
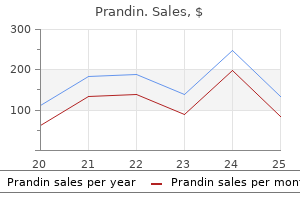
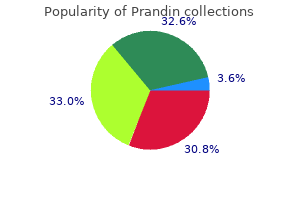
Prandin
| Contato
Página Inicial
Eric Lee Nuermberger, M.D.
- Professor of Medicine
https://www.hopkinsmedicine.org/profiles/results/directory/profile/0008886/eric-nuermberger
It is now thought that rodcone coupling forms an alternative roddriven pathway that may be important at intermediate light intensities diabetes symptoms passing out 2 mg prandin order overnight delivery, in the mesopic range diabetes symptoms pathophysiology order prandin with american express. In the human diabetes signs and symptoms purchase prandin with mastercard, however diabetes mellitus en ingles buy prandin 1 mg with mastercard, the adaptation dependence of these changes has a photopic (cone) signature diabetes signs uk cheap prandin 0.5 mg line. Rodcone coupling also is very dynamic and influenced by circadian rhythms, increasing at night and decreasing during the day, due to the influence of dopamine. From the viewpoint of signal information, the sign of the photoreceptor response makes no logical difference; photoreceptors produce graded responses modulated around the mean light level. When a photon is absorbed, the visual pigment is activated and then a cascade of other biochemical events is triggered. Thus, glutamate uptake also plays a key role in retinal neurotransmission because the clearance of glutamate must be rapid to provide a fast postsynaptic response to light. Glutamate, with its library of postsynaptic receptors, seems particularly suitable to orchestrate the large variety of postsynaptic responses at the cone pedicle. Rods operate in a manner essentially similar to cones: they hyperpolarize in response to light increases, albeit there are many molecular differences. However, everything about the rod pathway in the retina is designed for maximum sensitivity. Depending on the species, about 20100 rods converge on to a single rod bipolar cell87,88 and this high convergence also contributes to the high sensitivity of the rod pathway. If 100 rods converge to a single rod bipolar cell and 100 rod bipolar cells converge to a ganglion cell, then the absolute threshold for vision is determined by the product, approximately 1 photoisomerization per 10,000 rods. Second-OrderNeurons:Horizontaland BipolarCells Rods and cones make synaptic connections with bipolar and horizontal cells. B-type horizontal cells are always smaller and more numerous two to three times the A-type density. In central retina, there are four times as many H1s as H2s, decreasing to twice as many in peripheral retina. Packer and Dacey105 have recorded from many primate H1 cells and they make the interesting observation that central cells are not only smaller but less coupled, perhaps because they overlap less. Thus, the H1 receptive field in the fovea may be small enough, 2030 µm, to match the receptive field surround of midget ganglion cells. Horizontal cells are extensively coupled by gap junctions and their molecular identity has been determined for many species. These gap junctions have different properties so they are likely to be assembled from different connexins. The situation in the primate retina is still unknown but future progress should make it possible to test theories concerning horizontal cell coupling. HorizontalCellFunction There is general consensus that horizontal cells provide negative-feedback signals to cones and rods. This can be seen when a full field light flash, which hyperpolarizes photoreceptors and reduces their glutamate release. This causes a sustained hyperpolarization in the horizontal cells, which rest at a relative depolarized membrane potential in the dark. Upon hyperpolarization, horizontal cells send a feedback signal to the photoreceptors that shifts the activation function of their calcium channels to more negative potentials increasing their calcium current and their glutamate release. TheFeedbackMechanism the mechanism responsible for horizontal cell feedback to cones has been hotly debated for the past two decades. The connexin hemichannels act as large nonselective ion-channels and current flows through them into the resting (~ -40 mV) horizontal cell in the dark. Horizontal cell hyperpolarization to light increases the current through the hemichannels and the extracellular space, producing an even larger local depolarization in the photoreceptor near their calcium channels. As described above, this leads to an increase in calcium current and glutamate release. A role for hemichannels in this process is supported by pharmacologic and genetic manipulations. Here acidification of the extracellular space inhibits photoreceptor calcium channels133 and feedback is modulated by altering the pH in the synaptic cleft, which modulates the calcium current. A series of biotinylated tracers distinguishes three types of gap junction in retina. This disinhibits the photoreceptor calcium current and increases glutamate release from cones. To answer this question, we have to consider how horizontal cells contribute to visual signaling. As pointed out by Sterling, reading highcontrast images in bright artificial light is one thing,143 but in the natural scenes in the outside world visual objects often have very low contrast compared to their background. Here what is needed is a way to subtract the common background (which has little information) and amplify the remaining signal to enhance the visibility of small, low-contrast details. At least in part, this role is accomplished by horizontal cells in the outer retina. Horizontal cells have large receptive fields and are well suited to estimate mean luminance of a scene. An antibody against connexin 50 (green) labels gap junctions in the matrix of A-type horizontal cells. Coupling between A-type horizontal cells is mediated by connexin 50 gap junctions in the rabbit retina. Because our eyes are always moving we need to consider how to extract small, low-contrast details moving against the background. When horizontal cell feedback is slow, the receptive field surround it creates should lag temporally behind the center response in bipolar cells. Responses of neurons become more and more transient when going from the outer retina to the inner retina. Horizontal cells also have an impact on color vision, because they are connected to more than one cone type. This means that the feedback signal cones receive will have a different spectral sensitivity than the spectral sensitivity of the cones themselves. The signals will always be modified by horizontal cell action and thus by the other spectral cone types. The output of a cone will depend on the spectral composition of the global illumination. It has been proposed that these chromatic interactions at the photoreceptor/horizontal cell level lead to phenomena like "color constancy" and "color induction. There are approximately 912 kinds of cone bipolar cell in the mammalian species that have been studied thoroughly, i. Rod bipolar cells are numerous three times the density of any diffuse cone bipolar type. However, there are around 10 types of cone bipolar cell so, in total, they outnumber the rod bipolar cells by a factor of three to four. An increasing number of selective antibodies are now available to aid in the identification of specific cone bipolar cells. J Neurophysiol 1997;77:171630, with permission from the authors and the American Physiological Society. Half the bipolar cells carry signals greater than the local mean and the other half dimmer than the average. J Comp Neurol 2004;474:112, with permission of the authors and Wiley-Liss, a subsidiary of John Wiley. J Comp Neurol 1996;366:1533, with permission of the authors and Wiley-Liss, a subsidiary of John Wiley. A hyperpolarizing response to glutamate is unusual and this is an unusual receptor, which is only expressed in the retina. It has now been identified as mGluR6, one in a series of eight metabotropic glutamate receptors, so called because activation of these receptors turns on an intracellular signaling cascade. Light decreases glutamate release from photoreceptors and produces the opposite response. This mGluR6 pattern also provides a simple way to map the location of rod and cone terminals in the outer retina. The dendrites branch profusely but avoid the cone pedicles within the dendritic field. Instead, all the terminal dendrites invaginate a rod spherule and they are double-labeled for mGluR6. The other half of each mGluR6 doublet is claimed by another unlabeled rod bipolar dendrite. The high convergence allows the rod bipolar cell to collect signals from many rods but is also potentially noisy. However, the rod-to-rod bipolar synapse has a nonlinearity by which small signals are thresholded. Some near-threshold signals may be lost but when a photon signal is captured it has a high signal-to-noise ratio and is transmitted very reliably. They are thought to process signals under slightly different conditions, the primary being the most sensitive and the tertiary being the least sensitive. The conspicuous terminals of rod bipolar cells literally plug into holes in the meshwork of dendrites provided by these amacrine cell types. This is the so-called private line, one cone to one midget bipolar cell to one midget ganglion cell. Most investigators think this specialization of the primate retina was designed to achieve maximum acuity at high cone density. It may also, by virtue of the single cone connections, which are automatically color-coded, serve red/green color vision. Blue Cone Bipolar Cells In general, diffuse cone bipolar cells contact every cone within the dendritic field and this gives them a characteristic appearance. However, in the primate retina, one bipolar cell type is distinctly different in that it has long dendrites that bypass many cones to seek out only blue cones. J Comp Neurol 2004;474:112, with permission from the authors and Wiley-Liss, a subsidiary of John Wiley. J Comp Neurol 2002;448:23048, with permission from the authors and Wiley-Liss, a subsidiary of John Wiley. The source of the bipolar cell glycine was definitively established by blocking gap junctions with carbenoxolone. This changed the labeling pattern for glycine, which was subsequently diminished in bipolar cells. However, the Cx36 knockout may also interfere with rod/cone coupling in the outer retina. It has been suggested that this pathway operates in mesopic conditions of intermediate light intensity, though the primary rod pathway utilizing rod bipolar cells likely continues to function throughout the operating range of rod vision. However, the rod-driven responses persisted even in a transgenic mouse line in which cones were eliminated. In general, the different rod pathways may be designed to cover different intensity ranges and perhaps they are selectively connected to specific ganglion cell types but, as yet, there are no data on this point. There is physiologic evidence from the mouse retina that different ganglion cell types have different intensity response functions but the ganglion cell types have not been identified and the contributing pathways are unknown. J Comp Neurol 2001;436:33650, with permission from the authors and Wiley-Liss, a subsidiary of John Wiley. In general, the three major connections made by amacrine cells are feedback inhibition to bipolar cell terminals, feedforward inhibition to ganglion cells and serial inhibitory connections where amacrine cells are the postsynaptic targets of other amacrine cells. Approximately a quarter of the amacrine cells are wide-field and narrowly stratified with very high coverage as high as 100500. A cell with an overlap this high forms an extremely dense plexus of fine dendrites that blankets the entire retina. Thus, in the rabbit retina, the identification of all the amacrine cell types, started so long ago by Cajal and his contemporaries, is now almost complete. The mouse is probably the next best characterized because of the array of genetic tools that can be used for their analyses. In the case of the rod bipolar cell, feedback is mediated by two amacrine cell types, S1 and S2. Secondly, about half the ganglion cells (approximately eight types) are coupled to one or two amacrine cell types by gap junctions. These two groups need not be mutually exclusive and doubtless amacrine cells have many functions. In another calculation, we estimate there are 15 ganglion cell types forming independent circuits or channels. If each channel required two amacrine cells, that would produce a total of 30 amacrine cell types. While necessarily vague, these simple estimates indicate the variety of amacrine cell types may not be extravagant. General functions attributed to amacrine cells include feedback inhibition, surround inhibition, some forms of adaptation, signal averaging, and noise reduction. This is because a wave of inhibition sweeps the inner retina, like a vertical blank on a television screen. In one study, the inhibitory wave associated with saccades was attributed to wide-field amacrine cells. We know almost nothing except the shape of 75% of the amacrine cells, not their connections, physiology, or circuit functions in other words, little more than Cajal knew 100 years ago. As the means of targeting, imaging, and recording from visually identified cell types improves, we can expect further progress in this area. A major goal of visual neuroscientists is to characterize fully all the amacrine cells and integrate their function into the retinal circuitry. Several amacrine cells have been studied extensively, and their characteristics are described below. It is correctly written with a Roman numeral, which is retained from an early classification scheme, while other numbered amacrine cells use Arabic numerals. These large cells are relatively numerous so the dendritic overlap is huge with coverage factors as high as 500. Although the rabbit retina contains little endogenous serotonin, for some unknown reason these cells take up serotonin.
Molecular phylogenetic analysis of Cyclospora diabetes mellitus descompensada generic 1 mg prandin fast delivery, the human intestinal pathogen diabetes mellitus type 2 and high blood pressure cheap prandin 1 mg with amex, suggests that it is closely related to Eimeria species metabolic disease solutions buy prandin master card. Study of Cyclospora cayetanensis in health care facilities diabetes type 1 reason buy prandin toronto, sewage water blood glucose 313 generic 1 mg prandin amex, and green leafy vegetables in Nepal. The return of Cyclospora in 1997: Another outbreak of cyclosporiasis in North America associated with imported raspberries. Pathologic changes in the small bowel in nine patients with diarrhea associated with a coccidia-like body. Fuchsin fluorescence and autofluorescence in Cryptosporidium, Isospora, and Cyclospora oocysts. Placebo-controlled trial of co-trimoxazole for Cyclospora infections among travellers and foreign residents in Nepal. Treatment and prophylaxis of Isospora belli infection in patients with the acquired immunodeficiency syndrome. Clinical manifestations and therapy of Isospora belli infection in patients with the acquired immunodeficiency syndrome. Prevalence and clinical significance of intestinal microsporidiosis in human immunodeficiency virusinfected patients with and 163. Risk factors for intestinal microsporidiosis in patients with human immunodeficiency virus infection: A case-control study. Entercytozoon bieneusi infection in an immunocompetent patient who had acute diarrhea and who was not infected with the human immunodeficiency virus. Enterocytozoon bieneusi infection in patients who are not infected with human immunodeficiency virus. Improved lightmicroscopical detection of microsporidia spores in stool and duodenal aspirates. Polymerase chain reaction detection of Trypanosoma cruzi in human blood samples as a tool for diagnosis and treatment evaluation. Short report: Comparison of the effects of sublingual nifedipine and isosorbide dinitrate on oesophageal emptying in patients with chagasic achalasia. Modern travel, emigration,1,2 and consumption of "exotic" cuisines allow intestinal helminths to appear in any locale. People now acquire tropical helminths without leaving their industrialized temperate cities. Travel history is a critical, but often overlooked, aspect of the patient interview. Helminths may survive for decades within a host, so even a remote history of visits to or emigration from countries where helminths are endemic is important. Fresh food is flown around the world and often consumed raw, often at a great distance from its original point of origin. Physicians need to remain alert to the possibility of infection with these organisms because some cause severe disease that requires years to develop or occurs only under special circumstances. For example, patients might have occult Strongyloides stercoralis until treatment with glucocorticoids causes fulminant disease, occult Clonorchis sinensis until they develop cholangiocarcinoma, or occult Schistosoma mansoni until they develop portal hypertension and bleeding from esophageal varices. In developed countries, we usually diagnose an intestinal helminth because we stumble across it rather than because we actively pursue it. Helminths are complex organisms well adapted to their hosts; like quiet house guests, most cause no symptoms. Worms rarely cause diarrhea, but many medical laboratories do not assay formed stool routinely for parasite eggs. Physicians need to communicate their concerns of possible helminthic infection to laboratory personnel. A telephone call to the local laboratory before a sample is sent can improve diagnostic results dramatically. Occasionally, alarmed patients bring proglottids or whole worms that they passed with their stools. These specimens should be fixed in 5% aqueous formalin and sent for identification. Some helminthic infections are difficult to diagnose, especially when the worm burden is light. Diagnosis can require serologic evaluation, analysis of multiple stools, or use of concentration techniques in addition to a high level of physician awareness. Ancylostoma caninum causes eosinophilic enteritis but does not lay eggs when infecting people. Most persons colonized with helminths have no symptoms or illness attributable to the parasites. It is even possible that exposure to helminths affords some protection against disease owing to robust immune reactions. This article is divided into 3 sections: nematodes (roundworms), cestodes (tapeworms), and trematodes (flukes or flatworms). For the most part, each worm is addressed separately, noting its epidemiology, life cycle, clinical manifestations, diagnosis, and treatment. The parasite is acquired by ingesting 1969 1970 Section X SmallandLargeIntestine its eggs. Freshly deposited fertilized eggs incubate in the soil for 10 to 15 days while the embryo develops and molts twice, after which the eggs become infective. The eggs are remarkably stable, can survive freezing, and can remain viable for 7 to 10 years. The eggs are resistant to most chemical treatments including pickling, but they rapidly die in boiling water. Once ingested, eggs hatch in the duodenum and release their larvae, which penetrate the intestinal wall and enter the mesenteric venules and lymphatics. Larvae that migrate with portal blood pass to the liver, through the sinusoids to the hepatic veins, and then through the right side of the heart to enter the lungs. Larvae migrating via the lymphatics pass through mesenteric lymph nodes to the thoracic duct and enter the superior vena cava, also to arrive in the lungs. The larvae then lodge in the pulmonary capillaries and break into the alveoli, where they molt twice while growing to 1. Larvae then ascend the tracheobronchial tree, arrive in the hypopharynx, are again swallowed, and pass into the small intestine, where they molt again and finally mature. Because their eggs require incubation in the soil to become infective, Ascaris does not multiply in the host. Surgical specimen showing small intestinal obstruction caused by Ascaris lumbricoides. Ascaris worms can move in and out of the papilla, producing intermittent symptoms and fluctuating laboratory tests. Recurrent ascending cholangitis or acute pancreatitis from ascariasis is rare in highly developed Western countries but can be fatal if the diagnosis is not entertained and treatment is delayed. Most patients do not have specific symptoms or eosinophilia; eosinophilia is absent because the adult Ascaris lives in the intestinal lumen. Fertilized eggs are 35 × 55 µm and have a thick shell and outer layer; females also lay unfertilized eggs that are larger (90 × 44 µm) and have a thin shell and outer layer. Ascaris eggs that lose their outer layer resemble the eggs of hookworms; the outer coating is not necessary for viability and can become easily separated. Often, worms are found unexpectedly on endoscopy21,22 (Video 114-1) or are seen on radiologic imaging,23 or eggs are identified in stool specimens of patients with symptoms not directly attributable to the worms. Disease usually develops only in those with heavy worm burdens: pulmonary, intestinal, and hepatobiliary ascariasis are well described. Pulmonary ascariasis (Ascaris pneumonia) develops 4 to 16 days after ingesting infective eggs. The larvae migrate into the alveoli and elicit an inflammatory response that can cause consolidation. The pneumonia usually is self-limited but can be life-threatening if larvae are numerous. Large numbers of mature worms can cause severe intestinal symptoms including abdominal pain, distention, nausea, and vomiting. The most common complication of intestinal ascariasis is partial or complete small bowel obstruction; such patients often have a history of passing mature worms in their stool or vomitus. Albendazole is poorly absorbed but is still considered possibly teratogenic, and when possible, treatment of pregnant women with this agent should be delayed until after delivery. Previously, clinicians who work in endemic countries would avoid treatment of pregnant women; however, in areas where repeated pregnancy is common, this resulted in prolonged avoidance of potentially life-saving therapy. A recent study of 1257 women treated with albendazole showed no adverse effect of albendazole treatment on birth weight, perinatal mortality, or congenital anomaly compared with placebo. Because albendazole is poorly absorbed, ascaricidal tissue concentrations are not achieved. The first dose kills mature worms that have finished their migration to the intestine, and the second dose kills worms that were in transit when the first dose was given. Albendazole is well tolerated, but can cause nausea, vomiting, and abdominal pain. Surgery is not required unless the patient develops signs of volvulus, intussusception, or peritonitis. Albendazole may be held until after the obstruction has resolved and then is used to eradicate any remaining organisms. Hepatobiliary ascariasis also can be treated conservatively with fluid resuscitation, bowel rest, and antibiotics. This feature of albendazole is advantageous because were paralyzed worms within the duct unable to pass out through the sphincter of Oddi, they could become trapped in the bile duct. Patients with hepatobiliary ascariasis should be treated with albendazole each day for several days, because the worms only become susceptible to the drug after they migrate out of the bile duct. Worms also can invade the pancreatic duct, and intrapancreatic Ascaris can be treated just as hepatobiliary ascariasis. Ampullary sphincterotomy permits worms easier access to the ducts and can increase the risk of recurrent pancreaticobiliary ascariasis. The eggs hatch within the small intestine, and rhabditiform larvae migrate into the lumen. Filariform larvae are able to reinfect (autoinfect) the patient, thereby increasing the parasite burden and permitting prolonged colonization so that subclinical strongyloidiasis can exist for many decades after the host has left an endemic area. Patients with autoinfection, however, might develop a serpiginous urticarial rash (larva currens) caused by the rapid (5 to 10 cm/hour) dermal migration of filariform larvae, usually on the buttocks and resulting from larvae that enter the perianal skin after they exit the anus. Immunosuppression or glucocorticoid administration upsets this balance, with the result that previously asymptomatic, but chronically infested, patients develop fulminant, potentially fatal strongyloidiasis from massive autoinfection. In addition, glucocorticoids can act directly on the parasites to increase the development of infective filariform larvae. Migrating filariform larvae injure the intestinal mucosa and carry luminal bacteria into the bloodstream, resulting in polymicrobial sepsis with enteric organisms. Numerous larvae migrating through the lungs cause pneumonitis, and worms can arrive in unusual locations such as the brain. As a parasite, Strongyloides lives in the intestine and lays eggs that hatch while still in the intestine. Filariform larvae develop within the intestine, migrate along defined paths, and mature to increase the number of adult parasites in the host; this results in prolonged infection that may extend to 75 years after one leaves an endemic area. Strongyloides exists as a free-living organism that does not require a host to replicate. Patients from endemic areas, military veterans who served in Asia, and prisoners of war are at high risk for subclinical strongyloidiasis. Peripheral blood eosinophils may be elevated, but a normal eosinophil count does not argue against infestation with this parasite. Because chronic strongyloidiasis can remain subclinical and difficult to detect for decades, however, treatment of seropositive patients is warranted. Indeed, some argue that patients with only suspected Life Cycle Adult male and female S. Rhabditiform larvae develop in the soil into mature adults to complete the life cycle of this worm. Rhabditiform larvae (250 µm) also can develop into longer (500 µm) infective filariform larvae that can penetrate any area of skin that contacts soil, after which they migrate through the dermis to enter the cutaneous vasculature. The larvae circulate with the venous blood until they reach the lungs, where they break into the alveoli and ascend the bronchial tree. The worms then are swallowed with bronchial secretions and pass into the small intestine, where they embed in the jejunal mucosa and mature. A 10-fold more sensitive technique is to spread stool on an agar plate and look for serpentine tracks left by migrating larvae. Patients rapidly waste from escalating steatorrhea and protein-losing enteropathy. Eventually they manifest emaciation, anasarca, and hypotension; diarrhea produces severe hypokalemia. If untreated, patients die from cardiac failure or secondary bacterial sepsis, usually about 2 months after the initial onset of symptoms. The progressive disease is believed to result from an everincreasing number of poorly adapted intestinal parasites. In autopsy studies, the jejunal intestinal mucosa showed flattened, denuded villi with numerous plasma cells, lymphocytes, macrophages, and neutrophils infiltrating the lamina propria. Ivermectin paralyzes the intestinal adult worms but not the larvae migrating through tissue, and therefore patients can develop recurrent infestation from migrating larvae; a repeat dose after 2 weeks helps to prevent this outcome. Successful treatment causes a fall in antibody titer by 6 months in most (90%) patients. The parasite replicates in the host, producing an ever-increasing number of intestinal worms.
In severe cases diabetes diet guidelines 2013 order 1 mg prandin amex, because mucosal damage may persist for some time even after complete eradication of bacterial overgrowth medications used diabetes cheap generic prandin canada, nutritional support may be required over a prolonged period of time diabetes mellitus without complication buy 2 mg prandin free shipping. In these instances diabetes insipidus risk factors generic prandin 0.5 mg amex, the diagnostic and therapeutic approaches have been rather well developed and blood glucose ketones prandin 2 mg buy lowest price, to some degree, validated. Celiac disease: Management of persistent symptoms in patients on a gluten-free diet. Review article: Small intestinal bacterial overgrowth, bile acid malabsorption and gluten intolerance as possible causes of chronic watery diarrhoea. Methodology and indications of H2 breath testing in gastrointestinal diseases: the Rome Consensus Conference. Normal bacterial populations of the intestine and their relation to intestinal function. Small intestinal bacterial overgrowth in patients with cirrhosis: Prevalence and relation with spontaneous bacterial peritonitis. Bacterial populations contaminating the upper gut in patients with small intestinal overgrowth syndrome. Lactose intolerance in patients with chronic functional diarrhea; the role of small intestinal bacterial overgrowth. Small intestinal bacterial overgrowth and thiamine deficiency after Roux-en-Y gastric bypass surgery in obese patients. Endogenous ethanol production in a patient with chronic intestinal pseudo-obstruction and small bowel bacterial overgrowth. Small intestinal bacterial overgrowth in human cirrhosis is associated with systemic endotoxemia. The rate of bloodstream infection is high in infants with short bowel syndrome: Relationship with small bowel bacterial overgrowth, enteral feeding and inflammatory and immune responses. A case of non-alcoholic steatohepatitis and small intestinal bacterial overgrowth with peripheral edema caused by intestinal bypass surgery and relived by repair. Reactivation of arthritis induced by small bowel bacterial overgrowth in rates: Role of cytokines, bacteria and bacterial polymers. The interdigestive motor complex of normal subjects and patients with bacterial overgrowth of the small intestine. Evidence of prolonged oro-cecal transit time and small intestinal bacterial overgrowth in acromegalic patients. Patients with chronic renal failure have abnormal small intestinal motility and a high prevalence of small intestinal bacterial overgrowth. Jejunal diverticulosis: A heterogeneous disorder caused by a variety of abnormalities of smooth muscle or myenteric plexus. The metabolic and nutritional consequences of bacterial overgrowth in the small intestine. Increased incidence of small intestinal bacterial overgrowth during proton pump inhibitor therapy. Proton pump inhibitor use and the risk of small intestinal bacterial overgrowth: A meta-analysis. Proton pump inhibitor therapy use does not predispose to small intestinal bacterial overgrowth. Chronic diarrhea and malabsorption due to hypogammaglobulinemia: A report of twelve patients. Partially responsive celiac disease resulting from small intestinal bacterial overgrowth and lactose intolerance. High prevalence of small intestinal bacterial overgrowth in celiac patients with persistence of gastrointestinal symptoms after gluten withdrawal. Prevalence of small intestine bacterial overgrowth diagnosed by quantitative culture of intestinal aspirate in celiac disease. Double-blind randomized controlled trial of rifaximin for persistent symptoms in patients with celiac disease. Oral antibiotic therapy improves fat absorption in cystic fibrosis patients with small intestine bacterial overgrowth. Small intestinal bacterial overgrowth is frequent in cystic fibrosis: Combined hydrogen and methane measurements are required for its detection. Small intestinal bacterial overgrowth: Roles of antibiotics, prebiotics and probiotics. Diagnosis and pharmacological management of small intestinal bacterial overgrowth in children with intestinal failure. Small intestinal motility disturbances and bacterial overgrowth in patients with liver cirrhosis and portal hypertension. Small-intestinal bacterial overgrowth in cirrhosis is related to the severity of liver disease. Role of small intestinal bacterial overgrowth and delayed gastrointestinal transit time in cirrhotic patients with minimal hepatic encephalopathy. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Small intestinal bacterial overgrowth in rosacea: Clinical effectiveness of its eradication. Small intestinal bacterial overgrowth in patients with interstitial cystitis and gastrointestinal symptoms. Restless legs syndrome in patients with irritable bowel syndrome: Response to small intestinal bacterial overgrowth therapy. Leukocyte-subset counts in idiopathic parkinsonism provide clues to a pathogenic pathway involving small intestinal bacterial overgrowth. High prevalence of small intestinal bacterial overgrowth in patients with morbid obesity: A contributor to severe steatosis. Eradication of small intestinal bacterial overgrowth reduces symptoms of irritable bowel syndrome. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome: A double-blind, randomized, placebo-controlled study. Prevalence of small intestinal bacterial overgrowth in children with irritable bowel syndrome: A case-control study. Small intestine bacterial overgrowth and irritable bowel syndrome-related symptoms: Experience with rifaximin. Breath test for differential diagnosis between small intestinal bacterial overgrowth and irritable bowel disease: An observation on non-absorbable antibiotics. Comparison of lactulose and glucose breath test for diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Lactulose breath testing does not discriminate patients with irritable bowel syndrome from healthy controls. A 51-year-old with irritable bowel syndrome: Test or treat for bacterial overgrowth Bacterial overgrowth and irritable bowel syndrome: Unifying hypothesis or a spurious consequence of proton pump inhibitors Questioning the bacterial overgrowth hypothesis of irritable bowel syndrome: An epidemiologic and evolutionary perspective. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: A randomized trial. Bacterial contamination of the small intestine is an important cause of occult malabsorption in the elderly. Clinical predictors of small intestinal bacterial overgrowth by duodenal aspirate culture. Small intestinal bacterial overgrowth: Histopathologic features and clinical correlates in an underrecognized entity. Fecal calprotectin concentrations in patients with small intestinal bacterial overgrowth. Bacterial flora of the gastrointestinal tract in southern Indian control subjects and patients with tropical sprue. Diagnosis of bacterial overgrowth after culturing proximal small-bowel aspirate obtained during routine upper gastrointestinal endoscopy. Bacteriologic analysis of mucosal biopsy specimens for detecting small-intestinal bacterial overgrowth. A systematic review of diagnostic tests for small intestinal bacterial overgrowth. Simultaneous culture of saliva and jejunal aspirate in the investigation of small bowel bacterial overgrowth. Techniques used to characterize the intestinal microbiota: A guide for the clinician. Detection of bacterial deconjugation of bile salts by a convenient breath-analysis technic. Comparison of the one-gram d-[14C]xylose breath test to the [14C]bile acid breath test in patients with small-intestine bacterial overgrowth. Limitations in the use of 14C-glycocholate breath and stool bile acid determinations in patients with chronic diarrhea. Xylose catabolism in the experimental rat blind loop syndrome: Studies, including use of a newly developed d-[14C]xylose breath test. Detection of small intestine bacterial overgrowth by means of a 14C-d-xylose breath test. Comparison of the 1-gram [14C]xylose, 10-gram lactulose-H2, and 80-gram glucose-H2 breath tests in patients with small intestine bacterial overgrowth. Reduced accuracy of 14C-d-xylose breath test for detecting bacterial overgrowth in gastrointestinal motility disorders. Breath testing to evaluate lactose intolerance in irritable bowel syndrome correlates with lactulose testing and may not reflect true lactose malabsorption. Abnormal breath tests to lactose, fructose and sorbitol in irritable bowel syndrome may be explained by small intestinal bacterial overgrowth. Extra intestinal influences on exhaled breath hydrogen measurements during the investigation of gastrointestinal disease. Fasting breath hydrogen concentrations in gastric and smallintestinal bacterial overgrowth. Use of pulmonary hydrogen (H2) measurements to quantitate carbohydrate absorption. Reliability and reproducibility of breath hydrogen and methane in male diabetic subjects. The lactulose hydrogen breath test as a diagnostic test for small-bowel bacterial overgrowth. A randomized double-blind placebo-controlled trial of rifaximin in patients with abdominal bloating and flatulence. Utility of hydrogen breath tests in diagnosis of small intestinal bacterial overgrowth in malabsorption syndrome and its relationship with oro-cecal transit time. Diagnosis of small intestinal bacterial overgrowth in children: the use of lactulose in the breath hydrogen test as a screening test. Bacterial overgrowth without clinical malabsorption in elderly hypochlorhydric subjects. Urinary indican as a screening index of jejunal bacterial flora in Indian adulthood cirrhosis. Critical evaluation of diagnosing bacterial overgrowth in the proximal small intestine. Antibiotic therapy in small intestinal bacterial overgrowth: Rifaximin versus metronidazole. Efficacy of rifaximin, a nonabsorbed oral antibiotic, in the treatment of small intestinal bacterial overgrowth. Clinical trial: the combination of rifaximin with partially hydrolysed guar gum is more effective than rifaximin alone in eradicating small intestinal bacterial overgrowth. Specific areas of absorption of dietary constituents and secretions in the small intestine and colon. Macronutrients and micronutrients are absorbed predominantly in the proximal jejunum. The 3 common types of intestinal resection and anastomosis observed in patients with Short Bowel Syndrome: ileocolonic anastomosis, jejunocolonic anastomosis, and end-jejunostomy. Loss of Absorptive Surface Area Nutrient Malabsorption the length of the small intestine is estimated at 3 to 8 meters, and nutrient absorption is preserved until more than one half of the small intestine is resected. Enterocytes lining the small intestine appear uniform from the duodenum to the ileocecal valve, but a distinct proximal-to-distal gradient exists in both morphology and function. The ileum, however, eventually is able to compensate for jejunal loss, whereas the jejunum is unable to compensate for ileal absorption of bile salts and vitamin B12. Normal digestion and absorption depend on the gradual gastric emptying of partially digested nutrients, mixing of these nutrients with bile and pancreatic enzymes in the duodenum, and rapid digestion and absorption of the digestive products in the proximal small intestine. Rapid intestinal transit decreases nutrient-enterocyte contact time, and therefore, segmental absorption is decreased. Patients with a proximal jejunostomy are net secretors of salt and fluid, because jejunal fluid secretion is stimulated by oral intake and subsequent gastric emptying of nutrients; these patients excrete more fluid than they ingest and absorb, and accordingly, their fluid management may be challenging. Preservation of even some colon at surgery is highly beneficial for nutrient absorption. Moreover, the ileocecal valve acts as a brake to slow intestinal transit, thereby increasing nutrient-enterocyte contact time and enhancing absorption. It has been estimated that this intracolonic digestive process can generate up to 1000 kcal (4. Role of the colon as an important digestive organ in patients with short bowel syndrome. The proximal small bowel receives approximately 7 to 9 L daily of water and electrolytes from food and secretions each day, of which 6 to 8 L are reabsorbed (see Chapter 101). On unrestricted diets, patients with a proximal jejunostomy cannot reabsorb such large volumes, a consequence of which is that voluminous diarrhea develops, often complicated by hypovolemia, hyponatremia, and hypokalemia. For example, in 1 study,12 the diarrheal volume in 6 jejunostomy patients with a mean jejunal length of 50 cm ranged from 3. In the same study, 7 of 9 other jejunostomy patients who had a mean jejunal length of 120 cm were able to maintain positive water and sodium balance under the same conditions; absorption of water, sodium, and potassium in these 15 jejunostomy patients was correlated with jejunal length.
It may be caused by a disturbance in the arterial supply or venous drainage of the bowel and involve the small intestine diabetes insipidus in spanish purchase prandin paypal, colon diabetes insipidus kidney stones buy prandin 2 mg line, or both type 1 diabetes xanax discount 0.5 mg prandin visa. The common hepatic artery gives rise to the gastroduodenal syndrome x type 2 diabetes purchase prandin with a visa, right gastroepiploic diabetes insipidus nephrogenic cheap prandin 0.5 mg buy line, and anterior superior pancreaticoduodenal arterial branches. The splenic artery gives off pancreatic and left gastroepiploic arterial branches. It gives rise to 5 major vessels: the anterior and posterior inferior pancreaticoduodenal vessels, middle colic, right colic, and ileocolic arteries, as well as to a series of jejunal and ileal branches, all of which supply their named portions of intestine. Celiac and superior mesenteric arteries: A correlation of angiograms and dissections. It branches into the left colic artery, gives off multiple sigmoid branches, and terminates as the superior rectal artery. The distal rectum is supplied by branches of the internal iliac (hypogastric) artery. These vessels constitute the pancreaticoduodenal arcade and provide blood to the duodenum and pancreas. The splenic flexure and sigmoid colon have limited anastomoses, and ischemic damage is more common in these locations. Remarkably, the bowel can tolerate a 75% reduction of mesenteric blood flow and oxygen consumption for 12 hours with no changes on light microscopy, because only one fifth of the mesenteric capillaries are open at any time, and when oxygen delivery is decreased, the bowel adapts by increasing oxygen extraction. When a major vessel is occluded, collaterals open immediately in response to the drop in arterial pressure distal to Collateral and Anastomotic Circulation Abundant collateral circulation to the stomach, duodenum, and rectum accounts for the paucity of ischemic events in these areas. The presence of a prominent meandering artery indicates that collateral channels have been present for some time and occlusion is not acute. After several hours of ischemia, however, vasoconstriction develops in the obstructed bed, elevating its pressure and reducing collateral flow. If sustained for a prolonged period, the vasoconstriction can become irreversible and persist even after correction of the cause of the ischemic event. Such persistent vasoconstriction explains the operative findings of progressive bowel ischemia after cardiac function has been optimized and in the absence of arterial or venous obstruction. Blood flow is affected by a variety of systemic, humoral, local, and neural influences. Ischemic damage results both from hypoxia during the period of ischemia and reperfusion injury when blood flow is reestablished. More reinjury from brief ischemia appears during reperfusion, but as the ischemic period lengthens, hypoxia becomes more detrimental than reperfusion3; the injury after 3 hours of ischemia and 1 hour of reperfusion is more severe than that after 4 hours of ischemia. Reperfusion injury has been attributed to many factors, but particularly to reactive oxygen- and nitrogen-derived free radicals that can damage an array of molecules found in tissues, including nucleic acids, membrane lipids, enzymes, and receptors. Such widespread damage can result in the mucosal barrier being compromised through cell lysis, impaired cell function, and necrosis on reperfusion of ischemic tissues. The adherent leukocytes mediate microvascular injury by release of proteases and physical disruption of the endothelial barrier. In the acute forms, intestinal viability is threatened, whereas in the chronic forms, blood flow is inadequate to support the functional demands of the intestine. Regardless of the cause of the ischemic insult, the end results are similar: a spectrum of bowel injury that ranges from transient alteration of bowel function to transmural gangrene. Clinical manifestations vary with the extent and severity of ischemic injury and, to a lesser degree, with its cause. Initially, the pain is severe, but the abdomen usually is flat, soft, and sometimes not tender, or certainly less tender than expected based on the magnitude of the pain. The classic description of "pain out of proportion to abdominal findings" seems less accurate than previously believed, with only an estimated 29% of patients having this finding in the decade spanning from 2000 to 2010. Although abdominal findings early in the course of intestinal ischemia may be minimal or absent, increasing tenderness, rebound tenderness, and muscle guarding reflect progressive loss of intestinal viability. There is no serum marker yet demonstrated to be reliable to diagnose early ischemic bowel injury. In one study, the mortality rate of patients with normal plain film studies was 29%, whereas it was 78% in those with abnormal findings. Plain film of the abdomen showing an ileus and a formless fixed loop of small intestine (arrows) in a patient with acute mesenteric ischemia from a superior mesenteric artery embolus. Pneumatosis intestinalis (linearis) is a late sign of ischemic injury, connotes bowel necrosis, and mandates explorative laparotomy. Chapter 118 IntestinalIschemia 2081 models show that the mesentery is the first area to react to both arterial and venous compromise. Selective mesenteric angiography is also an invasive procedure with attendant risks and might delay surgical intervention if not readily available. Laparoscopy may be useful, but it too can be misleading because early in ischemic injury, blood flow may be shunted to the serosa, giving it a normal appearance even when the mucosa is necrotic. A total of 9 "first-looks" and 3 "second-looks" were performed, and the outcomes and complication rates were similar to a cohort of 8 patients who did not undergo diagnostic laparoscopy. The authors concluded that diagnostic laparoscopy was feasible, was safe, and had low invasiveness. Duration of symptoms parallels mortality, so early diagnosis and treatment are paramount to increasing the chance for survival. Less absolute indications for inclusion into this protocol consist of unexplained acute abdominal distention, colonoscopic evidence of isolated right-sided colonic ischemia, and acidosis without an identifiable cause. Resuscitation includes relief of acute congestive heart failure and correction of hypotension, hypovolemia, and cardiac arrhythmias. Ideally, patients are studied before (specific) radiologic signs appear, because these signs connote irreversibly damaged bowel. Even when the decision to operate has been based on clinical grounds, preoperative angiography should be performed, if possible, to manage the patient properly at and after laparotomy. One study assembled a team including gastroenterologists, vascular and abdominal surgeons, radiologists, and intensive care specialists, with a plan for all patients to undergo "medical management," including endovascular interventions. This multidisciplinary approach resulted in 95% survival at 30 days and 89% survival at 2 years. Solid lines show the conventional management plan; dotted lines show an alternative management plan. Gastroenterology 2000; 118:954; corrected version in Gastroenterology 2000; 119:281. The papaverine is infused by pump at a constant rate of 30 to 60 mg/hr; papaverine concentrations may vary with the need for fluid restriction. Angiographers can also attempt to intervene on the vascular occlusion directly as a surgery-sparing measure; several small studies and case series have shown this approach to have excellent success. The methodology used is based on the mechanism of the ischemia, the length of the occlusion, and the appearance of the underlying and distal arteries. Using an antegrade approach via the femoral artery, a guiding catheter is placed within the embolus, and a syringe is used to suction it simultaneously with sheath withdrawal; several passes are usually required to completely remove the embolus. This technique is used as an adjunct when there is low suspicion for transmural intestinal infarction and most of the clot was able to be removed via aspiration embolectomy. The number of stents used depends on the size of the lesion, and following stent placement the pressure gradient across the lesion is measured. If the pressure gradient is greater than 12 mm Hg there is a high risk of restenosis, and further intervention is required. Embolectomy, thrombectomy, or arterial bypass precedes evaluation of intestinal viability, because bowel that initially appears infarcted can show surprising recovery after adequate blood flow has been restored. Short segments of bowel that are nonviable or questionably viable after revascularization are resected, and a primary anastomosis is performed. If extensive portions of the bowel are of questionable viability, only the clearly necrotic bowel is resected, and re-exploration ("second look") is planned for within 12 to 24 hours. The interval between the first and second operations is used both to allow better demarcation between viable and nonviable bowel and to attempt to improve intestinal blood flow by using intra-arterial papaverine and maximizing cardiac output. Angiography typically reveals a rounded filling defect with nearly complete obstruction to flow. Emboli proximal to the origin of the ileocolic artery are considered major emboli. Exploration is usually performed in patients with major emboli after papaverine infusion is begun. The decision of whether to attempt endovascular treatment in patients with major emboli is dependent upon the skills of the endovascular interventionalist available at each medical center. Exploratory laparotomy is mandatory when peritonitis is present; embolectomy and bowel resection are performed as necessary. If possible, intra-arterial papaverine is begun before surgery and continued during surgery. If a second operation is planned, the infusion is continued through the second procedure until angiography shows the vasoconstriction has ceased. Vasodilatation is seen, and all vessels are patent except for a distal jejunal branch, which contains a piece of the inciting embolus (arrowhead) that broke off during the course of vasodilator therapy because of endogenous thrombolysis. Papaverine protected the bowel within the distribution of the embolized vessel by enabling vasodilatation and maintenance of adequate blood flow. The patient was operated on after 54 hours of papaverine, and it was confirmed that all the bowel appeared healthy and free of ischemic necrosis. Prospective studies and meta-analyses have shown that thrombolysis may be effective in resolving thrombi, improving symptoms, and avoiding surgery in patients with lesions amenable to such therapy. When streptokinase and papaverine were administered simultaneously, neither medication functioned as well as it did alone, and intestinal damage was intensified. The second portion of this study used these criteria to analyze 9 subsequent patients. If this is unsuccessful, papaverine infusion is begun before surgery is undertaken. At surgery, necrotic bowel is resected, and the remaining bowel is revascularized. A B Complications Complications of angiography and prolonged infusion of vasodilator drugs include transient acute tubular necrosis following angiography, local hematomas at the arterial puncture sites, catheter dislodgment, and fibrin clots on the arterial catheter. B, Marked vasodilatation is evident on repeat study after 48 hours of intra-arterial papaverine infusion. Operation is performed if peritoneal signs are present, and the infusion is continued during and after exploration. Necrotic bowel is resected; it is better to leave bowel of questionable viability and perform a second-look operation than to perform massive enterectomy, because compromised but viable bowel often improves with supportive measures. Infusions, usually discontinued after 24 hours, have been given for as long as 5 days. Evidence of coronary, cerebrovascular, or peripheral arterial insufficiency is common. Branches proximal and distal to the obstruction can show localized or diffuse vasoconstriction. However, the discoveries of primary and secondary hypercoagulable states and the use of estrogens for contraception and hormone replacement have led to more frequent identification of cause. Despite an extensive list of potential causes and risk factors, 21% to 49% of cases are still classified as idiopathic. The acuity of symptom onset and presentation is based on the nature of the thrombotic event. Transmural infarction can make it impossible to differentiate venous from arterial occlusion. Clinical features are determined by the location and timing of thrombus formation within the mesenteric vasculature, as mentioned above. The mean duration of pain before admission is 5 to 14 days but may be prolonged in as many as 25% of patients. Initial physical findings vary at different stages and with different degrees of ischemic injury, but guarding and rebound tenderness develop as bowel infarction evolves. The diagnosis is usually made on imaging studies ordered to evaluate the cause of undiagnosed pain. At autopsy, coexistent new and old thromboses have been found in nearly half of the patients. Characteristic findings on small bowel series include marked thickening of the bowel wall due to congestion and edema, with separation of loops and thumbprinting. Endoscopy and appropriate imaging studies should identify the cause and site of bleeding and the extent of thrombosis. The wall of the vein is sharply defined, with a rim of increased density surrounding the thrombus (arrows). In symptomatic patients, treatment is determined by the presence or absence of peritoneal signs; signs of peritonitis mandate laparotomy and resection of infarcted bowel. Immediate heparinization for 7 to 10 days has been shown to diminish recurrence and progression of thrombosis and improve survival. This technique decreased symptoms, mortality and the requirement for surgical intervention. Surgery might be considered for patients who are not good candidates for anticoagulation alone. Current recommendations for the duration of anticoagulation are not supported by evidence-based data, but rather are based on conventional practice. If an underlying hypercoagulable state is found, lifelong anticoagulation therapy is advised. If no underlying thrombophilic state is documented, a 3- to 6-month course of therapy is thought to be sufficient. Biopsies of affected regions are characterized by thickening of venous walls with calcification, marked submucosal fibrosis, deposition of collagen in the mucosa, and foamy macrophages in the vessel walls. Mild symptoms usually are self-limited, whereas severe symptoms may require hemicolectomy. Physical findings are those of an acute abdomen, and an inflammatory mass may be palpated.
Diagnosis the diagnosis of diversion colitis is based on the clinical picture and endoscopic and histologic findings diabetes test kit carrying case order 1 mg prandin amex. Lymphoid hyperplasia occurs in both disorders but tends to be more prominent in diversion colitis blood sugar 34 cheap prandin 2 mg buy on line. Pathology A spectrum of histologic changes has been described in diversion colitis diabete type 1 cure prandin 2 mg otc, ranging from lymphoid follicular hyperplasia and mixed mononuclear and neutrophilic infiltration to severe inflammation with crypt abscesses diabetic dog treats purchase prandin discount, mucin granulomas diabetic juicing recipe purchase prandin, and Paneth cell metaplasia32,33; large ulcers and transmural changes are absent, and crypt architecture generally is preserved. After extended periods following diversion, inflammatory pseudopolyps and strictures may develop. Treatment the preferred treatment of diversion colitis is surgical restoration of colonic continuity; this rapidly reverses symptoms and histologic changes. One report suggested that intraluminal irrigation with soluble and insoluble fiber solutions improved endoscopic and histologic abnormalities and might be useful to reduce inflammation prior to surgical restoration of bowel continuity. A large review of the literature encompassed 127 patients and indicated that colonic ulcers occur at any age, with a peak incidence in the fourth and fifth decades and a slight female predominance. Diagnosis Historically, nonspecific colonic ulcers usually were diagnosed at laparotomy after complications occurred. With the advent of endoscopy, many colonic ulcers are now diagnosed preoperatively and, in some cases, managed conservatively. Roentgen findings are nonspecific, however, and diagnostically inferior to direct inspection by colonoscopy. Hypotheses that have been advanced, but with little or no supporting evidence, include ischemia, cecal diverticulosis, and acidpeptic disease. Clinical Features the most frequent presenting symptoms are abdominal pain and bleeding. More than one half of patients with nonspecific colon ulcers present with acute or chronic abdominal pain, often in the right lower abdomen and mimicking appendicitis. The most common surgical procedures are local excision of the ulcer, oversewing of the ulcer if there is significant bleeding, and occasionally more extensive resections of the affected colon. Characteristic changes are not always found throughout the colon, and there is a predilection for involvement of the ascending colon. Pathologic changes in resected specimens of cathartic colon have included mucosal atrophy, chronic inflammation with thickening of the muscularis mucosae, submucosal fatty infiltration, and mild fibrosis. Irreversible strictures and degenerative changes in intestinal neurons are absent. Neuronal changes have been found in patients with chronic laxative abuse, but these patients did not exhibit cathartic colon as defined here. In the colon, Dieulafoy-type lesions appear to have a strong male predominance and have been reported in all age groups. The submucosal artery is tortuous and hypertrophic, curving toward the mucosa with persistence of caliber. Inflammation is absent, and the solitary mucosal ulceration extends no deeper than the upper submucosal layer of colon. Colonoscopy can identify the lesion in some cases52 but is often difficult or impossible, especially when bleeding continues or thorough cleansing of the colon cannot be accomplished. Selective mesenteric angiography is the diagnostic study of choice, and surgical resection has been the principal form of therapy. Even after angiographic detection of the bleeding site, precise localization of the lesion is frequently difficult, and more extended resection often is required. In some cases, colonic lesions appear as pseudopolyps, and successful treatment with sclerotherapy, electrocautery, or hemoclipping may obviate the need for surgery. Subsequent studies have reported changes in colonic epithelial cells and in the submucosa of patients with long-term laxative abuse, and both anthraquinones and bisacodyl have been implicated; however, the unclear nature and duration of laxative use and the inability to exclude preexisting conditions make the significance of these observations uncertain. Studies in rodents and in chronically constipated women do not support a deleterious effect of anthraquinones on the ultrastructure of colonic nerves,57 nor is there evidence to suggest that sennosides, bisacodyl, or related substances cause significant morphologic damage to the colonic enteric nervous system in either experimental animals or humans. In the more severe cases, electrolyte and fluid abnormalities such as hypokalemia and hypovolemia are associated with excessive thirst and weakness. In 1943, Heilbrun first described radiologic abnormalities of the colon and terminal ileum associated with prolonged abuse of irritant cathartics. It is important to emphasize that the term cathartic colon is based on barium enema characteristics and is not synonymous with prolonged use of laxatives or with laxative abuse. Indeed, misapplication of the term cathartic colon has led to inappropriate concerns over the chronic use of laxatives that, when used appropriately, is not associated with structural or functional damage to the colon. Cathartic colon is not the inevitable consequence of chronic laxative abuse, which may be associated with a variety of reversible symptoms as well as fluid and electrolyte abnormalities. In a review of 240 cases of chronic laxative abuse published in more than 70 reports, no case of cathartic colon was demonstrated. Although often thought to be irreversible, there is evidence that cathartic colon can partially or completely reverse after withdrawal of laxatives. In severe or refractory cases, subtotal colectomy or proctocolectomy has been effective. The cathartic colon is of historic interest and is unlikely to be identified in current clinical practice. The term cathartic colon should not be confused with "chronic laxative abuse syndrome," nor should the term imply that current laxatives are dangerous if used chronically but appropriately. A colonoscopic view of pseudomelanosis coli associated with the chronic use of senna laxatives in a patient with ulcerative proctitis. There is little or no pseudomelanin pigment (lipofuscin) in the distal 30 cm of colon where there is active mild colitis (left), in contrast to the heavy pigmentation in the remaining colon (right). First described in the early 19th century, the term melanosis coli was coined by Virchow in 1857 because the pigment was considered to be melanin or a melanin-like substance. Subsequently, histochemical and ultrastructural analysis proved the pigment to be not melanin, but lipofuscin, a "wear-and-tear" pigment that is composed of lipid-containing residues of lysosomal digestion. The association between pseudomelanosis coli and chronic use of anthraquinone laxatives is established firmly and is supported further by the development of characteristic pigmentation in laboratory animals after administration of anthraquinones. The condition is widely regarded as benign and reversible, and disappearance of the pigment generally occurs within a year of stopping laxatives. The pigment in pseudomelanosis coli is now thought to originate from either macrophages or organelles within epithelial cells after damage by anthraquinone laxatives, which causes cells to die by apoptosis. Such a sequence of damage has been demonstrated in guinea pigs exposed to anthraquinones. Abnormalities of colonic epithelial cells are noted on electron microscopy but not on light microscopy. Colonoscopic view of a colonic cancer that is pale and thus easily seen in contrast against the dark background of pseudomelanosis. The severity of the reaction depends on the type and concentration of the substance, the duration and extent of its contact with the mucosa, and perhaps the presence of underlying colonic disease. These agents produce liquefaction necrosis with mild to severe inflammation and saponification of the layers of the colon wall. Acute histologic changes include necrosis, leading, in more severe cases, to ulceration and formation of granulation tissue. Acute colitis may heal without residua or with fibrosis and scarring or progress to transmural necrosis and perforation. The severity of damage probably is related to the concentration of soap and duration of mucosal contact. Endoscopic findings have ranged from loss of the normal mucosal vascular pattern to aphthae to mucosal sloughing and ulceration. Hydrogen peroxide enemas are no longer frequently used, but at one time they were employed to relieve meconium ileus and to remove fecal impactions. There are reports of severe damage associated with use of hydrogen peroxide, including severe colitis, pneumatosis coli, perforation, sepsis, and death. Damage is believed to occur because of the hypertonicity of these agents, but the addition of Tween 80 to hyperosmolar agents to improve mucosal contrast may have contributed to mucosal damage because of its detergent properties. Most reports of injury have occurred in the colon proximal to an obstruction and mainly in the right colon, which suggests that prolonged contact with these agents predisposes to mucosal injury. Colonoscopic view of hydrogen peroxide colitis in a patient to whom hydrogen peroxide was given to help remove a fecal impaction. Both panels show the so-called snow-white sign, referring to the appearance of the stark white necrotic mucosa. Endoscopic view of glutaraldehyde colitis in a young man who had had a normal colonoscopy 3 hours before this photograph was taken. The colitis was caused by glutaraldehyde that had been used to disinfect the flexible sigmoidoscope after its previous use but had not been sufficiently cleansed from the instrument. He complained of "agonizing" pain during the sigmoidoscopic examination and began to pass bright red blood 2 hours later. Forced-air drying and rinsing of endoscope channels and the exterior of the instrument should ensure a chemical-free procedure. Patients and health care professionals should be cautioned that soapsuds enemas should not be used. Rectal instillation of substances for medicinal or ritualistic activities other than commercially available enemas should be discouraged. Surgery may be indicated in severe cases of bowel necrosis leading to gangrene or perforation. Indeed, high hydrogen content in the cysts has been documented,84 and cysts regress in patients fed an elemental diet to decrease the carbohydrate substrate for colonic bacteria. It has been hypothesized that gas cysts form by counterperfusion supersaturation of H2 gas by which super H2 production by colonic bacteria provides the condition for H2 tension in the colonic lumen to approach the level of N2 tension in the blood. In 1 study, stools from patients with pneumatosis coli were demonstrated to lack 2 major species of hydrogen-consuming bacteria. This uncommon disorder is characterized by multiple gas-filled cysts that are located in the submucosa and subserosa of the intestine. The most common symptoms are diarrhea (68%), mucus discharge (68%), rectal bleeding (60%), and constipation (48%). Physical examination may reveal an abdominal mass, and careful rectal examination may enable palpation of the cystic lesions. A plain abdominal film may identify radiolucent clusters or streaks along the bowel wall with pneumoperitoneum, if a cyst has ruptured. According to the mechanical theory, intraluminal gas enters the bowel wall under pressure through a defect or potential defect in the intestinal mucosa. The mucosal defect may result from direct trauma or increased intraluminal pressure. The plausibility of this theory, however, is diminished by the absence of a connection between the mucosa and the cysts and the presence of elevated levels of hydrogen gas in the cysts. This theory has been supported by clinical observations and laboratory experiments. They do not communicate with the intestinal lumen or with each other and have a spongy consistency that pops like a balloon when compressed. On cross-section they appear shiny and honeycombed, and range in size from a few millimeters to several centimeters. Single-contrast barium enema demonstrating the presence of gas-filled cysts in the wall of the colon (arrowheads) characteristic of pneumatosis coli. Histopathology of a large gas-filled cyst in the submucosa of the colon from a patient with pneumatosis coli. Mucosal changes vary from mild focal abnormalities to extensive changes including granulomas, abnormal crypts with branching, shortening, cryptitis and abscesses, dilatation, and rupture. Progressive fibrosis leads to a decrease in the size of the cysts and ultimately to their obliteration. The connective tissue surrounding the cysts may show a granulomatous inflammatory reaction made up of eosinophils, lymphocytes, macrophages, and plasma cells. Symptomatic patients may be treated successfully by breathing high-flow oxygen for several days or by use of hyperbaric oxygen, especially in resistant cases87; high oxygen levels lead to replacement of hydrogen by oxygen within the cysts and a corresponding reduction in their size. Because cysts may recur after oxygen therapy, a minimum of 48 hours of oxygen therapy is recommended to maximize the success rate. Metronidazole also has been used to treat pneumatosis coli, an observation that suggests that anaerobic bacteria play a role in the genesis of the disorder. Because cysts have been reported to recur after short courses of metronidazole, treatment should continue until complete resolution of the cysts is seen. In general, colonic resection is reserved for patients with complications such as intestinal obstruction and massive bleeding. Reversal of both macrophage abnormalities and clinical symptoms occurred after discontinuation of glucocorticoids and azathioprine. A possible genetic etiology was suggested by 1 report of colonic malakoplakia that clustered in a family. One of the histiocytes shows the characteristic ring-like MichaelisGutmann body (arrow), consisting of a central core of partially digested bacteria coated with iron and calcium phosphate. Diagnosis is by colonoscopy and biopsy, which generally reveal the following 3 patterns of the disease: 1. Diffuse colonic involvement, which is characteristic of immunosuppressed patients 3. Histology reveals the characteristic macrophages with voluminous cytoplasm that contains the classic von Hansemann histiocytes (intracellular organisms) and Michaelis-Gutmann bodies (intracytoplasmic concentric laminated inclusion bodies). The most common sites of colonic involvement are the rectum, sigmoid, and right colon, in descending order of frequency. Proposed etiologies are infection, immunosuppression, systemic illness, neoplasia, and a genetic disorder. Evidence for an infectious etiology is based on the finding that some patients with malakoplakia have associated chronic infections.
1 mg prandin purchase with mastercard. How to Make Healthy Tuna Salad| The Stay At Home Chef.
References
- Green DM, Breslow NE, Beckwith JB, et al: Screening of children with hemihypertrophy, aniridia, and Beckwith-Wiedemann syndrome in patients with Wilmsi tumor: a report from the National Wilms Tumor Study, Med Pediatr Oncol 21:188n192, 1993.
- Baumer JH, Jones RWA: Urinary tract infection in children, National Institute for Health and Clinical Excellence, Arch Dis Child Educ Pract Ed 92(6):189- 192, 2007.
- Beasley MB. Smoking-related small airway disease - a review and update. Adv Anat Pathol 2010;17:270-6.
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 1965;64:31-49.