with naloxone. You assess the patient, who tells you that he is a farmer and was feeling great until he worked the fields that afternoon. Shortly after loading the fertilizer spreader, he began to have nausea, vomiting, and profuse sweating. Organophosphates are a class of chemicals found in insecticides and fertilizers and are common in agricultural environments. This class of chemicals can gain access to the body through inhalation, ingestion, and absorption through the skin. Each year, more than 300,000 people globally are poisoned and die from exposure to organophosphates. Under normal conditions, acetylcholinesterase breaks down and deactivates the neurotransmitter acetylcholine. Without acetylcholinesterase present to break it down, acetylcholine builds up and causes overstimulation of the parasympathetic nervous system. Overstimulation of the parasympathetic nervous system results in both muscarinic and nicotinic effects. The most dangerous manifestations of organophosphate poisoning are excessive respiratory secretions (bronchorrhea), bronchospasm, and respiratory insufficiency. Of critical importance is that, if intubation is performed, the rapid depolarizing agent succinylcholine (Anectine) should not be used because it cannot be broken down and can result in prolonged paralysis of the patient. The most dangerous manifestations of organophosphate poisoning are respiratory complications. However, the patient remains tachycardic, with a heart rate of 140 beats/min and blood pressure of 184/105 mm Hg. As demonstrated in this case, atropine reverses the effects of the muscarinic receptors, but the nicotinic effects will persist and the patient will continue to have profound muscle weakness. Adverse Effects: Dizziness, blurred vision, hypertension, diplopia, hyperventilation, laryngospasm, nausea/vomiting, sinus tachycardia. Contraindications: Myasthenia gravis, renal failure, inability to control the airway. After overdose with a cyclic antidepressant, a patient begins to show a wide-complex tachycardia. What is the cardiovascular effect of a too-rapid administration of phenytoin (Dilantin) Why are gastric lavage and activated charcoal not effective in treating a methamphetamine overdose What is the initial drug used for the treatment of agitation in a patient who is intoxicated with cocaine When intubating a victim of organophosphate poisoning, why should you avoid using succinylcholine (Anectine) Rapid emesis from high-dose ipecac syrup in adults and children intoxicated with antiemetics and other drugs. A comparison of ipecac syrup and apomorphine in the immediate treatment of ingestion of poisons. American Academy of Clinical Toxicology; European Association of Poison Centres and Clinical Toxicologists. Position statement and practice guidelines on the use of multidose activated charcoal in the treatment of acute poisoning. Annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Acute beta blocker overdose: factors associated with the development of cardiovascular morbidity. Randomized, double-blind placebo-controlled trial of diazepam, nitroglycerin, or both for 15. A prospective randomized, controlled trial of benzodiazepines and nitroglycerine or nitroglycerine alone on the treatment of cocaine-associated with acute coronary syndromes. Clinical features of patients with acute organophosphate poisoning requiring intensive care. Prolonged succinylcholine-induced paralysis in organophosphate insecticide poisoning. Oximes in organophosphorus pesticide poisoning: a systemic review of clinical trials. Define nasal cannula, rebreather face mask, nonrebreather face mask, and Venturi mask. Demonstrate the proper procedure for administering medication through a metered-dose inhaler. Discuss medications used in the treatment of asthma: albuterol (Proventil, Ventolin), ipratropium bromide (Atrovent), and albuterol/ipratropium (Combivent). Discuss medications used as second-line therapy for acute exacerbation of asthma: dexamethasone (Decadron), methylprednisolone sodium succinate (Solu-Medrol), aminophylline, magnesium sulfate, and racemic epinephrine. Briefly describe the key treatment for patients with chronic obstructive pulmonary disease. Acute respiratory distress affects the young and old, male and female, and people of all ethnicities. Although the underlying pathologic condition causing the respiratory distress may be different, with the exception of acute pulmonary edema most of the prehospital care is aimed at treatment of reversible bronchial constriction, or bronchospasm. Her heart rate is 88 beats/min, blood pressure is 144/92 mm Hg, respiratory rate is 16 breaths/min, and oxygen saturation (SaO2) is 87%. Oxygen Although often overlooked as a drug, oxygen is the most commonly used medication in the prehospital setting. Oxygen is used daily by basic and advanced prehospital providers, sometimes with little consideration to its pharmacologic properties. Oxygen is a colorless and odorless gas stored in either green or aluminum cylinders at a pressure of 1,800 to 2,400 pounds per square inch (psi). As the oxygen passes through the attached regulator, the gas pressure is decreased to a working pressure of 60 psi. The quantity of oxygen delivered to a specific patient can be considered in terms of the concentration of inspired oxygen and flow. The atmosphere consists of 78% nitrogen, 21% oxygen, and a variety of other gases that compose the remaining 1%. The concentration of inspired oxygen is referred to as the fraction of inspired oxygen (FiO2). Because the percentage of oxygen in the atmosphere is 21%, the FiO2 in normal room air is 21%. When a patient has shortness of breath, chest pain, or shock, supplemental oxygen is administered to increase the concentration of oxygen breathed by the patient. Increasing the concentration of inspired oxygen increases the content of oxygen in blood and subsequently the amount of oxygen delivered to the heart and peripheral tissues. Oxygen Delivery Devices Oxygen delivery devices include the nasal cannula and face mask. The basic principle by which these devices work is the creation of a reservoir filled with oxygen-enriched gas. Nasal cannulas and nonrebreather face masks typically are the most commonly used noninvasive devices for delivering oxygen in the prehospital setting. However, patients involved in interfacility transfers may use additional devices, as described in this section. Oxygen flows through two nasal prongs into the oropharynx, which acts as an oxygen reservoir, resulting in an increase in the oxygen concentration. A nasal cannula set with a flow rate of 6 L/min is capable of delivering an oxygen concentration between 35 and 45%. Various oxygen face masks are capable of delivering an oxygen concentration based on the flow rate, reservoir of the mask, presence or absence of a reservoir bag, and side ports in the mask with directional valves. The simple oxygen face mask does not have a reservoir bag or unidirectional side ports. At a flow rate of 6 to 10 L/min, these masks are capable of delivering an FiO2 between 30 and 60%. During inspiration, the patient inhales oxygen in the reservoir, as well as some room air through the side ports. When the patient exhales, some of the expired breath goes back into the reservoir bag, where it is then rebreathed. The valve on the side of the mask prevents inhalation of room air during inspiration. One side of the mask is usually missing the one-way valve as a safety precaution to allow ambient air to enter the mask in the event of the loss of oxygen supply from an empty tank or disconnected tubing.
In the context of an inflamed pouch these worrying appearances were labelled as indefinite for dysplasia rather than as dysplasia arteria latin cheap midamor 45 mg without a prescription. The abnormalities have persisted for more than 15 years blood pressure chart 18 year old 45 mg midamor order otc, suggesting (with hindsight) that they are regenerative rather than dysplastic heart attack coub purchase midamor 45 mg with mastercard. Occasionally blood pressure medication effect on heart rate cheap midamor 45 mg on-line, crypt dysplasia may show high-grade cytological features arrhythmia journal articles cheap midamor online mastercard, including markedly enlarged nuclei with increased nuclear/cytoplasmic ratio, eosinophilic cytoplasm, irregularity of the nuclear membranes, and loss of nuclear polarity. High-grade changes are much less common than in conventional dysplasia, but should not deter pathologists from making the diagnosis of crypt dysplasia. Finally, active inflammation in the lamina propria or within the crypt epithelium in the affected area precludes a diagnosis of crypt dysplasia. Compared to specialists, nonspecialist or general pathologists tend to assign a higher grade of dysplasia. In some reports, it is a more powerful predictor Interobserver Variability Distinction between low-grade and high-grade dysplasia is important, because of the consequences for patient management. The diagnosis of dysplasia depends on assessment of a slide stained with haematoxylin and eosin (H&E). Because dysplasia represents a continuum of changes without defined histological cut-off points, the distinctions between low-grade and high-grade dysplasia are subjective. Variability is especially high for low-grade versus indefinite for dysplasia or reactive, while agreement levels are better for the two extremes of the spectrum, i. Some studies show that restriction of the proliferation marker Ki67 staining to the basal third of crypts excludes a diagnosis of dysplasia. In addition, a diffuse, strong, blocklike positivity for p16 immunohistochemistry may help confirm a diagnosis of high-grade intraepithelial neoplasia (see the section on anal canal neoplasia). Macroscopically, there are flat, polypoid, or depressed forms of gastric dysplasia. This develops in non-metaplastic gastric epithelium and is associated with the subsequent development of poorly differentiated intestinaltype adenocarcinoma. Microscopically, the dysplastic cells are typically cuboidal or low columnar and have clear or eosinophilic cytoplasm, loss of nuclear polarity, and hyperchromatic vesicular nuclei with nucleoli. The low-grade form of this type of dysplasia is difficult to differentiate from regenerative changes. Typically, the cells involve the neck region of the gastric foveolae and spare the mucosal surface and the deep gastric glands. Pyloric gland adenomas do not show conventional morphological features of dysplasia. Instead, they resemble non-dysplastic (reactive) epithelium: the cells are cuboidal with granular eosinophilic cytoplasm, and the nuclei are blander, more rounded, and less stratified than the nuclei of conventional dysplasia. Rarer Types of Gastric Dysplasia In addition to adenomatous dysplasia and gastric-type (foveolar or pyloric) dysplasia there are some rare forms of gastric dysplasia, i. Tubule neck dysplasia, which is the likely precursor lesion of poorly cohesive carcinomas, is characterised by enlarged, pale, Colorectal Dysplasia Sporadic Colorectal Dysplasia Conventional adenomas comprise dysplastic colonic epithelium in the setting of a circumscribed lesion (usually a polyp). Microscopically, adenomas are subdivided architecturally into tubular, villous, or tubulovillous. Villous adenomas have leaf- or finger-like projections of epithelium overlying a small amount of lamina propria. Although the histological criteria are not precise, villous adenomas according to some classifications should contain at least 75% villi, whereas tubular lesions should contain less than 25% villi. Tubulovillous adenomas have a mixture of tubular and villous structures with between 25% and 75% villous epithelium. Interobserver variability for the distinction between these types is consistently high, casting doubt on their prognostic value. Dysplasia is subdivided into low grade (encompassing the previous categories of mild and moderate) or high grade (corresponding to the previous category of severe). Intramucosal adenocarcinoma is the term for foci of intramucosal invasive growth (invasion of the mucosa or of the muscularis mucosae), usually in a setting of high-grade dysplasia. A diagnosis of invasive carcinoma requires infiltration beyond the muscularis mucosae into the submucosa. Because of sampling issues or poor orientation, some serrated lesions are difficult to classify. Compared to hyperplastic polyps, the serrated aspect is more obvious, with prominent serration in the lower third of the crypts rather than superficially. It has a villiform or filiform growth pattern and occurs more 123 Magali Svrcek and Roger M. Feakins commonly in the left colon, particularly the sigmoid, than in the right colon. Histologically, the lining of the villi comprises characteristic tall columnar cells with confluent pink eosinophilic cytoplasm and a narrow pencillate nucleus. Advances in endoscopic techniques and technologies have yielded improvements in the detection of previously invisible lesions. With new endoscopic techniques (including chromo-endoscopy and narrow band imaging), the yield of unconventional lesions is higher. This type of dysplasia may be characterised by round or oval and vesicular nuclei and may be dissimilar to conventional adenomatous dysplasia (which typically displays elongated, penicillate, pseudostratified nuclei with mitoses). Serration of the epithelium and enlarged goblet cells both extend to the base of the crypts. Therefore, it is difficult to recognise the lesion and to compare various studies with one another. Feakins non-keratinising squamous zone, and the distal zone of keratinising squamous epithelium. Classification using the same criteria and terminology for anal and uterine cervical lesions is an option. These pre-invasive changes may colonise the underlying anal glands and cutaneous adnexae, making the diagnosis of invasion potentially difficult. The behaviour of lowgrade squamous lesions is different in immunocompetent and immunocompromised patients. The atypia may represent low-grade dysplasia but could alternatively be regenerative and is difficult to classify. Summary There are similarities and differences between the features of dysplasia at various sites in the gastrointestinal tract. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical implications. Histological classification of intraepithelial neoplasias and microinvasive squamous carcinoma of the esophagus. Reproducibility of the diagnosis of dysplasia in Barrett esophagus: a reaffirmation. Squamous dysplasia and other precursor lesions related to esophageal squamous cell carcinoma. Intestinal low grade tubuloglandular adenocarcinoma in inflammatory bowel disease. Neoplasia without dysplasia: lessons from Barrett esophagus and other tubal gut neoplasms. Interobserver variability in the diagnosis of crypt dysplasia in Barrett esophagus. Interobserver variation between general and specialist gastrointestinal pathologists when grading dysplasia in ulcerative colitis. Guidelines for screening and surveillance of 128 Chapter 8: Gastrointestinal Dysplasia asymptomatic colorectal cancer in patients with inflammatory bowel disease. Role of immunohistochemical markers in predicting progression of dysplasia to advanced neoplasia in patients with ulcerative colitis. Comparison of p53 immunoexpression with allelic loss of p53 in ulcerative colitis-associated dysplasia and carcinoma. Biomarker-based prediction of inflammatory bowel disease-related colorectal cancer: a casecontrol. Immunohistochemical assessment of Ki67 and p53 expression assists the diagnosis and grading of ulcerative colitis-related dysplasia. Gastric adenomas: intestinal-type and gastrictype adenomas differ in the risk of adenocarcinoma and presence of background mucosal pathology. Dysplasia and dysregulation of proliferation in foveolar and surface epithelia of fundic gland polyps from patients with familial adenomatous polyposis. Serrated polyps of the large intestine: a morphologic and molecular review of an evolving concept. Serrated lesions of the colorectum: review and recommendations from an expert panel. Are dysplasia and colorectal cancer endoscopically visible in patients with ulcerative colitis Endoscopy in inflammatory bowel disease: advances in dysplasia detection and management. Feakins serrated polyposis in inflammatory bowel disease: a case series of a previously undescribed entity. Clinical, pathologic, and outcome study of hyperplastic and sessile serrated polyps in inflammatory bowel disease. Prevalence and anatomic distribution of serrated and adenomatous lesions in patients with inflammatory bowel disease. Association between serrated epithelial changes and colorectal dysplasia in inflammatory bowel disease. Feakins Oesophagus Classifications of the anatomy of the oesophagus usually describe upper, middle, and lower thirds. Other less popular classifications refer to cervical, upper thoracic, middle thoracic, and lower thoracic. Endoscopists use the distance from the incisors to define the location of a lesion within the oesophagus and proximal stomach. One definition requires basal cells to account for more than half of the lower third of the epithelial layer. There is maturation of epithelial cells towards the surface, where the cells are flatter, the nuclear:cytoplasmic ratio is lower, and the nuclei are elongated rather than round or ovoid. Keratinisation and/or a granular cell layer are abnormal features of oesophageal squamous epithelium. There is evidence of an association with squamous neoplasia but little evidence that epidermoid metaplasia is actually pre-neoplastic. This finding is of little significance, apart from its potential endoscopic resemblance to candidiasis and other conditions. Sparse melanocytes may be present in the oesophageal squamous epithelium and may occasionally form aggregates but are usually not identifiable on haematoxylin and eosin (H&E) staining. Endocrine cells are also infrequent and are difficult to recognise without the application of immunohistochemical stains. Inflammatory Cells in the Oesophageal Mucosa A few lymphocytes are typically present in the squamous epithelium, and they are more numerous distally than proximally. Large numbers may prompt a search for other evidence of inflammation and particularly for other types of inflammatory cell. The presence of even small numbers of eosinophils should prompt a search for other histological evidence of inflammation and/or gastro-oesophageal reflux. Intraepithelial neutrophils, unless very sparse (maximum 1 per hpf), are abnormal and are indicative of oesophageal inflammation. Lymphoid aggregates are sometimes present in the lamina propria, may be prominent, may include germinal centres (lymphoid follicles), and do not necessarily indicate oesophagitis. They open into the oesophageal lumen via transepithelial ducts lined by gastric foveolar-type columnar cells. Another suggestion is that submucosal glands may be useful for the distinction of true submucosa from lamina propria in the oesophagus. Papillae are finger-like projections of lamina propria that extend into the overlying epithelium and, in normal circumstances, occupy no more than half of the thickness of the Table 9. Up to 20 lymphocytes per hpf is acceptable in the oesophageal squamous epithelium. Given the frequency of reflux in the population, a minor degree of papillary elongation is common. In addition, many people with no other clinical evidence of reflux have papillary elongation and/or basal cell hyperplasia in the distal 30 mm of the oesophagus. In general, symptomatic patients with reflux show more severe histological changes than those who are asymptomatic. Compared to the muscularis mucosae of the stomach and intestine, the muscularis mucosae of the oesophagus is more deeply located and thicker (particularly in the distal oesophagus) and is longitudinal rather than a mixture of longitudinal 135 Roger M. It is usually not present in mucosal biopsies unless there is disruption of this layer by pathological conditions. If muscularis mucosae is present in the biopsy, its appearances can help distinguish oesophageal biopsies from gastric. Submucosal glands can occur at any level but are more prominent proximally and distally than in the mid oesophagus. Oncocytes are sparse and have bright pink cytoplasm that may reflect the presence of many mitochondria. In practice, 136 Chapter 9: Normal Oesophageal, Gastric and Duodenal Mucosa Practice Points 9. Opinions differ as to whether the cardia is a normal entity or a metaplastic area. Extension proximally may be secondary, at least in part, to chronic gastro-oesophageal reflux. Some authors believe that the normal cardia contains oxyntic glands (with parietal and chief cells) and is identical to the corpus mucosa, whereas others assert that the normal cardia comprises mucinous epithelium with mucous glands and/or mixed mucous/oxyntic glands and that this appearance does not indicate metaplasia. A characteristic finding of cardia mucosa is the presence of fairly well circumscribed aggregates of glands in the deep part of the mucosa around which there are smooth muscle fibres passing upwards from the muscularis mucosae and separating the glandular aggregates into lobules. In some studies, inflammation of the cardia mucosa immediately below the Z line in the absence of inflammation of the remaining stomach is a more sensitive marker of reflux than histological abnormalities of the squamous mucosa above the Z line.
On the other hand blood pressure information generic 45 mg midamor otc, focal and lobar resections are much commonly performed in older children and constitute 60% of the procedures in children older than 12 years of age hypertension 16090 order 45 mg midamor free shipping. Surgical interventions for hypothalamic hamartoma and multistage cortical resection in patients with tuberous sclerosis are just two examples of this group of lesions arrhythmia natural cure 45 mg midamor buy. Rasmussen syndrome and LandauKleffner syndrome also appear mainly in childhood blood pressure medication make you gain weight purchase generic midamor, and their management requires considerable medical and surgical expertise heart attack jaw pain generic 45 mg midamor free shipping. The number of pediatric epilepsy surgery centers as well as the number of young epilepsy patients undergoing epilepsy surgery has exponentially increased within the last decade. The age distribution of these patients has drastically changed and epilepsy surgery in infants has become much more common than before. Much sophisticated noninvasive and invasive neurophysiologic data acquisition techniques have been developed and the availability of outcome data for pediatric epilepsy surgery patients has significantly increased within the last decade. Advances in the neurosurgical technology and techniques as well as improving surgical skills and experience of epilepsy surgeons have resulted in increasingly sophisticated surgical procedures. Furthermore, refined pre- and postoperative neuropsychological assessment techniques and improved data accumulation methods have also provided valuable insights into the effect of current surgical interventions on the various life domains of the pediatric epilepsy patient. These developments have opened a unique window of opportunity for pediatric epilepsy surgery. The number of pediatric epilepsy surgery centers and children undergoing epilepsy surgery has increased dramatically over the past 10 years. The involvement of pediatric neurosurgeons in pediatric epilepsy cases has become a standard practice. As a result, pediatric epilepsy surgery has become an established, safe, and efficacious treatment modality in carefully selected children. However, pediatric epilepsy surgery still faces many hurdles, such as the lack of a consensus for the identification and selection criteria of surgical candidates as well as the lack of guidelines for determining the proper timing of surgery. Although surgical techniques are much more refined and safer than ever before, many new and potentially beneficial areas in pediatric epilepsy surgery 8 I Introduction to Epilepsy in Children remain open to exploration and development, including new neuromodulation procedures, such as deep brain stimulation and the application of ablation and radiosurgery techniques in children. Data from these procedures and similar treatment modalities are still limited or yet to be gathered. Because children, especially young children and infants, are still developing human beings, epilepsy is not fixed but is an evolving and complex process in this patient population. Therefore, the selection and referral of young patients for epilepsy surgery constitute a delicate endeavor, one that needs to be handled with great care and expertise. This is the unique challenge that the pediatric epilepsy surgery community now faces and must overcome. Conclusion Although pediatric epilepsy surgery is a well-established management option in the treatment of this highly vulnerable patient population, the accumulated data are still far from satisfactory in terms of provid- References 1. Proposed criteria for referral and evaluation of children for epilepsy surgery: recommendations of the Subcommission for Paediatric Epilepsy Surgery. Consequences of epilepsy in the developing brain: implications for surgical management. A method for surgical management of focal epilepsy, especially as it relates to children. Approach to pediatric epilepsy surgery: state of the art, part I: general principles and presurgical workup. Contrasts between pediatric and adult epilepsy surgery: rationale and strategy for focal resection. Developmental outcomes in children receiving resection surgery for medically intractable infantile spasms. The effect of surgery in encephalopathy with electrical status epilepticus during sleep. Curr Treat Options Neurol 2012;14(6):620629 1 Basic Considerations of Pediatric Epilepsy Surgery 32. Neurosurgical management of intractable rolandic epilepsy in children: role of resection in eloquent cortex. New York: Taylor and Francis; 2006:121-141 9 2 Summary A Historical Review of Epilepsy Surgery and Its Application in Children Deniz <;ataltepe and Oguz <;ataltepe the history of epilepsy surgery dates back to the late Nineteenth Century, with the first epilepsy surgery proce dure performed by Victor Horsley in 1886. Around the same time, Fedor Krause started a school of epilepsy surgery in Germany focusing on cortical stimulation and motor cortex mapping. The International League Against Epilepsy, which was established in 1909, brought together these seminal figures as well as the surgeons William Macewen and Harvey Cushing. Although pediatric patients were involved in these epilepsy surgery milestones, the first surgical series to focus on this spific patient popu lation was completed by Murray. The first International Pediatric Epilepsy Surgery Symposium took place in 1989, with meetings and workshops continuing to be held regularly to establish guidelines and recommendations for epilepsy surgery in the pediatric population. The history of epilepsy surgery, which is deeply intertwined with the history of modern neuro surgery, encompasses the early foundations of pediatric epilepsy surgery, and this specialty continues to be refined today. Keywords: history, epilepsy surgery, pediatric epilepsy surgery, Horsley, Penfield, Falconer not only opened the door to understanding the clinical aspects of epilepsy, but also paved the road for the surgical treatment of epilepsy patients and the initiation of modern neurosur gery. In a sense, the early history of epilepsy surgery is also the history of the initial stages of modern neurosurgery. Jackson was appointed assistant physician to the National Hospital for the Paralyzed and Epileptic in Queen Square, London in 1862 with the suQport of Charles Edouard Brown-Sequard. In 1864, he delivered a lecture on "the method of diagnostic neurology based on clin ical physiology" at London Hospital. In 1869, he gave the presti gious Goulstonian Lecture at the Royal College of Physicians on "the study and classification of diseases of the nervous system. He was the key figure in the history of epilepsy, even deemed to be the "father of epilepsy" accord ing to some accounts. His major impact on clinical neurology and neurosurgery came with his "cerebral localization" theory, which states that certain areas of the brain are related to different functions. Jackson defined the causal relation between abnormal cor tical neuronal activity and focal seizures with this concept, and he stated that "a convulsion is but a symptom, and implies only that there is an occasional, an excessive, and a disorderly discharge of nerve tissue on muscles. However, this was only based on his clinical observations and it was still a hypothesis. In 1870, Gustav Theodor Fritsch and Eduard Hitzig in Berlin electrically 2 · Introduction the history of modern epilepsy surgery starts in the late 19th century with a paradigm shift in our understanding of cortical functions and their clinical correlates. This conceptual change 2 A Historical Review of Epilepsy Surgery and Its Application in Children stimulated the motor cortex of awake dogs for the first time and showed that cortical stimulation of certain areas produced sim ilar responses with a predictable pattern. One of the students of this new exciting research area was Victor Horsley (18571916). As a researcher, Horsley performed numerous craniotomies on animals, particularly in macaque monkeys and orangutans, to study cortical localization and brain mapping and followed in the footsteps of Fritsch and Hitzig. In 1886, he was appointed as a staff surgeon to perform craniotomies on patients at the National Hospital for the Paralyzed and Epileptic in Queen Square, London. He performed the first epilepsy surgery procedure in the same year, in 1886, with both Jackson and Ferrier present in the operating theater. Horsley began his talk by stating that his presentation was to be "a simple description of that method of operating on the brain which I have adopted as one which successfully meets the various difficulties and dangers of the task. He continued his lecture by discussing three illustrative cases on which he had operated, all of which were epilepsy patients. Today, it is widely accepted that the first patient he presented, a 22yearold man, was the first modern epilepsy surgery case. He continued to operate on more epi lepsy patients and a year later, in 1887, he published a series of 10 surgically treated epilepsy patients. While Horsley made a splash with his surgeries and lectures, another British neurosurgeon, William Macewen (18481924) was also operating on epilepsy patients. Macewen, who had quite a different background than Horsley and no research experience, was also following localization techniques defined by Jackson. He worked on establishing cortical localization by observing the symptomatology of seizures. These were Jacksonian seizures starting from the face and progressing to the arm and leg. Macewen published two other articles that discussed various neurosurgical cases, including some epilepsy surgery cases. Shortly after, that toe was firmly extended in tonic spasm, which lasted about five minutes. More frequently it was followed by clonic con tractions of the muscles of the right foot, leg, and thigh, where the convulsions often terminated. Occasionally they extended to the muscles of the trunk, then to those of the right side of the face and right arm, the contractions ceasing in the order of accession. Rare ly did they involve the opposite side, and when they did, patient lost consciousness. On careful palpation of the ascending convolutions, there was found in the upper part of the ascending parietal, a circumscribed nodule buried in the cerebral substance, which on exposure by cutting through the grey mat ter, was seen to be a tubercular tumor, about the size of a hazel nut, which was easily shelled out. He had a special interest in epilepsy surgery and used electri cal stimulation during surgeries on the motor cortex from as early as 1893. His technique involved using monopolar stimulation to induce seizures, and then localizing the epileptogenic focus for resection. Krause was also likely the first surgeon to have performed intraoperative electrical stimulation of the cere bral cortex on a child. He reported a 15yearold patient with seizures since the age of 2, with the seizures being cured after surgery. Many prominent neurosurgeons, including William Macewen, Fedor Krause, and Harvey Cushing attended the meeting and delivered lectures. The figures he presented in this lecture neatly document his metic ulous cortical stimulation and mapping technique. After the First World War, many veterans in Europe suffered from seizures secondary to various traumatic brain injuries. In Germany, Hans Berger (18731941), a neuropsychiatrist at the University of Jena, conducted a series of experiments by placing needle electrodes under the scalps of patients who had skull defects following surgeries during the war period. Initially, he was unsure about the nature of the oscillations he had recorded and subsequently conducted many other experi ments, deciding to wait to publish his first paper on the human electroencephalogram until 1929. He was a pioneer in awake craniotomy with cortical stimulation as well as mapping of the human cortex. He used cortical stimulation in almost all brain surgery cases he performed and accumulat ed an enormous amount of experience and data that helped him to produce a detailed brain map based on his stimulation results. His fame attracted many neurosurgeons from the United States and Britain, including Fulton, Bucy, Bailey, and Penfield, to visit the Breslau Neurological Institute. He planned to expand his experience on cortical stimu lation by working with Foerster. Penfield and Foerster published papers together including a paper describing an expanded map of the human cortex in 1930 by showing detailed information about functional areas other than the motor cortex, including sensory, acoustic, and visual representations. This period at the early stage of his career form the groundwork for Penfield as a physiological surgeon of the human brain. He would later describe his time in Germany as "one of the greatest moments" in his life. Gradually, however, Penfield and Rasmussen went further by stimulating other cortical regions and identifying a variety of complex and higher cognitive responses including speech, secondary sensory and motor areas, autonomic function, and even "the sites of dreams and memories". This database covered the entire human cerebral cortex and its functional representations. Based on the data, they collected from more than 400 cortical stimula tions, the "homunculus" concept was gradually developed. Abnormal activities were localized to the left side over the region with traumatic injury. Thereafter, Penfield and Jasper introduced electrocorticography with subdural electrodes in the 1950s. The posterior borders of his resections reached the level of the central sulcus posterior ly. His lobectomy technique included the uncus, amygdala, and anterior 2 to 4 cm of the hippocampus in addition to the anterolateral temporal cortex. He operated on 68 cases between 1939 and 1949 and removed the hippo campus in only two cases. This approach led to a dramatic impact on our understanding of the pathology of temporal lobe epilepsy. Yaargil introduced the operating microscope and microsurgical techniques to neurosurgery in 1967. He also developed an innovative transsylvian approach to treat aneurysms and vascular malformations of the circle of Willis. Later, in 1973, Yaargil started to apply this technique to perform selective transsylvian amygdalohippocampectomy in patients with mesial temporal epilepsy. Additionally, Rasmussen revived hemispheric surgeries for patients with multilobar/hemispheric epilepsy by describing the function al hemispherectomy technique. During this 2 A Historical Review of Epilepsy Surgery and Its Application in Children time, another neurosurgeon in the same hospital, Jean Talairach, was focusing on stereotactic techniques and deep brain stimu lation. They also developed the concept of anatomoelectroclinical correlates to define the epileptogenic network. Chauvel joined Bancaud, to make SainteAnne Hos pital another magnet center in epilepsy surgery that attracted visitors and trainees from many other hospitals and countries. Lat er on, however, it became the most commonly used invasive monitoring technique in the United States. Reportedly, Falconer confided in one of his colleagues that "after establish ing the indication and methodology of temporal lobe surgery" he felt that "it is his mission to propagate and sell this knowl edge to encourage epileptologists to apply these techniques in pediatric years. In 1968, Crandall and his colleagues were the first to record the onset of a seizure in a human being using intracranial electrodes. Soon more reports specifically addressing epilepsy surgery in children began to be published. His first report included 17 patients (214 years old) in 1978, then 44 children (5 months to 14 years) in 1984, and, finally, 75 chil dren (5 months to 15 years) in 1987. Awake craniotomy with a child was extremely difficult, however, and only feasible for older chil dren. The series he published in 1987 is one of the earliest and largest series for invasive mon itoring in children with epilepsy.
Epileptiform activity (spikes and sharp waves) defines the irritative zone during the interictal state or ictal onset zone at the time of the seizure onset based on their location heart attack album order cheap midamor on line. Analyzing the habitual seizures is critical to determine that they are originating from one location or blood pressure medication pregnancy cheap 45 mg midamor amex, in some cases blood pressure 4 month old midamor 45 mg purchase line, to exclude nonepileptic seizures blood pressure medication midamor 45 mg purchase mastercard. Even if a lesion is present pulse pressure 46 midamor 45 mg purchase mastercard, ictal recordings confirm that the seizures arise from the lesion or are not multifocal. Focal sharp waves; spike and wave discharges; and slowing (especially polymorphic delta activity) or independent, synchronous, or time-locked (a time lag) bitemporal discharges may be seen. On the contrary, in the Miami series, a unilateral and well-localized ictal onset was seen in 33 children (54%); a lateralized but poorly localized or multilobular discharge occurred in 23 children; and an independent or synchronous, bilateral onset was seen in 3 children. Type 1 seizures likely originate in the hippocampus, whereas type 2 seizures have a neocortical origin. Moreover, interictal discharges can be seen in a bifrontal or generalized pattern; thus, the localization and lateralization of a spike source can be challenging and limited. For that reason, closely spaced electrode placement using 1010 array is recommended to improve the localization, while lateralization may remain limited. Epileptiform discharges from the mesial frontal areas may be best visualized in the vertex location, at Fz, Cz, and Pz electrodes. Interictal epileptiform discharges can be detected unless the epileptogenic focus is located on the dorsolateral surface. Bilateral or generalized spike discharges again can be seen if an epileptogenic focus is in the mesial surface. Widespread spike discharges or spike discharges with a field to the central or posterior contacts can be seen32 in the interictal state. Nine patients had an excellent outcome (Engel class 1 or 2), two patients had a poor outcome (Engel class 3), and four patients had unfavorable outcome (Engel class 4). In fact, hyperventilation can trigger epileptiform activity and or seizures in 60 to 70% of patients diagnosed with idiopathic generalized epilepsy. Similarly, seizures were activated by hyperventilation in 30% in 13 patients diagnosed with parietal/occipital epilepsy. However, because of the longer uptake time, glucose uptake continues to occur in the other cortical regions based on the seizure spread pattern. The glucose uptake may continue in the adjacent and contralateral regions while the uptake is normalized in the region of seizure onset. Pitfalls of Localization of Epileptiform Activity Seizure Semiology the clinical features of seizures vary based on the location of the epileptogenic focus. For instance, dystonia or other motor manifestation is seen more often at the onset of seizures arising from frontal lobe whereas oral or hand automatisms are often reported with temporal lobe seizures. The practitioners must be cautious interpretation of semiology, especially for the seizures originating from the extratemporal regions. Bilateral seizures preclude a focal cortical resection if occurring equally from both hemispheres. However, resection can be considered in selected cases if the majority of disabling seizures are from one side. Seizure semiology can be misleading for focal epilepsy in the presence of bilateral motor manifestations and absence of clinical features characteristic for focal epilepsy, such as behavioral arrest or automatisms in young children. The presence of cortical dysplasia in association with other epileptogenic lesions is known as "dual pathology. The coexisting epileptogenic lesions include hippocampal sclerosis, developmental tumors, gliosis, vascular malformation, and cortical dysplasia. Moreover, cortical dysplasia was identified in patients with perinatal infarction, up to 10%, confirmed by histopathology. Moreover, all had widespread cortical abnormality suggesting either perinatal or postnatal injury. Academic difficulties, behavioral problems, regression in developmental milestones are common and often lead to the diagnosis. Three ictal propagation patterns of temporal lobe seizures were described: (1) Spread from one mesial temporal region to the neighboring temporal or frontal neocortex; (2) Spread from one mesial temporal region to the other before the involvement of the ipsilateral temporal neocortex; and (3) Spread from one mesial temporal region to the contralateral mesial temporal region and then lateral temporal cortex in the contralateral hemisphere. If there has been previous surgery, such as prior resection with recurrent seizures, or a skull defect (breach rhythm), then there may be a distortion of epileptiform activity because of the skull defect, fluid-filled cavities, or distorted postoperative anatomy with adhesions. A cortical area of 10 to 20 square cm is often required to generate a scalp recognizable interictal spike or ictal rhythm. The amplitude is primarily dependent on source area and synchrony, and therefore it is a less important factor. Moreover, changes in deoxyhemoglobin and oxyhemoglobin levels correlated with interictal epileptiform discharges in the region of epileptogenic focus in 18 patients. All seizures were associated with significant local and remote hemodynamic changes. During the onset of the seizures, a significant decrease in deoxyhemoglobin was observed with a concurrent increase in oxyhemoglobin level which often outlasted the seizure duration. Furthermore, hemodynamic changes were also observed in the contralateral hemisphere at lesser extent, suggesting the possibility of seizure propagation despite the absence of epileptiform activity in the contralateral hemisphere. For instance, brief electrographic seizures were associated with subtle changes in hemoglobin level compared to the more prolonged seizures. Therefore, a negative baseline shift at the seizure onset is an indicator of particular site involving ictal process rather than spread pattern from the other areas. Data were analyzed using conventional filter setting first and then changing the filter setting to 0. For instance, depth electrodes provide recording from mesial structures with excellent spatial resolution and fewer artifacts. Similar activation pattern was also seen in the contralateral hemisphere to a lesser extent. Deoxyhemoglobin levels were more broadly distributed however lateralized the epileptogenic focus in five patients. Low-grade focal cortical dysplasia is associated with prenatal and perinatal brain injury. Different features of histopathological subtypes of pediatric focal cortical dysplasia. White matter abnormalities in patients with focal cortical dysplasia revealed by diffusion tensor imaging analysis in a voxelwise approach. Pathophysiological implications of focal cortical dysplasia of end folium for hippocampal sclerosis. Approach to pediatric epilepsy surgery: state of the art, Part I: general principles and presurgical workup. Involvement of dopamine receptors of the dorsal hippocampus on the acquisition and expression of morphine-induced place preference in rats. Occipital lobe epilepsy: clinical characteristics, surgical outcome, and role of diagnostic modalities. Epilepsia 2006;47(6):981990 14 Electroencephalography and Noninvasive Electrophysiological Assessment 37. Clinical manifestations and outcome in 82 patients treated surgically between 1929 and 1988. Influence of sleep and sleep deprivation on ictal and interictal epileptiform activity. Interictal spiking during wakefulness and sleep and the localization of foci in temporal lobe epilepsy. Treatment of electrical status epilepticus in sleep: a pooled analysis of 575 cases. Quantitative evaluation of neuronal loss in the dorsal hippocampus in rats with long-term pilocarpine seizures. Multilobar polymicrogyria, intractable drop attack seizures, and sleep-related electrical status epilepticus. Epilepsy surgery patients with cortical dysplasia: present and future therapeutic challenges. Morphological and electrophysiological characterization of abnormal cell types in pediatric cortical dysplasia. Involvement of the prefrontal cortex but not the dorsal hippocampus in the attentionenhancing effects of nicotine in rats. Epilepsy with dual pathology: surgical treatment of cortical dysplasia accompanied by hippocampal sclerosis. Time-dependent relationship between the dorsal hippocampus and the prefrontal cortex in spatial memory. Effects of dietary tryptophan variations on extracellular serotonin in the dorsal hippocampus of rats. Treatment of electrical status epilepticus during slow-wave sleep with highdose corticosteroid. Both dorsal and ventral hippocampus contribute to spatial learning in Long-Evans rats. Involuntary, unreinforced (pure) spatial learning is impaired by fimbria-fornix but not by dorsal hippocampus lesions. Medical management with diazepam for electrical status epilepticus during slow wave sleep in children. Treatment of epilepsy with electrical status epilepticus during slow sleep and its related disorders. Adverse effects of maternal ethanol consumption on development of dorsal hippocampus in rat offspring. Electroencephalographic source imaging: a prospective study of 152 operated epileptic patients. Subcellular relationships between cholinergic terminals and estrogen receptor-alpha in the dorsal hippocampus. Comparing noninvasive dense array and intracranial electroencephalography for localization of seizures. Language mapping can rarely be performed intraoperatively in younger children or older children with anxiety or language disorders. This critical mass of tissue is viewed as a function of the region of seizure onset, seizure propagation patterns, the areas that could become epileptogenic later, and the underlying structural lesion and functional abnormality. As in adults, surgical strategies in childhood are guided by semiology, structural and functional imaging abnormalities, and neurophysiological data. This task can be daunting given the heterogeneity of etiopathological substrates and maturational factors that influence the clinical presentation and investigative findings. Lastly, family dynamics play an important role when deciding the best surgical approach for each child. Multidisciplinary case review with experienced colleagues in the practices of neurology, neurosurgery, neuroradiology, and neuropsychology is recommended. However, there are many documented failures after lesionectomy in children,7,8 partly because lesional epilepsies are typically not due to homogeneous substrates. Following resection of only the tissue from which the fast frequencies emanated, she is now 2 years seizure free despite the large amount of residual focal cortical dysplasia. Careful planning of electrode positioning is vital in these cases since the divergence may arise from complex and rapid interaction between noncontiguous cortical sites, of which must be adequately sampled. When divergence occurs in the context of large or deep-seated lesions, a combination of subdural and strategically placed depth electrodes is recommended. Subdural electroencephalography recording (b), showing ictal onset at contacts 3 and 4 of the anterior temporal polar strip, with early involvement of the superior temporal convexity (contacts: 1920), which were subsequently shown to be critical language areas on functional mapping. Because language cortex exhibits greater degrees of reorganization under the age of 5, many centers opt for more aggressive large resections in the hope of forcing language transfer. Our presurgical evaluation strategy is driven by the intent to preserve predestined language sites unless they are involved at ictal onset. This task is made more challenging by the restricted electrical field sampling of a typical subdural electrode13 and the number of electrodes that can be placed in children. Spontaneous seizures are usually captured over 4 to 10 days; longer periods of up to 1 month may occasionally be required. Generally, 3 to 10 seizures are considered adequate, although multiple factors may influence the confidence of the reader, including stereotypy of onset and evolution, and their convergence with other data. Once the capture of spontaneous seizures is deemed complete, we reinstate full medication before attempting functional mapping via direct electrical cortical stimulation. Type of Electrodes Invasive electrodes are usually made of platinum and are configured for subdural or depth placement. Subdural electrodes spaced 5 to 10 mm apart and configured as strips (48 contacts) or grids (2064 contacts) are most suited to cover large areas of the neocortical convexity and basal and interhemispheric surfaces. Using a combination of subdural and depth electrodes results in comprehensive coverage of both the cortical surface and deep locations. The onset zone may be regarded as the region showing the initial transformation from the interictal state: the collective area revealing a group of patterns commonly observed during the initial phase of the seizure including bursts of focal fast activity, spike/polyspikes, runs of spikes, or electrodecrement. Very high frequencies27 or slow direct current shifts have also been observed but may be missed with conventional filter settings. Thus, objective definition of the ictal onset zone can be challenging, especially in patients with rapid propagation. This finding Surgical Insertion Subdural grid electrodes are implanted under direct observation after craniotomy, although strips may be placed via burr holes. Implantation may be guided by a stereotactic frame but this technique has limited application in the younger child where the calvarium is thin and skull framing is contraindicated. Implantation is generally well tolerated, but complications, including wound infection, cerebrospinal fluid leak, intracranial bleeding, or symptomatic pneumocephalus, have all been reported. Recording Current digital systems have high sampling rate capability, at 500 to 1,000 Hz, allowing detection of fast frequencies that may provide useful additional information. Seizure capture may be 15 Invasive Electrophysiological Monitoring may be appreciated only after the same change is consistently observed during ictal onset in several seizures.
Discount midamor 45 mg buy online. How to Reduce Blood Pressure Naturally | Swami Ramdev.
References
- Theodore WH, Newmark ME, Sato S et al. 18F-Fluorodeoxyglucose positron emission tomography in refractory complex partial seizures. Ann Neurol 14: 429-437, 1983.
- O'Brien S, Furman RR, Coutre SE, et al. Ibrutinib as initial therapy for elderly patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: an open-label, multicentre, phase 1b/2 trial. Lancet Oncol 2014;15(1):48-58.
- Shah M, Martinson NA, Chaisson RE, et al. Quantitative analysis of a urine-based assay for detection of lipoarabinomannan in patients with tuberculosis. J Clin Microbiol 2010; 48: 2972-2974.
- Du ZD, Hijazi ZM, Kleinman CS, Silverman NH, Larntx K, for the Amplatzer investigators. Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: results of a multi-center non-randomized trial. J Am Coll Cardiol 2000;39:1836-1844.
- Aylsworth AS. Clinical aspects of defects in the determination of laterality. Am J Med Genet 2001;101:345-55.
- Lang-Lazdunski L, Bille A, Papa S, et al. Pleurectomy/decortication, hyperthermic pleural lavage with povidoneiodine, prophylactic radiotherapy, and systemic chemotherapy in patients with malignant pleural mesothelioma: a 10-year experience. J Thorac Cardiovasc Surg 2015;149(2):558-565.
- Whelton PK, Appel LJ, Espeland MA, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled Trial of Nonpharmacologic Interventions in the Elderly (TONE). TONE Collaborative Research Group. JAMA 1998;279(11):839-846.
- Bruskewitz, R., Issa, M., Roehrborn, C. et al. A prospective, randomized 1-year clinical trial comparing transurethral needle ablation to transurethral resection of the prostate for the treatment of symptomatic benign prostatic hyperplasia. J Urol 1998;159:1588-1593.