
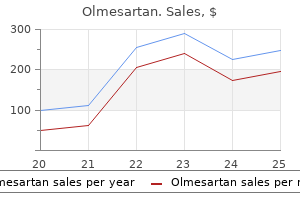
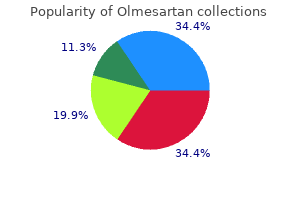
Olmesartan
| Contato
Página Inicial
Melissa M. Hudson, MD
- Director, Cancer Survivorship Division
- Member, Department of Oncology
- Saint Jude Children? Research Hospital
- Memphis, Tennessee
The tape is now sutured onto the top of the gastric tube (which has been created at an earlier stage; see previous text) pulse pressure chart order olmesartan with paypal. The gastric tube can be wrapped in a bowel bag or laparoscopic camera bag to facilitate atraumatic passage and can be brought up to the neck by pulling gently on the tape and pushing the gastric tube into the mediastinum hypertension benign buy genuine olmesartan line. A cervical anastomosis can subsequently be performed (see "Cervical Anastomosis") arrhythmia kinds buy 20 mg olmesartan with mastercard. The major disadvantages of using the stomach include the almost complete lack of peristaltic activity and the tendency for persistent reflux into the remaining cervical esophagus that is directly connected to the acid-secreting stomach arteria axilar order olmesartan in india. In long-term survivors blood pressure chart stage 2 buy generic olmesartan from india, this ongoing reflux can result in the development of interstitial metaplasia (Barrett) in the cervical remnant. As a result, when there is extensive involvement of the stomach and the esophagus, the use of an antiperistaltic or isoperistaltic left colon interposition is preferred. Also, in cases where creation of a (sufficiently oxygenated) gastric tube is technically not possible. This is probably explained by the difference in mediastinal dissection and pleural resection. Studies comparing cervical with intrathoracic anastomoses in patients who underwent neoadjuvant therapy are lacking. Theoretically, the gastric tube can be shorter in case of an intrathoracic anastomosis, with potentially improved oxygenation of the tip and thus enhanced anastomotic healing. On the contrary, radiation damage on the intrathoracic esophageal remnant might hamper intrathoracic anastomotic healing. This incision should extend from the sternal notch to a point halfway to the ear lobe. The omohyoid, sternohyoid, and sternothyroid muscles are divided laterally, and the jugular vein and carotid sheath are lateralized. Dissection is then continued posteriorly to the esophagus, down to the dissection plane with the prevertebral fascia, into the thoracic inlet where the dissection plane performed during the thoracotomy is reached. The esophagus is encircled with a Penrose drain and the upper thoracic esophagus is delivered into the neck. The esophagus is divided at the level of the thoracic inlet and the specimen is removed via the abdomen after tying a tape to the esophagus. The cervical remnant should not be too long, thus preventing that the anastomosis will ultimately retract into the upper chest with a possibly increased risk of intrathoracic manifestation in case of leakage. With use of the tape, which is tied to top of the gastric tube, the gastric pull-up can be completed. The previously created gastric tube can be wrapped in a plastic bag to facilitate atraumatic passage to the neck. Care should be taken to avoid excessive tension on the stomach or its gastroepiploic arcade during this maneuver and to avoid twisting of the stomach. The anastomosis is performed between the remaining cervical esophagus and the gastric tube. Several nonabsorbable sutures should be placed to normalize the size of the hiatus to prevent visceral herniation into the thorax. A nasogastric decompression tube is then carefully passed as well as a nasojejunal feeding tube. With care to prevent rotation, the cardia together with the gastric tube is delivered through the hiatus into the thoracic cavity, and the surgical specimen. Subsequently, the gastrotomy is made at the tip of the gastric tube, the circular stapling device is introduced, and an end-to-side anastomosis is created using a 25 mm or 29 mm circular stapling device. The gastrotomy is closed with a linear stapler and the linear staple line is oversewn. After completion of the anastomosis, omental tissue is wrapped around the anastomosis (omentoplasty). The left segment of the colon to be interposed derives its arterial supply from the ascending branch of the left colic artery and usually corresponds to the segment extending from the midtransverse colon to the proximal descending colon. This segment is mobilized by dissecting the middle colic artery back to its origin from the superior mesenteric artery where it arises as a single trunk in most patients. After the middle colic artery and vein have temporarily been occluded to ensure adequate collateral flow through the marginal artery, these vessels are ligated and divided. The apex of the arc portended by the vascular pedicle is then marked with a suture and the distance from this point to the neck is measured with an umbilical tape. This tape is used to measure proximally from the first marking stitch to determine the point of transection of the proximal colon. The divided colon is then passed through the bed of the resected esophagus wrapped in a bowel bag, and a single-layer monofilament running anastomosis is performed to the remaining cervical esophagus. Traction is gently applied to the colon from within the abdomen to eliminate redundancy, and the colon is secured to the left crus of the diaphragm with a nonabsorbable suture. The colon is then divided with a linear stapler 5 to 10 cm below the point where it enters the abdomen. Care should be exercised not to leave too long of an intraabdominal segment of colon, as this will result in food retention. The mesentery should be divided immediately adjacent to the wall of the colon to avoid injury to the vascular pedicle. A single-layered anastomosis is then performed between the distally divided colon and the Roux-en-Y jejunal loop, and colon continuity is restored by a colocolostomy. Alternatively, the left colon can be used in antiperistaltic position, which is based on a vascular pedicle of the middle colic artery and vein. In this way, the interposed segment can be longer by making use not only of the descending colon, but also (part of) the sigmoid colon. Finally, the right colon can be used including the ileocecal valve in an isoperistaltic position and again based on the middle colic vessels. The advantage of this technique is that the ileocecal valve will act as an antifreflux mechanism at the proximal anastomosis. We routinely perform a catheter jejunostomy to provide early postoperative enteral feeding and to avoid the need for parenteral nutrition in the event of postoperative complications such as an anastomotic leak. The jejunostomy catheter is removed when the patient is able to maintain body weight by oral feedings, usually 3 to 4 weeks postoperatively. These are large, technically demanding operations that are often performed on patients with compromised cardiopulmonary function. Nutritional disturbances are also common because of the combined effects of the cancer itself and the obstructing mass in the esophagus. Therefore an international system for defining and recording postoperative complications associated with esophagectomy has been developed. These complications can be minimized by early ambulation and careful attention to adequate pain control. The definition for subclinical anastomotic leakage was anastomotic leakage seen only on contrast radiography, and clinical anastomotic leakage was defined as anastomotic leakage resulting in a cervical salivary fistula (all patients had cervical anastomoses). When necessary, a mini-tracheostomy can provide invaluable assistance in clearing retained secretions. The shift of body fluids and the extensive mediastinal dissection that causes a systemic inflammatory response likely play a role in the pathogenesis. Although these are generally self-limiting, they do require cardiac monitoring and treatment, which can prolong the intensive care unit stay. Atrial fibrillation can also, for example, be caused by anastomotic dehiscence with secondary mediastinitis or by mechanical irritation by a chest tube. Anastomotic complications occur in 10% to 30% of patients depending on the definition and the type of reconstruction performed. We recommend early endoscopy in any patient who is known or suspected to have a substantial leak to exclude potentially life-threatening conduit ischemia, which can be present in as many as 14% of patients with an anastomotic leak. The optimal threshold for survival benefit was removal of 23 nodes, and the operation most likely to achieve this number was found to be an en bloc transthoracic resection. The results of this meta-analysis should be interpreted with caution, because both randomized and nonrandomized studies were included. Ultimately, this debate can only be resolved by the completion of a large randomized controlled trial. The concept of neoadjuvant therapy in esophageal cancer was spurred by a general disappointment in the results of primary resections, which resulted in survival of 35% or less at 5 years. A meta-analysis showed that both neoadjuvant chemotherapy and neoadjuvant chemoradiotherapy improve long-term survival. The applied neoadjuvant regimen consisted of cisplatin and fluorouracil with 45 Gy concurrent radiotherapy. No differences in 3-year overall survival rate and radical resection rate were found between both treatment arms. This is supported by the high rate of radical resections (92%) in the surgery-alone arm of the French trial. Twenty patients underwent salvage esophagectomy because of residual or recurrent disease without signs of distant metastases. A tailored approach to the management of these patients can now result in an overall 5-year survival of about 50%, which is a dramatic improvement compared with the dismal results reported in the (recent) past. However, the lack of high-quality evidence on these topics has led to persistence of substantial differences in the treatment approach between individual institutions. These differences underline the ongoing need for well-designed clinical trials on specific topics in the field of esophageal cancer surgery. Thanks to centralization of care with improvement in patient selection, in surgical technique and in perioperative management, perioperative morbidity and mortality nowadays have substantially decreased. With minimally invasive esophagectomy, thoracic surgeons must avoid falling into the same trap again! Mortality after esophagectomy for carcinoma of the esophagus: an analysis of risk factors. The surgical treatment of carcinoma of the oesophagus; with special reference to a new operation for growths of the middle third. A prospective randomized comparison of transhiatal and transthoracic resection for lower-third esophageal carcinoma. Oesophagectomy by a transhiatal approach or thoracotomy: a prospective randomized trial. Surgical therapy of esophageal carcinoma: the influence of surgical approach and esophageal resection on cardiopulmonary function. Three-field lymph node dissection for squamous cell and adenocarcinoma of the esophagus. Prevalence and location of nodal metastases in distal esophageal adenocarcinoma confined to the 29. Technical factors that affect anastomotic integrity following esophagectomy: systematic review and meta-analysis. Cervical or thoracic anastomosis after esophagectomy for cancer: a systematic review and meta-analysis. Intrathoracic manifestations of cervical anastomotic leaks after transthoracic esophagectomy for carcinoma. Intrathoracic manifestations of cervical anastomotic leaks after transhiatal and transthoracic oesophagectomy. Systematic review of the benefits and risks of neoadjuvant chemoradiation for oesophageal cancer. Reporting of short-term clinical outcomes after esophagectomy: a systematic review. The 30-day versus in-hospital and 90-day mortality after esophagectomy as indicators for quality of care. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. End-to-end versus end-to-side esophagogastrostomy after esophageal cancer resection: a prospective randomized study. Modern 5-year survival of resectable esophageal adenocarcinoma: single institution experience with 263 patients. Prognostic factors in adenocarcinoma of the esophagus or gastroesophageal junction. Prediction of survival in patients with oesophageal or junctional cancer receiving neoadjuvant chemoradiotherapy and surgery. The number of lymph nodes removed predicts survival in esophageal cancer: an international study on the impact of extent of surgical resection. Surgical resection strategy and the influence of radicality on outcomes in oesophageal cancer. Transthoracic versus transhiatal esophagectomy for the treatment of esophagogastric cancer: a meta-analysis. Impact of neoadjuvant chemoradiation on lymph node status in esophageal cancer: post hoc analysis of a randomized controlled trial. The effect of preoperative chemoradiotherapy on lymph node harvest after total mesorectal excision for rectal cancer. Lymph node retrieval during esophagectomy with and without neoadjuvant chemoradiotherapy: prognostic and therapeutic impact on survival. Multimodality treatment for esophageal adenocaricnoma: multi-center propensity-score matched study. Evolution of standardized clinical pathways: refining multidisciplinary care and process to improve outcomes of the surgical treatment of esophageal cancer. Salvage surgery after chemoradiotherapy in the management of esophageal cancer: is it a viable therapeutic option Comparing outcomes after transthoracic and transhiatal esophagectomy: a 5-year prospective cohort of 17,395 patients.
The majority of internal hernias are the result of congenital abnormalities of intestinal rotation and peritoneal attachment hypertension jnc guidelines generic 40 mg olmesartan otc. Failure of rotation results in entrapment of the duodenum in the mesocolon traversing through Waldeyer fossa at the root of the small bowel mesentery blood pressure chart for 35 year old man 20 mg olmesartan buy. Seventy-five percent of paraduodenal hernias occur on left side and 25% on right side hypertension benign olmesartan 40 mg with visa. Most children remain asymptomatic and the paraduodenal hernia is often an incidental finding during other evaluation arrhythmia or anxiety order olmesartan 40 mg. However arrhythmia consultants of connecticut order olmesartan 20 mg without prescription, this can also present with intermittent midabdominal discomfort as well as acute intestinal obstruction and even strangulation. An ongoing history of chronic abdominal symptoms can point to intermittent obstruction of the herniated intestine. As with any hernia, rapid identification is important to prevent strangulation and loss of intestine. The most sensitive test is cross-sectional imaging, with a higher yield of identification during a symptomatic period. Radiologic examination shows concern for a closed-loop obstruction with both afferent and efferent loops trapped with a mesenteric pedicle. In a right-sided paraduodenal hernia, there is reversal of the normal left-sided jejunal arteries. The surgical principles require reduction of the herniated contents, thorough examination to assess for viability, and closure of the hernia defect. In cases of left-sided paraduodenal hernia, the bowel often can be easily reduced and the peritoneal defect can be easily reapproximated. Right-sided paraduodenal hernias are often more challenging as the herniated contents can be fixed into the retroperitoneum. A lateral to medial approach is the safest option to avoid injury to the superior mesenteric artery, the ileocolic artery, and the right colic vein. A high index of suspicion should be kept in children who have recently experience rapid weight loss. Presenting symptoms can also be vague epigastric pain as well as nausea and emesis. Often there is a description of either intermittent or postprandial abdominal discomfort. Some patients can have symptomatic relief by bringing their knees up to their chest or lying on their stomach, which is thought to open the aortomesenteric angle. The syndrome is defined by radiographic evidence of the superior mesenteric artery compressing on the third portion of the duodenum with an aortomesenteric angle less than 22 degrees (normal 38 to 65 degrees) and an aortomesenteric distance less than 8 mm (normal 10 to 28 mm). Conservative management is the treatment of choice for this disease process in the absence of a pathologic condition that requires surgical intervention such as a mass or vascular aneurysm. As stated in the section on pyloric stenosis, correction of electrolyte abnormalities is paramount. Preferential nasojejunal feeding should be initiated when possible with total parenteral nutrition reserved for select cases. Laparoscopic excision of a gastric duplication cyst detected on antenatal ultrasound scan. An eighteen year follow-up after surgery for congenital microgastria-case report and review of literature. Aplasia cutis congenita associated with epidermolysis bullosa and pyloric atresia: the diagnostic role of prenatal ultrasonography. Dessanti A, Di Benedetto V, Iannuccelli M, Balata A, Cossu Rocca P, Di Benedetto A. Antenatally diagnosed right-sided stomach (dextrogastria): a rare rotational anomaly. Should we be concerned about jejunoileal atresia during repair of duodenal atresia Diamond-shaped anastomosis for duodenal atresia: an experience with 44 patients over 15 years. Open vs laparoscopic repair of congenital duodenal obstructions: a concurrent series. A pediatric case of an unusual type of annular pancreas presenting with duodenopancreatic reflux. Late-onset hypertrophic pyloric stenosis: definition of diagnostic criteria and algorithm for the management. Comparison of preoperative sonography with intraoperative findings in congenital hypertrophic pyloric stenosis. Diagnosis of hypertrophic pyloric stenosis: value of sonography when used in conjunction with clinical findings and laboratory data. Within the spectrum of this disease gastritis, gastroduodenal ulceration, dudodentitis, and villous atrophy have been described. Many studies have attempted to identify the environmental and genetic factors that lead to the abnormal immunomodulatory response that leads to this chronic inflammatory process. However, clinically significant gastroduodenal disease is more frequently described with Crohn disease with an incidence of 0. Most patients will have continuous disease involving the distal portion of the stomach, pylorus, and duodenum. Most children who present with Crohn disease will have classic symptoms of changes in bowel pattern and unexplained weight loss. In the subset who have gastroduodenal involvement, epigastric pain with or without blood-tinged emesis can be common presenting symptoms. Laboratory evaluation of these patients is reflective of a protein-losing enteropathy and nutritional deficiency. Evaluation of the stomach and duodenum with multiple biopsies is important for diagnosis. Irregularity of the evaluated mucosa with the classic cobblestone appearance and subsequent histologic identification of noncaseating granulomas is diagnostic. The mainstay of treatment for inflammatory bowel disease remains immunomodulatory therapy. For those children with gastroduodenal Crohn disease, many studies have shown a benefit of intense acid suppression as well as eradication of any concomitant Helicobacter pylori infection. This can often lead to significant healing when used in conjunction with standard therapies for Crohn disease. In some cases strictures can be managed with endoscopic balloon dilation with an acceptably low rate of perforation. Operative approaches for the treatment of stricture include duodenal strictureplasty and formal bypass via duodenoduodenostomy or gastrojejunostomy. Postoperative complications include anastomotic leak, proximal high-output enterocutaneous fistula, intraabdominal abscess, and recurrent stricture. Developmental posterior enteric remnants and spinal malformations: the split notochord syndrome. Prenatal diagnosis and postnatal resection of intraabdominal enteric duplications. Impact of surgical approach on outcome in 622 consecutive pyloromyotomies at a pediatric teaching institution. Laparoscopic pyloromyotomy for hypertrophic pyloric stenosis: a prospective, randomized controlled trial. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Venlafaxine pharmacobezoar causing intestinal ischemia requiring emergent hemicolectomy. Multiple magnet ingestion as a source of severe gastrointestinal complications requiring surgical intervention. Selective upper endoscopy for foreign body ingestion in children: an evaluation of management protocol after 282 cases. Primary gastric tumors of infancy and childhood: 54-year experience at a single institution. Trends in the prevalence of Helicobacter pylori in symptomatic children in the era of eradication. Superior mesenteric artery syndrome: a rare cause of complete intestinal obstruction in neonates. Superior mesenteric artery syndrome after minimally invasive correction of pectus excavatum: impact of post-operative weight loss. Left paraduodenal hernia causing small bowel obstruction in an adolescent patient. Volvulus of the small intestine caused by right paraduodenal hernia: a case report. Prada-Arias M, Sanchis-Solera L, Perez-Candela V, Wiehoff-Neumann A, Alonso-Jimenez L, Beltra-Pico R. Computed tomography diagnosis of symptomatic right paraduodenal hernia associated with enteric duplication cyst. Definition of phenotypic characteristics of childhood-onset inflammatory bowel disease. Upper gastrointestinal mucosal disease in pediatric Crohn disease and ulcerative colitis: a blinded, controlled study. As such, it is important to understand both the structure and function of the duodenum as it relates to alimentary surgery. This process starts at the beginning of the third week of embryonic development with primitive foregut demarcation from the midgut and hindgut. Early in the second month of gestation, the embryologic midgut migrates ventrally to descend into the yolk sac. Over the next several weeks, the midportion of the intestine elongates faster than the abdominal cavity expands, thereby enlarging the midgut loop, which continues to push into the umbilical cord. As this occurs, the midgut undergoes a counterclockwise 90-degree rotation around the superior mesenteric artery, forming "prearterial" and "postarterial" halves. Following this rotation, the cranial ("prearterial") segment of midgut (future duodenum and proximal small bowel) lies to the right of the caudal ("postarterial") segment (future colon). The cranial ("prearterial") segment continues to elongate into the umbilical cord until the tenth gestational week, after which the midgut returns into the abdomen. The cranial limb migrates back into the abdomen first, causing the duodenum to pass behind the superior mesenteric artery. During its return, the midgut rotates another 180 degrees (total rotation = 270 degrees). At the completion of these movements, the colon is situated anterior to the superior mesenteric artery, and the cecum is located at the level of the iliac crest. From the twelfth week of gestation until after birth, the colon elongates while the cecum remains in its original position. This colonic growth effectively produces an "ascent" of the hepatic flexure toward the right upper quadrant that seems like a cecal "descent. The future duodenum lies between the transverse septum of the ventral mesentery (the future primordium of the liver, the bile ducts, and the ventral pancreatic bud) and the dorsal mesentery (the future dorsal pancreatic bud). Initially, the duodenum is composed of a single layer of endodermal cells surrounded by undifferentiated mesenchymal cells. By the end of the fourth week of gestation, the duodenal mucosa begins to proliferate along the ventral wall near the origin of the hepatic diverticulum. During midgut rotation, mesenchymal tissue beyond the first portion of the duodenum increases along the dorsal aspect of the duodenum, fixing it to the retroperitoneum beyond this point. During fixation, this dorsal mesentery transforms into an avascular plane of loose connective tissue known as the fascia of Treitz (not to be confused with the ligament of Treitz). This plane is entered when lifting the duodenum medially during a Kocher maneuver. Later (fifth gestational week) the connecting elements between the hepatic diverticulum and the duodenum form the bile duct and, ultimately, the cystic duct and the gallbladder. Around the ninth week of gestation, rapid hepatic growth occurs secondary to the hematopoietic function of the liver and the formation of multiple hepatic sinusoids. At this time, the ventral mesentery produces the lesser omentum, the falciform ligament, and the hepatoduodenal ligament; these structures envelop the portal triad as it extends from the liver. Other structures within the portal triad include the hepatic artery and the portal vein. The portal vein develops from the primitive paired vitelline veins that arise in the yolk sac and pass up the body stalk to enter the developing heart. Two extrahepatic cross-connections develop between the paired vessels: the cranial anastomosis lies behind the duodenum and the caudal anastomosis passes in front of the duodenum. The name is derived from the Latin phrase intestinum duodenum digitorum, or "intestine of twelve digits. Although it is the shortest segment of small bowel, the duodenum is the initial site of contact for gastric secretions, bile, and digestive enzymes from the common bile duct and the pancreas. Thus it plays an important role in the regulation of digestion, absorption of essential micronutrients and macronutrients, and bowel motility. Its relationships to the major structures of the upper abdomen lend it to exposure during a large number of gastrointestinal surgical interventions. This preduodenal caudal anastomosis can persist as the portal vein, leading to the rare congenital anomaly known as a preduodenal portal vein. One week later the ventral pancreatic primordial bud arises at the base of the hepatic diverticulum. At the end of the sixth week, these two primordia fuse as the ventral pancreas migrates below and behind the dorsal pancreatic segment; these changes form portions of the adult pancreatic head and uncinate process.
In this group of patients there were no patients with dysplasia or buried Barrett pulse pressure 60 mmhg buy olmesartan toronto. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia a randomized clinical trial blood pressure medication used in pregnancy order olmesartan 40 mg. It has been stated that for ablation to be preferable to surveillance heart attack at 20 olmesartan 20 mg buy online, there should be a decreased risk of the important endpoints such as cancer heart attack full movie purchase olmesartan 40 mg free shipping, or worse cancer death; the decrease in risk should be durable without the need for repeated treatments blood pressure top number low 20 mg olmesartan for sale, and the treatment should be relatively easy to administer, without excessive cost or treatment risk. For patients with intermediate or low risk of malignant transformation, the decision between continued surveillance only or ablation with surveillance is complicated by the lack of comparative studies with the important endpoints of esophagectomy or cancer death. A prospective randomized trial of two different endoscopic resection techniques for early stage cancer of the esophagus. Meta-analysis of endoscopic submucosal dissection versus endoscopic mucosal resection for tumors of the gastrointestinal tract. Safety and efficacy of endoscopic mucosal therapy with radiofrequency ablation for 45. Ablation for Patients With Barrett or Dysplasia argon plasma coagulation and photodynamic therapy: a randomized prospective trial assessing efficacy and cost-effectiveness. Safety, tolerability, and efficacy of endoscopic low-pressure liquid nitrogen spray cryotherapy in the esophagus. Characterization of buried glands before and after radiofrequency ablation by using 3-dimensional optical coherence tomography (with videos). A comparison of endoscopic treatment and surgery in early esophageal cancer: an analysis of Surveillance, Epidemiology and End Results data. Chronic inflammation due to environmental exposures causes progression to dysplasia and eventually malignant change. Across all races, the death rate is approximately 5 times higher in men than women. The overall relative 5-year survival rate has increased from 4% in the 1970s to 18. With complete surgical resection, the relative 5-year survival rate is approximately 90% for pThis tumors, 75% for pT1, 45% for pT2, 30% for pT3, and 10% to 15% for pT4 disease. Over the past few decades, there has been a major shift in the incidence of esophageal cancer worldwide with trends differing by histologic subtype. The majority of new cases are diagnosed in people aged 65 to 74 years with a median age at diagnosis of 67. The age-adjusted incidence rate of esophageal cancer is highest in white and black men (7. In the United States alone, esophageal cancer accounts for 1% of new cancer diagnoses and 2. The two most common subtypes of primary esophageal cancer include adenocarcinoma and squamous cell carcinoma. These differ tremendously in their natural history, epidemiologic pattern, and risk factors. These differences may be accounted for by changes in the prevalence of known risk factors, such as gastroesophageal reflux and obesity. This article reviews the epidemiologic pattern, risk factors, and clinical manifestations of esophageal cancer and its histologic subtypes. As such, several studies have identified a correlation between obesity and the risk of esophageal cancer. In high-risk areas, such as countries within the esophageal cancer belt, poor nutritional status, low intake of fruits and vegetables, and drinking hot beverages are suggested to be partially responsible. The risk of cancer also increases as the segment length of Barrett increases, with long-segment Barrett (3 cm) having a transition rate of 0. In fact, studies have shown that reflux of bile salts also contributes to the development of Barrett esophagus. Similarly, it cannot be explained by reclassification of tumors of the gastric cardia because the incidence of tumors below the gastroesophageal junction has also increased over the past three decades. The increase in esophageal cancer may be explained by changes in the prevalence of its known risk factors. The most notable change has been in the increased prevalence of obesity, especially in the United States. Earlystage tumors are typically asymptomatic, which is why over 50% of patients present with regionally advanced or metastatic disease. Patients with metastatic disease may have hepatomegaly, pleural effusion, or lymphadenopathy, particularly in the left supraclavicular fossa (Virchow node). Several theories have been proposed to explain the changing epidemiology of esophageal cancer worldwide. Long-term esophageal cancer risk in patients with primary achalasia: a prospective study. Epidemiologic evidence of the protective effect of fruit and vegetables on cancer risk. Fruit and vegetable intake and esophageal cancer in a large prospective cohort study. Prospective study of risk factors for esophageal and gastric cancers in the Linxian general population trial cohort in China. Oesophageal cancer in Golestan Province, a high-incidence area in northern Iran-a review. High-temperature beverages and foods and esophageal cancer risk-a systematic review. Dietary supplement use and risk of neoplastic progression in esophageal adenocarcinoma: a prospective study. Nonsteroidal antiinflammatory drug use reduces risk of adenocarcinomas of the esophagus and esophagogastric junction in a pooled analysis. Nonsteroidal antiinflammatory drugs and the esophageal inflammation-metaplasiaadenocarcinoma sequence. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U. General and abdominal obesity and risk of esophageal and gastric adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition. A meta-analysis of body mass index and esophageal and gastric cardia adenocarcinoma. Squamous esophageal histology and subsequent risk of squamous cell carcinoma of the esophagus. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. Oesophageal cancer incidence in the United States by race, sex, and histologic type, 19772005. The synergistic effects of alcohol and tobacco consumption on the risk of esophageal squamous cell carcinoma: a meta-analysis. Associations of duration, intensity, and quantity of smoking with adenocarcinoma and squamous cell carcinoma of the esophagus. A prospective study of tobacco, alcohol, and the risk of esophageal and gastric cancer subtypes. Risk of esophageal adenocarcinoma in achalasia patients, a retrospective cohort study in Sweden. Gastroesophageal reflux, Barrett esophagus, and esophageal cancer: scientific review. American Gastroenterological Association medical position statement on the management of gastroesophageal reflux disease. Association between medications that relax the lower esophageal sphincter and risk for esophageal adenocarcinoma. Non-steroidal anti-inflammatory drugs, lower oesophageal sphincter-relaxing drugs and oesophageal cancer. Helicobacter pylori infection and esophageal cancer risk: an updated meta-analysis. An inverse relation between cagA+ strains of Helicobacter pylori infection and risk of esophageal and gastric cardia adenocarcinoma. Comparing trends in esophageal adenocarcinoma incidence and lifestyle factors between the United States, Spain, and the Netherlands. Esophageal cancer: results of an American College of Surgeons Patient Care Evaluation Study. Esophageal cancer remains one of the deadliest cancers with an overall 5-year survival rate estimated to be less than 18%. Although new technologies have upgraded staging accuracy, the best overall approach remains controversial. This article describes the current staging classifications and methods for esophageal cancer and highlights some of the difficulties and controversies. It extends from the hypopharynx, posterior to the trachea and the heart, to the stomach, passing through the esophageal hiatus. Through its descent, three critical anatomic points of narrowing are identified: the cricopharyngeus muscle, the bronchoaortic constriction, and the esophagogastric junction, which are also the most common sites of iatrogenic and mechanical perforation. The esophagus, a muscular tube, is composed of three general layers as follows: mucosa (stratified squamous epithelium), submucosa, and muscularis propria. The esophagus also can be divided into thirds with 50% of adenocarcinoma occurring in the lower third. Tumors in the middle or upper esophagus are considered higher stage compared with the lower one-third of the esophagus. The cervical esophagus extends from the esophageal orifice (lower border of the cricoid cartilage) to the sternal notch (or thoracic inlet). Typical endoscopic measurements for the cervical esophagus from the incisors are from 15 to less than 20 cm. The upper thoracic esophagus extends from the sternal notch to the azygos vein arch. The middle thoracic esophagus is bordered superiorly by the lower border of the azygos vein and inferiorly by the inferior pulmonary vein. Lymph node involvement and the number of lymph node metastases are important prognostic factors. The esophagus has a complex pattern of a dense and rich interconnected network of lymphatic vessels deep within submucosa that communicate freely longitudinally and transversally with the lymphatics of the muscular layers; thus, the pattern of lymph node metastases is very complex. Lymphatic channels in the submucosa facilitate the longitudinal spread of neoplastic cells along the esophageal wall. They can drain to cervical, tracheobronchial, mediastinal nodes, and gastric and celiac nodes. Many patients will present late in the disease process with unresectable tumors or distant metastasis. The most common metastatic sites are retroperitoneal or celiac lymph nodes, liver, lungs, and adrenals. Accurate staging of esophageal cancer is important as it impacts prognosis and facilitates staged directed treatment. Staging is done on the basis of depth of penetration in the wall of the esophagus or stomach (T stage), the number of lymph nodes involved (N stage) and evidence for metastatic spread to other organs (M stage). Anatomic location of the cancer in the esophagus, R status (Resection margins) and G status (Tumor differentiation) can also play an important role in assigning tumor stage and deciding on treatment approach. Staging that is assigned following investigation is typified as "clinical stage"; staging following endoscopic or surgical resection is classified as "pathologic stage. The results of tumor staging are best reviewed in a multidisciplinary tumor board where all the information can be assessed and appropriate treatment can be assigned in a multidisciplinary fashion. These include pretreatment stage or clinical stage, and postsurgical or pathologic stage. In addition, stage is further classified according to neoadjuvant therapy or at the time of recurrence. The clinical stage or pretreatment stage is the extent of disease defined by diagnostic studies such as physical examination, imaging tests, endoscopic examination, biopsies of the primary tumor, and surgical exploration without resection of the affected areas. The pathologic stage is defined by the same diagnostic studies used for clinical staging supplemented by findings from surgical resection and histologic examination of the surgically removed tissues. The posttherapy stage documents the extent of the disease after neoadjuvant therapy or when systemic therapy or radiation is the only treatment. The posttherapy stage may be recorded as clinical or pathologic, depending on the source of posttreatment information. The nomenclature is recorded by adding the prefix "yc" or "yp" such as: ycT, ycN, ycM, ypT, ypN, and ypM. Restaging is used to determine the extent of the disease following the completion of neoadjuvant therapy, and if a cancer recurs after treatment. Residual tumor is denoted by the symbol "R"; it reflects the effect of therapy and the completeness of surgical resection, and is a strong predictor of prognosis. In the United States, which uses the American College of Pathology designation of R1, it is "tumors at the surgical margin. Occasionally they originate from heterotopic gastric mucosa in the upper esophagus, or from mucosal and submucosal glands. It is a rare kind of malignancy characterized by mixed glandular and squamous differentiation as well as a propensity for aggressive clinical behavior. Cancers that are "well-differentiated" tend to grow and spread at a slower rate than tumors that are "undifferentiated" or "poorly differentiated. T stage is important in the prognostication and is crucial to determining suitability for surgical resection and establishing a treatment plan. Different N stages are defined as: · N0:Nopositivenode · N1:1to2nodes · N2:3to6nodes · N3:7ormorenodes There is no consensus on the ideal number of nodes that must be resected for optimal staging. Data suggest that the number of lymph nodes recovered-rather than their location-is an independent predictor of survival after esophagectomy. Moreover, patients who had 30 or more lymph nodes examined had significantly lower mortality than any other groups.
Living donor liver transplantation this was introduced because of the shortage of small cadaveric grafts for children arrhythmia reference guide buy olmesartan 20 mg online. This technique was used originally largely in children hypertension lifestyle changes generic olmesartan 20 mg on line, often with biliary atresia [84] hypertension orthostatic olmesartan 10 mg order online, graft before opening the blood supply to the liver heart attack 2o13 40 mg olmesartan purchase otc. Hepatic arterial anomalies are frequent blood pressure after exercise discount olmesartan online amex, and vessel grafts from the donor should be available for arterial reconstructions. In this example the main vascular and biliary structures are attached to the right lobe. Increasing use of left lobe grafts for adult recipients is being used in some centres, with technical modification to decrease risk of smallforsize syndrome. In small adults and children, the recipient undergoes an extended left hepatectomy and a left lateral segment or left lobe graft is used. Complications, particularly portal vein thrombosis and primary graft nonfunction, are increased. Auxiliary liver transplantation offers the possibility of a lifetime free of immunosuppressive therapy. Domino liver transplantation Structurally normal livers are removed to control a metabolic defect such as familial amyloid polyneuropathy [95]. Such a liver may be offered for transplant to an older recipient who has given full consent. The consequences of the metabolic defect will be delayed for between 10 and 20 years although there are reports of this occurring within an earlier timeframe in the transplant recipient [55]. Hepatocyte transplantation Transplantation of human hepatocytes is being developed to treat metabolic liver disease where a supply of normally functioning liver cells can correct a genetic deficiency [97]. Transplanted hepatocytes may be used to replace a missing or inactive enzyme, as in the CriglerNajjar syndrome [98], glycogen storage but this has been reduced due to the use of deceased donor split livers. The lack of donor liver grafts also contributed to the development of live liver donation in many countries in Asia. There are important ethical considerations concerning the donor, who is sometimes a relative, and must give free and informed consent. There must be a patient advocate, a doctor who has no connection with the recipient team. Livingrelated donation has been extended to the adult, using right, and more recently left, lobe grafts for patients with wellcompensated cirrhosis and mild portal hypertension, and in acute liver failure when a cadaveric donor is not available at short notice [85]. The risk of death did not vary based on the portion of liver donated (2/1000 for left lateral segment, 2. Longterm mortality of live liver donors was comparable to kidney donors and healthy participants in the National Health and Nutritional Examination Survey with a rate of 1. The required size of the donated liver is much greater for an adult than for a child. Below this limit, smallforsize syndrome, which is related to increased inflow from the portal vein through a reduced liver mass can occur. Despite the increased 742 Chapter 37 disease type 1a [99], and urea cycle disorders [100], or to inactivate a diseaseinducing gene or overexpress a normal gene [101]. Xenotransplantation Several nonhuman livers including pig, baboon, and chimpanzee livers have been transplanted into humans [103]. Starzl carried out the first chimpanzee to human liver transplantation in 1966 and in 1992, his patient survived for 70 days following a baboon liver transplant [104]. The main limitation is immunological, including hyperacute and delayed xenograft rejection and Tcell dependent xenograft rejection. Various control strategies are under investigation [105] but the problems will be difficult to overcome. Zoonotic infections, particularly viruses (especially porcine endogenous retroviruses) may be introduced with the xenotransplant. Liver transplantation in paediatrics the mean age is about 3 years, but successful transplant can be performed in infants within the first year of life [106]. The scarcity of paediatric donors necessitates adult reducedliver or splitliver donations. These are given with corticosteroids and/or azathioprine or mycophenolate mofetil. The calcineurin inhibitor agents, tacrolimus and ciclosporin are the mainstay of maintenance immunosuppression. Electrolyte disturbances include hyperkalaemia, hyperuricaemia, and hypomagnesaemia. Other complications include hypertension, weight gain, hirsutism, gingival hypertrophy, and diabetes mellitus. Ciclosporin and tacrolimus can interact with other drugs leading to changing blood levels (Table 37. It is better than ciclosporin in terms of patient and graft survival [108,109], and there is less chronic rejection. Sideeffects include nephrotoxicity, diabetes, diarrhoea, nausea, and vomiting, but less hypertension than with ciclosporin. Neurological complications (tremors and headache) are more prominent with tacrolimus compared to ciclosporin. The immunosuppressive effects of ciclosporin and tacrolimus are related to the total drug Table 37. Multiple therapy is usually given and the choice varies between centres and is nowadays tailored to both the individual patient and to the underlying disease. There is large interindividual variability in the drug metabolism and thus 12h trough levels are used to estimate the drug exposure. Mycophenolate mofetil, a noncompetitive inhibitor of inosine monophosphate dehydrogenase, is the most common additional agent used for maintenance immunosuppression. The main side effects include gastrointestinal symptoms and bone marrow suppression. Mycophenolate mofetil use is associated with an increased risk of first trimester spontaneous abortions and congenital malformations and thus it is advised that women discontinue this medication prior to conception [110]. The sideeffects include myelosuppression, cholestasis, peliosis hepatis, perisinusoidal fibrosis, and nodular regenerative hyperplasia. Studies have shown that the use of mycophenolate mofetil and concurrent reduction in calcineurin inhibitor therapy results in improvement in renal function when performed more than 1 year post liver transplant [111,112]. The use of sirolimus in the immediate posttransplant period is contraindicated given higher incidence of graft loss, death, hepatic artery/portal vein thrombosis, and sepsis. However, a number of studies have shown the safety of these agents is improved following the first month after transplantation [113]. The use of everolimus in combination with reduced dose tacrolimus 1 month posttransplant compared with standard exposure tacrolimus resulted in significantly improved renal function out to 36 months posttransplant [114]. The complete tacrolimus withdrawal arm in this study did have higher rates of acute rejection and thus everolimus monotherapy is not recommended. Sideeffects include pancytopenia, impaired wound healing, dyslipidemia, and oral and gastrointestinal ulcers. Previously, antilymphocyte globulin and Tcell antibodies were given to prevent acute rejection. These receptors are expressed only by activated lymphocytes and the monoclonal antibodies are given early to reduce acute rejection. The difficulties in balancing the risks of too much immunosuppression, which increases infections and risk of malignancy, with too little immunosuppression, which increases graft rejection, are still a major issue in liver transplantation. The tendency over past decades has been to reduce maintenance immunosuppression without increased loss of grafts. Tolerance Donor cells have been identified in the blood of recipients of liver transplantation. This chimerism could influence the host immune system with development of tolerance to donor tissues. After a successful 5year survival of a primary graft, between 15% and 30% of patients may be able to stop immunotherapy in the subsequent 3 years. The other twothirds developed graft abnormalities [117]; chimerism was not associated with tolerance. However, currently these patients cannot be predicted sufficiently well to plan withdrawal of immunosuppression. Postoperative course this is not always without complications, particularly in the adult. Further surgery such as for control of bleeding, biliary reconstruction, or draining abscesses may be necessary. The main indications are primary graft failure, hepatic arterial thrombosis, chronic rejection, and recurrent disease. Poor results are also related to the amount of blood products required during surgery, the need for renal support posttransplant, and repeated rejection. The causes of death are surgical technical complications, bacterial or fungal sepsis (either immediate or late), biliary leaks and hepatic rejection, with or without infections, often related to overimmunosuppression. The patient usually spends about 12 weeks in hospital and is usually fully rehabilitated by 6 months. Quality of life is usually excellent in the majority of patients with return to normal at home and work. More than 87% of paediatric survivors are fully rehabilitated with normal growth, both physical and psychosexual. Technical complications Surgical complications are most frequent in children with small vessels and bile ducts. Routine Doppler ultrasonography is used for detection of hepatic arterial, hepatic venous, portal venous or inferior vena caval stenosis or thrombosis. This is more likely if the removal of a diseased liver has left a raw area on the diaphragm, or if there have been adhesions from previous surgery or infection, or with split liver lobes. Alternatively it may be silent, presenting several weeks later with biliary complications [125] including leaks and strictures, and recurrent bacteraemia and abscesses. It may be silent, presenting as variceal bleeding weeks to months after the transplant. Hepatic vein occlusion is common in patients who have had liver transplantation for the BuddChiari syndrome. Occasionally, there is stricturing of the suprahepaticcaval anastomosis and this can be treated by balloon dilation. Biliary tract complications Bile secretion recovers spontaneously over a 1012day period and is strongly dependent upon bile salt secretion. The incidence of complication is 634% of all transplants, usually during the first 3 months [126,127]. The management requires a multidisciplinary approach involving transplant surgeons, endoscopists, and interventional radiologists. The majority of biliary complications can be resolved endoscopically [128], but it is important not to delay surgical intervention for a permanent biliary repair. Extrahepatic anastomotic strictures present after about 5 months as intermittent fever and fluctuating serum biochemical abnormalities. They develop in the donor common hepatic duct, with variable extension into the main intrahepatic ducts. On cholangiography, the wall of the duct may appear irregular and hazy, presumably reflecting areas of necrosis and oedema. They are associated with multifactorial damage to the hepatic arterial plexus around bile ducts. Peribiliary arteriolar endothelial damage contributes to segmental microvascular thrombosis and hence to multiple segmental biliary ischaemic strictures. Foreign bodies such as T tubes and stents may serve as a nidus for stone formation. An area of necrotic, infarcted hepatocytes with haemorrhage adjoins normal liver tissue. The causes include preexisting kidney disease, intraoperative or postoperative hypotension 746 Chapter 37 and shock, sepsis, suboptimal donor quality, primary non function, acute hepatic arterial thrombosis, nephrotoxic antibiotics, and ciclosporin or tacrolimus. Early reduction of glomerular filtration rate, such as less than 60 mL/min at 3 months, is strongly associated with subsequent renal failure, which may require kidney transplantation [133]. Pulmonary complications In infants, and rarely in adults, death during liver transplantation may be related to platelet aggregates in small lung vessels. Intravascular catheters, platelet infusions, and cell debris from the liver may contribute [134]. In the first 30 days, pneumonia is usually due to methicillinresistant Staphylococcus aureus, Pseudomonas, and less frequently Aspergillosis. In one report, 87% of patients with pneumonia required ventilation and 40% were bacteraemic. Pyrexia, leukocytosis, poor oxygenation, and cultures of the bronchial secretions indicate pneumonia and demand antibiotic therapy. The hepatopulmonary syndrome is usually corrected by liver transplant but only after a difficult posttransplant course with prolonged hypoxaemia, mechanical ventilation, and intensive care [136]. Portopulmonary hypertension usually requires continued therapy for some weeks, but improves after liver transplantation. Nonspecific cholestasis this is frequently seen in the first few days, with the serum bilirubin peaking at 1421 days. Liver biopsy suggests extrahepatic biliary obstruction but cholangiography is normal. Factors involved include mild preservation injury, sepsis, haemorrhage, and renal failure. Rejection Immunologically, the liver is a privileged organ with regard to transplantation, having a higher resistance to immunological attack than other organs.
The right crus is identified mrf-008 hypertension cheap olmesartan 20 mg mastercard, and an area approximately 2 to 3 cm below the gastroesophageal junction on the medial border of the right crus is opened with a Harmonic scalpel or similar energy device to allow the beginning of a tunnel for the lap band posterior to the stomach arrhythmia ecg order olmesartan with visa. There is a fair amount of fibrous tissue in this area blood pressure yoga order 10 mg olmesartan otc, and the goal is to develop a tunnel within this tissue that allows for some posterior security of the band heart attack low blood pressure purchase generic olmesartan pills, preventing migration in either direction blood pressure jump olmesartan 20 mg buy visa. Once the grasper has emerged in the area of the angle of His, the band itself is introduced into the abdomen via the 15-mm port. The band is then placed around the proximal stomach, 2 cm below the gastroesophageal junction, and with just that small amount of stomach above the top of the band. The fundus is now brought up over the left lateral and anterior portions of the band to cover the band and secure it further into position. Care should be taken to avoid placing the fundus over the buckle of the band because erosion may occur. The tubing is now brought out through the abdominal wall in a location where the port will be sited. We have favored placing the port just below the costal margin in the epigastric region. The tubing is brought out from the abdomen through a stab wound on the medial side of this incision, as far to the end of the incision as possible. This allows the tubing to emerge through the fascia and take a natural slow bend medially to be joined to the port. Securing the tubing to the port and then the port to the fascia in the incision site completes the operation except to visually confirm that addition of saline to the system causes the band to expand and not leak. However, complications can occur, and these have been well described in the literature. Any such symptoms of new onset need to be investigated promptly for either simple excessive restriction or, more commonly, prolapse of the band. Prolapse occurs when the stomach below the band herniates up into the central lumen of the band and too much stomach is forced into this space. In severe cases the prolapse can lead to ischemia and gangrene of the prolapsed portion of the stomach. Chronic prolapse is seen at times with surprisingly large protrusions of the distal stomach up and over the edge of the gastric band. Prolapse can occur at any time after the procedure, and its incidence slowly rises with duration of the band being in place. If doubt exists, a low-volume Gastrografin or barium swallow will confirm the diagnosis. This will, in most cases of acute prolapse, provide enough reduction in the restriction of the prolapsed stomach to allow it to slip back down through the band and resume its normal position. However, if removal of all fluid does not produce immediate relief of symptoms by the patient, a swallow study is indicated. If the swallow shows a large and persistent prolapse, emergent surgical therapy is indicated to laparoscopically reduce the prolapse and prevent gastric ischemia. A laparoscopic approach to freeing the buckle of the band, unbuckling the system, reducing the prolapse to its appropriate location, and repositioning and rebuckling the band is quite feasible. Chronic stenosis or band placement too high onto the distal esophagus may produce esophageal obstruction and dilation. Resolution of the obstruction will usually result in the esophagus regaining its normal size. Failure to secure the port to the fascia can result in the port turning in the subcutaneous space and being unable to be accessed for further adjustments. When such adjustments are made, a good rule of thumb is to have the patient drink several swallows of water quickly after the adjustment is made. If the patient feels the water stop and give a sensation of partial blockage, then the adjustment is too tight and must be loosened. Optimal restriction varies from patient to patient, but in general a goal of restriction to one cup of food or less at a meal and production of satiety for at least a few hours after eating are the goals of an optimal adjustment. It achieved initial popularity in the mid 1970s and has remained a standard operation since that time. The technique of creating the gastrojejunostomy and the length and location of the Roux limb has varied from surgeon to surgeon. No optimal technique or configuration has emerged, although some differences have been shown. Its performance using a laparoscopic approach has clearly been an improvement over the open approach, as with all other operations where minimal access has been used. Elimination of incisional hernias, decreased pain and recovery time, and decreased overall complication rates and mortality have all been confirmed with using the laparoscopic approach. Failure of a trial of dieting and mental stability are also considered standard criteria. Other criteria vary among surgeons and institutions, including upper and lower age limits, size limits, and requirements of cessation of addictive habits. The mesentery is then further divided with the Harmonic scalpel to obtain as deep a division of the mesentery as possible without encountering the very large vessels at the base of the mesentery. The proximal end of the Roux limb is then marked by suturing a small Penrose drain to it. Then the mesenteric defect at the enteroenterostomy is closed with a running permanent suture. The transverse colon mesentery is now grasped and elevated, exposing the lower portion of the mesentery near the ligament of Treitz. A defect is made in the mesentery to the left and a few centimeters above the ligament of Treitz. This location usually avoids major vessels, but the surgeon must be aware of the vascular anatomy, if visible, and cautious not to disrupt it unnecessarily. Openings between mesenteric vessels are easier to find than dealing with bleeding from major mesenteric vessels. Once the mesentery has been opened to expose the lesser sac, the posterior surface of the stomach can be seen. It is grasped and pulled out of the mesenteric defect a few centimeters, after which the plane below the stomach is confirmed with a grasper. Usually if one can pass 4 cm of bowel or more past the cut edge of the mesentery, that will suffice for later retrieval. It is very easy to have the bowel twisted a full 180 degrees or more between first passing it to the left upper quadrant then retrieving it to pass it through the transverse colon mesentery. The mesentery of the Roux limb must be visually confirmed without a doubt as being straight and vertical as the limb is passed superiorly through the transverse colon mesentery. The Harmonic scalpel is used to create an opening in the mesentery along the lesser curvature of the stomach. However, for very large patients, creating this opening at the incisura is advisable because the longer gastric pouch is often needed to allow the Roux limb to easily reach the proximal stomach without tension. Then I prefer to size the pouch with an Ewald tube (30 French) and place the stapler close to but not directly adjacent to the tube, which is visible by the contour it creates on the gastric surface. It is important to exclude the fundus from the proximal part of the newly created gastric pouch. Similarly, the anesthesiologist needs to double confirm there are no temperature probes or orogastric tubes in the stomach other than the Ewald tube. If it is not, the inferior surface of the transverse colon mesentery must again be exposed and the Roux limb passed into the retrogastric space again. I continue to use a retrogastric retrocolic location of the Roux limb due to the fact this is the shortest distance from between jejunum and proximal stomach. A more popular approach is to bring the Roux limb directly anterior to both transverse colon and distal stomach and create the gastrojejunostomy. This approach is technically easier, except when the mesentery of the Roux limb is short and there is difficulty in stretching the Roux limb to reach the proximal gastric pouch. For the retrocolic retrogastric approach, I now place the proximal suture line of the Roux limb directly adjacent to the distal part of the proximal gastric pouch. The distal 5 cm of gastric pouch is then tacked to the side of the proximal 5 cm of the Roux limb with a running absorbable suture. We have found that the linear stapler is associated with an insignificant incidence of postoperative stenosis, whereas the circular stapler in our experience yielded a 10% or higher stenosis rate. The Ewald tube serves as a good backstop against which to make a gastrotomy in the end of the pouch. We have not found that restricting the anastomotic size has any relationship to long-term postoperative weight loss. The staple defect is closed with a running layer of absorbable suture and reinforced with a second such layer. An intraoperative leak test is now performed by having the anesthesiologist forcefully inject a methylene blue dye solution into the lumen of the proximal pouch, after having readvanced the tip of the Ewald tube to that level. For this procedure, the Roux limb must be secured to the jejunum at the ligament of Treitz to prevent the Roux limb from telescoping up into the retrogastric space and becoming kinked and obstructed. Further sutures between the two limbs are placed, as well as sutures to close the space between the left lateral side of the Roux limb and the transverse colon mesentery. Port sites 12 mm or larger are closed with laparoscopically passed sutures for the fascia. Postoperative care includes providing adequate analgesia, early ambulation, liquids on postoperative day 1, and discharge on postoperative day 2 on our phase 2 gastric bypass diet (blenderized food). I still perform a Gastrografin swallow on the first postoperative day to confirm no distal obstruction, as well as no obvious leak. There was a significant improvement in obesity-related comorbid medical problems for all problems assessed after 10 years. Early small bowel obstruction may be in the 2% range and can be associated with major staple line disruptions. Internal hernias can lead to strangulation of large sections of the small bowel mesentery, with death or short gut syndrome resulting. The surgeon who sees a patient with a picture of small bowel obstruction after previous gastric bypass is obligated to prove that patient does not have an internal hernia and strangulation obstruction. Early operative intervention in this setting is the standard of care, whereas conservative therapy with nasogastric suction and intravenous fluids may allow strangulation to proceed to gangrene of the bowel. Use of absorbable suture, treatment for Helicobacter pylori, avoidance of nonsteroidal and aspirin-containing medications, and larger than optimal gastric pouch size all may contribute to the formation of marginal ulcers. The classic symptom of the problem is unremitting epigastric pain, unrelated to eating. However, persistent or chronic ulcers may result in obstruction or gastrogastric fistula to the defunctionalized stomach. In most cases, re-creation of the gastrojejunostomy and resection of the ulcer and any fistula is performed. However, in selected cases of chronic or repeated ulcers, takedown of the gastrojejunostomy and performance of a gastrogastrostomy, with gastric narrowing (converting to sleeve gastrectomy) or without gastric narrowing, may be the best option. Others never establish a firm enough change in eating and exercise habits to sustain the initial weight loss produced by the operation. Options for revisional surgery include performing further restrictive measures endoscopically or surgically or adding a malabsorptive component to the anatomy. Patients who underwent the new procedure were noted to have increased weight loss. The sleeve gastrectomy involves resection of the greater curvature of the stomach, leaving a small, tubular stomach based on the lesser curvature blood supply. It is easy for patients to understand and relatively straightforward for surgeons to perform. Because there is no malabsorptive component, patients are less likely to develop nutrient deficiencies. In addition, because the operation does not bypass any intestinal segments, there are no potential spaces for internal herniation. The indications, patient preparation, and positioning are similar to gastric bypass. Port placement is also similar to gastric bypass, although fewer 12-mm ports are needed because stapling is done through only one or two ports. Retraction of the left lobe of the liver provides exposure of the proximal stomach and the gastroesophageal junction. The pylorus is identified, and a position on the greater curvature of the stomach 4 cm from the pylorus is selected for the initial dissection. Alternatively, dissection is begun on the greater curvature in the mid-body and carried back to this point. Ultrasonic shears or a bipolar energy device is used to enter the lesser sac and divide the gastroepiploic arcade proximally from the point of entry along the entire greater curvature of the stomach, including the short gastric vessels. Division of the phrenoesophageal ligament completes mobilization of the fundus and allows for detection of a hiatal hernia. If one is discovered, the distal esophagus is freed of mediastinal attachments and brought into the abdomen. Dissection of posterior gastric adhesions to the body of the pancreas and retroperitoneum completes mobilization of the body of the stomach. Prior to stapling, any previously placed orogastric tubes are removed and the anesthesiologist inserts a bougie. With the assistance and guidance of the surgeon, it is positioned along the lesser curve and directed to the pylorus. The size of the bougie dilator varies from 32 to 50 French, but 36 French is the most common size. An initial linear stapler load is introduced through a right upper quadrant port, and the sleeve resection is begun at a point 4 to 5 cm proximal to the pylorus. We feel that matching the staple height to the thickness of the tissue aids in hemostasis. Care is taken not to staple too close to the incisura angularis because stenosis is common at this level.
40 mg olmesartan purchase free shipping. Top 10 Best Blood Pressure Monitor in India with price 2019 | Digital Blood Pressure Machine.
References
- American College of Sports Medicine. Guidelines for Exercise Testing and Prescription . 9th edition. (2013). Baltimore, MD: Lippincott Williams & Wilkins. 16.
- Vogt J, Rupprath G, Grimm T, et al. Qualitative and quantitative evaluation of supravalvular aortic stenosis by cross sectional echocardiography. Pediatr Cardiol. 1982;3:13-7.
- Putensen C, Mutz N, Putensen-Himmer G, et al. Spontaneous breathing during ventilator support improves ventilationperfusion distributions in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;159: 1241-1248.
- Joy JL, Baysal AI, Oh SJ. Reflex improvement after exercise in the Eaton-Lambert syndrome. Muscle Nerve. 1987;10:671-672.
- Wedzicha JA, Calverley PM, Seemungal TA, et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med 2008; 177: 19-26.
- D'Acunto C, Gurioli C, Neri I. Plaque stage mycosis fungoides treated with bexarotene at low dosage and UVBNB. J Dermatolog Treat 2010;21(1):45-48.
- Faris R, Flather MD, Purcell H, et al. Diuretics for heart failure. Cochrane Database Syst Rev. 2006;(1):CD003838.
- Veenhof AAFA, van der Peet DL, Cuesta MA: Perineal hernia after laparoscopic abdominoperineal resection for rectal cancer: Report of two cases. Dis Colon Rectum 50:1271, 2007.